Case ReportCostello Syndrome and Umbilical LigamentRhabdomyosarcoma in Two Pediatric PatientsCase Reports and Review of the Literature
Carlos Saacutenchez-Montenegro12 Alejandra Vilanova-Saacutenchez2 Saturnino Barrena-Delfa2
Jair Tenorio34 Fernando Santos-Simarro34 Sixto Garciacutea-Mintildeaur34 Pablo Lapunzina34
and Leopoldo Martiacutenez-Martiacutenez2
1Pediatric Surgical Oncology Section Oncology Service Department of Hematology-OncologyHospital Nacional de Ninos ldquoDr Carlos Saenz Herrerardquo Paseo Colon 1654-1000 San Jose Costa Rica2Oncology Section Department of Pediatric Surgery Hospital Universitario La Paz Paseo de la Castellana 261 28046 Madrid Spain3Institute of Medical and Molecular Genetics (INGEMM) Instituto de Investigacion Hospital Universitario La Paz (IdiPAZ)Paseo de la Castellana 261 28046 Madrid Spain4Centro de Investigacion Biomedica en Red de Enfermedades Raras (CIBERER) Instituto de Salud Carlos III (ISCIII)Calle Sinesio Delgado 4 28029 Madrid Spain
Correspondence should be addressed to Carlos Sanchez-Montenegro csanchezmsaludmadridorg
Received 5 October 2016 Revised 20 December 2016 Accepted 28 December 2016 Published 19 January 2017
Academic Editor Philip D Cotter
Copyright copy 2017 Carlos Sanchez-Montenegro et al This is an open access article distributed under the Creative CommonsAttribution License which permits unrestricted use distribution and reproduction in any medium provided the original work isproperly cited
Costello syndrome is caused by heterozygous de novo missense mutations in the protooncogene HRAS with tumor predispo-sition especially rhabdomyosarcoma We here report two pediatric patients with Costello syndrome and umbilical ligamentrhabdomyosarcoma A review of the literature published in English in MEDLINE from January 1971 to June 2016 using the searchterms ldquoCostello syndromerdquo and ldquorhabdomyosarcomardquowas performed including twonew cases thatwe describe Twenty-six patientswith Costello syndrome and rhabdomyosarcoma were recorded with mean age of diagnosis of 2 years and 8 months The mostcommon tumor location was the abdomenpelvis including four out of ten of those in the umbilical ligament The most commonhistological subtype was embryonal rhabdomyosarcoma Overall survival was 43 A total of 17 rhabdomyosarcomas in pediatricpatients arising in the umbilical ligament were recorded with mean age of diagnosis of 3 years and 4 months Overall survival was69 Costello syndrome is a poorly known disorder in pediatric oncology but their predisposition tomalignancies implies the needfor a new perspective on early diagnosis and aggressive medical and surgical treatment
1 Introduction
Costello syndrome (CS) (OMIM 218040) is a rare disorderwith a distinctive prenatal presentation postnatal feeding dif-ficulties and failure to thrive characteristic facial appearance(coarse features full lips and large mouth) abnormalitiesof the heart (hypertrophic cardiomyopathy pulmonary valvestenosis and tachyarrhythmia) skin and musculoskeletalsystem (soft skin deep palmar and plantar creases papil-lomata sparse or curly hair joint laxity ulnar deviation ofwrist and fingers and tight Achilles tendons) and tumor
predisposition such as rhabdomyosarcoma (RMS) neurob-lastoma or transitional cell carcinoma of the bladder [1]It was first described in 1971 by Costello a New Zealandpediatrician based on its distinctive phenotype [2ndash4] CS iscaused by heterozygous de novo missense mutations in theprotooncogene Harvey rat sarcoma viral oncogene homolog(HRAS) (chromosome 11p155) These mutations are presentin 100 of patients with CS but they are usually confirmedin 80ndash90 due to an inaccurate clinical diagnosis [4 5]Mutations result in a gain-of-function of the abnormalprotein product and increased activation of the Mitogen
HindawiCase Reports in GeneticsVolume 2017 Article ID 1587610 13 pageshttpsdoiorg10115520171587610
2 Case Reports in Genetics
(a) (b) (c)
(d) (e) (f)
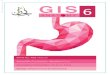
Figure 1 Patient 1 (a) Photograph of the physical features of the patient with low-set ears lower palpebral fissures hypertelorism broadnasal bridge thick lips and thin hair (b) Abdominal ultrasound showing the presence of a solid mass paravesical displacing the left ovaryand bladder without infiltrate surrounding structures (c) Initial MRI showing a hyperintense tumor predominantly heterogeneous intensityon T2-weighted sequence compressing the bladder ((d) and (e)) MRI on T1-weighted sequences after 3 cycles of chemotherapy with slightdecrease in left paravesical oval mass (f) Operative image indicating the presence of tumor originating in the left medial UL
activated protein kinase (MAPK) pathway [1] The mostcommon tumor associated with CS is RMS mainly involvingabdomen pelvis andor urogenital area [6] The first twoCS patients associated with RMS were described in 1998 [7]before that date this syndrome was mainly associated withbenign tumors especially papillomata [3]
We here report two children with CS and RMS of theumbilical ligament (UL) No prior correlation of this tumorlocation with CS had been described so far
2 Case Presentation
21 Case 1 This is a 44-year-old female She is thirdchild of healthy unrelated parents with no family historyof note Pregnancy was complicated with polyhydramniosThe patient was born from a preterm delivery (33 weeks)large (2840 gr) for gestational age She presented feedingdifficulties from the beginning that required nasogastrictube feeding and later gastrostomy at the age of 4 monthsCardiological examination showedmild pulmonary stenosisShe was referred to the Genetics Clinic for assessment atthe age of 6 months because of failure to thrive hypotoniaand dysmorphic features On examination she had featureshighly suggestive of a RASopathy but on account of the
skin findings (sparse hair glabellar capillary malformationa large 4 times 12 cm cafe-au-lait spot in her right flank and twoblue nevi in right temporal region and left groin) difficult todifferentiate with certainty between CS and Cardiofaciocuta-neous syndrome HoweverHRASmutation analysis demon-strated a common recurrent mutation (pG12S) confirmingthe diagnosis of CS in this child at the age of 7 months(Figure 1(a)) Because of the high risk of tumor developmentassociated with this condition close follow-up was indicatedaccording to the recommended tumor screening protocol [820] An abdominal ultrasound scan performed at the age of 16months revealed a 31 times 32mm paravesical solid pelvic masswith minimal intralesional vascularity no intraabdominalfree fluid or lymphadenopathies were seen The ovaries werenot involved (Figure 1(b)) Magnetic resonance imaging(MRI) showed a left paravesical tumor (3 times 5 times 27 cm)without associated lymphadenopathies hypointense on T1-weighted sequences and hyperintense with predominantlyheterogeneous intensity on T2-weighted sequencesThemasscaused compression and displacement of the bladder tothe right side (Figure 1(c)) Tumor markers were as fol-lows beta-subunit of human chorionic gonadotropin (120573-hCG) lt 2mUImL (normal lt 60) alpha-fetoprotein (120572FP)29 ngmL (normal lt 80) carcinoembryonic antigen (CEA)
Case Reports in Genetics 3
08 ngmL (normal lt 50) CA-153 197UImL (normal lt320) CA-199 437UImL (normal lt 370) and neuronspecific enolase (NSE) 2786 ngmL (normal 0ndash160)Thoraciccomputed tomography (CT) and scintigraphy showed noevidence of metastasis Bone marrow biopsy was normalTru-Cut biopsy guided by ultrasound reported an embryonalRMS with a proliferation index Ki-67 of 60 mesenchymalmalignant round cell and short spindle tumor vimentin(+) desmin (focal +) MyoD1 (focal +) CD99 (+ focalstaining) S100 protein (minus) pancytokeratins AE1AE3 (minus)synaptophysin (minus) and CD99 (minus) She was enrolled onthe standard risk group protocol European pediatric Softtissue Sarcoma Study Group (EpSSG) RMS 2005 subgroup Dwith 3 neoadjuvant chemotherapy cycles Preoperative MRIshowed a slight decrease in tumor size (32 times 3 times 25 cms)(Figures 1(d) and 1(e)) At the definitive surgery a 5 cmtumor dependent of the remaining left umbilical artery (leftmedial UL) located slightly to the left and displacing thebladder dome was found (Figure 1(f)) Complete resectionof the tumor was performed No pathological lymph nodeswere observed Final pathology report showed an embryonalRMS with signs of response to chemotherapy (maturationphenomenon at cytoplasmic and nuclear level of the tumorcellularity) with maximum cell proliferation index Ki-67 of5ndash10 almost all undifferentiated except in a small regionresection margins were negative for tumor (1ndash4mm fromthe edges of radial resection margin and 3 cm of UL)Chemotherapywas then continueduntil completing 25weeksand coadjuvant radiotherapy was administrated after thecompletion of chemotherapy At 23months of follow-up afterdiagnosis no residual tumor or relapse has been identified
22 Case 2 This is a 54-year-old female She is the first andonly child of a healthy nonconsanguineous couple with unre-markable family history Pregnancy was complicated withpolyhydramnios and delivery was preterm (34 weeks) with ahigh birth weight (2980 g +26 SD) She was admitted to theneonatal ward for investigation of a suspected dysmorphicsyndrome and initial FGFR3 molecular genetic testing forachondroplasia revealed no mutations Feeding difficultiesand failure to thrive were noted from the beginning requiringnutritional intervention and gastrostomy feeding from theage of 10 months She had a heart murmur with a normalechocardiogram She also had bronchomalacia and at MRInonspecific white matter hyperintensities in CNS She wasreferred to our clinical Genetics Clinic for evaluation at theage of 4 months and in view of her previous history andclinical findings CS was suspected HRAS Sanger sequencingdetected the common c34GgtA (pG12S) mutation confirm-ing the diagnosis of CS (Figure 2(a)) As part of the follow-up the recommended tumor screening protocol was arrangedand at the age of 3 years she underwent an abdominalultrasound that showed a tubular image running throughthe theoretical place of the umbilical arteries with a largercaliber on the right side of 56mm and associated echoesinside without Doppler flow (Figure 2(b)) Two subsequentultrasounds did not show any abnormality A new abdominalultrasound 9 months later reported the presence of a hypoe-choicmultilobulated solid tumor (53times 28 cm) in themidline
extending to the right in supravesical region with markedhypervascularization and extending cranially to the vicinityof the abdominal wall (Figures 2(c) and 2(d)) MRI showeda solid abdominal tumor (6 times 55 times 3 cm) composed ofnodular masses grouped in the UL region with involvementof the medial umbilical folds that were thickened throughoutthe iliac vessels region (Figure 2(e)) No regional metastaticdisease was observed Tumor markers were as follows 120572FPlt 13 ngmL CEA 53 ngmL and CA-199UImL No lungmetastases were observed in the thoracic CT scan and bonemarrow biopsywas normal She underwent a complete tumorresection (Figure 2(f)) The mass was located on the rightmedial UL (from its insertion into the right iliac artery tothe umbilicus) Pathology report showed a spindle cell RMSwith microscopic positive margins in 2 submitted samples(85 times 5 times 3 cm and 35 times 15 times 1 cm) and one resected lymphnode was negative for malignancy Tumor was composedof spindle cells that form cross linked bundles varyingdegrees with elongated oval nuclei vesicular configurationswith coarse chromatin The tumor had a pattern of nodulargrowth markedly myxoid stroma with microcystic focaldegeneration and 5 tumor necrosis no lymphovascularinvasion maximum proliferation index Ki67 of 30 musclespecific actin (+) desmin (+) WT1 (+ cytoplasmic) MyoD1(+ nuclear) and CD99 (minus) Two weeks after surgery thestandard risk group protocol EpSSG RMS 2005 subgroup B(Stage I) chemotherapy was started that includes ifosfamidevincristine and actinomycin D At 18 months of follow-up after diagnosis no residual tumor or relapse has beenidentified
3 Methods
We describe two new cases of RMS and CS based onmedicalrecords of patients diagnosed at the Institute of Medicaland Molecular Genetics and treated at the Departmentsof Pediatric Hematology-Oncology and Pediatric SurgeryUniversity Hospital La Paz (Madrid Spain) A review of theliterature published in English in MEDLINE from January1971 to June 2016 using the search terms CS and RMS wasdone also the references contained in these articles even ifthey were not indexed inMEDLINE were analyzed A reviewfrom January 1933 until June 2016 of all reported pediatriccases of UL RMS including as search criteria UL RMSurachus and umbilical arteries was performed
4 Results
In all cases analyzed and reviewed (same cases reportedin more than one publication were counted once) it waspossible to document the presence of 26 patients with CSand RMS (Table 1) [5ndash25] including the 2 cases describedherein The mean age of diagnosis was 2 years and 8 months(range 6 monthsndash7 years) It was slightly more commonin females than in males (12 1) The commonest locationwas the abdomenpelvis (1020) including 4 out of 10 ofthose in the UL The most common histological type wasembryonal RMS (1419) Seven out of nine patients who died(and with reported histology) showed embryonal RMS The
4 Case Reports in Genetics
(a) (b) (c)
(d) (e) (f)
Figure 2 Patient 2 (a) Photograph of the physical features of the patient with prominent forehead low-set ears lower palpebral fissureshypertelorism broad nasal bridge thick lips and anteverted slightly nostrils (b) Initial abdominal ultrasound showing the presence ofa tubular image caliber of 56mm extending in the theoretical location of the right umbilical artery ((c) and (d)) Follow-up abdominalultrasound in themidline showing amultilobulated hypoechoic solid tumorwithmarked hypervascularization extending from the proximityof the abdominal wall to the right supravesical region (e) MRI onT2-weighted sequence confirms the presence of several nodular massesgrouped with thickening of both medial umbilical folds the right to 4mm proximal to the umbilicus and 8mm adjacent to the iliac vesselsparavesical region portion (f) Operative image indicating the presence of tumor originating in the right medial UL
most frequent encountered HRAS mutation associated withRMS was pG12S (712) Only 4 deaths were documented inpatients with change in codon 12 (2 patients G12S 1 patientG12A and 1 patient G12C) Chemotherapy that was appliedvaries based on the protocols of the countries where theywerediagnosed (Table 2) [5ndash10 12ndash14 16ndash25] Overall survival wasabout 43 (921) Mortality was observed in 12 out of 21individuals in nine of them associated with neoplasia andin three associated with surgery
Similarly the total number of reported cases of ULRMS in pediatric patients either in the obliterated umbilicalarteries (medial UL) or in urachus (median UL) is 17including these 2 new cases (Table 3) [5 7ndash9 24ndash31] Themean age of diagnosis was 3 years and 4 months (range 4monthsndash6 years) It is slightly more common in females thanin males (14 1) Themost common location was the urachus(1517) The most common histological type was embryonalRMS (1215) and one-fourth (312) of patients who died withreported histology showed embryonal RMS Chemotherapyvaries based on the protocols of the countries where theywerediagnosed (Table 4) [7 24 26ndash31] Overall survival was 69
(1116) overall mortality was 31 (516) two-year absolutesurvival rate was 69 (1116) and five-year absolute survivalrate was 19 (316)
5 Discussion
The prevalence of CS is estimated to be 1 1290000 individ-uals in Japan and at least 1 500000 in the United Kingdomthe incidence was estimated to be 1 60000ndash100000 [4 22]The overall tumor incidence is approximately 10ndash15 overthe lifetime of individuals with an identified HRASmutation[1 4 9] RMS accounting in about 60 of all neoplasia [1]Based on the 300 cases of CS currently known [4] we foundan incidence of 87 RMS in patients with CS
