
Crohn’s diseasethe new challenge
Dr .Nahla A Azzam (MRCP)GI/ Medicine Consultant
KKUH

Objectives
-overview on the pathogenesis of CD
-Treatment options
-CD management approach
-Prevalence of CD in Saudi Arabia
-KKUH experience

Pathogenesis

Genetic SusceptibilityChromosome 1, 3, 7, 12, 16Chromosome 1, 3, 7, 12, 16
Polygenic traitPolygenic trait
EnvironmentalTriggers & Modifiers
Gut bacteriaGut bacteriaSmoking/nicotineSmoking/nicotine
Epithelial dysfunctionEpithelial dysfunction
IncreasedIncreasedImmune ResponseImmune Response
Innate & autoimmune Innate & autoimmune Macrophage activationMacrophage activation
T cell activationT cell activationCytokine/adhesion moleculeCytokine/adhesion molecule
expressionexpression
Current Model: Pathogenesis of Crohn’s Disease


Genetics


NOD2 geneNOD2 gene involved in NF-involved in NF-B activationB activation
--CARD: caspase-activation recruitment domainCARD: caspase-activation recruitment domainNBD: nucleotide-binding domainNBD: nucleotide-binding domainExpressed in monocyteExpressed in monocyte
--Leucine rich region (LRR) interacts with Leucine rich region (LRR) interacts with bacterial LPS to activate NF-kBbacterial LPS to activate NF-kB
1 28 124 220 273 577577 744 1044LRRCARD CARD NBD



Genotype relative risks (RR)Genotype relative risks (RR) for three major associated for three major associated NOD2NOD2 variants variants
Heterozygous RR : 1.5 - 4.0Heterozygous RR : 1.5 - 4.0
Homozygous RR : 15 - 40Homozygous RR : 15 - 40
Disease penetrance < 10% for homozygotesDisease penetrance < 10% for homozygotes
and compound heterozygotesand compound heterozygotes
NOD2NOD2 Population attributable risk for Population attributable risk for ilealileal disease ,Younger ,fibrostenoticdisease ,Younger ,fibrostenotic

New gene in IBD:IL23R
Encodes a subunit of the IL-23 receptor
IL-23 is required for colitis in mice models
Expressed in colon and TI
Mutations associated with
both CD and UC
Duerr RH et al. Science, 26 Oct 2006.


CD management

Unmet Needs in Crohn’s Disease Management
Accurate predictors of response to therapies
therapies or approaches change the natural history of IBD
Surgery
Hospitalization
Disability
Uncertain risk/benefit of combined therapies
*Kaplan-Meier analysis.Mekhjian HS, et al. Gastroenterology. 1979;77:907-913.
% o
f P
ati
en
ts20
40
60
80
100
5 10 15 20 25 30
Years After Onset
Cumulative Probability* of Surgery in Crohn’s Disease

CD therapeutic pyramid
SurgerySurgeryCyACyA
InfliximabInfliximabMTXMTX
AZA/6-MPAZA/6-MPSystemic Systemic
CorticosteroidsCorticosteroids
SurgerySurgeryCyACyA
InfliximabInfliximabMTXMTX
AZA/6-MPAZA/6-MPSystemic Systemic
CorticosteroidsCorticosteroids
AntibioticsAntibiotics5-ASA5-ASA
AntibioticsAntibiotics5-ASA5-ASA
Mild to ModerateMild to ModerateDiseaseDisease
Moderate to SevereModerate to SevereDiseaseDisease
BudesonideBudesonide
Hanauer SB, Sandborn W. Hanauer SB, Sandborn W. Am J Gastroenterol.Am J Gastroenterol. 2001;96:635–643. 2001;96:635–643.





Systemic circulation
10-20%
70% absorbed in ileum
Budesonide absorption & bioavailability



CD limited to small bowel
5ASA????
budesonide
prednisone
6MP/AZA
MTX
infliximab
Others: CyA, thalid… ,.
NPO + TPN

CD limited to colon
5ASA: Asacol, Colazal… ,
Abx: cipro, metro… ,
prednisone
6MP/AZA
MTX
infliximab
Others: CyA, thalid… ,.
NPO + TPN
ileostomy

Infliximab Indications:
-Mod to severe CD not responded to conventional therapy
-Fistulizing CD with drainage EC fistula
-Fistulizing CD that responded to induction infliximab
-steroid dependant CD that fail to attempt to taper the steroid

RemicadeContraindications
Absolute Class III/IV CH
Active bacterial infection
RelativeElderly
Severe co-morbidities
Bowel stricture?
Multiple sclerosis

