1
AASLD COVID-19 Clinical Oversight amp Publications Subcommittee Presents
COVID-19 and the Liver Reentry and Return to a Pre-Pandemic State
May 14 20204-5 pm ET
PresentersPatricia Harren DNP DCC
David C Mulligan MD FAASLDBilal Hameed MD
ModeratorKimberly Ann Brown MD FAASLD
Webinar ModeratorKimberly Ann Brown MD
FAASLDChief Division of
Gastroenterology amp Hepatology
Henry Ford Health System
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 2
Webinar PresenterPatricia Harren DNP DCC
Clinical Director of the Center for Liver Disease amp Transplantation Clinical Director for Pediatric Transplantation
amp Adult Abdominal Organ Transplantation
Columbia University
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 3
Webinar PresenterDavid C Mulligan MD FAASLDProfessor of Surgery and Chief
of Transplantation and Immunology
Yale University Yale New Haven Health System
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 4
Webinar PresenterBilal Hameed MD
Associate Professor of Medicine and the Hepatology Clinic Chief
University of California San Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 5
6
Connect with AASLD
aasldorgtwitterAASLDtweets
aasldorginstagram
aasldorgfacebook
aasldorglinkedinaasldorgyoutube
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 7
For resources and updates on COVID-19 and the liver visit aasldorgCOVID19
8
o Special Interest Group participationo Priority housing and registration with discounts to The Liver Meetingreg
and DDWreg
o Free or discounted subscriptions to AASLD journals HEPATOLOGY and Liver Transplantation
o Complimentary access to premier hepatology online education in LiverLearningreg
o Individual and corporate non-physician memberships available
AASLD Member Benefits
aasldorgmembership
9
Join the COVID-19 Discussion Community on Engage
engageaasldorgcovid19
10
New AASLD Journals App
Access all four AASLD Journals in a single app
aasldorgpublications
11
Submit abstracts at aasldorgLMabstracts
a a s l d f n d o r g d o n a t e
CME MOC and E
Available
a a s l d f n d o r g
You can help invest in the future of hepatology by supporting
more research amp advanced career training
Donate today to AASLD Foundation
Follow us on Twitter AASLDFoundation
aasldfoundationorgdonate
13
Register Now for May 28th Webinar
AASLD-ALEH COVID-19 amp the Liver in the Americas
aasldorgcalendar
14
COVID-19 and the Liver Reentry and Return to a Pre-Pandemic State
o Webinar Contributorso Presenter Introductions ndash Dr Kimberly Brown
o Housekeeping Itemso OpenSAFELY Study ndash Dr Kimberly Brown
o Expert Consensus Panel Update ndash Dr Oren Fixo Outpatient ndash Dr Bilal Hameedo Inpatient ndash Dr Patricia Harreno Transplant ndash Dr David Mulligan
o Panel Discussion QampA
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 15
Webinar Agenda
o Co-chair Oren K Fix MD MSc FAASLD Swedish Medical Center (Washington)
o Co-chair Elizabeth C Verna MD MS Columbia University (New York)
o Kimberly Brown MD Henry Ford Health System (Michigan)
o Jaime Chu MD Icahn School of Medicine at Mount Sinai (New York)
o Bilal Hameed MD University of California (California)
o Laura M Kulik MD Northwestern Medical Faculty Foundation (Illinois)
o Ryan M Kwok MD Uniformed Services University (Maryland)
o Brendan M McGuire MD University of Alabama (Alabama)
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 16
o Jennifer Price MD MBA FACP University of California San Francisco (California)
o Daniel S Pratt MD FAASLD Massachusetts General Hospital (Massachusetts)
o Nancy S Reau MD Rush University (Illinois)
o Mark W Russo MD MPH FAASLD Carolinas Medical Center (North Carolina)
o Michael Schilsky MD FAASLD Yale University (Connecticut)
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC (California)
o Andrew Reynolds (Patient Advocate)o Raymond Chung and K Rajender Reddy
(ex-officio)
Clinical Oversight amp Publications Subcommittee
Submit your questions in the QampA box at the top or bottom of your screen
Questions will be answered at the end of the presentation
Webinar QampA
Webinar ModeratorKimberly Ann Brown MD
FAASLDChief Division of
Gastroenterology amp Hepatology
Henry Ford Health System
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 18
Webinar PresenterBilal Hameed MD
Associate Professor of Medicine and the Hepatology Clinic Chief
University of California San Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 19
Webinar PresenterPatricia Harren DNP DCC
Clinical Director of the Center for Liver Disease amp Transplantation Clinical Director for Pediatric Transplantation
amp Adult Abdominal Organ Transplantation
Columbia University
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 20
Webinar PresenterDavid C Mulligan MD FAASLDProfessor of Surgery and Chief
of Transplantation and Immunology
Yale University Yale New Haven Health System
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 21
o Oren K Fix MD MSc FAASLD Swedish Medical Center (Washington)
o Elizabeth C Verna MD MS Columbia University (New York)
o Jaime Chu MD Icahn School of Medicine at Mount Sinai (New York)
o Karen Hoyt BA Patient Advocate
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 22
o Guadalupe Garcia-Tsao MD FAASLD Yale University (Connecticut)
o Ryutaro Hirose MD University of California San Francisco (California)
o K Gautham Reddy MD FAASLD University of Chicago Medical Center (Illinois)
Webinar Panelist
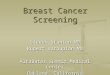
o OpenSAFELY Factors associated with COVID-19-related hospital deaths in the linked electronic health records of 17 million adult NHS patientsbull 17425445 adultsbull Feb 1 2020 to April 25 2020bull Primary outcome death in hospital in patients with confirmed
COVID-19 (5683 deaths)
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
httpsdoiorg1011012020050620092999
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
httpsdoiorg1011012020050620092999
HR adjusted for all other factors listed other than ethnicity
o Largest cohort study to date evaluating a variety of clinical factors for death from COVID-19
o Asians and blacks appear to be at increased risk of in-hospital death with only partial attribution to pre-existing clinical risk factors or deprivation
o Patients with pre-existing liver disease transplantation or on immunosuppression appear to have increased risk of in-hospital death when adjusted for agesex alone or fully adjusted
o Strengthsbull Largest cohort study to date representing 40 English populationbull Inclusion of variables including liver disease transplant for analysis
o Weaknessesbull Deaths related to patients with false-negative tests or died without testing would be missedbull Censoring patients at date of death from other causes or outside the hospital stopped 9
days short of study end bull Cohort limited to those practices using the EHR software SystmOne Some variable were
assumed absent if missing bull Characterization of ldquoliver diseaserdquo is general and not complete
o Further characterization of liver disease and potential risks due to etiology MELD etc will be helpful in future studies
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORGhttpsdoiorg1011012020050620092999
Expert Panel Consensus Statement
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 26
o First published online March 23rdo New update posted today
wwwaasldorgcovid19o Spanish and Portuguese
translations available onlineo Hepatology manuscript published
online
May 14th Update Major Changes
o Acknowledgement of possible link between COVID-19 and Kawasaki-like pediatric multisystem inflammatory syndrome
o Italian autopsy series describing involvement of hepatic vasculature including acute portal and sinusoidal thrombosis
o Introduction of SARS-CoV-2 antigen testing in addition to increasing availability of antibody testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 27
httpswwwhealthnygovpressreleases2020docs2020-05-06_covid19_pediatric_inflammatory_syndromepdfSonzogni et al Preprints 2020httpswwwfdagovnews-eventspress-announcementscoronavirus-covid-19-update-fda-authorizes-first-antigen-test-help-rapid-detection-virus-causes
May 14th Update Major Changes
o OpenSAFELY study from the UK chronic liver disease is a risk factor for in-hospital death from COVID-19
o Large US study also showed that chronic liver disease and cirrhosis are associated with higher COVID-19 mortality
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 28
Williamson et al MedRxiv 2020Singh and Khan Gastroenterol 2020
May 14th Update Major Changes
o Clarification that treatment of hepatitis B is not contraindicated in patients with or without COVID-19
o Recommendations regarding use of masks for patients and caregivers as well as providers in the clinic or hospital setting
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 29
May 14th Update Major Changes
o Evolving data on hydroxychloroquine suggesting it should no longer be used outside RCTs
o New data on triple therapy with lopinavir-ritonavir ribavirin and interferon-beta-1b showing more rapid viral clearance compared to lopinavir-ritonavir (phase 2 RCT)
o Reentry
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 30
Geleris et al N Eng J Med 2020Hung et al Lancet 2020
31
Impact of COVID-19 on Liver Disease Safe Outpatient Re-Entry Process
Bilal Hameed MDAssociate Professor of Medicine
Clinic Chief Hepatology University of California San Francisco
Outline
The COVID-19 effects on liver care Recommendations for re-entry and re-opening facilities Ambulatory re-entry and recovery challenges and plan
at UCSF Gradual re-entry of liver patients in the ambulatory
setting
The Untold Toll mdash The Pandemicrsquos Effects on Patients without COVID-19
httpswwwnejmorgdoifull101056NEJMms2009984query=featured_coronavirus
Patients with heart attacks strokes and even appendicitis vanish from
hospitals
The Pandemicrsquos Effects on Patients without COVID-1938 reduction in STEMI activations in the US
during COVID-19 pandemic
Garcia S et al Journal of the American College of Cardiology April 2020
Decrease in routine pediatric vaccination during COVID-19
httpswwwcdcgovmmwrvolumes69wr
Unexpected Consequences of the Pandemic
To expand capacity for COVID-19 patients on March 18th CMS recommended limiting non-essential care and procedures 8 week pause in usual care activities Fear of returning to care Change in patientrsquos perception of riskbenefit
Areas with lowstable incidence of COVID-19 CMS allowing non-emergent non-COVID-19 healthcare
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdf
COVID-19 Pandemic Impact on the Cirrhosis Care
Tapper EB et al Journal of Hepatology April 2020
COVID Surge
Loss of insurance
Outpatient Impact of COVID-19 Pandemic UCSF Experience Maximizing Appropriate Use of Video Visits during Re-entry
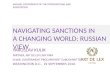
Prior State Current State Future State~20 of total visits were video visits
~95 of total visits are video visits
Appropriate mix of telehealth visits ~50
Continue expanding to -Patients that live far away -Post-ops amp post-discharge follow-up-Chronic disease management(NAFLDHBVHCV etc)-Free up clinic space
0
10000
20000
30000
40000
50000
60000
70000
End of April Double March volume
February 2 of all visits2nd largest video visit program in the
country among AMCs largest in California
End of March 60 of visits
UCSF Video Visits by Month (Jan 2015-April 2020)
0
100
200
300
400
500
600
700
800
900
Jul 2019 Aug Sep Oct Nov Dec Jan 2020 Feb Mar Apr
Able to see the same number of patients even during pandemic
Hepatology Video Visits by Month at UCSF
CMS Phase I Recommendations Re-opening Facilities for Non-emergent Non-COVID-19 Healthcare
In coordination with State and local public health officials evaluate the incidence and trends for COVID-19 in the area
Prioritize surgicalprocedural care and high-complexity chronic disease management and select preventive services
Consider establishing Non-COVID Care (NCC) zones that would screen all patients for symptoms of COVID-19
Sufficient resources should be available across phases of care including PPE healthy workforce testing capacity etc and without jeopardizing surge capacity
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdfhttpswwwwhitehousegovopeningamericacriteriahttpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
httpsdatasfgovorgstoriessdak2-gvuj
San Francisco COVID-19 Numbers
Ambulatory Re-entry and Recovery ndash Cascaded Principles
Ensure morbidity and mortality do not increase due to liver related illness and provide care in a safe manner
Continue to prioritize the health and safety of workforce Prioritize urgent patients Communicate consistently and transparently Invest appropriately in services and improvement efforts
Strategies to limit unnecessary exposure while continuing to provide high-quality care for our liver patients
bull Optimization and flexibility of schedules (hoursweekend)
bull Utilization of clinic spacebull Sustain telehealth bull Digital technology for symptoms
monitoring bull Staff redeployment
bull COVID symptoms check protocolbull Social distancing in clinicbull Masking and safety policiesbull Waiting rooms changesbull Visitor policies
bull Prioritize urgent patientsbull Back log data and referralsbull Pre-clinic communicationbull In clinic flow (Echeck in rooming
and check out policies)
bull Patient communication is the keybull Staff anxiety and stress reduction bull Focus on vulnerable populationbull Physician burn out and health needs bull Trainees re-entry and education
Staff and PatientSafety
Clinic Work Flows
Resource Utilization
Support and
Education
PatientCare
Ambulatory Recovery Challenges and PlanProviding Best Care While Living with COVID-19
Physical Distancing amp Safety Guidelines
Conversa Employee Screening Mychart Screener Apex texting for patients in
nearby waiting areas
Innovation and Improving Operations
Gradual Re-entry of Liver Patients in the Ambulatory Setting
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
Patient will be scheduled for modified evaluation with
Hepatology and social worker as video visit
Remainder of evaluation will be onsite when restrictions are lifted
1 Pre-clinicarrival COVID screening for patientscaregiver2 Universal masking
no
Re-entry of Liver Patients in Clinic June 2020
All new liver transplant evaluations and HCC diagnosis New decompensation or worsening symptoms Listed patients for transplant with decompensated cirrhosis Acute hepatitis or liver injury Early post transplant Patients with difficulty with telehealth
Re-entry of Liver Patients HCC Surveillance HCC surveillance should continue as close to schedule (an
arbitrary delay of 2 months were acceptable) Working on list of all delayed imaging and prioritizing them by
risk categoriesKnown HCC surveillance for treatment response elevated AFP
Key is working with Radiology (Options of imaging locally) Communication with patients and documentation is important No delay in HCC treatment (riskbenefits discussion)
httpswwwaasldorgsitesdefaultfiles2020-05AASLD-COVID19-ClinicalInsights-May42020
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
Fibroscan Not urgent but planning to
start June-July 2020 Huge back log Using radiology US protocol
for PPE (maskgoogles and gown) Flexible schedules based on
safety guidelines
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

Webinar ModeratorKimberly Ann Brown MD
FAASLDChief Division of
Gastroenterology amp Hepatology
Henry Ford Health System
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 2
Webinar PresenterPatricia Harren DNP DCC
Clinical Director of the Center for Liver Disease amp Transplantation Clinical Director for Pediatric Transplantation
amp Adult Abdominal Organ Transplantation
Columbia University
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 3
Webinar PresenterDavid C Mulligan MD FAASLDProfessor of Surgery and Chief
of Transplantation and Immunology
Yale University Yale New Haven Health System
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 4
Webinar PresenterBilal Hameed MD
Associate Professor of Medicine and the Hepatology Clinic Chief
University of California San Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 5
6
Connect with AASLD
aasldorgtwitterAASLDtweets
aasldorginstagram
aasldorgfacebook
aasldorglinkedinaasldorgyoutube
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 7
For resources and updates on COVID-19 and the liver visit aasldorgCOVID19
8
o Special Interest Group participationo Priority housing and registration with discounts to The Liver Meetingreg
and DDWreg
o Free or discounted subscriptions to AASLD journals HEPATOLOGY and Liver Transplantation
o Complimentary access to premier hepatology online education in LiverLearningreg
o Individual and corporate non-physician memberships available
AASLD Member Benefits
aasldorgmembership
9
Join the COVID-19 Discussion Community on Engage
engageaasldorgcovid19
10
New AASLD Journals App
Access all four AASLD Journals in a single app
aasldorgpublications
11
Submit abstracts at aasldorgLMabstracts
a a s l d f n d o r g d o n a t e
CME MOC and E
Available
a a s l d f n d o r g
You can help invest in the future of hepatology by supporting
more research amp advanced career training
Donate today to AASLD Foundation
Follow us on Twitter AASLDFoundation
aasldfoundationorgdonate
13
Register Now for May 28th Webinar
AASLD-ALEH COVID-19 amp the Liver in the Americas
aasldorgcalendar
14
COVID-19 and the Liver Reentry and Return to a Pre-Pandemic State
o Webinar Contributorso Presenter Introductions ndash Dr Kimberly Brown
o Housekeeping Itemso OpenSAFELY Study ndash Dr Kimberly Brown
o Expert Consensus Panel Update ndash Dr Oren Fixo Outpatient ndash Dr Bilal Hameedo Inpatient ndash Dr Patricia Harreno Transplant ndash Dr David Mulligan
o Panel Discussion QampA
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 15
Webinar Agenda
o Co-chair Oren K Fix MD MSc FAASLD Swedish Medical Center (Washington)
o Co-chair Elizabeth C Verna MD MS Columbia University (New York)
o Kimberly Brown MD Henry Ford Health System (Michigan)
o Jaime Chu MD Icahn School of Medicine at Mount Sinai (New York)
o Bilal Hameed MD University of California (California)
o Laura M Kulik MD Northwestern Medical Faculty Foundation (Illinois)
o Ryan M Kwok MD Uniformed Services University (Maryland)
o Brendan M McGuire MD University of Alabama (Alabama)
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 16
o Jennifer Price MD MBA FACP University of California San Francisco (California)
o Daniel S Pratt MD FAASLD Massachusetts General Hospital (Massachusetts)
o Nancy S Reau MD Rush University (Illinois)
o Mark W Russo MD MPH FAASLD Carolinas Medical Center (North Carolina)
o Michael Schilsky MD FAASLD Yale University (Connecticut)
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC (California)
o Andrew Reynolds (Patient Advocate)o Raymond Chung and K Rajender Reddy
(ex-officio)
Clinical Oversight amp Publications Subcommittee
Submit your questions in the QampA box at the top or bottom of your screen
Questions will be answered at the end of the presentation
Webinar QampA
Webinar ModeratorKimberly Ann Brown MD
FAASLDChief Division of
Gastroenterology amp Hepatology
Henry Ford Health System
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 18
Webinar PresenterBilal Hameed MD
Associate Professor of Medicine and the Hepatology Clinic Chief
University of California San Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 19
Webinar PresenterPatricia Harren DNP DCC
Clinical Director of the Center for Liver Disease amp Transplantation Clinical Director for Pediatric Transplantation
amp Adult Abdominal Organ Transplantation
Columbia University
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 20
Webinar PresenterDavid C Mulligan MD FAASLDProfessor of Surgery and Chief
of Transplantation and Immunology
Yale University Yale New Haven Health System
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 21
o Oren K Fix MD MSc FAASLD Swedish Medical Center (Washington)
o Elizabeth C Verna MD MS Columbia University (New York)
o Jaime Chu MD Icahn School of Medicine at Mount Sinai (New York)
o Karen Hoyt BA Patient Advocate
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 22
o Guadalupe Garcia-Tsao MD FAASLD Yale University (Connecticut)
o Ryutaro Hirose MD University of California San Francisco (California)
o K Gautham Reddy MD FAASLD University of Chicago Medical Center (Illinois)
Webinar Panelist
o OpenSAFELY Factors associated with COVID-19-related hospital deaths in the linked electronic health records of 17 million adult NHS patientsbull 17425445 adultsbull Feb 1 2020 to April 25 2020bull Primary outcome death in hospital in patients with confirmed
COVID-19 (5683 deaths)
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
httpsdoiorg1011012020050620092999
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
httpsdoiorg1011012020050620092999
HR adjusted for all other factors listed other than ethnicity
o Largest cohort study to date evaluating a variety of clinical factors for death from COVID-19
o Asians and blacks appear to be at increased risk of in-hospital death with only partial attribution to pre-existing clinical risk factors or deprivation
o Patients with pre-existing liver disease transplantation or on immunosuppression appear to have increased risk of in-hospital death when adjusted for agesex alone or fully adjusted
o Strengthsbull Largest cohort study to date representing 40 English populationbull Inclusion of variables including liver disease transplant for analysis
o Weaknessesbull Deaths related to patients with false-negative tests or died without testing would be missedbull Censoring patients at date of death from other causes or outside the hospital stopped 9
days short of study end bull Cohort limited to those practices using the EHR software SystmOne Some variable were
assumed absent if missing bull Characterization of ldquoliver diseaserdquo is general and not complete
o Further characterization of liver disease and potential risks due to etiology MELD etc will be helpful in future studies
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORGhttpsdoiorg1011012020050620092999
Expert Panel Consensus Statement
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 26
o First published online March 23rdo New update posted today
wwwaasldorgcovid19o Spanish and Portuguese
translations available onlineo Hepatology manuscript published
online
May 14th Update Major Changes
o Acknowledgement of possible link between COVID-19 and Kawasaki-like pediatric multisystem inflammatory syndrome
o Italian autopsy series describing involvement of hepatic vasculature including acute portal and sinusoidal thrombosis
o Introduction of SARS-CoV-2 antigen testing in addition to increasing availability of antibody testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 27
httpswwwhealthnygovpressreleases2020docs2020-05-06_covid19_pediatric_inflammatory_syndromepdfSonzogni et al Preprints 2020httpswwwfdagovnews-eventspress-announcementscoronavirus-covid-19-update-fda-authorizes-first-antigen-test-help-rapid-detection-virus-causes
May 14th Update Major Changes
o OpenSAFELY study from the UK chronic liver disease is a risk factor for in-hospital death from COVID-19
o Large US study also showed that chronic liver disease and cirrhosis are associated with higher COVID-19 mortality
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 28
Williamson et al MedRxiv 2020Singh and Khan Gastroenterol 2020
May 14th Update Major Changes
o Clarification that treatment of hepatitis B is not contraindicated in patients with or without COVID-19
o Recommendations regarding use of masks for patients and caregivers as well as providers in the clinic or hospital setting
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 29
May 14th Update Major Changes
o Evolving data on hydroxychloroquine suggesting it should no longer be used outside RCTs
o New data on triple therapy with lopinavir-ritonavir ribavirin and interferon-beta-1b showing more rapid viral clearance compared to lopinavir-ritonavir (phase 2 RCT)
o Reentry
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 30
Geleris et al N Eng J Med 2020Hung et al Lancet 2020
31
Impact of COVID-19 on Liver Disease Safe Outpatient Re-Entry Process
Bilal Hameed MDAssociate Professor of Medicine
Clinic Chief Hepatology University of California San Francisco
Outline
The COVID-19 effects on liver care Recommendations for re-entry and re-opening facilities Ambulatory re-entry and recovery challenges and plan
at UCSF Gradual re-entry of liver patients in the ambulatory
setting
The Untold Toll mdash The Pandemicrsquos Effects on Patients without COVID-19
httpswwwnejmorgdoifull101056NEJMms2009984query=featured_coronavirus
Patients with heart attacks strokes and even appendicitis vanish from
hospitals
The Pandemicrsquos Effects on Patients without COVID-1938 reduction in STEMI activations in the US
during COVID-19 pandemic
Garcia S et al Journal of the American College of Cardiology April 2020
Decrease in routine pediatric vaccination during COVID-19
httpswwwcdcgovmmwrvolumes69wr
Unexpected Consequences of the Pandemic
To expand capacity for COVID-19 patients on March 18th CMS recommended limiting non-essential care and procedures 8 week pause in usual care activities Fear of returning to care Change in patientrsquos perception of riskbenefit
Areas with lowstable incidence of COVID-19 CMS allowing non-emergent non-COVID-19 healthcare
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdf
COVID-19 Pandemic Impact on the Cirrhosis Care
Tapper EB et al Journal of Hepatology April 2020
COVID Surge
Loss of insurance
Outpatient Impact of COVID-19 Pandemic UCSF Experience Maximizing Appropriate Use of Video Visits during Re-entry
Prior State Current State Future State~20 of total visits were video visits
~95 of total visits are video visits
Appropriate mix of telehealth visits ~50
Continue expanding to -Patients that live far away -Post-ops amp post-discharge follow-up-Chronic disease management(NAFLDHBVHCV etc)-Free up clinic space
0
10000
20000
30000
40000
50000
60000
70000
End of April Double March volume
February 2 of all visits2nd largest video visit program in the
country among AMCs largest in California
End of March 60 of visits
UCSF Video Visits by Month (Jan 2015-April 2020)
0
100
200
300
400
500
600
700
800
900
Jul 2019 Aug Sep Oct Nov Dec Jan 2020 Feb Mar Apr
Able to see the same number of patients even during pandemic
Hepatology Video Visits by Month at UCSF
CMS Phase I Recommendations Re-opening Facilities for Non-emergent Non-COVID-19 Healthcare
In coordination with State and local public health officials evaluate the incidence and trends for COVID-19 in the area
Prioritize surgicalprocedural care and high-complexity chronic disease management and select preventive services
Consider establishing Non-COVID Care (NCC) zones that would screen all patients for symptoms of COVID-19
Sufficient resources should be available across phases of care including PPE healthy workforce testing capacity etc and without jeopardizing surge capacity
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdfhttpswwwwhitehousegovopeningamericacriteriahttpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
httpsdatasfgovorgstoriessdak2-gvuj
San Francisco COVID-19 Numbers
Ambulatory Re-entry and Recovery ndash Cascaded Principles
Ensure morbidity and mortality do not increase due to liver related illness and provide care in a safe manner
Continue to prioritize the health and safety of workforce Prioritize urgent patients Communicate consistently and transparently Invest appropriately in services and improvement efforts
Strategies to limit unnecessary exposure while continuing to provide high-quality care for our liver patients
bull Optimization and flexibility of schedules (hoursweekend)
bull Utilization of clinic spacebull Sustain telehealth bull Digital technology for symptoms
monitoring bull Staff redeployment
bull COVID symptoms check protocolbull Social distancing in clinicbull Masking and safety policiesbull Waiting rooms changesbull Visitor policies
bull Prioritize urgent patientsbull Back log data and referralsbull Pre-clinic communicationbull In clinic flow (Echeck in rooming
and check out policies)
bull Patient communication is the keybull Staff anxiety and stress reduction bull Focus on vulnerable populationbull Physician burn out and health needs bull Trainees re-entry and education
Staff and PatientSafety
Clinic Work Flows
Resource Utilization
Support and
Education
PatientCare
Ambulatory Recovery Challenges and PlanProviding Best Care While Living with COVID-19
Physical Distancing amp Safety Guidelines
Conversa Employee Screening Mychart Screener Apex texting for patients in
nearby waiting areas
Innovation and Improving Operations
Gradual Re-entry of Liver Patients in the Ambulatory Setting
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
Patient will be scheduled for modified evaluation with
Hepatology and social worker as video visit
Remainder of evaluation will be onsite when restrictions are lifted
1 Pre-clinicarrival COVID screening for patientscaregiver2 Universal masking
no
Re-entry of Liver Patients in Clinic June 2020
All new liver transplant evaluations and HCC diagnosis New decompensation or worsening symptoms Listed patients for transplant with decompensated cirrhosis Acute hepatitis or liver injury Early post transplant Patients with difficulty with telehealth
Re-entry of Liver Patients HCC Surveillance HCC surveillance should continue as close to schedule (an
arbitrary delay of 2 months were acceptable) Working on list of all delayed imaging and prioritizing them by
risk categoriesKnown HCC surveillance for treatment response elevated AFP
Key is working with Radiology (Options of imaging locally) Communication with patients and documentation is important No delay in HCC treatment (riskbenefits discussion)
httpswwwaasldorgsitesdefaultfiles2020-05AASLD-COVID19-ClinicalInsights-May42020
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
Fibroscan Not urgent but planning to
start June-July 2020 Huge back log Using radiology US protocol
for PPE (maskgoogles and gown) Flexible schedules based on
safety guidelines
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

Webinar PresenterPatricia Harren DNP DCC
Clinical Director of the Center for Liver Disease amp Transplantation Clinical Director for Pediatric Transplantation
amp Adult Abdominal Organ Transplantation
Columbia University
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 3
Webinar PresenterDavid C Mulligan MD FAASLDProfessor of Surgery and Chief
of Transplantation and Immunology
Yale University Yale New Haven Health System
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 4
Webinar PresenterBilal Hameed MD
Associate Professor of Medicine and the Hepatology Clinic Chief
University of California San Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 5
6
Connect with AASLD
aasldorgtwitterAASLDtweets
aasldorginstagram
aasldorgfacebook
aasldorglinkedinaasldorgyoutube
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 7
For resources and updates on COVID-19 and the liver visit aasldorgCOVID19
8
o Special Interest Group participationo Priority housing and registration with discounts to The Liver Meetingreg
and DDWreg
o Free or discounted subscriptions to AASLD journals HEPATOLOGY and Liver Transplantation
o Complimentary access to premier hepatology online education in LiverLearningreg
o Individual and corporate non-physician memberships available
AASLD Member Benefits
aasldorgmembership
9
Join the COVID-19 Discussion Community on Engage
engageaasldorgcovid19
10
New AASLD Journals App
Access all four AASLD Journals in a single app
aasldorgpublications
11
Submit abstracts at aasldorgLMabstracts
a a s l d f n d o r g d o n a t e
CME MOC and E
Available
a a s l d f n d o r g
You can help invest in the future of hepatology by supporting
more research amp advanced career training
Donate today to AASLD Foundation
Follow us on Twitter AASLDFoundation
aasldfoundationorgdonate
13
Register Now for May 28th Webinar
AASLD-ALEH COVID-19 amp the Liver in the Americas
aasldorgcalendar
14
COVID-19 and the Liver Reentry and Return to a Pre-Pandemic State
o Webinar Contributorso Presenter Introductions ndash Dr Kimberly Brown
o Housekeeping Itemso OpenSAFELY Study ndash Dr Kimberly Brown
o Expert Consensus Panel Update ndash Dr Oren Fixo Outpatient ndash Dr Bilal Hameedo Inpatient ndash Dr Patricia Harreno Transplant ndash Dr David Mulligan
o Panel Discussion QampA
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 15
Webinar Agenda
o Co-chair Oren K Fix MD MSc FAASLD Swedish Medical Center (Washington)
o Co-chair Elizabeth C Verna MD MS Columbia University (New York)
o Kimberly Brown MD Henry Ford Health System (Michigan)
o Jaime Chu MD Icahn School of Medicine at Mount Sinai (New York)
o Bilal Hameed MD University of California (California)
o Laura M Kulik MD Northwestern Medical Faculty Foundation (Illinois)
o Ryan M Kwok MD Uniformed Services University (Maryland)
o Brendan M McGuire MD University of Alabama (Alabama)
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 16
o Jennifer Price MD MBA FACP University of California San Francisco (California)
o Daniel S Pratt MD FAASLD Massachusetts General Hospital (Massachusetts)
o Nancy S Reau MD Rush University (Illinois)
o Mark W Russo MD MPH FAASLD Carolinas Medical Center (North Carolina)
o Michael Schilsky MD FAASLD Yale University (Connecticut)
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC (California)
o Andrew Reynolds (Patient Advocate)o Raymond Chung and K Rajender Reddy
(ex-officio)
Clinical Oversight amp Publications Subcommittee
Submit your questions in the QampA box at the top or bottom of your screen
Questions will be answered at the end of the presentation
Webinar QampA
Webinar ModeratorKimberly Ann Brown MD
FAASLDChief Division of
Gastroenterology amp Hepatology
Henry Ford Health System
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 18
Webinar PresenterBilal Hameed MD
Associate Professor of Medicine and the Hepatology Clinic Chief
University of California San Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 19
Webinar PresenterPatricia Harren DNP DCC
Clinical Director of the Center for Liver Disease amp Transplantation Clinical Director for Pediatric Transplantation
amp Adult Abdominal Organ Transplantation
Columbia University
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 20
Webinar PresenterDavid C Mulligan MD FAASLDProfessor of Surgery and Chief
of Transplantation and Immunology
Yale University Yale New Haven Health System
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 21
o Oren K Fix MD MSc FAASLD Swedish Medical Center (Washington)
o Elizabeth C Verna MD MS Columbia University (New York)
o Jaime Chu MD Icahn School of Medicine at Mount Sinai (New York)
o Karen Hoyt BA Patient Advocate
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 22
o Guadalupe Garcia-Tsao MD FAASLD Yale University (Connecticut)
o Ryutaro Hirose MD University of California San Francisco (California)
o K Gautham Reddy MD FAASLD University of Chicago Medical Center (Illinois)
Webinar Panelist
o OpenSAFELY Factors associated with COVID-19-related hospital deaths in the linked electronic health records of 17 million adult NHS patientsbull 17425445 adultsbull Feb 1 2020 to April 25 2020bull Primary outcome death in hospital in patients with confirmed
COVID-19 (5683 deaths)
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
httpsdoiorg1011012020050620092999
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
httpsdoiorg1011012020050620092999
HR adjusted for all other factors listed other than ethnicity
o Largest cohort study to date evaluating a variety of clinical factors for death from COVID-19
o Asians and blacks appear to be at increased risk of in-hospital death with only partial attribution to pre-existing clinical risk factors or deprivation
o Patients with pre-existing liver disease transplantation or on immunosuppression appear to have increased risk of in-hospital death when adjusted for agesex alone or fully adjusted
o Strengthsbull Largest cohort study to date representing 40 English populationbull Inclusion of variables including liver disease transplant for analysis
o Weaknessesbull Deaths related to patients with false-negative tests or died without testing would be missedbull Censoring patients at date of death from other causes or outside the hospital stopped 9
days short of study end bull Cohort limited to those practices using the EHR software SystmOne Some variable were
assumed absent if missing bull Characterization of ldquoliver diseaserdquo is general and not complete
o Further characterization of liver disease and potential risks due to etiology MELD etc will be helpful in future studies
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORGhttpsdoiorg1011012020050620092999
Expert Panel Consensus Statement
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 26
o First published online March 23rdo New update posted today
wwwaasldorgcovid19o Spanish and Portuguese
translations available onlineo Hepatology manuscript published
online
May 14th Update Major Changes
o Acknowledgement of possible link between COVID-19 and Kawasaki-like pediatric multisystem inflammatory syndrome
o Italian autopsy series describing involvement of hepatic vasculature including acute portal and sinusoidal thrombosis
o Introduction of SARS-CoV-2 antigen testing in addition to increasing availability of antibody testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 27
httpswwwhealthnygovpressreleases2020docs2020-05-06_covid19_pediatric_inflammatory_syndromepdfSonzogni et al Preprints 2020httpswwwfdagovnews-eventspress-announcementscoronavirus-covid-19-update-fda-authorizes-first-antigen-test-help-rapid-detection-virus-causes
May 14th Update Major Changes
o OpenSAFELY study from the UK chronic liver disease is a risk factor for in-hospital death from COVID-19
o Large US study also showed that chronic liver disease and cirrhosis are associated with higher COVID-19 mortality
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 28
Williamson et al MedRxiv 2020Singh and Khan Gastroenterol 2020
May 14th Update Major Changes
o Clarification that treatment of hepatitis B is not contraindicated in patients with or without COVID-19
o Recommendations regarding use of masks for patients and caregivers as well as providers in the clinic or hospital setting
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 29
May 14th Update Major Changes
o Evolving data on hydroxychloroquine suggesting it should no longer be used outside RCTs
o New data on triple therapy with lopinavir-ritonavir ribavirin and interferon-beta-1b showing more rapid viral clearance compared to lopinavir-ritonavir (phase 2 RCT)
o Reentry
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 30
Geleris et al N Eng J Med 2020Hung et al Lancet 2020
31
Impact of COVID-19 on Liver Disease Safe Outpatient Re-Entry Process
Bilal Hameed MDAssociate Professor of Medicine
Clinic Chief Hepatology University of California San Francisco
Outline
The COVID-19 effects on liver care Recommendations for re-entry and re-opening facilities Ambulatory re-entry and recovery challenges and plan
at UCSF Gradual re-entry of liver patients in the ambulatory
setting
The Untold Toll mdash The Pandemicrsquos Effects on Patients without COVID-19
httpswwwnejmorgdoifull101056NEJMms2009984query=featured_coronavirus
Patients with heart attacks strokes and even appendicitis vanish from
hospitals
The Pandemicrsquos Effects on Patients without COVID-1938 reduction in STEMI activations in the US
during COVID-19 pandemic
Garcia S et al Journal of the American College of Cardiology April 2020
Decrease in routine pediatric vaccination during COVID-19
httpswwwcdcgovmmwrvolumes69wr
Unexpected Consequences of the Pandemic
To expand capacity for COVID-19 patients on March 18th CMS recommended limiting non-essential care and procedures 8 week pause in usual care activities Fear of returning to care Change in patientrsquos perception of riskbenefit
Areas with lowstable incidence of COVID-19 CMS allowing non-emergent non-COVID-19 healthcare
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdf
COVID-19 Pandemic Impact on the Cirrhosis Care
Tapper EB et al Journal of Hepatology April 2020
COVID Surge
Loss of insurance
Outpatient Impact of COVID-19 Pandemic UCSF Experience Maximizing Appropriate Use of Video Visits during Re-entry
Prior State Current State Future State~20 of total visits were video visits
~95 of total visits are video visits
Appropriate mix of telehealth visits ~50
Continue expanding to -Patients that live far away -Post-ops amp post-discharge follow-up-Chronic disease management(NAFLDHBVHCV etc)-Free up clinic space
0
10000
20000
30000
40000
50000
60000
70000
End of April Double March volume
February 2 of all visits2nd largest video visit program in the
country among AMCs largest in California
End of March 60 of visits
UCSF Video Visits by Month (Jan 2015-April 2020)
0
100
200
300
400
500
600
700
800
900
Jul 2019 Aug Sep Oct Nov Dec Jan 2020 Feb Mar Apr
Able to see the same number of patients even during pandemic
Hepatology Video Visits by Month at UCSF
CMS Phase I Recommendations Re-opening Facilities for Non-emergent Non-COVID-19 Healthcare
In coordination with State and local public health officials evaluate the incidence and trends for COVID-19 in the area
Prioritize surgicalprocedural care and high-complexity chronic disease management and select preventive services
Consider establishing Non-COVID Care (NCC) zones that would screen all patients for symptoms of COVID-19
Sufficient resources should be available across phases of care including PPE healthy workforce testing capacity etc and without jeopardizing surge capacity
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdfhttpswwwwhitehousegovopeningamericacriteriahttpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
httpsdatasfgovorgstoriessdak2-gvuj
San Francisco COVID-19 Numbers
Ambulatory Re-entry and Recovery ndash Cascaded Principles
Ensure morbidity and mortality do not increase due to liver related illness and provide care in a safe manner
Continue to prioritize the health and safety of workforce Prioritize urgent patients Communicate consistently and transparently Invest appropriately in services and improvement efforts
Strategies to limit unnecessary exposure while continuing to provide high-quality care for our liver patients
bull Optimization and flexibility of schedules (hoursweekend)
bull Utilization of clinic spacebull Sustain telehealth bull Digital technology for symptoms
monitoring bull Staff redeployment
bull COVID symptoms check protocolbull Social distancing in clinicbull Masking and safety policiesbull Waiting rooms changesbull Visitor policies
bull Prioritize urgent patientsbull Back log data and referralsbull Pre-clinic communicationbull In clinic flow (Echeck in rooming
and check out policies)
bull Patient communication is the keybull Staff anxiety and stress reduction bull Focus on vulnerable populationbull Physician burn out and health needs bull Trainees re-entry and education
Staff and PatientSafety
Clinic Work Flows
Resource Utilization
Support and
Education
PatientCare
Ambulatory Recovery Challenges and PlanProviding Best Care While Living with COVID-19
Physical Distancing amp Safety Guidelines
Conversa Employee Screening Mychart Screener Apex texting for patients in
nearby waiting areas
Innovation and Improving Operations
Gradual Re-entry of Liver Patients in the Ambulatory Setting
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
Patient will be scheduled for modified evaluation with
Hepatology and social worker as video visit
Remainder of evaluation will be onsite when restrictions are lifted
1 Pre-clinicarrival COVID screening for patientscaregiver2 Universal masking
no
Re-entry of Liver Patients in Clinic June 2020
All new liver transplant evaluations and HCC diagnosis New decompensation or worsening symptoms Listed patients for transplant with decompensated cirrhosis Acute hepatitis or liver injury Early post transplant Patients with difficulty with telehealth
Re-entry of Liver Patients HCC Surveillance HCC surveillance should continue as close to schedule (an
arbitrary delay of 2 months were acceptable) Working on list of all delayed imaging and prioritizing them by
risk categoriesKnown HCC surveillance for treatment response elevated AFP
Key is working with Radiology (Options of imaging locally) Communication with patients and documentation is important No delay in HCC treatment (riskbenefits discussion)
httpswwwaasldorgsitesdefaultfiles2020-05AASLD-COVID19-ClinicalInsights-May42020
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
Fibroscan Not urgent but planning to
start June-July 2020 Huge back log Using radiology US protocol
for PPE (maskgoogles and gown) Flexible schedules based on
safety guidelines
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

Webinar PresenterDavid C Mulligan MD FAASLDProfessor of Surgery and Chief
of Transplantation and Immunology
Yale University Yale New Haven Health System
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 4
Webinar PresenterBilal Hameed MD
Associate Professor of Medicine and the Hepatology Clinic Chief
University of California San Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 5
6
Connect with AASLD
aasldorgtwitterAASLDtweets
aasldorginstagram
aasldorgfacebook
aasldorglinkedinaasldorgyoutube
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 7
For resources and updates on COVID-19 and the liver visit aasldorgCOVID19
8
o Special Interest Group participationo Priority housing and registration with discounts to The Liver Meetingreg
and DDWreg
o Free or discounted subscriptions to AASLD journals HEPATOLOGY and Liver Transplantation
o Complimentary access to premier hepatology online education in LiverLearningreg
o Individual and corporate non-physician memberships available
AASLD Member Benefits
aasldorgmembership
9
Join the COVID-19 Discussion Community on Engage
engageaasldorgcovid19
10
New AASLD Journals App
Access all four AASLD Journals in a single app
aasldorgpublications
11
Submit abstracts at aasldorgLMabstracts
a a s l d f n d o r g d o n a t e
CME MOC and E
Available
a a s l d f n d o r g
You can help invest in the future of hepatology by supporting
more research amp advanced career training
Donate today to AASLD Foundation
Follow us on Twitter AASLDFoundation
aasldfoundationorgdonate
13
Register Now for May 28th Webinar
AASLD-ALEH COVID-19 amp the Liver in the Americas
aasldorgcalendar
14
COVID-19 and the Liver Reentry and Return to a Pre-Pandemic State
o Webinar Contributorso Presenter Introductions ndash Dr Kimberly Brown
o Housekeeping Itemso OpenSAFELY Study ndash Dr Kimberly Brown
o Expert Consensus Panel Update ndash Dr Oren Fixo Outpatient ndash Dr Bilal Hameedo Inpatient ndash Dr Patricia Harreno Transplant ndash Dr David Mulligan
o Panel Discussion QampA
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 15
Webinar Agenda
o Co-chair Oren K Fix MD MSc FAASLD Swedish Medical Center (Washington)
o Co-chair Elizabeth C Verna MD MS Columbia University (New York)
o Kimberly Brown MD Henry Ford Health System (Michigan)
o Jaime Chu MD Icahn School of Medicine at Mount Sinai (New York)
o Bilal Hameed MD University of California (California)
o Laura M Kulik MD Northwestern Medical Faculty Foundation (Illinois)
o Ryan M Kwok MD Uniformed Services University (Maryland)
o Brendan M McGuire MD University of Alabama (Alabama)
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 16
o Jennifer Price MD MBA FACP University of California San Francisco (California)
o Daniel S Pratt MD FAASLD Massachusetts General Hospital (Massachusetts)
o Nancy S Reau MD Rush University (Illinois)
o Mark W Russo MD MPH FAASLD Carolinas Medical Center (North Carolina)
o Michael Schilsky MD FAASLD Yale University (Connecticut)
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC (California)
o Andrew Reynolds (Patient Advocate)o Raymond Chung and K Rajender Reddy
(ex-officio)
Clinical Oversight amp Publications Subcommittee
Submit your questions in the QampA box at the top or bottom of your screen
Questions will be answered at the end of the presentation
Webinar QampA
Webinar ModeratorKimberly Ann Brown MD
FAASLDChief Division of
Gastroenterology amp Hepatology
Henry Ford Health System
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 18
Webinar PresenterBilal Hameed MD
Associate Professor of Medicine and the Hepatology Clinic Chief
University of California San Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 19
Webinar PresenterPatricia Harren DNP DCC
Clinical Director of the Center for Liver Disease amp Transplantation Clinical Director for Pediatric Transplantation
amp Adult Abdominal Organ Transplantation
Columbia University
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 20
Webinar PresenterDavid C Mulligan MD FAASLDProfessor of Surgery and Chief
of Transplantation and Immunology
Yale University Yale New Haven Health System
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 21
o Oren K Fix MD MSc FAASLD Swedish Medical Center (Washington)
o Elizabeth C Verna MD MS Columbia University (New York)
o Jaime Chu MD Icahn School of Medicine at Mount Sinai (New York)
o Karen Hoyt BA Patient Advocate
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 22
o Guadalupe Garcia-Tsao MD FAASLD Yale University (Connecticut)
o Ryutaro Hirose MD University of California San Francisco (California)
o K Gautham Reddy MD FAASLD University of Chicago Medical Center (Illinois)
Webinar Panelist
o OpenSAFELY Factors associated with COVID-19-related hospital deaths in the linked electronic health records of 17 million adult NHS patientsbull 17425445 adultsbull Feb 1 2020 to April 25 2020bull Primary outcome death in hospital in patients with confirmed
COVID-19 (5683 deaths)
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
httpsdoiorg1011012020050620092999
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
httpsdoiorg1011012020050620092999
HR adjusted for all other factors listed other than ethnicity
o Largest cohort study to date evaluating a variety of clinical factors for death from COVID-19
o Asians and blacks appear to be at increased risk of in-hospital death with only partial attribution to pre-existing clinical risk factors or deprivation
o Patients with pre-existing liver disease transplantation or on immunosuppression appear to have increased risk of in-hospital death when adjusted for agesex alone or fully adjusted
o Strengthsbull Largest cohort study to date representing 40 English populationbull Inclusion of variables including liver disease transplant for analysis
o Weaknessesbull Deaths related to patients with false-negative tests or died without testing would be missedbull Censoring patients at date of death from other causes or outside the hospital stopped 9
days short of study end bull Cohort limited to those practices using the EHR software SystmOne Some variable were
assumed absent if missing bull Characterization of ldquoliver diseaserdquo is general and not complete
o Further characterization of liver disease and potential risks due to etiology MELD etc will be helpful in future studies
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORGhttpsdoiorg1011012020050620092999
Expert Panel Consensus Statement
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 26
o First published online March 23rdo New update posted today
wwwaasldorgcovid19o Spanish and Portuguese
translations available onlineo Hepatology manuscript published
online
May 14th Update Major Changes
o Acknowledgement of possible link between COVID-19 and Kawasaki-like pediatric multisystem inflammatory syndrome
o Italian autopsy series describing involvement of hepatic vasculature including acute portal and sinusoidal thrombosis
o Introduction of SARS-CoV-2 antigen testing in addition to increasing availability of antibody testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 27
httpswwwhealthnygovpressreleases2020docs2020-05-06_covid19_pediatric_inflammatory_syndromepdfSonzogni et al Preprints 2020httpswwwfdagovnews-eventspress-announcementscoronavirus-covid-19-update-fda-authorizes-first-antigen-test-help-rapid-detection-virus-causes
May 14th Update Major Changes
o OpenSAFELY study from the UK chronic liver disease is a risk factor for in-hospital death from COVID-19
o Large US study also showed that chronic liver disease and cirrhosis are associated with higher COVID-19 mortality
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 28
Williamson et al MedRxiv 2020Singh and Khan Gastroenterol 2020
May 14th Update Major Changes
o Clarification that treatment of hepatitis B is not contraindicated in patients with or without COVID-19
o Recommendations regarding use of masks for patients and caregivers as well as providers in the clinic or hospital setting
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 29
May 14th Update Major Changes
o Evolving data on hydroxychloroquine suggesting it should no longer be used outside RCTs
o New data on triple therapy with lopinavir-ritonavir ribavirin and interferon-beta-1b showing more rapid viral clearance compared to lopinavir-ritonavir (phase 2 RCT)
o Reentry
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 30
Geleris et al N Eng J Med 2020Hung et al Lancet 2020
31
Impact of COVID-19 on Liver Disease Safe Outpatient Re-Entry Process
Bilal Hameed MDAssociate Professor of Medicine
Clinic Chief Hepatology University of California San Francisco
Outline
The COVID-19 effects on liver care Recommendations for re-entry and re-opening facilities Ambulatory re-entry and recovery challenges and plan
at UCSF Gradual re-entry of liver patients in the ambulatory
setting
The Untold Toll mdash The Pandemicrsquos Effects on Patients without COVID-19
httpswwwnejmorgdoifull101056NEJMms2009984query=featured_coronavirus
Patients with heart attacks strokes and even appendicitis vanish from
hospitals
The Pandemicrsquos Effects on Patients without COVID-1938 reduction in STEMI activations in the US
during COVID-19 pandemic
Garcia S et al Journal of the American College of Cardiology April 2020
Decrease in routine pediatric vaccination during COVID-19
httpswwwcdcgovmmwrvolumes69wr
Unexpected Consequences of the Pandemic
To expand capacity for COVID-19 patients on March 18th CMS recommended limiting non-essential care and procedures 8 week pause in usual care activities Fear of returning to care Change in patientrsquos perception of riskbenefit
Areas with lowstable incidence of COVID-19 CMS allowing non-emergent non-COVID-19 healthcare
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdf
COVID-19 Pandemic Impact on the Cirrhosis Care
Tapper EB et al Journal of Hepatology April 2020
COVID Surge
Loss of insurance
Outpatient Impact of COVID-19 Pandemic UCSF Experience Maximizing Appropriate Use of Video Visits during Re-entry
Prior State Current State Future State~20 of total visits were video visits
~95 of total visits are video visits
Appropriate mix of telehealth visits ~50
Continue expanding to -Patients that live far away -Post-ops amp post-discharge follow-up-Chronic disease management(NAFLDHBVHCV etc)-Free up clinic space
0
10000
20000
30000
40000
50000
60000
70000
End of April Double March volume
February 2 of all visits2nd largest video visit program in the
country among AMCs largest in California
End of March 60 of visits
UCSF Video Visits by Month (Jan 2015-April 2020)
0
100
200
300
400
500
600
700
800
900
Jul 2019 Aug Sep Oct Nov Dec Jan 2020 Feb Mar Apr
Able to see the same number of patients even during pandemic
Hepatology Video Visits by Month at UCSF
CMS Phase I Recommendations Re-opening Facilities for Non-emergent Non-COVID-19 Healthcare
In coordination with State and local public health officials evaluate the incidence and trends for COVID-19 in the area
Prioritize surgicalprocedural care and high-complexity chronic disease management and select preventive services
Consider establishing Non-COVID Care (NCC) zones that would screen all patients for symptoms of COVID-19
Sufficient resources should be available across phases of care including PPE healthy workforce testing capacity etc and without jeopardizing surge capacity
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdfhttpswwwwhitehousegovopeningamericacriteriahttpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
httpsdatasfgovorgstoriessdak2-gvuj
San Francisco COVID-19 Numbers
Ambulatory Re-entry and Recovery ndash Cascaded Principles
Ensure morbidity and mortality do not increase due to liver related illness and provide care in a safe manner
Continue to prioritize the health and safety of workforce Prioritize urgent patients Communicate consistently and transparently Invest appropriately in services and improvement efforts
Strategies to limit unnecessary exposure while continuing to provide high-quality care for our liver patients
bull Optimization and flexibility of schedules (hoursweekend)
bull Utilization of clinic spacebull Sustain telehealth bull Digital technology for symptoms
monitoring bull Staff redeployment
bull COVID symptoms check protocolbull Social distancing in clinicbull Masking and safety policiesbull Waiting rooms changesbull Visitor policies
bull Prioritize urgent patientsbull Back log data and referralsbull Pre-clinic communicationbull In clinic flow (Echeck in rooming
and check out policies)
bull Patient communication is the keybull Staff anxiety and stress reduction bull Focus on vulnerable populationbull Physician burn out and health needs bull Trainees re-entry and education
Staff and PatientSafety
Clinic Work Flows
Resource Utilization
Support and
Education
PatientCare
Ambulatory Recovery Challenges and PlanProviding Best Care While Living with COVID-19
Physical Distancing amp Safety Guidelines
Conversa Employee Screening Mychart Screener Apex texting for patients in
nearby waiting areas
Innovation and Improving Operations
Gradual Re-entry of Liver Patients in the Ambulatory Setting
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
Patient will be scheduled for modified evaluation with
Hepatology and social worker as video visit
Remainder of evaluation will be onsite when restrictions are lifted
1 Pre-clinicarrival COVID screening for patientscaregiver2 Universal masking
no
Re-entry of Liver Patients in Clinic June 2020
All new liver transplant evaluations and HCC diagnosis New decompensation or worsening symptoms Listed patients for transplant with decompensated cirrhosis Acute hepatitis or liver injury Early post transplant Patients with difficulty with telehealth
Re-entry of Liver Patients HCC Surveillance HCC surveillance should continue as close to schedule (an
arbitrary delay of 2 months were acceptable) Working on list of all delayed imaging and prioritizing them by
risk categoriesKnown HCC surveillance for treatment response elevated AFP
Key is working with Radiology (Options of imaging locally) Communication with patients and documentation is important No delay in HCC treatment (riskbenefits discussion)
httpswwwaasldorgsitesdefaultfiles2020-05AASLD-COVID19-ClinicalInsights-May42020
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
Fibroscan Not urgent but planning to
start June-July 2020 Huge back log Using radiology US protocol
for PPE (maskgoogles and gown) Flexible schedules based on
safety guidelines
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