CS is the first disorder associated with germlinemutations in the Ras family of guanosine-51015840-triphosphate(GTP)ases [21] HRAS has six exons five exons are encodedfor a protein of 189 amino acids with a molecular weight of21 kDa [4] Missense mutations at codons 12 and 13 are inconstitutively active GTP-bound conformation and activatedownstream effectors such as MAPK phosphatidylinositol3-kinases (PI3K) and ral guanine nucleotide dissociation
Case Reports in Genetics 5
Table1Ch
aracteris
ticso
fpatientsw
ithCostello
synd
romea
ndrhabdo
myosarcom
a
PT number
Author
Year
Cou
ntry
Sex
Age
atdiagno
sis(yearsm
onths)
Symptom
sLo
catio
nHistolog
yMutation
AAC
(NS)
Therapy
Outcome
1Ke
rretal
[78]
1998
England
F2y
4mVo
miting
Con
stipatio
nRe
troperiton
ealleft
psoasm
ayor
muscle
Embryonal
G12S
(34GgtA)lowast
[9]
SCh
TRe
lapsetumor-fr
eeageo
f7years
2Ke
rretal
[78]
1998
England
F3y
2mAb
dominal
mass
Pelvis
urachu
s(m
edianUL)
adherent
tothe
bladder
Embryonal
G12A
(35GgtC)
[5]
SCh
T
Histologyshow
edextend
ingup
tothe
resectionmargin
Diedaged
5years
[59]
3Feingold
[810]
1999
USA
M6m
Tumor
Rightfoo
tAlveolar
NDF
SCh
TTu
mor-fr
eeageo
f20
years[11]
4Bisogn
oetal
[8912]
1999
Italy
M1y
8mCon
stipatio
nAb
dominal
pain
Lower
abdo
men
pelvis
abdo
minal
walllowast
Embryonal
NDF
SCh
TOnlybiop
syDiedaged
2yearsa
nd3mon
ths
5Sigaud
yetal
[813]
2000
France
M6y
NDF
Inguinalscrotal
Embryonal
NDF
NDF
NDF
6Grip
petal
[81415]
2002
USA
M5y
6mAb
dominal
pain
Pelvis
pulm
onary
metastasesw
aspresent
Embryonal
NDF
SCh
TDiedaft
errecurrence
[14]
7Grip
petal
[8]
2002
USA
F3y
7mAb
dominal
pain
Emesis
Upp
erabdo
men
masse
ncasingthe
superio
rmesenteric
anceliaca
rteries
Sing
lepu
lmon
ary
nodu
le
Pleomorph
icNDF
ChT
Diedaged
4years
8Grip
petal
[8]
2002
USA
F2y
6mAb
dominal
mass
Pelvis
bladder
Embryonal
NDF
ChT
RTS
Diedaged
7yearsfor
recurrency
ofRM
Sfib
rosarcom
a[16]
9Grip
petal
[8]
2002
USA
NDF
7mPerin
eal
grow
thPerin
eal
Embryonal
NDF
ChT
RTS
Tumor-fr
eeageo
f2years
10Grip
petal
[8]
2002
USA
NDF
1y11m
Prop
tosis
Leftorbit
Unk
nown
NDF
SRT
Tumor-fr
eeageo
f4years
11Ka
wam
eetal
[17]
2003
Japan
F1y
4mAb
dominal
mass
Pelvis
Spindlec
ell
NDF
SCh
TTu
mor-fr
eeageo
f7years
6 Case Reports in GeneticsTa
ble1Con
tinued
PT number
Author
Year
Cou
ntry
Sex
Age
atdiagno
sis(yearsm
onths)
Symptom
sLo
catio
nHistolog
yMutation
AAC
(NS)
Therapy
Outcome
12Ke
rretal
[18]
2003
UK
M2y
2mLargep
elvic
mass
Retro
vesic
ular
mass
byultrasou
ndEm
bryonal
NDF
ChT
Diedaged
2yearsa
nd4mon
ths
13OrsquoNealetal
[19]
2004
USA
F3y
Right-s
ided
cervicofacial
mass
Parameningeal
infratem
poralfossa
right
perip
arotid
mastic
ator
space
region
Alveolar
NDF
ChTS
RT
Clinicalgrou
p3T2
bN0stage3
Dieddu
ringsurgery
14Grip
p[20]
2005
USA
F3y
2mFacialmass
Rightinfratempo
ral
fossa
Mixed
alveolar
and
embryonal
NDF
ChTS
Dieddu
ringsurgery
byventric
ular
tachycardiafollowed
rapidlyby
lossof
heartrhythm
15Ao
kietal
[2122]
2005
Japan
F7y
2mNDF
NDF
NDF
G12S
(34GgtA)
NDF
NDF
16Grip
petal
[9]
2006
USA
M2y
NDF
NDF
NDF
G12S
(34GgtA)
NDF
Tumor-fr
eeageo
f11
yearslowast
17Ke
rretal[5]
2006
UK
NDF
7mNDF
Metastatic
arising
from
thep
rosta
teEm
bryonal
[23]
G12C
(34GgtT)
NDF
Diedaged
7mon
ths
18Ke
rretal[5]
2006
UK
NDF
NDF
NDF
NDF
NDF
G12S
(34GgtA)
NDF
Diedaged
7years
19Ke
rretal[5]
2006
UK
NDF
NDF
NDF
NDF
NDF
G12A
(35GgtC)
NDF
NDF
20Lo
etal[23]
2008
UK
M2y
3mRe
spira
tory
functio
ndeterio
rated
Rightlun
gNDF
G12S
(34GgtA)
SDiedfewweeks
later
surgery
21Ahm
adiand
Harley[6]
2010
USA
M2y
Increasedwork
ofbreathing
Nasop
haryngeal
Embryonal
NDF
SCh
TRT
Clinicalgrou
pIIA
(T1N
0M0)
Tumor-fr
eeageo
f3years
22Ab
eetal[22]
2012
Japan
NDF
NDF
NDF
NDF
NDF
NDF
NDF
Died
23Menke
etal
[2425]
2015
Germany
F3y
Abdo
minal
mass
Lower
anterio
rabdo
menabo
vethe
urinarybladderlowast
(urachus-m
edianUL
bylocatio
n)
Embryonal
G12C
(34GgtT)
SCh
T
R1resection
(marginaltum
orresid
ue)Tu
mor-fr
eeageo
f6years
24Kr
atze
tal
[25]
2015
Germany
M1y
NDF
NDF
Embryonal
G12S
(34GgtA)
NDF
NDF
25
Sanchez-
Mon
tenegro
etal(this
repo
rt)
2017
Spain
F2y
4mAs
ymptom
atic
LeftmedialU
LEm
bryonal
G12A
(35GgtC)
ChTS
RTTu
mor-fr
eeageo
f4yearsa
nd4mon
ths
26
Sanchez-
Mon
tenegro
etal(this
repo
rt)
2017
Spain
F3y
10m
Asym
ptom
atic
Rightm
edialU
LSpindlec
ell
G12S
(34GgtA)
SCh
TTu
mor-fr
eeageo
f5yearsa
nd4mon
ths
AAC
aminoacid
changeC
hTchemotherapyFfem
aleMm
aleNDFno
datafoun
dNSnu
cleotides
ubstitutio
nPT
patientR
TradiotherapySsurgeryU
Lum
bilicalligam
entlowastPerson
alcommun
icationby
author
Case Reports in Genetics 7
Table 2 Chemotherapy of patients with Costello syndrome and rhabdomyosarcoma
PTnumber Chemotherapy protocol
1Initially with VCR ACD and CTX After debulking continued on ChT using IFOS VCR and ACD After the second coursewhen she developed IFOS induced encephalopathy she was changed back to pulses of VCR ACD and CTX given every 3weeks for 9 courses [7]
2Initially IFOS ACD and VCR After 4 courses CTX was substituted for IFOS because hemorrhagic cystitis Tx complicatedby recurrent episodes of moderately severe diarrhoea and febrile neutropenia requiring readmission to hospital Tx wascompleted after six courses of ChT [7]
3 Tx consisted of below the knee amputation and ChT (DOX ACD VCR and CTX) [10]
4
Tx was implemented according to the Italian protocol for pediatric soft tissue sarcoma Three courses of ChT including VCR(0025mgkg day 1) IFOS (50mgkg days 1 and 2) and alternating ACD (0025mgkg day 1) and DOX (07mgkg day 1) wereadministered Symptoms regressed and the CT scan showed a reduction in tumor volume of more than two-thirds After 3more courses of ChT the patient experienced abdominal pain A repeat abdominal CT scan showed an increase in the pelvicmass Despite the administration of a different ChT with CBDCA (11mgkg day 1) and VP-16 (3mgkg for 3 doses) the tumorcontinued to grow and the child died 7 months after the diagnosis of RMS [12]
5 NDF [13]
6
The first cycle of ChT with VCR ACD and CTX and topotecan reduced the tumor size [16] The tumor was surgicallyremoved after the first ChT [8] Debulking S was required because of rapid growth and tumor necrosis The protocol wascontinued and was deemed sufficiently successful to withhold RT One month after completion of the first protocol tumorrecurrence necessitated a second round of ChT with irinotecan and DOXThe latter drug was administered about 1 weekbefore he died during which time he had tachycardia (heart rate 180ndash20 bpm) [14]
7 The tumor did not respond to ChT and she died shortly after her 4th birthday [8]8 Tx was a combination of S ChT and RT continued until age of 35 years [8]9-10 NDF [8]11 PT had later generalized tonic-clonic seizures during her Tx for RMS [17]12 Despite extensive ChT the tumor progressed rapidly and the PT died 2 months later [18]
13 Induction ChT was commenced with the initial 12-week course of VCR ACD and CTX based on the Intermediate RiskProtocol D9803 of the COG [19]
14 ChT did not result in tumor shrinkage therefore surgical resection was performed [20]15ndash22 NDF [5 6 9 21ndash23]23 ChT according to the cooperative soft tissue sarcoma protocol (CWS-2002 P) was well tolerated by the PT [24]24 NDF [25]
25 ChT in the standard risk group protocol EpSSG RMS 2005 subgroup D 3 preoperative cycles of IFOS (2 doses at 100mgkg)VCR (005mgkg) and ACD (005mgkg)
26 ChT (postoperative 15 days) in the standard risk group protocol EpSSG RMS 2005 subgroup B (Stage I) cycles of IFOS (2doses of 3 gm2d) VCR (15mgm2) and ACD (15mgm2) was initiated
ACD actinomycin D CBDCA carboplatin ChT chemotherapy COG childrenrsquos oncology group CTX cyclophosphamide CT computed tomography CWSCooperative Weichteilsarkom Studie (Cooperative Soft Tissue Sarcoma Study) DOX Doxorubicin EpSSG European pediatric Soft tissue sarcoma StudyGroup IFOS ifosfamide NDF no data found PT patient RMS rhabdomyosarcoma RT radiotherapy S surgery Tx treatment VCR vincristine VP-16etoposide
stimulator (RalGDS) [16 21] in signaling pathways control-ling cell proliferation and differentiation [9]
Themajority of patients with CS had 34GgtA transition incodon 12 (80) [4 16] More than 95 of the mutations arepredicted to result in substitution of the glycine in position12 or 13 of the protein product [1] All individuals withmalignancy had a codon 12 mutation (especially G12A 47patients) [5 21] The rare G12V mutation is associated witha more severe early lethal phenotype some patients diefrom respiratory distress hypertrophic cardiomyopathy ormalignant tachycardia prior to being diagnosed with CS [1]As far as we know no individual with G13C has developed amalignant tumor [4 32]
RMS is the most common soft tissue sarcoma of infancyIts incidence is between 4 and 7 cases per 1 million childrenyounger than 15 years [8 12] The age peak is between 2 and5 years with a slight male predominance (12ndash141) Thesetumors may arise anywhere in the body and fewer than 20are located in the pelvis [12]Most RMS tumors are originatedin the head and neck region urogenital tract and extremities[33] The most common histologic type seen in gt50 isembryonal followed by alveolar in 20ndash30 PleomorphicRMS is rare (1) and has a poor prognosis [8] AlveolarRMS is characterized by the translocation t(213)(q35q14) in70 of cases and the variant translocation t(113)(p36q14)in a smaller percentage of cases Evidence accumulates
8 Case Reports in Genetics
Table3Ch
aracteris
ticso
fPediatricPatie
ntsw
ithUmbilicalLigamentR
habd
omyosarcom
a
PT number
Author
Year
Cou
ntry
Sex
Age
atdiagno
sis(yearsm
onths)
Symptom
sLo
catio
nSize
(cm)
Histology
IRS
grou
pTh
erapy
Outcome
1Ra
nsom
[2627]
1933
USA
F4m
Massb
elowthe
umbilicus
and
extend
ing
somew
hattothe
right
Urachus
(medianUL)
attached
alon
gthea
nterior
wallfrom
theu
mbilicus
tothea
pexof
theb
ladd
er
115
Spindle
cell
ISM
AC
RT
Lastcheck-up
exam
ination(2
years)
show
edno
evidence
ofrecurrence
2Ishikawae
tal[28]
1985
Japan
F1y
4mAb
dominalmass
abdo
minalpain
hemop
erito
neum
Urachal(m
edianUL)
intra-abdo
minalruptureo
fthetum
or
Fist-
sized
NDF
IVSM
ACNDF
3Yo
koyamae
tal[2729]
1997
Japan
M2y
Episo
diclow
erabdo
minalpain
Urachus
(medianUL)
extraperito
neallocated
betweentheu
mbilicus
and
apex
oftheb
ladd
erandwas
adherin
gtig
htlyto
both
Theb
ilateralm
edialU
Lweres
eenenterin
gthe
tumorR
upturedwith
asm
alln
umbero
fdissem
inated
tumors
scatteredon
them
esentery
andDou
glas
pouch
12Em
bryonal
IVSM
AI
ChT
At2yearso
ffollo
w-upno
recurrence
hadbeen
detected
4lowastKe
rretal
[78]
1998
England
F3y
2mAb
dominalmass
Urachus
(medianUL)
adherent
totheb
ladd
erNDF
Embryonal
IIaSM
II
ChT
Histologyshow
edextend
ingup
tothe
resectionmargin
Diedaged
5years
[59]
5Schu
lzand
OrsquoLeary
[2730]
2001
Scotland
M2y
NDF
Urachus
(medianUL)
NDF
Embryonal
NDF
SCh
TRT
Tumor-fr
eeageo
f26
years
6Fernandeze
tal[27]
2007
Spain
F6y
Intractable
constip
ation
nauseaabd
ominal
painles
smass
Urachus
(medianUL)
infiltratingthev
entral
abdo
minalwalland
fixed
tothev
esicaldo
me
135
Embryonal
IbSM
IC
ChT
At4yearso
ffollo
w-upthep
atient
remains
welland
free
ofclinicald
isease
7lowastMenke
etal
[2425]
2015
Germany
F3y
Abdo
minalmass
Lower
anterio
rabd
omen
abovethe
urinarybladderamp
(urachusm
edianULby
locatio
n)
NDF
Embryonal
IIaSM
II
ChT
R1resection
(marginaltum
orresid
ue)Tu
mor-fr
eeageo
f6years
8Ch
eikh
elard
etal[31]
2015
Dx
1983
France
F5y
5mNDF
Urachus
(medianUL)
periton
ealm
etastasesa
ndhypo
gastric
lymph
nodes
5NDF
IVSM
AI
ChT
Died31
mon
thsa
fter
diagno
siswith
relap
sein
periton
ealliver
at11mon
ths
Case Reports in Genetics 9
Table3Con
tinued
PT number
Author
Year
Cou
ntry
Sex
Age
atdiagno
sis(yearsm
onths)
Symptom
sLo
catio
nSize
(cm)
Histology
IRS
grou
pTh
erapy
Outcome
9Ch
eikh
elard
etal[31]
2015
Dx
2003
France
F3y
3mPeriton
ealrup
ture
poor
generalstatus
Urachus
(medianUL)
lumbo
aorticandexternal
iliac
lymph
nodes
10Alveolar
IVSM
AI
ChTRT
Died57
mon
thsa
fter
diagno
siswith
relap
sein
periton
ealliver
at30
mon
ths
10Ch
eikh
elard
etal[31]
2015
Dx
2005
France
F2y
6mMasspo
orgeneral
statusdysuria
Urachus
(medianUL)
15Em
bryonal
III
SMII
ChTRT
Died37
mon
thsa
fter
diagno
siswith
periton
ealrelapse
at19
mon
ths
11Ch
eikh
elard
etal[31]
2015
Dx
2005
France
M4y
2mMasspo
orgeneral
statusdysuria
Urachus
(medianUL)
periton
ealm
etastasesa
ndiliac
lumbo
aorticlymph
nodes
10Em
bryonal
IVSM
II
ChTRT
Relapsed
multifocalat
82mon
thsfollo
w-up
100mon
ths
12Ch
eikh
elard
etal[31]
2015
Dx
2005
France
M5y
3mMasspo
orgeneral
status
Urachus
(medianUL)
periton
ealm
etastasesa
ndmesenteric
lymph
nodes
106
Embryonal
IVSM
IC
ChTRT
Tumor
freea
fter9
5mon
thssince
diagno
sis
13Ch
eikh
elard
etal[31]
2015
Dx
2006
France
M2y
5mMasspo
orgeneral
statusob
structiv
erenalinsuffi
ciency
Urachus
(medianUL)
periton
ealbon
emetastases
andhypo
gastric
lymph
nodes
21Em
bryonal
IVSM
II
ChTRT
Bone
progression
after
16mon
thsdied
18aft
erdiagno
sis
14Ch
eikh
elard
etal[31]
2015
Dx
2010
France
M4y
5mAb
dominalpain
Urachus
(medianUL)
7Em
bryonal
III
SMIC
ChT
Tumor
freea
fter18
mon
thssince
diagno
sis
15Ch
eikh
elard
etal[31]
2015
Dx
2010
France
M6y
Abdo
minalpain
Urachus
(medianUL)
periton
ealm
etastases
14Em
bryonal
IVSM
AI
ChTRT
Tumor
freea
fter4
5mon
thssince
diagno
sis
16lowast
Sanchez-
Mon
tenegro
etal(this
repo
rt)
2017
Dx
2015
Spain
F2y
4mAs
ymptom
atic
LeftmedialU
L5
Embryonal
IaCh
TSM
IC
RT
Tumor-fr
eeageo
f3yearsa
nd9mon
ths
17lowast
Sanchez-
Mon
tenegro
etal(this
repo
rt)
2017
Dx
2015
Spain
F3y
10m
Asym
ptom
atic
Rightm
edialU
L85
Spindle
cell
IIaSM
II
ChT
Tumor-fr
eeageo
f4yearsa
nd5mon
ths
ChT
chem
otherapyD
xdiagno
sed
Ffemale
IRS
intergroup
rhabdo
myosarcom
aMm
ale
NDF
nodata
foun
dRT
radiotherapy
Ssurgery
SMAIsurgerymacroscop
ically
incomplete
SMAC
surgery
macroscop
icallycompleteSM
ICsurgery
microscop
icallycompleteSM
IIsurgery
microscop
icallyincompleteULum
bilicalligam
ent
ampPerson
alcommun
icationby
authorlowast
Patientsw
ithCostello
synd
rome
10 Case Reports in Genetics
Table 4 Chemotherapy of pediatric patients with umbilical ligament rhabdomyosarcoma
PTnumber Chemotherapy protocol
1-2 No ChT [26 28]3 After establishment of the final diagnosis he was treated with combined ChT including VCR ACD and CTX [29]
4lowastInitially IFOS ACD and VCR After 4 courses CTX was substituted for IFOS because of hemorrhagic cystitis Tx complicatedby recurrent episodes of moderately severe diarrhoea and febrile neutropenia requiring readmission to hospital Tx wascompleted after six courses of ChT [7]
5 NDF [30]
6 PT started induction of ChT 2 weeks after S Induction regimen included 9 cycles of IVA (IFOS VCR and ACD) that were welltolerated with minimal systemic complications (Tx 953 of the MMT 95 SIOP protocol for RMS) [27]
7lowast ChT according to the cooperative soft tissue sarcoma protocol (CWS-2002 P) was well tolerated by the PT [24]8 Adjuvant ChT with 10 cycles of IFOS VCR and ACD [31]9 Adjuvant ChT with 6 cycles of IFOS VCR and VP-16 and 9 cycles of VCR ACD CTXACD and CTX [31]10 Neoadjuvant ChT with 6 cycles of IFOS VCR and ACD and adjuvant ChT with 3 cycles of IFOS VCR and ACD [31]
11 Neoadjuvant ChT with 1 cycle of CTX VCR and PRED 2 cycles IFOS VCR and ACD and 4 cycles of IFOS VCR ACD andDOX and adjuvant ChT with 3 cycles of IFOS VCR and ACD [31]
12 Neoadjuvant ChT with 1 cycle of CTX VCR and PRED and 5 cycles of IFOS VCR ACD and DOX and adjuvant ChT with 2cycles of IFOS VCR ACD and DOX and 1 cycle of IFOS VCR and ACD [31]
13 Neoadjuvant ChT with 2 cycles of VCR ACD and CTX + and 3 cycles of IFOS VCR ACD and DOX and adjuvant ChT with 3cycles of IFOS VCR and ACD [31]
14 Neoadjuvant ChT with 4 cycles of IFOS VCR ACD and DOX and adjuvant ChT with 5 cycles of IFOS VCR ACD [31]
15 Neoadjuvant ChT with 4 cycles of IFOS VCR ACD DOX 3 cycles of IFOS VCR ACD and adjuvant ChT with 1 cycle of IFOSVCR ACD 1 cycle of IFOS VCR [31]
16lowastChT in the standard risk group protocol EpSSG RMS 2005 subgroup D 3 preoperative cycles of IFOS (2 doses at 100mgkg)VCR (005mgkg) and ACD (005mgkg)
17lowastChT (postoperative 15 days) in the standard risk group protocol EpSSG RMS 2005 subgroup B (Stage I) cycles of IFOS (2 dosesof 3 gm2d) VCR (15mgm2) and ACD (15mgm2) was initiated