Anti-TNF Biologic Agents Indications, Route of Administration, and Dosing
Infliximab (infusion)Induction dose:5 mg/kg IV at 0, 2, and 6 weeks
Maintenance dose:5 mg/kg IV q 8 weeks
Adalimumab (SQ, pre-filled syringe, injectable pen)
significant efficacy in phase III studies in CD
Loading dose:160 mg at week 0; 80 mg at week 2
Maintenance dose:40 mg SQ weekly or every other week
Certolizumab pegol (subcutaneous)
significant efficacy in phase III studies in CD
Loading dose:400 mg SQ at weeks 0, 2, 4
Maintenance dose:400 mg SQ q 4 weeks

Major Clinical Trials With TNF Antagonists in Crohn’s Disease
AgentStudy NameReferenceAim of Study
Infliximab
—Targan et al.N Engl J Med 1997Induction
—Present et al.N Engl J Med 1999Induction (F)
—Rutgeerts et al. Gastroenterology 1999
Maintenance
ACCENT IHanauer et al.Lancet 2002Maintenance
ACCENT IISands et al.N Engl J Med 2004
Lichtenstein et al.Gastroenterol 2005Maintenance (F)
REACHHyams et al.DDW 2006Induction &Maintenance (P)
Adalimumab
CLASSIC IHanauer et al.Gastroenterol 2006Induction
CLASSIC IISandborn et al.UEGW 2005Maintenance
CHARMColombel et al.DDW 2006Maintenance
Certolizumab
—Schreiber et al.Gastroenterol 2005Induction
PRECiSE 1Sandborn et al.DDW 2006Induction &Maintenance
PRECiSE 2Schreiber et al.UEGW 2005Maintenance
F = fistulas; P = pediatric.

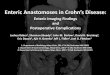
ACCENT II: Number of Crohn’s Disease-Related Hospitalizations per 100 Patients Through Week 54
Rutgeerts P, et al. Gastroenterology. 2004;126:402–413.
Episodic Strategy
5 mg/kg Scheduled
Strategy
10 mg/kg Scheduled
Strategy
Combined Scheduled
Strategy
Ho
spit
aliz
atio
ns
per
100
Pat
ien
ts
p = 0.047 p = 0.023 p = 0.014
0
10
20
30
40
50
N = 188 192 193 385

ACCENT II: Cumulative Number of Surgeries Over Time in RespondersC
um
ula
tive
Nu
mb
er
of
Su
rger
ies
& P
roce
du
res
Weeks
Randomization
Infliximab 5 mg/kg maintenance (n = 96) Placebo maintenance (n = 99)
Lichtenstein GR, et al. Gastroenterology. 2005;128:862–869.
0
25
50
75
100
125
0 2 6 14 22 30 38 46 54


Major Clinical Trials With TNF Antagonists in Crohn’s Disease
AgentStudy NameReferenceAim of Study
Infliximab
—Targan et al.N Engl J Med 1997Induction
—Present et al.N Engl J Med 1999Induction (F)
—Rutgeerts et al. Gastroenterology 1999
Maintenance
ACCENT IHanauer et al.Lancet 2002Maintenance
ACCENT IISands et al.N Engl J Med 2004
Lichtenstein et al.Gastroenterol 2005Maintenance (F)
REACHHyams et al.DDW 2006Induction &Maintenance (P)
Adalimumab
CLASSIC IHanauer et al.Gastroenterol 2006Induction
CLASSIC IISandborn et al.UEGW 2005Maintenance
CHARMColombel et al.DDW 2006Maintenance
Certolizumab
—Schreiber et al.Gastroenterol 2005Induction
PRECiSE 1Sandborn et al.DDW 2006Induction &Maintenance
PRECiSE 2Schreiber et al.UEGW 2005Maintenance
F = fistulas; P = pediatric.

CLASSIC 1 trial

CHARM: Clinical Remission of CD Over Time With Adalimumab
Randomized Responders (n = 499)
* *
* **
* * * *
*
**
* * * * **
†
% o
f P
atie
nts
Weeks
47
40
41
36
1712
*p < 0.001 vs placebo; †p = 0.005 vs placebo.Colombel JF, et al. DDW 2006, Abstract 686d.
0
10
20
30
40
50
60
0 10 20 30 40 50 60
Placebo Adalimumab 40 mg EOW Adalimumab 40 mg weekly
26 56