Webinar PresenterBilal Hameed MD
Associate Professor of Medicine and the Hepatology Clinic Chief
University of California San Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 5
6
Connect with AASLD
aasldorgtwitterAASLDtweets
aasldorginstagram
aasldorgfacebook
aasldorglinkedinaasldorgyoutube
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 7
For resources and updates on COVID-19 and the liver visit aasldorgCOVID19
8
o Special Interest Group participationo Priority housing and registration with discounts to The Liver Meetingreg
and DDWreg
o Free or discounted subscriptions to AASLD journals HEPATOLOGY and Liver Transplantation
o Complimentary access to premier hepatology online education in LiverLearningreg
o Individual and corporate non-physician memberships available
AASLD Member Benefits
aasldorgmembership
9
Join the COVID-19 Discussion Community on Engage
engageaasldorgcovid19
10
New AASLD Journals App
Access all four AASLD Journals in a single app
aasldorgpublications
11
Submit abstracts at aasldorgLMabstracts
a a s l d f n d o r g d o n a t e
CME MOC and E
Available
a a s l d f n d o r g
You can help invest in the future of hepatology by supporting
more research amp advanced career training
Donate today to AASLD Foundation
Follow us on Twitter AASLDFoundation
aasldfoundationorgdonate
13
Register Now for May 28th Webinar
AASLD-ALEH COVID-19 amp the Liver in the Americas
aasldorgcalendar
14
COVID-19 and the Liver Reentry and Return to a Pre-Pandemic State
o Webinar Contributorso Presenter Introductions ndash Dr Kimberly Brown
o Housekeeping Itemso OpenSAFELY Study ndash Dr Kimberly Brown
o Expert Consensus Panel Update ndash Dr Oren Fixo Outpatient ndash Dr Bilal Hameedo Inpatient ndash Dr Patricia Harreno Transplant ndash Dr David Mulligan
o Panel Discussion QampA
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 15
Webinar Agenda
o Co-chair Oren K Fix MD MSc FAASLD Swedish Medical Center (Washington)
o Co-chair Elizabeth C Verna MD MS Columbia University (New York)
o Kimberly Brown MD Henry Ford Health System (Michigan)
o Jaime Chu MD Icahn School of Medicine at Mount Sinai (New York)
o Bilal Hameed MD University of California (California)
o Laura M Kulik MD Northwestern Medical Faculty Foundation (Illinois)
o Ryan M Kwok MD Uniformed Services University (Maryland)
o Brendan M McGuire MD University of Alabama (Alabama)
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 16
o Jennifer Price MD MBA FACP University of California San Francisco (California)
o Daniel S Pratt MD FAASLD Massachusetts General Hospital (Massachusetts)
o Nancy S Reau MD Rush University (Illinois)
o Mark W Russo MD MPH FAASLD Carolinas Medical Center (North Carolina)
o Michael Schilsky MD FAASLD Yale University (Connecticut)
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC (California)
o Andrew Reynolds (Patient Advocate)o Raymond Chung and K Rajender Reddy
(ex-officio)
Clinical Oversight amp Publications Subcommittee
Submit your questions in the QampA box at the top or bottom of your screen
Questions will be answered at the end of the presentation
Webinar QampA
Webinar ModeratorKimberly Ann Brown MD
FAASLDChief Division of
Gastroenterology amp Hepatology
Henry Ford Health System
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 18
Webinar PresenterBilal Hameed MD
Associate Professor of Medicine and the Hepatology Clinic Chief
University of California San Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 19
Webinar PresenterPatricia Harren DNP DCC
Clinical Director of the Center for Liver Disease amp Transplantation Clinical Director for Pediatric Transplantation
amp Adult Abdominal Organ Transplantation
Columbia University
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 20
Webinar PresenterDavid C Mulligan MD FAASLDProfessor of Surgery and Chief
of Transplantation and Immunology
Yale University Yale New Haven Health System
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 21
o Oren K Fix MD MSc FAASLD Swedish Medical Center (Washington)
o Elizabeth C Verna MD MS Columbia University (New York)
o Jaime Chu MD Icahn School of Medicine at Mount Sinai (New York)
o Karen Hoyt BA Patient Advocate
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 22
o Guadalupe Garcia-Tsao MD FAASLD Yale University (Connecticut)
o Ryutaro Hirose MD University of California San Francisco (California)
o K Gautham Reddy MD FAASLD University of Chicago Medical Center (Illinois)
Webinar Panelist
o OpenSAFELY Factors associated with COVID-19-related hospital deaths in the linked electronic health records of 17 million adult NHS patientsbull 17425445 adultsbull Feb 1 2020 to April 25 2020bull Primary outcome death in hospital in patients with confirmed
COVID-19 (5683 deaths)
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
httpsdoiorg1011012020050620092999
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
httpsdoiorg1011012020050620092999
HR adjusted for all other factors listed other than ethnicity
o Largest cohort study to date evaluating a variety of clinical factors for death from COVID-19
o Asians and blacks appear to be at increased risk of in-hospital death with only partial attribution to pre-existing clinical risk factors or deprivation
o Patients with pre-existing liver disease transplantation or on immunosuppression appear to have increased risk of in-hospital death when adjusted for agesex alone or fully adjusted
o Strengthsbull Largest cohort study to date representing 40 English populationbull Inclusion of variables including liver disease transplant for analysis
o Weaknessesbull Deaths related to patients with false-negative tests or died without testing would be missedbull Censoring patients at date of death from other causes or outside the hospital stopped 9
days short of study end bull Cohort limited to those practices using the EHR software SystmOne Some variable were
assumed absent if missing bull Characterization of ldquoliver diseaserdquo is general and not complete
o Further characterization of liver disease and potential risks due to etiology MELD etc will be helpful in future studies
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORGhttpsdoiorg1011012020050620092999
Expert Panel Consensus Statement
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 26
o First published online March 23rdo New update posted today
wwwaasldorgcovid19o Spanish and Portuguese
translations available onlineo Hepatology manuscript published
online
May 14th Update Major Changes
o Acknowledgement of possible link between COVID-19 and Kawasaki-like pediatric multisystem inflammatory syndrome
o Italian autopsy series describing involvement of hepatic vasculature including acute portal and sinusoidal thrombosis
o Introduction of SARS-CoV-2 antigen testing in addition to increasing availability of antibody testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 27
httpswwwhealthnygovpressreleases2020docs2020-05-06_covid19_pediatric_inflammatory_syndromepdfSonzogni et al Preprints 2020httpswwwfdagovnews-eventspress-announcementscoronavirus-covid-19-update-fda-authorizes-first-antigen-test-help-rapid-detection-virus-causes
May 14th Update Major Changes
o OpenSAFELY study from the UK chronic liver disease is a risk factor for in-hospital death from COVID-19
o Large US study also showed that chronic liver disease and cirrhosis are associated with higher COVID-19 mortality
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 28
Williamson et al MedRxiv 2020Singh and Khan Gastroenterol 2020
May 14th Update Major Changes
o Clarification that treatment of hepatitis B is not contraindicated in patients with or without COVID-19
o Recommendations regarding use of masks for patients and caregivers as well as providers in the clinic or hospital setting
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 29
May 14th Update Major Changes
o Evolving data on hydroxychloroquine suggesting it should no longer be used outside RCTs
o New data on triple therapy with lopinavir-ritonavir ribavirin and interferon-beta-1b showing more rapid viral clearance compared to lopinavir-ritonavir (phase 2 RCT)
o Reentry
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 30
Geleris et al N Eng J Med 2020Hung et al Lancet 2020
31
Impact of COVID-19 on Liver Disease Safe Outpatient Re-Entry Process
Bilal Hameed MDAssociate Professor of Medicine
Clinic Chief Hepatology University of California San Francisco
Outline
The COVID-19 effects on liver care Recommendations for re-entry and re-opening facilities Ambulatory re-entry and recovery challenges and plan
at UCSF Gradual re-entry of liver patients in the ambulatory
setting
The Untold Toll mdash The Pandemicrsquos Effects on Patients without COVID-19
httpswwwnejmorgdoifull101056NEJMms2009984query=featured_coronavirus
Patients with heart attacks strokes and even appendicitis vanish from
hospitals
The Pandemicrsquos Effects on Patients without COVID-1938 reduction in STEMI activations in the US
during COVID-19 pandemic
Garcia S et al Journal of the American College of Cardiology April 2020
Decrease in routine pediatric vaccination during COVID-19
httpswwwcdcgovmmwrvolumes69wr
Unexpected Consequences of the Pandemic
To expand capacity for COVID-19 patients on March 18th CMS recommended limiting non-essential care and procedures 8 week pause in usual care activities Fear of returning to care Change in patientrsquos perception of riskbenefit
Areas with lowstable incidence of COVID-19 CMS allowing non-emergent non-COVID-19 healthcare
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdf
COVID-19 Pandemic Impact on the Cirrhosis Care
Tapper EB et al Journal of Hepatology April 2020
COVID Surge
Loss of insurance
Outpatient Impact of COVID-19 Pandemic UCSF Experience Maximizing Appropriate Use of Video Visits during Re-entry
Prior State Current State Future State~20 of total visits were video visits
~95 of total visits are video visits
Appropriate mix of telehealth visits ~50
Continue expanding to -Patients that live far away -Post-ops amp post-discharge follow-up-Chronic disease management(NAFLDHBVHCV etc)-Free up clinic space
0
10000
20000
30000
40000
50000
60000
70000
End of April Double March volume
February 2 of all visits2nd largest video visit program in the
country among AMCs largest in California
End of March 60 of visits
UCSF Video Visits by Month (Jan 2015-April 2020)
0
100
200
300
400
500
600
700
800
900
Jul 2019 Aug Sep Oct Nov Dec Jan 2020 Feb Mar Apr
Able to see the same number of patients even during pandemic
Hepatology Video Visits by Month at UCSF
CMS Phase I Recommendations Re-opening Facilities for Non-emergent Non-COVID-19 Healthcare
In coordination with State and local public health officials evaluate the incidence and trends for COVID-19 in the area
Prioritize surgicalprocedural care and high-complexity chronic disease management and select preventive services
Consider establishing Non-COVID Care (NCC) zones that would screen all patients for symptoms of COVID-19
Sufficient resources should be available across phases of care including PPE healthy workforce testing capacity etc and without jeopardizing surge capacity
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdfhttpswwwwhitehousegovopeningamericacriteriahttpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
httpsdatasfgovorgstoriessdak2-gvuj
San Francisco COVID-19 Numbers
Ambulatory Re-entry and Recovery ndash Cascaded Principles
Ensure morbidity and mortality do not increase due to liver related illness and provide care in a safe manner
Continue to prioritize the health and safety of workforce Prioritize urgent patients Communicate consistently and transparently Invest appropriately in services and improvement efforts
Strategies to limit unnecessary exposure while continuing to provide high-quality care for our liver patients
bull Optimization and flexibility of schedules (hoursweekend)
bull Utilization of clinic spacebull Sustain telehealth bull Digital technology for symptoms
monitoring bull Staff redeployment
bull COVID symptoms check protocolbull Social distancing in clinicbull Masking and safety policiesbull Waiting rooms changesbull Visitor policies
bull Prioritize urgent patientsbull Back log data and referralsbull Pre-clinic communicationbull In clinic flow (Echeck in rooming
and check out policies)
bull Patient communication is the keybull Staff anxiety and stress reduction bull Focus on vulnerable populationbull Physician burn out and health needs bull Trainees re-entry and education
Staff and PatientSafety
Clinic Work Flows
Resource Utilization
Support and
Education
PatientCare
Ambulatory Recovery Challenges and PlanProviding Best Care While Living with COVID-19
Physical Distancing amp Safety Guidelines
Conversa Employee Screening Mychart Screener Apex texting for patients in
nearby waiting areas
Innovation and Improving Operations
Gradual Re-entry of Liver Patients in the Ambulatory Setting
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
Patient will be scheduled for modified evaluation with
Hepatology and social worker as video visit
Remainder of evaluation will be onsite when restrictions are lifted
1 Pre-clinicarrival COVID screening for patientscaregiver2 Universal masking
no
Re-entry of Liver Patients in Clinic June 2020
All new liver transplant evaluations and HCC diagnosis New decompensation or worsening symptoms Listed patients for transplant with decompensated cirrhosis Acute hepatitis or liver injury Early post transplant Patients with difficulty with telehealth
Re-entry of Liver Patients HCC Surveillance HCC surveillance should continue as close to schedule (an
arbitrary delay of 2 months were acceptable) Working on list of all delayed imaging and prioritizing them by
risk categoriesKnown HCC surveillance for treatment response elevated AFP
Key is working with Radiology (Options of imaging locally) Communication with patients and documentation is important No delay in HCC treatment (riskbenefits discussion)
httpswwwaasldorgsitesdefaultfiles2020-05AASLD-COVID19-ClinicalInsights-May42020
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
Fibroscan Not urgent but planning to
start June-July 2020 Huge back log Using radiology US protocol
for PPE (maskgoogles and gown) Flexible schedules based on
safety guidelines
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

6
Connect with AASLD
aasldorgtwitterAASLDtweets
aasldorginstagram
aasldorgfacebook
aasldorglinkedinaasldorgyoutube
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 7
For resources and updates on COVID-19 and the liver visit aasldorgCOVID19
8
o Special Interest Group participationo Priority housing and registration with discounts to The Liver Meetingreg
and DDWreg
o Free or discounted subscriptions to AASLD journals HEPATOLOGY and Liver Transplantation
o Complimentary access to premier hepatology online education in LiverLearningreg
o Individual and corporate non-physician memberships available
AASLD Member Benefits
aasldorgmembership
9
Join the COVID-19 Discussion Community on Engage
engageaasldorgcovid19
10
New AASLD Journals App
Access all four AASLD Journals in a single app
aasldorgpublications
11
Submit abstracts at aasldorgLMabstracts
a a s l d f n d o r g d o n a t e
CME MOC and E
Available
a a s l d f n d o r g
You can help invest in the future of hepatology by supporting
more research amp advanced career training
Donate today to AASLD Foundation
Follow us on Twitter AASLDFoundation
aasldfoundationorgdonate
13
Register Now for May 28th Webinar
AASLD-ALEH COVID-19 amp the Liver in the Americas
aasldorgcalendar
14
COVID-19 and the Liver Reentry and Return to a Pre-Pandemic State
o Webinar Contributorso Presenter Introductions ndash Dr Kimberly Brown
o Housekeeping Itemso OpenSAFELY Study ndash Dr Kimberly Brown
o Expert Consensus Panel Update ndash Dr Oren Fixo Outpatient ndash Dr Bilal Hameedo Inpatient ndash Dr Patricia Harreno Transplant ndash Dr David Mulligan
o Panel Discussion QampA
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 15
Webinar Agenda
o Co-chair Oren K Fix MD MSc FAASLD Swedish Medical Center (Washington)
o Co-chair Elizabeth C Verna MD MS Columbia University (New York)
o Kimberly Brown MD Henry Ford Health System (Michigan)
o Jaime Chu MD Icahn School of Medicine at Mount Sinai (New York)
o Bilal Hameed MD University of California (California)
o Laura M Kulik MD Northwestern Medical Faculty Foundation (Illinois)
o Ryan M Kwok MD Uniformed Services University (Maryland)
o Brendan M McGuire MD University of Alabama (Alabama)
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 16
o Jennifer Price MD MBA FACP University of California San Francisco (California)
o Daniel S Pratt MD FAASLD Massachusetts General Hospital (Massachusetts)
o Nancy S Reau MD Rush University (Illinois)
o Mark W Russo MD MPH FAASLD Carolinas Medical Center (North Carolina)
o Michael Schilsky MD FAASLD Yale University (Connecticut)
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC (California)
o Andrew Reynolds (Patient Advocate)o Raymond Chung and K Rajender Reddy
(ex-officio)
Clinical Oversight amp Publications Subcommittee
Submit your questions in the QampA box at the top or bottom of your screen
Questions will be answered at the end of the presentation
Webinar QampA
Webinar ModeratorKimberly Ann Brown MD
FAASLDChief Division of
Gastroenterology amp Hepatology
Henry Ford Health System
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 18
Webinar PresenterBilal Hameed MD
Associate Professor of Medicine and the Hepatology Clinic Chief
University of California San Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 19
Webinar PresenterPatricia Harren DNP DCC
Clinical Director of the Center for Liver Disease amp Transplantation Clinical Director for Pediatric Transplantation
amp Adult Abdominal Organ Transplantation
Columbia University
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 20
Webinar PresenterDavid C Mulligan MD FAASLDProfessor of Surgery and Chief
of Transplantation and Immunology
Yale University Yale New Haven Health System
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 21
o Oren K Fix MD MSc FAASLD Swedish Medical Center (Washington)
o Elizabeth C Verna MD MS Columbia University (New York)
o Jaime Chu MD Icahn School of Medicine at Mount Sinai (New York)
o Karen Hoyt BA Patient Advocate
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 22
o Guadalupe Garcia-Tsao MD FAASLD Yale University (Connecticut)
o Ryutaro Hirose MD University of California San Francisco (California)
o K Gautham Reddy MD FAASLD University of Chicago Medical Center (Illinois)
Webinar Panelist
o OpenSAFELY Factors associated with COVID-19-related hospital deaths in the linked electronic health records of 17 million adult NHS patientsbull 17425445 adultsbull Feb 1 2020 to April 25 2020bull Primary outcome death in hospital in patients with confirmed
COVID-19 (5683 deaths)
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
httpsdoiorg1011012020050620092999
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
httpsdoiorg1011012020050620092999
HR adjusted for all other factors listed other than ethnicity
o Largest cohort study to date evaluating a variety of clinical factors for death from COVID-19
o Asians and blacks appear to be at increased risk of in-hospital death with only partial attribution to pre-existing clinical risk factors or deprivation
o Patients with pre-existing liver disease transplantation or on immunosuppression appear to have increased risk of in-hospital death when adjusted for agesex alone or fully adjusted
o Strengthsbull Largest cohort study to date representing 40 English populationbull Inclusion of variables including liver disease transplant for analysis
o Weaknessesbull Deaths related to patients with false-negative tests or died without testing would be missedbull Censoring patients at date of death from other causes or outside the hospital stopped 9
days short of study end bull Cohort limited to those practices using the EHR software SystmOne Some variable were
assumed absent if missing bull Characterization of ldquoliver diseaserdquo is general and not complete
o Further characterization of liver disease and potential risks due to etiology MELD etc will be helpful in future studies
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORGhttpsdoiorg1011012020050620092999
Expert Panel Consensus Statement
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 26
o First published online March 23rdo New update posted today
wwwaasldorgcovid19o Spanish and Portuguese
translations available onlineo Hepatology manuscript published
online
May 14th Update Major Changes
o Acknowledgement of possible link between COVID-19 and Kawasaki-like pediatric multisystem inflammatory syndrome
o Italian autopsy series describing involvement of hepatic vasculature including acute portal and sinusoidal thrombosis
o Introduction of SARS-CoV-2 antigen testing in addition to increasing availability of antibody testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 27
httpswwwhealthnygovpressreleases2020docs2020-05-06_covid19_pediatric_inflammatory_syndromepdfSonzogni et al Preprints 2020httpswwwfdagovnews-eventspress-announcementscoronavirus-covid-19-update-fda-authorizes-first-antigen-test-help-rapid-detection-virus-causes
May 14th Update Major Changes
o OpenSAFELY study from the UK chronic liver disease is a risk factor for in-hospital death from COVID-19
o Large US study also showed that chronic liver disease and cirrhosis are associated with higher COVID-19 mortality
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 28
Williamson et al MedRxiv 2020Singh and Khan Gastroenterol 2020
May 14th Update Major Changes
o Clarification that treatment of hepatitis B is not contraindicated in patients with or without COVID-19
o Recommendations regarding use of masks for patients and caregivers as well as providers in the clinic or hospital setting
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 29
May 14th Update Major Changes
o Evolving data on hydroxychloroquine suggesting it should no longer be used outside RCTs
o New data on triple therapy with lopinavir-ritonavir ribavirin and interferon-beta-1b showing more rapid viral clearance compared to lopinavir-ritonavir (phase 2 RCT)
o Reentry
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 30
Geleris et al N Eng J Med 2020Hung et al Lancet 2020
31
Impact of COVID-19 on Liver Disease Safe Outpatient Re-Entry Process
Bilal Hameed MDAssociate Professor of Medicine
Clinic Chief Hepatology University of California San Francisco
Outline
The COVID-19 effects on liver care Recommendations for re-entry and re-opening facilities Ambulatory re-entry and recovery challenges and plan
at UCSF Gradual re-entry of liver patients in the ambulatory
setting
The Untold Toll mdash The Pandemicrsquos Effects on Patients without COVID-19
httpswwwnejmorgdoifull101056NEJMms2009984query=featured_coronavirus
Patients with heart attacks strokes and even appendicitis vanish from
hospitals
The Pandemicrsquos Effects on Patients without COVID-1938 reduction in STEMI activations in the US
during COVID-19 pandemic
Garcia S et al Journal of the American College of Cardiology April 2020
Decrease in routine pediatric vaccination during COVID-19
httpswwwcdcgovmmwrvolumes69wr
Unexpected Consequences of the Pandemic
To expand capacity for COVID-19 patients on March 18th CMS recommended limiting non-essential care and procedures 8 week pause in usual care activities Fear of returning to care Change in patientrsquos perception of riskbenefit
Areas with lowstable incidence of COVID-19 CMS allowing non-emergent non-COVID-19 healthcare
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdf
COVID-19 Pandemic Impact on the Cirrhosis Care
Tapper EB et al Journal of Hepatology April 2020
COVID Surge
Loss of insurance
Outpatient Impact of COVID-19 Pandemic UCSF Experience Maximizing Appropriate Use of Video Visits during Re-entry
Prior State Current State Future State~20 of total visits were video visits
~95 of total visits are video visits
Appropriate mix of telehealth visits ~50
Continue expanding to -Patients that live far away -Post-ops amp post-discharge follow-up-Chronic disease management(NAFLDHBVHCV etc)-Free up clinic space
0
10000
20000
30000
40000
50000
60000
70000
End of April Double March volume
February 2 of all visits2nd largest video visit program in the
country among AMCs largest in California
End of March 60 of visits
UCSF Video Visits by Month (Jan 2015-April 2020)
0
100
200
300
400
500
600
700
800
900
Jul 2019 Aug Sep Oct Nov Dec Jan 2020 Feb Mar Apr
Able to see the same number of patients even during pandemic
Hepatology Video Visits by Month at UCSF
CMS Phase I Recommendations Re-opening Facilities for Non-emergent Non-COVID-19 Healthcare
In coordination with State and local public health officials evaluate the incidence and trends for COVID-19 in the area
Prioritize surgicalprocedural care and high-complexity chronic disease management and select preventive services
Consider establishing Non-COVID Care (NCC) zones that would screen all patients for symptoms of COVID-19
Sufficient resources should be available across phases of care including PPE healthy workforce testing capacity etc and without jeopardizing surge capacity
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdfhttpswwwwhitehousegovopeningamericacriteriahttpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
httpsdatasfgovorgstoriessdak2-gvuj
San Francisco COVID-19 Numbers
Ambulatory Re-entry and Recovery ndash Cascaded Principles
Ensure morbidity and mortality do not increase due to liver related illness and provide care in a safe manner
Continue to prioritize the health and safety of workforce Prioritize urgent patients Communicate consistently and transparently Invest appropriately in services and improvement efforts
Strategies to limit unnecessary exposure while continuing to provide high-quality care for our liver patients
bull Optimization and flexibility of schedules (hoursweekend)
bull Utilization of clinic spacebull Sustain telehealth bull Digital technology for symptoms
monitoring bull Staff redeployment
bull COVID symptoms check protocolbull Social distancing in clinicbull Masking and safety policiesbull Waiting rooms changesbull Visitor policies
bull Prioritize urgent patientsbull Back log data and referralsbull Pre-clinic communicationbull In clinic flow (Echeck in rooming
and check out policies)
bull Patient communication is the keybull Staff anxiety and stress reduction bull Focus on vulnerable populationbull Physician burn out and health needs bull Trainees re-entry and education
Staff and PatientSafety
Clinic Work Flows
Resource Utilization
Support and
Education
PatientCare
Ambulatory Recovery Challenges and PlanProviding Best Care While Living with COVID-19
Physical Distancing amp Safety Guidelines
Conversa Employee Screening Mychart Screener Apex texting for patients in
nearby waiting areas
Innovation and Improving Operations
Gradual Re-entry of Liver Patients in the Ambulatory Setting
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
Patient will be scheduled for modified evaluation with
Hepatology and social worker as video visit
Remainder of evaluation will be onsite when restrictions are lifted
1 Pre-clinicarrival COVID screening for patientscaregiver2 Universal masking
no
Re-entry of Liver Patients in Clinic June 2020
All new liver transplant evaluations and HCC diagnosis New decompensation or worsening symptoms Listed patients for transplant with decompensated cirrhosis Acute hepatitis or liver injury Early post transplant Patients with difficulty with telehealth
Re-entry of Liver Patients HCC Surveillance HCC surveillance should continue as close to schedule (an
arbitrary delay of 2 months were acceptable) Working on list of all delayed imaging and prioritizing them by
risk categoriesKnown HCC surveillance for treatment response elevated AFP
Key is working with Radiology (Options of imaging locally) Communication with patients and documentation is important No delay in HCC treatment (riskbenefits discussion)
httpswwwaasldorgsitesdefaultfiles2020-05AASLD-COVID19-ClinicalInsights-May42020
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
Fibroscan Not urgent but planning to
start June-July 2020 Huge back log Using radiology US protocol
for PPE (maskgoogles and gown) Flexible schedules based on
safety guidelines
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 7
For resources and updates on COVID-19 and the liver visit aasldorgCOVID19
8
o Special Interest Group participationo Priority housing and registration with discounts to The Liver Meetingreg
and DDWreg
o Free or discounted subscriptions to AASLD journals HEPATOLOGY and Liver Transplantation
o Complimentary access to premier hepatology online education in LiverLearningreg
o Individual and corporate non-physician memberships available
AASLD Member Benefits
aasldorgmembership
9
Join the COVID-19 Discussion Community on Engage
engageaasldorgcovid19
10
New AASLD Journals App
Access all four AASLD Journals in a single app
aasldorgpublications
11
Submit abstracts at aasldorgLMabstracts
a a s l d f n d o r g d o n a t e
CME MOC and E
Available
a a s l d f n d o r g
You can help invest in the future of hepatology by supporting
more research amp advanced career training
Donate today to AASLD Foundation
Follow us on Twitter AASLDFoundation
aasldfoundationorgdonate
13
Register Now for May 28th Webinar
AASLD-ALEH COVID-19 amp the Liver in the Americas
aasldorgcalendar
14
COVID-19 and the Liver Reentry and Return to a Pre-Pandemic State
o Webinar Contributorso Presenter Introductions ndash Dr Kimberly Brown
o Housekeeping Itemso OpenSAFELY Study ndash Dr Kimberly Brown
o Expert Consensus Panel Update ndash Dr Oren Fixo Outpatient ndash Dr Bilal Hameedo Inpatient ndash Dr Patricia Harreno Transplant ndash Dr David Mulligan
o Panel Discussion QampA
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 15
Webinar Agenda
o Co-chair Oren K Fix MD MSc FAASLD Swedish Medical Center (Washington)
o Co-chair Elizabeth C Verna MD MS Columbia University (New York)
o Kimberly Brown MD Henry Ford Health System (Michigan)
o Jaime Chu MD Icahn School of Medicine at Mount Sinai (New York)
o Bilal Hameed MD University of California (California)
o Laura M Kulik MD Northwestern Medical Faculty Foundation (Illinois)
o Ryan M Kwok MD Uniformed Services University (Maryland)
o Brendan M McGuire MD University of Alabama (Alabama)
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 16
o Jennifer Price MD MBA FACP University of California San Francisco (California)
o Daniel S Pratt MD FAASLD Massachusetts General Hospital (Massachusetts)
o Nancy S Reau MD Rush University (Illinois)
o Mark W Russo MD MPH FAASLD Carolinas Medical Center (North Carolina)
o Michael Schilsky MD FAASLD Yale University (Connecticut)
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC (California)
o Andrew Reynolds (Patient Advocate)o Raymond Chung and K Rajender Reddy
(ex-officio)
Clinical Oversight amp Publications Subcommittee
Submit your questions in the QampA box at the top or bottom of your screen
Questions will be answered at the end of the presentation
Webinar QampA
Webinar ModeratorKimberly Ann Brown MD
FAASLDChief Division of
Gastroenterology amp Hepatology
Henry Ford Health System
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 18
Webinar PresenterBilal Hameed MD
Associate Professor of Medicine and the Hepatology Clinic Chief
University of California San Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 19
Webinar PresenterPatricia Harren DNP DCC
Clinical Director of the Center for Liver Disease amp Transplantation Clinical Director for Pediatric Transplantation
amp Adult Abdominal Organ Transplantation
Columbia University
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 20
Webinar PresenterDavid C Mulligan MD FAASLDProfessor of Surgery and Chief
of Transplantation and Immunology
Yale University Yale New Haven Health System
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 21
o Oren K Fix MD MSc FAASLD Swedish Medical Center (Washington)
o Elizabeth C Verna MD MS Columbia University (New York)
o Jaime Chu MD Icahn School of Medicine at Mount Sinai (New York)
o Karen Hoyt BA Patient Advocate
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 22
o Guadalupe Garcia-Tsao MD FAASLD Yale University (Connecticut)
o Ryutaro Hirose MD University of California San Francisco (California)
o K Gautham Reddy MD FAASLD University of Chicago Medical Center (Illinois)
Webinar Panelist
o OpenSAFELY Factors associated with COVID-19-related hospital deaths in the linked electronic health records of 17 million adult NHS patientsbull 17425445 adultsbull Feb 1 2020 to April 25 2020bull Primary outcome death in hospital in patients with confirmed
COVID-19 (5683 deaths)
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
httpsdoiorg1011012020050620092999
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
httpsdoiorg1011012020050620092999
HR adjusted for all other factors listed other than ethnicity
o Largest cohort study to date evaluating a variety of clinical factors for death from COVID-19
o Asians and blacks appear to be at increased risk of in-hospital death with only partial attribution to pre-existing clinical risk factors or deprivation
o Patients with pre-existing liver disease transplantation or on immunosuppression appear to have increased risk of in-hospital death when adjusted for agesex alone or fully adjusted
o Strengthsbull Largest cohort study to date representing 40 English populationbull Inclusion of variables including liver disease transplant for analysis
o Weaknessesbull Deaths related to patients with false-negative tests or died without testing would be missedbull Censoring patients at date of death from other causes or outside the hospital stopped 9
days short of study end bull Cohort limited to those practices using the EHR software SystmOne Some variable were
assumed absent if missing bull Characterization of ldquoliver diseaserdquo is general and not complete
o Further characterization of liver disease and potential risks due to etiology MELD etc will be helpful in future studies
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORGhttpsdoiorg1011012020050620092999
Expert Panel Consensus Statement
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 26
o First published online March 23rdo New update posted today
wwwaasldorgcovid19o Spanish and Portuguese
translations available onlineo Hepatology manuscript published
online
May 14th Update Major Changes
o Acknowledgement of possible link between COVID-19 and Kawasaki-like pediatric multisystem inflammatory syndrome
o Italian autopsy series describing involvement of hepatic vasculature including acute portal and sinusoidal thrombosis
o Introduction of SARS-CoV-2 antigen testing in addition to increasing availability of antibody testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 27
httpswwwhealthnygovpressreleases2020docs2020-05-06_covid19_pediatric_inflammatory_syndromepdfSonzogni et al Preprints 2020httpswwwfdagovnews-eventspress-announcementscoronavirus-covid-19-update-fda-authorizes-first-antigen-test-help-rapid-detection-virus-causes
May 14th Update Major Changes
o OpenSAFELY study from the UK chronic liver disease is a risk factor for in-hospital death from COVID-19
o Large US study also showed that chronic liver disease and cirrhosis are associated with higher COVID-19 mortality
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 28
Williamson et al MedRxiv 2020Singh and Khan Gastroenterol 2020
May 14th Update Major Changes
o Clarification that treatment of hepatitis B is not contraindicated in patients with or without COVID-19
o Recommendations regarding use of masks for patients and caregivers as well as providers in the clinic or hospital setting
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 29
May 14th Update Major Changes
o Evolving data on hydroxychloroquine suggesting it should no longer be used outside RCTs
o New data on triple therapy with lopinavir-ritonavir ribavirin and interferon-beta-1b showing more rapid viral clearance compared to lopinavir-ritonavir (phase 2 RCT)
o Reentry
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 30
Geleris et al N Eng J Med 2020Hung et al Lancet 2020
31
Impact of COVID-19 on Liver Disease Safe Outpatient Re-Entry Process
Bilal Hameed MDAssociate Professor of Medicine
Clinic Chief Hepatology University of California San Francisco
Outline
The COVID-19 effects on liver care Recommendations for re-entry and re-opening facilities Ambulatory re-entry and recovery challenges and plan
at UCSF Gradual re-entry of liver patients in the ambulatory
setting
The Untold Toll mdash The Pandemicrsquos Effects on Patients without COVID-19
httpswwwnejmorgdoifull101056NEJMms2009984query=featured_coronavirus
Patients with heart attacks strokes and even appendicitis vanish from
hospitals
The Pandemicrsquos Effects on Patients without COVID-1938 reduction in STEMI activations in the US
during COVID-19 pandemic
Garcia S et al Journal of the American College of Cardiology April 2020
Decrease in routine pediatric vaccination during COVID-19
httpswwwcdcgovmmwrvolumes69wr
Unexpected Consequences of the Pandemic
To expand capacity for COVID-19 patients on March 18th CMS recommended limiting non-essential care and procedures 8 week pause in usual care activities Fear of returning to care Change in patientrsquos perception of riskbenefit
Areas with lowstable incidence of COVID-19 CMS allowing non-emergent non-COVID-19 healthcare
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdf
COVID-19 Pandemic Impact on the Cirrhosis Care
Tapper EB et al Journal of Hepatology April 2020
COVID Surge
Loss of insurance
Outpatient Impact of COVID-19 Pandemic UCSF Experience Maximizing Appropriate Use of Video Visits during Re-entry
Prior State Current State Future State~20 of total visits were video visits
~95 of total visits are video visits
Appropriate mix of telehealth visits ~50
Continue expanding to -Patients that live far away -Post-ops amp post-discharge follow-up-Chronic disease management(NAFLDHBVHCV etc)-Free up clinic space
0
10000
20000
30000
40000
50000
60000
70000
End of April Double March volume
February 2 of all visits2nd largest video visit program in the
country among AMCs largest in California
End of March 60 of visits
UCSF Video Visits by Month (Jan 2015-April 2020)
0
100
200
300
400
500
600
700
800
900
Jul 2019 Aug Sep Oct Nov Dec Jan 2020 Feb Mar Apr
Able to see the same number of patients even during pandemic
Hepatology Video Visits by Month at UCSF
CMS Phase I Recommendations Re-opening Facilities for Non-emergent Non-COVID-19 Healthcare
In coordination with State and local public health officials evaluate the incidence and trends for COVID-19 in the area
Prioritize surgicalprocedural care and high-complexity chronic disease management and select preventive services
Consider establishing Non-COVID Care (NCC) zones that would screen all patients for symptoms of COVID-19
Sufficient resources should be available across phases of care including PPE healthy workforce testing capacity etc and without jeopardizing surge capacity
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdfhttpswwwwhitehousegovopeningamericacriteriahttpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
httpsdatasfgovorgstoriessdak2-gvuj
San Francisco COVID-19 Numbers
Ambulatory Re-entry and Recovery ndash Cascaded Principles
Ensure morbidity and mortality do not increase due to liver related illness and provide care in a safe manner
Continue to prioritize the health and safety of workforce Prioritize urgent patients Communicate consistently and transparently Invest appropriately in services and improvement efforts
Strategies to limit unnecessary exposure while continuing to provide high-quality care for our liver patients
bull Optimization and flexibility of schedules (hoursweekend)
bull Utilization of clinic spacebull Sustain telehealth bull Digital technology for symptoms
monitoring bull Staff redeployment
bull COVID symptoms check protocolbull Social distancing in clinicbull Masking and safety policiesbull Waiting rooms changesbull Visitor policies
bull Prioritize urgent patientsbull Back log data and referralsbull Pre-clinic communicationbull In clinic flow (Echeck in rooming
and check out policies)
bull Patient communication is the keybull Staff anxiety and stress reduction bull Focus on vulnerable populationbull Physician burn out and health needs bull Trainees re-entry and education
Staff and PatientSafety
Clinic Work Flows
Resource Utilization
Support and
Education
PatientCare
Ambulatory Recovery Challenges and PlanProviding Best Care While Living with COVID-19
Physical Distancing amp Safety Guidelines
Conversa Employee Screening Mychart Screener Apex texting for patients in
nearby waiting areas
Innovation and Improving Operations
Gradual Re-entry of Liver Patients in the Ambulatory Setting
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
Patient will be scheduled for modified evaluation with
Hepatology and social worker as video visit
Remainder of evaluation will be onsite when restrictions are lifted
1 Pre-clinicarrival COVID screening for patientscaregiver2 Universal masking
no
Re-entry of Liver Patients in Clinic June 2020
All new liver transplant evaluations and HCC diagnosis New decompensation or worsening symptoms Listed patients for transplant with decompensated cirrhosis Acute hepatitis or liver injury Early post transplant Patients with difficulty with telehealth
Re-entry of Liver Patients HCC Surveillance HCC surveillance should continue as close to schedule (an
arbitrary delay of 2 months were acceptable) Working on list of all delayed imaging and prioritizing them by
risk categoriesKnown HCC surveillance for treatment response elevated AFP
Key is working with Radiology (Options of imaging locally) Communication with patients and documentation is important No delay in HCC treatment (riskbenefits discussion)
httpswwwaasldorgsitesdefaultfiles2020-05AASLD-COVID19-ClinicalInsights-May42020
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
Fibroscan Not urgent but planning to
start June-July 2020 Huge back log Using radiology US protocol
for PPE (maskgoogles and gown) Flexible schedules based on
safety guidelines
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

