CPD Motivation 1
Postural Stability Instructor Update:
Motivation
Welcome to LondonThursday 12th October
CPD Motivation 2
Programme for the day
1. PSI experiences in motivation in falls prevention, drop out, barriers and motivation
2. Understanding behaviour change, listening and talking about physical activity
Lunch break
3. Strategies to increase adherence - induction, goal setting and support
4. Increasing participation through choices, planning for next steps and evaluation
CPD Motivation 3
Aims of the Day
• to review instructors’ experience of motivating participants and the barriers they face in adopting and maintaining exercise behaviour
• to introduce instructors to the theoretical principles of motivation and adherence to exercise
• to introduce instructors to the specific motivational issues related to exercise and falls programmes
• to introduce exercise instructors to strategies designed to support exercise participation
• to enable instructors to practise listening and talking about overcoming barriers to exercise
and ………?
CPD Motivation 4
Session 1
PSI experiences of motivation in falls prevention
CPD Motivation 5
From referral to regular physical activity/exercise
• The process• Assessed at risk/or a faller• Advice/referral (from ?)• Preparation and exploration• Early Adoption• Action• Maintenance• Sustained participation in physical activity
CPD Motivation 6
Introductory task
Identify two practical examples of barriers or drop out you have
encountered in your practice and be prepared to
share with the group
CPD Motivation 7
PSI investigation
From the results of the PSI review, identify the top four
barriers, motivators and
reasons for drop out cited

CPD Motivation 8
Barriers to physical activity
• Intrinsic barriers - are those that relate to the individual’s beliefs, motives and experiences concerning physical activity. These are most likely to be addressed by those who provide counselling, advice, motivation - for example, a peer mentor, health visitor or GP
• Extrinsic barriers - are those that relate to the broader physical activity environment, the attitudes of others and the types of opportunities that are available. These barriers are more likely to be influenced by other people and those responsible for policy and strategic developments.
CPD Motivation 9
Previous experiences
• Limited opportunities and experiences in school (How long ago ?)
• Physical activity not associated with fitness and health
• Armed forces
• Limited experiences of sport
• All aspects of life were more physically demanding
CPD Motivation 10
Older people’s sources of beliefs
• The media (radio, TV, magazines, newspapers)
• Workplace, H.P leaflets • ‘Common sense’• Personal experiences (and experiences of
others)• Medical and health professionals
authoritative(Finch, 1997)
CPD Motivation 11
Beliefs about activity
• It’s good for you.• It’s common sense.• General health benefits• Specific health benefits e.g. weight control,
mental well-being, specific conditions• Maintenance of function• Onset of ageing as a signal(Finch, 1997)
CPD Motivation 12
Moderation “at our age”
• “You can overdo it.”
• Gentler activities are more suitable.
• It depends on the individual.
• Might make something worse
• Fears over breathlessness and increased heart rate.
(Finch, 1997)
CPD Motivation 13
Beliefs – exceptions to the positive view
• The health ‘lottery’
• A fashion for exercise nowadays
• “You need to be fit to do physical activity.”
• Too late to start
• Dangers when you stop
• “It can become an obsession.” (Finch, 1997)
CPD Motivation 14
Overcoming barriers
• The association between physical activity and exercise and sport
• Frequency
• Intensity
• Old age is a time to slow down.
• Reassurance and education (Finch, 1997)
CPD Motivation 15
Beliefs about activity – the underlying motivators
• To maintain suppleness and agility, and control weight
• ‘Feeling better’• Enjoyment• Prevent future illness• Manage existing health problems• To keep going, be independent (live longer
rare)• Adventure/challenge, new learning (Finch, 1997)
CPD Motivation 16
Overcoming concerns about being active
• “I don’t think I should start at my age.”
• “I’m worried I might hurt something.”
• “I have to take it easy at my age.”
• “My aches and pains will get worse.”
• “Can I do exercise with my blood pressure ?”
advice/views of a GP powerful.
