CPR / DNARProject ECHO
Dr Cliona Lorton
26th March 2020
All slides ©Dr Cliona Lorton, information correct as of 26/3/2020

Introduction
• Session request: DNACPR
• Advance Care Planning
• Evolving situation and questions
• Brief session today
• Further session(s)
• Anticipatory Rx separate session
• Applies to Republic of Ireland settings
Advance Care
Planning
CPR Discussions

Project ECHO
26.3.18
Image from https://voxeu.org/content/here-be-dragons

Outline
• Advance care planning recap (previous ECHO sessions)
• CPR and DNACPR
• Current context• Same
• Different
• Recommendations and resources
• Questions

Advance Care Planning
• A process of discussion and reflection about goals, values and preferences for future care in the context of an anticipated deterioration in a person’s condition with loss of capacity to make decisions and communicate these to others 1
• “Discussion and reflection” : person, health and social care team
1. The Palliative Care Programme HSE 2012

Decision-making Capacity1
• Ability of a person to understand at the time a decision is to be made, the nature and consequences of the decision in the context of the available choices at that time
• Decision-making is time and issue specific
• Capacity is presumed
1. The Palliative Care Programme HSE 2012

Advance Healthcare Directive
• Expression made by a person who has capacity (in writing, to include voice, video recording and speech recognition technologies) of their will and preferences concerning specific treatment decisions in the context of an anticipated deterioration in their condition with loss of decision- making capacity to make these decisions, to give consent to or to refuse treatment and communicate them to others.
• Legally binding under ADMC Act 2015 (not fully enacted yet)
• Right to refuse treatment
• Can request but not oblige treatment
Oireachtas. Assisted Decision Making (Capacity) Act [Internet]. Oireachtas; 2015.

Advance Care Planning: Why?
• Care in keeping with person’s wishes (where possible)
• Improve end of life care
• Guide healthcare team and family when making decisions on patient’s behalf

Advance Care Planning: When?
• Typically• Diagnosis of life-limiting illness
• Transition point in life-limiting illness e.g. stopping chemotherapy
• Disease-specific triggers e.g. SOB on minimal exertion in heart failure
• During / after hospital admission
• Patient request
• Likely to die in next 12 months (“would you be surprised? – No”)• 80% of adults in care home setting
• ** COVID-19**

Advance Care Planning: How?
• Healthcare professional well-informed
• Privacy
• Support / involvement of loved ones if wished by patient
• Discuss at best time for patient• Ideally not at time of crisis
• Simple language
• Time taken
Documented : who, what discussed, decisions, signed, dated

Advance Care Planning: What?
• Concerns
• Understanding of condition
• Goals
• Values
• Preferences
• Discuss risks / benefits• Hospital admission, iv antibiotics, ventilation, CPR
• Place of care and death
• Religious rites, funeral preferences

Cardiopulmonary Resuscitation(CPR)
70% survival!1
1. Portanova Resuscitation 2015

CPR in Real Life
• CPR in NH residents: 30 day survival 1.7%1
• Risks• Hypoxic brain injury and long-term neurological loss• Traumatic – fractures, organ puncture
• There is no obligation to start or continue treatment, including resuscitation, if you judge that the treatment• is unlikely to work or• might cause the patient more harm than benefit or • is likely to cause the patient pain, discomfort or distress that will outweigh the
benefits it may bring 2
1. Pape Resuscitation 20182. Medical Council. Guide to Professional Conduct and Ethics for
Registered Medical Practitioners (Amended)8th Edition 2019

Do Not Attempt CPR Order (DNAR / DNACPR)1
• Individual assessment based on likelihood of success v risks
• Responsibility: most senior doctor (GP in community)
Should • consult with other healthcare professionals who know patient
• consult with a patient who wishes to participate in discussions
1. HSE National Consent Policy V.1.3

Do Not Attempt CPR Order (DNAR / DNACPR)1
• If patient does not have capacity• respect an existing decision to refuse CPR• explain nature, benefits and risks to loved ones
• NOT seeking permission
• Here “good practice to inform those close to the patient”
• UK: must consult unless believe would cause distress2
• Emergency – decisions in patient’s best interests
1. HSE National Consent Policy V.1.32. Tracey v Cambridge Hospitals NHS, Winspear v City Hospitals
Sunderland NHS

CPR Decisions
3 groups
1. Cardiorespiratory arrest unlikely
2. Cardiorespiratory arrest, as a terminal event, is considered inevitable• CPR would not be clinically indicated
3. Cardiorespiratory arrest is considered possible or likely
*could include currently stable residents but at risk if COVID-19
Discussion should occur in context of overall discussion of care goals and preferences

Documentation
• Whether or not to attempt CPR
• Clearly and accurately documented in the individual’s healthcare record by the professional who discussed
• Include • How the decision was made
• Date
• Rationale
• Who was involved in discussion

Documentation and Decisions
• No national document yet
• Ambulance service require “recent and reliable evidence from a clinical source stating that the patient is not for resuscitation” • Otherwise obliged to perform CPR
• Inform ambulance when making contact that DNAR in place
• Have written document to hand when arrive
• ? Part of routine handover