ACD actinomycin D ChT chemotherapy CTX cyclophosphamide CWS Cooperative Weichteilsarkom Studie (Cooperative Soft Tissue Sarcoma Study)DOX Doxorubicin EpSSG European pediatric Soft tissue sarcoma Study Group IFOS ifosfamide MMT malignant mesenchymal tumor NDF no datafound PRED prednisone PT patient RMS rhabdomyosarcoma S surgery SIOP Societe Internationale DrsquoOncologie Pediatrique (International Society ofPediatric Oncology) Tx treatment VCR vincristine VP-16 etoposide lowastPatients with Costello syndrome
that alveolar RMS and embryonal RMS are two differentdisorders while alveolar RMS may originate from primitiveuncommitted mesodermal cells embryonal RMS originatesprobably from more differentiated myoblasts Ras protein-specific guanine nucleotide-releasing factor 1 (RasGRF1)plays an important role in alveolar RMS pathogenesis Theseinteresting concepts however need more evidence [33]
The umbilicus caudally originates the common ligamentwhich is divided into obliterated umbilical arteries (medialUL) and urachus (median UL) The urachus varies from3 to 10 cm in length and from 8 to 10mm in diameterIt is a three-layered tubular structure the innermost layerbeing lined with transitional epithelium in 70 of casesand with columnar epithelium in 30 The structure issurrounded by connective tissue and outermost muscularlayer in continuity with the detrusor muscle Along its pathfrom the bladder to the umbilicus the urachus lies betweenthe transverse fascia and the parietal peritoneum containedin the pyramidal retropubic perivesical preperitoneal spacecompartmentalized by umbilicovesical fascia along with themedial umbilical ligaments and the bladder Occasionallythe urachus may merge with one or both of the obliteratedumbilical arteries (medial UL) and there may be a slight
deviation to the right or left of the midline [34] The urachusis an embryological remnant resulting from the obliterationof the allantoic channel which attaches the bladder dome tothe umbilicus [31]
Urachal malignant tumors are extremely rare represent-ing less than 05 of all bladder cancers and 001 of alltumors They may arise from any portion of the urachus andare most commonly found in adults and males (60ndash70)Although sarcomas represent only 8 they are the mostfrequent urachal neoplasms reported in patients youngerthan 20 years of age (67) [27] Poor prognosis is a commonfeature in adults and pediatric urachalmalignancies with 50to 60 of 5-year survival In contrast the 5-year event-freesurvival in pelvic RMS was reported to be about 51 [31]
This indolent and rather large urachal tumor was mostlyrevealed by an uncomplicated progressing mass withoutprodromic urological symptomsThedelay of diagnosis couldbe explained by a long asymptomatic progression of thetumor in a preperitoneal location which allows an importantlocal spreading before diagnosis Even in patients withouttumor rupture peritoneal involvement appeared to be the keypoint in the prognosis of urachal RMS Systematic cytologyat diagnosis could be more accurate to evaluate peritoneal
Case Reports in Genetics 11
extension in order to avoid understaging and adjust adjuvantlocoregional treatment [31]
Previously only 12 patients with RMS arising from theurachus (median UL) in children without CS have beenreported in the English literature (Table 3) By 2011 therewere29 reported cases of cancer in patients withCS 19 RMS (meanage of 23 years 9 embryonal 1 alveolar 1 mixed histology1 pleomorphic 1 spindle cell type and 6 unclassified) 5neuroblastomas 4 bladder cancer and 1 fibrosarcoma [35]
Loss of heterozygosity for 11p155 in RMS from individu-als with CS suggests that loss of the wild-type allele is the sec-ond hit in tumor development [6 16 36] Whereas theHRASmutation in a sporadic malignancy in the general populationis present only within the tumor cells in CS an identicalmutation is present in every single cell of the individualthus accounting for the tumor predisposition [1] implicatingan alternate mechanism of rhabdomyosarcogenesis [16] Inaddition one patient with CS and uniparental trisomy dueto triplication of the mutated paternal HRAS gene was alsoreported RMS typically displays loss of heterozygosity ofthe 11p155 region because of paternal uniparental disomyand approximately 28 of cases harbor mutations in genesof growth signaling pathways In reports of uniparentaldisomy plus HRAS mutation the latter was heterozygousand therefore must have occurred after the developmentof uniparental disomy [24] The functional analysis alsorevealed that CS-causing mutant HRAS proteins causedoncogene-induced senescence in human fibroblasts [37]Theimportant role of PI3K-protein-kinase B (AKT) signalingin Ras-mediated transformation and tumorigenesis is high-lighted by constitutive AKT activation in RMS cell lines andclinical samples Thus prolonged PI3K-AKT signaling mightalso be implicated in the development of soft tissue sarcomain patients with CS [38]
Only four out of 11 patients were diagnosed with CS priorto the RMS diagnosis in 5 patients CS was diagnosed afterthe RMS and in the remaining 2 the order was unknown[20] In 2003 a further three unpublished cases of RMS inchildren with CS were known through the International CSSupport Group [18] and for that reason there is possiblyunderdiagnosis of RMS in patients with CS
A screening protocol was proposed consisting of ultra-sound examination of the abdomen and pelvis every 3ndash6 months until age of 8ndash10 years for RMS and abdomi-nal neuroblastoma urine catecholamine metabolite analysisevery 6ndash12 months until age of 5 years for neuroblastomaand urinalysis for hematuria annually for bladder carcinomaafter age of 10 years The prior diagnosis of CS was theprerequisite for the implementation of a tumor screeningprotocol [8] The recommendation based on the presumedfast doubling time of RMS was abdominal sonographyscreening for RMS that should be done in similar intervalsof every four months until stronger evidence would suggestotherwise [39] Screening for neuroblastoma is no longerrecommended becausemany CS patients without identifiabletumor show elevated catecholamine metabolites in urine itappears that in this patient group an elevation above thenormal limit defined as 2 standard deviations (SD) above themean for age is more likely to be a variant rather than a sign
of a neuroblastoma [1 40] A French monitoring protocolproposed the determination of catecholamines and theirmetabolites in urine every six months until the age of 5 yearsand ultrasound abdominopelvic every six months until theend of the puberty seeking hematuria dipstick from6monthsto the age of 10 [41] The protocol in our hospital for patientswith CS includes an abdominal and pelvic ultrasound 3times during the first year of life and in childhood every 6months until age of 10 [42] We believe that the best optionis to perform a pelvic abdominal ultrasound every 3 monthsduring the first eight years of life and then controls accordingto medical criteria This is even more necessary in patientswith possible UL RMS because diagnosis was usually done inadvanced stages with a poor survival It is possible that withclose monitoring after an early diagnosis will detect initialstages of the tumor in previously not described locations
Head and neck MRI scans can be performed less fre-quently Ear examination and tympanometry every 4 to 6months to detect middle ear effusion which would raisesuspicion for a nasopharyngeal mass are also recommended[6]
The outcome of CS patients with RMS has been compa-rable to that for patients without the syndrome with a 5-yearsurvival rate of 65 to 70 [19] but according to this reviewit could be worse than the general population Neoplasia wasnoted at the cause of death in five (22) patients with CS[4 15] but in our study the mortality associated with RMSwas 43 Because the long-term survival in RMS is basedon the histology of the tumor and the extent of disease atdiagnosis early diagnosis may alter the treatment regimenand improve prognosis This could be particularly importantin patients with CS who often are medically fragile [20]
The RasMAPK pathway is an attractive target in thetreatment of cancer utilizing small molecule therapeuticsthat specifically inhibits the pathway Ras pathway agentssuch as farnesyltransferase inhibitors (tipifarnib and lona-farnib) that prevent posttranslational modification of Rasare being evaluated for cancer treatment and may be oftherapeutic use for syndromes in this pathway especially CSIn addition B-Raf protooncogene serinethreonine kinase(BRAF) and mitogenextracellular signal-regulated kinase(MEK) inhibitors offer the same potential in the possibletreatment of CS Since the RasMAPK pathway has targets forinhibition in cancer treatment there aremany smallmoleculetherapeutics that are in development or undergoing clinicaltrials with some already FDA approval [43]
6 ConclusionsCS is a syndrome poorly known in oncology but theirpredisposition tomalignancies includingULRMS implies theneed for a new perspective on early diagnosis and aggressivemedical and surgical treatment
ConsentInformed consent was obtained from the new two individualparticipants included in the study and has been properlydocumented with the parental approval to the use of patientrsquosimages and complementary studies
12 Case Reports in Genetics
Competing Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
Special thanks are due to Israel Fernandez Pineda MDAssistantMember and Surgery Fellowship ProgramDirectorSt Jude Childrenrsquos Research Hospital (Memphis TN) for therecommendations and corrections to the manuscript
References
[1] E Quezada and K W Gripp ldquoCostello syndrome and relateddisordersrdquo Current Opinion in Pediatrics vol 19 no 6 pp 636ndash644 2007
[2] JM Costello ldquoA new syndromerdquoNewZealandMedical Journalvol 74 article 397 1971
[3] JMCostello ldquoAnew syndromemental subnormality andnasalpapillomatardquo Australian Paediatric Journal vol 13 no 2 pp114ndash118 1977
[4] K W Gripp and A E Lin ldquoCostello syndrome a Rasmitogenactivated protein kinase pathway syndrome (rasopathy) result-ing from HRAS germline mutationsrdquo Genetics in Medicine vol14 no 3 pp 285ndash292 2012
[5] B Kerr M-A Delrue S Sigaudy et al ldquoGenotype-phenotypecorrelation in Costello syndrome HRAS mutation analysis in43 casesrdquo Journal of Medical Genetics vol 43 no 5 pp 401ndash4052006
[6] N Ahmadi and E Harley ldquoCostello syndrome and the impor-tance of cancer screeningrdquo Archives of OtolaryngologymdashHeadand Neck Surgery vol 136 no 10 pp 1028ndash1029 2010
[7] B Kerr O B Eden R Dandamudi et al ldquoCostello syndrometwo cases with embryonal rhabdomyosarcomardquo Journal ofMedical Genetics vol 35 no 12 pp 1036ndash1039 1998
[8] K W Gripp C I Scott Jr L Nicholson et al ldquoFive additionalCostello syndrome patients with rhabdomyosarcoma proposalfor a tumor screening protocolrdquo American Journal of MedicalGenetics vol 108 no 1 pp 80ndash87 2002
[9] K W Gripp A E Lin D L Stabley et al ldquoHRAS mutationanalysis in Costello syndrome genotype and phenotype corre-lationrdquo American Journal of Medical Genetics Part A vol 140no 1 pp 1ndash7 2006
[10] M Feingold ldquoCostello syndrome and rhabdomyosarcomardquoJournal of Medical Genetics vol 36 no 7 pp 582ndash583 1999
[11] S M White J M Graham Jr B Kerr et al ldquoThe adultphenotype in Costello syndromerdquo American Journal of MedicalGenetics A vol 136 no 2 pp 128ndash135 2005
[12] G Bisogno A Murgia I Mammi M S Strafella and M CarlildquoRhabdomyosarcoma in a patient with cardio-facio-cutaneoussyndromerdquo Journal of Pediatric HematologyOncology vol 21no 5 pp 424ndash427 1999
[13] S Sigaudy G Vittu A David et al ldquoCostello syndrome reportof six patients including one with an embryonal rhabdomyosar-comardquoEuropean Journal of Pediatrics vol 159 no 3 pp 139ndash1422000
[14] A Hinek M A Teitell L Schoyer et al ldquoMyocardial storage ofchondroitin sulfate-containing moieties in Costello syndromepatients with severe hypertrophic cardiomyopathyrdquo AmericanJournal of Medical Genetics vol 133 no 1 pp 1ndash12 2005
[15] A E Lin P D Grossfeld R M Hamilton et al ldquoFurtherdelineation of cardiac abnormalities in Costello syndromerdquoAmerican Journal of Medical Genetics vol 111 no 2 pp 115ndash1292002
[16] A L Estep W E Tidyman M A Teitell P D Cotter and KA Rauen ldquoHRASmutations in Costello syndrome detection ofconstitutional activating mutations in codon 12 and 13 and lossof wild-type allele in malignancyrdquo American Journal of MedicalGenetics vol 140 no 1 pp 8ndash16 2006
[17] H KawameMMatsui K Kurosawa et al ldquoFurther delineationof the behavioral and neurologic features inCostello syndromerdquoAmerican Journal of Medical Genetics vol 118A no 1 pp 8ndash142003
[18] B Kerr M A Einaudi P Clayton et al ldquoIs growth hormonetreatment beneficial or harmful in Costello syndromerdquo Journalof medical genetics vol 40 no 6 article e74 2003
[19] J P OrsquoNeal J Ramdas W E Wood and P K PellitterildquoParameningeal rhabdomyosarcoma in a patient with Costellosyndromerdquo Journal of Pediatric HematologyOncology vol 26no 6 pp 389ndash392 2004
[20] K W Gripp ldquoTumor predisposition in Costello syndromerdquoAmerican Journal of Medical Genetics Part C Seminars inMedical Genetics vol 137C no 1 pp 72ndash77 2005
[21] Y Aoki T Niihori H Kawame et al ldquoGermline mutationsin HRAS proto-oncogene cause Costello syndromerdquo NatureGenetics vol 37 no 10 pp 1038ndash1040 2005
[22] Y Abe Y Aoki S Kuriyama et al ldquoPrevalence and clinicalfeatures of Costello syndrome and cardio-facio-cutaneous syn-drome in Japan findings from a nationwide epidemiologicalsurveyrdquo American Journal of Medical Genetics Part A vol 158no 5 pp 1083ndash1094 2012
[23] I F M Lo C Brewer N Shannon et al ldquoSevere neonatal man-ifestations of Costello syndromerdquo Journal of Medical Geneticsvol 45 no 3 pp 167ndash171 2008
[24] J Menke S Pauli M Sigler et al ldquoUniparental trisomy of amutated HRASproto-oncogene in embryonal rhabdomyosar-coma of a patient with costello syndromerdquo Journal of ClinicalOncology vol 33 no 13 pp e62ndashe65 2015
[25] C P Kratz L Franke H Peters et al ldquoCancer spectrum andfrequency among children with Noonan Costello and cardio-facio-cutaneous syndromesrdquo British Journal of Cancer vol 112no 8 pp 1392ndash1397 2015
[26] H K Ransom ldquoSarcoma of the urachus review of the literaturewith report of an additional caserdquo The American Journal ofSurgery vol 22 no 2 pp 187ndash191 1933
[27] E M L-T Fernandez N H Siverio R L Almaraz L MViota J R Luis and L D Flores ldquoRadical surgery and IVA-chemotherapeutic regimen to treat embryonal rhabdomyosar-coma of the urachus case reportrdquo Pediatric Hematology andOncology vol 24 no 7 pp 543ndash550 2007
[28] M Ishikawa T Nishi R Yamada et al ldquoA case of urachalsarcoma in childhood case report and review of the worldliteraturerdquo Journal of the Japanese Society of Pediatric Surgeonsvol 21 pp 128ndash135 1985
[29] S Yokoyama YHayashida J Nagahama et al ldquoRhabdomyosar-coma of the urachus a case reportrdquo Acta Cytologica vol 41 no4 pp 1293ndash1298 1997
[30] U Schulz and C P OrsquoLeary ldquoSpinal AVM epidermal nevusand rhabdomyosarcoma a rare neurocutaneous syndromerdquoNeurology vol 56 no 3 pp 395ndash397 2001
Case Reports in Genetics 13
[31] A Cheikhelard S Irtan D Orbach et al ldquoUrachal rhab-domyosarcoma in childhood a rare entity with a poor out-comerdquo Journal of Pediatric Surgery vol 50 no 8 pp 1329ndash13332015
[32] K W Gripp E Hopkins K Sol-Church et al ldquoPhenotypicanalysis of individuals with Costello syndrome due to HRASpG13Crdquo American Journal of Medical Genetics Part A vol 155no 4 pp 706ndash716 2011
[33] M Tarnowski G Schneider G Amann et al ldquoRasGRF1 reg-ulates proliferation and metastatic behavior of human alveolarrhabdomyosarcomasrdquo International Journal of Oncology vol 41no 3 pp 995ndash1004 2012
[34] J-S Yu K W Kim H-J Lee Y-J Lee C-S Yoon and M-J Kim ldquoUrachal remnant diseases spectrum of CT and USfindingsrdquo Radiographics vol 21 no 2 pp 451ndash461 2001