CPD Motivation 17
‘Triggers’ and life events
• Wanting to play with grandchildren• Physiological signs of ageing• Retirement, children leaving home• Onset of ailment or illness• Moving home• Bereavement • Maintaining independence • Acute/crisis event a fall or MI (Finch, 1997)
CPD Motivation 18
Extrinsic barriers
• Skills and attitudes of others, e.g. exercise instructors, GPs, leisure/recreation managers, family and friends
• Appropriate programming
• Accessible opportunities (transport)
• Safe activity environments (parks, well-lit streets, traffic)
• Positive images of older people
CPD Motivation 19
Barriers to physical activity including programming
Intrinsic Programming Extrinsic
Poor self image, self efficacy
No history of positive
experience of exercise
Fear of over-exertion
Inconvenient time
Location and transport
Boredom
Exercising alone
Poor instruction
Too easy, too hard
Lack of family/partner
support
Social support
Weather/season
Medical problems
(Jones & Rose 2005)
CPD Motivation 20
Understanding older people’s views of falls prevention advice:
focus group and interview study
Lucy Yardley & Chris Todd
with Margaret Donovan-Hall and Kate Francis (HT Aged 2005)
CPD Motivation 21
Aims
• to explore older people’s views of different types of falls prevention advice
• to identify features of communications about balance training and falls prevention that may result in negative experiences
• to discover how messages may be improved
CPD Motivation 22
Method
• Nine focus groups with 45 people (35 women and 10 men) aged 66 to 90
• Interviews with 21 participants (14 men and six women) aged 61 to 94
• Recruited from sheltered accommodation, church groups, senior citizen clubs, leisure centres, university staff newsletter, opportunity sampling
• Explored past experiences, presented and discussed different types of advice about balance training/falls prevention
CPD Motivation 23
Findings
Perceptions of available falls prevention advice
• Reported none received! (though actually some mention of receiving information)
• Perceived falls prevention in terms of hazard reduction (rather than balance improvement), often through restriction of personal (physical) activity
CPD Motivation 24
Perceptions of falls prevention messages presented
Discussion of falling prevention is beneficial
‘I think it would be helpful if someone knows what you should do and what you shouldn’t do’
‘I think it would give me more confidence of building up your balance if I read this [leaflet about improving balance] now. I think it would give me more confidence when I’m out.’
(Members of focus group of women aged 78 to 95 living in sheltered accommodation)
CPD Motivation 25
Perceptions of falls prevention messages presented (cont).
It’s good advice BUT- they wouldn’t necessarily act on (all of) it‘It’s all good. I mean its good advice, yes,
excellent, I agree. I doesn’t mean to say I do it all but I agree.’
- it may not fit with their circumstances, lifestyle, prioritised goals
‘ No, no, no, no, no, no ... Nobody would go around with padding.’
CPD Motivation 26
Perceptions of falls prevention messages presented (cont).
It’s good advice - for ‘them’- only seen as relevant to ‘elderly’‘Because we’re that much fitter -- we don’t really take too
much notice of it, only for other people, for other disabled or elderly people that we have to watch … we always watch older people anyway’.
(male participant aged 79 in sheltered accommodation)- rejected by fit, younger people, seen as humiliating‘I wouldn’t go for that [advice] because it didn’t apply to me
in any shape or form. Is there a bit of pride, is there a bit of “Well, you know, I’m not there yet”?’
(Denial ?)
CPD Motivation 27
Perceptions of falls prevention messages presented cont.
Falls prevention advice unnecessary, upsetting‘It can make you feel – somebody producing the
leaflets here – that these people here are senile and they just don’t have any common sense and they need to be told everything.’
‘The last thing you want as you get older is to be told that you’ve got to be conscious every time you go out and might fall, you don’t want that, otherwise your life’s gone.’
(female participant, 78, who had recently fallen)
CPD Motivation 28
Participants’ suggestions for future advice
• Incorporate falls prevention activities into lifestyle and general exercise programmes, and promote these activities as enjoyable, interesting, sociable
• Offer suggestions in constructive manner recognising individual’s knowledge and choice regarding their own lifestyle, and giving explanations for suggestions
CPD Motivation 29
Evidence about falls - 1
• Exercise - Perceived positive factors and benefits• Noticeable benefit/improvement (restoring/maintaining
fitness and functioning, better health –blood pressure, dizziness, diabetes)
• Feel and look good (less stiff, less pain, more mobile, strong, energetic, better balance, mood, weight loss)
• Able to do more things (walk, do without stick, climb stairs, travel, go out alone, go shopping, ADLs)
• Maintaining and increasing independence• Social contact (bond formed through prolonged contact
with group)• Confidence/pride in achievement (general increase in
self-confidence, approval of family/friends/doctor)• Enjoy the activity (get out of house, use equipment)
CPD Motivation 30
Evidence about falls - 2
• Exercise - Negative factors• Health problems (actual and perceived
interference)• No observed positive effects when tried
programme (didn’t work !)• Not liking social contacts in classes (peers or
leader!)• Unpleasant experiences (fatigue, pain etc.) or
not enjoyable• Low motivation or perceived relevance• Other priorities (caring for dependents, holidays,
other appointments, housework, bingo)
CPD Motivation 31
Evidence about falls - 3• What are the key motivations for older
people to take up strength and balance training exercises?
• thinking you are the kind of person who should do these activities (self-efficacy)
• thinking other people think you should do these exercises
• believing that these activities would be enjoyable• concern about the risk of a future fall• (NOT having recent falls, or risk factors for falls)
CPD Motivation 32
Session 2
Understanding change, listening and talking
CPD Motivation 33
Advising older people to become active
• Use of a health educator and an extended consultation time
• Assessment of problem areas• Recognition of readiness to change• Goals agreed by both the older person and the
professional• Identification and recognition of social and
environmental barriers • Tailored action plan (specifies activity)• A choice and range of accessible local activities
including lifestyle activities• Supplementary educational materials• Systematic follow-up and support over a period of time
Promoting physical activity with older people. Recommendations for practice (BHF 2003)
CPD Motivation 34
Pre-exercise assessment
• Health
• Function
• Readiness to exercise(Later Life Training Manaul)
How do we assess readiness to exercise among participants ?