8
o Special Interest Group participationo Priority housing and registration with discounts to The Liver Meetingreg
and DDWreg
o Free or discounted subscriptions to AASLD journals HEPATOLOGY and Liver Transplantation
o Complimentary access to premier hepatology online education in LiverLearningreg
o Individual and corporate non-physician memberships available
AASLD Member Benefits
aasldorgmembership
9
Join the COVID-19 Discussion Community on Engage
engageaasldorgcovid19
10
New AASLD Journals App
Access all four AASLD Journals in a single app
aasldorgpublications
11
Submit abstracts at aasldorgLMabstracts
a a s l d f n d o r g d o n a t e
CME MOC and E
Available
a a s l d f n d o r g
You can help invest in the future of hepatology by supporting
more research amp advanced career training
Donate today to AASLD Foundation
Follow us on Twitter AASLDFoundation
aasldfoundationorgdonate
13
Register Now for May 28th Webinar
AASLD-ALEH COVID-19 amp the Liver in the Americas
aasldorgcalendar
14
COVID-19 and the Liver Reentry and Return to a Pre-Pandemic State
o Webinar Contributorso Presenter Introductions ndash Dr Kimberly Brown
o Housekeeping Itemso OpenSAFELY Study ndash Dr Kimberly Brown
o Expert Consensus Panel Update ndash Dr Oren Fixo Outpatient ndash Dr Bilal Hameedo Inpatient ndash Dr Patricia Harreno Transplant ndash Dr David Mulligan
o Panel Discussion QampA
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 15
Webinar Agenda
o Co-chair Oren K Fix MD MSc FAASLD Swedish Medical Center (Washington)
o Co-chair Elizabeth C Verna MD MS Columbia University (New York)
o Kimberly Brown MD Henry Ford Health System (Michigan)
o Jaime Chu MD Icahn School of Medicine at Mount Sinai (New York)
o Bilal Hameed MD University of California (California)
o Laura M Kulik MD Northwestern Medical Faculty Foundation (Illinois)
o Ryan M Kwok MD Uniformed Services University (Maryland)
o Brendan M McGuire MD University of Alabama (Alabama)
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 16
o Jennifer Price MD MBA FACP University of California San Francisco (California)
o Daniel S Pratt MD FAASLD Massachusetts General Hospital (Massachusetts)
o Nancy S Reau MD Rush University (Illinois)
o Mark W Russo MD MPH FAASLD Carolinas Medical Center (North Carolina)
o Michael Schilsky MD FAASLD Yale University (Connecticut)
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC (California)
o Andrew Reynolds (Patient Advocate)o Raymond Chung and K Rajender Reddy
(ex-officio)
Clinical Oversight amp Publications Subcommittee
Submit your questions in the QampA box at the top or bottom of your screen
Questions will be answered at the end of the presentation
Webinar QampA
Webinar ModeratorKimberly Ann Brown MD
FAASLDChief Division of
Gastroenterology amp Hepatology
Henry Ford Health System
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 18
Webinar PresenterBilal Hameed MD
Associate Professor of Medicine and the Hepatology Clinic Chief
University of California San Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 19
Webinar PresenterPatricia Harren DNP DCC
Clinical Director of the Center for Liver Disease amp Transplantation Clinical Director for Pediatric Transplantation
amp Adult Abdominal Organ Transplantation
Columbia University
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 20
Webinar PresenterDavid C Mulligan MD FAASLDProfessor of Surgery and Chief
of Transplantation and Immunology
Yale University Yale New Haven Health System
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 21
o Oren K Fix MD MSc FAASLD Swedish Medical Center (Washington)
o Elizabeth C Verna MD MS Columbia University (New York)
o Jaime Chu MD Icahn School of Medicine at Mount Sinai (New York)
o Karen Hoyt BA Patient Advocate
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 22
o Guadalupe Garcia-Tsao MD FAASLD Yale University (Connecticut)
o Ryutaro Hirose MD University of California San Francisco (California)
o K Gautham Reddy MD FAASLD University of Chicago Medical Center (Illinois)
Webinar Panelist
o OpenSAFELY Factors associated with COVID-19-related hospital deaths in the linked electronic health records of 17 million adult NHS patientsbull 17425445 adultsbull Feb 1 2020 to April 25 2020bull Primary outcome death in hospital in patients with confirmed
COVID-19 (5683 deaths)
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
httpsdoiorg1011012020050620092999
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
httpsdoiorg1011012020050620092999
HR adjusted for all other factors listed other than ethnicity
o Largest cohort study to date evaluating a variety of clinical factors for death from COVID-19
o Asians and blacks appear to be at increased risk of in-hospital death with only partial attribution to pre-existing clinical risk factors or deprivation
o Patients with pre-existing liver disease transplantation or on immunosuppression appear to have increased risk of in-hospital death when adjusted for agesex alone or fully adjusted
o Strengthsbull Largest cohort study to date representing 40 English populationbull Inclusion of variables including liver disease transplant for analysis
o Weaknessesbull Deaths related to patients with false-negative tests or died without testing would be missedbull Censoring patients at date of death from other causes or outside the hospital stopped 9
days short of study end bull Cohort limited to those practices using the EHR software SystmOne Some variable were
assumed absent if missing bull Characterization of ldquoliver diseaserdquo is general and not complete
o Further characterization of liver disease and potential risks due to etiology MELD etc will be helpful in future studies
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORGhttpsdoiorg1011012020050620092999
Expert Panel Consensus Statement
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 26
o First published online March 23rdo New update posted today
wwwaasldorgcovid19o Spanish and Portuguese
translations available onlineo Hepatology manuscript published
online
May 14th Update Major Changes
o Acknowledgement of possible link between COVID-19 and Kawasaki-like pediatric multisystem inflammatory syndrome
o Italian autopsy series describing involvement of hepatic vasculature including acute portal and sinusoidal thrombosis
o Introduction of SARS-CoV-2 antigen testing in addition to increasing availability of antibody testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 27
httpswwwhealthnygovpressreleases2020docs2020-05-06_covid19_pediatric_inflammatory_syndromepdfSonzogni et al Preprints 2020httpswwwfdagovnews-eventspress-announcementscoronavirus-covid-19-update-fda-authorizes-first-antigen-test-help-rapid-detection-virus-causes
May 14th Update Major Changes
o OpenSAFELY study from the UK chronic liver disease is a risk factor for in-hospital death from COVID-19
o Large US study also showed that chronic liver disease and cirrhosis are associated with higher COVID-19 mortality
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 28
Williamson et al MedRxiv 2020Singh and Khan Gastroenterol 2020
May 14th Update Major Changes
o Clarification that treatment of hepatitis B is not contraindicated in patients with or without COVID-19
o Recommendations regarding use of masks for patients and caregivers as well as providers in the clinic or hospital setting
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 29
May 14th Update Major Changes
o Evolving data on hydroxychloroquine suggesting it should no longer be used outside RCTs
o New data on triple therapy with lopinavir-ritonavir ribavirin and interferon-beta-1b showing more rapid viral clearance compared to lopinavir-ritonavir (phase 2 RCT)
o Reentry
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 30
Geleris et al N Eng J Med 2020Hung et al Lancet 2020
31
Impact of COVID-19 on Liver Disease Safe Outpatient Re-Entry Process
Bilal Hameed MDAssociate Professor of Medicine
Clinic Chief Hepatology University of California San Francisco
Outline
The COVID-19 effects on liver care Recommendations for re-entry and re-opening facilities Ambulatory re-entry and recovery challenges and plan
at UCSF Gradual re-entry of liver patients in the ambulatory
setting
The Untold Toll mdash The Pandemicrsquos Effects on Patients without COVID-19
httpswwwnejmorgdoifull101056NEJMms2009984query=featured_coronavirus
Patients with heart attacks strokes and even appendicitis vanish from
hospitals
The Pandemicrsquos Effects on Patients without COVID-1938 reduction in STEMI activations in the US
during COVID-19 pandemic
Garcia S et al Journal of the American College of Cardiology April 2020
Decrease in routine pediatric vaccination during COVID-19
httpswwwcdcgovmmwrvolumes69wr
Unexpected Consequences of the Pandemic
To expand capacity for COVID-19 patients on March 18th CMS recommended limiting non-essential care and procedures 8 week pause in usual care activities Fear of returning to care Change in patientrsquos perception of riskbenefit
Areas with lowstable incidence of COVID-19 CMS allowing non-emergent non-COVID-19 healthcare
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdf
COVID-19 Pandemic Impact on the Cirrhosis Care
Tapper EB et al Journal of Hepatology April 2020
COVID Surge
Loss of insurance
Outpatient Impact of COVID-19 Pandemic UCSF Experience Maximizing Appropriate Use of Video Visits during Re-entry
Prior State Current State Future State~20 of total visits were video visits
~95 of total visits are video visits
Appropriate mix of telehealth visits ~50
Continue expanding to -Patients that live far away -Post-ops amp post-discharge follow-up-Chronic disease management(NAFLDHBVHCV etc)-Free up clinic space
0
10000
20000
30000
40000
50000
60000
70000
End of April Double March volume
February 2 of all visits2nd largest video visit program in the
country among AMCs largest in California
End of March 60 of visits
UCSF Video Visits by Month (Jan 2015-April 2020)
0
100
200
300
400
500
600
700
800
900
Jul 2019 Aug Sep Oct Nov Dec Jan 2020 Feb Mar Apr
Able to see the same number of patients even during pandemic
Hepatology Video Visits by Month at UCSF
CMS Phase I Recommendations Re-opening Facilities for Non-emergent Non-COVID-19 Healthcare
In coordination with State and local public health officials evaluate the incidence and trends for COVID-19 in the area
Prioritize surgicalprocedural care and high-complexity chronic disease management and select preventive services
Consider establishing Non-COVID Care (NCC) zones that would screen all patients for symptoms of COVID-19
Sufficient resources should be available across phases of care including PPE healthy workforce testing capacity etc and without jeopardizing surge capacity
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdfhttpswwwwhitehousegovopeningamericacriteriahttpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
httpsdatasfgovorgstoriessdak2-gvuj
San Francisco COVID-19 Numbers
Ambulatory Re-entry and Recovery ndash Cascaded Principles
Ensure morbidity and mortality do not increase due to liver related illness and provide care in a safe manner
Continue to prioritize the health and safety of workforce Prioritize urgent patients Communicate consistently and transparently Invest appropriately in services and improvement efforts
Strategies to limit unnecessary exposure while continuing to provide high-quality care for our liver patients
bull Optimization and flexibility of schedules (hoursweekend)
bull Utilization of clinic spacebull Sustain telehealth bull Digital technology for symptoms
monitoring bull Staff redeployment
bull COVID symptoms check protocolbull Social distancing in clinicbull Masking and safety policiesbull Waiting rooms changesbull Visitor policies
bull Prioritize urgent patientsbull Back log data and referralsbull Pre-clinic communicationbull In clinic flow (Echeck in rooming
and check out policies)
bull Patient communication is the keybull Staff anxiety and stress reduction bull Focus on vulnerable populationbull Physician burn out and health needs bull Trainees re-entry and education
Staff and PatientSafety
Clinic Work Flows
Resource Utilization
Support and
Education
PatientCare
Ambulatory Recovery Challenges and PlanProviding Best Care While Living with COVID-19
Physical Distancing amp Safety Guidelines
Conversa Employee Screening Mychart Screener Apex texting for patients in
nearby waiting areas
Innovation and Improving Operations
Gradual Re-entry of Liver Patients in the Ambulatory Setting
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
Patient will be scheduled for modified evaluation with
Hepatology and social worker as video visit
Remainder of evaluation will be onsite when restrictions are lifted
1 Pre-clinicarrival COVID screening for patientscaregiver2 Universal masking
no
Re-entry of Liver Patients in Clinic June 2020
All new liver transplant evaluations and HCC diagnosis New decompensation or worsening symptoms Listed patients for transplant with decompensated cirrhosis Acute hepatitis or liver injury Early post transplant Patients with difficulty with telehealth
Re-entry of Liver Patients HCC Surveillance HCC surveillance should continue as close to schedule (an
arbitrary delay of 2 months were acceptable) Working on list of all delayed imaging and prioritizing them by
risk categoriesKnown HCC surveillance for treatment response elevated AFP
Key is working with Radiology (Options of imaging locally) Communication with patients and documentation is important No delay in HCC treatment (riskbenefits discussion)
httpswwwaasldorgsitesdefaultfiles2020-05AASLD-COVID19-ClinicalInsights-May42020
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
Fibroscan Not urgent but planning to
start June-July 2020 Huge back log Using radiology US protocol
for PPE (maskgoogles and gown) Flexible schedules based on
safety guidelines
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

9
Join the COVID-19 Discussion Community on Engage
engageaasldorgcovid19
10
New AASLD Journals App
Access all four AASLD Journals in a single app
aasldorgpublications
11
Submit abstracts at aasldorgLMabstracts
a a s l d f n d o r g d o n a t e
CME MOC and E
Available
a a s l d f n d o r g
You can help invest in the future of hepatology by supporting
more research amp advanced career training
Donate today to AASLD Foundation
Follow us on Twitter AASLDFoundation
aasldfoundationorgdonate
13
Register Now for May 28th Webinar
AASLD-ALEH COVID-19 amp the Liver in the Americas
aasldorgcalendar
14
COVID-19 and the Liver Reentry and Return to a Pre-Pandemic State
o Webinar Contributorso Presenter Introductions ndash Dr Kimberly Brown
o Housekeeping Itemso OpenSAFELY Study ndash Dr Kimberly Brown
o Expert Consensus Panel Update ndash Dr Oren Fixo Outpatient ndash Dr Bilal Hameedo Inpatient ndash Dr Patricia Harreno Transplant ndash Dr David Mulligan
o Panel Discussion QampA
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 15
Webinar Agenda
o Co-chair Oren K Fix MD MSc FAASLD Swedish Medical Center (Washington)
o Co-chair Elizabeth C Verna MD MS Columbia University (New York)
o Kimberly Brown MD Henry Ford Health System (Michigan)
o Jaime Chu MD Icahn School of Medicine at Mount Sinai (New York)
o Bilal Hameed MD University of California (California)
o Laura M Kulik MD Northwestern Medical Faculty Foundation (Illinois)
o Ryan M Kwok MD Uniformed Services University (Maryland)
o Brendan M McGuire MD University of Alabama (Alabama)
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 16
o Jennifer Price MD MBA FACP University of California San Francisco (California)
o Daniel S Pratt MD FAASLD Massachusetts General Hospital (Massachusetts)
o Nancy S Reau MD Rush University (Illinois)
o Mark W Russo MD MPH FAASLD Carolinas Medical Center (North Carolina)
o Michael Schilsky MD FAASLD Yale University (Connecticut)
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC (California)
o Andrew Reynolds (Patient Advocate)o Raymond Chung and K Rajender Reddy
(ex-officio)
Clinical Oversight amp Publications Subcommittee
Submit your questions in the QampA box at the top or bottom of your screen
Questions will be answered at the end of the presentation
Webinar QampA
Webinar ModeratorKimberly Ann Brown MD
FAASLDChief Division of
Gastroenterology amp Hepatology
Henry Ford Health System
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 18
Webinar PresenterBilal Hameed MD
Associate Professor of Medicine and the Hepatology Clinic Chief
University of California San Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 19
Webinar PresenterPatricia Harren DNP DCC
Clinical Director of the Center for Liver Disease amp Transplantation Clinical Director for Pediatric Transplantation
amp Adult Abdominal Organ Transplantation
Columbia University
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 20
Webinar PresenterDavid C Mulligan MD FAASLDProfessor of Surgery and Chief
of Transplantation and Immunology
Yale University Yale New Haven Health System
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 21
o Oren K Fix MD MSc FAASLD Swedish Medical Center (Washington)
o Elizabeth C Verna MD MS Columbia University (New York)
o Jaime Chu MD Icahn School of Medicine at Mount Sinai (New York)
o Karen Hoyt BA Patient Advocate
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 22
o Guadalupe Garcia-Tsao MD FAASLD Yale University (Connecticut)
o Ryutaro Hirose MD University of California San Francisco (California)
o K Gautham Reddy MD FAASLD University of Chicago Medical Center (Illinois)
Webinar Panelist
o OpenSAFELY Factors associated with COVID-19-related hospital deaths in the linked electronic health records of 17 million adult NHS patientsbull 17425445 adultsbull Feb 1 2020 to April 25 2020bull Primary outcome death in hospital in patients with confirmed
COVID-19 (5683 deaths)
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
httpsdoiorg1011012020050620092999
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
httpsdoiorg1011012020050620092999
HR adjusted for all other factors listed other than ethnicity
o Largest cohort study to date evaluating a variety of clinical factors for death from COVID-19
o Asians and blacks appear to be at increased risk of in-hospital death with only partial attribution to pre-existing clinical risk factors or deprivation
o Patients with pre-existing liver disease transplantation or on immunosuppression appear to have increased risk of in-hospital death when adjusted for agesex alone or fully adjusted
o Strengthsbull Largest cohort study to date representing 40 English populationbull Inclusion of variables including liver disease transplant for analysis
o Weaknessesbull Deaths related to patients with false-negative tests or died without testing would be missedbull Censoring patients at date of death from other causes or outside the hospital stopped 9
days short of study end bull Cohort limited to those practices using the EHR software SystmOne Some variable were
assumed absent if missing bull Characterization of ldquoliver diseaserdquo is general and not complete
o Further characterization of liver disease and potential risks due to etiology MELD etc will be helpful in future studies
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORGhttpsdoiorg1011012020050620092999
Expert Panel Consensus Statement
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 26
o First published online March 23rdo New update posted today
wwwaasldorgcovid19o Spanish and Portuguese
translations available onlineo Hepatology manuscript published
online
May 14th Update Major Changes
o Acknowledgement of possible link between COVID-19 and Kawasaki-like pediatric multisystem inflammatory syndrome
o Italian autopsy series describing involvement of hepatic vasculature including acute portal and sinusoidal thrombosis
o Introduction of SARS-CoV-2 antigen testing in addition to increasing availability of antibody testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 27
httpswwwhealthnygovpressreleases2020docs2020-05-06_covid19_pediatric_inflammatory_syndromepdfSonzogni et al Preprints 2020httpswwwfdagovnews-eventspress-announcementscoronavirus-covid-19-update-fda-authorizes-first-antigen-test-help-rapid-detection-virus-causes
May 14th Update Major Changes
o OpenSAFELY study from the UK chronic liver disease is a risk factor for in-hospital death from COVID-19
o Large US study also showed that chronic liver disease and cirrhosis are associated with higher COVID-19 mortality
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 28
Williamson et al MedRxiv 2020Singh and Khan Gastroenterol 2020
May 14th Update Major Changes
o Clarification that treatment of hepatitis B is not contraindicated in patients with or without COVID-19
o Recommendations regarding use of masks for patients and caregivers as well as providers in the clinic or hospital setting
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 29
May 14th Update Major Changes
o Evolving data on hydroxychloroquine suggesting it should no longer be used outside RCTs
o New data on triple therapy with lopinavir-ritonavir ribavirin and interferon-beta-1b showing more rapid viral clearance compared to lopinavir-ritonavir (phase 2 RCT)
o Reentry
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 30
Geleris et al N Eng J Med 2020Hung et al Lancet 2020
31
Impact of COVID-19 on Liver Disease Safe Outpatient Re-Entry Process
Bilal Hameed MDAssociate Professor of Medicine
Clinic Chief Hepatology University of California San Francisco
Outline
The COVID-19 effects on liver care Recommendations for re-entry and re-opening facilities Ambulatory re-entry and recovery challenges and plan
at UCSF Gradual re-entry of liver patients in the ambulatory
setting
The Untold Toll mdash The Pandemicrsquos Effects on Patients without COVID-19
httpswwwnejmorgdoifull101056NEJMms2009984query=featured_coronavirus
Patients with heart attacks strokes and even appendicitis vanish from
hospitals
The Pandemicrsquos Effects on Patients without COVID-1938 reduction in STEMI activations in the US
during COVID-19 pandemic
Garcia S et al Journal of the American College of Cardiology April 2020
Decrease in routine pediatric vaccination during COVID-19
httpswwwcdcgovmmwrvolumes69wr
Unexpected Consequences of the Pandemic
To expand capacity for COVID-19 patients on March 18th CMS recommended limiting non-essential care and procedures 8 week pause in usual care activities Fear of returning to care Change in patientrsquos perception of riskbenefit
Areas with lowstable incidence of COVID-19 CMS allowing non-emergent non-COVID-19 healthcare
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdf
COVID-19 Pandemic Impact on the Cirrhosis Care
Tapper EB et al Journal of Hepatology April 2020
COVID Surge
Loss of insurance
Outpatient Impact of COVID-19 Pandemic UCSF Experience Maximizing Appropriate Use of Video Visits during Re-entry
Prior State Current State Future State~20 of total visits were video visits
~95 of total visits are video visits
Appropriate mix of telehealth visits ~50
Continue expanding to -Patients that live far away -Post-ops amp post-discharge follow-up-Chronic disease management(NAFLDHBVHCV etc)-Free up clinic space
0
10000
20000
30000
40000
50000
60000
70000
End of April Double March volume
February 2 of all visits2nd largest video visit program in the
country among AMCs largest in California
End of March 60 of visits
UCSF Video Visits by Month (Jan 2015-April 2020)
0
100
200
300
400
500
600
700
800
900
Jul 2019 Aug Sep Oct Nov Dec Jan 2020 Feb Mar Apr
Able to see the same number of patients even during pandemic
Hepatology Video Visits by Month at UCSF
CMS Phase I Recommendations Re-opening Facilities for Non-emergent Non-COVID-19 Healthcare
In coordination with State and local public health officials evaluate the incidence and trends for COVID-19 in the area
Prioritize surgicalprocedural care and high-complexity chronic disease management and select preventive services
Consider establishing Non-COVID Care (NCC) zones that would screen all patients for symptoms of COVID-19
Sufficient resources should be available across phases of care including PPE healthy workforce testing capacity etc and without jeopardizing surge capacity
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdfhttpswwwwhitehousegovopeningamericacriteriahttpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
httpsdatasfgovorgstoriessdak2-gvuj
San Francisco COVID-19 Numbers
Ambulatory Re-entry and Recovery ndash Cascaded Principles
Ensure morbidity and mortality do not increase due to liver related illness and provide care in a safe manner
Continue to prioritize the health and safety of workforce Prioritize urgent patients Communicate consistently and transparently Invest appropriately in services and improvement efforts
Strategies to limit unnecessary exposure while continuing to provide high-quality care for our liver patients
bull Optimization and flexibility of schedules (hoursweekend)
bull Utilization of clinic spacebull Sustain telehealth bull Digital technology for symptoms
monitoring bull Staff redeployment
bull COVID symptoms check protocolbull Social distancing in clinicbull Masking and safety policiesbull Waiting rooms changesbull Visitor policies
bull Prioritize urgent patientsbull Back log data and referralsbull Pre-clinic communicationbull In clinic flow (Echeck in rooming
and check out policies)
bull Patient communication is the keybull Staff anxiety and stress reduction bull Focus on vulnerable populationbull Physician burn out and health needs bull Trainees re-entry and education
Staff and PatientSafety
Clinic Work Flows
Resource Utilization
Support and
Education
PatientCare
Ambulatory Recovery Challenges and PlanProviding Best Care While Living with COVID-19
Physical Distancing amp Safety Guidelines
Conversa Employee Screening Mychart Screener Apex texting for patients in
nearby waiting areas
Innovation and Improving Operations
Gradual Re-entry of Liver Patients in the Ambulatory Setting
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
Patient will be scheduled for modified evaluation with
Hepatology and social worker as video visit
Remainder of evaluation will be onsite when restrictions are lifted
1 Pre-clinicarrival COVID screening for patientscaregiver2 Universal masking
no
Re-entry of Liver Patients in Clinic June 2020
All new liver transplant evaluations and HCC diagnosis New decompensation or worsening symptoms Listed patients for transplant with decompensated cirrhosis Acute hepatitis or liver injury Early post transplant Patients with difficulty with telehealth
Re-entry of Liver Patients HCC Surveillance HCC surveillance should continue as close to schedule (an
arbitrary delay of 2 months were acceptable) Working on list of all delayed imaging and prioritizing them by
risk categoriesKnown HCC surveillance for treatment response elevated AFP
Key is working with Radiology (Options of imaging locally) Communication with patients and documentation is important No delay in HCC treatment (riskbenefits discussion)
httpswwwaasldorgsitesdefaultfiles2020-05AASLD-COVID19-ClinicalInsights-May42020
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
Fibroscan Not urgent but planning to
start June-July 2020 Huge back log Using radiology US protocol
for PPE (maskgoogles and gown) Flexible schedules based on
safety guidelines
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

10
New AASLD Journals App
Access all four AASLD Journals in a single app
aasldorgpublications
11
Submit abstracts at aasldorgLMabstracts
a a s l d f n d o r g d o n a t e
CME MOC and E
Available
a a s l d f n d o r g
You can help invest in the future of hepatology by supporting
more research amp advanced career training
Donate today to AASLD Foundation
Follow us on Twitter AASLDFoundation
aasldfoundationorgdonate
13
Register Now for May 28th Webinar
AASLD-ALEH COVID-19 amp the Liver in the Americas
aasldorgcalendar
14
COVID-19 and the Liver Reentry and Return to a Pre-Pandemic State
o Webinar Contributorso Presenter Introductions ndash Dr Kimberly Brown
o Housekeeping Itemso OpenSAFELY Study ndash Dr Kimberly Brown
o Expert Consensus Panel Update ndash Dr Oren Fixo Outpatient ndash Dr Bilal Hameedo Inpatient ndash Dr Patricia Harreno Transplant ndash Dr David Mulligan
o Panel Discussion QampA
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 15
Webinar Agenda
o Co-chair Oren K Fix MD MSc FAASLD Swedish Medical Center (Washington)
o Co-chair Elizabeth C Verna MD MS Columbia University (New York)
o Kimberly Brown MD Henry Ford Health System (Michigan)
o Jaime Chu MD Icahn School of Medicine at Mount Sinai (New York)
o Bilal Hameed MD University of California (California)
o Laura M Kulik MD Northwestern Medical Faculty Foundation (Illinois)
o Ryan M Kwok MD Uniformed Services University (Maryland)
o Brendan M McGuire MD University of Alabama (Alabama)
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 16
o Jennifer Price MD MBA FACP University of California San Francisco (California)
o Daniel S Pratt MD FAASLD Massachusetts General Hospital (Massachusetts)
o Nancy S Reau MD Rush University (Illinois)
o Mark W Russo MD MPH FAASLD Carolinas Medical Center (North Carolina)
o Michael Schilsky MD FAASLD Yale University (Connecticut)
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC (California)
o Andrew Reynolds (Patient Advocate)o Raymond Chung and K Rajender Reddy
(ex-officio)
Clinical Oversight amp Publications Subcommittee
Submit your questions in the QampA box at the top or bottom of your screen
Questions will be answered at the end of the presentation
Webinar QampA
Webinar ModeratorKimberly Ann Brown MD
FAASLDChief Division of
Gastroenterology amp Hepatology
Henry Ford Health System
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 18
Webinar PresenterBilal Hameed MD
Associate Professor of Medicine and the Hepatology Clinic Chief
University of California San Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 19
Webinar PresenterPatricia Harren DNP DCC
Clinical Director of the Center for Liver Disease amp Transplantation Clinical Director for Pediatric Transplantation
amp Adult Abdominal Organ Transplantation
Columbia University
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 20
Webinar PresenterDavid C Mulligan MD FAASLDProfessor of Surgery and Chief
of Transplantation and Immunology
Yale University Yale New Haven Health System
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 21
o Oren K Fix MD MSc FAASLD Swedish Medical Center (Washington)
o Elizabeth C Verna MD MS Columbia University (New York)
o Jaime Chu MD Icahn School of Medicine at Mount Sinai (New York)
o Karen Hoyt BA Patient Advocate
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 22
o Guadalupe Garcia-Tsao MD FAASLD Yale University (Connecticut)
o Ryutaro Hirose MD University of California San Francisco (California)
o K Gautham Reddy MD FAASLD University of Chicago Medical Center (Illinois)
Webinar Panelist
o OpenSAFELY Factors associated with COVID-19-related hospital deaths in the linked electronic health records of 17 million adult NHS patientsbull 17425445 adultsbull Feb 1 2020 to April 25 2020bull Primary outcome death in hospital in patients with confirmed
COVID-19 (5683 deaths)
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
httpsdoiorg1011012020050620092999
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
httpsdoiorg1011012020050620092999
HR adjusted for all other factors listed other than ethnicity
o Largest cohort study to date evaluating a variety of clinical factors for death from COVID-19
o Asians and blacks appear to be at increased risk of in-hospital death with only partial attribution to pre-existing clinical risk factors or deprivation
o Patients with pre-existing liver disease transplantation or on immunosuppression appear to have increased risk of in-hospital death when adjusted for agesex alone or fully adjusted
o Strengthsbull Largest cohort study to date representing 40 English populationbull Inclusion of variables including liver disease transplant for analysis
o Weaknessesbull Deaths related to patients with false-negative tests or died without testing would be missedbull Censoring patients at date of death from other causes or outside the hospital stopped 9
days short of study end bull Cohort limited to those practices using the EHR software SystmOne Some variable were
assumed absent if missing bull Characterization of ldquoliver diseaserdquo is general and not complete
o Further characterization of liver disease and potential risks due to etiology MELD etc will be helpful in future studies
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORGhttpsdoiorg1011012020050620092999
Expert Panel Consensus Statement
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 26
o First published online March 23rdo New update posted today
wwwaasldorgcovid19o Spanish and Portuguese
translations available onlineo Hepatology manuscript published
online
May 14th Update Major Changes
o Acknowledgement of possible link between COVID-19 and Kawasaki-like pediatric multisystem inflammatory syndrome
o Italian autopsy series describing involvement of hepatic vasculature including acute portal and sinusoidal thrombosis
o Introduction of SARS-CoV-2 antigen testing in addition to increasing availability of antibody testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 27
httpswwwhealthnygovpressreleases2020docs2020-05-06_covid19_pediatric_inflammatory_syndromepdfSonzogni et al Preprints 2020httpswwwfdagovnews-eventspress-announcementscoronavirus-covid-19-update-fda-authorizes-first-antigen-test-help-rapid-detection-virus-causes
May 14th Update Major Changes
o OpenSAFELY study from the UK chronic liver disease is a risk factor for in-hospital death from COVID-19
o Large US study also showed that chronic liver disease and cirrhosis are associated with higher COVID-19 mortality
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 28
Williamson et al MedRxiv 2020Singh and Khan Gastroenterol 2020
May 14th Update Major Changes
o Clarification that treatment of hepatitis B is not contraindicated in patients with or without COVID-19
o Recommendations regarding use of masks for patients and caregivers as well as providers in the clinic or hospital setting
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 29
May 14th Update Major Changes
o Evolving data on hydroxychloroquine suggesting it should no longer be used outside RCTs
o New data on triple therapy with lopinavir-ritonavir ribavirin and interferon-beta-1b showing more rapid viral clearance compared to lopinavir-ritonavir (phase 2 RCT)
o Reentry
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 30
Geleris et al N Eng J Med 2020Hung et al Lancet 2020
31
Impact of COVID-19 on Liver Disease Safe Outpatient Re-Entry Process
Bilal Hameed MDAssociate Professor of Medicine
Clinic Chief Hepatology University of California San Francisco
Outline
The COVID-19 effects on liver care Recommendations for re-entry and re-opening facilities Ambulatory re-entry and recovery challenges and plan
at UCSF Gradual re-entry of liver patients in the ambulatory
setting
The Untold Toll mdash The Pandemicrsquos Effects on Patients without COVID-19
httpswwwnejmorgdoifull101056NEJMms2009984query=featured_coronavirus
Patients with heart attacks strokes and even appendicitis vanish from
hospitals
The Pandemicrsquos Effects on Patients without COVID-1938 reduction in STEMI activations in the US
during COVID-19 pandemic
Garcia S et al Journal of the American College of Cardiology April 2020
Decrease in routine pediatric vaccination during COVID-19
httpswwwcdcgovmmwrvolumes69wr
Unexpected Consequences of the Pandemic
To expand capacity for COVID-19 patients on March 18th CMS recommended limiting non-essential care and procedures 8 week pause in usual care activities Fear of returning to care Change in patientrsquos perception of riskbenefit
Areas with lowstable incidence of COVID-19 CMS allowing non-emergent non-COVID-19 healthcare
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdf
COVID-19 Pandemic Impact on the Cirrhosis Care
Tapper EB et al Journal of Hepatology April 2020
COVID Surge
Loss of insurance
Outpatient Impact of COVID-19 Pandemic UCSF Experience Maximizing Appropriate Use of Video Visits during Re-entry
Prior State Current State Future State~20 of total visits were video visits
~95 of total visits are video visits
Appropriate mix of telehealth visits ~50
Continue expanding to -Patients that live far away -Post-ops amp post-discharge follow-up-Chronic disease management(NAFLDHBVHCV etc)-Free up clinic space
0
10000
20000
30000
40000
50000
60000
70000
End of April Double March volume
February 2 of all visits2nd largest video visit program in the
country among AMCs largest in California
End of March 60 of visits
UCSF Video Visits by Month (Jan 2015-April 2020)
0
100
200
300
400
500
600
700
800
900
Jul 2019 Aug Sep Oct Nov Dec Jan 2020 Feb Mar Apr
Able to see the same number of patients even during pandemic
Hepatology Video Visits by Month at UCSF
CMS Phase I Recommendations Re-opening Facilities for Non-emergent Non-COVID-19 Healthcare
In coordination with State and local public health officials evaluate the incidence and trends for COVID-19 in the area
Prioritize surgicalprocedural care and high-complexity chronic disease management and select preventive services
Consider establishing Non-COVID Care (NCC) zones that would screen all patients for symptoms of COVID-19
Sufficient resources should be available across phases of care including PPE healthy workforce testing capacity etc and without jeopardizing surge capacity
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdfhttpswwwwhitehousegovopeningamericacriteriahttpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
httpsdatasfgovorgstoriessdak2-gvuj
San Francisco COVID-19 Numbers
Ambulatory Re-entry and Recovery ndash Cascaded Principles
Ensure morbidity and mortality do not increase due to liver related illness and provide care in a safe manner
Continue to prioritize the health and safety of workforce Prioritize urgent patients Communicate consistently and transparently Invest appropriately in services and improvement efforts
Strategies to limit unnecessary exposure while continuing to provide high-quality care for our liver patients
bull Optimization and flexibility of schedules (hoursweekend)
bull Utilization of clinic spacebull Sustain telehealth bull Digital technology for symptoms
monitoring bull Staff redeployment
bull COVID symptoms check protocolbull Social distancing in clinicbull Masking and safety policiesbull Waiting rooms changesbull Visitor policies
bull Prioritize urgent patientsbull Back log data and referralsbull Pre-clinic communicationbull In clinic flow (Echeck in rooming
and check out policies)
bull Patient communication is the keybull Staff anxiety and stress reduction bull Focus on vulnerable populationbull Physician burn out and health needs bull Trainees re-entry and education
Staff and PatientSafety
Clinic Work Flows
Resource Utilization
Support and
Education
PatientCare
Ambulatory Recovery Challenges and PlanProviding Best Care While Living with COVID-19
Physical Distancing amp Safety Guidelines
Conversa Employee Screening Mychart Screener Apex texting for patients in
nearby waiting areas
Innovation and Improving Operations
Gradual Re-entry of Liver Patients in the Ambulatory Setting
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
Patient will be scheduled for modified evaluation with
Hepatology and social worker as video visit
Remainder of evaluation will be onsite when restrictions are lifted
1 Pre-clinicarrival COVID screening for patientscaregiver2 Universal masking
no
Re-entry of Liver Patients in Clinic June 2020
All new liver transplant evaluations and HCC diagnosis New decompensation or worsening symptoms Listed patients for transplant with decompensated cirrhosis Acute hepatitis or liver injury Early post transplant Patients with difficulty with telehealth
Re-entry of Liver Patients HCC Surveillance HCC surveillance should continue as close to schedule (an
arbitrary delay of 2 months were acceptable) Working on list of all delayed imaging and prioritizing them by
risk categoriesKnown HCC surveillance for treatment response elevated AFP
Key is working with Radiology (Options of imaging locally) Communication with patients and documentation is important No delay in HCC treatment (riskbenefits discussion)
httpswwwaasldorgsitesdefaultfiles2020-05AASLD-COVID19-ClinicalInsights-May42020
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
Fibroscan Not urgent but planning to
start June-July 2020 Huge back log Using radiology US protocol
for PPE (maskgoogles and gown) Flexible schedules based on
safety guidelines
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

11
Submit abstracts at aasldorgLMabstracts
a a s l d f n d o r g d o n a t e
CME MOC and E
Available
a a s l d f n d o r g
You can help invest in the future of hepatology by supporting
more research amp advanced career training
Donate today to AASLD Foundation
Follow us on Twitter AASLDFoundation
aasldfoundationorgdonate
13
Register Now for May 28th Webinar
AASLD-ALEH COVID-19 amp the Liver in the Americas
aasldorgcalendar
14
COVID-19 and the Liver Reentry and Return to a Pre-Pandemic State
o Webinar Contributorso Presenter Introductions ndash Dr Kimberly Brown
o Housekeeping Itemso OpenSAFELY Study ndash Dr Kimberly Brown
o Expert Consensus Panel Update ndash Dr Oren Fixo Outpatient ndash Dr Bilal Hameedo Inpatient ndash Dr Patricia Harreno Transplant ndash Dr David Mulligan
o Panel Discussion QampA
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 15
Webinar Agenda
o Co-chair Oren K Fix MD MSc FAASLD Swedish Medical Center (Washington)
o Co-chair Elizabeth C Verna MD MS Columbia University (New York)
o Kimberly Brown MD Henry Ford Health System (Michigan)
o Jaime Chu MD Icahn School of Medicine at Mount Sinai (New York)
o Bilal Hameed MD University of California (California)
o Laura M Kulik MD Northwestern Medical Faculty Foundation (Illinois)
o Ryan M Kwok MD Uniformed Services University (Maryland)
o Brendan M McGuire MD University of Alabama (Alabama)
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 16
o Jennifer Price MD MBA FACP University of California San Francisco (California)
o Daniel S Pratt MD FAASLD Massachusetts General Hospital (Massachusetts)
o Nancy S Reau MD Rush University (Illinois)
o Mark W Russo MD MPH FAASLD Carolinas Medical Center (North Carolina)
o Michael Schilsky MD FAASLD Yale University (Connecticut)
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC (California)
o Andrew Reynolds (Patient Advocate)o Raymond Chung and K Rajender Reddy
(ex-officio)
Clinical Oversight amp Publications Subcommittee
Submit your questions in the QampA box at the top or bottom of your screen
Questions will be answered at the end of the presentation
Webinar QampA
Webinar ModeratorKimberly Ann Brown MD
FAASLDChief Division of
Gastroenterology amp Hepatology
Henry Ford Health System
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 18
Webinar PresenterBilal Hameed MD
Associate Professor of Medicine and the Hepatology Clinic Chief
University of California San Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 19
Webinar PresenterPatricia Harren DNP DCC
Clinical Director of the Center for Liver Disease amp Transplantation Clinical Director for Pediatric Transplantation
amp Adult Abdominal Organ Transplantation
Columbia University
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 20
Webinar PresenterDavid C Mulligan MD FAASLDProfessor of Surgery and Chief
of Transplantation and Immunology
Yale University Yale New Haven Health System
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 21
o Oren K Fix MD MSc FAASLD Swedish Medical Center (Washington)
o Elizabeth C Verna MD MS Columbia University (New York)
o Jaime Chu MD Icahn School of Medicine at Mount Sinai (New York)
o Karen Hoyt BA Patient Advocate
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 22
o Guadalupe Garcia-Tsao MD FAASLD Yale University (Connecticut)
o Ryutaro Hirose MD University of California San Francisco (California)
o K Gautham Reddy MD FAASLD University of Chicago Medical Center (Illinois)
Webinar Panelist
o OpenSAFELY Factors associated with COVID-19-related hospital deaths in the linked electronic health records of 17 million adult NHS patientsbull 17425445 adultsbull Feb 1 2020 to April 25 2020bull Primary outcome death in hospital in patients with confirmed
COVID-19 (5683 deaths)
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
httpsdoiorg1011012020050620092999
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
httpsdoiorg1011012020050620092999
HR adjusted for all other factors listed other than ethnicity
o Largest cohort study to date evaluating a variety of clinical factors for death from COVID-19
o Asians and blacks appear to be at increased risk of in-hospital death with only partial attribution to pre-existing clinical risk factors or deprivation
o Patients with pre-existing liver disease transplantation or on immunosuppression appear to have increased risk of in-hospital death when adjusted for agesex alone or fully adjusted
o Strengthsbull Largest cohort study to date representing 40 English populationbull Inclusion of variables including liver disease transplant for analysis
o Weaknessesbull Deaths related to patients with false-negative tests or died without testing would be missedbull Censoring patients at date of death from other causes or outside the hospital stopped 9
days short of study end bull Cohort limited to those practices using the EHR software SystmOne Some variable were
assumed absent if missing bull Characterization of ldquoliver diseaserdquo is general and not complete
o Further characterization of liver disease and potential risks due to etiology MELD etc will be helpful in future studies
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORGhttpsdoiorg1011012020050620092999
Expert Panel Consensus Statement
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 26
o First published online March 23rdo New update posted today
wwwaasldorgcovid19o Spanish and Portuguese
translations available onlineo Hepatology manuscript published
online
May 14th Update Major Changes
o Acknowledgement of possible link between COVID-19 and Kawasaki-like pediatric multisystem inflammatory syndrome
o Italian autopsy series describing involvement of hepatic vasculature including acute portal and sinusoidal thrombosis
o Introduction of SARS-CoV-2 antigen testing in addition to increasing availability of antibody testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 27
httpswwwhealthnygovpressreleases2020docs2020-05-06_covid19_pediatric_inflammatory_syndromepdfSonzogni et al Preprints 2020httpswwwfdagovnews-eventspress-announcementscoronavirus-covid-19-update-fda-authorizes-first-antigen-test-help-rapid-detection-virus-causes
May 14th Update Major Changes
o OpenSAFELY study from the UK chronic liver disease is a risk factor for in-hospital death from COVID-19
o Large US study also showed that chronic liver disease and cirrhosis are associated with higher COVID-19 mortality
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 28
Williamson et al MedRxiv 2020Singh and Khan Gastroenterol 2020
May 14th Update Major Changes
o Clarification that treatment of hepatitis B is not contraindicated in patients with or without COVID-19
o Recommendations regarding use of masks for patients and caregivers as well as providers in the clinic or hospital setting
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 29
May 14th Update Major Changes
o Evolving data on hydroxychloroquine suggesting it should no longer be used outside RCTs
o New data on triple therapy with lopinavir-ritonavir ribavirin and interferon-beta-1b showing more rapid viral clearance compared to lopinavir-ritonavir (phase 2 RCT)
o Reentry
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 30
Geleris et al N Eng J Med 2020Hung et al Lancet 2020
31
Impact of COVID-19 on Liver Disease Safe Outpatient Re-Entry Process
Bilal Hameed MDAssociate Professor of Medicine
Clinic Chief Hepatology University of California San Francisco
Outline
The COVID-19 effects on liver care Recommendations for re-entry and re-opening facilities Ambulatory re-entry and recovery challenges and plan
at UCSF Gradual re-entry of liver patients in the ambulatory
setting
The Untold Toll mdash The Pandemicrsquos Effects on Patients without COVID-19
httpswwwnejmorgdoifull101056NEJMms2009984query=featured_coronavirus
Patients with heart attacks strokes and even appendicitis vanish from
hospitals
The Pandemicrsquos Effects on Patients without COVID-1938 reduction in STEMI activations in the US
during COVID-19 pandemic
Garcia S et al Journal of the American College of Cardiology April 2020
Decrease in routine pediatric vaccination during COVID-19
httpswwwcdcgovmmwrvolumes69wr
Unexpected Consequences of the Pandemic
To expand capacity for COVID-19 patients on March 18th CMS recommended limiting non-essential care and procedures 8 week pause in usual care activities Fear of returning to care Change in patientrsquos perception of riskbenefit
Areas with lowstable incidence of COVID-19 CMS allowing non-emergent non-COVID-19 healthcare
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdf
COVID-19 Pandemic Impact on the Cirrhosis Care
Tapper EB et al Journal of Hepatology April 2020
COVID Surge
Loss of insurance
Outpatient Impact of COVID-19 Pandemic UCSF Experience Maximizing Appropriate Use of Video Visits during Re-entry
Prior State Current State Future State~20 of total visits were video visits
~95 of total visits are video visits
Appropriate mix of telehealth visits ~50
Continue expanding to -Patients that live far away -Post-ops amp post-discharge follow-up-Chronic disease management(NAFLDHBVHCV etc)-Free up clinic space
0
10000
20000
30000
40000
50000
60000
70000
End of April Double March volume
February 2 of all visits2nd largest video visit program in the
country among AMCs largest in California
End of March 60 of visits
UCSF Video Visits by Month (Jan 2015-April 2020)
0
100
200
300
400
500
600
700
800
900
Jul 2019 Aug Sep Oct Nov Dec Jan 2020 Feb Mar Apr
Able to see the same number of patients even during pandemic
Hepatology Video Visits by Month at UCSF
CMS Phase I Recommendations Re-opening Facilities for Non-emergent Non-COVID-19 Healthcare
In coordination with State and local public health officials evaluate the incidence and trends for COVID-19 in the area
Prioritize surgicalprocedural care and high-complexity chronic disease management and select preventive services
Consider establishing Non-COVID Care (NCC) zones that would screen all patients for symptoms of COVID-19
Sufficient resources should be available across phases of care including PPE healthy workforce testing capacity etc and without jeopardizing surge capacity
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdfhttpswwwwhitehousegovopeningamericacriteriahttpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
httpsdatasfgovorgstoriessdak2-gvuj
San Francisco COVID-19 Numbers
Ambulatory Re-entry and Recovery ndash Cascaded Principles
Ensure morbidity and mortality do not increase due to liver related illness and provide care in a safe manner
Continue to prioritize the health and safety of workforce Prioritize urgent patients Communicate consistently and transparently Invest appropriately in services and improvement efforts
Strategies to limit unnecessary exposure while continuing to provide high-quality care for our liver patients
bull Optimization and flexibility of schedules (hoursweekend)
bull Utilization of clinic spacebull Sustain telehealth bull Digital technology for symptoms
monitoring bull Staff redeployment
bull COVID symptoms check protocolbull Social distancing in clinicbull Masking and safety policiesbull Waiting rooms changesbull Visitor policies
bull Prioritize urgent patientsbull Back log data and referralsbull Pre-clinic communicationbull In clinic flow (Echeck in rooming
and check out policies)
bull Patient communication is the keybull Staff anxiety and stress reduction bull Focus on vulnerable populationbull Physician burn out and health needs bull Trainees re-entry and education
Staff and PatientSafety
Clinic Work Flows
Resource Utilization
Support and
Education
PatientCare
Ambulatory Recovery Challenges and PlanProviding Best Care While Living with COVID-19
Physical Distancing amp Safety Guidelines
Conversa Employee Screening Mychart Screener Apex texting for patients in
nearby waiting areas
Innovation and Improving Operations
Gradual Re-entry of Liver Patients in the Ambulatory Setting
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
Patient will be scheduled for modified evaluation with
Hepatology and social worker as video visit
Remainder of evaluation will be onsite when restrictions are lifted
1 Pre-clinicarrival COVID screening for patientscaregiver2 Universal masking
no
Re-entry of Liver Patients in Clinic June 2020
All new liver transplant evaluations and HCC diagnosis New decompensation or worsening symptoms Listed patients for transplant with decompensated cirrhosis Acute hepatitis or liver injury Early post transplant Patients with difficulty with telehealth
Re-entry of Liver Patients HCC Surveillance HCC surveillance should continue as close to schedule (an
arbitrary delay of 2 months were acceptable) Working on list of all delayed imaging and prioritizing them by
risk categoriesKnown HCC surveillance for treatment response elevated AFP
Key is working with Radiology (Options of imaging locally) Communication with patients and documentation is important No delay in HCC treatment (riskbenefits discussion)
httpswwwaasldorgsitesdefaultfiles2020-05AASLD-COVID19-ClinicalInsights-May42020
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
Fibroscan Not urgent but planning to
start June-July 2020 Huge back log Using radiology US protocol
for PPE (maskgoogles and gown) Flexible schedules based on
safety guidelines
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