[35] C P Kratz S Rapisuwon H Reed H Hasle and P S Rosen-berg ldquoCancer in Noonan Costello cardiofaciocutaneous andLEOPARD syndromesrdquo American Journal of Medical GeneticsPart C Seminars in Medical Genetics vol 157 no 2 pp 83ndash892011
[36] B Kerr M L Mucchielli S Sigaudy et al ldquoIs the locus forCostello syndrome on 11prdquo Journal of Medical Genetics vol 40no 6 pp 469ndash471 2003
[37] TNiihori YAokiNOkamoto et al ldquoHRASmutants identifiedin Costello syndrome patients can induce cellular senescencepossible implications for the pathogenesis of Costello syn-dromerdquo Journal of Human Genetics vol 56 no 10 pp 707ndash7152011
[38] G Rosenberger S Meien and K Kutsche ldquoOncogenic HRASmutations cause prolonged PI3K signaling in response toepidermal growth factor in fibroblasts of patients with costellosyndromerdquo Human Mutation vol 30 no 3 pp 352ndash362 2009
[39] M R DeBaun ldquoScreening for cancer in children with Costellosyndromerdquo American Journal of Medical Genetics vol 108 no1 pp 88ndash90 2002
[40] K W Gripp H Kawame D H Viskochil and L NicholsonldquoElevated catecholamine metabolites in patients with Costellosyndromerdquo American Journal of Medical Genetics vol 128 no1 pp 48ndash51 2004
[41] M-ADelrue B Arveiler andD Lacombe ldquoCostello syndromeclinical features and tumoral riskrdquo Archives de Pediatrie vol 9no 10 pp 1059ndash1063 2002
[42] V Martınez-Gonzalez and P Lapunzina Sındrome de CostelloGrupodeTrabajo sobreCancer en SındromeGeneticos Polimar-formativos (GT-CSGP) httpswwworphanetdatapathoProesCSGP-Costello-3pdf
[43] K A Rauen A Banerjee W R Bishop et al ldquoCostello andcardio-facio-cutaneous syndromes moving toward clinical tri-als in RASopathiesrdquo American Journal of Medical Genetics PartC Seminars inMedical Genetics vol 157 no 2 pp 136ndash146 2011
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

2 Case Reports in Genetics
(a) (b) (c)
(d) (e) (f)
Figure 1 Patient 1 (a) Photograph of the physical features of the patient with low-set ears lower palpebral fissures hypertelorism broadnasal bridge thick lips and thin hair (b) Abdominal ultrasound showing the presence of a solid mass paravesical displacing the left ovaryand bladder without infiltrate surrounding structures (c) Initial MRI showing a hyperintense tumor predominantly heterogeneous intensityon T2-weighted sequence compressing the bladder ((d) and (e)) MRI on T1-weighted sequences after 3 cycles of chemotherapy with slightdecrease in left paravesical oval mass (f) Operative image indicating the presence of tumor originating in the left medial UL
activated protein kinase (MAPK) pathway [1] The mostcommon tumor associated with CS is RMS mainly involvingabdomen pelvis andor urogenital area [6] The first twoCS patients associated with RMS were described in 1998 [7]before that date this syndrome was mainly associated withbenign tumors especially papillomata [3]
We here report two children with CS and RMS of theumbilical ligament (UL) No prior correlation of this tumorlocation with CS had been described so far
2 Case Presentation
21 Case 1 This is a 44-year-old female She is thirdchild of healthy unrelated parents with no family historyof note Pregnancy was complicated with polyhydramniosThe patient was born from a preterm delivery (33 weeks)large (2840 gr) for gestational age She presented feedingdifficulties from the beginning that required nasogastrictube feeding and later gastrostomy at the age of 4 monthsCardiological examination showedmild pulmonary stenosisShe was referred to the Genetics Clinic for assessment atthe age of 6 months because of failure to thrive hypotoniaand dysmorphic features On examination she had featureshighly suggestive of a RASopathy but on account of the
skin findings (sparse hair glabellar capillary malformationa large 4 times 12 cm cafe-au-lait spot in her right flank and twoblue nevi in right temporal region and left groin) difficult todifferentiate with certainty between CS and Cardiofaciocuta-neous syndrome HoweverHRASmutation analysis demon-strated a common recurrent mutation (pG12S) confirmingthe diagnosis of CS in this child at the age of 7 months(Figure 1(a)) Because of the high risk of tumor developmentassociated with this condition close follow-up was indicatedaccording to the recommended tumor screening protocol [820] An abdominal ultrasound scan performed at the age of 16months revealed a 31 times 32mm paravesical solid pelvic masswith minimal intralesional vascularity no intraabdominalfree fluid or lymphadenopathies were seen The ovaries werenot involved (Figure 1(b)) Magnetic resonance imaging(MRI) showed a left paravesical tumor (3 times 5 times 27 cm)without associated lymphadenopathies hypointense on T1-weighted sequences and hyperintense with predominantlyheterogeneous intensity on T2-weighted sequencesThemasscaused compression and displacement of the bladder tothe right side (Figure 1(c)) Tumor markers were as fol-lows beta-subunit of human chorionic gonadotropin (120573-hCG) lt 2mUImL (normal lt 60) alpha-fetoprotein (120572FP)29 ngmL (normal lt 80) carcinoembryonic antigen (CEA)
Case Reports in Genetics 3
08 ngmL (normal lt 50) CA-153 197UImL (normal lt320) CA-199 437UImL (normal lt 370) and neuronspecific enolase (NSE) 2786 ngmL (normal 0ndash160)Thoraciccomputed tomography (CT) and scintigraphy showed noevidence of metastasis Bone marrow biopsy was normalTru-Cut biopsy guided by ultrasound reported an embryonalRMS with a proliferation index Ki-67 of 60 mesenchymalmalignant round cell and short spindle tumor vimentin(+) desmin (focal +) MyoD1 (focal +) CD99 (+ focalstaining) S100 protein (minus) pancytokeratins AE1AE3 (minus)synaptophysin (minus) and CD99 (minus) She was enrolled onthe standard risk group protocol European pediatric Softtissue Sarcoma Study Group (EpSSG) RMS 2005 subgroup Dwith 3 neoadjuvant chemotherapy cycles Preoperative MRIshowed a slight decrease in tumor size (32 times 3 times 25 cms)(Figures 1(d) and 1(e)) At the definitive surgery a 5 cmtumor dependent of the remaining left umbilical artery (leftmedial UL) located slightly to the left and displacing thebladder dome was found (Figure 1(f)) Complete resectionof the tumor was performed No pathological lymph nodeswere observed Final pathology report showed an embryonalRMS with signs of response to chemotherapy (maturationphenomenon at cytoplasmic and nuclear level of the tumorcellularity) with maximum cell proliferation index Ki-67 of5ndash10 almost all undifferentiated except in a small regionresection margins were negative for tumor (1ndash4mm fromthe edges of radial resection margin and 3 cm of UL)Chemotherapywas then continueduntil completing 25weeksand coadjuvant radiotherapy was administrated after thecompletion of chemotherapy At 23months of follow-up afterdiagnosis no residual tumor or relapse has been identified
22 Case 2 This is a 54-year-old female She is the first andonly child of a healthy nonconsanguineous couple with unre-markable family history Pregnancy was complicated withpolyhydramnios and delivery was preterm (34 weeks) with ahigh birth weight (2980 g +26 SD) She was admitted to theneonatal ward for investigation of a suspected dysmorphicsyndrome and initial FGFR3 molecular genetic testing forachondroplasia revealed no mutations Feeding difficultiesand failure to thrive were noted from the beginning requiringnutritional intervention and gastrostomy feeding from theage of 10 months She had a heart murmur with a normalechocardiogram She also had bronchomalacia and at MRInonspecific white matter hyperintensities in CNS She wasreferred to our clinical Genetics Clinic for evaluation at theage of 4 months and in view of her previous history andclinical findings CS was suspected HRAS Sanger sequencingdetected the common c34GgtA (pG12S) mutation confirm-ing the diagnosis of CS (Figure 2(a)) As part of the follow-up the recommended tumor screening protocol was arrangedand at the age of 3 years she underwent an abdominalultrasound that showed a tubular image running throughthe theoretical place of the umbilical arteries with a largercaliber on the right side of 56mm and associated echoesinside without Doppler flow (Figure 2(b)) Two subsequentultrasounds did not show any abnormality A new abdominalultrasound 9 months later reported the presence of a hypoe-choicmultilobulated solid tumor (53times 28 cm) in themidline
extending to the right in supravesical region with markedhypervascularization and extending cranially to the vicinityof the abdominal wall (Figures 2(c) and 2(d)) MRI showeda solid abdominal tumor (6 times 55 times 3 cm) composed ofnodular masses grouped in the UL region with involvementof the medial umbilical folds that were thickened throughoutthe iliac vessels region (Figure 2(e)) No regional metastaticdisease was observed Tumor markers were as follows 120572FPlt 13 ngmL CEA 53 ngmL and CA-199UImL No lungmetastases were observed in the thoracic CT scan and bonemarrow biopsywas normal She underwent a complete tumorresection (Figure 2(f)) The mass was located on the rightmedial UL (from its insertion into the right iliac artery tothe umbilicus) Pathology report showed a spindle cell RMSwith microscopic positive margins in 2 submitted samples(85 times 5 times 3 cm and 35 times 15 times 1 cm) and one resected lymphnode was negative for malignancy Tumor was composedof spindle cells that form cross linked bundles varyingdegrees with elongated oval nuclei vesicular configurationswith coarse chromatin The tumor had a pattern of nodulargrowth markedly myxoid stroma with microcystic focaldegeneration and 5 tumor necrosis no lymphovascularinvasion maximum proliferation index Ki67 of 30 musclespecific actin (+) desmin (+) WT1 (+ cytoplasmic) MyoD1(+ nuclear) and CD99 (minus) Two weeks after surgery thestandard risk group protocol EpSSG RMS 2005 subgroup B(Stage I) chemotherapy was started that includes ifosfamidevincristine and actinomycin D At 18 months of follow-up after diagnosis no residual tumor or relapse has beenidentified
3 Methods
We describe two new cases of RMS and CS based onmedicalrecords of patients diagnosed at the Institute of Medicaland Molecular Genetics and treated at the Departmentsof Pediatric Hematology-Oncology and Pediatric SurgeryUniversity Hospital La Paz (Madrid Spain) A review of theliterature published in English in MEDLINE from January1971 to June 2016 using the search terms CS and RMS wasdone also the references contained in these articles even ifthey were not indexed inMEDLINE were analyzed A reviewfrom January 1933 until June 2016 of all reported pediatriccases of UL RMS including as search criteria UL RMSurachus and umbilical arteries was performed
4 Results
In all cases analyzed and reviewed (same cases reportedin more than one publication were counted once) it waspossible to document the presence of 26 patients with CSand RMS (Table 1) [5ndash25] including the 2 cases describedherein The mean age of diagnosis was 2 years and 8 months(range 6 monthsndash7 years) It was slightly more commonin females than in males (12 1) The commonest locationwas the abdomenpelvis (1020) including 4 out of 10 ofthose in the UL The most common histological type wasembryonal RMS (1419) Seven out of nine patients who died(and with reported histology) showed embryonal RMS The
4 Case Reports in Genetics
(a) (b) (c)
(d) (e) (f)
Figure 2 Patient 2 (a) Photograph of the physical features of the patient with prominent forehead low-set ears lower palpebral fissureshypertelorism broad nasal bridge thick lips and anteverted slightly nostrils (b) Initial abdominal ultrasound showing the presence ofa tubular image caliber of 56mm extending in the theoretical location of the right umbilical artery ((c) and (d)) Follow-up abdominalultrasound in themidline showing amultilobulated hypoechoic solid tumorwithmarked hypervascularization extending from the proximityof the abdominal wall to the right supravesical region (e) MRI onT2-weighted sequence confirms the presence of several nodular massesgrouped with thickening of both medial umbilical folds the right to 4mm proximal to the umbilicus and 8mm adjacent to the iliac vesselsparavesical region portion (f) Operative image indicating the presence of tumor originating in the right medial UL
most frequent encountered HRAS mutation associated withRMS was pG12S (712) Only 4 deaths were documented inpatients with change in codon 12 (2 patients G12S 1 patientG12A and 1 patient G12C) Chemotherapy that was appliedvaries based on the protocols of the countries where theywerediagnosed (Table 2) [5ndash10 12ndash14 16ndash25] Overall survival wasabout 43 (921) Mortality was observed in 12 out of 21individuals in nine of them associated with neoplasia andin three associated with surgery
Similarly the total number of reported cases of ULRMS in pediatric patients either in the obliterated umbilicalarteries (medial UL) or in urachus (median UL) is 17including these 2 new cases (Table 3) [5 7ndash9 24ndash31] Themean age of diagnosis was 3 years and 4 months (range 4monthsndash6 years) It is slightly more common in females thanin males (14 1) Themost common location was the urachus(1517) The most common histological type was embryonalRMS (1215) and one-fourth (312) of patients who died withreported histology showed embryonal RMS Chemotherapyvaries based on the protocols of the countries where theywerediagnosed (Table 4) [7 24 26ndash31] Overall survival was 69
(1116) overall mortality was 31 (516) two-year absolutesurvival rate was 69 (1116) and five-year absolute survivalrate was 19 (316)
5 Discussion
The prevalence of CS is estimated to be 1 1290000 individ-uals in Japan and at least 1 500000 in the United Kingdomthe incidence was estimated to be 1 60000ndash100000 [4 22]The overall tumor incidence is approximately 10ndash15 overthe lifetime of individuals with an identified HRASmutation[1 4 9] RMS accounting in about 60 of all neoplasia [1]Based on the 300 cases of CS currently known [4] we foundan incidence of 87 RMS in patients with CS
CS is the first disorder associated with germlinemutations in the Ras family of guanosine-51015840-triphosphate(GTP)ases [21] HRAS has six exons five exons are encodedfor a protein of 189 amino acids with a molecular weight of21 kDa [4] Missense mutations at codons 12 and 13 are inconstitutively active GTP-bound conformation and activatedownstream effectors such as MAPK phosphatidylinositol3-kinases (PI3K) and ral guanine nucleotide dissociation
Case Reports in Genetics 5
Table1Ch
aracteris
ticso
fpatientsw
ithCostello
synd
romea
ndrhabdo
myosarcom
a
PT number
Author
Year
Cou
ntry
Sex
Age
atdiagno
sis(yearsm
onths)
Symptom
sLo
catio
nHistolog
yMutation
AAC
(NS)
Therapy
Outcome
1Ke
rretal
[78]
1998
England
F2y
4mVo
miting
Con
stipatio
nRe
troperiton
ealleft
psoasm
ayor
muscle
Embryonal
G12S
(34GgtA)lowast
[9]
SCh
TRe
lapsetumor-fr
eeageo
f7years
2Ke
rretal
[78]
1998
England
F3y
2mAb
dominal
mass
Pelvis
urachu
s(m
edianUL)
adherent
tothe
bladder
Embryonal
G12A
(35GgtC)
[5]
SCh
T
Histologyshow
edextend
ingup
tothe
resectionmargin
Diedaged
5years
[59]
3Feingold
[810]
1999
USA
M6m
Tumor
Rightfoo
tAlveolar
NDF
SCh
TTu
mor-fr
eeageo
f20
years[11]
4Bisogn
oetal
[8912]
1999
Italy
M1y
8mCon
stipatio
nAb
dominal
pain
Lower
abdo
men
pelvis
abdo
minal
walllowast
Embryonal
NDF
SCh
TOnlybiop
syDiedaged
2yearsa
nd3mon
ths
5Sigaud
yetal
[813]
2000
France
M6y
NDF
Inguinalscrotal
Embryonal
NDF
NDF
NDF
6Grip
petal
[81415]
2002
USA
M5y
6mAb
dominal
pain
Pelvis
pulm
onary
metastasesw
aspresent
Embryonal
NDF
SCh
TDiedaft
errecurrence
[14]
7Grip
petal
[8]
2002
USA
F3y
7mAb
dominal
pain
Emesis
Upp
erabdo
men
masse
ncasingthe
superio
rmesenteric
anceliaca
rteries
Sing
lepu
lmon
ary
nodu
le
Pleomorph
icNDF
ChT
Diedaged
4years
8Grip
petal
[8]
2002
USA
F2y
6mAb
dominal
mass
Pelvis
bladder
Embryonal
NDF
ChT
RTS
Diedaged
7yearsfor
recurrency
ofRM
Sfib
rosarcom
a[16]
9Grip
petal
[8]
2002
USA
NDF
7mPerin
eal
grow
thPerin
eal
Embryonal
NDF
ChT
RTS
Tumor-fr
eeageo
f2years
10Grip
petal
[8]
2002
USA
NDF
1y11m
Prop