CPD Motivation 35
Lifetime model of physical activity
Staying
active
“Not doing Starting
A lot or
sedentary” out
Stopping Restarting
Time
CPD Motivation 36
Generic models of behaviour change
• Theory of Reasoned Action – intention determined by attitude towards behaviour and social influences (Fishbean & Azjen 1975)
• Theory of Planned Behaviour + perceived behavioural control (confidence and opportunity) (Azjen 1985)
• Social Cognitive Theory - Self Efficacy and knowledge of health risks (Bandura 1986)
CPD Motivation 37
Models of behaviour changeSummary - Change is more likely when
• Perceived benefits of physical activity outweigh the costs• Becoming more active will lead to social approval, not
disapproval• Being more active will lead to self-satisfaction and is
consistent with highly valued, broader life goals• Desirable outcomes are within one’s personal control,
achievable through one’s own actions• There are few obstacles/barriers to achieving desirable
outcomes• Opportunities and access to physical activity are high

CPD Motivation 38
the decisional balance between benefits and cost – starting a
walking regime
Get out of the house and get some fresh air.
(Might) loose some weight
Meet some new people
Will help with my blood pressure
Difficult to get into the mood
Shopping will take longer
I’ve got a stiff knee
There are other things I want to do
Janis and Mann 1977
CPD Motivation 39
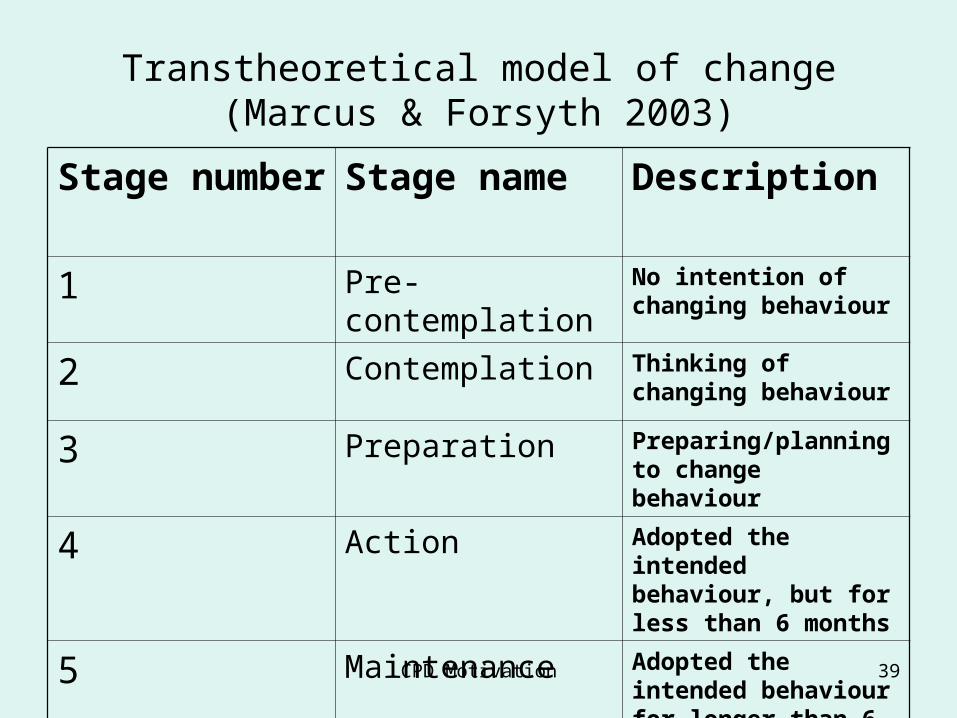
Transtheoretical model of change (Marcus & Forsyth 2003)
Stage number Stage name Description
1 Pre-contemplation No intention of changing behaviour
2 Contemplation Thinking of changing behaviour
3 Preparation Preparing/planning to change behaviour
4 Action Adopted the intended behaviour, but for less than 6 months
5 Maintenance Adopted the intended behaviour for longer than 6 months
CPD Motivation 40
Relapse
Relapse
(commonly described as dropping out) is identified as being very relevant (it
happens to most people !)
it is not a stage as such, but may appear between the stages.