a a s l d f n d o r g d o n a t e
CME MOC and E
Available
a a s l d f n d o r g
You can help invest in the future of hepatology by supporting
more research amp advanced career training
Donate today to AASLD Foundation
Follow us on Twitter AASLDFoundation
aasldfoundationorgdonate
13
Register Now for May 28th Webinar
AASLD-ALEH COVID-19 amp the Liver in the Americas
aasldorgcalendar
14
COVID-19 and the Liver Reentry and Return to a Pre-Pandemic State
o Webinar Contributorso Presenter Introductions ndash Dr Kimberly Brown
o Housekeeping Itemso OpenSAFELY Study ndash Dr Kimberly Brown
o Expert Consensus Panel Update ndash Dr Oren Fixo Outpatient ndash Dr Bilal Hameedo Inpatient ndash Dr Patricia Harreno Transplant ndash Dr David Mulligan
o Panel Discussion QampA
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 15
Webinar Agenda
o Co-chair Oren K Fix MD MSc FAASLD Swedish Medical Center (Washington)
o Co-chair Elizabeth C Verna MD MS Columbia University (New York)
o Kimberly Brown MD Henry Ford Health System (Michigan)
o Jaime Chu MD Icahn School of Medicine at Mount Sinai (New York)
o Bilal Hameed MD University of California (California)
o Laura M Kulik MD Northwestern Medical Faculty Foundation (Illinois)
o Ryan M Kwok MD Uniformed Services University (Maryland)
o Brendan M McGuire MD University of Alabama (Alabama)
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 16
o Jennifer Price MD MBA FACP University of California San Francisco (California)
o Daniel S Pratt MD FAASLD Massachusetts General Hospital (Massachusetts)
o Nancy S Reau MD Rush University (Illinois)
o Mark W Russo MD MPH FAASLD Carolinas Medical Center (North Carolina)
o Michael Schilsky MD FAASLD Yale University (Connecticut)
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC (California)
o Andrew Reynolds (Patient Advocate)o Raymond Chung and K Rajender Reddy
(ex-officio)
Clinical Oversight amp Publications Subcommittee
Submit your questions in the QampA box at the top or bottom of your screen
Questions will be answered at the end of the presentation
Webinar QampA
Webinar ModeratorKimberly Ann Brown MD
FAASLDChief Division of
Gastroenterology amp Hepatology
Henry Ford Health System
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 18
Webinar PresenterBilal Hameed MD
Associate Professor of Medicine and the Hepatology Clinic Chief
University of California San Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 19
Webinar PresenterPatricia Harren DNP DCC
Clinical Director of the Center for Liver Disease amp Transplantation Clinical Director for Pediatric Transplantation
amp Adult Abdominal Organ Transplantation
Columbia University
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 20
Webinar PresenterDavid C Mulligan MD FAASLDProfessor of Surgery and Chief
of Transplantation and Immunology
Yale University Yale New Haven Health System
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 21
o Oren K Fix MD MSc FAASLD Swedish Medical Center (Washington)
o Elizabeth C Verna MD MS Columbia University (New York)
o Jaime Chu MD Icahn School of Medicine at Mount Sinai (New York)
o Karen Hoyt BA Patient Advocate
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 22
o Guadalupe Garcia-Tsao MD FAASLD Yale University (Connecticut)
o Ryutaro Hirose MD University of California San Francisco (California)
o K Gautham Reddy MD FAASLD University of Chicago Medical Center (Illinois)
Webinar Panelist
o OpenSAFELY Factors associated with COVID-19-related hospital deaths in the linked electronic health records of 17 million adult NHS patientsbull 17425445 adultsbull Feb 1 2020 to April 25 2020bull Primary outcome death in hospital in patients with confirmed
COVID-19 (5683 deaths)
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
httpsdoiorg1011012020050620092999
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
httpsdoiorg1011012020050620092999
HR adjusted for all other factors listed other than ethnicity
o Largest cohort study to date evaluating a variety of clinical factors for death from COVID-19
o Asians and blacks appear to be at increased risk of in-hospital death with only partial attribution to pre-existing clinical risk factors or deprivation
o Patients with pre-existing liver disease transplantation or on immunosuppression appear to have increased risk of in-hospital death when adjusted for agesex alone or fully adjusted
o Strengthsbull Largest cohort study to date representing 40 English populationbull Inclusion of variables including liver disease transplant for analysis
o Weaknessesbull Deaths related to patients with false-negative tests or died without testing would be missedbull Censoring patients at date of death from other causes or outside the hospital stopped 9
days short of study end bull Cohort limited to those practices using the EHR software SystmOne Some variable were
assumed absent if missing bull Characterization of ldquoliver diseaserdquo is general and not complete
o Further characterization of liver disease and potential risks due to etiology MELD etc will be helpful in future studies
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORGhttpsdoiorg1011012020050620092999
Expert Panel Consensus Statement
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 26
o First published online March 23rdo New update posted today
wwwaasldorgcovid19o Spanish and Portuguese
translations available onlineo Hepatology manuscript published
online
May 14th Update Major Changes
o Acknowledgement of possible link between COVID-19 and Kawasaki-like pediatric multisystem inflammatory syndrome
o Italian autopsy series describing involvement of hepatic vasculature including acute portal and sinusoidal thrombosis
o Introduction of SARS-CoV-2 antigen testing in addition to increasing availability of antibody testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 27
httpswwwhealthnygovpressreleases2020docs2020-05-06_covid19_pediatric_inflammatory_syndromepdfSonzogni et al Preprints 2020httpswwwfdagovnews-eventspress-announcementscoronavirus-covid-19-update-fda-authorizes-first-antigen-test-help-rapid-detection-virus-causes
May 14th Update Major Changes
o OpenSAFELY study from the UK chronic liver disease is a risk factor for in-hospital death from COVID-19
o Large US study also showed that chronic liver disease and cirrhosis are associated with higher COVID-19 mortality
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 28
Williamson et al MedRxiv 2020Singh and Khan Gastroenterol 2020
May 14th Update Major Changes
o Clarification that treatment of hepatitis B is not contraindicated in patients with or without COVID-19
o Recommendations regarding use of masks for patients and caregivers as well as providers in the clinic or hospital setting
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 29
May 14th Update Major Changes
o Evolving data on hydroxychloroquine suggesting it should no longer be used outside RCTs
o New data on triple therapy with lopinavir-ritonavir ribavirin and interferon-beta-1b showing more rapid viral clearance compared to lopinavir-ritonavir (phase 2 RCT)
o Reentry
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 30
Geleris et al N Eng J Med 2020Hung et al Lancet 2020
31
Impact of COVID-19 on Liver Disease Safe Outpatient Re-Entry Process
Bilal Hameed MDAssociate Professor of Medicine
Clinic Chief Hepatology University of California San Francisco
Outline
The COVID-19 effects on liver care Recommendations for re-entry and re-opening facilities Ambulatory re-entry and recovery challenges and plan
at UCSF Gradual re-entry of liver patients in the ambulatory
setting
The Untold Toll mdash The Pandemicrsquos Effects on Patients without COVID-19
httpswwwnejmorgdoifull101056NEJMms2009984query=featured_coronavirus
Patients with heart attacks strokes and even appendicitis vanish from
hospitals
The Pandemicrsquos Effects on Patients without COVID-1938 reduction in STEMI activations in the US
during COVID-19 pandemic
Garcia S et al Journal of the American College of Cardiology April 2020
Decrease in routine pediatric vaccination during COVID-19
httpswwwcdcgovmmwrvolumes69wr
Unexpected Consequences of the Pandemic
To expand capacity for COVID-19 patients on March 18th CMS recommended limiting non-essential care and procedures 8 week pause in usual care activities Fear of returning to care Change in patientrsquos perception of riskbenefit
Areas with lowstable incidence of COVID-19 CMS allowing non-emergent non-COVID-19 healthcare
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdf
COVID-19 Pandemic Impact on the Cirrhosis Care
Tapper EB et al Journal of Hepatology April 2020
COVID Surge
Loss of insurance
Outpatient Impact of COVID-19 Pandemic UCSF Experience Maximizing Appropriate Use of Video Visits during Re-entry
Prior State Current State Future State~20 of total visits were video visits
~95 of total visits are video visits
Appropriate mix of telehealth visits ~50
Continue expanding to -Patients that live far away -Post-ops amp post-discharge follow-up-Chronic disease management(NAFLDHBVHCV etc)-Free up clinic space
0
10000
20000
30000
40000
50000
60000
70000
End of April Double March volume
February 2 of all visits2nd largest video visit program in the
country among AMCs largest in California
End of March 60 of visits
UCSF Video Visits by Month (Jan 2015-April 2020)
0
100
200
300
400
500
600
700
800
900
Jul 2019 Aug Sep Oct Nov Dec Jan 2020 Feb Mar Apr
Able to see the same number of patients even during pandemic
Hepatology Video Visits by Month at UCSF
CMS Phase I Recommendations Re-opening Facilities for Non-emergent Non-COVID-19 Healthcare
In coordination with State and local public health officials evaluate the incidence and trends for COVID-19 in the area
Prioritize surgicalprocedural care and high-complexity chronic disease management and select preventive services
Consider establishing Non-COVID Care (NCC) zones that would screen all patients for symptoms of COVID-19
Sufficient resources should be available across phases of care including PPE healthy workforce testing capacity etc and without jeopardizing surge capacity
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdfhttpswwwwhitehousegovopeningamericacriteriahttpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
httpsdatasfgovorgstoriessdak2-gvuj
San Francisco COVID-19 Numbers
Ambulatory Re-entry and Recovery ndash Cascaded Principles
Ensure morbidity and mortality do not increase due to liver related illness and provide care in a safe manner
Continue to prioritize the health and safety of workforce Prioritize urgent patients Communicate consistently and transparently Invest appropriately in services and improvement efforts
Strategies to limit unnecessary exposure while continuing to provide high-quality care for our liver patients
bull Optimization and flexibility of schedules (hoursweekend)
bull Utilization of clinic spacebull Sustain telehealth bull Digital technology for symptoms
monitoring bull Staff redeployment
bull COVID symptoms check protocolbull Social distancing in clinicbull Masking and safety policiesbull Waiting rooms changesbull Visitor policies
bull Prioritize urgent patientsbull Back log data and referralsbull Pre-clinic communicationbull In clinic flow (Echeck in rooming
and check out policies)
bull Patient communication is the keybull Staff anxiety and stress reduction bull Focus on vulnerable populationbull Physician burn out and health needs bull Trainees re-entry and education
Staff and PatientSafety
Clinic Work Flows
Resource Utilization
Support and
Education
PatientCare
Ambulatory Recovery Challenges and PlanProviding Best Care While Living with COVID-19
Physical Distancing amp Safety Guidelines
Conversa Employee Screening Mychart Screener Apex texting for patients in
nearby waiting areas
Innovation and Improving Operations
Gradual Re-entry of Liver Patients in the Ambulatory Setting
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
Patient will be scheduled for modified evaluation with
Hepatology and social worker as video visit
Remainder of evaluation will be onsite when restrictions are lifted
1 Pre-clinicarrival COVID screening for patientscaregiver2 Universal masking
no
Re-entry of Liver Patients in Clinic June 2020
All new liver transplant evaluations and HCC diagnosis New decompensation or worsening symptoms Listed patients for transplant with decompensated cirrhosis Acute hepatitis or liver injury Early post transplant Patients with difficulty with telehealth
Re-entry of Liver Patients HCC Surveillance HCC surveillance should continue as close to schedule (an
arbitrary delay of 2 months were acceptable) Working on list of all delayed imaging and prioritizing them by
risk categoriesKnown HCC surveillance for treatment response elevated AFP
Key is working with Radiology (Options of imaging locally) Communication with patients and documentation is important No delay in HCC treatment (riskbenefits discussion)
httpswwwaasldorgsitesdefaultfiles2020-05AASLD-COVID19-ClinicalInsights-May42020
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
Fibroscan Not urgent but planning to
start June-July 2020 Huge back log Using radiology US protocol
for PPE (maskgoogles and gown) Flexible schedules based on
safety guidelines
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

13
Register Now for May 28th Webinar
AASLD-ALEH COVID-19 amp the Liver in the Americas
aasldorgcalendar
14
COVID-19 and the Liver Reentry and Return to a Pre-Pandemic State
o Webinar Contributorso Presenter Introductions ndash Dr Kimberly Brown
o Housekeeping Itemso OpenSAFELY Study ndash Dr Kimberly Brown
o Expert Consensus Panel Update ndash Dr Oren Fixo Outpatient ndash Dr Bilal Hameedo Inpatient ndash Dr Patricia Harreno Transplant ndash Dr David Mulligan
o Panel Discussion QampA
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 15
Webinar Agenda
o Co-chair Oren K Fix MD MSc FAASLD Swedish Medical Center (Washington)
o Co-chair Elizabeth C Verna MD MS Columbia University (New York)
o Kimberly Brown MD Henry Ford Health System (Michigan)
o Jaime Chu MD Icahn School of Medicine at Mount Sinai (New York)
o Bilal Hameed MD University of California (California)
o Laura M Kulik MD Northwestern Medical Faculty Foundation (Illinois)
o Ryan M Kwok MD Uniformed Services University (Maryland)
o Brendan M McGuire MD University of Alabama (Alabama)
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 16
o Jennifer Price MD MBA FACP University of California San Francisco (California)
o Daniel S Pratt MD FAASLD Massachusetts General Hospital (Massachusetts)
o Nancy S Reau MD Rush University (Illinois)
o Mark W Russo MD MPH FAASLD Carolinas Medical Center (North Carolina)
o Michael Schilsky MD FAASLD Yale University (Connecticut)
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC (California)
o Andrew Reynolds (Patient Advocate)o Raymond Chung and K Rajender Reddy
(ex-officio)
Clinical Oversight amp Publications Subcommittee
Submit your questions in the QampA box at the top or bottom of your screen
Questions will be answered at the end of the presentation
Webinar QampA
Webinar ModeratorKimberly Ann Brown MD
FAASLDChief Division of
Gastroenterology amp Hepatology
Henry Ford Health System
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 18
Webinar PresenterBilal Hameed MD
Associate Professor of Medicine and the Hepatology Clinic Chief
University of California San Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 19
Webinar PresenterPatricia Harren DNP DCC
Clinical Director of the Center for Liver Disease amp Transplantation Clinical Director for Pediatric Transplantation
amp Adult Abdominal Organ Transplantation
Columbia University
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 20
Webinar PresenterDavid C Mulligan MD FAASLDProfessor of Surgery and Chief
of Transplantation and Immunology
Yale University Yale New Haven Health System
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 21
o Oren K Fix MD MSc FAASLD Swedish Medical Center (Washington)
o Elizabeth C Verna MD MS Columbia University (New York)
o Jaime Chu MD Icahn School of Medicine at Mount Sinai (New York)
o Karen Hoyt BA Patient Advocate
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 22
o Guadalupe Garcia-Tsao MD FAASLD Yale University (Connecticut)
o Ryutaro Hirose MD University of California San Francisco (California)
o K Gautham Reddy MD FAASLD University of Chicago Medical Center (Illinois)
Webinar Panelist
o OpenSAFELY Factors associated with COVID-19-related hospital deaths in the linked electronic health records of 17 million adult NHS patientsbull 17425445 adultsbull Feb 1 2020 to April 25 2020bull Primary outcome death in hospital in patients with confirmed
COVID-19 (5683 deaths)
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
httpsdoiorg1011012020050620092999
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
httpsdoiorg1011012020050620092999
HR adjusted for all other factors listed other than ethnicity
o Largest cohort study to date evaluating a variety of clinical factors for death from COVID-19
o Asians and blacks appear to be at increased risk of in-hospital death with only partial attribution to pre-existing clinical risk factors or deprivation
o Patients with pre-existing liver disease transplantation or on immunosuppression appear to have increased risk of in-hospital death when adjusted for agesex alone or fully adjusted
o Strengthsbull Largest cohort study to date representing 40 English populationbull Inclusion of variables including liver disease transplant for analysis
o Weaknessesbull Deaths related to patients with false-negative tests or died without testing would be missedbull Censoring patients at date of death from other causes or outside the hospital stopped 9
days short of study end bull Cohort limited to those practices using the EHR software SystmOne Some variable were
assumed absent if missing bull Characterization of ldquoliver diseaserdquo is general and not complete
o Further characterization of liver disease and potential risks due to etiology MELD etc will be helpful in future studies
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORGhttpsdoiorg1011012020050620092999
Expert Panel Consensus Statement
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 26
o First published online March 23rdo New update posted today
wwwaasldorgcovid19o Spanish and Portuguese
translations available onlineo Hepatology manuscript published
online
May 14th Update Major Changes
o Acknowledgement of possible link between COVID-19 and Kawasaki-like pediatric multisystem inflammatory syndrome
o Italian autopsy series describing involvement of hepatic vasculature including acute portal and sinusoidal thrombosis
o Introduction of SARS-CoV-2 antigen testing in addition to increasing availability of antibody testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 27
httpswwwhealthnygovpressreleases2020docs2020-05-06_covid19_pediatric_inflammatory_syndromepdfSonzogni et al Preprints 2020httpswwwfdagovnews-eventspress-announcementscoronavirus-covid-19-update-fda-authorizes-first-antigen-test-help-rapid-detection-virus-causes
May 14th Update Major Changes
o OpenSAFELY study from the UK chronic liver disease is a risk factor for in-hospital death from COVID-19
o Large US study also showed that chronic liver disease and cirrhosis are associated with higher COVID-19 mortality
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 28
Williamson et al MedRxiv 2020Singh and Khan Gastroenterol 2020
May 14th Update Major Changes
o Clarification that treatment of hepatitis B is not contraindicated in patients with or without COVID-19
o Recommendations regarding use of masks for patients and caregivers as well as providers in the clinic or hospital setting
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 29
May 14th Update Major Changes
o Evolving data on hydroxychloroquine suggesting it should no longer be used outside RCTs
o New data on triple therapy with lopinavir-ritonavir ribavirin and interferon-beta-1b showing more rapid viral clearance compared to lopinavir-ritonavir (phase 2 RCT)
o Reentry
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 30
Geleris et al N Eng J Med 2020Hung et al Lancet 2020
31
Impact of COVID-19 on Liver Disease Safe Outpatient Re-Entry Process
Bilal Hameed MDAssociate Professor of Medicine
Clinic Chief Hepatology University of California San Francisco
Outline
The COVID-19 effects on liver care Recommendations for re-entry and re-opening facilities Ambulatory re-entry and recovery challenges and plan
at UCSF Gradual re-entry of liver patients in the ambulatory
setting
The Untold Toll mdash The Pandemicrsquos Effects on Patients without COVID-19
httpswwwnejmorgdoifull101056NEJMms2009984query=featured_coronavirus
Patients with heart attacks strokes and even appendicitis vanish from
hospitals
The Pandemicrsquos Effects on Patients without COVID-1938 reduction in STEMI activations in the US
during COVID-19 pandemic
Garcia S et al Journal of the American College of Cardiology April 2020
Decrease in routine pediatric vaccination during COVID-19
httpswwwcdcgovmmwrvolumes69wr
Unexpected Consequences of the Pandemic
To expand capacity for COVID-19 patients on March 18th CMS recommended limiting non-essential care and procedures 8 week pause in usual care activities Fear of returning to care Change in patientrsquos perception of riskbenefit
Areas with lowstable incidence of COVID-19 CMS allowing non-emergent non-COVID-19 healthcare
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdf
COVID-19 Pandemic Impact on the Cirrhosis Care
Tapper EB et al Journal of Hepatology April 2020
COVID Surge
Loss of insurance
Outpatient Impact of COVID-19 Pandemic UCSF Experience Maximizing Appropriate Use of Video Visits during Re-entry
Prior State Current State Future State~20 of total visits were video visits
~95 of total visits are video visits
Appropriate mix of telehealth visits ~50
Continue expanding to -Patients that live far away -Post-ops amp post-discharge follow-up-Chronic disease management(NAFLDHBVHCV etc)-Free up clinic space
0
10000
20000
30000
40000
50000
60000
70000
End of April Double March volume
February 2 of all visits2nd largest video visit program in the
country among AMCs largest in California
End of March 60 of visits
UCSF Video Visits by Month (Jan 2015-April 2020)
0
100
200
300
400
500
600
700
800
900
Jul 2019 Aug Sep Oct Nov Dec Jan 2020 Feb Mar Apr
Able to see the same number of patients even during pandemic
Hepatology Video Visits by Month at UCSF
CMS Phase I Recommendations Re-opening Facilities for Non-emergent Non-COVID-19 Healthcare
In coordination with State and local public health officials evaluate the incidence and trends for COVID-19 in the area
Prioritize surgicalprocedural care and high-complexity chronic disease management and select preventive services
Consider establishing Non-COVID Care (NCC) zones that would screen all patients for symptoms of COVID-19
Sufficient resources should be available across phases of care including PPE healthy workforce testing capacity etc and without jeopardizing surge capacity
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdfhttpswwwwhitehousegovopeningamericacriteriahttpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
httpsdatasfgovorgstoriessdak2-gvuj
San Francisco COVID-19 Numbers
Ambulatory Re-entry and Recovery ndash Cascaded Principles
Ensure morbidity and mortality do not increase due to liver related illness and provide care in a safe manner
Continue to prioritize the health and safety of workforce Prioritize urgent patients Communicate consistently and transparently Invest appropriately in services and improvement efforts
Strategies to limit unnecessary exposure while continuing to provide high-quality care for our liver patients
bull Optimization and flexibility of schedules (hoursweekend)
bull Utilization of clinic spacebull Sustain telehealth bull Digital technology for symptoms
monitoring bull Staff redeployment
bull COVID symptoms check protocolbull Social distancing in clinicbull Masking and safety policiesbull Waiting rooms changesbull Visitor policies
bull Prioritize urgent patientsbull Back log data and referralsbull Pre-clinic communicationbull In clinic flow (Echeck in rooming
and check out policies)
bull Patient communication is the keybull Staff anxiety and stress reduction bull Focus on vulnerable populationbull Physician burn out and health needs bull Trainees re-entry and education
Staff and PatientSafety
Clinic Work Flows
Resource Utilization
Support and
Education
PatientCare
Ambulatory Recovery Challenges and PlanProviding Best Care While Living with COVID-19
Physical Distancing amp Safety Guidelines
Conversa Employee Screening Mychart Screener Apex texting for patients in
nearby waiting areas
Innovation and Improving Operations
Gradual Re-entry of Liver Patients in the Ambulatory Setting
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
Patient will be scheduled for modified evaluation with
Hepatology and social worker as video visit
Remainder of evaluation will be onsite when restrictions are lifted
1 Pre-clinicarrival COVID screening for patientscaregiver2 Universal masking
no
Re-entry of Liver Patients in Clinic June 2020
All new liver transplant evaluations and HCC diagnosis New decompensation or worsening symptoms Listed patients for transplant with decompensated cirrhosis Acute hepatitis or liver injury Early post transplant Patients with difficulty with telehealth
Re-entry of Liver Patients HCC Surveillance HCC surveillance should continue as close to schedule (an
arbitrary delay of 2 months were acceptable) Working on list of all delayed imaging and prioritizing them by
risk categoriesKnown HCC surveillance for treatment response elevated AFP
Key is working with Radiology (Options of imaging locally) Communication with patients and documentation is important No delay in HCC treatment (riskbenefits discussion)
httpswwwaasldorgsitesdefaultfiles2020-05AASLD-COVID19-ClinicalInsights-May42020
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
Fibroscan Not urgent but planning to
start June-July 2020 Huge back log Using radiology US protocol
for PPE (maskgoogles and gown) Flexible schedules based on
safety guidelines
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

14
COVID-19 and the Liver Reentry and Return to a Pre-Pandemic State
o Webinar Contributorso Presenter Introductions ndash Dr Kimberly Brown
o Housekeeping Itemso OpenSAFELY Study ndash Dr Kimberly Brown
o Expert Consensus Panel Update ndash Dr Oren Fixo Outpatient ndash Dr Bilal Hameedo Inpatient ndash Dr Patricia Harreno Transplant ndash Dr David Mulligan
o Panel Discussion QampA
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 15
Webinar Agenda
o Co-chair Oren K Fix MD MSc FAASLD Swedish Medical Center (Washington)
o Co-chair Elizabeth C Verna MD MS Columbia University (New York)
o Kimberly Brown MD Henry Ford Health System (Michigan)
o Jaime Chu MD Icahn School of Medicine at Mount Sinai (New York)
o Bilal Hameed MD University of California (California)
o Laura M Kulik MD Northwestern Medical Faculty Foundation (Illinois)
o Ryan M Kwok MD Uniformed Services University (Maryland)
o Brendan M McGuire MD University of Alabama (Alabama)
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 16
o Jennifer Price MD MBA FACP University of California San Francisco (California)
o Daniel S Pratt MD FAASLD Massachusetts General Hospital (Massachusetts)
o Nancy S Reau MD Rush University (Illinois)
o Mark W Russo MD MPH FAASLD Carolinas Medical Center (North Carolina)
o Michael Schilsky MD FAASLD Yale University (Connecticut)
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC (California)
o Andrew Reynolds (Patient Advocate)o Raymond Chung and K Rajender Reddy
(ex-officio)
Clinical Oversight amp Publications Subcommittee
Submit your questions in the QampA box at the top or bottom of your screen
Questions will be answered at the end of the presentation
Webinar QampA
Webinar ModeratorKimberly Ann Brown MD
FAASLDChief Division of
Gastroenterology amp Hepatology
Henry Ford Health System
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 18
Webinar PresenterBilal Hameed MD
Associate Professor of Medicine and the Hepatology Clinic Chief
University of California San Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 19
Webinar PresenterPatricia Harren DNP DCC
Clinical Director of the Center for Liver Disease amp Transplantation Clinical Director for Pediatric Transplantation
amp Adult Abdominal Organ Transplantation
Columbia University
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 20
Webinar PresenterDavid C Mulligan MD FAASLDProfessor of Surgery and Chief
of Transplantation and Immunology
Yale University Yale New Haven Health System
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 21
o Oren K Fix MD MSc FAASLD Swedish Medical Center (Washington)
o Elizabeth C Verna MD MS Columbia University (New York)
o Jaime Chu MD Icahn School of Medicine at Mount Sinai (New York)
o Karen Hoyt BA Patient Advocate
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 22
o Guadalupe Garcia-Tsao MD FAASLD Yale University (Connecticut)
o Ryutaro Hirose MD University of California San Francisco (California)
o K Gautham Reddy MD FAASLD University of Chicago Medical Center (Illinois)
Webinar Panelist
o OpenSAFELY Factors associated with COVID-19-related hospital deaths in the linked electronic health records of 17 million adult NHS patientsbull 17425445 adultsbull Feb 1 2020 to April 25 2020bull Primary outcome death in hospital in patients with confirmed
COVID-19 (5683 deaths)
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
httpsdoiorg1011012020050620092999
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
httpsdoiorg1011012020050620092999
HR adjusted for all other factors listed other than ethnicity
o Largest cohort study to date evaluating a variety of clinical factors for death from COVID-19
o Asians and blacks appear to be at increased risk of in-hospital death with only partial attribution to pre-existing clinical risk factors or deprivation
o Patients with pre-existing liver disease transplantation or on immunosuppression appear to have increased risk of in-hospital death when adjusted for agesex alone or fully adjusted
o Strengthsbull Largest cohort study to date representing 40 English populationbull Inclusion of variables including liver disease transplant for analysis
o Weaknessesbull Deaths related to patients with false-negative tests or died without testing would be missedbull Censoring patients at date of death from other causes or outside the hospital stopped 9
days short of study end bull Cohort limited to those practices using the EHR software SystmOne Some variable were
assumed absent if missing bull Characterization of ldquoliver diseaserdquo is general and not complete
o Further characterization of liver disease and potential risks due to etiology MELD etc will be helpful in future studies
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORGhttpsdoiorg1011012020050620092999
Expert Panel Consensus Statement
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 26
o First published online March 23rdo New update posted today
wwwaasldorgcovid19o Spanish and Portuguese
translations available onlineo Hepatology manuscript published
online
May 14th Update Major Changes
o Acknowledgement of possible link between COVID-19 and Kawasaki-like pediatric multisystem inflammatory syndrome
o Italian autopsy series describing involvement of hepatic vasculature including acute portal and sinusoidal thrombosis
o Introduction of SARS-CoV-2 antigen testing in addition to increasing availability of antibody testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 27
httpswwwhealthnygovpressreleases2020docs2020-05-06_covid19_pediatric_inflammatory_syndromepdfSonzogni et al Preprints 2020httpswwwfdagovnews-eventspress-announcementscoronavirus-covid-19-update-fda-authorizes-first-antigen-test-help-rapid-detection-virus-causes
May 14th Update Major Changes
o OpenSAFELY study from the UK chronic liver disease is a risk factor for in-hospital death from COVID-19
o Large US study also showed that chronic liver disease and cirrhosis are associated with higher COVID-19 mortality
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 28
Williamson et al MedRxiv 2020Singh and Khan Gastroenterol 2020
May 14th Update Major Changes
o Clarification that treatment of hepatitis B is not contraindicated in patients with or without COVID-19
o Recommendations regarding use of masks for patients and caregivers as well as providers in the clinic or hospital setting
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 29
May 14th Update Major Changes
o Evolving data on hydroxychloroquine suggesting it should no longer be used outside RCTs
o New data on triple therapy with lopinavir-ritonavir ribavirin and interferon-beta-1b showing more rapid viral clearance compared to lopinavir-ritonavir (phase 2 RCT)
o Reentry
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 30
Geleris et al N Eng J Med 2020Hung et al Lancet 2020
31
Impact of COVID-19 on Liver Disease Safe Outpatient Re-Entry Process
Bilal Hameed MDAssociate Professor of Medicine
Clinic Chief Hepatology University of California San Francisco
Outline
The COVID-19 effects on liver care Recommendations for re-entry and re-opening facilities Ambulatory re-entry and recovery challenges and plan
at UCSF Gradual re-entry of liver patients in the ambulatory
setting
The Untold Toll mdash The Pandemicrsquos Effects on Patients without COVID-19
httpswwwnejmorgdoifull101056NEJMms2009984query=featured_coronavirus
Patients with heart attacks strokes and even appendicitis vanish from
hospitals
The Pandemicrsquos Effects on Patients without COVID-1938 reduction in STEMI activations in the US
during COVID-19 pandemic
Garcia S et al Journal of the American College of Cardiology April 2020
Decrease in routine pediatric vaccination during COVID-19
httpswwwcdcgovmmwrvolumes69wr
Unexpected Consequences of the Pandemic
To expand capacity for COVID-19 patients on March 18th CMS recommended limiting non-essential care and procedures 8 week pause in usual care activities Fear of returning to care Change in patientrsquos perception of riskbenefit
Areas with lowstable incidence of COVID-19 CMS allowing non-emergent non-COVID-19 healthcare
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdf
COVID-19 Pandemic Impact on the Cirrhosis Care
Tapper EB et al Journal of Hepatology April 2020
COVID Surge
Loss of insurance
Outpatient Impact of COVID-19 Pandemic UCSF Experience Maximizing Appropriate Use of Video Visits during Re-entry
Prior State Current State Future State~20 of total visits were video visits
~95 of total visits are video visits
Appropriate mix of telehealth visits ~50
Continue expanding to -Patients that live far away -Post-ops amp post-discharge follow-up-Chronic disease management(NAFLDHBVHCV etc)-Free up clinic space
0
10000
20000
30000
40000
50000
60000
70000
End of April Double March volume
February 2 of all visits2nd largest video visit program in the
country among AMCs largest in California
End of March 60 of visits
UCSF Video Visits by Month (Jan 2015-April 2020)
0
100
200
300
400
500
600
700
800
900
Jul 2019 Aug Sep Oct Nov Dec Jan 2020 Feb Mar Apr
Able to see the same number of patients even during pandemic
Hepatology Video Visits by Month at UCSF
CMS Phase I Recommendations Re-opening Facilities for Non-emergent Non-COVID-19 Healthcare
In coordination with State and local public health officials evaluate the incidence and trends for COVID-19 in the area
Prioritize surgicalprocedural care and high-complexity chronic disease management and select preventive services
Consider establishing Non-COVID Care (NCC) zones that would screen all patients for symptoms of COVID-19
Sufficient resources should be available across phases of care including PPE healthy workforce testing capacity etc and without jeopardizing surge capacity
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdfhttpswwwwhitehousegovopeningamericacriteriahttpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
httpsdatasfgovorgstoriessdak2-gvuj
San Francisco COVID-19 Numbers
Ambulatory Re-entry and Recovery ndash Cascaded Principles
Ensure morbidity and mortality do not increase due to liver related illness and provide care in a safe manner
Continue to prioritize the health and safety of workforce Prioritize urgent patients Communicate consistently and transparently Invest appropriately in services and improvement efforts
Strategies to limit unnecessary exposure while continuing to provide high-quality care for our liver patients
bull Optimization and flexibility of schedules (hoursweekend)
bull Utilization of clinic spacebull Sustain telehealth bull Digital technology for symptoms
monitoring bull Staff redeployment
bull COVID symptoms check protocolbull Social distancing in clinicbull Masking and safety policiesbull Waiting rooms changesbull Visitor policies
bull Prioritize urgent patientsbull Back log data and referralsbull Pre-clinic communicationbull In clinic flow (Echeck in rooming
and check out policies)
bull Patient communication is the keybull Staff anxiety and stress reduction bull Focus on vulnerable populationbull Physician burn out and health needs bull Trainees re-entry and education
Staff and PatientSafety
Clinic Work Flows
Resource Utilization
Support and
Education
PatientCare
Ambulatory Recovery Challenges and PlanProviding Best Care While Living with COVID-19
Physical Distancing amp Safety Guidelines
Conversa Employee Screening Mychart Screener Apex texting for patients in
nearby waiting areas
Innovation and Improving Operations
Gradual Re-entry of Liver Patients in the Ambulatory Setting
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
Patient will be scheduled for modified evaluation with
Hepatology and social worker as video visit
Remainder of evaluation will be onsite when restrictions are lifted
1 Pre-clinicarrival COVID screening for patientscaregiver2 Universal masking
no
Re-entry of Liver Patients in Clinic June 2020
All new liver transplant evaluations and HCC diagnosis New decompensation or worsening symptoms Listed patients for transplant with decompensated cirrhosis Acute hepatitis or liver injury Early post transplant Patients with difficulty with telehealth
Re-entry of Liver Patients HCC Surveillance HCC surveillance should continue as close to schedule (an
arbitrary delay of 2 months were acceptable) Working on list of all delayed imaging and prioritizing them by
risk categoriesKnown HCC surveillance for treatment response elevated AFP
Key is working with Radiology (Options of imaging locally) Communication with patients and documentation is important No delay in HCC treatment (riskbenefits discussion)
httpswwwaasldorgsitesdefaultfiles2020-05AASLD-COVID19-ClinicalInsights-May42020
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
Fibroscan Not urgent but planning to
start June-July 2020 Huge back log Using radiology US protocol
for PPE (maskgoogles and gown) Flexible schedules based on
safety guidelines
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

o Webinar Contributorso Presenter Introductions ndash Dr Kimberly Brown
o Housekeeping Itemso OpenSAFELY Study ndash Dr Kimberly Brown
o Expert Consensus Panel Update ndash Dr Oren Fixo Outpatient ndash Dr Bilal Hameedo Inpatient ndash Dr Patricia Harreno Transplant ndash Dr David Mulligan
o Panel Discussion QampA
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 15
Webinar Agenda
o Co-chair Oren K Fix MD MSc FAASLD Swedish Medical Center (Washington)
o Co-chair Elizabeth C Verna MD MS Columbia University (New York)
o Kimberly Brown MD Henry Ford Health System (Michigan)
o Jaime Chu MD Icahn School of Medicine at Mount Sinai (New York)
o Bilal Hameed MD University of California (California)
o Laura M Kulik MD Northwestern Medical Faculty Foundation (Illinois)
o Ryan M Kwok MD Uniformed Services University (Maryland)
o Brendan M McGuire MD University of Alabama (Alabama)
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 16
o Jennifer Price MD MBA FACP University of California San Francisco (California)
o Daniel S Pratt MD FAASLD Massachusetts General Hospital (Massachusetts)
o Nancy S Reau MD Rush University (Illinois)
o Mark W Russo MD MPH FAASLD Carolinas Medical Center (North Carolina)
o Michael Schilsky MD FAASLD Yale University (Connecticut)
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC (California)
o Andrew Reynolds (Patient Advocate)o Raymond Chung and K Rajender Reddy
(ex-officio)
Clinical Oversight amp Publications Subcommittee
Submit your questions in the QampA box at the top or bottom of your screen
Questions will be answered at the end of the presentation
Webinar QampA
Webinar ModeratorKimberly Ann Brown MD
FAASLDChief Division of
Gastroenterology amp Hepatology
Henry Ford Health System
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 18
Webinar PresenterBilal Hameed MD
Associate Professor of Medicine and the Hepatology Clinic Chief
University of California San Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 19
Webinar PresenterPatricia Harren DNP DCC
Clinical Director of the Center for Liver Disease amp Transplantation Clinical Director for Pediatric Transplantation
amp Adult Abdominal Organ Transplantation
Columbia University
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 20
Webinar PresenterDavid C Mulligan MD FAASLDProfessor of Surgery and Chief
of Transplantation and Immunology
Yale University Yale New Haven Health System
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 21
o Oren K Fix MD MSc FAASLD Swedish Medical Center (Washington)
o Elizabeth C Verna MD MS Columbia University (New York)
o Jaime Chu MD Icahn School of Medicine at Mount Sinai (New York)
o Karen Hoyt BA Patient Advocate
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 22
o Guadalupe Garcia-Tsao MD FAASLD Yale University (Connecticut)
o Ryutaro Hirose MD University of California San Francisco (California)
o K Gautham Reddy MD FAASLD University of Chicago Medical Center (Illinois)
Webinar Panelist
o OpenSAFELY Factors associated with COVID-19-related hospital deaths in the linked electronic health records of 17 million adult NHS patientsbull 17425445 adultsbull Feb 1 2020 to April 25 2020bull Primary outcome death in hospital in patients with confirmed
COVID-19 (5683 deaths)
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
httpsdoiorg1011012020050620092999
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
httpsdoiorg1011012020050620092999
HR adjusted for all other factors listed other than ethnicity
o Largest cohort study to date evaluating a variety of clinical factors for death from COVID-19
o Asians and blacks appear to be at increased risk of in-hospital death with only partial attribution to pre-existing clinical risk factors or deprivation
o Patients with pre-existing liver disease transplantation or on immunosuppression appear to have increased risk of in-hospital death when adjusted for agesex alone or fully adjusted
o Strengthsbull Largest cohort study to date representing 40 English populationbull Inclusion of variables including liver disease transplant for analysis
o Weaknessesbull Deaths related to patients with false-negative tests or died without testing would be missedbull Censoring patients at date of death from other causes or outside the hospital stopped 9
days short of study end bull Cohort limited to those practices using the EHR software SystmOne Some variable were
assumed absent if missing bull Characterization of ldquoliver diseaserdquo is general and not complete
o Further characterization of liver disease and potential risks due to etiology MELD etc will be helpful in future studies
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORGhttpsdoiorg1011012020050620092999
Expert Panel Consensus Statement
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 26
o First published online March 23rdo New update posted today
wwwaasldorgcovid19o Spanish and Portuguese
translations available onlineo Hepatology manuscript published
online
May 14th Update Major Changes
o Acknowledgement of possible link between COVID-19 and Kawasaki-like pediatric multisystem inflammatory syndrome
o Italian autopsy series describing involvement of hepatic vasculature including acute portal and sinusoidal thrombosis
o Introduction of SARS-CoV-2 antigen testing in addition to increasing availability of antibody testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 27
httpswwwhealthnygovpressreleases2020docs2020-05-06_covid19_pediatric_inflammatory_syndromepdfSonzogni et al Preprints 2020httpswwwfdagovnews-eventspress-announcementscoronavirus-covid-19-update-fda-authorizes-first-antigen-test-help-rapid-detection-virus-causes
May 14th Update Major Changes
o OpenSAFELY study from the UK chronic liver disease is a risk factor for in-hospital death from COVID-19
o Large US study also showed that chronic liver disease and cirrhosis are associated with higher COVID-19 mortality
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 28
Williamson et al MedRxiv 2020Singh and Khan Gastroenterol 2020
May 14th Update Major Changes
o Clarification that treatment of hepatitis B is not contraindicated in patients with or without COVID-19
o Recommendations regarding use of masks for patients and caregivers as well as providers in the clinic or hospital setting
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 29
May 14th Update Major Changes
o Evolving data on hydroxychloroquine suggesting it should no longer be used outside RCTs
o New data on triple therapy with lopinavir-ritonavir ribavirin and interferon-beta-1b showing more rapid viral clearance compared to lopinavir-ritonavir (phase 2 RCT)
o Reentry
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 30
Geleris et al N Eng J Med 2020Hung et al Lancet 2020
31
Impact of COVID-19 on Liver Disease Safe Outpatient Re-Entry Process
Bilal Hameed MDAssociate Professor of Medicine
Clinic Chief Hepatology University of California San Francisco
Outline
The COVID-19 effects on liver care Recommendations for re-entry and re-opening facilities Ambulatory re-entry and recovery challenges and plan
at UCSF Gradual re-entry of liver patients in the ambulatory
setting
The Untold Toll mdash The Pandemicrsquos Effects on Patients without COVID-19
httpswwwnejmorgdoifull101056NEJMms2009984query=featured_coronavirus
Patients with heart attacks strokes and even appendicitis vanish from
hospitals
The Pandemicrsquos Effects on Patients without COVID-1938 reduction in STEMI activations in the US
during COVID-19 pandemic
Garcia S et al Journal of the American College of Cardiology April 2020
Decrease in routine pediatric vaccination during COVID-19
httpswwwcdcgovmmwrvolumes69wr
Unexpected Consequences of the Pandemic
To expand capacity for COVID-19 patients on March 18th CMS recommended limiting non-essential care and procedures 8 week pause in usual care activities Fear of returning to care Change in patientrsquos perception of riskbenefit
Areas with lowstable incidence of COVID-19 CMS allowing non-emergent non-COVID-19 healthcare
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdf
COVID-19 Pandemic Impact on the Cirrhosis Care
Tapper EB et al Journal of Hepatology April 2020
COVID Surge
Loss of insurance
Outpatient Impact of COVID-19 Pandemic UCSF Experience Maximizing Appropriate Use of Video Visits during Re-entry
Prior State Current State Future State~20 of total visits were video visits
~95 of total visits are video visits
Appropriate mix of telehealth visits ~50
Continue expanding to -Patients that live far away -Post-ops amp post-discharge follow-up-Chronic disease management(NAFLDHBVHCV etc)-Free up clinic space
0
10000
20000
30000
40000
50000
60000
70000
End of April Double March volume
February 2 of all visits2nd largest video visit program in the
country among AMCs largest in California
End of March 60 of visits
UCSF Video Visits by Month (Jan 2015-April 2020)
0
100
200
300
400
500
600
700
800
900
Jul 2019 Aug Sep Oct Nov Dec Jan 2020 Feb Mar Apr
Able to see the same number of patients even during pandemic
Hepatology Video Visits by Month at UCSF
CMS Phase I Recommendations Re-opening Facilities for Non-emergent Non-COVID-19 Healthcare
In coordination with State and local public health officials evaluate the incidence and trends for COVID-19 in the area
Prioritize surgicalprocedural care and high-complexity chronic disease management and select preventive services
Consider establishing Non-COVID Care (NCC) zones that would screen all patients for symptoms of COVID-19
Sufficient resources should be available across phases of care including PPE healthy workforce testing capacity etc and without jeopardizing surge capacity
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdfhttpswwwwhitehousegovopeningamericacriteriahttpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
httpsdatasfgovorgstoriessdak2-gvuj
San Francisco COVID-19 Numbers
Ambulatory Re-entry and Recovery ndash Cascaded Principles
Ensure morbidity and mortality do not increase due to liver related illness and provide care in a safe manner
Continue to prioritize the health and safety of workforce Prioritize urgent patients Communicate consistently and transparently Invest appropriately in services and improvement efforts
Strategies to limit unnecessary exposure while continuing to provide high-quality care for our liver patients
bull Optimization and flexibility of schedules (hoursweekend)
bull Utilization of clinic spacebull Sustain telehealth bull Digital technology for symptoms
monitoring bull Staff redeployment
bull COVID symptoms check protocolbull Social distancing in clinicbull Masking and safety policiesbull Waiting rooms changesbull Visitor policies
bull Prioritize urgent patientsbull Back log data and referralsbull Pre-clinic communicationbull In clinic flow (Echeck in rooming
and check out policies)
bull Patient communication is the keybull Staff anxiety and stress reduction bull Focus on vulnerable populationbull Physician burn out and health needs bull Trainees re-entry and education
Staff and PatientSafety
Clinic Work Flows
Resource Utilization
Support and
Education
PatientCare
Ambulatory Recovery Challenges and PlanProviding Best Care While Living with COVID-19
Physical Distancing amp Safety Guidelines
Conversa Employee Screening Mychart Screener Apex texting for patients in
nearby waiting areas
Innovation and Improving Operations
Gradual Re-entry of Liver Patients in the Ambulatory Setting
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
Patient will be scheduled for modified evaluation with
Hepatology and social worker as video visit
Remainder of evaluation will be onsite when restrictions are lifted
1 Pre-clinicarrival COVID screening for patientscaregiver2 Universal masking
no
Re-entry of Liver Patients in Clinic June 2020
All new liver transplant evaluations and HCC diagnosis New decompensation or worsening symptoms Listed patients for transplant with decompensated cirrhosis Acute hepatitis or liver injury Early post transplant Patients with difficulty with telehealth
Re-entry of Liver Patients HCC Surveillance HCC surveillance should continue as close to schedule (an
arbitrary delay of 2 months were acceptable) Working on list of all delayed imaging and prioritizing them by
risk categoriesKnown HCC surveillance for treatment response elevated AFP
Key is working with Radiology (Options of imaging locally) Communication with patients and documentation is important No delay in HCC treatment (riskbenefits discussion)
httpswwwaasldorgsitesdefaultfiles2020-05AASLD-COVID19-ClinicalInsights-May42020
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
Fibroscan Not urgent but planning to
start June-July 2020 Huge back log Using radiology US protocol
for PPE (maskgoogles and gown) Flexible schedules based on
safety guidelines
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