tosis
Leftorbit
Unk
nown
NDF
SRT
Tumor-fr
eeageo
f4years
11Ka
wam
eetal
[17]
2003
Japan
F1y
4mAb
dominal
mass
Pelvis
Spindlec
ell
NDF
SCh
TTu
mor-fr
eeageo
f7years
6 Case Reports in GeneticsTa
ble1Con
tinued
PT number
Author
Year
Cou
ntry
Sex
Age
atdiagno
sis(yearsm
onths)
Symptom
sLo
catio
nHistolog
yMutation
AAC
(NS)
Therapy
Outcome
12Ke
rretal
[18]
2003
UK
M2y
2mLargep
elvic
mass
Retro
vesic
ular
mass
byultrasou
ndEm
bryonal
NDF
ChT
Diedaged
2yearsa
nd4mon
ths
13OrsquoNealetal
[19]
2004
USA
F3y
Right-s
ided
cervicofacial
mass
Parameningeal
infratem
poralfossa
right
perip
arotid
mastic
ator
space
region
Alveolar
NDF
ChTS
RT
Clinicalgrou
p3T2
bN0stage3
Dieddu
ringsurgery
14Grip
p[20]
2005
USA
F3y
2mFacialmass
Rightinfratempo
ral
fossa
Mixed
alveolar
and
embryonal
NDF
ChTS
Dieddu
ringsurgery
byventric
ular
tachycardiafollowed
rapidlyby
lossof
heartrhythm
15Ao
kietal
[2122]
2005
Japan
F7y
2mNDF
NDF
NDF
G12S
(34GgtA)
NDF
NDF
16Grip
petal
[9]
2006
USA
M2y
NDF
NDF
NDF
G12S
(34GgtA)
NDF
Tumor-fr
eeageo
f11
yearslowast
17Ke
rretal[5]
2006
UK
NDF
7mNDF
Metastatic
arising
from
thep
rosta
teEm
bryonal
[23]
G12C
(34GgtT)
NDF
Diedaged
7mon
ths
18Ke
rretal[5]
2006
UK
NDF
NDF
NDF
NDF
NDF
G12S
(34GgtA)
NDF
Diedaged
7years
19Ke
rretal[5]
2006
UK
NDF
NDF
NDF
NDF
NDF
G12A
(35GgtC)
NDF
NDF
20Lo
etal[23]
2008
UK
M2y
3mRe
spira
tory
functio
ndeterio
rated
Rightlun
gNDF
G12S
(34GgtA)
SDiedfewweeks
later
surgery
21Ahm
adiand
Harley[6]
2010
USA
M2y
Increasedwork
ofbreathing
Nasop
haryngeal
Embryonal
NDF
SCh
TRT
Clinicalgrou
pIIA
(T1N
0M0)
Tumor-fr
eeageo
f3years
22Ab
eetal[22]
2012
Japan
NDF
NDF
NDF
NDF
NDF
NDF
NDF
Died
23Menke
etal
[2425]
2015
Germany
F3y
Abdo
minal
mass
Lower
anterio
rabdo
menabo
vethe
urinarybladderlowast
(urachus-m
edianUL
bylocatio
n)
Embryonal
G12C
(34GgtT)
SCh
T
R1resection
(marginaltum
orresid
ue)Tu
mor-fr
eeageo
f6years
24Kr
atze
tal
[25]
2015
Germany
M1y
NDF
NDF
Embryonal
G12S
(34GgtA)
NDF
NDF
25
Sanchez-
Mon
tenegro
etal(this
repo
rt)
2017
Spain
F2y
4mAs
ymptom
atic
LeftmedialU
LEm
bryonal
G12A
(35GgtC)
ChTS
RTTu
mor-fr
eeageo
f4yearsa
nd4mon
ths
26
Sanchez-
Mon
tenegro
etal(this
repo
rt)
2017
Spain
F3y
10m
Asym
ptom
atic
Rightm
edialU
LSpindlec
ell
G12S
(34GgtA)
SCh
TTu
mor-fr
eeageo
f5yearsa
nd4mon
ths
AAC
aminoacid
changeC
hTchemotherapyFfem
aleMm
aleNDFno
datafoun
dNSnu
cleotides
ubstitutio
nPT
patientR
TradiotherapySsurgeryU
Lum
bilicalligam
entlowastPerson
alcommun
icationby
author
Case Reports in Genetics 7
Table 2 Chemotherapy of patients with Costello syndrome and rhabdomyosarcoma
PTnumber Chemotherapy protocol
1Initially with VCR ACD and CTX After debulking continued on ChT using IFOS VCR and ACD After the second coursewhen she developed IFOS induced encephalopathy she was changed back to pulses of VCR ACD and CTX given every 3weeks for 9 courses [7]
2Initially IFOS ACD and VCR After 4 courses CTX was substituted for IFOS because hemorrhagic cystitis Tx complicatedby recurrent episodes of moderately severe diarrhoea and febrile neutropenia requiring readmission to hospital Tx wascompleted after six courses of ChT [7]
3 Tx consisted of below the knee amputation and ChT (DOX ACD VCR and CTX) [10]
4
Tx was implemented according to the Italian protocol for pediatric soft tissue sarcoma Three courses of ChT including VCR(0025mgkg day 1) IFOS (50mgkg days 1 and 2) and alternating ACD (0025mgkg day 1) and DOX (07mgkg day 1) wereadministered Symptoms regressed and the CT scan showed a reduction in tumor volume of more than two-thirds After 3more courses of ChT the patient experienced abdominal pain A repeat abdominal CT scan showed an increase in the pelvicmass Despite the administration of a different ChT with CBDCA (11mgkg day 1) and VP-16 (3mgkg for 3 doses) the tumorcontinued to grow and the child died 7 months after the diagnosis of RMS [12]
5 NDF [13]
6
The first cycle of ChT with VCR ACD and CTX and topotecan reduced the tumor size [16] The tumor was surgicallyremoved after the first ChT [8] Debulking S was required because of rapid growth and tumor necrosis The protocol wascontinued and was deemed sufficiently successful to withhold RT One month after completion of the first protocol tumorrecurrence necessitated a second round of ChT with irinotecan and DOXThe latter drug was administered about 1 weekbefore he died during which time he had tachycardia (heart rate 180ndash20 bpm) [14]
7 The tumor did not respond to ChT and she died shortly after her 4th birthday [8]8 Tx was a combination of S ChT and RT continued until age of 35 years [8]9-10 NDF [8]11 PT had later generalized tonic-clonic seizures during her Tx for RMS [17]12 Despite extensive ChT the tumor progressed rapidly and the PT died 2 months later [18]
13 Induction ChT was commenced with the initial 12-week course of VCR ACD and CTX based on the Intermediate RiskProtocol D9803 of the COG [19]
14 ChT did not result in tumor shrinkage therefore surgical resection was performed [20]15ndash22 NDF [5 6 9 21ndash23]23 ChT according to the cooperative soft tissue sarcoma protocol (CWS-2002 P) was well tolerated by the PT [24]24 NDF [25]
25 ChT in the standard risk group protocol EpSSG RMS 2005 subgroup D 3 preoperative cycles of IFOS (2 doses at 100mgkg)VCR (005mgkg) and ACD (005mgkg)
26 ChT (postoperative 15 days) in the standard risk group protocol EpSSG RMS 2005 subgroup B (Stage I) cycles of IFOS (2doses of 3 gm2d) VCR (15mgm2) and ACD (15mgm2) was initiated
ACD actinomycin D CBDCA carboplatin ChT chemotherapy COG childrenrsquos oncology group CTX cyclophosphamide CT computed tomography CWSCooperative Weichteilsarkom Studie (Cooperative Soft Tissue Sarcoma Study) DOX Doxorubicin EpSSG European pediatric Soft tissue sarcoma StudyGroup IFOS ifosfamide NDF no data found PT patient RMS rhabdomyosarcoma RT radiotherapy S surgery Tx treatment VCR vincristine VP-16etoposide
stimulator (RalGDS) [16 21] in signaling pathways control-ling cell proliferation and differentiation [9]
Themajority of patients with CS had 34GgtA transition incodon 12 (80) [4 16] More than 95 of the mutations arepredicted to result in substitution of the glycine in position12 or 13 of the protein product [1] All individuals withmalignancy had a codon 12 mutation (especially G12A 47patients) [5 21] The rare G12V mutation is associated witha more severe early lethal phenotype some patients diefrom respiratory distress hypertrophic cardiomyopathy ormalignant tachycardia prior to being diagnosed with CS [1]As far as we know no individual with G13C has developed amalignant tumor [4 32]
RMS is the most common soft tissue sarcoma of infancyIts incidence is between 4 and 7 cases per 1 million childrenyounger than 15 years [8 12] The age peak is between 2 and5 years with a slight male predominance (12ndash141) Thesetumors may arise anywhere in the body and fewer than 20are located in the pelvis [12]Most RMS tumors are originatedin the head and neck region urogenital tract and extremities[33] The most common histologic type seen in gt50 isembryonal followed by alveolar in 20ndash30 PleomorphicRMS is rare (1) and has a poor prognosis [8] AlveolarRMS is characterized by the translocation t(213)(q35q14) in70 of cases and the variant translocation t(113)(p36q14)in a smaller percentage of cases Evidence accumulates
8 Case Reports in Genetics
Table3Ch
aracteris
ticso
fPediatricPatie
ntsw
ithUmbilicalLigamentR
habd
omyosarcom
a
PT number
Author
Year
Cou
ntry
Sex
Age
atdiagno
sis(yearsm
onths)
Symptom
sLo
catio
nSize
(cm)
Histology
IRS
grou
pTh
erapy
Outcome
1Ra
nsom
[2627]
1933
USA
F4m
Massb
elowthe
umbilicus
and
extend
ing
somew
hattothe
right
Urachus
(medianUL)
attached
alon
gthea
nterior
wallfrom
theu
mbilicus
tothea
pexof
theb
ladd
er
115
Spindle
cell
ISM
AC
RT
Lastcheck-up
exam
ination(2
years)
show
edno
evidence
ofrecurrence
2Ishikawae
tal[28]
1985
Japan
F1y
4mAb
dominalmass
abdo
minalpain
hemop
erito
neum
Urachal(m
edianUL)
intra-abdo
minalruptureo
fthetum
or
Fist-
sized
NDF
IVSM
ACNDF
3Yo
koyamae
tal[2729]
1997
Japan
M2y
Episo
diclow
erabdo
minalpain
Urachus
(medianUL)
extraperito
neallocated
betweentheu
mbilicus
and
apex
oftheb
ladd
erandwas
adherin
gtig
htlyto
both
Theb
ilateralm
edialU
Lweres
eenenterin
gthe
tumorR
upturedwith
asm
alln
umbero
fdissem
inated
tumors
scatteredon
them
esentery
andDou
glas
pouch
12Em
bryonal
IVSM
AI
ChT
At2yearso
ffollo
w-upno
recurrence
hadbeen
detected
4lowastKe
rretal
[78]
1998
England
F3y
2mAb
dominalmass
Urachus
(medianUL)
adherent
totheb
ladd
erNDF
Embryonal
IIaSM
II
ChT
Histologyshow
edextend
ingup
tothe
resectionmargin
Diedaged
5years
[59]
5Schu
lzand
OrsquoLeary
[2730]
2001
Scotland
M2y
NDF
Urachus
(medianUL)
NDF
Embryonal
NDF
SCh
TRT
Tumor-fr
eeageo
f26
years
6Fernandeze
tal[27]
2007
Spain
F6y
Intractable
constip
ation
nauseaabd
ominal
painles
smass
Urachus
(medianUL)
infiltratingthev
entral
abdo
minalwalland
fixed
tothev
esicaldo
me
135
Embryonal
IbSM
IC
ChT
At4yearso
ffollo
w-upthep
atient
remains
welland
free
ofclinicald
isease
7lowastMenke
etal
[2425]
2015
Germany
F3y
Abdo
minalmass
Lower
anterio
rabd
omen
abovethe
urinarybladderamp
(urachusm
edianULby
locatio
n)
NDF
Embryonal
IIaSM
II
ChT
R1resection
(marginaltum
orresid
ue)Tu
mor-fr
eeageo
f6years
8Ch
eikh
elard
etal[31]
2015
Dx
1983
France
F5y
5mNDF
Urachus
(medianUL)
periton
ealm
etastasesa
ndhypo
gastric
lymph
nodes
5NDF
IVSM
AI
ChT
Died31
mon
thsa
fter
diagno
siswith
relap
sein
periton
ealliver
at11mon
ths
Case Reports in Genetics 9
Table3Con
tinued
PT number
Author
Year
Cou
ntry
Sex
Age
atdiagno
sis(yearsm
onths)
Symptom
sLo
catio
nSize
(cm)
Histology
IRS
grou
pTh
erapy
Outcome
9Ch
eikh
elard
etal[31]
2015
Dx
2003
France
F3y
3mPeriton
ealrup
ture
poor
generalstatus
Urachus
(medianUL)
lumbo
aorticandexternal
iliac
lymph
nodes
10Alveolar
IVSM
AI
ChTRT
Died57
mon
thsa
fter
diagno
siswith
relap
sein
periton
ealliver
at30
mon
ths
10Ch
eikh
elard
etal[31]
2015
Dx
2005
France
F2y
6mMasspo
orgeneral
statusdysuria
Urachus
(medianUL)
15Em
bryonal
III
SMII
ChTRT
Died37
mon
thsa
fter
diagno
siswith
periton
ealrelapse
at19
mon
ths
11Ch
eikh
elard
etal[31]
2015
Dx
2005
France
M4y
2mMasspo
orgeneral
statusdysuria
Urachus
(medianUL)
periton
ealm
etastasesa
ndiliac
lumbo
aorticlymph
nodes
10Em
bryonal
IVSM
II
ChTRT
Relapsed
multifocalat
82mon
thsfollo
w-up
100mon
ths
12Ch
eikh
elard
etal[31]
2015
Dx
2005
France
M5y
3mMasspo
orgeneral
status
Urachus
(medianUL)
periton
ealm
etastasesa
ndmesenteric
lymph
nodes
106
Embryonal
IVSM
IC
ChTRT
Tumor
freea
fter9
5mon
thssince
diagno
sis
13Ch
eikh
elard
etal[31]
2015
Dx
2006
France
M2y
5mMasspo
orgeneral
statusob
structiv
erenalinsuffi
ciency
Urachus
(medianUL)
periton
ealbon
emetastases
andhypo
gastric
lymph
nodes
21Em
bryonal
IVSM
II
ChTRT
Bone
progression
after
16mon
thsdied
18aft
erdiagno
sis
14Ch
eikh
elard
etal[31]
2015
Dx
2010
France
M4y
5mAb
dominalpain
Urachus
(medianUL)
7Em
bryonal
III
SMIC
ChT
Tumor
freea
fter18
mon
thssince
diagno
sis
15Ch
eikh
elard
etal[31]
2015
Dx
2010
France
M6y
Abdo
minalpain
Urachus
(medianUL)
periton
ealm
etastases
14Em
bryonal
IVSM
AI
ChTRT
Tumor
freea
fter4
5mon
thssince
diagno
sis
16lowast
Sanchez-
Mon
tenegro
etal(this
repo
rt)
2017
Dx
2015
Spain
F2y
4mAs
ymptom
atic
LeftmedialU
L5
Embryonal
IaCh
TSM
IC
RT
Tumor-fr
eeageo
f3yearsa
nd9mon
ths
17lowast
Sanchez-
Mon
tenegro
etal(this
repo
rt)
2017
Dx
2015
Spain
F3y
10m
Asym
ptom
atic
Rightm
edialU
L85
Spindle
cell
IIaSM
II
ChT
Tumor-fr
eeageo
f4yearsa
nd5mon
ths
ChT
chem
otherapyD
xdiagno
sed
Ffemale
IRS
intergroup
rhabdo
myosarcom
aMm
ale
NDF
nodata
foun
dRT
radiotherapy
Ssurgery
SMAIsurgerymacroscop
ically
incomplete
SMAC
surgery
macroscop
icallycompleteSM
ICsurgery
microscop
icallycompleteSM
IIsurgery
microscop
icallyincompleteULum
bilicalligam
ent
ampPerson
alcommun
icationby
authorlowast
Patientsw
ithCostello
synd
rome
10 Case Reports in Genetics
Table 4 Chemotherapy of pediatric patients with umbilical ligament rhabdomyosarcoma
PTnumber Chemotherapy protocol
1-2 No ChT [26 28]3 After establishment of the final diagnosis he was treated with combined ChT including VCR ACD and CTX [29]
4lowastInitially IFOS ACD and VCR After 4 courses CTX was substituted for IFOS because of hemorrhagic cystitis Tx complicatedby recurrent episodes of moderately severe diarrhoea and febrile neutropenia requiring readmission to hospital Tx wascompleted after six courses of ChT [7]
5 NDF [30]
6 PT started induction of ChT 2 weeks after S Induction regimen included 9 cycles of IVA (IFOS VCR and ACD) that were welltolerated with minimal systemic complications (Tx 953 of the MMT 95 SIOP protocol for RMS) [27]
7lowast ChT according to the cooperative soft tissue sarcoma protocol (CWS-2002 P) was well tolerated by the PT [24]8 Adjuvant ChT with 10 cycles of IFOS VCR and ACD [31]9 Adjuvant ChT with 6 cycles of IFOS VCR and VP-16 and 9 cycles of VCR ACD CTXACD and CTX [31]10 Neoadjuvant ChT with 6 cycles of IFOS VCR and ACD and adjuvant ChT with 3 cycles of IFOS VCR and ACD [31]
11 Neoadjuvant ChT with 1 cycle of CTX VCR and PRED 2 cycles IFOS VCR and ACD and 4 cycles of IFOS VCR ACD andDOX and adjuvant ChT with 3 cycles of IFOS VCR and ACD [31]
12 Neoadjuvant ChT with 1 cycle of CTX VCR and PRED and 5 cycles of IFOS VCR ACD and DOX and adjuvant ChT with 2cycles of IFOS VCR ACD and DOX and 1 cycle of IFOS VCR and ACD [31]
13 Neoadjuvant ChT with 2 cycles of VCR ACD and CTX + and 3 cycles of IFOS VCR ACD and DOX and adjuvant ChT with 3cycles of IFOS VCR and ACD [31]
14 Neoadjuvant ChT with 4 cycles of IFOS VCR ACD and DOX and adjuvant ChT with 5 cycles of IFOS VCR ACD [31]
15 Neoadjuvant ChT with 4 cycles of IFOS VCR ACD DOX 3 cycles of IFOS VCR ACD and adjuvant ChT with 1 cycle of IFOSVCR ACD 1 cycle of IFOS VCR [31]
16lowastChT in the standard risk group protocol EpSSG RMS 2005 subgroup D 3 preoperative cycles of IFOS (2 doses at 100mgkg)VCR (005mgkg) and ACD (005mgkg)
17lowastChT (postoperative 15 days) in the standard risk group protocol EpSSG RMS 2005 subgroup B (Stage I) cycles of IFOS (2 dosesof 3 gm2d) VCR (15mgm2) and ACD (15mgm2) was initiated
ACD actinomycin D ChT chemotherapy CTX cyclophosphamide CWS Cooperative Weichteilsarkom Studie (Cooperative Soft Tissue Sarcoma Study)DOX Doxorubicin EpSSG European pediatric Soft tissue sarcoma Study Group IFOS ifosfamide MMT malignant mesenchymal tumor NDF no datafound PRED prednisone PT patient RMS rhabdomyosarcoma S surgery SIOP Societe Internationale DrsquoOncologie Pediatrique (International Society ofPediatric Oncology) Tx treatment VCR vincristine VP-16 etoposide lowastPatients with Costello syndrome
that alveolar RMS and embryonal RMS are two differentdisorders while alveolar RMS may originate from primitiveuncommitted mesodermal cells embryonal RMS originatesprobably from more differentiated myoblasts Ras protein-specific guanine nucleotide-releasing factor 1 (RasGRF1)plays an important role in alveolar RMS pathogenesis Theseinteresting concepts however need more evidence [33]
The umbilicus caudally originates the common ligamentwhich is divided into obliterated umbilical arteries (medialUL) and urachus (median UL) The urachus varies from3 to 10 cm in length and from 8 to 10mm in diameterIt is a three-layered tubular structure the innermost layerbeing lined with transitional epithelium in 70 of casesand with columnar epithelium in 30 The structure issurrounded by connective tissue and outermost muscularlayer in continuity with the detrusor muscle Along its pathfrom the bladder to the umbilicus the urachus lies betweenthe transverse fascia and the parietal peritoneum containedin the pyramidal retropubic perivesical preperitoneal spacecompartmentalized by umbilicovesical fascia along with themedial umbilical ligaments and the bladder Occasionallythe urachus may merge with one or both of the obliteratedumbilical arteries (medial UL) and there may be a slight
deviation to the right or left of the midline [34] The urachusis an embryological remnant resulting from the obliterationof the allantoic channel which attaches the bladder dome tothe umbilicus [31]