Challenges
• Disagreements• usually misunderstandings : likelihood of success or “no treatment”
• Further discussion often resolves
• If not, offer second independent opinion
• Person doesn’t want to discuss• May wish to defer discussion
• May ask nominated person to discuss on their behalf (NOT make decision)
• May prefer healthcare team to do what they “think is best”
• Document this

Current Context

COVID-19
• Predictors of poor survival• Older age
• Co-morbidity• Hypertension
• Cardiovascular disease
• Diabetes
• Also cancer, immunosuppression, chronic lung disease
• Treatment• Supportive
• Early mechanical (invasive) ventilation- prolonged 7-14 days NB
• Specific treatments: experimental

CPR in COVID-19
• May have cardiac arrest due to COVID-19 or co-existing illness
• Aerosol-Generating Procedure i.e. ↑ risk of transmission
• Full PPE1
• In unlikely event of successful CPR +/- defibrillation: what next?
• Hospitalisation
1. Resuscitation Council UK March 2020

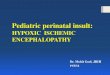
Hospital in the coming weeks / months

Capacity
Beds
25,000 needed
14,000 capacity

Hospitalisation
• COVID-19 +• No current specific treatment• Aggressive supportive care (ventilation/ICU) – burdensome, high mortality• Hostile hospital environment• Last days in hospital isolation
• COVID-19 –• Care likely to be compromised by pandemic• May become infected

Advance Care Planning in COVID-19
• Risks and benefits have changed (↑ risks, ↓benefits)
• May be many patients in short time
• Currently stable patients - should consider for all NH residents
• May deteriorate quickly• Family members may be sick
• Documentation essential (OOH, agency staff…)

Advance Care Planning in COVID-19
• Things to consider
• Interventions• IV / SC fluids
• Antibiotics (if suspected bacterial infection)
• Transfer to acute hospital
• Attempt CPR
• People to consult
• Other views or preferences

Symptom control (general)
• Individualised assessment always
Last days of life: key symptoms and medications
• Dyspnoea / cough : opioid (morphine sulphate), midazolam
• Anxiety / agitated delirium : midazolam, levomepromazine / haloperidol
• Pain: opioid (morphine sulphate)
• Anti-secretory: hyoscine butylbromide (Buscopan) or glycopyrronium
• Nausea / vomiting: levomepromazine / haloperidol

Dying with COVID-19
• Mode of death• Respiratory failure / Acute Respiratory Distress Syndrome (ARDS)
• Myocarditis / cardiac failure
• Sepsis / septic shock
• (Acute renal failure)
• We can apply experience from other diseases – end-stage COPD, heart failure
• Principles remain the same

Anticipatory Prescribing
(will be separate session)
• Engage with GPs (swamped)• Proactive
• Medication supply lines – liaise with pharmacy now (swamped)
• Safe custody requirements: ? Storage ?Register books
• Oxygen – requirements unknown
• ? maximum you can provide (pumped)
• Liaise with provider, may have different ordering processes, limits etc

Communication
• Heightened tensions
• Communication barriers• PPE
• Phone rather than face to face
• Advance care planning – who are contacts? Check the phone numbers incl alternative contacts
• Listening, acknowledging key

Communication: specific phrases and tips
• Examples from VITALtalk website
• No visitors: “The risk of spreading the virus is so high that I am sorry to say we cannot allow visitors. We can help you be in contact electronically. I wish I could let you visit, because I know it’s important. Sadly, it is not possible now”
VitalTalk COVID Communication Skills www.vitaltalk.org

Communication: specific phrases and tips
• Examples from VITALtalk website
• Decisions: “I imagine you are worried and want the best possible care. Right now, the hospital has become a dangerous place unless you really, really need it.”
• Planning: “We will continue to take care of you. The best case is that you don’t get the virus. The worst case is that you get the virus despite our precautions—and then we will keep you here and make sure you are comfortable for as long as you are with us”
VitalTalk COVID Communication Skills www.vitaltalk.org

Care for Staff
• Difficult times
• Fear
• Worry
• Sickness
• Multiple bereavements of residents

Project ECHO
26.3.18
Image from https://voxeu.org/content/here-be-dragons

Image from www.mapsinternational.com

End of Life Care in Nursing Home Setting
• Residents cared for by people they know
• Familiar environment
• Family know the team
• Dignity
• Experience in caring for dying – this will translate
• Established links with palliative care

Head Start
• Advantage: Experience of other countries: head start
• Chance to plan
• Who has documented advance care plan? DNAR? List of which residents need to have this clarified. Which family members to involve? Discuss as a team
• Further session (? next week)
• Specific scenarios
• Staff queries and concerns – likely some in common across sites
(NOT individual patient advice)

Resources
Advance Care Planning• The Palliative HubDNAR• HSE Toolbox Talks: End of life care, CPR and DNAR decisionsPalliative and end of life care in context of COVID-19• European Association of Palliative Care www.eapcnet.euCommunication around COVID-19• https://www.vitaltalk.org/guides/covid-19-communication-skills/Coping with stress during COVID-19• https://learn.nes.nhs.scot/741/quality-improvement-zone

Summary
• Hospitalisation : risk increasing, benefits reducing
• Can provide individualised and good care in residential setting
• Advance Care Planning more important than ever now
• Now is the opportunity to do so
Recommended