o Co-chair Oren K Fix MD MSc FAASLD Swedish Medical Center (Washington)
o Co-chair Elizabeth C Verna MD MS Columbia University (New York)
o Kimberly Brown MD Henry Ford Health System (Michigan)
o Jaime Chu MD Icahn School of Medicine at Mount Sinai (New York)
o Bilal Hameed MD University of California (California)
o Laura M Kulik MD Northwestern Medical Faculty Foundation (Illinois)
o Ryan M Kwok MD Uniformed Services University (Maryland)
o Brendan M McGuire MD University of Alabama (Alabama)
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 16
o Jennifer Price MD MBA FACP University of California San Francisco (California)
o Daniel S Pratt MD FAASLD Massachusetts General Hospital (Massachusetts)
o Nancy S Reau MD Rush University (Illinois)
o Mark W Russo MD MPH FAASLD Carolinas Medical Center (North Carolina)
o Michael Schilsky MD FAASLD Yale University (Connecticut)
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC (California)
o Andrew Reynolds (Patient Advocate)o Raymond Chung and K Rajender Reddy
(ex-officio)
Clinical Oversight amp Publications Subcommittee
Submit your questions in the QampA box at the top or bottom of your screen
Questions will be answered at the end of the presentation
Webinar QampA
Webinar ModeratorKimberly Ann Brown MD
FAASLDChief Division of
Gastroenterology amp Hepatology
Henry Ford Health System
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 18
Webinar PresenterBilal Hameed MD
Associate Professor of Medicine and the Hepatology Clinic Chief
University of California San Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 19
Webinar PresenterPatricia Harren DNP DCC
Clinical Director of the Center for Liver Disease amp Transplantation Clinical Director for Pediatric Transplantation
amp Adult Abdominal Organ Transplantation
Columbia University
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 20
Webinar PresenterDavid C Mulligan MD FAASLDProfessor of Surgery and Chief
of Transplantation and Immunology
Yale University Yale New Haven Health System
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 21
o Oren K Fix MD MSc FAASLD Swedish Medical Center (Washington)
o Elizabeth C Verna MD MS Columbia University (New York)
o Jaime Chu MD Icahn School of Medicine at Mount Sinai (New York)
o Karen Hoyt BA Patient Advocate
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 22
o Guadalupe Garcia-Tsao MD FAASLD Yale University (Connecticut)
o Ryutaro Hirose MD University of California San Francisco (California)
o K Gautham Reddy MD FAASLD University of Chicago Medical Center (Illinois)
Webinar Panelist
o OpenSAFELY Factors associated with COVID-19-related hospital deaths in the linked electronic health records of 17 million adult NHS patientsbull 17425445 adultsbull Feb 1 2020 to April 25 2020bull Primary outcome death in hospital in patients with confirmed
COVID-19 (5683 deaths)
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
httpsdoiorg1011012020050620092999
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
httpsdoiorg1011012020050620092999
HR adjusted for all other factors listed other than ethnicity
o Largest cohort study to date evaluating a variety of clinical factors for death from COVID-19
o Asians and blacks appear to be at increased risk of in-hospital death with only partial attribution to pre-existing clinical risk factors or deprivation
o Patients with pre-existing liver disease transplantation or on immunosuppression appear to have increased risk of in-hospital death when adjusted for agesex alone or fully adjusted
o Strengthsbull Largest cohort study to date representing 40 English populationbull Inclusion of variables including liver disease transplant for analysis
o Weaknessesbull Deaths related to patients with false-negative tests or died without testing would be missedbull Censoring patients at date of death from other causes or outside the hospital stopped 9
days short of study end bull Cohort limited to those practices using the EHR software SystmOne Some variable were
assumed absent if missing bull Characterization of ldquoliver diseaserdquo is general and not complete
o Further characterization of liver disease and potential risks due to etiology MELD etc will be helpful in future studies
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORGhttpsdoiorg1011012020050620092999
Expert Panel Consensus Statement
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 26
o First published online March 23rdo New update posted today
wwwaasldorgcovid19o Spanish and Portuguese
translations available onlineo Hepatology manuscript published
online
May 14th Update Major Changes
o Acknowledgement of possible link between COVID-19 and Kawasaki-like pediatric multisystem inflammatory syndrome
o Italian autopsy series describing involvement of hepatic vasculature including acute portal and sinusoidal thrombosis
o Introduction of SARS-CoV-2 antigen testing in addition to increasing availability of antibody testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 27
httpswwwhealthnygovpressreleases2020docs2020-05-06_covid19_pediatric_inflammatory_syndromepdfSonzogni et al Preprints 2020httpswwwfdagovnews-eventspress-announcementscoronavirus-covid-19-update-fda-authorizes-first-antigen-test-help-rapid-detection-virus-causes
May 14th Update Major Changes
o OpenSAFELY study from the UK chronic liver disease is a risk factor for in-hospital death from COVID-19
o Large US study also showed that chronic liver disease and cirrhosis are associated with higher COVID-19 mortality
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 28
Williamson et al MedRxiv 2020Singh and Khan Gastroenterol 2020
May 14th Update Major Changes
o Clarification that treatment of hepatitis B is not contraindicated in patients with or without COVID-19
o Recommendations regarding use of masks for patients and caregivers as well as providers in the clinic or hospital setting
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 29
May 14th Update Major Changes
o Evolving data on hydroxychloroquine suggesting it should no longer be used outside RCTs
o New data on triple therapy with lopinavir-ritonavir ribavirin and interferon-beta-1b showing more rapid viral clearance compared to lopinavir-ritonavir (phase 2 RCT)
o Reentry
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 30
Geleris et al N Eng J Med 2020Hung et al Lancet 2020
31
Impact of COVID-19 on Liver Disease Safe Outpatient Re-Entry Process
Bilal Hameed MDAssociate Professor of Medicine
Clinic Chief Hepatology University of California San Francisco
Outline
The COVID-19 effects on liver care Recommendations for re-entry and re-opening facilities Ambulatory re-entry and recovery challenges and plan
at UCSF Gradual re-entry of liver patients in the ambulatory
setting
The Untold Toll mdash The Pandemicrsquos Effects on Patients without COVID-19
httpswwwnejmorgdoifull101056NEJMms2009984query=featured_coronavirus
Patients with heart attacks strokes and even appendicitis vanish from
hospitals
The Pandemicrsquos Effects on Patients without COVID-1938 reduction in STEMI activations in the US
during COVID-19 pandemic
Garcia S et al Journal of the American College of Cardiology April 2020
Decrease in routine pediatric vaccination during COVID-19
httpswwwcdcgovmmwrvolumes69wr
Unexpected Consequences of the Pandemic
To expand capacity for COVID-19 patients on March 18th CMS recommended limiting non-essential care and procedures 8 week pause in usual care activities Fear of returning to care Change in patientrsquos perception of riskbenefit
Areas with lowstable incidence of COVID-19 CMS allowing non-emergent non-COVID-19 healthcare
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdf
COVID-19 Pandemic Impact on the Cirrhosis Care
Tapper EB et al Journal of Hepatology April 2020
COVID Surge
Loss of insurance
Outpatient Impact of COVID-19 Pandemic UCSF Experience Maximizing Appropriate Use of Video Visits during Re-entry
Prior State Current State Future State~20 of total visits were video visits
~95 of total visits are video visits
Appropriate mix of telehealth visits ~50
Continue expanding to -Patients that live far away -Post-ops amp post-discharge follow-up-Chronic disease management(NAFLDHBVHCV etc)-Free up clinic space
0
10000
20000
30000
40000
50000
60000
70000
End of April Double March volume
February 2 of all visits2nd largest video visit program in the
country among AMCs largest in California
End of March 60 of visits
UCSF Video Visits by Month (Jan 2015-April 2020)
0
100
200
300
400
500
600
700
800
900
Jul 2019 Aug Sep Oct Nov Dec Jan 2020 Feb Mar Apr
Able to see the same number of patients even during pandemic
Hepatology Video Visits by Month at UCSF
CMS Phase I Recommendations Re-opening Facilities for Non-emergent Non-COVID-19 Healthcare
In coordination with State and local public health officials evaluate the incidence and trends for COVID-19 in the area
Prioritize surgicalprocedural care and high-complexity chronic disease management and select preventive services
Consider establishing Non-COVID Care (NCC) zones that would screen all patients for symptoms of COVID-19
Sufficient resources should be available across phases of care including PPE healthy workforce testing capacity etc and without jeopardizing surge capacity
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdfhttpswwwwhitehousegovopeningamericacriteriahttpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
httpsdatasfgovorgstoriessdak2-gvuj
San Francisco COVID-19 Numbers
Ambulatory Re-entry and Recovery ndash Cascaded Principles
Ensure morbidity and mortality do not increase due to liver related illness and provide care in a safe manner
Continue to prioritize the health and safety of workforce Prioritize urgent patients Communicate consistently and transparently Invest appropriately in services and improvement efforts
Strategies to limit unnecessary exposure while continuing to provide high-quality care for our liver patients
bull Optimization and flexibility of schedules (hoursweekend)
bull Utilization of clinic spacebull Sustain telehealth bull Digital technology for symptoms
monitoring bull Staff redeployment
bull COVID symptoms check protocolbull Social distancing in clinicbull Masking and safety policiesbull Waiting rooms changesbull Visitor policies
bull Prioritize urgent patientsbull Back log data and referralsbull Pre-clinic communicationbull In clinic flow (Echeck in rooming
and check out policies)
bull Patient communication is the keybull Staff anxiety and stress reduction bull Focus on vulnerable populationbull Physician burn out and health needs bull Trainees re-entry and education
Staff and PatientSafety
Clinic Work Flows
Resource Utilization
Support and
Education
PatientCare
Ambulatory Recovery Challenges and PlanProviding Best Care While Living with COVID-19
Physical Distancing amp Safety Guidelines
Conversa Employee Screening Mychart Screener Apex texting for patients in
nearby waiting areas
Innovation and Improving Operations
Gradual Re-entry of Liver Patients in the Ambulatory Setting
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
Patient will be scheduled for modified evaluation with
Hepatology and social worker as video visit
Remainder of evaluation will be onsite when restrictions are lifted
1 Pre-clinicarrival COVID screening for patientscaregiver2 Universal masking
no
Re-entry of Liver Patients in Clinic June 2020
All new liver transplant evaluations and HCC diagnosis New decompensation or worsening symptoms Listed patients for transplant with decompensated cirrhosis Acute hepatitis or liver injury Early post transplant Patients with difficulty with telehealth
Re-entry of Liver Patients HCC Surveillance HCC surveillance should continue as close to schedule (an
arbitrary delay of 2 months were acceptable) Working on list of all delayed imaging and prioritizing them by
risk categoriesKnown HCC surveillance for treatment response elevated AFP
Key is working with Radiology (Options of imaging locally) Communication with patients and documentation is important No delay in HCC treatment (riskbenefits discussion)
httpswwwaasldorgsitesdefaultfiles2020-05AASLD-COVID19-ClinicalInsights-May42020
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
Fibroscan Not urgent but planning to
start June-July 2020 Huge back log Using radiology US protocol
for PPE (maskgoogles and gown) Flexible schedules based on
safety guidelines
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

Submit your questions in the QampA box at the top or bottom of your screen
Questions will be answered at the end of the presentation
Webinar QampA
Webinar ModeratorKimberly Ann Brown MD
FAASLDChief Division of
Gastroenterology amp Hepatology
Henry Ford Health System
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 18
Webinar PresenterBilal Hameed MD
Associate Professor of Medicine and the Hepatology Clinic Chief
University of California San Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 19
Webinar PresenterPatricia Harren DNP DCC
Clinical Director of the Center for Liver Disease amp Transplantation Clinical Director for Pediatric Transplantation
amp Adult Abdominal Organ Transplantation
Columbia University
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 20
Webinar PresenterDavid C Mulligan MD FAASLDProfessor of Surgery and Chief
of Transplantation and Immunology
Yale University Yale New Haven Health System
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 21
o Oren K Fix MD MSc FAASLD Swedish Medical Center (Washington)
o Elizabeth C Verna MD MS Columbia University (New York)
o Jaime Chu MD Icahn School of Medicine at Mount Sinai (New York)
o Karen Hoyt BA Patient Advocate
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 22
o Guadalupe Garcia-Tsao MD FAASLD Yale University (Connecticut)
o Ryutaro Hirose MD University of California San Francisco (California)
o K Gautham Reddy MD FAASLD University of Chicago Medical Center (Illinois)
Webinar Panelist
o OpenSAFELY Factors associated with COVID-19-related hospital deaths in the linked electronic health records of 17 million adult NHS patientsbull 17425445 adultsbull Feb 1 2020 to April 25 2020bull Primary outcome death in hospital in patients with confirmed
COVID-19 (5683 deaths)
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
httpsdoiorg1011012020050620092999
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
httpsdoiorg1011012020050620092999
HR adjusted for all other factors listed other than ethnicity
o Largest cohort study to date evaluating a variety of clinical factors for death from COVID-19
o Asians and blacks appear to be at increased risk of in-hospital death with only partial attribution to pre-existing clinical risk factors or deprivation
o Patients with pre-existing liver disease transplantation or on immunosuppression appear to have increased risk of in-hospital death when adjusted for agesex alone or fully adjusted
o Strengthsbull Largest cohort study to date representing 40 English populationbull Inclusion of variables including liver disease transplant for analysis
o Weaknessesbull Deaths related to patients with false-negative tests or died without testing would be missedbull Censoring patients at date of death from other causes or outside the hospital stopped 9
days short of study end bull Cohort limited to those practices using the EHR software SystmOne Some variable were
assumed absent if missing bull Characterization of ldquoliver diseaserdquo is general and not complete
o Further characterization of liver disease and potential risks due to etiology MELD etc will be helpful in future studies
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORGhttpsdoiorg1011012020050620092999
Expert Panel Consensus Statement
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 26
o First published online March 23rdo New update posted today
wwwaasldorgcovid19o Spanish and Portuguese
translations available onlineo Hepatology manuscript published
online
May 14th Update Major Changes
o Acknowledgement of possible link between COVID-19 and Kawasaki-like pediatric multisystem inflammatory syndrome
o Italian autopsy series describing involvement of hepatic vasculature including acute portal and sinusoidal thrombosis
o Introduction of SARS-CoV-2 antigen testing in addition to increasing availability of antibody testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 27
httpswwwhealthnygovpressreleases2020docs2020-05-06_covid19_pediatric_inflammatory_syndromepdfSonzogni et al Preprints 2020httpswwwfdagovnews-eventspress-announcementscoronavirus-covid-19-update-fda-authorizes-first-antigen-test-help-rapid-detection-virus-causes
May 14th Update Major Changes
o OpenSAFELY study from the UK chronic liver disease is a risk factor for in-hospital death from COVID-19
o Large US study also showed that chronic liver disease and cirrhosis are associated with higher COVID-19 mortality
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 28
Williamson et al MedRxiv 2020Singh and Khan Gastroenterol 2020
May 14th Update Major Changes
o Clarification that treatment of hepatitis B is not contraindicated in patients with or without COVID-19
o Recommendations regarding use of masks for patients and caregivers as well as providers in the clinic or hospital setting
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 29
May 14th Update Major Changes
o Evolving data on hydroxychloroquine suggesting it should no longer be used outside RCTs
o New data on triple therapy with lopinavir-ritonavir ribavirin and interferon-beta-1b showing more rapid viral clearance compared to lopinavir-ritonavir (phase 2 RCT)
o Reentry
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 30
Geleris et al N Eng J Med 2020Hung et al Lancet 2020
31
Impact of COVID-19 on Liver Disease Safe Outpatient Re-Entry Process
Bilal Hameed MDAssociate Professor of Medicine
Clinic Chief Hepatology University of California San Francisco
Outline
The COVID-19 effects on liver care Recommendations for re-entry and re-opening facilities Ambulatory re-entry and recovery challenges and plan
at UCSF Gradual re-entry of liver patients in the ambulatory
setting
The Untold Toll mdash The Pandemicrsquos Effects on Patients without COVID-19
httpswwwnejmorgdoifull101056NEJMms2009984query=featured_coronavirus
Patients with heart attacks strokes and even appendicitis vanish from
hospitals
The Pandemicrsquos Effects on Patients without COVID-1938 reduction in STEMI activations in the US
during COVID-19 pandemic
Garcia S et al Journal of the American College of Cardiology April 2020
Decrease in routine pediatric vaccination during COVID-19
httpswwwcdcgovmmwrvolumes69wr
Unexpected Consequences of the Pandemic
To expand capacity for COVID-19 patients on March 18th CMS recommended limiting non-essential care and procedures 8 week pause in usual care activities Fear of returning to care Change in patientrsquos perception of riskbenefit
Areas with lowstable incidence of COVID-19 CMS allowing non-emergent non-COVID-19 healthcare
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdf
COVID-19 Pandemic Impact on the Cirrhosis Care
Tapper EB et al Journal of Hepatology April 2020
COVID Surge
Loss of insurance
Outpatient Impact of COVID-19 Pandemic UCSF Experience Maximizing Appropriate Use of Video Visits during Re-entry
Prior State Current State Future State~20 of total visits were video visits
~95 of total visits are video visits
Appropriate mix of telehealth visits ~50
Continue expanding to -Patients that live far away -Post-ops amp post-discharge follow-up-Chronic disease management(NAFLDHBVHCV etc)-Free up clinic space
0
10000
20000
30000
40000
50000
60000
70000
End of April Double March volume
February 2 of all visits2nd largest video visit program in the
country among AMCs largest in California
End of March 60 of visits
UCSF Video Visits by Month (Jan 2015-April 2020)
0
100
200
300
400
500
600
700
800
900
Jul 2019 Aug Sep Oct Nov Dec Jan 2020 Feb Mar Apr
Able to see the same number of patients even during pandemic
Hepatology Video Visits by Month at UCSF
CMS Phase I Recommendations Re-opening Facilities for Non-emergent Non-COVID-19 Healthcare
In coordination with State and local public health officials evaluate the incidence and trends for COVID-19 in the area
Prioritize surgicalprocedural care and high-complexity chronic disease management and select preventive services
Consider establishing Non-COVID Care (NCC) zones that would screen all patients for symptoms of COVID-19
Sufficient resources should be available across phases of care including PPE healthy workforce testing capacity etc and without jeopardizing surge capacity
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdfhttpswwwwhitehousegovopeningamericacriteriahttpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
httpsdatasfgovorgstoriessdak2-gvuj
San Francisco COVID-19 Numbers
Ambulatory Re-entry and Recovery ndash Cascaded Principles
Ensure morbidity and mortality do not increase due to liver related illness and provide care in a safe manner
Continue to prioritize the health and safety of workforce Prioritize urgent patients Communicate consistently and transparently Invest appropriately in services and improvement efforts
Strategies to limit unnecessary exposure while continuing to provide high-quality care for our liver patients
bull Optimization and flexibility of schedules (hoursweekend)
bull Utilization of clinic spacebull Sustain telehealth bull Digital technology for symptoms
monitoring bull Staff redeployment
bull COVID symptoms check protocolbull Social distancing in clinicbull Masking and safety policiesbull Waiting rooms changesbull Visitor policies
bull Prioritize urgent patientsbull Back log data and referralsbull Pre-clinic communicationbull In clinic flow (Echeck in rooming
and check out policies)
bull Patient communication is the keybull Staff anxiety and stress reduction bull Focus on vulnerable populationbull Physician burn out and health needs bull Trainees re-entry and education
Staff and PatientSafety
Clinic Work Flows
Resource Utilization
Support and
Education
PatientCare
Ambulatory Recovery Challenges and PlanProviding Best Care While Living with COVID-19
Physical Distancing amp Safety Guidelines
Conversa Employee Screening Mychart Screener Apex texting for patients in
nearby waiting areas
Innovation and Improving Operations
Gradual Re-entry of Liver Patients in the Ambulatory Setting
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
Patient will be scheduled for modified evaluation with
Hepatology and social worker as video visit
Remainder of evaluation will be onsite when restrictions are lifted
1 Pre-clinicarrival COVID screening for patientscaregiver2 Universal masking
no
Re-entry of Liver Patients in Clinic June 2020
All new liver transplant evaluations and HCC diagnosis New decompensation or worsening symptoms Listed patients for transplant with decompensated cirrhosis Acute hepatitis or liver injury Early post transplant Patients with difficulty with telehealth
Re-entry of Liver Patients HCC Surveillance HCC surveillance should continue as close to schedule (an
arbitrary delay of 2 months were acceptable) Working on list of all delayed imaging and prioritizing them by
risk categoriesKnown HCC surveillance for treatment response elevated AFP
Key is working with Radiology (Options of imaging locally) Communication with patients and documentation is important No delay in HCC treatment (riskbenefits discussion)
httpswwwaasldorgsitesdefaultfiles2020-05AASLD-COVID19-ClinicalInsights-May42020
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
Fibroscan Not urgent but planning to
start June-July 2020 Huge back log Using radiology US protocol
for PPE (maskgoogles and gown) Flexible schedules based on
safety guidelines
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

Webinar ModeratorKimberly Ann Brown MD
FAASLDChief Division of
Gastroenterology amp Hepatology
Henry Ford Health System
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 18
Webinar PresenterBilal Hameed MD
Associate Professor of Medicine and the Hepatology Clinic Chief
University of California San Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 19
Webinar PresenterPatricia Harren DNP DCC
Clinical Director of the Center for Liver Disease amp Transplantation Clinical Director for Pediatric Transplantation
amp Adult Abdominal Organ Transplantation
Columbia University
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 20
Webinar PresenterDavid C Mulligan MD FAASLDProfessor of Surgery and Chief
of Transplantation and Immunology
Yale University Yale New Haven Health System
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 21
o Oren K Fix MD MSc FAASLD Swedish Medical Center (Washington)
o Elizabeth C Verna MD MS Columbia University (New York)
o Jaime Chu MD Icahn School of Medicine at Mount Sinai (New York)
o Karen Hoyt BA Patient Advocate
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 22
o Guadalupe Garcia-Tsao MD FAASLD Yale University (Connecticut)
o Ryutaro Hirose MD University of California San Francisco (California)
o K Gautham Reddy MD FAASLD University of Chicago Medical Center (Illinois)
Webinar Panelist
o OpenSAFELY Factors associated with COVID-19-related hospital deaths in the linked electronic health records of 17 million adult NHS patientsbull 17425445 adultsbull Feb 1 2020 to April 25 2020bull Primary outcome death in hospital in patients with confirmed
COVID-19 (5683 deaths)
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
httpsdoiorg1011012020050620092999
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
httpsdoiorg1011012020050620092999
HR adjusted for all other factors listed other than ethnicity
o Largest cohort study to date evaluating a variety of clinical factors for death from COVID-19
o Asians and blacks appear to be at increased risk of in-hospital death with only partial attribution to pre-existing clinical risk factors or deprivation
o Patients with pre-existing liver disease transplantation or on immunosuppression appear to have increased risk of in-hospital death when adjusted for agesex alone or fully adjusted
o Strengthsbull Largest cohort study to date representing 40 English populationbull Inclusion of variables including liver disease transplant for analysis
o Weaknessesbull Deaths related to patients with false-negative tests or died without testing would be missedbull Censoring patients at date of death from other causes or outside the hospital stopped 9
days short of study end bull Cohort limited to those practices using the EHR software SystmOne Some variable were
assumed absent if missing bull Characterization of ldquoliver diseaserdquo is general and not complete
o Further characterization of liver disease and potential risks due to etiology MELD etc will be helpful in future studies
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORGhttpsdoiorg1011012020050620092999
Expert Panel Consensus Statement
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 26
o First published online March 23rdo New update posted today
wwwaasldorgcovid19o Spanish and Portuguese
translations available onlineo Hepatology manuscript published
online
May 14th Update Major Changes
o Acknowledgement of possible link between COVID-19 and Kawasaki-like pediatric multisystem inflammatory syndrome
o Italian autopsy series describing involvement of hepatic vasculature including acute portal and sinusoidal thrombosis
o Introduction of SARS-CoV-2 antigen testing in addition to increasing availability of antibody testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 27
httpswwwhealthnygovpressreleases2020docs2020-05-06_covid19_pediatric_inflammatory_syndromepdfSonzogni et al Preprints 2020httpswwwfdagovnews-eventspress-announcementscoronavirus-covid-19-update-fda-authorizes-first-antigen-test-help-rapid-detection-virus-causes
May 14th Update Major Changes
o OpenSAFELY study from the UK chronic liver disease is a risk factor for in-hospital death from COVID-19
o Large US study also showed that chronic liver disease and cirrhosis are associated with higher COVID-19 mortality
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 28
Williamson et al MedRxiv 2020Singh and Khan Gastroenterol 2020
May 14th Update Major Changes
o Clarification that treatment of hepatitis B is not contraindicated in patients with or without COVID-19
o Recommendations regarding use of masks for patients and caregivers as well as providers in the clinic or hospital setting
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 29
May 14th Update Major Changes
o Evolving data on hydroxychloroquine suggesting it should no longer be used outside RCTs
o New data on triple therapy with lopinavir-ritonavir ribavirin and interferon-beta-1b showing more rapid viral clearance compared to lopinavir-ritonavir (phase 2 RCT)
o Reentry
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 30
Geleris et al N Eng J Med 2020Hung et al Lancet 2020
31
Impact of COVID-19 on Liver Disease Safe Outpatient Re-Entry Process
Bilal Hameed MDAssociate Professor of Medicine
Clinic Chief Hepatology University of California San Francisco
Outline
The COVID-19 effects on liver care Recommendations for re-entry and re-opening facilities Ambulatory re-entry and recovery challenges and plan
at UCSF Gradual re-entry of liver patients in the ambulatory
setting
The Untold Toll mdash The Pandemicrsquos Effects on Patients without COVID-19
httpswwwnejmorgdoifull101056NEJMms2009984query=featured_coronavirus
Patients with heart attacks strokes and even appendicitis vanish from
hospitals
The Pandemicrsquos Effects on Patients without COVID-1938 reduction in STEMI activations in the US
during COVID-19 pandemic
Garcia S et al Journal of the American College of Cardiology April 2020
Decrease in routine pediatric vaccination during COVID-19
httpswwwcdcgovmmwrvolumes69wr
Unexpected Consequences of the Pandemic
To expand capacity for COVID-19 patients on March 18th CMS recommended limiting non-essential care and procedures 8 week pause in usual care activities Fear of returning to care Change in patientrsquos perception of riskbenefit
Areas with lowstable incidence of COVID-19 CMS allowing non-emergent non-COVID-19 healthcare
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdf
COVID-19 Pandemic Impact on the Cirrhosis Care
Tapper EB et al Journal of Hepatology April 2020
COVID Surge
Loss of insurance
Outpatient Impact of COVID-19 Pandemic UCSF Experience Maximizing Appropriate Use of Video Visits during Re-entry
Prior State Current State Future State~20 of total visits were video visits
~95 of total visits are video visits
Appropriate mix of telehealth visits ~50
Continue expanding to -Patients that live far away -Post-ops amp post-discharge follow-up-Chronic disease management(NAFLDHBVHCV etc)-Free up clinic space
0
10000
20000
30000
40000
50000
60000
70000
End of April Double March volume
February 2 of all visits2nd largest video visit program in the
country among AMCs largest in California
End of March 60 of visits
UCSF Video Visits by Month (Jan 2015-April 2020)
0
100
200
300
400
500
600
700
800
900
Jul 2019 Aug Sep Oct Nov Dec Jan 2020 Feb Mar Apr
Able to see the same number of patients even during pandemic
Hepatology Video Visits by Month at UCSF
CMS Phase I Recommendations Re-opening Facilities for Non-emergent Non-COVID-19 Healthcare
In coordination with State and local public health officials evaluate the incidence and trends for COVID-19 in the area
Prioritize surgicalprocedural care and high-complexity chronic disease management and select preventive services
Consider establishing Non-COVID Care (NCC) zones that would screen all patients for symptoms of COVID-19
Sufficient resources should be available across phases of care including PPE healthy workforce testing capacity etc and without jeopardizing surge capacity
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdfhttpswwwwhitehousegovopeningamericacriteriahttpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
httpsdatasfgovorgstoriessdak2-gvuj
San Francisco COVID-19 Numbers
Ambulatory Re-entry and Recovery ndash Cascaded Principles
Ensure morbidity and mortality do not increase due to liver related illness and provide care in a safe manner
Continue to prioritize the health and safety of workforce Prioritize urgent patients Communicate consistently and transparently Invest appropriately in services and improvement efforts
Strategies to limit unnecessary exposure while continuing to provide high-quality care for our liver patients
bull Optimization and flexibility of schedules (hoursweekend)
bull Utilization of clinic spacebull Sustain telehealth bull Digital technology for symptoms
monitoring bull Staff redeployment
bull COVID symptoms check protocolbull Social distancing in clinicbull Masking and safety policiesbull Waiting rooms changesbull Visitor policies
bull Prioritize urgent patientsbull Back log data and referralsbull Pre-clinic communicationbull In clinic flow (Echeck in rooming
and check out policies)
bull Patient communication is the keybull Staff anxiety and stress reduction bull Focus on vulnerable populationbull Physician burn out and health needs bull Trainees re-entry and education
Staff and PatientSafety
Clinic Work Flows
Resource Utilization
Support and
Education
PatientCare
Ambulatory Recovery Challenges and PlanProviding Best Care While Living with COVID-19
Physical Distancing amp Safety Guidelines
Conversa Employee Screening Mychart Screener Apex texting for patients in
nearby waiting areas
Innovation and Improving Operations
Gradual Re-entry of Liver Patients in the Ambulatory Setting
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
Patient will be scheduled for modified evaluation with
Hepatology and social worker as video visit
Remainder of evaluation will be onsite when restrictions are lifted
1 Pre-clinicarrival COVID screening for patientscaregiver2 Universal masking
no
Re-entry of Liver Patients in Clinic June 2020
All new liver transplant evaluations and HCC diagnosis New decompensation or worsening symptoms Listed patients for transplant with decompensated cirrhosis Acute hepatitis or liver injury Early post transplant Patients with difficulty with telehealth
Re-entry of Liver Patients HCC Surveillance HCC surveillance should continue as close to schedule (an
arbitrary delay of 2 months were acceptable) Working on list of all delayed imaging and prioritizing them by
risk categoriesKnown HCC surveillance for treatment response elevated AFP
Key is working with Radiology (Options of imaging locally) Communication with patients and documentation is important No delay in HCC treatment (riskbenefits discussion)
httpswwwaasldorgsitesdefaultfiles2020-05AASLD-COVID19-ClinicalInsights-May42020
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
Fibroscan Not urgent but planning to
start June-July 2020 Huge back log Using radiology US protocol
for PPE (maskgoogles and gown) Flexible schedules based on
safety guidelines
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

Webinar PresenterBilal Hameed MD
Associate Professor of Medicine and the Hepatology Clinic Chief
University of California San Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 19
Webinar PresenterPatricia Harren DNP DCC
Clinical Director of the Center for Liver Disease amp Transplantation Clinical Director for Pediatric Transplantation
amp Adult Abdominal Organ Transplantation
Columbia University
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 20
Webinar PresenterDavid C Mulligan MD FAASLDProfessor of Surgery and Chief
of Transplantation and Immunology
Yale University Yale New Haven Health System
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 21
o Oren K Fix MD MSc FAASLD Swedish Medical Center (Washington)
o Elizabeth C Verna MD MS Columbia University (New York)
o Jaime Chu MD Icahn School of Medicine at Mount Sinai (New York)
o Karen Hoyt BA Patient Advocate
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 22
o Guadalupe Garcia-Tsao MD FAASLD Yale University (Connecticut)
o Ryutaro Hirose MD University of California San Francisco (California)
o K Gautham Reddy MD FAASLD University of Chicago Medical Center (Illinois)
Webinar Panelist
o OpenSAFELY Factors associated with COVID-19-related hospital deaths in the linked electronic health records of 17 million adult NHS patientsbull 17425445 adultsbull Feb 1 2020 to April 25 2020bull Primary outcome death in hospital in patients with confirmed
COVID-19 (5683 deaths)
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
httpsdoiorg1011012020050620092999
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
httpsdoiorg1011012020050620092999
HR adjusted for all other factors listed other than ethnicity
o Largest cohort study to date evaluating a variety of clinical factors for death from COVID-19
o Asians and blacks appear to be at increased risk of in-hospital death with only partial attribution to pre-existing clinical risk factors or deprivation
o Patients with pre-existing liver disease transplantation or on immunosuppression appear to have increased risk of in-hospital death when adjusted for agesex alone or fully adjusted
o Strengthsbull Largest cohort study to date representing 40 English populationbull Inclusion of variables including liver disease transplant for analysis
o Weaknessesbull Deaths related to patients with false-negative tests or died without testing would be missedbull Censoring patients at date of death from other causes or outside the hospital stopped 9
days short of study end bull Cohort limited to those practices using the EHR software SystmOne Some variable were
assumed absent if missing bull Characterization of ldquoliver diseaserdquo is general and not complete
o Further characterization of liver disease and potential risks due to etiology MELD etc will be helpful in future studies
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORGhttpsdoiorg1011012020050620092999
Expert Panel Consensus Statement
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 26
o First published online March 23rdo New update posted today
wwwaasldorgcovid19o Spanish and Portuguese
translations available onlineo Hepatology manuscript published
online
May 14th Update Major Changes
o Acknowledgement of possible link between COVID-19 and Kawasaki-like pediatric multisystem inflammatory syndrome
o Italian autopsy series describing involvement of hepatic vasculature including acute portal and sinusoidal thrombosis
o Introduction of SARS-CoV-2 antigen testing in addition to increasing availability of antibody testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 27
httpswwwhealthnygovpressreleases2020docs2020-05-06_covid19_pediatric_inflammatory_syndromepdfSonzogni et al Preprints 2020httpswwwfdagovnews-eventspress-announcementscoronavirus-covid-19-update-fda-authorizes-first-antigen-test-help-rapid-detection-virus-causes
May 14th Update Major Changes
o OpenSAFELY study from the UK chronic liver disease is a risk factor for in-hospital death from COVID-19
o Large US study also showed that chronic liver disease and cirrhosis are associated with higher COVID-19 mortality
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 28
Williamson et al MedRxiv 2020Singh and Khan Gastroenterol 2020
May 14th Update Major Changes
o Clarification that treatment of hepatitis B is not contraindicated in patients with or without COVID-19
o Recommendations regarding use of masks for patients and caregivers as well as providers in the clinic or hospital setting
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 29
May 14th Update Major Changes
o Evolving data on hydroxychloroquine suggesting it should no longer be used outside RCTs
o New data on triple therapy with lopinavir-ritonavir ribavirin and interferon-beta-1b showing more rapid viral clearance compared to lopinavir-ritonavir (phase 2 RCT)
o Reentry
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 30
Geleris et al N Eng J Med 2020Hung et al Lancet 2020
31
Impact of COVID-19 on Liver Disease Safe Outpatient Re-Entry Process
Bilal Hameed MDAssociate Professor of Medicine
Clinic Chief Hepatology University of California San Francisco
Outline
The COVID-19 effects on liver care Recommendations for re-entry and re-opening facilities Ambulatory re-entry and recovery challenges and plan
at UCSF Gradual re-entry of liver patients in the ambulatory
setting
The Untold Toll mdash The Pandemicrsquos Effects on Patients without COVID-19
httpswwwnejmorgdoifull101056NEJMms2009984query=featured_coronavirus
Patients with heart attacks strokes and even appendicitis vanish from
hospitals
The Pandemicrsquos Effects on Patients without COVID-1938 reduction in STEMI activations in the US
during COVID-19 pandemic
Garcia S et al Journal of the American College of Cardiology April 2020
Decrease in routine pediatric vaccination during COVID-19
httpswwwcdcgovmmwrvolumes69wr
Unexpected Consequences of the Pandemic
To expand capacity for COVID-19 patients on March 18th CMS recommended limiting non-essential care and procedures 8 week pause in usual care activities Fear of returning to care Change in patientrsquos perception of riskbenefit
Areas with lowstable incidence of COVID-19 CMS allowing non-emergent non-COVID-19 healthcare
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdf
COVID-19 Pandemic Impact on the Cirrhosis Care
Tapper EB et al Journal of Hepatology April 2020
COVID Surge
Loss of insurance
Outpatient Impact of COVID-19 Pandemic UCSF Experience Maximizing Appropriate Use of Video Visits during Re-entry
Prior State Current State Future State~20 of total visits were video visits
~95 of total visits are video visits
Appropriate mix of telehealth visits ~50
Continue expanding to -Patients that live far away -Post-ops amp post-discharge follow-up-Chronic disease management(NAFLDHBVHCV etc)-Free up clinic space
0
10000
20000
30000
40000
50000
60000
70000
End of April Double March volume
February 2 of all visits2nd largest video visit program in the
country among AMCs largest in California
End of March 60 of visits
UCSF Video Visits by Month (Jan 2015-April 2020)
0
100
200
300
400
500
600
700
800
900
Jul 2019 Aug Sep Oct Nov Dec Jan 2020 Feb Mar Apr
Able to see the same number of patients even during pandemic
Hepatology Video Visits by Month at UCSF
CMS Phase I Recommendations Re-opening Facilities for Non-emergent Non-COVID-19 Healthcare
In coordination with State and local public health officials evaluate the incidence and trends for COVID-19 in the area
Prioritize surgicalprocedural care and high-complexity chronic disease management and select preventive services
Consider establishing Non-COVID Care (NCC) zones that would screen all patients for symptoms of COVID-19
Sufficient resources should be available across phases of care including PPE healthy workforce testing capacity etc and without jeopardizing surge capacity
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdfhttpswwwwhitehousegovopeningamericacriteriahttpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
httpsdatasfgovorgstoriessdak2-gvuj
San Francisco COVID-19 Numbers
Ambulatory Re-entry and Recovery ndash Cascaded Principles
Ensure morbidity and mortality do not increase due to liver related illness and provide care in a safe manner
Continue to prioritize the health and safety of workforce Prioritize urgent patients Communicate consistently and transparently Invest appropriately in services and improvement efforts
Strategies to limit unnecessary exposure while continuing to provide high-quality care for our liver patients
bull Optimization and flexibility of schedules (hoursweekend)
bull Utilization of clinic spacebull Sustain telehealth bull Digital technology for symptoms
monitoring bull Staff redeployment
bull COVID symptoms check protocolbull Social distancing in clinicbull Masking and safety policiesbull Waiting rooms changesbull Visitor policies
bull Prioritize urgent patientsbull Back log data and referralsbull Pre-clinic communicationbull In clinic flow (Echeck in rooming
and check out policies)
bull Patient communication is the keybull Staff anxiety and stress reduction bull Focus on vulnerable populationbull Physician burn out and health needs bull Trainees re-entry and education
Staff and PatientSafety
Clinic Work Flows
Resource Utilization
Support and
Education
PatientCare
Ambulatory Recovery Challenges and PlanProviding Best Care While Living with COVID-19
Physical Distancing amp Safety Guidelines
Conversa Employee Screening Mychart Screener Apex texting for patients in
nearby waiting areas
Innovation and Improving Operations
Gradual Re-entry of Liver Patients in the Ambulatory Setting
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
Patient will be scheduled for modified evaluation with
Hepatology and social worker as video visit
Remainder of evaluation will be onsite when restrictions are lifted
1 Pre-clinicarrival COVID screening for patientscaregiver2 Universal masking
no
Re-entry of Liver Patients in Clinic June 2020
All new liver transplant evaluations and HCC diagnosis New decompensation or worsening symptoms Listed patients for transplant with decompensated cirrhosis Acute hepatitis or liver injury Early post transplant Patients with difficulty with telehealth
Re-entry of Liver Patients HCC Surveillance HCC surveillance should continue as close to schedule (an
arbitrary delay of 2 months were acceptable) Working on list of all delayed imaging and prioritizing them by
risk categoriesKnown HCC surveillance for treatment response elevated AFP
Key is working with Radiology (Options of imaging locally) Communication with patients and documentation is important No delay in HCC treatment (riskbenefits discussion)
httpswwwaasldorgsitesdefaultfiles2020-05AASLD-COVID19-ClinicalInsights-May42020
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
Fibroscan Not urgent but planning to
start June-July 2020 Huge back log Using radiology US protocol
for PPE (maskgoogles and gown) Flexible schedules based on
safety guidelines
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

Webinar PresenterPatricia Harren DNP DCC
Clinical Director of the Center for Liver Disease amp Transplantation Clinical Director for Pediatric Transplantation
amp Adult Abdominal Organ Transplantation
Columbia University
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 20
Webinar PresenterDavid C Mulligan MD FAASLDProfessor of Surgery and Chief
of Transplantation and Immunology
Yale University Yale New Haven Health System
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 21
o Oren K Fix MD MSc FAASLD Swedish Medical Center (Washington)
o Elizabeth C Verna MD MS Columbia University (New York)
o Jaime Chu MD Icahn School of Medicine at Mount Sinai (New York)
o Karen Hoyt BA Patient Advocate
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 22
o Guadalupe Garcia-Tsao MD FAASLD Yale University (Connecticut)
o Ryutaro Hirose MD University of California San Francisco (California)
o K Gautham Reddy MD FAASLD University of Chicago Medical Center (Illinois)
Webinar Panelist
o OpenSAFELY Factors associated with COVID-19-related hospital deaths in the linked electronic health records of 17 million adult NHS patientsbull 17425445 adultsbull Feb 1 2020 to April 25 2020bull Primary outcome death in hospital in patients with confirmed
COVID-19 (5683 deaths)
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
httpsdoiorg1011012020050620092999
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
httpsdoiorg1011012020050620092999
HR adjusted for all other factors listed other than ethnicity
o Largest cohort study to date evaluating a variety of clinical factors for death from COVID-19
o Asians and blacks appear to be at increased risk of in-hospital death with only partial attribution to pre-existing clinical risk factors or deprivation
o Patients with pre-existing liver disease transplantation or on immunosuppression appear to have increased risk of in-hospital death when adjusted for agesex alone or fully adjusted
o Strengthsbull Largest cohort study to date representing 40 English populationbull Inclusion of variables including liver disease transplant for analysis
o Weaknessesbull Deaths related to patients with false-negative tests or died without testing would be missedbull Censoring patients at date of death from other causes or outside the hospital stopped 9
days short of study end bull Cohort limited to those practices using the EHR software SystmOne Some variable were
assumed absent if missing bull Characterization of ldquoliver diseaserdquo is general and not complete
o Further characterization of liver disease and potential risks due to etiology MELD etc will be helpful in future studies
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORGhttpsdoiorg1011012020050620092999
Expert Panel Consensus Statement
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 26
o First published online March 23rdo New update posted today
wwwaasldorgcovid19o Spanish and Portuguese
translations available onlineo Hepatology manuscript published
online
May 14th Update Major Changes
o Acknowledgement of possible link between COVID-19 and Kawasaki-like pediatric multisystem inflammatory syndrome
o Italian autopsy series describing involvement of hepatic vasculature including acute portal and sinusoidal thrombosis
o Introduction of SARS-CoV-2 antigen testing in addition to increasing availability of antibody testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 27
httpswwwhealthnygovpressreleases2020docs2020-05-06_covid19_pediatric_inflammatory_syndromepdfSonzogni et al Preprints 2020httpswwwfdagovnews-eventspress-announcementscoronavirus-covid-19-update-fda-authorizes-first-antigen-test-help-rapid-detection-virus-causes
May 14th Update Major Changes
o OpenSAFELY study from the UK chronic liver disease is a risk factor for in-hospital death from COVID-19
o Large US study also showed that chronic liver disease and cirrhosis are associated with higher COVID-19 mortality
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 28
Williamson et al MedRxiv 2020Singh and Khan Gastroenterol 2020
May 14th Update Major Changes
o Clarification that treatment of hepatitis B is not contraindicated in patients with or without COVID-19
o Recommendations regarding use of masks for patients and caregivers as well as providers in the clinic or hospital setting
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 29
May 14th Update Major Changes
o Evolving data on hydroxychloroquine suggesting it should no longer be used outside RCTs
o New data on triple therapy with lopinavir-ritonavir ribavirin and interferon-beta-1b showing more rapid viral clearance compared to lopinavir-ritonavir (phase 2 RCT)
o Reentry
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 30
Geleris et al N Eng J Med 2020Hung et al Lancet 2020
31
Impact of COVID-19 on Liver Disease Safe Outpatient Re-Entry Process
Bilal Hameed MDAssociate Professor of Medicine
Clinic Chief Hepatology University of California San Francisco
Outline
The COVID-19 effects on liver care Recommendations for re-entry and re-opening facilities Ambulatory re-entry and recovery challenges and plan
at UCSF Gradual re-entry of liver patients in the ambulatory
setting
The Untold Toll mdash The Pandemicrsquos Effects on Patients without COVID-19
httpswwwnejmorgdoifull101056NEJMms2009984query=featured_coronavirus
Patients with heart attacks strokes and even appendicitis vanish from
hospitals
The Pandemicrsquos Effects on Patients without COVID-1938 reduction in STEMI activations in the US
during COVID-19 pandemic
Garcia S et al Journal of the American College of Cardiology April 2020
Decrease in routine pediatric vaccination during COVID-19
httpswwwcdcgovmmwrvolumes69wr
Unexpected Consequences of the Pandemic
To expand capacity for COVID-19 patients on March 18th CMS recommended limiting non-essential care and procedures 8 week pause in usual care activities Fear of returning to care Change in patientrsquos perception of riskbenefit
Areas with lowstable incidence of COVID-19 CMS allowing non-emergent non-COVID-19 healthcare
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdf
COVID-19 Pandemic Impact on the Cirrhosis Care
Tapper EB et al Journal of Hepatology April 2020
COVID Surge
Loss of insurance
Outpatient Impact of COVID-19 Pandemic UCSF Experience Maximizing Appropriate Use of Video Visits during Re-entry
Prior State Current State Future State~20 of total visits were video visits
~95 of total visits are video visits
Appropriate mix of telehealth visits ~50
Continue expanding to -Patients that live far away -Post-ops amp post-discharge follow-up-Chronic disease management(NAFLDHBVHCV etc)-Free up clinic space
0
10000
20000
30000
40000
50000
60000
70000
End of April Double March volume
February 2 of all visits2nd largest video visit program in the
country among AMCs largest in California
End of March 60 of visits
UCSF Video Visits by Month (Jan 2015-April 2020)
0
100
200
300
400
500
600
700
800
900
Jul 2019 Aug Sep Oct Nov Dec Jan 2020 Feb Mar Apr
Able to see the same number of patients even during pandemic
Hepatology Video Visits by Month at UCSF
CMS Phase I Recommendations Re-opening Facilities for Non-emergent Non-COVID-19 Healthcare
In coordination with State and local public health officials evaluate the incidence and trends for COVID-19 in the area
Prioritize surgicalprocedural care and high-complexity chronic disease management and select preventive services
Consider establishing Non-COVID Care (NCC) zones that would screen all patients for symptoms of COVID-19
Sufficient resources should be available across phases of care including PPE healthy workforce testing capacity etc and without jeopardizing surge capacity
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdfhttpswwwwhitehousegovopeningamericacriteriahttpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
httpsdatasfgovorgstoriessdak2-gvuj
San Francisco COVID-19 Numbers
Ambulatory Re-entry and Recovery ndash Cascaded Principles
Ensure morbidity and mortality do not increase due to liver related illness and provide care in a safe manner
Continue to prioritize the health and safety of workforce Prioritize urgent patients Communicate consistently and transparently Invest appropriately in services and improvement efforts
Strategies to limit unnecessary exposure while continuing to provide high-quality care for our liver patients
bull Optimization and flexibility of schedules (hoursweekend)
bull Utilization of clinic spacebull Sustain telehealth bull Digital technology for symptoms
monitoring bull Staff redeployment
bull COVID symptoms check protocolbull Social distancing in clinicbull Masking and safety policiesbull Waiting rooms changesbull Visitor policies
bull Prioritize urgent patientsbull Back log data and referralsbull Pre-clinic communicationbull In clinic flow (Echeck in rooming
and check out policies)
bull Patient communication is the keybull Staff anxiety and stress reduction bull Focus on vulnerable populationbull Physician burn out and health needs bull Trainees re-entry and education
Staff and PatientSafety
Clinic Work Flows
Resource Utilization
Support and
Education
PatientCare
Ambulatory Recovery Challenges and PlanProviding Best Care While Living with COVID-19
Physical Distancing amp Safety Guidelines
Conversa Employee Screening Mychart Screener Apex texting for patients in
nearby waiting areas
Innovation and Improving Operations
Gradual Re-entry of Liver Patients in the Ambulatory Setting
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
Patient will be scheduled for modified evaluation with
Hepatology and social worker as video visit
Remainder of evaluation will be onsite when restrictions are lifted
1 Pre-clinicarrival COVID screening for patientscaregiver2 Universal masking
no
Re-entry of Liver Patients in Clinic June 2020
All new liver transplant evaluations and HCC diagnosis New decompensation or worsening symptoms Listed patients for transplant with decompensated cirrhosis Acute hepatitis or liver injury Early post transplant Patients with difficulty with telehealth
Re-entry of Liver Patients HCC Surveillance HCC surveillance should continue as close to schedule (an
arbitrary delay of 2 months were acceptable) Working on list of all delayed imaging and prioritizing them by
risk categoriesKnown HCC surveillance for treatment response elevated AFP
Key is working with Radiology (Options of imaging locally) Communication with patients and documentation is important No delay in HCC treatment (riskbenefits discussion)
httpswwwaasldorgsitesdefaultfiles2020-05AASLD-COVID19-ClinicalInsights-May42020
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
Fibroscan Not urgent but planning to
start June-July 2020 Huge back log Using radiology US protocol
for PPE (maskgoogles and gown) Flexible schedules based on
safety guidelines
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