CPD Motivation 41
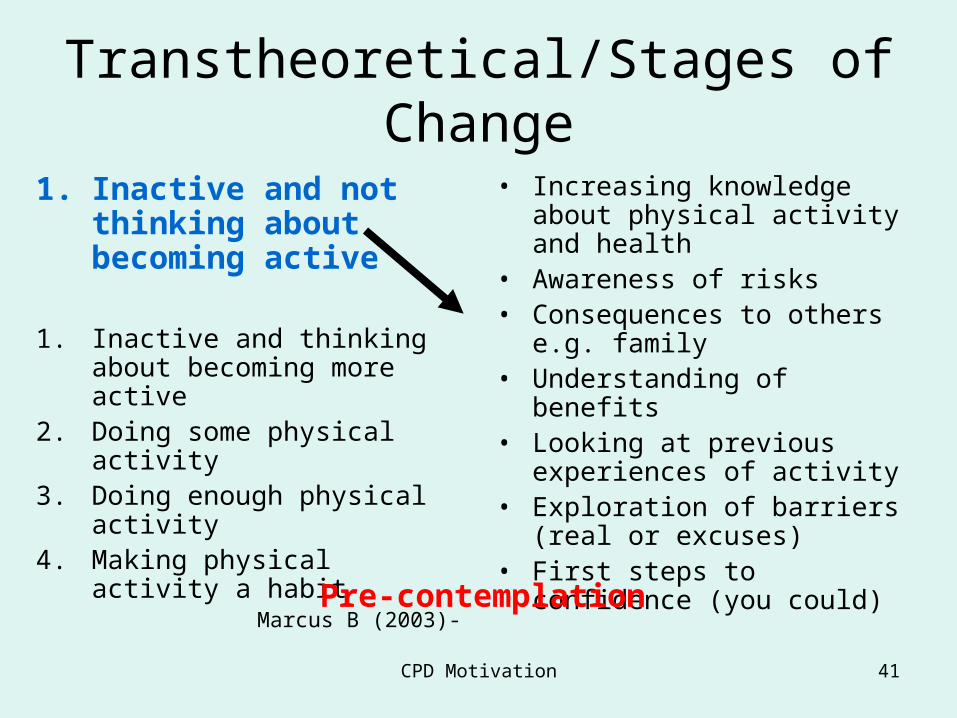
Transtheoretical/Stages of Change
1. Inactive and not thinking about becoming active
1. Inactive and thinking about becoming more active
2. Doing some physical activity3. Doing enough physical activity4. Making physical activity a habit
Marcus B (2003)-
• Increasing knowledge about physical activity and health
• Awareness of risks• Consequences to others e.g.
family• Understanding of benefits• Looking at previous experiences
of activity• Exploration of barriers (real or
excuses)• First steps to confidence (you
could)
Pre-contemplation
CPD Motivation 42
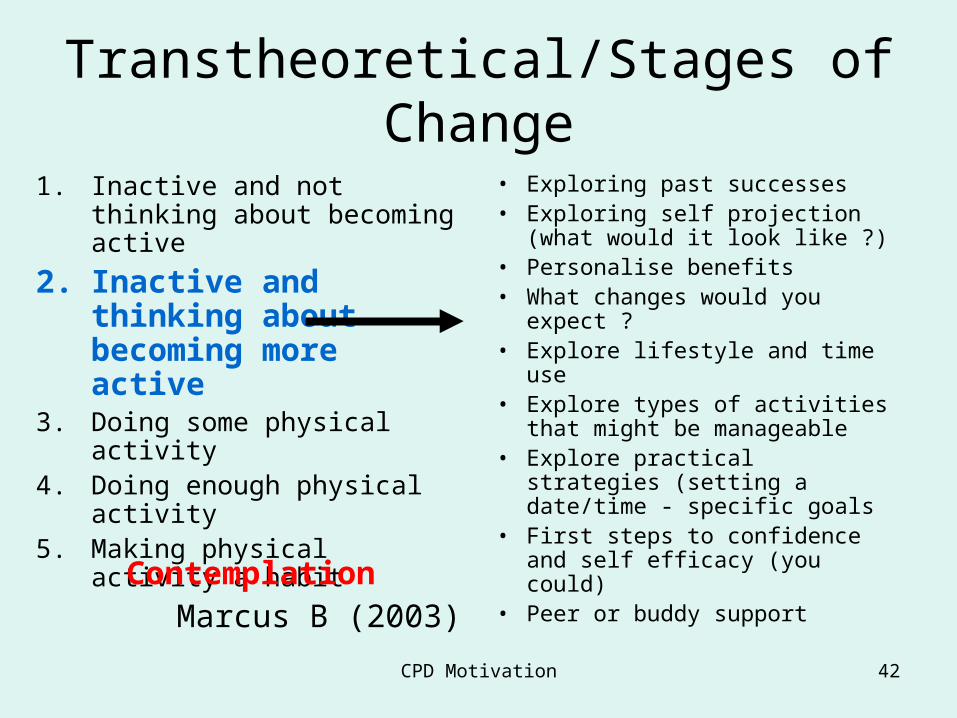
Transtheoretical/Stages of Change
1. Inactive and not thinking about becoming active
2. Inactive and thinking about becoming more active
3. Doing some physical activity4. Doing enough physical activity5. Making physical activity a habit
Marcus B (2003)
• Exploring past successes• Exploring self projection (what
would it look like ?)• Personalise benefits• What changes would you
expect ?• Explore lifestyle and time use• Explore types of activities that
might be manageable • Explore practical strategies
(setting a date/time - specific goals
• First steps to confidence and self efficacy (you could)
• Peer or buddy support