Urachal malignant tumors are extremely rare represent-ing less than 05 of all bladder cancers and 001 of alltumors They may arise from any portion of the urachus andare most commonly found in adults and males (60ndash70)Although sarcomas represent only 8 they are the mostfrequent urachal neoplasms reported in patients youngerthan 20 years of age (67) [27] Poor prognosis is a commonfeature in adults and pediatric urachalmalignancies with 50to 60 of 5-year survival In contrast the 5-year event-freesurvival in pelvic RMS was reported to be about 51 [31]
This indolent and rather large urachal tumor was mostlyrevealed by an uncomplicated progressing mass withoutprodromic urological symptomsThedelay of diagnosis couldbe explained by a long asymptomatic progression of thetumor in a preperitoneal location which allows an importantlocal spreading before diagnosis Even in patients withouttumor rupture peritoneal involvement appeared to be the keypoint in the prognosis of urachal RMS Systematic cytologyat diagnosis could be more accurate to evaluate peritoneal
Case Reports in Genetics 11
extension in order to avoid understaging and adjust adjuvantlocoregional treatment [31]
Previously only 12 patients with RMS arising from theurachus (median UL) in children without CS have beenreported in the English literature (Table 3) By 2011 therewere29 reported cases of cancer in patients withCS 19 RMS (meanage of 23 years 9 embryonal 1 alveolar 1 mixed histology1 pleomorphic 1 spindle cell type and 6 unclassified) 5neuroblastomas 4 bladder cancer and 1 fibrosarcoma [35]
Loss of heterozygosity for 11p155 in RMS from individu-als with CS suggests that loss of the wild-type allele is the sec-ond hit in tumor development [6 16 36] Whereas theHRASmutation in a sporadic malignancy in the general populationis present only within the tumor cells in CS an identicalmutation is present in every single cell of the individualthus accounting for the tumor predisposition [1] implicatingan alternate mechanism of rhabdomyosarcogenesis [16] Inaddition one patient with CS and uniparental trisomy dueto triplication of the mutated paternal HRAS gene was alsoreported RMS typically displays loss of heterozygosity ofthe 11p155 region because of paternal uniparental disomyand approximately 28 of cases harbor mutations in genesof growth signaling pathways In reports of uniparentaldisomy plus HRAS mutation the latter was heterozygousand therefore must have occurred after the developmentof uniparental disomy [24] The functional analysis alsorevealed that CS-causing mutant HRAS proteins causedoncogene-induced senescence in human fibroblasts [37]Theimportant role of PI3K-protein-kinase B (AKT) signalingin Ras-mediated transformation and tumorigenesis is high-lighted by constitutive AKT activation in RMS cell lines andclinical samples Thus prolonged PI3K-AKT signaling mightalso be implicated in the development of soft tissue sarcomain patients with CS [38]
Only four out of 11 patients were diagnosed with CS priorto the RMS diagnosis in 5 patients CS was diagnosed afterthe RMS and in the remaining 2 the order was unknown[20] In 2003 a further three unpublished cases of RMS inchildren with CS were known through the International CSSupport Group [18] and for that reason there is possiblyunderdiagnosis of RMS in patients with CS
A screening protocol was proposed consisting of ultra-sound examination of the abdomen and pelvis every 3ndash6 months until age of 8ndash10 years for RMS and abdomi-nal neuroblastoma urine catecholamine metabolite analysisevery 6ndash12 months until age of 5 years for neuroblastomaand urinalysis for hematuria annually for bladder carcinomaafter age of 10 years The prior diagnosis of CS was theprerequisite for the implementation of a tumor screeningprotocol [8] The recommendation based on the presumedfast doubling time of RMS was abdominal sonographyscreening for RMS that should be done in similar intervalsof every four months until stronger evidence would suggestotherwise [39] Screening for neuroblastoma is no longerrecommended becausemany CS patients without identifiabletumor show elevated catecholamine metabolites in urine itappears that in this patient group an elevation above thenormal limit defined as 2 standard deviations (SD) above themean for age is more likely to be a variant rather than a sign
of a neuroblastoma [1 40] A French monitoring protocolproposed the determination of catecholamines and theirmetabolites in urine every six months until the age of 5 yearsand ultrasound abdominopelvic every six months until theend of the puberty seeking hematuria dipstick from6monthsto the age of 10 [41] The protocol in our hospital for patientswith CS includes an abdominal and pelvic ultrasound 3times during the first year of life and in childhood every 6months until age of 10 [42] We believe that the best optionis to perform a pelvic abdominal ultrasound every 3 monthsduring the first eight years of life and then controls accordingto medical criteria This is even more necessary in patientswith possible UL RMS because diagnosis was usually done inadvanced stages with a poor survival It is possible that withclose monitoring after an early diagnosis will detect initialstages of the tumor in previously not described locations
Head and neck MRI scans can be performed less fre-quently Ear examination and tympanometry every 4 to 6months to detect middle ear effusion which would raisesuspicion for a nasopharyngeal mass are also recommended[6]
The outcome of CS patients with RMS has been compa-rable to that for patients without the syndrome with a 5-yearsurvival rate of 65 to 70 [19] but according to this reviewit could be worse than the general population Neoplasia wasnoted at the cause of death in five (22) patients with CS[4 15] but in our study the mortality associated with RMSwas 43 Because the long-term survival in RMS is basedon the histology of the tumor and the extent of disease atdiagnosis early diagnosis may alter the treatment regimenand improve prognosis This could be particularly importantin patients with CS who often are medically fragile [20]
The RasMAPK pathway is an attractive target in thetreatment of cancer utilizing small molecule therapeuticsthat specifically inhibits the pathway Ras pathway agentssuch as farnesyltransferase inhibitors (tipifarnib and lona-farnib) that prevent posttranslational modification of Rasare being evaluated for cancer treatment and may be oftherapeutic use for syndromes in this pathway especially CSIn addition B-Raf protooncogene serinethreonine kinase(BRAF) and mitogenextracellular signal-regulated kinase(MEK) inhibitors offer the same potential in the possibletreatment of CS Since the RasMAPK pathway has targets forinhibition in cancer treatment there aremany smallmoleculetherapeutics that are in development or undergoing clinicaltrials with some already FDA approval [43]
6 ConclusionsCS is a syndrome poorly known in oncology but theirpredisposition tomalignancies includingULRMS implies theneed for a new perspective on early diagnosis and aggressivemedical and surgical treatment
ConsentInformed consent was obtained from the new two individualparticipants included in the study and has been properlydocumented with the parental approval to the use of patientrsquosimages and complementary studies
12 Case Reports in Genetics
Competing Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
Special thanks are due to Israel Fernandez Pineda MDAssistantMember and Surgery Fellowship ProgramDirectorSt Jude Childrenrsquos Research Hospital (Memphis TN) for therecommendations and corrections to the manuscript
References
[1] E Quezada and K W Gripp ldquoCostello syndrome and relateddisordersrdquo Current Opinion in Pediatrics vol 19 no 6 pp 636ndash644 2007
[2] JM Costello ldquoA new syndromerdquoNewZealandMedical Journalvol 74 article 397 1971
[3] JMCostello ldquoAnew syndromemental subnormality andnasalpapillomatardquo Australian Paediatric Journal vol 13 no 2 pp114ndash118 1977
[4] K W Gripp and A E Lin ldquoCostello syndrome a Rasmitogenactivated protein kinase pathway syndrome (rasopathy) result-ing from HRAS germline mutationsrdquo Genetics in Medicine vol14 no 3 pp 285ndash292 2012
[5] B Kerr M-A Delrue S Sigaudy et al ldquoGenotype-phenotypecorrelation in Costello syndrome HRAS mutation analysis in43 casesrdquo Journal of Medical Genetics vol 43 no 5 pp 401ndash4052006
[6] N Ahmadi and E Harley ldquoCostello syndrome and the impor-tance of cancer screeningrdquo Archives of OtolaryngologymdashHeadand Neck Surgery vol 136 no 10 pp 1028ndash1029 2010
[7] B Kerr O B Eden R Dandamudi et al ldquoCostello syndrometwo cases with embryonal rhabdomyosarcomardquo Journal ofMedical Genetics vol 35 no 12 pp 1036ndash1039 1998
[8] K W Gripp C I Scott Jr L Nicholson et al ldquoFive additionalCostello syndrome patients with rhabdomyosarcoma proposalfor a tumor screening protocolrdquo American Journal of MedicalGenetics vol 108 no 1 pp 80ndash87 2002
[9] K W Gripp A E Lin D L Stabley et al ldquoHRAS mutationanalysis in Costello syndrome genotype and phenotype corre-lationrdquo American Journal of Medical Genetics Part A vol 140no 1 pp 1ndash7 2006
[10] M Feingold ldquoCostello syndrome and rhabdomyosarcomardquoJournal of Medical Genetics vol 36 no 7 pp 582ndash583 1999
[11] S M White J M Graham Jr B Kerr et al ldquoThe adultphenotype in Costello syndromerdquo American Journal of MedicalGenetics A vol 136 no 2 pp 128ndash135 2005
[12] G Bisogno A Murgia I Mammi M S Strafella and M CarlildquoRhabdomyosarcoma in a patient with cardio-facio-cutaneoussyndromerdquo Journal of Pediatric HematologyOncology vol 21no 5 pp 424ndash427 1999
[13] S Sigaudy G Vittu A David et al ldquoCostello syndrome reportof six patients including one with an embryonal rhabdomyosar-comardquoEuropean Journal of Pediatrics vol 159 no 3 pp 139ndash1422000
[14] A Hinek M A Teitell L Schoyer et al ldquoMyocardial storage ofchondroitin sulfate-containing moieties in Costello syndromepatients with severe hypertrophic cardiomyopathyrdquo AmericanJournal of Medical Genetics vol 133 no 1 pp 1ndash12 2005
[15] A E Lin P D Grossfeld R M Hamilton et al ldquoFurtherdelineation of cardiac abnormalities in Costello syndromerdquoAmerican Journal of Medical Genetics vol 111 no 2 pp 115ndash1292002
[16] A L Estep W E Tidyman M A Teitell P D Cotter and KA Rauen ldquoHRASmutations in Costello syndrome detection ofconstitutional activating mutations in codon 12 and 13 and lossof wild-type allele in malignancyrdquo American Journal of MedicalGenetics vol 140 no 1 pp 8ndash16 2006
[17] H KawameMMatsui K Kurosawa et al ldquoFurther delineationof the behavioral and neurologic features inCostello syndromerdquoAmerican Journal of Medical Genetics vol 118A no 1 pp 8ndash142003
[18] B Kerr M A Einaudi P Clayton et al ldquoIs growth hormonetreatment beneficial or harmful in Costello syndromerdquo Journalof medical genetics vol 40 no 6 article e74 2003
[19] J P OrsquoNeal J Ramdas W E Wood and P K PellitterildquoParameningeal rhabdomyosarcoma in a patient with Costellosyndromerdquo Journal of Pediatric HematologyOncology vol 26no 6 pp 389ndash392 2004
[20] K W Gripp ldquoTumor predisposition in Costello syndromerdquoAmerican Journal of Medical Genetics Part C Seminars inMedical Genetics vol 137C no 1 pp 72ndash77 2005
[21] Y Aoki T Niihori H Kawame et al ldquoGermline mutationsin HRAS proto-oncogene cause Costello syndromerdquo NatureGenetics vol 37 no 10 pp 1038ndash1040 2005
[22] Y Abe Y Aoki S Kuriyama et al ldquoPrevalence and clinicalfeatures of Costello syndrome and cardio-facio-cutaneous syn-drome in Japan findings from a nationwide epidemiologicalsurveyrdquo American Journal of Medical Genetics Part A vol 158no 5 pp 1083ndash1094 2012
[23] I F M Lo C Brewer N Shannon et al ldquoSevere neonatal man-ifestations of Costello syndromerdquo Journal of Medical Geneticsvol 45 no 3 pp 167ndash171 2008
[24] J Menke S Pauli M Sigler et al ldquoUniparental trisomy of amutated HRASproto-oncogene in embryonal rhabdomyosar-coma of a patient with costello syndromerdquo Journal of ClinicalOncology vol 33 no 13 pp e62ndashe65 2015
[25] C P Kratz L Franke H Peters et al ldquoCancer spectrum andfrequency among children with Noonan Costello and cardio-facio-cutaneous syndromesrdquo British Journal of Cancer vol 112no 8 pp 1392ndash1397 2015
[26] H K Ransom ldquoSarcoma of the urachus review of the literaturewith report of an additional caserdquo The American Journal ofSurgery vol 22 no 2 pp 187ndash191 1933
[27] E M L-T Fernandez N H Siverio R L Almaraz L MViota J R Luis and L D Flores ldquoRadical surgery and IVA-chemotherapeutic regimen to treat embryonal rhabdomyosar-coma of the urachus case reportrdquo Pediatric Hematology andOncology vol 24 no 7 pp 543ndash550 2007
[28] M Ishikawa T Nishi R Yamada et al ldquoA case of urachalsarcoma in childhood case report and review of the worldliteraturerdquo Journal of the Japanese Society of Pediatric Surgeonsvol 21 pp 128ndash135 1985
[29] S Yokoyama YHayashida J Nagahama et al ldquoRhabdomyosar-coma of the urachus a case reportrdquo Acta Cytologica vol 41 no4 pp 1293ndash1298 1997
[30] U Schulz and C P OrsquoLeary ldquoSpinal AVM epidermal nevusand rhabdomyosarcoma a rare neurocutaneous syndromerdquoNeurology vol 56 no 3 pp 395ndash397 2001
Case Reports in Genetics 13
[31] A Cheikhelard S Irtan D Orbach et al ldquoUrachal rhab-domyosarcoma in childhood a rare entity with a poor out-comerdquo Journal of Pediatric Surgery vol 50 no 8 pp 1329ndash13332015
[32] K W Gripp E Hopkins K Sol-Church et al ldquoPhenotypicanalysis of individuals with Costello syndrome due to HRASpG13Crdquo American Journal of Medical Genetics Part A vol 155no 4 pp 706ndash716 2011
[33] M Tarnowski G Schneider G Amann et al ldquoRasGRF1 reg-ulates proliferation and metastatic behavior of human alveolarrhabdomyosarcomasrdquo International Journal of Oncology vol 41no 3 pp 995ndash1004 2012
[34] J-S Yu K W Kim H-J Lee Y-J Lee C-S Yoon and M-J Kim ldquoUrachal remnant diseases spectrum of CT and USfindingsrdquo Radiographics vol 21 no 2 pp 451ndash461 2001
[35] C P Kratz S Rapisuwon H Reed H Hasle and P S Rosen-berg ldquoCancer in Noonan Costello cardiofaciocutaneous andLEOPARD syndromesrdquo American Journal of Medical GeneticsPart C Seminars in Medical Genetics vol 157 no 2 pp 83ndash892011
[36] B Kerr M L Mucchielli S Sigaudy et al ldquoIs the locus forCostello syndrome on 11prdquo Journal of Medical Genetics vol 40no 6 pp 469ndash471 2003
[37] TNiihori YAokiNOkamoto et al ldquoHRASmutants identifiedin Costello syndrome patients can induce cellular senescencepossible implications for the pathogenesis of Costello syn-dromerdquo Journal of Human Genetics vol 56 no 10 pp 707ndash7152011
[38] G Rosenberger S Meien and K Kutsche ldquoOncogenic HRASmutations cause prolonged PI3K signaling in response toepidermal growth factor in fibroblasts of patients with costellosyndromerdquo Human Mutation vol 30 no 3 pp 352ndash362 2009
[39] M R DeBaun ldquoScreening for cancer in children with Costellosyndromerdquo American Journal of Medical Genetics vol 108 no1 pp 88ndash90 2002
[40] K W Gripp H Kawame D H Viskochil and L NicholsonldquoElevated catecholamine metabolites in patients with Costellosyndromerdquo American Journal of Medical Genetics vol 128 no1 pp 48ndash51 2004
[41] M-ADelrue B Arveiler andD Lacombe ldquoCostello syndromeclinical features and tumoral riskrdquo Archives de Pediatrie vol 9no 10 pp 1059ndash1063 2002
[42] V Martınez-Gonzalez and P Lapunzina Sındrome de CostelloGrupodeTrabajo sobreCancer en SındromeGeneticos Polimar-formativos (GT-CSGP) httpswwworphanetdatapathoProesCSGP-Costello-3pdf
[43] K A Rauen A Banerjee W R Bishop et al ldquoCostello andcardio-facio-cutaneous syndromes moving toward clinical tri-als in RASopathiesrdquo American Journal of Medical Genetics PartC Seminars inMedical Genetics vol 157 no 2 pp 136ndash146 2011
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Case Reports in Genetics 3