Webinar PresenterDavid C Mulligan MD FAASLDProfessor of Surgery and Chief
of Transplantation and Immunology
Yale University Yale New Haven Health System
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 21
o Oren K Fix MD MSc FAASLD Swedish Medical Center (Washington)
o Elizabeth C Verna MD MS Columbia University (New York)
o Jaime Chu MD Icahn School of Medicine at Mount Sinai (New York)
o Karen Hoyt BA Patient Advocate
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 22
o Guadalupe Garcia-Tsao MD FAASLD Yale University (Connecticut)
o Ryutaro Hirose MD University of California San Francisco (California)
o K Gautham Reddy MD FAASLD University of Chicago Medical Center (Illinois)
Webinar Panelist
o OpenSAFELY Factors associated with COVID-19-related hospital deaths in the linked electronic health records of 17 million adult NHS patientsbull 17425445 adultsbull Feb 1 2020 to April 25 2020bull Primary outcome death in hospital in patients with confirmed
COVID-19 (5683 deaths)
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
httpsdoiorg1011012020050620092999
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
httpsdoiorg1011012020050620092999
HR adjusted for all other factors listed other than ethnicity
o Largest cohort study to date evaluating a variety of clinical factors for death from COVID-19
o Asians and blacks appear to be at increased risk of in-hospital death with only partial attribution to pre-existing clinical risk factors or deprivation
o Patients with pre-existing liver disease transplantation or on immunosuppression appear to have increased risk of in-hospital death when adjusted for agesex alone or fully adjusted
o Strengthsbull Largest cohort study to date representing 40 English populationbull Inclusion of variables including liver disease transplant for analysis
o Weaknessesbull Deaths related to patients with false-negative tests or died without testing would be missedbull Censoring patients at date of death from other causes or outside the hospital stopped 9
days short of study end bull Cohort limited to those practices using the EHR software SystmOne Some variable were
assumed absent if missing bull Characterization of ldquoliver diseaserdquo is general and not complete
o Further characterization of liver disease and potential risks due to etiology MELD etc will be helpful in future studies
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORGhttpsdoiorg1011012020050620092999
Expert Panel Consensus Statement
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 26
o First published online March 23rdo New update posted today
wwwaasldorgcovid19o Spanish and Portuguese
translations available onlineo Hepatology manuscript published
online
May 14th Update Major Changes
o Acknowledgement of possible link between COVID-19 and Kawasaki-like pediatric multisystem inflammatory syndrome
o Italian autopsy series describing involvement of hepatic vasculature including acute portal and sinusoidal thrombosis
o Introduction of SARS-CoV-2 antigen testing in addition to increasing availability of antibody testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 27
httpswwwhealthnygovpressreleases2020docs2020-05-06_covid19_pediatric_inflammatory_syndromepdfSonzogni et al Preprints 2020httpswwwfdagovnews-eventspress-announcementscoronavirus-covid-19-update-fda-authorizes-first-antigen-test-help-rapid-detection-virus-causes
May 14th Update Major Changes
o OpenSAFELY study from the UK chronic liver disease is a risk factor for in-hospital death from COVID-19
o Large US study also showed that chronic liver disease and cirrhosis are associated with higher COVID-19 mortality
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 28
Williamson et al MedRxiv 2020Singh and Khan Gastroenterol 2020
May 14th Update Major Changes
o Clarification that treatment of hepatitis B is not contraindicated in patients with or without COVID-19
o Recommendations regarding use of masks for patients and caregivers as well as providers in the clinic or hospital setting
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 29
May 14th Update Major Changes
o Evolving data on hydroxychloroquine suggesting it should no longer be used outside RCTs
o New data on triple therapy with lopinavir-ritonavir ribavirin and interferon-beta-1b showing more rapid viral clearance compared to lopinavir-ritonavir (phase 2 RCT)
o Reentry
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 30
Geleris et al N Eng J Med 2020Hung et al Lancet 2020
31
Impact of COVID-19 on Liver Disease Safe Outpatient Re-Entry Process
Bilal Hameed MDAssociate Professor of Medicine
Clinic Chief Hepatology University of California San Francisco
Outline
The COVID-19 effects on liver care Recommendations for re-entry and re-opening facilities Ambulatory re-entry and recovery challenges and plan
at UCSF Gradual re-entry of liver patients in the ambulatory
setting
The Untold Toll mdash The Pandemicrsquos Effects on Patients without COVID-19
httpswwwnejmorgdoifull101056NEJMms2009984query=featured_coronavirus
Patients with heart attacks strokes and even appendicitis vanish from
hospitals
The Pandemicrsquos Effects on Patients without COVID-1938 reduction in STEMI activations in the US
during COVID-19 pandemic
Garcia S et al Journal of the American College of Cardiology April 2020
Decrease in routine pediatric vaccination during COVID-19
httpswwwcdcgovmmwrvolumes69wr
Unexpected Consequences of the Pandemic
To expand capacity for COVID-19 patients on March 18th CMS recommended limiting non-essential care and procedures 8 week pause in usual care activities Fear of returning to care Change in patientrsquos perception of riskbenefit
Areas with lowstable incidence of COVID-19 CMS allowing non-emergent non-COVID-19 healthcare
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdf
COVID-19 Pandemic Impact on the Cirrhosis Care
Tapper EB et al Journal of Hepatology April 2020
COVID Surge
Loss of insurance
Outpatient Impact of COVID-19 Pandemic UCSF Experience Maximizing Appropriate Use of Video Visits during Re-entry
Prior State Current State Future State~20 of total visits were video visits
~95 of total visits are video visits
Appropriate mix of telehealth visits ~50
Continue expanding to -Patients that live far away -Post-ops amp post-discharge follow-up-Chronic disease management(NAFLDHBVHCV etc)-Free up clinic space
0
10000
20000
30000
40000
50000
60000
70000
End of April Double March volume
February 2 of all visits2nd largest video visit program in the
country among AMCs largest in California
End of March 60 of visits
UCSF Video Visits by Month (Jan 2015-April 2020)
0
100
200
300
400
500
600
700
800
900
Jul 2019 Aug Sep Oct Nov Dec Jan 2020 Feb Mar Apr
Able to see the same number of patients even during pandemic
Hepatology Video Visits by Month at UCSF
CMS Phase I Recommendations Re-opening Facilities for Non-emergent Non-COVID-19 Healthcare
In coordination with State and local public health officials evaluate the incidence and trends for COVID-19 in the area
Prioritize surgicalprocedural care and high-complexity chronic disease management and select preventive services
Consider establishing Non-COVID Care (NCC) zones that would screen all patients for symptoms of COVID-19
Sufficient resources should be available across phases of care including PPE healthy workforce testing capacity etc and without jeopardizing surge capacity
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdfhttpswwwwhitehousegovopeningamericacriteriahttpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
httpsdatasfgovorgstoriessdak2-gvuj
San Francisco COVID-19 Numbers
Ambulatory Re-entry and Recovery ndash Cascaded Principles
Ensure morbidity and mortality do not increase due to liver related illness and provide care in a safe manner
Continue to prioritize the health and safety of workforce Prioritize urgent patients Communicate consistently and transparently Invest appropriately in services and improvement efforts
Strategies to limit unnecessary exposure while continuing to provide high-quality care for our liver patients
bull Optimization and flexibility of schedules (hoursweekend)
bull Utilization of clinic spacebull Sustain telehealth bull Digital technology for symptoms
monitoring bull Staff redeployment
bull COVID symptoms check protocolbull Social distancing in clinicbull Masking and safety policiesbull Waiting rooms changesbull Visitor policies
bull Prioritize urgent patientsbull Back log data and referralsbull Pre-clinic communicationbull In clinic flow (Echeck in rooming
and check out policies)
bull Patient communication is the keybull Staff anxiety and stress reduction bull Focus on vulnerable populationbull Physician burn out and health needs bull Trainees re-entry and education
Staff and PatientSafety
Clinic Work Flows
Resource Utilization
Support and
Education
PatientCare
Ambulatory Recovery Challenges and PlanProviding Best Care While Living with COVID-19
Physical Distancing amp Safety Guidelines
Conversa Employee Screening Mychart Screener Apex texting for patients in
nearby waiting areas
Innovation and Improving Operations
Gradual Re-entry of Liver Patients in the Ambulatory Setting
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
Patient will be scheduled for modified evaluation with
Hepatology and social worker as video visit
Remainder of evaluation will be onsite when restrictions are lifted
1 Pre-clinicarrival COVID screening for patientscaregiver2 Universal masking
no
Re-entry of Liver Patients in Clinic June 2020
All new liver transplant evaluations and HCC diagnosis New decompensation or worsening symptoms Listed patients for transplant with decompensated cirrhosis Acute hepatitis or liver injury Early post transplant Patients with difficulty with telehealth
Re-entry of Liver Patients HCC Surveillance HCC surveillance should continue as close to schedule (an
arbitrary delay of 2 months were acceptable) Working on list of all delayed imaging and prioritizing them by
risk categoriesKnown HCC surveillance for treatment response elevated AFP
Key is working with Radiology (Options of imaging locally) Communication with patients and documentation is important No delay in HCC treatment (riskbenefits discussion)
httpswwwaasldorgsitesdefaultfiles2020-05AASLD-COVID19-ClinicalInsights-May42020
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
Fibroscan Not urgent but planning to
start June-July 2020 Huge back log Using radiology US protocol
for PPE (maskgoogles and gown) Flexible schedules based on
safety guidelines
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

o Oren K Fix MD MSc FAASLD Swedish Medical Center (Washington)
o Elizabeth C Verna MD MS Columbia University (New York)
o Jaime Chu MD Icahn School of Medicine at Mount Sinai (New York)
o Karen Hoyt BA Patient Advocate
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 22
o Guadalupe Garcia-Tsao MD FAASLD Yale University (Connecticut)
o Ryutaro Hirose MD University of California San Francisco (California)
o K Gautham Reddy MD FAASLD University of Chicago Medical Center (Illinois)
Webinar Panelist
o OpenSAFELY Factors associated with COVID-19-related hospital deaths in the linked electronic health records of 17 million adult NHS patientsbull 17425445 adultsbull Feb 1 2020 to April 25 2020bull Primary outcome death in hospital in patients with confirmed
COVID-19 (5683 deaths)
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
httpsdoiorg1011012020050620092999
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
httpsdoiorg1011012020050620092999
HR adjusted for all other factors listed other than ethnicity
o Largest cohort study to date evaluating a variety of clinical factors for death from COVID-19
o Asians and blacks appear to be at increased risk of in-hospital death with only partial attribution to pre-existing clinical risk factors or deprivation
o Patients with pre-existing liver disease transplantation or on immunosuppression appear to have increased risk of in-hospital death when adjusted for agesex alone or fully adjusted
o Strengthsbull Largest cohort study to date representing 40 English populationbull Inclusion of variables including liver disease transplant for analysis
o Weaknessesbull Deaths related to patients with false-negative tests or died without testing would be missedbull Censoring patients at date of death from other causes or outside the hospital stopped 9
days short of study end bull Cohort limited to those practices using the EHR software SystmOne Some variable were
assumed absent if missing bull Characterization of ldquoliver diseaserdquo is general and not complete
o Further characterization of liver disease and potential risks due to etiology MELD etc will be helpful in future studies
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORGhttpsdoiorg1011012020050620092999
Expert Panel Consensus Statement
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 26
o First published online March 23rdo New update posted today
wwwaasldorgcovid19o Spanish and Portuguese
translations available onlineo Hepatology manuscript published
online
May 14th Update Major Changes
o Acknowledgement of possible link between COVID-19 and Kawasaki-like pediatric multisystem inflammatory syndrome
o Italian autopsy series describing involvement of hepatic vasculature including acute portal and sinusoidal thrombosis
o Introduction of SARS-CoV-2 antigen testing in addition to increasing availability of antibody testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 27
httpswwwhealthnygovpressreleases2020docs2020-05-06_covid19_pediatric_inflammatory_syndromepdfSonzogni et al Preprints 2020httpswwwfdagovnews-eventspress-announcementscoronavirus-covid-19-update-fda-authorizes-first-antigen-test-help-rapid-detection-virus-causes
May 14th Update Major Changes
o OpenSAFELY study from the UK chronic liver disease is a risk factor for in-hospital death from COVID-19
o Large US study also showed that chronic liver disease and cirrhosis are associated with higher COVID-19 mortality
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 28
Williamson et al MedRxiv 2020Singh and Khan Gastroenterol 2020
May 14th Update Major Changes
o Clarification that treatment of hepatitis B is not contraindicated in patients with or without COVID-19
o Recommendations regarding use of masks for patients and caregivers as well as providers in the clinic or hospital setting
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 29
May 14th Update Major Changes
o Evolving data on hydroxychloroquine suggesting it should no longer be used outside RCTs
o New data on triple therapy with lopinavir-ritonavir ribavirin and interferon-beta-1b showing more rapid viral clearance compared to lopinavir-ritonavir (phase 2 RCT)
o Reentry
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 30
Geleris et al N Eng J Med 2020Hung et al Lancet 2020
31
Impact of COVID-19 on Liver Disease Safe Outpatient Re-Entry Process
Bilal Hameed MDAssociate Professor of Medicine
Clinic Chief Hepatology University of California San Francisco
Outline
The COVID-19 effects on liver care Recommendations for re-entry and re-opening facilities Ambulatory re-entry and recovery challenges and plan
at UCSF Gradual re-entry of liver patients in the ambulatory
setting
The Untold Toll mdash The Pandemicrsquos Effects on Patients without COVID-19
httpswwwnejmorgdoifull101056NEJMms2009984query=featured_coronavirus
Patients with heart attacks strokes and even appendicitis vanish from
hospitals
The Pandemicrsquos Effects on Patients without COVID-1938 reduction in STEMI activations in the US
during COVID-19 pandemic
Garcia S et al Journal of the American College of Cardiology April 2020
Decrease in routine pediatric vaccination during COVID-19
httpswwwcdcgovmmwrvolumes69wr
Unexpected Consequences of the Pandemic
To expand capacity for COVID-19 patients on March 18th CMS recommended limiting non-essential care and procedures 8 week pause in usual care activities Fear of returning to care Change in patientrsquos perception of riskbenefit
Areas with lowstable incidence of COVID-19 CMS allowing non-emergent non-COVID-19 healthcare
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdf
COVID-19 Pandemic Impact on the Cirrhosis Care
Tapper EB et al Journal of Hepatology April 2020
COVID Surge
Loss of insurance
Outpatient Impact of COVID-19 Pandemic UCSF Experience Maximizing Appropriate Use of Video Visits during Re-entry
Prior State Current State Future State~20 of total visits were video visits
~95 of total visits are video visits
Appropriate mix of telehealth visits ~50
Continue expanding to -Patients that live far away -Post-ops amp post-discharge follow-up-Chronic disease management(NAFLDHBVHCV etc)-Free up clinic space
0
10000
20000
30000
40000
50000
60000
70000
End of April Double March volume
February 2 of all visits2nd largest video visit program in the
country among AMCs largest in California
End of March 60 of visits
UCSF Video Visits by Month (Jan 2015-April 2020)
0
100
200
300
400
500
600
700
800
900
Jul 2019 Aug Sep Oct Nov Dec Jan 2020 Feb Mar Apr
Able to see the same number of patients even during pandemic
Hepatology Video Visits by Month at UCSF
CMS Phase I Recommendations Re-opening Facilities for Non-emergent Non-COVID-19 Healthcare
In coordination with State and local public health officials evaluate the incidence and trends for COVID-19 in the area
Prioritize surgicalprocedural care and high-complexity chronic disease management and select preventive services
Consider establishing Non-COVID Care (NCC) zones that would screen all patients for symptoms of COVID-19
Sufficient resources should be available across phases of care including PPE healthy workforce testing capacity etc and without jeopardizing surge capacity
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdfhttpswwwwhitehousegovopeningamericacriteriahttpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
httpsdatasfgovorgstoriessdak2-gvuj
San Francisco COVID-19 Numbers
Ambulatory Re-entry and Recovery ndash Cascaded Principles
Ensure morbidity and mortality do not increase due to liver related illness and provide care in a safe manner
Continue to prioritize the health and safety of workforce Prioritize urgent patients Communicate consistently and transparently Invest appropriately in services and improvement efforts
Strategies to limit unnecessary exposure while continuing to provide high-quality care for our liver patients
bull Optimization and flexibility of schedules (hoursweekend)
bull Utilization of clinic spacebull Sustain telehealth bull Digital technology for symptoms
monitoring bull Staff redeployment
bull COVID symptoms check protocolbull Social distancing in clinicbull Masking and safety policiesbull Waiting rooms changesbull Visitor policies
bull Prioritize urgent patientsbull Back log data and referralsbull Pre-clinic communicationbull In clinic flow (Echeck in rooming
and check out policies)
bull Patient communication is the keybull Staff anxiety and stress reduction bull Focus on vulnerable populationbull Physician burn out and health needs bull Trainees re-entry and education
Staff and PatientSafety
Clinic Work Flows
Resource Utilization
Support and
Education
PatientCare
Ambulatory Recovery Challenges and PlanProviding Best Care While Living with COVID-19
Physical Distancing amp Safety Guidelines
Conversa Employee Screening Mychart Screener Apex texting for patients in
nearby waiting areas
Innovation and Improving Operations
Gradual Re-entry of Liver Patients in the Ambulatory Setting
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
Patient will be scheduled for modified evaluation with
Hepatology and social worker as video visit
Remainder of evaluation will be onsite when restrictions are lifted
1 Pre-clinicarrival COVID screening for patientscaregiver2 Universal masking
no
Re-entry of Liver Patients in Clinic June 2020
All new liver transplant evaluations and HCC diagnosis New decompensation or worsening symptoms Listed patients for transplant with decompensated cirrhosis Acute hepatitis or liver injury Early post transplant Patients with difficulty with telehealth
Re-entry of Liver Patients HCC Surveillance HCC surveillance should continue as close to schedule (an
arbitrary delay of 2 months were acceptable) Working on list of all delayed imaging and prioritizing them by
risk categoriesKnown HCC surveillance for treatment response elevated AFP
Key is working with Radiology (Options of imaging locally) Communication with patients and documentation is important No delay in HCC treatment (riskbenefits discussion)
httpswwwaasldorgsitesdefaultfiles2020-05AASLD-COVID19-ClinicalInsights-May42020
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
Fibroscan Not urgent but planning to
start June-July 2020 Huge back log Using radiology US protocol
for PPE (maskgoogles and gown) Flexible schedules based on
safety guidelines
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

o OpenSAFELY Factors associated with COVID-19-related hospital deaths in the linked electronic health records of 17 million adult NHS patientsbull 17425445 adultsbull Feb 1 2020 to April 25 2020bull Primary outcome death in hospital in patients with confirmed
COVID-19 (5683 deaths)
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
httpsdoiorg1011012020050620092999
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
httpsdoiorg1011012020050620092999
HR adjusted for all other factors listed other than ethnicity
o Largest cohort study to date evaluating a variety of clinical factors for death from COVID-19
o Asians and blacks appear to be at increased risk of in-hospital death with only partial attribution to pre-existing clinical risk factors or deprivation
o Patients with pre-existing liver disease transplantation or on immunosuppression appear to have increased risk of in-hospital death when adjusted for agesex alone or fully adjusted
o Strengthsbull Largest cohort study to date representing 40 English populationbull Inclusion of variables including liver disease transplant for analysis
o Weaknessesbull Deaths related to patients with false-negative tests or died without testing would be missedbull Censoring patients at date of death from other causes or outside the hospital stopped 9
days short of study end bull Cohort limited to those practices using the EHR software SystmOne Some variable were
assumed absent if missing bull Characterization of ldquoliver diseaserdquo is general and not complete
o Further characterization of liver disease and potential risks due to etiology MELD etc will be helpful in future studies
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORGhttpsdoiorg1011012020050620092999
Expert Panel Consensus Statement
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 26
o First published online March 23rdo New update posted today
wwwaasldorgcovid19o Spanish and Portuguese
translations available onlineo Hepatology manuscript published
online
May 14th Update Major Changes
o Acknowledgement of possible link between COVID-19 and Kawasaki-like pediatric multisystem inflammatory syndrome
o Italian autopsy series describing involvement of hepatic vasculature including acute portal and sinusoidal thrombosis
o Introduction of SARS-CoV-2 antigen testing in addition to increasing availability of antibody testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 27
httpswwwhealthnygovpressreleases2020docs2020-05-06_covid19_pediatric_inflammatory_syndromepdfSonzogni et al Preprints 2020httpswwwfdagovnews-eventspress-announcementscoronavirus-covid-19-update-fda-authorizes-first-antigen-test-help-rapid-detection-virus-causes
May 14th Update Major Changes
o OpenSAFELY study from the UK chronic liver disease is a risk factor for in-hospital death from COVID-19
o Large US study also showed that chronic liver disease and cirrhosis are associated with higher COVID-19 mortality
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 28
Williamson et al MedRxiv 2020Singh and Khan Gastroenterol 2020
May 14th Update Major Changes
o Clarification that treatment of hepatitis B is not contraindicated in patients with or without COVID-19
o Recommendations regarding use of masks for patients and caregivers as well as providers in the clinic or hospital setting
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 29
May 14th Update Major Changes
o Evolving data on hydroxychloroquine suggesting it should no longer be used outside RCTs
o New data on triple therapy with lopinavir-ritonavir ribavirin and interferon-beta-1b showing more rapid viral clearance compared to lopinavir-ritonavir (phase 2 RCT)
o Reentry
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 30
Geleris et al N Eng J Med 2020Hung et al Lancet 2020
31
Impact of COVID-19 on Liver Disease Safe Outpatient Re-Entry Process
Bilal Hameed MDAssociate Professor of Medicine
Clinic Chief Hepatology University of California San Francisco
Outline
The COVID-19 effects on liver care Recommendations for re-entry and re-opening facilities Ambulatory re-entry and recovery challenges and plan
at UCSF Gradual re-entry of liver patients in the ambulatory
setting
The Untold Toll mdash The Pandemicrsquos Effects on Patients without COVID-19
httpswwwnejmorgdoifull101056NEJMms2009984query=featured_coronavirus
Patients with heart attacks strokes and even appendicitis vanish from
hospitals
The Pandemicrsquos Effects on Patients without COVID-1938 reduction in STEMI activations in the US
during COVID-19 pandemic
Garcia S et al Journal of the American College of Cardiology April 2020
Decrease in routine pediatric vaccination during COVID-19
httpswwwcdcgovmmwrvolumes69wr
Unexpected Consequences of the Pandemic
To expand capacity for COVID-19 patients on March 18th CMS recommended limiting non-essential care and procedures 8 week pause in usual care activities Fear of returning to care Change in patientrsquos perception of riskbenefit
Areas with lowstable incidence of COVID-19 CMS allowing non-emergent non-COVID-19 healthcare
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdf
COVID-19 Pandemic Impact on the Cirrhosis Care
Tapper EB et al Journal of Hepatology April 2020
COVID Surge
Loss of insurance
Outpatient Impact of COVID-19 Pandemic UCSF Experience Maximizing Appropriate Use of Video Visits during Re-entry
Prior State Current State Future State~20 of total visits were video visits
~95 of total visits are video visits
Appropriate mix of telehealth visits ~50
Continue expanding to -Patients that live far away -Post-ops amp post-discharge follow-up-Chronic disease management(NAFLDHBVHCV etc)-Free up clinic space
0
10000
20000
30000
40000
50000
60000
70000
End of April Double March volume
February 2 of all visits2nd largest video visit program in the
country among AMCs largest in California
End of March 60 of visits
UCSF Video Visits by Month (Jan 2015-April 2020)
0
100
200
300
400
500
600
700
800
900
Jul 2019 Aug Sep Oct Nov Dec Jan 2020 Feb Mar Apr
Able to see the same number of patients even during pandemic
Hepatology Video Visits by Month at UCSF
CMS Phase I Recommendations Re-opening Facilities for Non-emergent Non-COVID-19 Healthcare
In coordination with State and local public health officials evaluate the incidence and trends for COVID-19 in the area
Prioritize surgicalprocedural care and high-complexity chronic disease management and select preventive services
Consider establishing Non-COVID Care (NCC) zones that would screen all patients for symptoms of COVID-19
Sufficient resources should be available across phases of care including PPE healthy workforce testing capacity etc and without jeopardizing surge capacity
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdfhttpswwwwhitehousegovopeningamericacriteriahttpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
httpsdatasfgovorgstoriessdak2-gvuj
San Francisco COVID-19 Numbers
Ambulatory Re-entry and Recovery ndash Cascaded Principles
Ensure morbidity and mortality do not increase due to liver related illness and provide care in a safe manner
Continue to prioritize the health and safety of workforce Prioritize urgent patients Communicate consistently and transparently Invest appropriately in services and improvement efforts
Strategies to limit unnecessary exposure while continuing to provide high-quality care for our liver patients
bull Optimization and flexibility of schedules (hoursweekend)
bull Utilization of clinic spacebull Sustain telehealth bull Digital technology for symptoms
monitoring bull Staff redeployment
bull COVID symptoms check protocolbull Social distancing in clinicbull Masking and safety policiesbull Waiting rooms changesbull Visitor policies
bull Prioritize urgent patientsbull Back log data and referralsbull Pre-clinic communicationbull In clinic flow (Echeck in rooming
and check out policies)
bull Patient communication is the keybull Staff anxiety and stress reduction bull Focus on vulnerable populationbull Physician burn out and health needs bull Trainees re-entry and education
Staff and PatientSafety
Clinic Work Flows
Resource Utilization
Support and
Education
PatientCare
Ambulatory Recovery Challenges and PlanProviding Best Care While Living with COVID-19
Physical Distancing amp Safety Guidelines
Conversa Employee Screening Mychart Screener Apex texting for patients in
nearby waiting areas
Innovation and Improving Operations
Gradual Re-entry of Liver Patients in the Ambulatory Setting
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
Patient will be scheduled for modified evaluation with
Hepatology and social worker as video visit
Remainder of evaluation will be onsite when restrictions are lifted
1 Pre-clinicarrival COVID screening for patientscaregiver2 Universal masking
no
Re-entry of Liver Patients in Clinic June 2020
All new liver transplant evaluations and HCC diagnosis New decompensation or worsening symptoms Listed patients for transplant with decompensated cirrhosis Acute hepatitis or liver injury Early post transplant Patients with difficulty with telehealth
Re-entry of Liver Patients HCC Surveillance HCC surveillance should continue as close to schedule (an
arbitrary delay of 2 months were acceptable) Working on list of all delayed imaging and prioritizing them by
risk categoriesKnown HCC surveillance for treatment response elevated AFP
Key is working with Radiology (Options of imaging locally) Communication with patients and documentation is important No delay in HCC treatment (riskbenefits discussion)
httpswwwaasldorgsitesdefaultfiles2020-05AASLD-COVID19-ClinicalInsights-May42020
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
Fibroscan Not urgent but planning to
start June-July 2020 Huge back log Using radiology US protocol
for PPE (maskgoogles and gown) Flexible schedules based on
safety guidelines
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
httpsdoiorg1011012020050620092999
HR adjusted for all other factors listed other than ethnicity
o Largest cohort study to date evaluating a variety of clinical factors for death from COVID-19
o Asians and blacks appear to be at increased risk of in-hospital death with only partial attribution to pre-existing clinical risk factors or deprivation
o Patients with pre-existing liver disease transplantation or on immunosuppression appear to have increased risk of in-hospital death when adjusted for agesex alone or fully adjusted
o Strengthsbull Largest cohort study to date representing 40 English populationbull Inclusion of variables including liver disease transplant for analysis
o Weaknessesbull Deaths related to patients with false-negative tests or died without testing would be missedbull Censoring patients at date of death from other causes or outside the hospital stopped 9
days short of study end bull Cohort limited to those practices using the EHR software SystmOne Some variable were
assumed absent if missing bull Characterization of ldquoliver diseaserdquo is general and not complete
o Further characterization of liver disease and potential risks due to etiology MELD etc will be helpful in future studies
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORGhttpsdoiorg1011012020050620092999
Expert Panel Consensus Statement
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 26
o First published online March 23rdo New update posted today
wwwaasldorgcovid19o Spanish and Portuguese
translations available onlineo Hepatology manuscript published
online
May 14th Update Major Changes
o Acknowledgement of possible link between COVID-19 and Kawasaki-like pediatric multisystem inflammatory syndrome
o Italian autopsy series describing involvement of hepatic vasculature including acute portal and sinusoidal thrombosis
o Introduction of SARS-CoV-2 antigen testing in addition to increasing availability of antibody testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 27
httpswwwhealthnygovpressreleases2020docs2020-05-06_covid19_pediatric_inflammatory_syndromepdfSonzogni et al Preprints 2020httpswwwfdagovnews-eventspress-announcementscoronavirus-covid-19-update-fda-authorizes-first-antigen-test-help-rapid-detection-virus-causes
May 14th Update Major Changes
o OpenSAFELY study from the UK chronic liver disease is a risk factor for in-hospital death from COVID-19
o Large US study also showed that chronic liver disease and cirrhosis are associated with higher COVID-19 mortality
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 28
Williamson et al MedRxiv 2020Singh and Khan Gastroenterol 2020
May 14th Update Major Changes
o Clarification that treatment of hepatitis B is not contraindicated in patients with or without COVID-19
o Recommendations regarding use of masks for patients and caregivers as well as providers in the clinic or hospital setting
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 29
May 14th Update Major Changes
o Evolving data on hydroxychloroquine suggesting it should no longer be used outside RCTs
o New data on triple therapy with lopinavir-ritonavir ribavirin and interferon-beta-1b showing more rapid viral clearance compared to lopinavir-ritonavir (phase 2 RCT)
o Reentry
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 30
Geleris et al N Eng J Med 2020Hung et al Lancet 2020
31
Impact of COVID-19 on Liver Disease Safe Outpatient Re-Entry Process
Bilal Hameed MDAssociate Professor of Medicine
Clinic Chief Hepatology University of California San Francisco
Outline
The COVID-19 effects on liver care Recommendations for re-entry and re-opening facilities Ambulatory re-entry and recovery challenges and plan
at UCSF Gradual re-entry of liver patients in the ambulatory
setting
The Untold Toll mdash The Pandemicrsquos Effects on Patients without COVID-19
httpswwwnejmorgdoifull101056NEJMms2009984query=featured_coronavirus
Patients with heart attacks strokes and even appendicitis vanish from
hospitals
The Pandemicrsquos Effects on Patients without COVID-1938 reduction in STEMI activations in the US
during COVID-19 pandemic
Garcia S et al Journal of the American College of Cardiology April 2020
Decrease in routine pediatric vaccination during COVID-19
httpswwwcdcgovmmwrvolumes69wr
Unexpected Consequences of the Pandemic
To expand capacity for COVID-19 patients on March 18th CMS recommended limiting non-essential care and procedures 8 week pause in usual care activities Fear of returning to care Change in patientrsquos perception of riskbenefit
Areas with lowstable incidence of COVID-19 CMS allowing non-emergent non-COVID-19 healthcare
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdf
COVID-19 Pandemic Impact on the Cirrhosis Care
Tapper EB et al Journal of Hepatology April 2020
COVID Surge
Loss of insurance
Outpatient Impact of COVID-19 Pandemic UCSF Experience Maximizing Appropriate Use of Video Visits during Re-entry
Prior State Current State Future State~20 of total visits were video visits
~95 of total visits are video visits
Appropriate mix of telehealth visits ~50
Continue expanding to -Patients that live far away -Post-ops amp post-discharge follow-up-Chronic disease management(NAFLDHBVHCV etc)-Free up clinic space
0
10000
20000
30000
40000
50000
60000
70000
End of April Double March volume
February 2 of all visits2nd largest video visit program in the
country among AMCs largest in California
End of March 60 of visits
UCSF Video Visits by Month (Jan 2015-April 2020)
0
100
200
300
400
500
600
700
800
900
Jul 2019 Aug Sep Oct Nov Dec Jan 2020 Feb Mar Apr
Able to see the same number of patients even during pandemic
Hepatology Video Visits by Month at UCSF
CMS Phase I Recommendations Re-opening Facilities for Non-emergent Non-COVID-19 Healthcare
In coordination with State and local public health officials evaluate the incidence and trends for COVID-19 in the area
Prioritize surgicalprocedural care and high-complexity chronic disease management and select preventive services
Consider establishing Non-COVID Care (NCC) zones that would screen all patients for symptoms of COVID-19
Sufficient resources should be available across phases of care including PPE healthy workforce testing capacity etc and without jeopardizing surge capacity
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdfhttpswwwwhitehousegovopeningamericacriteriahttpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
httpsdatasfgovorgstoriessdak2-gvuj
San Francisco COVID-19 Numbers
Ambulatory Re-entry and Recovery ndash Cascaded Principles
Ensure morbidity and mortality do not increase due to liver related illness and provide care in a safe manner
Continue to prioritize the health and safety of workforce Prioritize urgent patients Communicate consistently and transparently Invest appropriately in services and improvement efforts
Strategies to limit unnecessary exposure while continuing to provide high-quality care for our liver patients
bull Optimization and flexibility of schedules (hoursweekend)
bull Utilization of clinic spacebull Sustain telehealth bull Digital technology for symptoms
monitoring bull Staff redeployment
bull COVID symptoms check protocolbull Social distancing in clinicbull Masking and safety policiesbull Waiting rooms changesbull Visitor policies
bull Prioritize urgent patientsbull Back log data and referralsbull Pre-clinic communicationbull In clinic flow (Echeck in rooming
and check out policies)
bull Patient communication is the keybull Staff anxiety and stress reduction bull Focus on vulnerable populationbull Physician burn out and health needs bull Trainees re-entry and education
Staff and PatientSafety
Clinic Work Flows
Resource Utilization
Support and
Education
PatientCare
Ambulatory Recovery Challenges and PlanProviding Best Care While Living with COVID-19
Physical Distancing amp Safety Guidelines
Conversa Employee Screening Mychart Screener Apex texting for patients in
nearby waiting areas
Innovation and Improving Operations
Gradual Re-entry of Liver Patients in the Ambulatory Setting
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
Patient will be scheduled for modified evaluation with
Hepatology and social worker as video visit
Remainder of evaluation will be onsite when restrictions are lifted
1 Pre-clinicarrival COVID screening for patientscaregiver2 Universal masking
no
Re-entry of Liver Patients in Clinic June 2020
All new liver transplant evaluations and HCC diagnosis New decompensation or worsening symptoms Listed patients for transplant with decompensated cirrhosis Acute hepatitis or liver injury Early post transplant Patients with difficulty with telehealth
Re-entry of Liver Patients HCC Surveillance HCC surveillance should continue as close to schedule (an
arbitrary delay of 2 months were acceptable) Working on list of all delayed imaging and prioritizing them by
risk categoriesKnown HCC surveillance for treatment response elevated AFP
Key is working with Radiology (Options of imaging locally) Communication with patients and documentation is important No delay in HCC treatment (riskbenefits discussion)
httpswwwaasldorgsitesdefaultfiles2020-05AASLD-COVID19-ClinicalInsights-May42020
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
Fibroscan Not urgent but planning to
start June-July 2020 Huge back log Using radiology US protocol
for PPE (maskgoogles and gown) Flexible schedules based on
safety guidelines
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

o Largest cohort study to date evaluating a variety of clinical factors for death from COVID-19
o Asians and blacks appear to be at increased risk of in-hospital death with only partial attribution to pre-existing clinical risk factors or deprivation
o Patients with pre-existing liver disease transplantation or on immunosuppression appear to have increased risk of in-hospital death when adjusted for agesex alone or fully adjusted
o Strengthsbull Largest cohort study to date representing 40 English populationbull Inclusion of variables including liver disease transplant for analysis
o Weaknessesbull Deaths related to patients with false-negative tests or died without testing would be missedbull Censoring patients at date of death from other causes or outside the hospital stopped 9
days short of study end bull Cohort limited to those practices using the EHR software SystmOne Some variable were
assumed absent if missing bull Characterization of ldquoliver diseaserdquo is general and not complete
o Further characterization of liver disease and potential risks due to etiology MELD etc will be helpful in future studies
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORGhttpsdoiorg1011012020050620092999
Expert Panel Consensus Statement
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 26
o First published online March 23rdo New update posted today
wwwaasldorgcovid19o Spanish and Portuguese
translations available onlineo Hepatology manuscript published
online
May 14th Update Major Changes
o Acknowledgement of possible link between COVID-19 and Kawasaki-like pediatric multisystem inflammatory syndrome
o Italian autopsy series describing involvement of hepatic vasculature including acute portal and sinusoidal thrombosis
o Introduction of SARS-CoV-2 antigen testing in addition to increasing availability of antibody testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 27
httpswwwhealthnygovpressreleases2020docs2020-05-06_covid19_pediatric_inflammatory_syndromepdfSonzogni et al Preprints 2020httpswwwfdagovnews-eventspress-announcementscoronavirus-covid-19-update-fda-authorizes-first-antigen-test-help-rapid-detection-virus-causes
May 14th Update Major Changes
o OpenSAFELY study from the UK chronic liver disease is a risk factor for in-hospital death from COVID-19
o Large US study also showed that chronic liver disease and cirrhosis are associated with higher COVID-19 mortality
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 28
Williamson et al MedRxiv 2020Singh and Khan Gastroenterol 2020
May 14th Update Major Changes
o Clarification that treatment of hepatitis B is not contraindicated in patients with or without COVID-19
o Recommendations regarding use of masks for patients and caregivers as well as providers in the clinic or hospital setting
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 29
May 14th Update Major Changes
o Evolving data on hydroxychloroquine suggesting it should no longer be used outside RCTs
o New data on triple therapy with lopinavir-ritonavir ribavirin and interferon-beta-1b showing more rapid viral clearance compared to lopinavir-ritonavir (phase 2 RCT)
o Reentry
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 30
Geleris et al N Eng J Med 2020Hung et al Lancet 2020
31
Impact of COVID-19 on Liver Disease Safe Outpatient Re-Entry Process
Bilal Hameed MDAssociate Professor of Medicine
Clinic Chief Hepatology University of California San Francisco
Outline
The COVID-19 effects on liver care Recommendations for re-entry and re-opening facilities Ambulatory re-entry and recovery challenges and plan
at UCSF Gradual re-entry of liver patients in the ambulatory
setting
The Untold Toll mdash The Pandemicrsquos Effects on Patients without COVID-19
httpswwwnejmorgdoifull101056NEJMms2009984query=featured_coronavirus
Patients with heart attacks strokes and even appendicitis vanish from
hospitals
The Pandemicrsquos Effects on Patients without COVID-1938 reduction in STEMI activations in the US
during COVID-19 pandemic
Garcia S et al Journal of the American College of Cardiology April 2020
Decrease in routine pediatric vaccination during COVID-19
httpswwwcdcgovmmwrvolumes69wr
Unexpected Consequences of the Pandemic
To expand capacity for COVID-19 patients on March 18th CMS recommended limiting non-essential care and procedures 8 week pause in usual care activities Fear of returning to care Change in patientrsquos perception of riskbenefit
Areas with lowstable incidence of COVID-19 CMS allowing non-emergent non-COVID-19 healthcare
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdf
COVID-19 Pandemic Impact on the Cirrhosis Care
Tapper EB et al Journal of Hepatology April 2020
COVID Surge
Loss of insurance
Outpatient Impact of COVID-19 Pandemic UCSF Experience Maximizing Appropriate Use of Video Visits during Re-entry
Prior State Current State Future State~20 of total visits were video visits
~95 of total visits are video visits
Appropriate mix of telehealth visits ~50
Continue expanding to -Patients that live far away -Post-ops amp post-discharge follow-up-Chronic disease management(NAFLDHBVHCV etc)-Free up clinic space
0
10000
20000
30000
40000
50000
60000
70000
End of April Double March volume
February 2 of all visits2nd largest video visit program in the
country among AMCs largest in California
End of March 60 of visits
UCSF Video Visits by Month (Jan 2015-April 2020)
0
100
200
300
400
500
600
700
800
900
Jul 2019 Aug Sep Oct Nov Dec Jan 2020 Feb Mar Apr
Able to see the same number of patients even during pandemic
Hepatology Video Visits by Month at UCSF
CMS Phase I Recommendations Re-opening Facilities for Non-emergent Non-COVID-19 Healthcare
In coordination with State and local public health officials evaluate the incidence and trends for COVID-19 in the area
Prioritize surgicalprocedural care and high-complexity chronic disease management and select preventive services
Consider establishing Non-COVID Care (NCC) zones that would screen all patients for symptoms of COVID-19
Sufficient resources should be available across phases of care including PPE healthy workforce testing capacity etc and without jeopardizing surge capacity
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdfhttpswwwwhitehousegovopeningamericacriteriahttpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
httpsdatasfgovorgstoriessdak2-gvuj
San Francisco COVID-19 Numbers
Ambulatory Re-entry and Recovery ndash Cascaded Principles
Ensure morbidity and mortality do not increase due to liver related illness and provide care in a safe manner
Continue to prioritize the health and safety of workforce Prioritize urgent patients Communicate consistently and transparently Invest appropriately in services and improvement efforts
Strategies to limit unnecessary exposure while continuing to provide high-quality care for our liver patients
bull Optimization and flexibility of schedules (hoursweekend)
bull Utilization of clinic spacebull Sustain telehealth bull Digital technology for symptoms
monitoring bull Staff redeployment
bull COVID symptoms check protocolbull Social distancing in clinicbull Masking and safety policiesbull Waiting rooms changesbull Visitor policies
bull Prioritize urgent patientsbull Back log data and referralsbull Pre-clinic communicationbull In clinic flow (Echeck in rooming
and check out policies)
bull Patient communication is the keybull Staff anxiety and stress reduction bull Focus on vulnerable populationbull Physician burn out and health needs bull Trainees re-entry and education
Staff and PatientSafety
Clinic Work Flows
Resource Utilization
Support and
Education
PatientCare
Ambulatory Recovery Challenges and PlanProviding Best Care While Living with COVID-19
Physical Distancing amp Safety Guidelines
Conversa Employee Screening Mychart Screener Apex texting for patients in
nearby waiting areas
Innovation and Improving Operations
Gradual Re-entry of Liver Patients in the Ambulatory Setting
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
Patient will be scheduled for modified evaluation with
Hepatology and social worker as video visit
Remainder of evaluation will be onsite when restrictions are lifted
1 Pre-clinicarrival COVID screening for patientscaregiver2 Universal masking
no
Re-entry of Liver Patients in Clinic June 2020
All new liver transplant evaluations and HCC diagnosis New decompensation or worsening symptoms Listed patients for transplant with decompensated cirrhosis Acute hepatitis or liver injury Early post transplant Patients with difficulty with telehealth
Re-entry of Liver Patients HCC Surveillance HCC surveillance should continue as close to schedule (an
arbitrary delay of 2 months were acceptable) Working on list of all delayed imaging and prioritizing them by
risk categoriesKnown HCC surveillance for treatment response elevated AFP
Key is working with Radiology (Options of imaging locally) Communication with patients and documentation is important No delay in HCC treatment (riskbenefits discussion)
httpswwwaasldorgsitesdefaultfiles2020-05AASLD-COVID19-ClinicalInsights-May42020
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
Fibroscan Not urgent but planning to
start June-July 2020 Huge back log Using radiology US protocol
for PPE (maskgoogles and gown) Flexible schedules based on
safety guidelines
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

Expert Panel Consensus Statement
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 26
o First published online March 23rdo New update posted today
wwwaasldorgcovid19o Spanish and Portuguese
translations available onlineo Hepatology manuscript published
online
May 14th Update Major Changes
o Acknowledgement of possible link between COVID-19 and Kawasaki-like pediatric multisystem inflammatory syndrome
o Italian autopsy series describing involvement of hepatic vasculature including acute portal and sinusoidal thrombosis
o Introduction of SARS-CoV-2 antigen testing in addition to increasing availability of antibody testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 27
httpswwwhealthnygovpressreleases2020docs2020-05-06_covid19_pediatric_inflammatory_syndromepdfSonzogni et al Preprints 2020httpswwwfdagovnews-eventspress-announcementscoronavirus-covid-19-update-fda-authorizes-first-antigen-test-help-rapid-detection-virus-causes
May 14th Update Major Changes
o OpenSAFELY study from the UK chronic liver disease is a risk factor for in-hospital death from COVID-19
o Large US study also showed that chronic liver disease and cirrhosis are associated with higher COVID-19 mortality
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 28
Williamson et al MedRxiv 2020Singh and Khan Gastroenterol 2020
May 14th Update Major Changes
o Clarification that treatment of hepatitis B is not contraindicated in patients with or without COVID-19
o Recommendations regarding use of masks for patients and caregivers as well as providers in the clinic or hospital setting
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 29
May 14th Update Major Changes
o Evolving data on hydroxychloroquine suggesting it should no longer be used outside RCTs
o New data on triple therapy with lopinavir-ritonavir ribavirin and interferon-beta-1b showing more rapid viral clearance compared to lopinavir-ritonavir (phase 2 RCT)
o Reentry
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 30
Geleris et al N Eng J Med 2020Hung et al Lancet 2020
31
Impact of COVID-19 on Liver Disease Safe Outpatient Re-Entry Process
Bilal Hameed MDAssociate Professor of Medicine
Clinic Chief Hepatology University of California San Francisco
Outline
The COVID-19 effects on liver care Recommendations for re-entry and re-opening facilities Ambulatory re-entry and recovery challenges and plan
at UCSF Gradual re-entry of liver patients in the ambulatory
setting
The Untold Toll mdash The Pandemicrsquos Effects on Patients without COVID-19
httpswwwnejmorgdoifull101056NEJMms2009984query=featured_coronavirus
Patients with heart attacks strokes and even appendicitis vanish from
hospitals
The Pandemicrsquos Effects on Patients without COVID-1938 reduction in STEMI activations in the US
during COVID-19 pandemic
Garcia S et al Journal of the American College of Cardiology April 2020
Decrease in routine pediatric vaccination during COVID-19
httpswwwcdcgovmmwrvolumes69wr
Unexpected Consequences of the Pandemic
To expand capacity for COVID-19 patients on March 18th CMS recommended limiting non-essential care and procedures 8 week pause in usual care activities Fear of returning to care Change in patientrsquos perception of riskbenefit
Areas with lowstable incidence of COVID-19 CMS allowing non-emergent non-COVID-19 healthcare
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdf
COVID-19 Pandemic Impact on the Cirrhosis Care
Tapper EB et al Journal of Hepatology April 2020
COVID Surge
Loss of insurance
Outpatient Impact of COVID-19 Pandemic UCSF Experience Maximizing Appropriate Use of Video Visits during Re-entry
Prior State Current State Future State~20 of total visits were video visits
~95 of total visits are video visits
Appropriate mix of telehealth visits ~50
Continue expanding to -Patients that live far away -Post-ops amp post-discharge follow-up-Chronic disease management(NAFLDHBVHCV etc)-Free up clinic space
0
10000
20000
30000
40000
50000
60000
70000
End of April Double March volume
February 2 of all visits2nd largest video visit program in the
country among AMCs largest in California
End of March 60 of visits
UCSF Video Visits by Month (Jan 2015-April 2020)
0
100
200
300
400
500
600
700
800
900
Jul 2019 Aug Sep Oct Nov Dec Jan 2020 Feb Mar Apr
Able to see the same number of patients even during pandemic
Hepatology Video Visits by Month at UCSF
CMS Phase I Recommendations Re-opening Facilities for Non-emergent Non-COVID-19 Healthcare
In coordination with State and local public health officials evaluate the incidence and trends for COVID-19 in the area
Prioritize surgicalprocedural care and high-complexity chronic disease management and select preventive services
Consider establishing Non-COVID Care (NCC) zones that would screen all patients for symptoms of COVID-19
Sufficient resources should be available across phases of care including PPE healthy workforce testing capacity etc and without jeopardizing surge capacity
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdfhttpswwwwhitehousegovopeningamericacriteriahttpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
httpsdatasfgovorgstoriessdak2-gvuj
San Francisco COVID-19 Numbers
Ambulatory Re-entry and Recovery ndash Cascaded Principles
Ensure morbidity and mortality do not increase due to liver related illness and provide care in a safe manner
Continue to prioritize the health and safety of workforce Prioritize urgent patients Communicate consistently and transparently Invest appropriately in services and improvement efforts
Strategies to limit unnecessary exposure while continuing to provide high-quality care for our liver patients
bull Optimization and flexibility of schedules (hoursweekend)
bull Utilization of clinic spacebull Sustain telehealth bull Digital technology for symptoms
monitoring bull Staff redeployment
bull COVID symptoms check protocolbull Social distancing in clinicbull Masking and safety policiesbull Waiting rooms changesbull Visitor policies
bull Prioritize urgent patientsbull Back log data and referralsbull Pre-clinic communicationbull In clinic flow (Echeck in rooming
and check out policies)
bull Patient communication is the keybull Staff anxiety and stress reduction bull Focus on vulnerable populationbull Physician burn out and health needs bull Trainees re-entry and education
Staff and PatientSafety
Clinic Work Flows
Resource Utilization
Support and
Education
PatientCare
Ambulatory Recovery Challenges and PlanProviding Best Care While Living with COVID-19
Physical Distancing amp Safety Guidelines
Conversa Employee Screening Mychart Screener Apex texting for patients in
nearby waiting areas
Innovation and Improving Operations
Gradual Re-entry of Liver Patients in the Ambulatory Setting
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
Patient will be scheduled for modified evaluation with
Hepatology and social worker as video visit
Remainder of evaluation will be onsite when restrictions are lifted
1 Pre-clinicarrival COVID screening for patientscaregiver2 Universal masking
no
Re-entry of Liver Patients in Clinic June 2020
All new liver transplant evaluations and HCC diagnosis New decompensation or worsening symptoms Listed patients for transplant with decompensated cirrhosis Acute hepatitis or liver injury Early post transplant Patients with difficulty with telehealth
Re-entry of Liver Patients HCC Surveillance HCC surveillance should continue as close to schedule (an
arbitrary delay of 2 months were acceptable) Working on list of all delayed imaging and prioritizing them by
risk categoriesKnown HCC surveillance for treatment response elevated AFP
Key is working with Radiology (Options of imaging locally) Communication with patients and documentation is important No delay in HCC treatment (riskbenefits discussion)
httpswwwaasldorgsitesdefaultfiles2020-05AASLD-COVID19-ClinicalInsights-May42020
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
Fibroscan Not urgent but planning to
start June-July 2020 Huge back log Using radiology US protocol
for PPE (maskgoogles and gown) Flexible schedules based on
safety guidelines
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