Contemplation
CPD Motivation 43
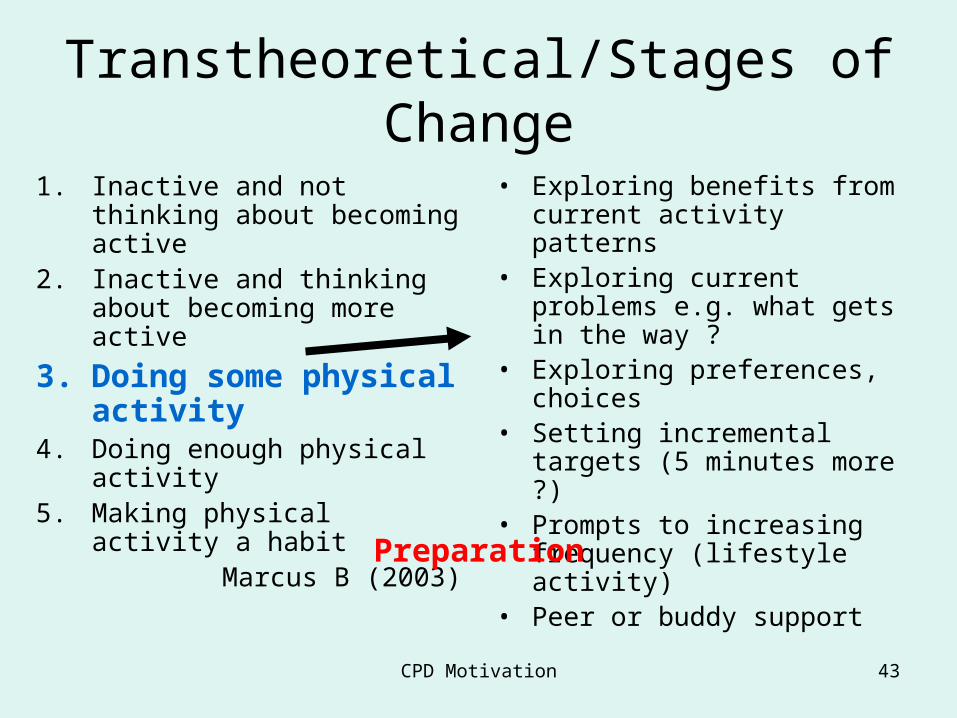
Transtheoretical/Stages of Change
1. Inactive and not thinking about becoming active
2. Inactive and thinking about becoming more active
3. Doing some physical activity
4. Doing enough physical activity5. Making physical activity a habit
Marcus B (2003)
• Exploring benefits from current activity patterns
• Exploring current problems e.g. what gets in the way ?
• Exploring preferences, choices• Setting incremental targets (5
minutes more ?)• Prompts to increasing
frequency (lifestyle activity)• Peer or buddy support
Preparation
CPD Motivation 44
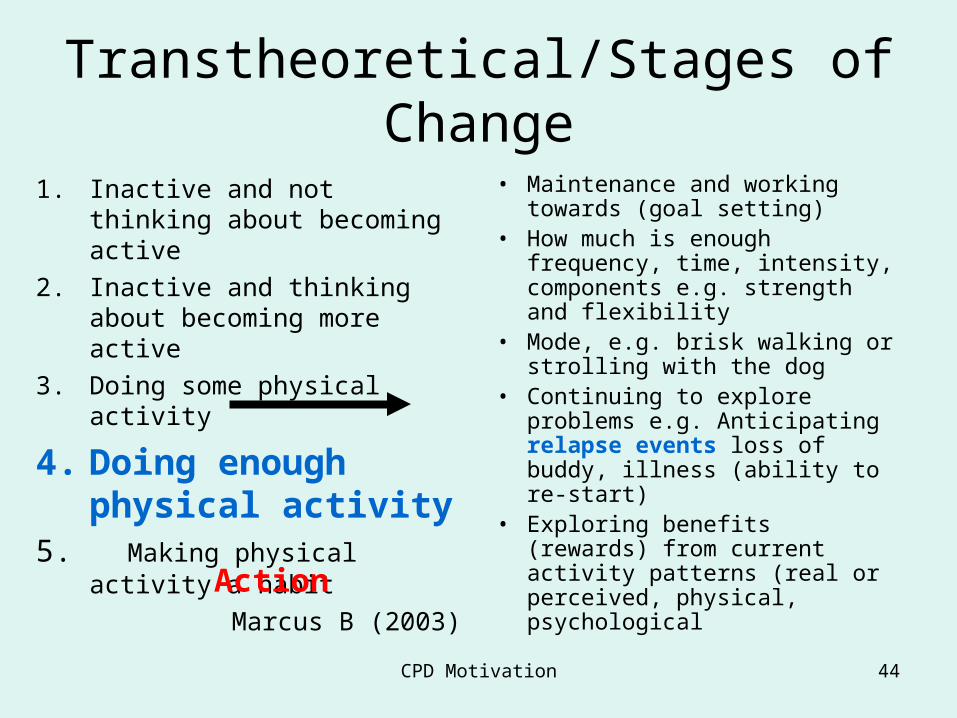
Transtheoretical/Stages of Change
1. Inactive and not thinking about becoming active
2. Inactive and thinking about becoming more active
3. Doing some physical activity
4. Doing enough physical activity
5. Making physical activity a habit
Marcus B (2003)
• Maintenance and working towards (goal setting)
• How much is enough frequency, time, intensity, components e.g. strength and flexibility
• Mode, e.g. brisk walking or strolling with the dog
• Continuing to explore problems e.g. Anticipating relapse events loss of buddy, illness (ability to re-start)