08 ngmL (normal lt 50) CA-153 197UImL (normal lt320) CA-199 437UImL (normal lt 370) and neuronspecific enolase (NSE) 2786 ngmL (normal 0ndash160)Thoraciccomputed tomography (CT) and scintigraphy showed noevidence of metastasis Bone marrow biopsy was normalTru-Cut biopsy guided by ultrasound reported an embryonalRMS with a proliferation index Ki-67 of 60 mesenchymalmalignant round cell and short spindle tumor vimentin(+) desmin (focal +) MyoD1 (focal +) CD99 (+ focalstaining) S100 protein (minus) pancytokeratins AE1AE3 (minus)synaptophysin (minus) and CD99 (minus) She was enrolled onthe standard risk group protocol European pediatric Softtissue Sarcoma Study Group (EpSSG) RMS 2005 subgroup Dwith 3 neoadjuvant chemotherapy cycles Preoperative MRIshowed a slight decrease in tumor size (32 times 3 times 25 cms)(Figures 1(d) and 1(e)) At the definitive surgery a 5 cmtumor dependent of the remaining left umbilical artery (leftmedial UL) located slightly to the left and displacing thebladder dome was found (Figure 1(f)) Complete resectionof the tumor was performed No pathological lymph nodeswere observed Final pathology report showed an embryonalRMS with signs of response to chemotherapy (maturationphenomenon at cytoplasmic and nuclear level of the tumorcellularity) with maximum cell proliferation index Ki-67 of5ndash10 almost all undifferentiated except in a small regionresection margins were negative for tumor (1ndash4mm fromthe edges of radial resection margin and 3 cm of UL)Chemotherapywas then continueduntil completing 25weeksand coadjuvant radiotherapy was administrated after thecompletion of chemotherapy At 23months of follow-up afterdiagnosis no residual tumor or relapse has been identified
22 Case 2 This is a 54-year-old female She is the first andonly child of a healthy nonconsanguineous couple with unre-markable family history Pregnancy was complicated withpolyhydramnios and delivery was preterm (34 weeks) with ahigh birth weight (2980 g +26 SD) She was admitted to theneonatal ward for investigation of a suspected dysmorphicsyndrome and initial FGFR3 molecular genetic testing forachondroplasia revealed no mutations Feeding difficultiesand failure to thrive were noted from the beginning requiringnutritional intervention and gastrostomy feeding from theage of 10 months She had a heart murmur with a normalechocardiogram She also had bronchomalacia and at MRInonspecific white matter hyperintensities in CNS She wasreferred to our clinical Genetics Clinic for evaluation at theage of 4 months and in view of her previous history andclinical findings CS was suspected HRAS Sanger sequencingdetected the common c34GgtA (pG12S) mutation confirm-ing the diagnosis of CS (Figure 2(a)) As part of the follow-up the recommended tumor screening protocol was arrangedand at the age of 3 years she underwent an abdominalultrasound that showed a tubular image running throughthe theoretical place of the umbilical arteries with a largercaliber on the right side of 56mm and associated echoesinside without Doppler flow (Figure 2(b)) Two subsequentultrasounds did not show any abnormality A new abdominalultrasound 9 months later reported the presence of a hypoe-choicmultilobulated solid tumor (53times 28 cm) in themidline
extending to the right in supravesical region with markedhypervascularization and extending cranially to the vicinityof the abdominal wall (Figures 2(c) and 2(d)) MRI showeda solid abdominal tumor (6 times 55 times 3 cm) composed ofnodular masses grouped in the UL region with involvementof the medial umbilical folds that were thickened throughoutthe iliac vessels region (Figure 2(e)) No regional metastaticdisease was observed Tumor markers were as follows 120572FPlt 13 ngmL CEA 53 ngmL and CA-199UImL No lungmetastases were observed in the thoracic CT scan and bonemarrow biopsywas normal She underwent a complete tumorresection (Figure 2(f)) The mass was located on the rightmedial UL (from its insertion into the right iliac artery tothe umbilicus) Pathology report showed a spindle cell RMSwith microscopic positive margins in 2 submitted samples(85 times 5 times 3 cm and 35 times 15 times 1 cm) and one resected lymphnode was negative for malignancy Tumor was composedof spindle cells that form cross linked bundles varyingdegrees with elongated oval nuclei vesicular configurationswith coarse chromatin The tumor had a pattern of nodulargrowth markedly myxoid stroma with microcystic focaldegeneration and 5 tumor necrosis no lymphovascularinvasion maximum proliferation index Ki67 of 30 musclespecific actin (+) desmin (+) WT1 (+ cytoplasmic) MyoD1(+ nuclear) and CD99 (minus) Two weeks after surgery thestandard risk group protocol EpSSG RMS 2005 subgroup B(Stage I) chemotherapy was started that includes ifosfamidevincristine and actinomycin D At 18 months of follow-up after diagnosis no residual tumor or relapse has beenidentified
3 Methods
We describe two new cases of RMS and CS based onmedicalrecords of patients diagnosed at the Institute of Medicaland Molecular Genetics and treated at the Departmentsof Pediatric Hematology-Oncology and Pediatric SurgeryUniversity Hospital La Paz (Madrid Spain) A review of theliterature published in English in MEDLINE from January1971 to June 2016 using the search terms CS and RMS wasdone also the references contained in these articles even ifthey were not indexed inMEDLINE were analyzed A reviewfrom January 1933 until June 2016 of all reported pediatriccases of UL RMS including as search criteria UL RMSurachus and umbilical arteries was performed
4 Results
In all cases analyzed and reviewed (same cases reportedin more than one publication were counted once) it waspossible to document the presence of 26 patients with CSand RMS (Table 1) [5ndash25] including the 2 cases describedherein The mean age of diagnosis was 2 years and 8 months(range 6 monthsndash7 years) It was slightly more commonin females than in males (12 1) The commonest locationwas the abdomenpelvis (1020) including 4 out of 10 ofthose in the UL The most common histological type wasembryonal RMS (1419) Seven out of nine patients who died(and with reported histology) showed embryonal RMS The
4 Case Reports in Genetics
(a) (b) (c)
(d) (e) (f)
Figure 2 Patient 2 (a) Photograph of the physical features of the patient with prominent forehead low-set ears lower palpebral fissureshypertelorism broad nasal bridge thick lips and anteverted slightly nostrils (b) Initial abdominal ultrasound showing the presence ofa tubular image caliber of 56mm extending in the theoretical location of the right umbilical artery ((c) and (d)) Follow-up abdominalultrasound in themidline showing amultilobulated hypoechoic solid tumorwithmarked hypervascularization extending from the proximityof the abdominal wall to the right supravesical region (e) MRI onT2-weighted sequence confirms the presence of several nodular massesgrouped with thickening of both medial umbilical folds the right to 4mm proximal to the umbilicus and 8mm adjacent to the iliac vesselsparavesical region portion (f) Operative image indicating the presence of tumor originating in the right medial UL
most frequent encountered HRAS mutation associated withRMS was pG12S (712) Only 4 deaths were documented inpatients with change in codon 12 (2 patients G12S 1 patientG12A and 1 patient G12C) Chemotherapy that was appliedvaries based on the protocols of the countries where theywerediagnosed (Table 2) [5ndash10 12ndash14 16ndash25] Overall survival wasabout 43 (921) Mortality was observed in 12 out of 21individuals in nine of them associated with neoplasia andin three associated with surgery
Similarly the total number of reported cases of ULRMS in pediatric patients either in the obliterated umbilicalarteries (medial UL) or in urachus (median UL) is 17including these 2 new cases (Table 3) [5 7ndash9 24ndash31] Themean age of diagnosis was 3 years and 4 months (range 4monthsndash6 years) It is slightly more common in females thanin males (14 1) Themost common location was the urachus(1517) The most common histological type was embryonalRMS (1215) and one-fourth (312) of patients who died withreported histology showed embryonal RMS Chemotherapyvaries based on the protocols of the countries where theywerediagnosed (Table 4) [7 24 26ndash31] Overall survival was 69
(1116) overall mortality was 31 (516) two-year absolutesurvival rate was 69 (1116) and five-year absolute survivalrate was 19 (316)
5 Discussion
The prevalence of CS is estimated to be 1 1290000 individ-uals in Japan and at least 1 500000 in the United Kingdomthe incidence was estimated to be 1 60000ndash100000 [4 22]The overall tumor incidence is approximately 10ndash15 overthe lifetime of individuals with an identified HRASmutation[1 4 9] RMS accounting in about 60 of all neoplasia [1]Based on the 300 cases of CS currently known [4] we foundan incidence of 87 RMS in patients with CS
CS is the first disorder associated with germlinemutations in the Ras family of guanosine-51015840-triphosphate(GTP)ases [21] HRAS has six exons five exons are encodedfor a protein of 189 amino acids with a molecular weight of21 kDa [4] Missense mutations at codons 12 and 13 are inconstitutively active GTP-bound conformation and activatedownstream effectors such as MAPK phosphatidylinositol3-kinases (PI3K) and ral guanine nucleotide dissociation
Case Reports in Genetics 5
Table1Ch
aracteris
ticso
fpatientsw
ithCostello
synd
romea
ndrhabdo
myosarcom
a
PT number
Author
Year
Cou
ntry
Sex
Age
atdiagno
sis(yearsm
onths)
Symptom
sLo
catio
nHistolog
yMutation
AAC
(NS)
Therapy
Outcome
1Ke
rretal
[78]
1998
England
F2y
4mVo
miting
Con
stipatio
nRe
troperiton
ealleft
psoasm
ayor
muscle
Embryonal
G12S
(34GgtA)lowast
[9]
SCh
TRe
lapsetumor-fr
eeageo
f7years
2Ke
rretal
[78]
1998
England
F3y
2mAb
dominal
mass
Pelvis
urachu
s(m
edianUL)
adherent
tothe
bladder
Embryonal
G12A
(35GgtC)
[5]
SCh
T
Histologyshow
edextend
ingup
tothe
resectionmargin
Diedaged
5years
[59]
3Feingold
[810]
1999
USA
M6m
Tumor
Rightfoo
tAlveolar
NDF
SCh
TTu
mor-fr
eeageo
f20
years[11]
4Bisogn
oetal
[8912]
1999
Italy
M1y
8mCon
stipatio
nAb
dominal
pain
Lower
abdo
men
pelvis
abdo
minal
walllowast
Embryonal
NDF
SCh
TOnlybiop
syDiedaged
2yearsa
nd3mon
ths
5Sigaud
yetal
[813]
2000
France
M6y
NDF
Inguinalscrotal
Embryonal
NDF
NDF
NDF
6Grip
petal
[81415]
2002
USA
M5y
6mAb
dominal
pain
Pelvis
pulm
onary
metastasesw
aspresent
Embryonal
NDF
SCh
TDiedaft
errecurrence
[14]
7Grip
petal
[8]
2002
USA
F3y
7mAb
dominal
pain
Emesis
Upp
erabdo
men
masse
ncasingthe
superio
rmesenteric
anceliaca
rteries
Sing
lepu
lmon
ary
nodu
le
Pleomorph
icNDF
ChT
Diedaged
4years
8Grip
petal
[8]
2002
USA
F2y
6mAb
dominal
mass
Pelvis
bladder
Embryonal
NDF
ChT
RTS
Diedaged
7yearsfor
recurrency
ofRM
Sfib
rosarcom
a[16]
9Grip
petal
[8]
2002
USA
NDF
7mPerin
eal
grow
thPerin
eal
Embryonal
NDF
ChT
RTS
Tumor-fr
eeageo
f2years
10Grip
petal
[8]
2002
USA
NDF
1y11m
Prop
tosis
Leftorbit
Unk
nown
NDF
SRT
Tumor-fr
eeageo
f4years
11Ka
wam
eetal
[17]
2003
Japan
F1y
4mAb
dominal
mass
Pelvis
Spindlec
ell
NDF
SCh
TTu
mor-fr
eeageo
f7years
6 Case Reports in GeneticsTa
ble1Con
tinued
PT number
Author
Year
Cou
ntry
Sex
Age
atdiagno
sis(yearsm
onths)
Symptom
sLo
catio
nHistolog
yMutation
AAC
(NS)
Therapy
Outcome
12Ke
rretal
[18]
2003
UK
M2y
2mLargep
elvic
mass
Retro
vesic
ular
mass
byultrasou
ndEm
bryonal
NDF
ChT
Diedaged
2yearsa
nd4mon
ths
13OrsquoNealetal
[19]
2004
USA
F3y
Right-s
ided
cervicofacial
mass
Parameningeal
infratem
poralfossa
right
perip
arotid
mastic
ator
space
region
Alveolar
NDF
ChTS
RT
Clinicalgrou
p3T2
bN0stage3
Dieddu
ringsurgery
14Grip
p[20]
2005
USA
F3y
2mFacialmass
Rightinfratempo
ral
fossa
Mixed
alveolar
and
embryonal
NDF
ChTS
Dieddu
ringsurgery
byventric
ular
tachycardiafollowed
rapidlyby
lossof
heartrhythm
15Ao
kietal
[2122]
2005
Japan
F7y
2mNDF
NDF
NDF
G12S
(34GgtA)
NDF
NDF
16Grip
petal
[9]
2006
USA
M2y
NDF
NDF
NDF
G12S
(34GgtA)
NDF
Tumor-fr
eeageo
f11
yearslowast
17Ke
rretal[5]
2006
UK
NDF
7mNDF
Metastatic
arising
from
thep
rosta
teEm
bryonal
[23]
G12C
(34GgtT)
NDF
Diedaged
7mon
ths
18Ke
rretal[5]
2006
UK
NDF
NDF
NDF
NDF
NDF
G12S
(34GgtA)
NDF
Diedaged
7years
19Ke
rretal[5]
2006
UK
NDF
NDF
NDF
NDF
NDF
G12A
(35GgtC)
NDF
NDF
20Lo
etal[23]
2008
UK
M2y
3mRe
spira
tory
functio
ndeterio
rated
Rightlun
gNDF
G12S
(34GgtA)
SDiedfewweeks
later
surgery
21Ahm
adiand
Harley[6]
2010
USA
M2y
Increasedwork
ofbreathing
Nasop
haryngeal
Embryonal
NDF
SCh
TRT
Clinicalgrou
pIIA
(T1N
0M0)
Tumor-fr
eeageo
f3years
22Ab
eetal[22]
2012
Japan
NDF
NDF
NDF
NDF
NDF
NDF
NDF
Died
23Menke
etal
[2425]
2015
Germany
F3y
Abdo
minal
mass
Lower
anterio
rabdo
menabo
vethe
urinarybladderlowast
(urachus-m
edianUL
bylocatio
n)
Embryonal
G12C
(34GgtT)
SCh
T
R1resection
(marginaltum
orresid
ue)Tu
mor-fr
eeageo
f6years
24Kr
atze
tal
[25]
2015
Germany
M1y
NDF
NDF
Embryonal
G12S
(34GgtA)
NDF
NDF
25
Sanchez-
Mon
tenegro
etal(this
repo
rt)
2017
Spain
F2y
4mAs
ymptom
atic
LeftmedialU
LEm
bryonal
G12A
(35GgtC)
ChTS
RTTu
mor-fr
eeageo
f4yearsa
nd4mon
ths
26
Sanchez-
Mon
tenegro
etal(this
repo
rt)
2017
Spain
F3y
10m
Asym
ptom
atic
Rightm
edialU
LSpindlec
ell
G12S
(34GgtA)
SCh
TTu
mor-fr
eeageo
f5yearsa
nd4mon
ths
AAC
aminoacid
changeC
hTchemotherapyFfem
aleMm
aleNDFno
datafoun
dNSnu
cleotides
ubstitutio
nPT
patientR
TradiotherapySsurgeryU
Lum
bilicalligam
entlowastPerson
alcommun
icationby
author
Case Reports in Genetics 7
Table 2 Chemotherapy of patients with Costello syndrome and rhabdomyosarcoma
PTnumber Chemotherapy protocol
1Initially with VCR ACD and CTX After debulking continued on ChT using IFOS VCR and ACD After the second coursewhen she developed IFOS induced encephalopathy she was changed back to pulses of VCR ACD and CTX given every 3weeks for 9 courses [7]
2Initially IFOS ACD and VCR After 4 courses CTX was substituted for IFOS because hemorrhagic cystitis Tx complicatedby recurrent episodes of moderately severe diarrhoea and febrile neutropenia requiring readmission to hospital Tx wascompleted after six courses of ChT [7]
3 Tx consisted of below the knee amputation and ChT (DOX ACD VCR and CTX) [10]
4
Tx was implemented according to the Italian protocol for pediatric soft tissue sarcoma Three courses of ChT including VCR(0025mgkg day 1) IFOS (50mgkg days 1 and 2) and alternating ACD (0025mgkg day 1) and DOX (07mgkg day 1) wereadministered Symptoms regressed and the CT scan showed a reduction in tumor volume of more than two-thirds After 3more courses of ChT the patient experienced abdominal pain A repeat abdominal CT scan showed an increase in the pelvicmass Despite the administration of a different ChT with CBDCA (11mgkg day 1) and VP-16 (3mgkg for 3 doses) the tumorcontinued to grow and the child died 7 months after the diagnosis of RMS [12]
5 NDF [13]
6
The first cycle of ChT with VCR ACD and CTX and topotecan reduced the tumor size [16] The tumor was surgicallyremoved after the first ChT [8] Debulking S was required because of rapid growth and tumor necrosis The protocol wascontinued and was deemed sufficiently successful to withhold RT One month after completion of the first protocol tumorrecurrence necessitated a second round of ChT with irinotecan and DOXThe latter drug was administered about 1 weekbefore he died during which time he had tachycardia (heart rate 180ndash20 bpm) [14]
7 The tumor did not respond to ChT and she died shortly after her 4th birthday [8]8 Tx was a combination of S ChT and RT continued until age of 35 years [8]9-10 NDF [8]11 PT had later generalized tonic-clonic seizures during her Tx for RMS [17]12 Despite extensive ChT the tumor progressed rapidly and the PT died 2 months later [18]
13 Induction ChT was commenced with the initial 12-week course of VCR ACD and CTX based on the Intermediate RiskProtocol D9803 of the COG [19]
14 ChT did not result in tumor shrinkage therefore surgical resection was performed [20]15ndash22 NDF [5 6 9 21ndash23]23 ChT according to the cooperative soft tissue sarcoma protocol (CWS-2002 P) was well tolerated by the PT [24]24 NDF [25]
25 ChT in the standard risk group protocol EpSSG RMS 2005 subgroup D 3 preoperative cycles of IFOS (2 doses at 100mgkg)VCR (005mgkg) and ACD (005mgkg)