May 14th Update Major Changes
o Acknowledgement of possible link between COVID-19 and Kawasaki-like pediatric multisystem inflammatory syndrome
o Italian autopsy series describing involvement of hepatic vasculature including acute portal and sinusoidal thrombosis
o Introduction of SARS-CoV-2 antigen testing in addition to increasing availability of antibody testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 27
httpswwwhealthnygovpressreleases2020docs2020-05-06_covid19_pediatric_inflammatory_syndromepdfSonzogni et al Preprints 2020httpswwwfdagovnews-eventspress-announcementscoronavirus-covid-19-update-fda-authorizes-first-antigen-test-help-rapid-detection-virus-causes
May 14th Update Major Changes
o OpenSAFELY study from the UK chronic liver disease is a risk factor for in-hospital death from COVID-19
o Large US study also showed that chronic liver disease and cirrhosis are associated with higher COVID-19 mortality
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 28
Williamson et al MedRxiv 2020Singh and Khan Gastroenterol 2020
May 14th Update Major Changes
o Clarification that treatment of hepatitis B is not contraindicated in patients with or without COVID-19
o Recommendations regarding use of masks for patients and caregivers as well as providers in the clinic or hospital setting
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 29
May 14th Update Major Changes
o Evolving data on hydroxychloroquine suggesting it should no longer be used outside RCTs
o New data on triple therapy with lopinavir-ritonavir ribavirin and interferon-beta-1b showing more rapid viral clearance compared to lopinavir-ritonavir (phase 2 RCT)
o Reentry
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 30
Geleris et al N Eng J Med 2020Hung et al Lancet 2020
31
Impact of COVID-19 on Liver Disease Safe Outpatient Re-Entry Process
Bilal Hameed MDAssociate Professor of Medicine
Clinic Chief Hepatology University of California San Francisco
Outline
The COVID-19 effects on liver care Recommendations for re-entry and re-opening facilities Ambulatory re-entry and recovery challenges and plan
at UCSF Gradual re-entry of liver patients in the ambulatory
setting
The Untold Toll mdash The Pandemicrsquos Effects on Patients without COVID-19
httpswwwnejmorgdoifull101056NEJMms2009984query=featured_coronavirus
Patients with heart attacks strokes and even appendicitis vanish from
hospitals
The Pandemicrsquos Effects on Patients without COVID-1938 reduction in STEMI activations in the US
during COVID-19 pandemic
Garcia S et al Journal of the American College of Cardiology April 2020
Decrease in routine pediatric vaccination during COVID-19
httpswwwcdcgovmmwrvolumes69wr
Unexpected Consequences of the Pandemic
To expand capacity for COVID-19 patients on March 18th CMS recommended limiting non-essential care and procedures 8 week pause in usual care activities Fear of returning to care Change in patientrsquos perception of riskbenefit
Areas with lowstable incidence of COVID-19 CMS allowing non-emergent non-COVID-19 healthcare
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdf
COVID-19 Pandemic Impact on the Cirrhosis Care
Tapper EB et al Journal of Hepatology April 2020
COVID Surge
Loss of insurance
Outpatient Impact of COVID-19 Pandemic UCSF Experience Maximizing Appropriate Use of Video Visits during Re-entry
Prior State Current State Future State~20 of total visits were video visits
~95 of total visits are video visits
Appropriate mix of telehealth visits ~50
Continue expanding to -Patients that live far away -Post-ops amp post-discharge follow-up-Chronic disease management(NAFLDHBVHCV etc)-Free up clinic space
0
10000
20000
30000
40000
50000
60000
70000
End of April Double March volume
February 2 of all visits2nd largest video visit program in the
country among AMCs largest in California
End of March 60 of visits
UCSF Video Visits by Month (Jan 2015-April 2020)
0
100
200
300
400
500
600
700
800
900
Jul 2019 Aug Sep Oct Nov Dec Jan 2020 Feb Mar Apr
Able to see the same number of patients even during pandemic
Hepatology Video Visits by Month at UCSF
CMS Phase I Recommendations Re-opening Facilities for Non-emergent Non-COVID-19 Healthcare
In coordination with State and local public health officials evaluate the incidence and trends for COVID-19 in the area
Prioritize surgicalprocedural care and high-complexity chronic disease management and select preventive services
Consider establishing Non-COVID Care (NCC) zones that would screen all patients for symptoms of COVID-19
Sufficient resources should be available across phases of care including PPE healthy workforce testing capacity etc and without jeopardizing surge capacity
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdfhttpswwwwhitehousegovopeningamericacriteriahttpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
httpsdatasfgovorgstoriessdak2-gvuj
San Francisco COVID-19 Numbers
Ambulatory Re-entry and Recovery ndash Cascaded Principles
Ensure morbidity and mortality do not increase due to liver related illness and provide care in a safe manner
Continue to prioritize the health and safety of workforce Prioritize urgent patients Communicate consistently and transparently Invest appropriately in services and improvement efforts
Strategies to limit unnecessary exposure while continuing to provide high-quality care for our liver patients
bull Optimization and flexibility of schedules (hoursweekend)
bull Utilization of clinic spacebull Sustain telehealth bull Digital technology for symptoms
monitoring bull Staff redeployment
bull COVID symptoms check protocolbull Social distancing in clinicbull Masking and safety policiesbull Waiting rooms changesbull Visitor policies
bull Prioritize urgent patientsbull Back log data and referralsbull Pre-clinic communicationbull In clinic flow (Echeck in rooming
and check out policies)
bull Patient communication is the keybull Staff anxiety and stress reduction bull Focus on vulnerable populationbull Physician burn out and health needs bull Trainees re-entry and education
Staff and PatientSafety
Clinic Work Flows
Resource Utilization
Support and
Education
PatientCare
Ambulatory Recovery Challenges and PlanProviding Best Care While Living with COVID-19
Physical Distancing amp Safety Guidelines
Conversa Employee Screening Mychart Screener Apex texting for patients in
nearby waiting areas
Innovation and Improving Operations
Gradual Re-entry of Liver Patients in the Ambulatory Setting
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
Patient will be scheduled for modified evaluation with
Hepatology and social worker as video visit
Remainder of evaluation will be onsite when restrictions are lifted
1 Pre-clinicarrival COVID screening for patientscaregiver2 Universal masking
no
Re-entry of Liver Patients in Clinic June 2020
All new liver transplant evaluations and HCC diagnosis New decompensation or worsening symptoms Listed patients for transplant with decompensated cirrhosis Acute hepatitis or liver injury Early post transplant Patients with difficulty with telehealth
Re-entry of Liver Patients HCC Surveillance HCC surveillance should continue as close to schedule (an
arbitrary delay of 2 months were acceptable) Working on list of all delayed imaging and prioritizing them by
risk categoriesKnown HCC surveillance for treatment response elevated AFP
Key is working with Radiology (Options of imaging locally) Communication with patients and documentation is important No delay in HCC treatment (riskbenefits discussion)
httpswwwaasldorgsitesdefaultfiles2020-05AASLD-COVID19-ClinicalInsights-May42020
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
Fibroscan Not urgent but planning to
start June-July 2020 Huge back log Using radiology US protocol
for PPE (maskgoogles and gown) Flexible schedules based on
safety guidelines
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

May 14th Update Major Changes
o OpenSAFELY study from the UK chronic liver disease is a risk factor for in-hospital death from COVID-19
o Large US study also showed that chronic liver disease and cirrhosis are associated with higher COVID-19 mortality
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 28
Williamson et al MedRxiv 2020Singh and Khan Gastroenterol 2020
May 14th Update Major Changes
o Clarification that treatment of hepatitis B is not contraindicated in patients with or without COVID-19
o Recommendations regarding use of masks for patients and caregivers as well as providers in the clinic or hospital setting
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 29
May 14th Update Major Changes
o Evolving data on hydroxychloroquine suggesting it should no longer be used outside RCTs
o New data on triple therapy with lopinavir-ritonavir ribavirin and interferon-beta-1b showing more rapid viral clearance compared to lopinavir-ritonavir (phase 2 RCT)
o Reentry
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 30
Geleris et al N Eng J Med 2020Hung et al Lancet 2020
31
Impact of COVID-19 on Liver Disease Safe Outpatient Re-Entry Process
Bilal Hameed MDAssociate Professor of Medicine
Clinic Chief Hepatology University of California San Francisco
Outline
The COVID-19 effects on liver care Recommendations for re-entry and re-opening facilities Ambulatory re-entry and recovery challenges and plan
at UCSF Gradual re-entry of liver patients in the ambulatory
setting
The Untold Toll mdash The Pandemicrsquos Effects on Patients without COVID-19
httpswwwnejmorgdoifull101056NEJMms2009984query=featured_coronavirus
Patients with heart attacks strokes and even appendicitis vanish from
hospitals
The Pandemicrsquos Effects on Patients without COVID-1938 reduction in STEMI activations in the US
during COVID-19 pandemic
Garcia S et al Journal of the American College of Cardiology April 2020
Decrease in routine pediatric vaccination during COVID-19
httpswwwcdcgovmmwrvolumes69wr
Unexpected Consequences of the Pandemic
To expand capacity for COVID-19 patients on March 18th CMS recommended limiting non-essential care and procedures 8 week pause in usual care activities Fear of returning to care Change in patientrsquos perception of riskbenefit
Areas with lowstable incidence of COVID-19 CMS allowing non-emergent non-COVID-19 healthcare
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdf
COVID-19 Pandemic Impact on the Cirrhosis Care
Tapper EB et al Journal of Hepatology April 2020
COVID Surge
Loss of insurance
Outpatient Impact of COVID-19 Pandemic UCSF Experience Maximizing Appropriate Use of Video Visits during Re-entry
Prior State Current State Future State~20 of total visits were video visits
~95 of total visits are video visits
Appropriate mix of telehealth visits ~50
Continue expanding to -Patients that live far away -Post-ops amp post-discharge follow-up-Chronic disease management(NAFLDHBVHCV etc)-Free up clinic space
0
10000
20000
30000
40000
50000
60000
70000
End of April Double March volume
February 2 of all visits2nd largest video visit program in the
country among AMCs largest in California
End of March 60 of visits
UCSF Video Visits by Month (Jan 2015-April 2020)
0
100
200
300
400
500
600
700
800
900
Jul 2019 Aug Sep Oct Nov Dec Jan 2020 Feb Mar Apr
Able to see the same number of patients even during pandemic
Hepatology Video Visits by Month at UCSF
CMS Phase I Recommendations Re-opening Facilities for Non-emergent Non-COVID-19 Healthcare
In coordination with State and local public health officials evaluate the incidence and trends for COVID-19 in the area
Prioritize surgicalprocedural care and high-complexity chronic disease management and select preventive services
Consider establishing Non-COVID Care (NCC) zones that would screen all patients for symptoms of COVID-19
Sufficient resources should be available across phases of care including PPE healthy workforce testing capacity etc and without jeopardizing surge capacity
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdfhttpswwwwhitehousegovopeningamericacriteriahttpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
httpsdatasfgovorgstoriessdak2-gvuj
San Francisco COVID-19 Numbers
Ambulatory Re-entry and Recovery ndash Cascaded Principles
Ensure morbidity and mortality do not increase due to liver related illness and provide care in a safe manner
Continue to prioritize the health and safety of workforce Prioritize urgent patients Communicate consistently and transparently Invest appropriately in services and improvement efforts
Strategies to limit unnecessary exposure while continuing to provide high-quality care for our liver patients
bull Optimization and flexibility of schedules (hoursweekend)
bull Utilization of clinic spacebull Sustain telehealth bull Digital technology for symptoms
monitoring bull Staff redeployment
bull COVID symptoms check protocolbull Social distancing in clinicbull Masking and safety policiesbull Waiting rooms changesbull Visitor policies
bull Prioritize urgent patientsbull Back log data and referralsbull Pre-clinic communicationbull In clinic flow (Echeck in rooming
and check out policies)
bull Patient communication is the keybull Staff anxiety and stress reduction bull Focus on vulnerable populationbull Physician burn out and health needs bull Trainees re-entry and education
Staff and PatientSafety
Clinic Work Flows
Resource Utilization
Support and
Education
PatientCare
Ambulatory Recovery Challenges and PlanProviding Best Care While Living with COVID-19
Physical Distancing amp Safety Guidelines
Conversa Employee Screening Mychart Screener Apex texting for patients in
nearby waiting areas
Innovation and Improving Operations
Gradual Re-entry of Liver Patients in the Ambulatory Setting
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
Patient will be scheduled for modified evaluation with
Hepatology and social worker as video visit
Remainder of evaluation will be onsite when restrictions are lifted
1 Pre-clinicarrival COVID screening for patientscaregiver2 Universal masking
no
Re-entry of Liver Patients in Clinic June 2020
All new liver transplant evaluations and HCC diagnosis New decompensation or worsening symptoms Listed patients for transplant with decompensated cirrhosis Acute hepatitis or liver injury Early post transplant Patients with difficulty with telehealth
Re-entry of Liver Patients HCC Surveillance HCC surveillance should continue as close to schedule (an
arbitrary delay of 2 months were acceptable) Working on list of all delayed imaging and prioritizing them by
risk categoriesKnown HCC surveillance for treatment response elevated AFP
Key is working with Radiology (Options of imaging locally) Communication with patients and documentation is important No delay in HCC treatment (riskbenefits discussion)
httpswwwaasldorgsitesdefaultfiles2020-05AASLD-COVID19-ClinicalInsights-May42020
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
Fibroscan Not urgent but planning to
start June-July 2020 Huge back log Using radiology US protocol
for PPE (maskgoogles and gown) Flexible schedules based on
safety guidelines
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

May 14th Update Major Changes
o Clarification that treatment of hepatitis B is not contraindicated in patients with or without COVID-19
o Recommendations regarding use of masks for patients and caregivers as well as providers in the clinic or hospital setting
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 29
May 14th Update Major Changes
o Evolving data on hydroxychloroquine suggesting it should no longer be used outside RCTs
o New data on triple therapy with lopinavir-ritonavir ribavirin and interferon-beta-1b showing more rapid viral clearance compared to lopinavir-ritonavir (phase 2 RCT)
o Reentry
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 30
Geleris et al N Eng J Med 2020Hung et al Lancet 2020
31
Impact of COVID-19 on Liver Disease Safe Outpatient Re-Entry Process
Bilal Hameed MDAssociate Professor of Medicine
Clinic Chief Hepatology University of California San Francisco
Outline
The COVID-19 effects on liver care Recommendations for re-entry and re-opening facilities Ambulatory re-entry and recovery challenges and plan
at UCSF Gradual re-entry of liver patients in the ambulatory
setting
The Untold Toll mdash The Pandemicrsquos Effects on Patients without COVID-19
httpswwwnejmorgdoifull101056NEJMms2009984query=featured_coronavirus
Patients with heart attacks strokes and even appendicitis vanish from
hospitals
The Pandemicrsquos Effects on Patients without COVID-1938 reduction in STEMI activations in the US
during COVID-19 pandemic
Garcia S et al Journal of the American College of Cardiology April 2020
Decrease in routine pediatric vaccination during COVID-19
httpswwwcdcgovmmwrvolumes69wr
Unexpected Consequences of the Pandemic
To expand capacity for COVID-19 patients on March 18th CMS recommended limiting non-essential care and procedures 8 week pause in usual care activities Fear of returning to care Change in patientrsquos perception of riskbenefit
Areas with lowstable incidence of COVID-19 CMS allowing non-emergent non-COVID-19 healthcare
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdf
COVID-19 Pandemic Impact on the Cirrhosis Care
Tapper EB et al Journal of Hepatology April 2020
COVID Surge
Loss of insurance
Outpatient Impact of COVID-19 Pandemic UCSF Experience Maximizing Appropriate Use of Video Visits during Re-entry
Prior State Current State Future State~20 of total visits were video visits
~95 of total visits are video visits
Appropriate mix of telehealth visits ~50
Continue expanding to -Patients that live far away -Post-ops amp post-discharge follow-up-Chronic disease management(NAFLDHBVHCV etc)-Free up clinic space
0
10000
20000
30000
40000
50000
60000
70000
End of April Double March volume
February 2 of all visits2nd largest video visit program in the
country among AMCs largest in California
End of March 60 of visits
UCSF Video Visits by Month (Jan 2015-April 2020)
0
100
200
300
400
500
600
700
800
900
Jul 2019 Aug Sep Oct Nov Dec Jan 2020 Feb Mar Apr
Able to see the same number of patients even during pandemic
Hepatology Video Visits by Month at UCSF
CMS Phase I Recommendations Re-opening Facilities for Non-emergent Non-COVID-19 Healthcare
In coordination with State and local public health officials evaluate the incidence and trends for COVID-19 in the area
Prioritize surgicalprocedural care and high-complexity chronic disease management and select preventive services
Consider establishing Non-COVID Care (NCC) zones that would screen all patients for symptoms of COVID-19
Sufficient resources should be available across phases of care including PPE healthy workforce testing capacity etc and without jeopardizing surge capacity
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdfhttpswwwwhitehousegovopeningamericacriteriahttpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
httpsdatasfgovorgstoriessdak2-gvuj
San Francisco COVID-19 Numbers
Ambulatory Re-entry and Recovery ndash Cascaded Principles
Ensure morbidity and mortality do not increase due to liver related illness and provide care in a safe manner
Continue to prioritize the health and safety of workforce Prioritize urgent patients Communicate consistently and transparently Invest appropriately in services and improvement efforts
Strategies to limit unnecessary exposure while continuing to provide high-quality care for our liver patients
bull Optimization and flexibility of schedules (hoursweekend)
bull Utilization of clinic spacebull Sustain telehealth bull Digital technology for symptoms
monitoring bull Staff redeployment
bull COVID symptoms check protocolbull Social distancing in clinicbull Masking and safety policiesbull Waiting rooms changesbull Visitor policies
bull Prioritize urgent patientsbull Back log data and referralsbull Pre-clinic communicationbull In clinic flow (Echeck in rooming
and check out policies)
bull Patient communication is the keybull Staff anxiety and stress reduction bull Focus on vulnerable populationbull Physician burn out and health needs bull Trainees re-entry and education
Staff and PatientSafety
Clinic Work Flows
Resource Utilization
Support and
Education
PatientCare
Ambulatory Recovery Challenges and PlanProviding Best Care While Living with COVID-19
Physical Distancing amp Safety Guidelines
Conversa Employee Screening Mychart Screener Apex texting for patients in
nearby waiting areas
Innovation and Improving Operations
Gradual Re-entry of Liver Patients in the Ambulatory Setting
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
Patient will be scheduled for modified evaluation with
Hepatology and social worker as video visit
Remainder of evaluation will be onsite when restrictions are lifted
1 Pre-clinicarrival COVID screening for patientscaregiver2 Universal masking
no
Re-entry of Liver Patients in Clinic June 2020
All new liver transplant evaluations and HCC diagnosis New decompensation or worsening symptoms Listed patients for transplant with decompensated cirrhosis Acute hepatitis or liver injury Early post transplant Patients with difficulty with telehealth
Re-entry of Liver Patients HCC Surveillance HCC surveillance should continue as close to schedule (an
arbitrary delay of 2 months were acceptable) Working on list of all delayed imaging and prioritizing them by
risk categoriesKnown HCC surveillance for treatment response elevated AFP
Key is working with Radiology (Options of imaging locally) Communication with patients and documentation is important No delay in HCC treatment (riskbenefits discussion)
httpswwwaasldorgsitesdefaultfiles2020-05AASLD-COVID19-ClinicalInsights-May42020
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
Fibroscan Not urgent but planning to
start June-July 2020 Huge back log Using radiology US protocol
for PPE (maskgoogles and gown) Flexible schedules based on
safety guidelines
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

May 14th Update Major Changes
o Evolving data on hydroxychloroquine suggesting it should no longer be used outside RCTs
o New data on triple therapy with lopinavir-ritonavir ribavirin and interferon-beta-1b showing more rapid viral clearance compared to lopinavir-ritonavir (phase 2 RCT)
o Reentry
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG 30
Geleris et al N Eng J Med 2020Hung et al Lancet 2020
31
Impact of COVID-19 on Liver Disease Safe Outpatient Re-Entry Process
Bilal Hameed MDAssociate Professor of Medicine
Clinic Chief Hepatology University of California San Francisco
Outline
The COVID-19 effects on liver care Recommendations for re-entry and re-opening facilities Ambulatory re-entry and recovery challenges and plan
at UCSF Gradual re-entry of liver patients in the ambulatory
setting
The Untold Toll mdash The Pandemicrsquos Effects on Patients without COVID-19
httpswwwnejmorgdoifull101056NEJMms2009984query=featured_coronavirus
Patients with heart attacks strokes and even appendicitis vanish from
hospitals
The Pandemicrsquos Effects on Patients without COVID-1938 reduction in STEMI activations in the US
during COVID-19 pandemic
Garcia S et al Journal of the American College of Cardiology April 2020
Decrease in routine pediatric vaccination during COVID-19
httpswwwcdcgovmmwrvolumes69wr
Unexpected Consequences of the Pandemic
To expand capacity for COVID-19 patients on March 18th CMS recommended limiting non-essential care and procedures 8 week pause in usual care activities Fear of returning to care Change in patientrsquos perception of riskbenefit
Areas with lowstable incidence of COVID-19 CMS allowing non-emergent non-COVID-19 healthcare
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdf
COVID-19 Pandemic Impact on the Cirrhosis Care
Tapper EB et al Journal of Hepatology April 2020
COVID Surge
Loss of insurance
Outpatient Impact of COVID-19 Pandemic UCSF Experience Maximizing Appropriate Use of Video Visits during Re-entry
Prior State Current State Future State~20 of total visits were video visits
~95 of total visits are video visits
Appropriate mix of telehealth visits ~50
Continue expanding to -Patients that live far away -Post-ops amp post-discharge follow-up-Chronic disease management(NAFLDHBVHCV etc)-Free up clinic space
0
10000
20000
30000
40000
50000
60000
70000
End of April Double March volume
February 2 of all visits2nd largest video visit program in the
country among AMCs largest in California
End of March 60 of visits
UCSF Video Visits by Month (Jan 2015-April 2020)
0
100
200
300
400
500
600
700
800
900
Jul 2019 Aug Sep Oct Nov Dec Jan 2020 Feb Mar Apr
Able to see the same number of patients even during pandemic
Hepatology Video Visits by Month at UCSF
CMS Phase I Recommendations Re-opening Facilities for Non-emergent Non-COVID-19 Healthcare
In coordination with State and local public health officials evaluate the incidence and trends for COVID-19 in the area
Prioritize surgicalprocedural care and high-complexity chronic disease management and select preventive services
Consider establishing Non-COVID Care (NCC) zones that would screen all patients for symptoms of COVID-19
Sufficient resources should be available across phases of care including PPE healthy workforce testing capacity etc and without jeopardizing surge capacity
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdfhttpswwwwhitehousegovopeningamericacriteriahttpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
httpsdatasfgovorgstoriessdak2-gvuj
San Francisco COVID-19 Numbers
Ambulatory Re-entry and Recovery ndash Cascaded Principles
Ensure morbidity and mortality do not increase due to liver related illness and provide care in a safe manner
Continue to prioritize the health and safety of workforce Prioritize urgent patients Communicate consistently and transparently Invest appropriately in services and improvement efforts
Strategies to limit unnecessary exposure while continuing to provide high-quality care for our liver patients
bull Optimization and flexibility of schedules (hoursweekend)
bull Utilization of clinic spacebull Sustain telehealth bull Digital technology for symptoms
monitoring bull Staff redeployment
bull COVID symptoms check protocolbull Social distancing in clinicbull Masking and safety policiesbull Waiting rooms changesbull Visitor policies
bull Prioritize urgent patientsbull Back log data and referralsbull Pre-clinic communicationbull In clinic flow (Echeck in rooming
and check out policies)
bull Patient communication is the keybull Staff anxiety and stress reduction bull Focus on vulnerable populationbull Physician burn out and health needs bull Trainees re-entry and education
Staff and PatientSafety
Clinic Work Flows
Resource Utilization
Support and
Education
PatientCare
Ambulatory Recovery Challenges and PlanProviding Best Care While Living with COVID-19
Physical Distancing amp Safety Guidelines
Conversa Employee Screening Mychart Screener Apex texting for patients in
nearby waiting areas
Innovation and Improving Operations
Gradual Re-entry of Liver Patients in the Ambulatory Setting
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
Patient will be scheduled for modified evaluation with
Hepatology and social worker as video visit
Remainder of evaluation will be onsite when restrictions are lifted
1 Pre-clinicarrival COVID screening for patientscaregiver2 Universal masking
no
Re-entry of Liver Patients in Clinic June 2020
All new liver transplant evaluations and HCC diagnosis New decompensation or worsening symptoms Listed patients for transplant with decompensated cirrhosis Acute hepatitis or liver injury Early post transplant Patients with difficulty with telehealth
Re-entry of Liver Patients HCC Surveillance HCC surveillance should continue as close to schedule (an
arbitrary delay of 2 months were acceptable) Working on list of all delayed imaging and prioritizing them by
risk categoriesKnown HCC surveillance for treatment response elevated AFP
Key is working with Radiology (Options of imaging locally) Communication with patients and documentation is important No delay in HCC treatment (riskbenefits discussion)
httpswwwaasldorgsitesdefaultfiles2020-05AASLD-COVID19-ClinicalInsights-May42020
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
Fibroscan Not urgent but planning to
start June-July 2020 Huge back log Using radiology US protocol
for PPE (maskgoogles and gown) Flexible schedules based on
safety guidelines
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

31
Impact of COVID-19 on Liver Disease Safe Outpatient Re-Entry Process
Bilal Hameed MDAssociate Professor of Medicine
Clinic Chief Hepatology University of California San Francisco
Outline
The COVID-19 effects on liver care Recommendations for re-entry and re-opening facilities Ambulatory re-entry and recovery challenges and plan
at UCSF Gradual re-entry of liver patients in the ambulatory
setting
The Untold Toll mdash The Pandemicrsquos Effects on Patients without COVID-19
httpswwwnejmorgdoifull101056NEJMms2009984query=featured_coronavirus
Patients with heart attacks strokes and even appendicitis vanish from
hospitals
The Pandemicrsquos Effects on Patients without COVID-1938 reduction in STEMI activations in the US
during COVID-19 pandemic
Garcia S et al Journal of the American College of Cardiology April 2020
Decrease in routine pediatric vaccination during COVID-19
httpswwwcdcgovmmwrvolumes69wr
Unexpected Consequences of the Pandemic
To expand capacity for COVID-19 patients on March 18th CMS recommended limiting non-essential care and procedures 8 week pause in usual care activities Fear of returning to care Change in patientrsquos perception of riskbenefit
Areas with lowstable incidence of COVID-19 CMS allowing non-emergent non-COVID-19 healthcare
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdf
COVID-19 Pandemic Impact on the Cirrhosis Care
Tapper EB et al Journal of Hepatology April 2020
COVID Surge
Loss of insurance
Outpatient Impact of COVID-19 Pandemic UCSF Experience Maximizing Appropriate Use of Video Visits during Re-entry
Prior State Current State Future State~20 of total visits were video visits
~95 of total visits are video visits
Appropriate mix of telehealth visits ~50
Continue expanding to -Patients that live far away -Post-ops amp post-discharge follow-up-Chronic disease management(NAFLDHBVHCV etc)-Free up clinic space
0
10000
20000
30000
40000
50000
60000
70000
End of April Double March volume
February 2 of all visits2nd largest video visit program in the
country among AMCs largest in California
End of March 60 of visits
UCSF Video Visits by Month (Jan 2015-April 2020)
0
100
200
300
400
500
600
700
800
900
Jul 2019 Aug Sep Oct Nov Dec Jan 2020 Feb Mar Apr
Able to see the same number of patients even during pandemic
Hepatology Video Visits by Month at UCSF
CMS Phase I Recommendations Re-opening Facilities for Non-emergent Non-COVID-19 Healthcare
In coordination with State and local public health officials evaluate the incidence and trends for COVID-19 in the area
Prioritize surgicalprocedural care and high-complexity chronic disease management and select preventive services
Consider establishing Non-COVID Care (NCC) zones that would screen all patients for symptoms of COVID-19
Sufficient resources should be available across phases of care including PPE healthy workforce testing capacity etc and without jeopardizing surge capacity
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdfhttpswwwwhitehousegovopeningamericacriteriahttpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
httpsdatasfgovorgstoriessdak2-gvuj
San Francisco COVID-19 Numbers
Ambulatory Re-entry and Recovery ndash Cascaded Principles
Ensure morbidity and mortality do not increase due to liver related illness and provide care in a safe manner
Continue to prioritize the health and safety of workforce Prioritize urgent patients Communicate consistently and transparently Invest appropriately in services and improvement efforts
Strategies to limit unnecessary exposure while continuing to provide high-quality care for our liver patients
bull Optimization and flexibility of schedules (hoursweekend)
bull Utilization of clinic spacebull Sustain telehealth bull Digital technology for symptoms
monitoring bull Staff redeployment
bull COVID symptoms check protocolbull Social distancing in clinicbull Masking and safety policiesbull Waiting rooms changesbull Visitor policies
bull Prioritize urgent patientsbull Back log data and referralsbull Pre-clinic communicationbull In clinic flow (Echeck in rooming
and check out policies)
bull Patient communication is the keybull Staff anxiety and stress reduction bull Focus on vulnerable populationbull Physician burn out and health needs bull Trainees re-entry and education
Staff and PatientSafety
Clinic Work Flows
Resource Utilization
Support and
Education
PatientCare
Ambulatory Recovery Challenges and PlanProviding Best Care While Living with COVID-19
Physical Distancing amp Safety Guidelines
Conversa Employee Screening Mychart Screener Apex texting for patients in
nearby waiting areas
Innovation and Improving Operations
Gradual Re-entry of Liver Patients in the Ambulatory Setting
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
Patient will be scheduled for modified evaluation with
Hepatology and social worker as video visit
Remainder of evaluation will be onsite when restrictions are lifted
1 Pre-clinicarrival COVID screening for patientscaregiver2 Universal masking
no
Re-entry of Liver Patients in Clinic June 2020
All new liver transplant evaluations and HCC diagnosis New decompensation or worsening symptoms Listed patients for transplant with decompensated cirrhosis Acute hepatitis or liver injury Early post transplant Patients with difficulty with telehealth
Re-entry of Liver Patients HCC Surveillance HCC surveillance should continue as close to schedule (an
arbitrary delay of 2 months were acceptable) Working on list of all delayed imaging and prioritizing them by
risk categoriesKnown HCC surveillance for treatment response elevated AFP
Key is working with Radiology (Options of imaging locally) Communication with patients and documentation is important No delay in HCC treatment (riskbenefits discussion)
httpswwwaasldorgsitesdefaultfiles2020-05AASLD-COVID19-ClinicalInsights-May42020
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
Fibroscan Not urgent but planning to
start June-July 2020 Huge back log Using radiology US protocol
for PPE (maskgoogles and gown) Flexible schedules based on
safety guidelines
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

Outline
The COVID-19 effects on liver care Recommendations for re-entry and re-opening facilities Ambulatory re-entry and recovery challenges and plan
at UCSF Gradual re-entry of liver patients in the ambulatory
setting
The Untold Toll mdash The Pandemicrsquos Effects on Patients without COVID-19
httpswwwnejmorgdoifull101056NEJMms2009984query=featured_coronavirus
Patients with heart attacks strokes and even appendicitis vanish from
hospitals
The Pandemicrsquos Effects on Patients without COVID-1938 reduction in STEMI activations in the US
during COVID-19 pandemic
Garcia S et al Journal of the American College of Cardiology April 2020
Decrease in routine pediatric vaccination during COVID-19
httpswwwcdcgovmmwrvolumes69wr
Unexpected Consequences of the Pandemic
To expand capacity for COVID-19 patients on March 18th CMS recommended limiting non-essential care and procedures 8 week pause in usual care activities Fear of returning to care Change in patientrsquos perception of riskbenefit
Areas with lowstable incidence of COVID-19 CMS allowing non-emergent non-COVID-19 healthcare
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdf
COVID-19 Pandemic Impact on the Cirrhosis Care
Tapper EB et al Journal of Hepatology April 2020
COVID Surge
Loss of insurance
Outpatient Impact of COVID-19 Pandemic UCSF Experience Maximizing Appropriate Use of Video Visits during Re-entry
Prior State Current State Future State~20 of total visits were video visits
~95 of total visits are video visits
Appropriate mix of telehealth visits ~50
Continue expanding to -Patients that live far away -Post-ops amp post-discharge follow-up-Chronic disease management(NAFLDHBVHCV etc)-Free up clinic space
0
10000
20000
30000
40000
50000
60000
70000
End of April Double March volume
February 2 of all visits2nd largest video visit program in the
country among AMCs largest in California
End of March 60 of visits
UCSF Video Visits by Month (Jan 2015-April 2020)
0
100
200
300
400
500
600
700
800
900
Jul 2019 Aug Sep Oct Nov Dec Jan 2020 Feb Mar Apr
Able to see the same number of patients even during pandemic
Hepatology Video Visits by Month at UCSF
CMS Phase I Recommendations Re-opening Facilities for Non-emergent Non-COVID-19 Healthcare
In coordination with State and local public health officials evaluate the incidence and trends for COVID-19 in the area
Prioritize surgicalprocedural care and high-complexity chronic disease management and select preventive services
Consider establishing Non-COVID Care (NCC) zones that would screen all patients for symptoms of COVID-19
Sufficient resources should be available across phases of care including PPE healthy workforce testing capacity etc and without jeopardizing surge capacity
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdfhttpswwwwhitehousegovopeningamericacriteriahttpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
httpsdatasfgovorgstoriessdak2-gvuj
San Francisco COVID-19 Numbers
Ambulatory Re-entry and Recovery ndash Cascaded Principles
Ensure morbidity and mortality do not increase due to liver related illness and provide care in a safe manner
Continue to prioritize the health and safety of workforce Prioritize urgent patients Communicate consistently and transparently Invest appropriately in services and improvement efforts
Strategies to limit unnecessary exposure while continuing to provide high-quality care for our liver patients
bull Optimization and flexibility of schedules (hoursweekend)
bull Utilization of clinic spacebull Sustain telehealth bull Digital technology for symptoms
monitoring bull Staff redeployment
bull COVID symptoms check protocolbull Social distancing in clinicbull Masking and safety policiesbull Waiting rooms changesbull Visitor policies
bull Prioritize urgent patientsbull Back log data and referralsbull Pre-clinic communicationbull In clinic flow (Echeck in rooming
and check out policies)
bull Patient communication is the keybull Staff anxiety and stress reduction bull Focus on vulnerable populationbull Physician burn out and health needs bull Trainees re-entry and education
Staff and PatientSafety
Clinic Work Flows
Resource Utilization
Support and
Education
PatientCare
Ambulatory Recovery Challenges and PlanProviding Best Care While Living with COVID-19
Physical Distancing amp Safety Guidelines
Conversa Employee Screening Mychart Screener Apex texting for patients in
nearby waiting areas
Innovation and Improving Operations
Gradual Re-entry of Liver Patients in the Ambulatory Setting
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
Patient will be scheduled for modified evaluation with
Hepatology and social worker as video visit
Remainder of evaluation will be onsite when restrictions are lifted
1 Pre-clinicarrival COVID screening for patientscaregiver2 Universal masking
no
Re-entry of Liver Patients in Clinic June 2020
All new liver transplant evaluations and HCC diagnosis New decompensation or worsening symptoms Listed patients for transplant with decompensated cirrhosis Acute hepatitis or liver injury Early post transplant Patients with difficulty with telehealth
Re-entry of Liver Patients HCC Surveillance HCC surveillance should continue as close to schedule (an
arbitrary delay of 2 months were acceptable) Working on list of all delayed imaging and prioritizing them by
risk categoriesKnown HCC surveillance for treatment response elevated AFP
Key is working with Radiology (Options of imaging locally) Communication with patients and documentation is important No delay in HCC treatment (riskbenefits discussion)
httpswwwaasldorgsitesdefaultfiles2020-05AASLD-COVID19-ClinicalInsights-May42020
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
Fibroscan Not urgent but planning to
start June-July 2020 Huge back log Using radiology US protocol
for PPE (maskgoogles and gown) Flexible schedules based on
safety guidelines
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

The Untold Toll mdash The Pandemicrsquos Effects on Patients without COVID-19
httpswwwnejmorgdoifull101056NEJMms2009984query=featured_coronavirus
Patients with heart attacks strokes and even appendicitis vanish from
hospitals
The Pandemicrsquos Effects on Patients without COVID-1938 reduction in STEMI activations in the US
during COVID-19 pandemic
Garcia S et al Journal of the American College of Cardiology April 2020
Decrease in routine pediatric vaccination during COVID-19
httpswwwcdcgovmmwrvolumes69wr
Unexpected Consequences of the Pandemic
To expand capacity for COVID-19 patients on March 18th CMS recommended limiting non-essential care and procedures 8 week pause in usual care activities Fear of returning to care Change in patientrsquos perception of riskbenefit
Areas with lowstable incidence of COVID-19 CMS allowing non-emergent non-COVID-19 healthcare
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdf
COVID-19 Pandemic Impact on the Cirrhosis Care
Tapper EB et al Journal of Hepatology April 2020
COVID Surge
Loss of insurance
Outpatient Impact of COVID-19 Pandemic UCSF Experience Maximizing Appropriate Use of Video Visits during Re-entry
Prior State Current State Future State~20 of total visits were video visits
~95 of total visits are video visits
Appropriate mix of telehealth visits ~50
Continue expanding to -Patients that live far away -Post-ops amp post-discharge follow-up-Chronic disease management(NAFLDHBVHCV etc)-Free up clinic space
0
10000
20000
30000
40000
50000
60000
70000
End of April Double March volume
February 2 of all visits2nd largest video visit program in the
country among AMCs largest in California
End of March 60 of visits
UCSF Video Visits by Month (Jan 2015-April 2020)
0
100
200
300
400
500
600
700
800
900
Jul 2019 Aug Sep Oct Nov Dec Jan 2020 Feb Mar Apr
Able to see the same number of patients even during pandemic
Hepatology Video Visits by Month at UCSF
CMS Phase I Recommendations Re-opening Facilities for Non-emergent Non-COVID-19 Healthcare
In coordination with State and local public health officials evaluate the incidence and trends for COVID-19 in the area
Prioritize surgicalprocedural care and high-complexity chronic disease management and select preventive services
Consider establishing Non-COVID Care (NCC) zones that would screen all patients for symptoms of COVID-19
Sufficient resources should be available across phases of care including PPE healthy workforce testing capacity etc and without jeopardizing surge capacity
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdfhttpswwwwhitehousegovopeningamericacriteriahttpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
httpsdatasfgovorgstoriessdak2-gvuj
San Francisco COVID-19 Numbers
Ambulatory Re-entry and Recovery ndash Cascaded Principles
Ensure morbidity and mortality do not increase due to liver related illness and provide care in a safe manner
Continue to prioritize the health and safety of workforce Prioritize urgent patients Communicate consistently and transparently Invest appropriately in services and improvement efforts
Strategies to limit unnecessary exposure while continuing to provide high-quality care for our liver patients
bull Optimization and flexibility of schedules (hoursweekend)
bull Utilization of clinic spacebull Sustain telehealth bull Digital technology for symptoms
monitoring bull Staff redeployment
bull COVID symptoms check protocolbull Social distancing in clinicbull Masking and safety policiesbull Waiting rooms changesbull Visitor policies
bull Prioritize urgent patientsbull Back log data and referralsbull Pre-clinic communicationbull In clinic flow (Echeck in rooming
and check out policies)
bull Patient communication is the keybull Staff anxiety and stress reduction bull Focus on vulnerable populationbull Physician burn out and health needs bull Trainees re-entry and education
Staff and PatientSafety
Clinic Work Flows
Resource Utilization
Support and
Education
PatientCare
Ambulatory Recovery Challenges and PlanProviding Best Care While Living with COVID-19
Physical Distancing amp Safety Guidelines
Conversa Employee Screening Mychart Screener Apex texting for patients in
nearby waiting areas
Innovation and Improving Operations
Gradual Re-entry of Liver Patients in the Ambulatory Setting
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
Patient will be scheduled for modified evaluation with
Hepatology and social worker as video visit
Remainder of evaluation will be onsite when restrictions are lifted
1 Pre-clinicarrival COVID screening for patientscaregiver2 Universal masking
no
Re-entry of Liver Patients in Clinic June 2020
All new liver transplant evaluations and HCC diagnosis New decompensation or worsening symptoms Listed patients for transplant with decompensated cirrhosis Acute hepatitis or liver injury Early post transplant Patients with difficulty with telehealth
Re-entry of Liver Patients HCC Surveillance HCC surveillance should continue as close to schedule (an
arbitrary delay of 2 months were acceptable) Working on list of all delayed imaging and prioritizing them by
risk categoriesKnown HCC surveillance for treatment response elevated AFP
Key is working with Radiology (Options of imaging locally) Communication with patients and documentation is important No delay in HCC treatment (riskbenefits discussion)
httpswwwaasldorgsitesdefaultfiles2020-05AASLD-COVID19-ClinicalInsights-May42020
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
Fibroscan Not urgent but planning to
start June-July 2020 Huge back log Using radiology US protocol
for PPE (maskgoogles and gown) Flexible schedules based on
safety guidelines
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

The Pandemicrsquos Effects on Patients without COVID-1938 reduction in STEMI activations in the US
during COVID-19 pandemic
Garcia S et al Journal of the American College of Cardiology April 2020
Decrease in routine pediatric vaccination during COVID-19
httpswwwcdcgovmmwrvolumes69wr
Unexpected Consequences of the Pandemic
To expand capacity for COVID-19 patients on March 18th CMS recommended limiting non-essential care and procedures 8 week pause in usual care activities Fear of returning to care Change in patientrsquos perception of riskbenefit
Areas with lowstable incidence of COVID-19 CMS allowing non-emergent non-COVID-19 healthcare
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdf
COVID-19 Pandemic Impact on the Cirrhosis Care
Tapper EB et al Journal of Hepatology April 2020
COVID Surge
Loss of insurance
Outpatient Impact of COVID-19 Pandemic UCSF Experience Maximizing Appropriate Use of Video Visits during Re-entry
Prior State Current State Future State~20 of total visits were video visits
~95 of total visits are video visits
Appropriate mix of telehealth visits ~50
Continue expanding to -Patients that live far away -Post-ops amp post-discharge follow-up-Chronic disease management(NAFLDHBVHCV etc)-Free up clinic space
0
10000
20000
30000
40000
50000
60000
70000
End of April Double March volume
February 2 of all visits2nd largest video visit program in the
country among AMCs largest in California
End of March 60 of visits
UCSF Video Visits by Month (Jan 2015-April 2020)
0
100
200
300
400
500
600
700
800
900
Jul 2019 Aug Sep Oct Nov Dec Jan 2020 Feb Mar Apr
Able to see the same number of patients even during pandemic
Hepatology Video Visits by Month at UCSF
CMS Phase I Recommendations Re-opening Facilities for Non-emergent Non-COVID-19 Healthcare
In coordination with State and local public health officials evaluate the incidence and trends for COVID-19 in the area
Prioritize surgicalprocedural care and high-complexity chronic disease management and select preventive services
Consider establishing Non-COVID Care (NCC) zones that would screen all patients for symptoms of COVID-19
Sufficient resources should be available across phases of care including PPE healthy workforce testing capacity etc and without jeopardizing surge capacity
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdfhttpswwwwhitehousegovopeningamericacriteriahttpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
httpsdatasfgovorgstoriessdak2-gvuj
San Francisco COVID-19 Numbers
Ambulatory Re-entry and Recovery ndash Cascaded Principles
Ensure morbidity and mortality do not increase due to liver related illness and provide care in a safe manner
Continue to prioritize the health and safety of workforce Prioritize urgent patients Communicate consistently and transparently Invest appropriately in services and improvement efforts
Strategies to limit unnecessary exposure while continuing to provide high-quality care for our liver patients
bull Optimization and flexibility of schedules (hoursweekend)
bull Utilization of clinic spacebull Sustain telehealth bull Digital technology for symptoms
monitoring bull Staff redeployment
bull COVID symptoms check protocolbull Social distancing in clinicbull Masking and safety policiesbull Waiting rooms changesbull Visitor policies
bull Prioritize urgent patientsbull Back log data and referralsbull Pre-clinic communicationbull In clinic flow (Echeck in rooming
and check out policies)
bull Patient communication is the keybull Staff anxiety and stress reduction bull Focus on vulnerable populationbull Physician burn out and health needs bull Trainees re-entry and education
Staff and PatientSafety
Clinic Work Flows
Resource Utilization
Support and
Education
PatientCare
Ambulatory Recovery Challenges and PlanProviding Best Care While Living with COVID-19
Physical Distancing amp Safety Guidelines
Conversa Employee Screening Mychart Screener Apex texting for patients in
nearby waiting areas
Innovation and Improving Operations
Gradual Re-entry of Liver Patients in the Ambulatory Setting
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
Patient will be scheduled for modified evaluation with
Hepatology and social worker as video visit
Remainder of evaluation will be onsite when restrictions are lifted
1 Pre-clinicarrival COVID screening for patientscaregiver2 Universal masking
no
Re-entry of Liver Patients in Clinic June 2020
All new liver transplant evaluations and HCC diagnosis New decompensation or worsening symptoms Listed patients for transplant with decompensated cirrhosis Acute hepatitis or liver injury Early post transplant Patients with difficulty with telehealth
Re-entry of Liver Patients HCC Surveillance HCC surveillance should continue as close to schedule (an
arbitrary delay of 2 months were acceptable) Working on list of all delayed imaging and prioritizing them by
risk categoriesKnown HCC surveillance for treatment response elevated AFP
Key is working with Radiology (Options of imaging locally) Communication with patients and documentation is important No delay in HCC treatment (riskbenefits discussion)
httpswwwaasldorgsitesdefaultfiles2020-05AASLD-COVID19-ClinicalInsights-May42020
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
Fibroscan Not urgent but planning to
start June-July 2020 Huge back log Using radiology US protocol
for PPE (maskgoogles and gown) Flexible schedules based on
safety guidelines
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