• Exploring benefits (rewards) from current activity patterns (real or perceived, physical, psychological
Action
CPD Motivation 45
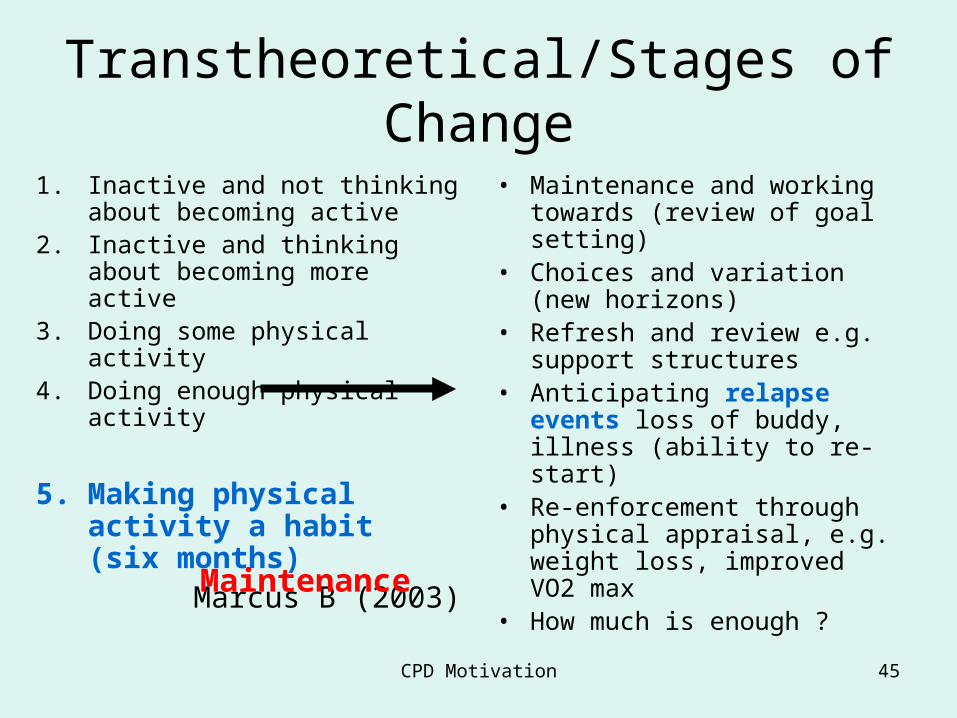
Transtheoretical/Stages of Change
1. Inactive and not thinking about becoming active
2. Inactive and thinking about becoming more active
3. Doing some physical activity4. Doing enough physical activity
5. Making physical activity a habit (six months)
Marcus B (2003)
• Maintenance and working towards (review of goal setting)
• Choices and variation (new horizons)
• Refresh and review e.g. support structures
• Anticipating relapse events loss of buddy, illness (ability to re-start)
• Re-enforcement through physical appraisal, e.g. weight loss, improved VO2 max
• How much is enough ?Maintenance
CPD Motivation 46
Lapse or Relapse model
• What are the situations that might result in drop out ?
CPD Motivation 47
Lapse or Relapse model
• What are the situations that might result in drop out ?
• It poured with rain all day• Injury/illness• I didn’t want to go• Increased work/caring• Loss of buddy, partner• Moving houseMonitoring to anticipate – relapse is normal
CPD Motivation 48
Lapse or Relapse model
What’s the difference ?
• Lapse is missing a session or two
• Relapse returning to sedentary behaviour
What’s your role once relapse occurs ?