Top-Down Versus Step-Up Strategies in CD
• Newly diagnosed CD of < 4 years’ duration (N = 129)
• Naive to immunomodulators and biologics
Step-up (n = 64)
Steroids
+ IFX
+ AZA MTX
Steroids
Steroids
Top-down(n = 65)IFX (Wk 0, 2, 6)
+ AZA
IFX + AZA
+ (episodic) IFX
Steroids
Hommes D, et al. DDW 2006, Abstract 749.
CDAI < 150 Points AND No Steroids AND No Surgery
Weeks
% o
f P
atie
nts
Step-upTop-down
*
0
20
40
60
80
100
0 20 40 60 80 100
Co-primary endpoints6 & 12 months
†*
* P < 0.01; † P <0.05

Top-Down Versus Step-Up TrialClinical Results at 2 Years
Hommes D, et al. DDW 2006, Abstract 749.; D’Haens GR, et al. DDW 2006. Abstract 764.
Reduction and Disappearance of Ulcers
% o
f P
atie
nts
88
71
47
30
p < 0.001
p < 0.001
0
20
40
60
80
100
Reduction Disappearance
Step-upTop-down
Weeks
% o
f P
atie
nts
Patients Receiving Infliximab
0
50
100
0 20 40 60 80 100
Step-upTop-down
0
50
100
% o
f P
atie
nts
Patients Receiving Immunosuppressants

Unanswered Questions About Biologic Therapy in IBD
Do biologics change long-term outcomes in IBD ?
Economic burden ,safety
immunosuppressives beneficial indefinitely or just early?
Where should biologic therapy fit in our treatment algorithm?“Top down” approach?


Before 1982, Kirsner and shorter observed that inflammatory bowel disease was rare or non existent in Saudi Arabia Kirsner JB, Shorter RG. Recent developments in non-specificinflammatory bowel disease .
N Engl J Med 1982; 306: 837-848
Mokhtar and his group from King Abdul- Aziz University in Jeddah reported the first two
cases of Crohn’s disease in Saudi’s 1982
Mokhtar A, Khan MA. Crohn’s disease in Saudi Arabia. Saudi Med J 1982; 3: 207-208

Epidemiology and outcome of Crohn’s disease in a teaching hospital in Riyadh
Abdullah S. Al-Ghamdi, Ibrahim A. Al-Mofleh, Rashed S. Al-Rashed, Saleh M. Al-Amri, Abdulrahman M. Aljebreen, World J Gastroenterol 2004;10(9):1341-1344

retrospective analysis of 77 patients of crohn’s seen for 20 years (between 1983
and 2002) .
Abdullah S. Al-Ghamdi, Ibrahim A. Al-Mofleh, Rashed S. Al-Rashed, Saleh M. Al-Amri, Abdulrahman M. Aljebreen, World J Gastroenterol 2004;10(9):1341-1344


Emerge of Crohn’s Disease Incidence in Saudi Arabia; Tertiary
Care Centre Experience
Azzam N et al Abstract in the 9th GI &liver conference Abha , SA 7-10 may 2007

METHODS
Retrospective analysis of 42 CD patients diagnosed (between 2003 and 2005) was performed.
Individual case records were reviewed with regard to history, clinical findings, the disease extent, location, clinical pattern, treatment and outcome.

Clinical features of CD patients
Age26.5 y
Male 18) 42%(
Female 24) 58%(
Duration since diagnosis
3 Y
Family HX of IBD3) 7%(
Saudi92%

Presenting symptoms
Abdominal Pain41)97%(
Diarrhoea 40)95%(
Bleeding P/R21)50%(
Vomiting14)33%(
Fever7)16%(
WT loss21)50%(

Disease location
0%
5%
10%
15%
20%
25%
30%
35%
40%
Diseaselocations
ileal
colonic
ilocolonic
duodenal

CD types
0%
10%
20%
30%
40%
50%
60%
70%
C D types
C D types
inflammatory
fistulizing
fibrostenotic

Result
Forty -Two patients with Crohn's disease were reviewed .
The incidence of the CD was increased significant in KKUH from 77 patients diagnosed as Crohn’s disease from (1983-2002) to 42 new patients with CD within
(2003-2005) The patients had more severe disease and
more colonic involvement .

Conclusion
-This study shows an increase in the incidence of CD in Saudi population in tertiary centre especially in the last 3 years
-National data registry is needed for the true prevalence of crohn’s diasease in Saudi Arabia

Recommended













![[Abd_Ar-Rahman_'Azzam]_The_Life_of_the_Prophet_Muh( ).pdf](https://img.pdfslide.us/doc/110x75/563db864550346aa9a9349a2/abdar-rahmanazzamthelifeoftheprophetmuhbookzzorgpdf-57082c7e95717.jpg)