Unexpected Consequences of the Pandemic
To expand capacity for COVID-19 patients on March 18th CMS recommended limiting non-essential care and procedures 8 week pause in usual care activities Fear of returning to care Change in patientrsquos perception of riskbenefit
Areas with lowstable incidence of COVID-19 CMS allowing non-emergent non-COVID-19 healthcare
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdf
COVID-19 Pandemic Impact on the Cirrhosis Care
Tapper EB et al Journal of Hepatology April 2020
COVID Surge
Loss of insurance
Outpatient Impact of COVID-19 Pandemic UCSF Experience Maximizing Appropriate Use of Video Visits during Re-entry
Prior State Current State Future State~20 of total visits were video visits
~95 of total visits are video visits
Appropriate mix of telehealth visits ~50
Continue expanding to -Patients that live far away -Post-ops amp post-discharge follow-up-Chronic disease management(NAFLDHBVHCV etc)-Free up clinic space
0
10000
20000
30000
40000
50000
60000
70000
End of April Double March volume
February 2 of all visits2nd largest video visit program in the
country among AMCs largest in California
End of March 60 of visits
UCSF Video Visits by Month (Jan 2015-April 2020)
0
100
200
300
400
500
600
700
800
900
Jul 2019 Aug Sep Oct Nov Dec Jan 2020 Feb Mar Apr
Able to see the same number of patients even during pandemic
Hepatology Video Visits by Month at UCSF
CMS Phase I Recommendations Re-opening Facilities for Non-emergent Non-COVID-19 Healthcare
In coordination with State and local public health officials evaluate the incidence and trends for COVID-19 in the area
Prioritize surgicalprocedural care and high-complexity chronic disease management and select preventive services
Consider establishing Non-COVID Care (NCC) zones that would screen all patients for symptoms of COVID-19
Sufficient resources should be available across phases of care including PPE healthy workforce testing capacity etc and without jeopardizing surge capacity
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdfhttpswwwwhitehousegovopeningamericacriteriahttpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
httpsdatasfgovorgstoriessdak2-gvuj
San Francisco COVID-19 Numbers
Ambulatory Re-entry and Recovery ndash Cascaded Principles
Ensure morbidity and mortality do not increase due to liver related illness and provide care in a safe manner
Continue to prioritize the health and safety of workforce Prioritize urgent patients Communicate consistently and transparently Invest appropriately in services and improvement efforts
Strategies to limit unnecessary exposure while continuing to provide high-quality care for our liver patients
bull Optimization and flexibility of schedules (hoursweekend)
bull Utilization of clinic spacebull Sustain telehealth bull Digital technology for symptoms
monitoring bull Staff redeployment
bull COVID symptoms check protocolbull Social distancing in clinicbull Masking and safety policiesbull Waiting rooms changesbull Visitor policies
bull Prioritize urgent patientsbull Back log data and referralsbull Pre-clinic communicationbull In clinic flow (Echeck in rooming
and check out policies)
bull Patient communication is the keybull Staff anxiety and stress reduction bull Focus on vulnerable populationbull Physician burn out and health needs bull Trainees re-entry and education
Staff and PatientSafety
Clinic Work Flows
Resource Utilization
Support and
Education
PatientCare
Ambulatory Recovery Challenges and PlanProviding Best Care While Living with COVID-19
Physical Distancing amp Safety Guidelines
Conversa Employee Screening Mychart Screener Apex texting for patients in
nearby waiting areas
Innovation and Improving Operations
Gradual Re-entry of Liver Patients in the Ambulatory Setting
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
Patient will be scheduled for modified evaluation with
Hepatology and social worker as video visit
Remainder of evaluation will be onsite when restrictions are lifted
1 Pre-clinicarrival COVID screening for patientscaregiver2 Universal masking
no
Re-entry of Liver Patients in Clinic June 2020
All new liver transplant evaluations and HCC diagnosis New decompensation or worsening symptoms Listed patients for transplant with decompensated cirrhosis Acute hepatitis or liver injury Early post transplant Patients with difficulty with telehealth
Re-entry of Liver Patients HCC Surveillance HCC surveillance should continue as close to schedule (an
arbitrary delay of 2 months were acceptable) Working on list of all delayed imaging and prioritizing them by
risk categoriesKnown HCC surveillance for treatment response elevated AFP
Key is working with Radiology (Options of imaging locally) Communication with patients and documentation is important No delay in HCC treatment (riskbenefits discussion)
httpswwwaasldorgsitesdefaultfiles2020-05AASLD-COVID19-ClinicalInsights-May42020
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
Fibroscan Not urgent but planning to
start June-July 2020 Huge back log Using radiology US protocol
for PPE (maskgoogles and gown) Flexible schedules based on
safety guidelines
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

COVID-19 Pandemic Impact on the Cirrhosis Care
Tapper EB et al Journal of Hepatology April 2020
COVID Surge
Loss of insurance
Outpatient Impact of COVID-19 Pandemic UCSF Experience Maximizing Appropriate Use of Video Visits during Re-entry
Prior State Current State Future State~20 of total visits were video visits
~95 of total visits are video visits
Appropriate mix of telehealth visits ~50
Continue expanding to -Patients that live far away -Post-ops amp post-discharge follow-up-Chronic disease management(NAFLDHBVHCV etc)-Free up clinic space
0
10000
20000
30000
40000
50000
60000
70000
End of April Double March volume
February 2 of all visits2nd largest video visit program in the
country among AMCs largest in California
End of March 60 of visits
UCSF Video Visits by Month (Jan 2015-April 2020)
0
100
200
300
400
500
600
700
800
900
Jul 2019 Aug Sep Oct Nov Dec Jan 2020 Feb Mar Apr
Able to see the same number of patients even during pandemic
Hepatology Video Visits by Month at UCSF
CMS Phase I Recommendations Re-opening Facilities for Non-emergent Non-COVID-19 Healthcare
In coordination with State and local public health officials evaluate the incidence and trends for COVID-19 in the area
Prioritize surgicalprocedural care and high-complexity chronic disease management and select preventive services
Consider establishing Non-COVID Care (NCC) zones that would screen all patients for symptoms of COVID-19
Sufficient resources should be available across phases of care including PPE healthy workforce testing capacity etc and without jeopardizing surge capacity
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdfhttpswwwwhitehousegovopeningamericacriteriahttpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
httpsdatasfgovorgstoriessdak2-gvuj
San Francisco COVID-19 Numbers
Ambulatory Re-entry and Recovery ndash Cascaded Principles
Ensure morbidity and mortality do not increase due to liver related illness and provide care in a safe manner
Continue to prioritize the health and safety of workforce Prioritize urgent patients Communicate consistently and transparently Invest appropriately in services and improvement efforts
Strategies to limit unnecessary exposure while continuing to provide high-quality care for our liver patients
bull Optimization and flexibility of schedules (hoursweekend)
bull Utilization of clinic spacebull Sustain telehealth bull Digital technology for symptoms
monitoring bull Staff redeployment
bull COVID symptoms check protocolbull Social distancing in clinicbull Masking and safety policiesbull Waiting rooms changesbull Visitor policies
bull Prioritize urgent patientsbull Back log data and referralsbull Pre-clinic communicationbull In clinic flow (Echeck in rooming
and check out policies)
bull Patient communication is the keybull Staff anxiety and stress reduction bull Focus on vulnerable populationbull Physician burn out and health needs bull Trainees re-entry and education
Staff and PatientSafety
Clinic Work Flows
Resource Utilization
Support and
Education
PatientCare
Ambulatory Recovery Challenges and PlanProviding Best Care While Living with COVID-19
Physical Distancing amp Safety Guidelines
Conversa Employee Screening Mychart Screener Apex texting for patients in
nearby waiting areas
Innovation and Improving Operations
Gradual Re-entry of Liver Patients in the Ambulatory Setting
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
Patient will be scheduled for modified evaluation with
Hepatology and social worker as video visit
Remainder of evaluation will be onsite when restrictions are lifted
1 Pre-clinicarrival COVID screening for patientscaregiver2 Universal masking
no
Re-entry of Liver Patients in Clinic June 2020
All new liver transplant evaluations and HCC diagnosis New decompensation or worsening symptoms Listed patients for transplant with decompensated cirrhosis Acute hepatitis or liver injury Early post transplant Patients with difficulty with telehealth
Re-entry of Liver Patients HCC Surveillance HCC surveillance should continue as close to schedule (an
arbitrary delay of 2 months were acceptable) Working on list of all delayed imaging and prioritizing them by
risk categoriesKnown HCC surveillance for treatment response elevated AFP
Key is working with Radiology (Options of imaging locally) Communication with patients and documentation is important No delay in HCC treatment (riskbenefits discussion)
httpswwwaasldorgsitesdefaultfiles2020-05AASLD-COVID19-ClinicalInsights-May42020
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
Fibroscan Not urgent but planning to
start June-July 2020 Huge back log Using radiology US protocol
for PPE (maskgoogles and gown) Flexible schedules based on
safety guidelines
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

Outpatient Impact of COVID-19 Pandemic UCSF Experience Maximizing Appropriate Use of Video Visits during Re-entry
Prior State Current State Future State~20 of total visits were video visits
~95 of total visits are video visits
Appropriate mix of telehealth visits ~50
Continue expanding to -Patients that live far away -Post-ops amp post-discharge follow-up-Chronic disease management(NAFLDHBVHCV etc)-Free up clinic space
0
10000
20000
30000
40000
50000
60000
70000
End of April Double March volume
February 2 of all visits2nd largest video visit program in the
country among AMCs largest in California
End of March 60 of visits
UCSF Video Visits by Month (Jan 2015-April 2020)
0
100
200
300
400
500
600
700
800
900
Jul 2019 Aug Sep Oct Nov Dec Jan 2020 Feb Mar Apr
Able to see the same number of patients even during pandemic
Hepatology Video Visits by Month at UCSF
CMS Phase I Recommendations Re-opening Facilities for Non-emergent Non-COVID-19 Healthcare
In coordination with State and local public health officials evaluate the incidence and trends for COVID-19 in the area
Prioritize surgicalprocedural care and high-complexity chronic disease management and select preventive services
Consider establishing Non-COVID Care (NCC) zones that would screen all patients for symptoms of COVID-19
Sufficient resources should be available across phases of care including PPE healthy workforce testing capacity etc and without jeopardizing surge capacity
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdfhttpswwwwhitehousegovopeningamericacriteriahttpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
httpsdatasfgovorgstoriessdak2-gvuj
San Francisco COVID-19 Numbers
Ambulatory Re-entry and Recovery ndash Cascaded Principles
Ensure morbidity and mortality do not increase due to liver related illness and provide care in a safe manner
Continue to prioritize the health and safety of workforce Prioritize urgent patients Communicate consistently and transparently Invest appropriately in services and improvement efforts
Strategies to limit unnecessary exposure while continuing to provide high-quality care for our liver patients
bull Optimization and flexibility of schedules (hoursweekend)
bull Utilization of clinic spacebull Sustain telehealth bull Digital technology for symptoms
monitoring bull Staff redeployment
bull COVID symptoms check protocolbull Social distancing in clinicbull Masking and safety policiesbull Waiting rooms changesbull Visitor policies
bull Prioritize urgent patientsbull Back log data and referralsbull Pre-clinic communicationbull In clinic flow (Echeck in rooming
and check out policies)
bull Patient communication is the keybull Staff anxiety and stress reduction bull Focus on vulnerable populationbull Physician burn out and health needs bull Trainees re-entry and education
Staff and PatientSafety
Clinic Work Flows
Resource Utilization
Support and
Education
PatientCare
Ambulatory Recovery Challenges and PlanProviding Best Care While Living with COVID-19
Physical Distancing amp Safety Guidelines
Conversa Employee Screening Mychart Screener Apex texting for patients in
nearby waiting areas
Innovation and Improving Operations
Gradual Re-entry of Liver Patients in the Ambulatory Setting
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
Patient will be scheduled for modified evaluation with
Hepatology and social worker as video visit
Remainder of evaluation will be onsite when restrictions are lifted
1 Pre-clinicarrival COVID screening for patientscaregiver2 Universal masking
no
Re-entry of Liver Patients in Clinic June 2020
All new liver transplant evaluations and HCC diagnosis New decompensation or worsening symptoms Listed patients for transplant with decompensated cirrhosis Acute hepatitis or liver injury Early post transplant Patients with difficulty with telehealth
Re-entry of Liver Patients HCC Surveillance HCC surveillance should continue as close to schedule (an
arbitrary delay of 2 months were acceptable) Working on list of all delayed imaging and prioritizing them by
risk categoriesKnown HCC surveillance for treatment response elevated AFP
Key is working with Radiology (Options of imaging locally) Communication with patients and documentation is important No delay in HCC treatment (riskbenefits discussion)
httpswwwaasldorgsitesdefaultfiles2020-05AASLD-COVID19-ClinicalInsights-May42020
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
Fibroscan Not urgent but planning to
start June-July 2020 Huge back log Using radiology US protocol
for PPE (maskgoogles and gown) Flexible schedules based on
safety guidelines
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

0
10000
20000
30000
40000
50000
60000
70000
End of April Double March volume
February 2 of all visits2nd largest video visit program in the
country among AMCs largest in California
End of March 60 of visits
UCSF Video Visits by Month (Jan 2015-April 2020)
0
100
200
300
400
500
600
700
800
900
Jul 2019 Aug Sep Oct Nov Dec Jan 2020 Feb Mar Apr
Able to see the same number of patients even during pandemic
Hepatology Video Visits by Month at UCSF
CMS Phase I Recommendations Re-opening Facilities for Non-emergent Non-COVID-19 Healthcare
In coordination with State and local public health officials evaluate the incidence and trends for COVID-19 in the area
Prioritize surgicalprocedural care and high-complexity chronic disease management and select preventive services
Consider establishing Non-COVID Care (NCC) zones that would screen all patients for symptoms of COVID-19
Sufficient resources should be available across phases of care including PPE healthy workforce testing capacity etc and without jeopardizing surge capacity
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdfhttpswwwwhitehousegovopeningamericacriteriahttpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
httpsdatasfgovorgstoriessdak2-gvuj
San Francisco COVID-19 Numbers
Ambulatory Re-entry and Recovery ndash Cascaded Principles
Ensure morbidity and mortality do not increase due to liver related illness and provide care in a safe manner
Continue to prioritize the health and safety of workforce Prioritize urgent patients Communicate consistently and transparently Invest appropriately in services and improvement efforts
Strategies to limit unnecessary exposure while continuing to provide high-quality care for our liver patients
bull Optimization and flexibility of schedules (hoursweekend)
bull Utilization of clinic spacebull Sustain telehealth bull Digital technology for symptoms
monitoring bull Staff redeployment
bull COVID symptoms check protocolbull Social distancing in clinicbull Masking and safety policiesbull Waiting rooms changesbull Visitor policies
bull Prioritize urgent patientsbull Back log data and referralsbull Pre-clinic communicationbull In clinic flow (Echeck in rooming
and check out policies)
bull Patient communication is the keybull Staff anxiety and stress reduction bull Focus on vulnerable populationbull Physician burn out and health needs bull Trainees re-entry and education
Staff and PatientSafety
Clinic Work Flows
Resource Utilization
Support and
Education
PatientCare
Ambulatory Recovery Challenges and PlanProviding Best Care While Living with COVID-19
Physical Distancing amp Safety Guidelines
Conversa Employee Screening Mychart Screener Apex texting for patients in
nearby waiting areas
Innovation and Improving Operations
Gradual Re-entry of Liver Patients in the Ambulatory Setting
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
Patient will be scheduled for modified evaluation with
Hepatology and social worker as video visit
Remainder of evaluation will be onsite when restrictions are lifted
1 Pre-clinicarrival COVID screening for patientscaregiver2 Universal masking
no
Re-entry of Liver Patients in Clinic June 2020
All new liver transplant evaluations and HCC diagnosis New decompensation or worsening symptoms Listed patients for transplant with decompensated cirrhosis Acute hepatitis or liver injury Early post transplant Patients with difficulty with telehealth
Re-entry of Liver Patients HCC Surveillance HCC surveillance should continue as close to schedule (an
arbitrary delay of 2 months were acceptable) Working on list of all delayed imaging and prioritizing them by
risk categoriesKnown HCC surveillance for treatment response elevated AFP
Key is working with Radiology (Options of imaging locally) Communication with patients and documentation is important No delay in HCC treatment (riskbenefits discussion)
httpswwwaasldorgsitesdefaultfiles2020-05AASLD-COVID19-ClinicalInsights-May42020
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
Fibroscan Not urgent but planning to
start June-July 2020 Huge back log Using radiology US protocol
for PPE (maskgoogles and gown) Flexible schedules based on
safety guidelines
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

0
100
200
300
400
500
600
700
800
900
Jul 2019 Aug Sep Oct Nov Dec Jan 2020 Feb Mar Apr
Able to see the same number of patients even during pandemic
Hepatology Video Visits by Month at UCSF
CMS Phase I Recommendations Re-opening Facilities for Non-emergent Non-COVID-19 Healthcare
In coordination with State and local public health officials evaluate the incidence and trends for COVID-19 in the area
Prioritize surgicalprocedural care and high-complexity chronic disease management and select preventive services
Consider establishing Non-COVID Care (NCC) zones that would screen all patients for symptoms of COVID-19
Sufficient resources should be available across phases of care including PPE healthy workforce testing capacity etc and without jeopardizing surge capacity
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdfhttpswwwwhitehousegovopeningamericacriteriahttpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
httpsdatasfgovorgstoriessdak2-gvuj
San Francisco COVID-19 Numbers
Ambulatory Re-entry and Recovery ndash Cascaded Principles
Ensure morbidity and mortality do not increase due to liver related illness and provide care in a safe manner
Continue to prioritize the health and safety of workforce Prioritize urgent patients Communicate consistently and transparently Invest appropriately in services and improvement efforts
Strategies to limit unnecessary exposure while continuing to provide high-quality care for our liver patients
bull Optimization and flexibility of schedules (hoursweekend)
bull Utilization of clinic spacebull Sustain telehealth bull Digital technology for symptoms
monitoring bull Staff redeployment
bull COVID symptoms check protocolbull Social distancing in clinicbull Masking and safety policiesbull Waiting rooms changesbull Visitor policies
bull Prioritize urgent patientsbull Back log data and referralsbull Pre-clinic communicationbull In clinic flow (Echeck in rooming
and check out policies)
bull Patient communication is the keybull Staff anxiety and stress reduction bull Focus on vulnerable populationbull Physician burn out and health needs bull Trainees re-entry and education
Staff and PatientSafety
Clinic Work Flows
Resource Utilization
Support and
Education
PatientCare
Ambulatory Recovery Challenges and PlanProviding Best Care While Living with COVID-19
Physical Distancing amp Safety Guidelines
Conversa Employee Screening Mychart Screener Apex texting for patients in
nearby waiting areas
Innovation and Improving Operations
Gradual Re-entry of Liver Patients in the Ambulatory Setting
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
Patient will be scheduled for modified evaluation with
Hepatology and social worker as video visit
Remainder of evaluation will be onsite when restrictions are lifted
1 Pre-clinicarrival COVID screening for patientscaregiver2 Universal masking
no
Re-entry of Liver Patients in Clinic June 2020
All new liver transplant evaluations and HCC diagnosis New decompensation or worsening symptoms Listed patients for transplant with decompensated cirrhosis Acute hepatitis or liver injury Early post transplant Patients with difficulty with telehealth
Re-entry of Liver Patients HCC Surveillance HCC surveillance should continue as close to schedule (an
arbitrary delay of 2 months were acceptable) Working on list of all delayed imaging and prioritizing them by
risk categoriesKnown HCC surveillance for treatment response elevated AFP
Key is working with Radiology (Options of imaging locally) Communication with patients and documentation is important No delay in HCC treatment (riskbenefits discussion)
httpswwwaasldorgsitesdefaultfiles2020-05AASLD-COVID19-ClinicalInsights-May42020
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
Fibroscan Not urgent but planning to
start June-July 2020 Huge back log Using radiology US protocol
for PPE (maskgoogles and gown) Flexible schedules based on
safety guidelines
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

CMS Phase I Recommendations Re-opening Facilities for Non-emergent Non-COVID-19 Healthcare
In coordination with State and local public health officials evaluate the incidence and trends for COVID-19 in the area
Prioritize surgicalprocedural care and high-complexity chronic disease management and select preventive services
Consider establishing Non-COVID Care (NCC) zones that would screen all patients for symptoms of COVID-19
Sufficient resources should be available across phases of care including PPE healthy workforce testing capacity etc and without jeopardizing surge capacity
httpswwwcmsgovfilesdocumentcovid-flexibility-reopen-essential-non-covid-servicespdfhttpswwwwhitehousegovopeningamericacriteriahttpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
httpsdatasfgovorgstoriessdak2-gvuj
San Francisco COVID-19 Numbers
Ambulatory Re-entry and Recovery ndash Cascaded Principles
Ensure morbidity and mortality do not increase due to liver related illness and provide care in a safe manner
Continue to prioritize the health and safety of workforce Prioritize urgent patients Communicate consistently and transparently Invest appropriately in services and improvement efforts
Strategies to limit unnecessary exposure while continuing to provide high-quality care for our liver patients
bull Optimization and flexibility of schedules (hoursweekend)
bull Utilization of clinic spacebull Sustain telehealth bull Digital technology for symptoms
monitoring bull Staff redeployment
bull COVID symptoms check protocolbull Social distancing in clinicbull Masking and safety policiesbull Waiting rooms changesbull Visitor policies
bull Prioritize urgent patientsbull Back log data and referralsbull Pre-clinic communicationbull In clinic flow (Echeck in rooming
and check out policies)
bull Patient communication is the keybull Staff anxiety and stress reduction bull Focus on vulnerable populationbull Physician burn out and health needs bull Trainees re-entry and education
Staff and PatientSafety
Clinic Work Flows
Resource Utilization
Support and
Education
PatientCare
Ambulatory Recovery Challenges and PlanProviding Best Care While Living with COVID-19
Physical Distancing amp Safety Guidelines
Conversa Employee Screening Mychart Screener Apex texting for patients in
nearby waiting areas
Innovation and Improving Operations
Gradual Re-entry of Liver Patients in the Ambulatory Setting
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
Patient will be scheduled for modified evaluation with
Hepatology and social worker as video visit
Remainder of evaluation will be onsite when restrictions are lifted
1 Pre-clinicarrival COVID screening for patientscaregiver2 Universal masking
no
Re-entry of Liver Patients in Clinic June 2020
All new liver transplant evaluations and HCC diagnosis New decompensation or worsening symptoms Listed patients for transplant with decompensated cirrhosis Acute hepatitis or liver injury Early post transplant Patients with difficulty with telehealth
Re-entry of Liver Patients HCC Surveillance HCC surveillance should continue as close to schedule (an
arbitrary delay of 2 months were acceptable) Working on list of all delayed imaging and prioritizing them by
risk categoriesKnown HCC surveillance for treatment response elevated AFP
Key is working with Radiology (Options of imaging locally) Communication with patients and documentation is important No delay in HCC treatment (riskbenefits discussion)
httpswwwaasldorgsitesdefaultfiles2020-05AASLD-COVID19-ClinicalInsights-May42020
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
Fibroscan Not urgent but planning to
start June-July 2020 Huge back log Using radiology US protocol
for PPE (maskgoogles and gown) Flexible schedules based on
safety guidelines
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

httpsdatasfgovorgstoriessdak2-gvuj
San Francisco COVID-19 Numbers
Ambulatory Re-entry and Recovery ndash Cascaded Principles
Ensure morbidity and mortality do not increase due to liver related illness and provide care in a safe manner
Continue to prioritize the health and safety of workforce Prioritize urgent patients Communicate consistently and transparently Invest appropriately in services and improvement efforts
Strategies to limit unnecessary exposure while continuing to provide high-quality care for our liver patients
bull Optimization and flexibility of schedules (hoursweekend)
bull Utilization of clinic spacebull Sustain telehealth bull Digital technology for symptoms
monitoring bull Staff redeployment
bull COVID symptoms check protocolbull Social distancing in clinicbull Masking and safety policiesbull Waiting rooms changesbull Visitor policies
bull Prioritize urgent patientsbull Back log data and referralsbull Pre-clinic communicationbull In clinic flow (Echeck in rooming
and check out policies)
bull Patient communication is the keybull Staff anxiety and stress reduction bull Focus on vulnerable populationbull Physician burn out and health needs bull Trainees re-entry and education
Staff and PatientSafety
Clinic Work Flows
Resource Utilization
Support and
Education
PatientCare
Ambulatory Recovery Challenges and PlanProviding Best Care While Living with COVID-19
Physical Distancing amp Safety Guidelines
Conversa Employee Screening Mychart Screener Apex texting for patients in
nearby waiting areas
Innovation and Improving Operations
Gradual Re-entry of Liver Patients in the Ambulatory Setting
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
Patient will be scheduled for modified evaluation with
Hepatology and social worker as video visit
Remainder of evaluation will be onsite when restrictions are lifted
1 Pre-clinicarrival COVID screening for patientscaregiver2 Universal masking
no
Re-entry of Liver Patients in Clinic June 2020
All new liver transplant evaluations and HCC diagnosis New decompensation or worsening symptoms Listed patients for transplant with decompensated cirrhosis Acute hepatitis or liver injury Early post transplant Patients with difficulty with telehealth
Re-entry of Liver Patients HCC Surveillance HCC surveillance should continue as close to schedule (an
arbitrary delay of 2 months were acceptable) Working on list of all delayed imaging and prioritizing them by
risk categoriesKnown HCC surveillance for treatment response elevated AFP
Key is working with Radiology (Options of imaging locally) Communication with patients and documentation is important No delay in HCC treatment (riskbenefits discussion)
httpswwwaasldorgsitesdefaultfiles2020-05AASLD-COVID19-ClinicalInsights-May42020
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
Fibroscan Not urgent but planning to
start June-July 2020 Huge back log Using radiology US protocol
for PPE (maskgoogles and gown) Flexible schedules based on
safety guidelines
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

Ambulatory Re-entry and Recovery ndash Cascaded Principles
Ensure morbidity and mortality do not increase due to liver related illness and provide care in a safe manner
Continue to prioritize the health and safety of workforce Prioritize urgent patients Communicate consistently and transparently Invest appropriately in services and improvement efforts
Strategies to limit unnecessary exposure while continuing to provide high-quality care for our liver patients
bull Optimization and flexibility of schedules (hoursweekend)
bull Utilization of clinic spacebull Sustain telehealth bull Digital technology for symptoms
monitoring bull Staff redeployment
bull COVID symptoms check protocolbull Social distancing in clinicbull Masking and safety policiesbull Waiting rooms changesbull Visitor policies
bull Prioritize urgent patientsbull Back log data and referralsbull Pre-clinic communicationbull In clinic flow (Echeck in rooming
and check out policies)
bull Patient communication is the keybull Staff anxiety and stress reduction bull Focus on vulnerable populationbull Physician burn out and health needs bull Trainees re-entry and education
Staff and PatientSafety
Clinic Work Flows
Resource Utilization
Support and
Education
PatientCare
Ambulatory Recovery Challenges and PlanProviding Best Care While Living with COVID-19
Physical Distancing amp Safety Guidelines
Conversa Employee Screening Mychart Screener Apex texting for patients in
nearby waiting areas
Innovation and Improving Operations
Gradual Re-entry of Liver Patients in the Ambulatory Setting
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
Patient will be scheduled for modified evaluation with
Hepatology and social worker as video visit
Remainder of evaluation will be onsite when restrictions are lifted
1 Pre-clinicarrival COVID screening for patientscaregiver2 Universal masking
no
Re-entry of Liver Patients in Clinic June 2020
All new liver transplant evaluations and HCC diagnosis New decompensation or worsening symptoms Listed patients for transplant with decompensated cirrhosis Acute hepatitis or liver injury Early post transplant Patients with difficulty with telehealth
Re-entry of Liver Patients HCC Surveillance HCC surveillance should continue as close to schedule (an
arbitrary delay of 2 months were acceptable) Working on list of all delayed imaging and prioritizing them by
risk categoriesKnown HCC surveillance for treatment response elevated AFP
Key is working with Radiology (Options of imaging locally) Communication with patients and documentation is important No delay in HCC treatment (riskbenefits discussion)
httpswwwaasldorgsitesdefaultfiles2020-05AASLD-COVID19-ClinicalInsights-May42020
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
Fibroscan Not urgent but planning to
start June-July 2020 Huge back log Using radiology US protocol
for PPE (maskgoogles and gown) Flexible schedules based on
safety guidelines
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

bull Optimization and flexibility of schedules (hoursweekend)
bull Utilization of clinic spacebull Sustain telehealth bull Digital technology for symptoms
monitoring bull Staff redeployment
bull COVID symptoms check protocolbull Social distancing in clinicbull Masking and safety policiesbull Waiting rooms changesbull Visitor policies
bull Prioritize urgent patientsbull Back log data and referralsbull Pre-clinic communicationbull In clinic flow (Echeck in rooming
and check out policies)
bull Patient communication is the keybull Staff anxiety and stress reduction bull Focus on vulnerable populationbull Physician burn out and health needs bull Trainees re-entry and education
Staff and PatientSafety
Clinic Work Flows
Resource Utilization
Support and
Education
PatientCare
Ambulatory Recovery Challenges and PlanProviding Best Care While Living with COVID-19
Physical Distancing amp Safety Guidelines
Conversa Employee Screening Mychart Screener Apex texting for patients in
nearby waiting areas
Innovation and Improving Operations
Gradual Re-entry of Liver Patients in the Ambulatory Setting
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
Patient will be scheduled for modified evaluation with
Hepatology and social worker as video visit
Remainder of evaluation will be onsite when restrictions are lifted
1 Pre-clinicarrival COVID screening for patientscaregiver2 Universal masking
no
Re-entry of Liver Patients in Clinic June 2020
All new liver transplant evaluations and HCC diagnosis New decompensation or worsening symptoms Listed patients for transplant with decompensated cirrhosis Acute hepatitis or liver injury Early post transplant Patients with difficulty with telehealth
Re-entry of Liver Patients HCC Surveillance HCC surveillance should continue as close to schedule (an
arbitrary delay of 2 months were acceptable) Working on list of all delayed imaging and prioritizing them by
risk categoriesKnown HCC surveillance for treatment response elevated AFP
Key is working with Radiology (Options of imaging locally) Communication with patients and documentation is important No delay in HCC treatment (riskbenefits discussion)
httpswwwaasldorgsitesdefaultfiles2020-05AASLD-COVID19-ClinicalInsights-May42020
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
Fibroscan Not urgent but planning to
start June-July 2020 Huge back log Using radiology US protocol
for PPE (maskgoogles and gown) Flexible schedules based on
safety guidelines
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

Physical Distancing amp Safety Guidelines
Conversa Employee Screening Mychart Screener Apex texting for patients in
nearby waiting areas
Innovation and Improving Operations
Gradual Re-entry of Liver Patients in the Ambulatory Setting
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
Patient will be scheduled for modified evaluation with
Hepatology and social worker as video visit
Remainder of evaluation will be onsite when restrictions are lifted
1 Pre-clinicarrival COVID screening for patientscaregiver2 Universal masking
no
Re-entry of Liver Patients in Clinic June 2020
All new liver transplant evaluations and HCC diagnosis New decompensation or worsening symptoms Listed patients for transplant with decompensated cirrhosis Acute hepatitis or liver injury Early post transplant Patients with difficulty with telehealth
Re-entry of Liver Patients HCC Surveillance HCC surveillance should continue as close to schedule (an
arbitrary delay of 2 months were acceptable) Working on list of all delayed imaging and prioritizing them by
risk categoriesKnown HCC surveillance for treatment response elevated AFP
Key is working with Radiology (Options of imaging locally) Communication with patients and documentation is important No delay in HCC treatment (riskbenefits discussion)
httpswwwaasldorgsitesdefaultfiles2020-05AASLD-COVID19-ClinicalInsights-May42020
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
Fibroscan Not urgent but planning to
start June-July 2020 Huge back log Using radiology US protocol
for PPE (maskgoogles and gown) Flexible schedules based on
safety guidelines
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

Conversa Employee Screening Mychart Screener Apex texting for patients in
nearby waiting areas
Innovation and Improving Operations
Gradual Re-entry of Liver Patients in the Ambulatory Setting
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
Patient will be scheduled for modified evaluation with
Hepatology and social worker as video visit
Remainder of evaluation will be onsite when restrictions are lifted
1 Pre-clinicarrival COVID screening for patientscaregiver2 Universal masking
no
Re-entry of Liver Patients in Clinic June 2020
All new liver transplant evaluations and HCC diagnosis New decompensation or worsening symptoms Listed patients for transplant with decompensated cirrhosis Acute hepatitis or liver injury Early post transplant Patients with difficulty with telehealth
Re-entry of Liver Patients HCC Surveillance HCC surveillance should continue as close to schedule (an
arbitrary delay of 2 months were acceptable) Working on list of all delayed imaging and prioritizing them by
risk categoriesKnown HCC surveillance for treatment response elevated AFP
Key is working with Radiology (Options of imaging locally) Communication with patients and documentation is important No delay in HCC treatment (riskbenefits discussion)
httpswwwaasldorgsitesdefaultfiles2020-05AASLD-COVID19-ClinicalInsights-May42020
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
Fibroscan Not urgent but planning to
start June-July 2020 Huge back log Using radiology US protocol
for PPE (maskgoogles and gown) Flexible schedules based on
safety guidelines
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

Gradual Re-entry of Liver Patients in the Ambulatory Setting
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
Patient will be scheduled for modified evaluation with
Hepatology and social worker as video visit
Remainder of evaluation will be onsite when restrictions are lifted
1 Pre-clinicarrival COVID screening for patientscaregiver2 Universal masking
no
Re-entry of Liver Patients in Clinic June 2020
All new liver transplant evaluations and HCC diagnosis New decompensation or worsening symptoms Listed patients for transplant with decompensated cirrhosis Acute hepatitis or liver injury Early post transplant Patients with difficulty with telehealth
Re-entry of Liver Patients HCC Surveillance HCC surveillance should continue as close to schedule (an
arbitrary delay of 2 months were acceptable) Working on list of all delayed imaging and prioritizing them by
risk categoriesKnown HCC surveillance for treatment response elevated AFP
Key is working with Radiology (Options of imaging locally) Communication with patients and documentation is important No delay in HCC treatment (riskbenefits discussion)
httpswwwaasldorgsitesdefaultfiles2020-05AASLD-COVID19-ClinicalInsights-May42020
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
Fibroscan Not urgent but planning to
start June-July 2020 Huge back log Using radiology US protocol
for PPE (maskgoogles and gown) Flexible schedules based on
safety guidelines
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
Patient will be scheduled for modified evaluation with
Hepatology and social worker as video visit
Remainder of evaluation will be onsite when restrictions are lifted
1 Pre-clinicarrival COVID screening for patientscaregiver2 Universal masking
no
Re-entry of Liver Patients in Clinic June 2020
All new liver transplant evaluations and HCC diagnosis New decompensation or worsening symptoms Listed patients for transplant with decompensated cirrhosis Acute hepatitis or liver injury Early post transplant Patients with difficulty with telehealth
Re-entry of Liver Patients HCC Surveillance HCC surveillance should continue as close to schedule (an
arbitrary delay of 2 months were acceptable) Working on list of all delayed imaging and prioritizing them by
risk categoriesKnown HCC surveillance for treatment response elevated AFP
Key is working with Radiology (Options of imaging locally) Communication with patients and documentation is important No delay in HCC treatment (riskbenefits discussion)
httpswwwaasldorgsitesdefaultfiles2020-05AASLD-COVID19-ClinicalInsights-May42020
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
Fibroscan Not urgent but planning to
start June-July 2020 Huge back log Using radiology US protocol
for PPE (maskgoogles and gown) Flexible schedules based on
safety guidelines
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

MELD gt24or HCCException orMELD 20-24 and any of the complications below
1) Hospitalization within the previous 3 months for any complication ndash HE volume overload SBP GI bleeding or AKI 2) Severe fluid retention requiring LVP or thoracentesis3) Records or referral indicating a potential living donorPatient will be scheduled for ON-SITE
evaluation (One care-giver allowed)
Day of evaluationPatient up for onsite video visits in clinic room
RN Education via on site video visits Hepatologist visit via onsite Zoom or in-personSurgeon visit via onsite Zoom or in-person (surgeon on campus)Labs and US on site at UCSFSocial work and Nutrition visit via onsite Zoom
yes
LIVER TRANSPLANT EVALUATION DURING COVID-19 WORKFLOW
Patient will be scheduled for modified evaluation with
Hepatology and social worker as video visit
Remainder of evaluation will be onsite when restrictions are lifted
1 Pre-clinicarrival COVID screening for patientscaregiver2 Universal masking
no
Re-entry of Liver Patients in Clinic June 2020
All new liver transplant evaluations and HCC diagnosis New decompensation or worsening symptoms Listed patients for transplant with decompensated cirrhosis Acute hepatitis or liver injury Early post transplant Patients with difficulty with telehealth
Re-entry of Liver Patients HCC Surveillance HCC surveillance should continue as close to schedule (an
arbitrary delay of 2 months were acceptable) Working on list of all delayed imaging and prioritizing them by
risk categoriesKnown HCC surveillance for treatment response elevated AFP
Key is working with Radiology (Options of imaging locally) Communication with patients and documentation is important No delay in HCC treatment (riskbenefits discussion)
httpswwwaasldorgsitesdefaultfiles2020-05AASLD-COVID19-ClinicalInsights-May42020
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
Fibroscan Not urgent but planning to
start June-July 2020 Huge back log Using radiology US protocol
for PPE (maskgoogles and gown) Flexible schedules based on
safety guidelines
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

Re-entry of Liver Patients in Clinic June 2020
All new liver transplant evaluations and HCC diagnosis New decompensation or worsening symptoms Listed patients for transplant with decompensated cirrhosis Acute hepatitis or liver injury Early post transplant Patients with difficulty with telehealth
Re-entry of Liver Patients HCC Surveillance HCC surveillance should continue as close to schedule (an
arbitrary delay of 2 months were acceptable) Working on list of all delayed imaging and prioritizing them by
risk categoriesKnown HCC surveillance for treatment response elevated AFP
Key is working with Radiology (Options of imaging locally) Communication with patients and documentation is important No delay in HCC treatment (riskbenefits discussion)
httpswwwaasldorgsitesdefaultfiles2020-05AASLD-COVID19-ClinicalInsights-May42020
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
Fibroscan Not urgent but planning to
start June-July 2020 Huge back log Using radiology US protocol
for PPE (maskgoogles and gown) Flexible schedules based on
safety guidelines
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

Re-entry of Liver Patients HCC Surveillance HCC surveillance should continue as close to schedule (an
arbitrary delay of 2 months were acceptable) Working on list of all delayed imaging and prioritizing them by
risk categoriesKnown HCC surveillance for treatment response elevated AFP
Key is working with Radiology (Options of imaging locally) Communication with patients and documentation is important No delay in HCC treatment (riskbenefits discussion)
httpswwwaasldorgsitesdefaultfiles2020-05AASLD-COVID19-ClinicalInsights-May42020
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
Fibroscan Not urgent but planning to
start June-July 2020 Huge back log Using radiology US protocol
for PPE (maskgoogles and gown) Flexible schedules based on
safety guidelines
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
Fibroscan Not urgent but planning to
start June-July 2020 Huge back log Using radiology US protocol
for PPE (maskgoogles and gown) Flexible schedules based on
safety guidelines
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

Liver Biopsies Rule out rejection or
autoimmune hepatitis diagnosis Going over the back log and
prioritizing biopsies (June 2020) Updating radiology protocols No COVID testing for outpatient
biopsies (standard PPE)
Fibroscan Not urgent but planning to
start June-July 2020 Huge back log Using radiology US protocol
for PPE (maskgoogles and gown) Flexible schedules based on
safety guidelines
httpswwwfacsorgcovid-19legislative-regulatoryexecutive-orders
Re-entry of Liver Patients Procedures
54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

54
Reentry and Return to a Pre-Pandemic StateInpatient Setting
Patricia Harren DNP DCCClinical Director of Transplant ServicesColumbia University Medical Center
o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

o Institutions are under major financial constraints due to the lack of operative and ambulatory services
o Increased cost of supplies and overtime staffingo Increase need for expensive equipment Bedsventilatorso Increase in laboratory expenses for testing
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

o Over Capacity Strugglesbull Emergency Departmentbull ICU (NYP 422 to 970 beds in 19 days)
bull OR suites still needed for ICU patientsbull Entire units still a mix of ICU and Step down patientsbull COVID Free ICU needed
bull Dialysis both CVVH and HD staffing and supply issues bull Beds
bull Still high volume of COVID patients admittedbull Step down need for trached patientsbull Increased need for rehab bedsbull ldquoField Hospitalrdquo patients need disposition
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

o PPE improving but still shortagesbull NYS Governor ldquosuggestionmandaterdquo
Institutions need a stockpile of 90 supply of all PPE equal to the amount used at PEAK
Masks100000day = 9000000 in reserve PLUS current needs met
This is compounded by increased prices and low availability
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

o Transplant Cases 2019-2020
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

o OR Schedule Restart
bull OR suites converted back from ICU to ORbull COVID Free ICU and Units bull Rapid COVID testing needed for aerosolized proceduresbull Operational Radiology Department bull Operational Interventional Radiologybull Operational Cardiac Catherization Lab
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

o COVID Testing bull Currently COVID negative needed within 48 hours bull Rapid PCR Test (2 hours) prior to procedures regardless of if
aerosolizedbull Consider Rapid testing for all elective admissions and
transfers (hold in ED until testing results)
bull Broader testing in the coming weeks to months needed to monitor for outbreaks
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

o Staffingbull Many redeployed employees from outpatient areas staffing
units due to increased acuity still neededbull Increase number of travel staffbull Units no longer specialized bull Employee PCR amp Antibody testing When and how often
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

o Visitation Policybull Current State No visitors permitted unless on Palliative Care
unit for end of life visitbull Patients hesitating to come to ED or Admission bull Struggles with staff contacting families bull Discharge coordination sometimes difficult
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

o Lessons Learnedbull Start with more restrictions and more protection and reduce as
data indicatesbull Limited Visitorsbull More testing of staffbull More testing not just with symptomsbull Testing non COVID inpatients periodically especially prior to
proceduresbull Secure your valuable PPEbull Increase of Telemedicine is valuable and needed
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

o How to make patients feel safe to returnbull Project confidence bull People respond to tangibles
bull Screening at entrancesbull Wearing masks - every one all the timebull Doing testing pre admissionpre proceduresbull Observing good hand hygienebull Being consistent
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

66
Impact of COVID-19 on Liver Transplantation Creating Safe Plans For Re-
Entry
David C Mulligan MD FACS FAASLD FASTProfessor and Chair Transplantation and Immunology
Yale UniversityYale New Haven Health System
Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

Impact of COVID-19 on Transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Lan Zhu MD Tongji Hospital of Tongji Medical College
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Beatriz Dominguez-Gil Organizacion Nacional de Trasplantes
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Organ Donation
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

Variable Liver Transplant Activityo Not all transplant
centers decreased liver transplants
o Centers in COVID spared geographies and those with resources to minimize exposure to patients continued to transplant
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Impact of COVID-19 on Transplant in Ontario Canada
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Gastroenterology 2020 May 3 pii S0016-5085(20)30585-0 doi 101053jgastro202004064 [Epub ahead of print]Clinical Characteristics and Outcomes of COVID-19 Among Patients with Pre-Existing Liver Disease in United States A Multi-Center Research Network Study Singh S1 Khan A2
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Courtesy of Darin Treleaven MD MSc McMaster University
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

Additional Considerations
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recipient testing strategiesbull Immediately prior to transplantbull Upon dischargebull Need for direct vs Telehealth visits postopbull Testing of caregiver(s) and quarantine
Timing to restart living donationbull Testing of donor with quarantine prior to surgerybull Testing at discharge and quarantine for 2 weeks
Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

Conclusionso Re-Entry is complex and difficulto Effort to determine correct timing
depending onbull COVID-19 prevalencebull Hospital staff space suppliesbull Blood product suppliesbull Adequate pre- and post- testing
o Ability to be flexible on rebound to minimize COVID exposure
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

o Chair K Rajender Reddy MD FAASLD University of Pennsylvania Medical Center
o Chair Raymond T Chung MD FAASLD Massachusetts General Hospital
o Emily Blumberg MD University of Pennsylvania Medical Center
o Robert S Brown MD MPH FAASLD Weill Cornell Medical Center
o Jaime Chu MD Icahn School of Medicine at Mount Sinai
o David E Cohen MD PhD FAASLD Weill Cornell Medical Center
o Oren K Fix MD MSc FAASLD Swedish Medical Center
o Robert J Fontana MD FAASLD University of Michigan Hospitals and Health Centers
o Elizabeth K Goacher PA-C MHS Duke University o Bilal Hameed MD University of California San
Francisco
copy AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG2020 80
o Laura M Kulik MD Northwestern Medical Faculty Foundation
o John R Lake MD FAASLD University of Minnesota
o Rohit Loomba MD University of California San Diego
o David C Mulligan MD VACS FAASLD Yale University
o Mark W Russo MD MPH FAASLD Carolinas Medical Center
o Michael Schilsky MD FAASLD Yale-New Haven Hospital
o Norah Terrault MD MPH FAASLD Keck Medical Center of USC
o David L Thomas MD Johns Hopkins Medicineo Elizabeth C Verna MD Columbia University o Karen Hoyt Patient Advocate
COVID-19 Task Force
Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

Please submit your questions to the QampA Chat now
Panel Discussion
AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG

AASLDrsquos COVID-19 ResourcesFollowShare COVID-19 Resources Webpage wwwaasldorgcovid19
JoinEngage COVID-19 Care Community on AASLDrsquos online community Engage Open to all members Log in to Engage with your AASLD user name and password engageaasldorgcovid19
Submit Hepatology Liver Transplantation Hep Commun all accepting and fast tracking review of COVID-19 original articles case reports
copy 2020 AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES WWWAASLDORG
Recommended