CPD Motivation 49
Key questions to ask (exploring thoughts)
• Importance question - I wonder how important being active is for you ?
• General questions - What kinds of physical activity do you do at the moment ?
• Benefits question - Imagine if you did more, what benefits would you expect to see ?
• Barriers question - What things prevent you from being more active ?
• Concerns question - What things worry you about being more active ?
CPD Motivation 50
Listening and talking about physical activity
Our response
1. Respond to barriers
2. Investigate neutral responses
3. Build upon positive answers (reinforce through goal setting)
CPD Motivation 51
Neutral responses
• Well I don’t know but ……
• Imagine if…
• What could you see yourself doing ?
• How could we get there ?
CPD Motivation 52
Motivation
Helping people make decisions…..
Helping people to motivate themselves
CPD Motivation 53
So far !
• PSI perceptions of motivation, barriers• Evidence around physical activity and
older people• Evidence relating to falls advice and
exercise• Theory of helping people change
behaviour• Listening and talking about physical
activity
CPD Motivation 54
Session 3
Strategies to increase adherence• Induction strategies
• Goal setting
• Support strategies

CPD Motivation 55
Getting started
Once they have made a decision to come
The induction process
What are the most common questions and concerns that appear at this stage ?
CPD Motivation 56
Common barriers
• Fear of falling or fear of the unknown
• Over-exertion
• Harming oneself
• Make a condition worse
• Others ?
CPD Motivation 57
The induction session
What’s the model of best practice ?
What are the key elements you need to cover
(outlined in LLT manual)
CPD Motivation 58
Goal setting – 6 steps
1. Expectations (during individual screening or initial assessment ?)
2. Set own goals SMART - long term and short term (Early goals must be achieved so behavioural goals not outcomes (self-efficacy)
3. Monitor and provide feedback4. Reward and incentives5. Problem solving to overcome obstacles6. Promote long term adherence
(Jones and Rose 2005)
CPD Motivation 59
Goal setting
• Behavioural • Outcome goals
What short term goals can we set that lead to early success and
achievement ?

CPD Motivation 60
Goal setting
• Behavioural (short term)
• To attend the next three classes
• To keep Tuesdays clear
• Outcome goals (long term)
• To increase strength• To improve balance• To improve
independence
Establish patterns of behaviour and success that will lead to longer term goals
CPD Motivation 61
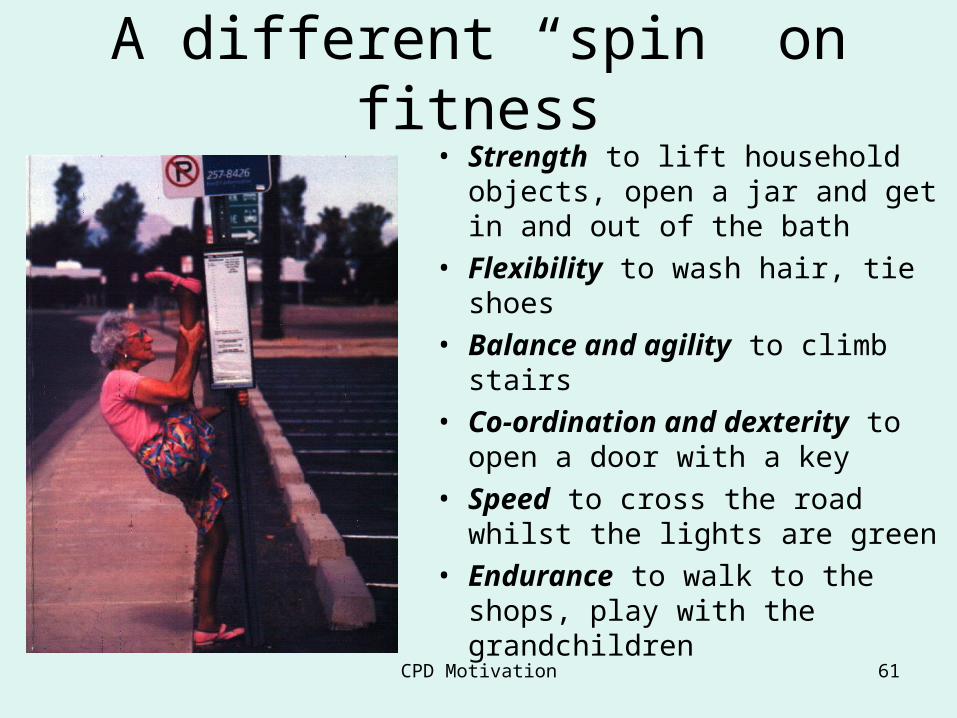
A different “spin” on fitness• Strength to lift household
objects, open a jar and get in and out of the bath
• Flexibility to wash hair, tie shoes• Balance and agility to climb
stairs• Co-ordination and dexterity to
open a door with a key• Speed to cross the road whilst
the lights are green• Endurance to walk to the shops,
play with the grandchildren

CPD Motivation 62
Getting our message across
Strong arms give
better hugs
CPD Motivation 63
Getting our message across
“She deserves to dance with Grandpa”
CPD Motivation 64
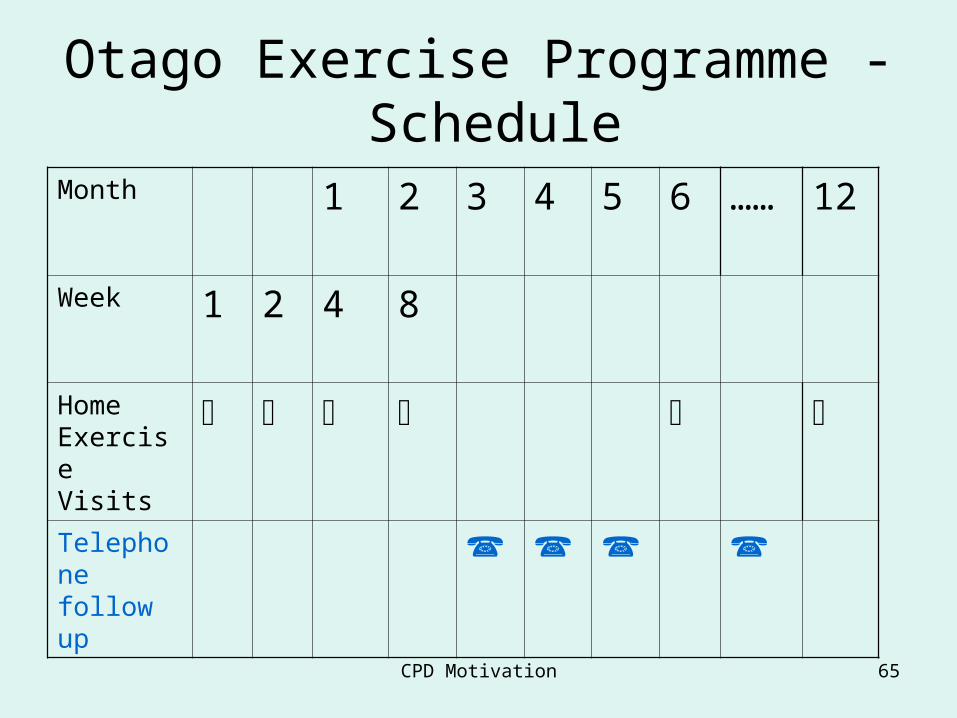
Otago Exercise Programme - Schedule
• X 4 home visits in first 2 months
• Booster visit at 6 months
• 1 hour first visit, 30 mins.v subsequent visits
• Telephone call x 1 p/m between visits
• Exercises (warm up, strength, balance, flexibility, cool down)
• Walking
CPD Motivation 65
Otago Exercise Programme - Schedule
Month 1 2 3 4 5 6 ……
12
Week 1 2 4 8
Home Exercise Visits
Telephone follow up
CPD Motivation 66
Support strategies
• All literature provides strong evidence that they are effective (NICE, HDA, CDC, Campbell, FAME)
• Communication strategies
• Technologies
• Activities
Which are the “three best buys ?”
CPD Motivation 67
Kirklees PAMs
• Local exercise referral programme for “at risk” and CHD rehab
• Volunteer buddies attached to programme• Trained in understanding physical activity and
health, understanding barriers and motivation• Integral to programme e.g. “Meet and greet”, 1
to 1 support• NB Not instructors• 96% + within programme beyond 12 months
CPD Motivation 68
Session 4
Increasing participation through choices
• Home based exercise
• Active Lifestyles approaches
• Summary and evaluation
CPD Motivation 69
Increasing participation through choices
Evidence supports effectiveness of outcomes
• Home based exercise
• Active Lifestyles approaches e.g. the promotion of walking
• Exit routes
CPD Motivation 70
Home based exercise and walking
• From home or at home ?
• Evidence is equivocal
• Ease of access
• 20 minutes max ?
• Strategies to improve ?
CPD Motivation 71
Independent choices
What strategies have you employed that have lead to success in
• Home based exercise programme
• Walking
• Access and exit to other programmes
CPD Motivation 72
Implications for practice
Learning Actions
1 1
2 2
3 3
CPD Motivation 73
Aims of the Day - reflection
• to review instructors’ experience of motivating participants and the barriers they face in adopting and maintaining exercise behaviour
• to introduce instructors to the theoretical principles of motivation and adherence to exercise
• to introduce instructors to the specific motivational issues related to exercise and falls programmes
• to introduce exercise instructors to strategies designed to support exercise participation
• to enable instructors to practise listening and talking about overcoming barriers to exercise
and ………?
CPD Motivation 74
Evaluation
Other information (certificates)
Safe journey home
www.laterlifetraining.co.uk
Recommended