26 ChT (postoperative 15 days) in the standard risk group protocol EpSSG RMS 2005 subgroup B (Stage I) cycles of IFOS (2doses of 3 gm2d) VCR (15mgm2) and ACD (15mgm2) was initiated
ACD actinomycin D CBDCA carboplatin ChT chemotherapy COG childrenrsquos oncology group CTX cyclophosphamide CT computed tomography CWSCooperative Weichteilsarkom Studie (Cooperative Soft Tissue Sarcoma Study) DOX Doxorubicin EpSSG European pediatric Soft tissue sarcoma StudyGroup IFOS ifosfamide NDF no data found PT patient RMS rhabdomyosarcoma RT radiotherapy S surgery Tx treatment VCR vincristine VP-16etoposide
stimulator (RalGDS) [16 21] in signaling pathways control-ling cell proliferation and differentiation [9]
Themajority of patients with CS had 34GgtA transition incodon 12 (80) [4 16] More than 95 of the mutations arepredicted to result in substitution of the glycine in position12 or 13 of the protein product [1] All individuals withmalignancy had a codon 12 mutation (especially G12A 47patients) [5 21] The rare G12V mutation is associated witha more severe early lethal phenotype some patients diefrom respiratory distress hypertrophic cardiomyopathy ormalignant tachycardia prior to being diagnosed with CS [1]As far as we know no individual with G13C has developed amalignant tumor [4 32]
RMS is the most common soft tissue sarcoma of infancyIts incidence is between 4 and 7 cases per 1 million childrenyounger than 15 years [8 12] The age peak is between 2 and5 years with a slight male predominance (12ndash141) Thesetumors may arise anywhere in the body and fewer than 20are located in the pelvis [12]Most RMS tumors are originatedin the head and neck region urogenital tract and extremities[33] The most common histologic type seen in gt50 isembryonal followed by alveolar in 20ndash30 PleomorphicRMS is rare (1) and has a poor prognosis [8] AlveolarRMS is characterized by the translocation t(213)(q35q14) in70 of cases and the variant translocation t(113)(p36q14)in a smaller percentage of cases Evidence accumulates
8 Case Reports in Genetics
Table3Ch
aracteris
ticso
fPediatricPatie
ntsw
ithUmbilicalLigamentR
habd
omyosarcom
a
PT number
Author
Year
Cou
ntry
Sex
Age
atdiagno
sis(yearsm
onths)
Symptom
sLo
catio
nSize
(cm)
Histology
IRS
grou
pTh
erapy
Outcome
1Ra
nsom
[2627]
1933
USA
F4m
Massb
elowthe
umbilicus
and
extend
ing
somew
hattothe
right
Urachus
(medianUL)
attached
alon
gthea
nterior
wallfrom
theu
mbilicus
tothea
pexof
theb
ladd
er
115
Spindle
cell
ISM
AC
RT
Lastcheck-up
exam
ination(2
years)
show
edno
evidence
ofrecurrence
2Ishikawae
tal[28]
1985
Japan
F1y
4mAb
dominalmass
abdo
minalpain
hemop
erito
neum
Urachal(m
edianUL)
intra-abdo
minalruptureo
fthetum
or
Fist-
sized
NDF
IVSM
ACNDF
3Yo
koyamae
tal[2729]
1997
Japan
M2y
Episo
diclow
erabdo
minalpain
Urachus
(medianUL)
extraperito
neallocated
betweentheu
mbilicus
and
apex
oftheb
ladd
erandwas
adherin
gtig
htlyto
both
Theb
ilateralm
edialU
Lweres
eenenterin
gthe
tumorR
upturedwith
asm
alln
umbero
fdissem
inated
tumors
scatteredon
them
esentery
andDou
glas
pouch
12Em
bryonal
IVSM
AI
ChT
At2yearso
ffollo
w-upno
recurrence
hadbeen
detected
4lowastKe
rretal
[78]
1998
England
F3y
2mAb
dominalmass
Urachus
(medianUL)
adherent
totheb
ladd
erNDF
Embryonal
IIaSM
II
ChT
Histologyshow
edextend
ingup
tothe
resectionmargin
Diedaged
5years
[59]
5Schu
lzand
OrsquoLeary
[2730]
2001
Scotland
M2y
NDF
Urachus
(medianUL)
NDF
Embryonal
NDF
SCh
TRT
Tumor-fr
eeageo
f26
years
6Fernandeze
tal[27]
2007
Spain
F6y
Intractable
constip
ation
nauseaabd
ominal
painles
smass
Urachus
(medianUL)
infiltratingthev
entral
abdo
minalwalland
fixed
tothev
esicaldo
me
135
Embryonal
IbSM
IC
ChT
At4yearso
ffollo
w-upthep
atient
remains
welland
free
ofclinicald
isease
7lowastMenke
etal
[2425]
2015
Germany
F3y
Abdo
minalmass
Lower
anterio
rabd
omen
abovethe
urinarybladderamp
(urachusm
edianULby
locatio
n)
NDF
Embryonal
IIaSM
II
ChT
R1resection
(marginaltum
orresid
ue)Tu
mor-fr
eeageo
f6years
8Ch
eikh
elard
etal[31]
2015
Dx
1983
France
F5y
5mNDF
Urachus
(medianUL)
periton
ealm
etastasesa
ndhypo
gastric
lymph
nodes
5NDF
IVSM
AI
ChT
Died31
mon
thsa
fter
diagno
siswith
relap
sein
periton
ealliver
at11mon
ths
Case Reports in Genetics 9
Table3Con
tinued
PT number
Author
Year
Cou
ntry
Sex
Age
atdiagno
sis(yearsm
onths)
Symptom
sLo
catio
nSize
(cm)
Histology
IRS
grou
pTh
erapy
Outcome
9Ch
eikh
elard
etal[31]
2015
Dx
2003
France
F3y
3mPeriton
ealrup
ture
poor
generalstatus
Urachus
(medianUL)
lumbo
aorticandexternal
iliac
lymph
nodes
10Alveolar
IVSM
AI
ChTRT
Died57
mon
thsa
fter
diagno
siswith
relap
sein
periton
ealliver
at30
mon
ths
10Ch
eikh
elard
etal[31]
2015
Dx
2005
France
F2y
6mMasspo
orgeneral
statusdysuria
Urachus
(medianUL)
15Em
bryonal
III
SMII
ChTRT
Died37
mon
thsa
fter
diagno
siswith
periton
ealrelapse
at19
mon
ths
11Ch
eikh
elard
etal[31]
2015
Dx
2005
France
M4y
2mMasspo
orgeneral
statusdysuria
Urachus
(medianUL)
periton
ealm
etastasesa
ndiliac
lumbo
aorticlymph
nodes
10Em
bryonal
IVSM
II
ChTRT
Relapsed
multifocalat
82mon
thsfollo
w-up
100mon
ths
12Ch
eikh
elard
etal[31]
2015
Dx
2005
France
M5y
3mMasspo
orgeneral
status
Urachus
(medianUL)
periton
ealm
etastasesa
ndmesenteric
lymph
nodes
106
Embryonal
IVSM
IC
ChTRT
Tumor
freea
fter9
5mon
thssince
diagno
sis
13Ch
eikh
elard
etal[31]
2015
Dx
2006
France
M2y
5mMasspo
orgeneral
statusob
structiv
erenalinsuffi
ciency
Urachus
(medianUL)
periton
ealbon
emetastases
andhypo
gastric
lymph
nodes
21Em
bryonal
IVSM
II
ChTRT
Bone
progression
after
16mon
thsdied
18aft
erdiagno
sis
14Ch
eikh
elard
etal[31]
2015
Dx
2010
France
M4y
5mAb
dominalpain
Urachus
(medianUL)
7Em
bryonal
III
SMIC
ChT
Tumor
freea
fter18
mon
thssince
diagno
sis
15Ch
eikh
elard
etal[31]
2015
Dx
2010
France
M6y
Abdo
minalpain
Urachus
(medianUL)
periton
ealm
etastases
14Em
bryonal
IVSM
AI
ChTRT
Tumor
freea
fter4
5mon
thssince
diagno
sis
16lowast
Sanchez-
Mon
tenegro
etal(this
repo
rt)
2017
Dx
2015
Spain
F2y
4mAs
ymptom
atic
LeftmedialU
L5
Embryonal
IaCh
TSM
IC
RT
Tumor-fr
eeageo
f3yearsa
nd9mon
ths
17lowast
Sanchez-
Mon
tenegro
etal(this
repo
rt)
2017
Dx
2015
Spain
F3y
10m
Asym
ptom
atic
Rightm
edialU
L85
Spindle
cell
IIaSM
II
ChT
Tumor-fr
eeageo
f4yearsa
nd5mon
ths
ChT
chem
otherapyD
xdiagno
sed
Ffemale
IRS
intergroup
rhabdo
myosarcom
aMm
ale
NDF
nodata
foun
dRT
radiotherapy
Ssurgery
SMAIsurgerymacroscop
ically
incomplete
SMAC
surgery
macroscop
icallycompleteSM
ICsurgery
microscop
icallycompleteSM
IIsurgery
microscop
icallyincompleteULum
bilicalligam
ent
ampPerson
alcommun
icationby
authorlowast
Patientsw
ithCostello
synd
rome
10 Case Reports in Genetics
Table 4 Chemotherapy of pediatric patients with umbilical ligament rhabdomyosarcoma
PTnumber Chemotherapy protocol
1-2 No ChT [26 28]3 After establishment of the final diagnosis he was treated with combined ChT including VCR ACD and CTX [29]
4lowastInitially IFOS ACD and VCR After 4 courses CTX was substituted for IFOS because of hemorrhagic cystitis Tx complicatedby recurrent episodes of moderately severe diarrhoea and febrile neutropenia requiring readmission to hospital Tx wascompleted after six courses of ChT [7]
5 NDF [30]
6 PT started induction of ChT 2 weeks after S Induction regimen included 9 cycles of IVA (IFOS VCR and ACD) that were welltolerated with minimal systemic complications (Tx 953 of the MMT 95 SIOP protocol for RMS) [27]
7lowast ChT according to the cooperative soft tissue sarcoma protocol (CWS-2002 P) was well tolerated by the PT [24]8 Adjuvant ChT with 10 cycles of IFOS VCR and ACD [31]9 Adjuvant ChT with 6 cycles of IFOS VCR and VP-16 and 9 cycles of VCR ACD CTXACD and CTX [31]10 Neoadjuvant ChT with 6 cycles of IFOS VCR and ACD and adjuvant ChT with 3 cycles of IFOS VCR and ACD [31]
11 Neoadjuvant ChT with 1 cycle of CTX VCR and PRED 2 cycles IFOS VCR and ACD and 4 cycles of IFOS VCR ACD andDOX and adjuvant ChT with 3 cycles of IFOS VCR and ACD [31]
12 Neoadjuvant ChT with 1 cycle of CTX VCR and PRED and 5 cycles of IFOS VCR ACD and DOX and adjuvant ChT with 2cycles of IFOS VCR ACD and DOX and 1 cycle of IFOS VCR and ACD [31]
13 Neoadjuvant ChT with 2 cycles of VCR ACD and CTX + and 3 cycles of IFOS VCR ACD and DOX and adjuvant ChT with 3cycles of IFOS VCR and ACD [31]
14 Neoadjuvant ChT with 4 cycles of IFOS VCR ACD and DOX and adjuvant ChT with 5 cycles of IFOS VCR ACD [31]
15 Neoadjuvant ChT with 4 cycles of IFOS VCR ACD DOX 3 cycles of IFOS VCR ACD and adjuvant ChT with 1 cycle of IFOSVCR ACD 1 cycle of IFOS VCR [31]
16lowastChT in the standard risk group protocol EpSSG RMS 2005 subgroup D 3 preoperative cycles of IFOS (2 doses at 100mgkg)VCR (005mgkg) and ACD (005mgkg)
17lowastChT (postoperative 15 days) in the standard risk group protocol EpSSG RMS 2005 subgroup B (Stage I) cycles of IFOS (2 dosesof 3 gm2d) VCR (15mgm2) and ACD (15mgm2) was initiated
ACD actinomycin D ChT chemotherapy CTX cyclophosphamide CWS Cooperative Weichteilsarkom Studie (Cooperative Soft Tissue Sarcoma Study)DOX Doxorubicin EpSSG European pediatric Soft tissue sarcoma Study Group IFOS ifosfamide MMT malignant mesenchymal tumor NDF no datafound PRED prednisone PT patient RMS rhabdomyosarcoma S surgery SIOP Societe Internationale DrsquoOncologie Pediatrique (International Society ofPediatric Oncology) Tx treatment VCR vincristine VP-16 etoposide lowastPatients with Costello syndrome
that alveolar RMS and embryonal RMS are two differentdisorders while alveolar RMS may originate from primitiveuncommitted mesodermal cells embryonal RMS originatesprobably from more differentiated myoblasts Ras protein-specific guanine nucleotide-releasing factor 1 (RasGRF1)plays an important role in alveolar RMS pathogenesis Theseinteresting concepts however need more evidence [33]
The umbilicus caudally originates the common ligamentwhich is divided into obliterated umbilical arteries (medialUL) and urachus (median UL) The urachus varies from3 to 10 cm in length and from 8 to 10mm in diameterIt is a three-layered tubular structure the innermost layerbeing lined with transitional epithelium in 70 of casesand with columnar epithelium in 30 The structure issurrounded by connective tissue and outermost muscularlayer in continuity with the detrusor muscle Along its pathfrom the bladder to the umbilicus the urachus lies betweenthe transverse fascia and the parietal peritoneum containedin the pyramidal retropubic perivesical preperitoneal spacecompartmentalized by umbilicovesical fascia along with themedial umbilical ligaments and the bladder Occasionallythe urachus may merge with one or both of the obliteratedumbilical arteries (medial UL) and there may be a slight
deviation to the right or left of the midline [34] The urachusis an embryological remnant resulting from the obliterationof the allantoic channel which attaches the bladder dome tothe umbilicus [31]
Urachal malignant tumors are extremely rare represent-ing less than 05 of all bladder cancers and 001 of alltumors They may arise from any portion of the urachus andare most commonly found in adults and males (60ndash70)Although sarcomas represent only 8 they are the mostfrequent urachal neoplasms reported in patients youngerthan 20 years of age (67) [27] Poor prognosis is a commonfeature in adults and pediatric urachalmalignancies with 50to 60 of 5-year survival In contrast the 5-year event-freesurvival in pelvic RMS was reported to be about 51 [31]
This indolent and rather large urachal tumor was mostlyrevealed by an uncomplicated progressing mass withoutprodromic urological symptomsThedelay of diagnosis couldbe explained by a long asymptomatic progression of thetumor in a preperitoneal location which allows an importantlocal spreading before diagnosis Even in patients withouttumor rupture peritoneal involvement appeared to be the keypoint in the prognosis of urachal RMS Systematic cytologyat diagnosis could be more accurate to evaluate peritoneal
Case Reports in Genetics 11
extension in order to avoid understaging and adjust adjuvantlocoregional treatment [31]
Previously only 12 patients with RMS arising from theurachus (median UL) in children without CS have beenreported in the English literature (Table 3) By 2011 therewere29 reported cases of cancer in patients withCS 19 RMS (meanage of 23 years 9 embryonal 1 alveolar 1 mixed histology1 pleomorphic 1 spindle cell type and 6 unclassified) 5neuroblastomas 4 bladder cancer and 1 fibrosarcoma [35]
Loss of heterozygosity for 11p155 in RMS from individu-als with CS suggests that loss of the wild-type allele is the sec-ond hit in tumor development [6 16 36] Whereas theHRASmutation in a sporadic malignancy in the general populationis present only within the tumor cells in CS an identicalmutation is present in every single cell of the individualthus accounting for the tumor predisposition [1] implicatingan alternate mechanism of rhabdomyosarcogenesis [16] Inaddition one patient with CS and uniparental trisomy dueto triplication of the mutated paternal HRAS gene was alsoreported RMS typically displays loss of heterozygosity ofthe 11p155 region because of paternal uniparental disomyand approximately 28 of cases harbor mutations in genesof growth signaling pathways In reports of uniparentaldisomy plus HRAS mutation the latter was heterozygousand therefore must have occurred after the developmentof uniparental disomy [24] The functional analysis alsorevealed that CS-causing mutant HRAS proteins causedoncogene-induced senescence in human fibroblasts [37]Theimportant role of PI3K-protein-kinase B (AKT) signalingin Ras-mediated transformation and tumorigenesis is high-lighted by constitutive AKT activation in RMS cell lines andclinical samples Thus prolonged PI3K-AKT signaling mightalso be implicated in the development of soft tissue sarcomain patients with CS [38]
Only four out of 11 patients were diagnosed with CS priorto the RMS diagnosis in 5 patients CS was diagnosed afterthe RMS and in the remaining 2 the order was unknown[20] In 2003 a further three unpublished cases of RMS inchildren with CS were known through the International CSSupport Group [18] and for that reason there is possiblyunderdiagnosis of RMS in patients with CS
A screening protocol was proposed consisting of ultra-sound examination of the abdomen and pelvis every 3ndash6 months until age of 8ndash10 years for RMS and abdomi-nal neuroblastoma urine catecholamine metabolite analysisevery 6ndash12 months until age of 5 years for neuroblastomaand urinalysis for hematuria annually for bladder carcinomaafter age of 10 years The prior diagnosis of CS was theprerequisite for the implementation of a tumor screeningprotocol [8] The recommendation based on the presumedfast doubling time of RMS was abdominal sonographyscreening for RMS that should be done in similar intervalsof every four months until stronger evidence would suggestotherwise [39] Screening for neuroblastoma is no longerrecommended becausemany CS patients without identifiabletumor show elevated catecholamine metabolites in urine itappears that in this patient group an elevation above thenormal limit defined as 2 standard deviations (SD) above themean for age is more likely to be a variant rather than a sign
of a neuroblastoma [1 40] A French monitoring protocolproposed the determination of catecholamines and theirmetabolites in urine every six months until the age of 5 yearsand ultrasound abdominopelvic every six months until theend of the puberty seeking hematuria dipstick from6monthsto the age of 10 [41] The protocol in our hospital for patientswith CS includes an abdominal and pelvic ultrasound 3times during the first year of life and in childhood every 6months until age of 10 [42] We believe that the best optionis to perform a pelvic abdominal ultrasound every 3 monthsduring the first eight years of life and then controls accordingto medical criteria This is even more necessary in patientswith possible UL RMS because diagnosis was usually done inadvanced stages with a poor survival It is possible that withclose monitoring after an early diagnosis will detect initialstages of the tumor in previously not described locations
Head and neck MRI scans can be performed less fre-quently Ear examination and tympanometry every 4 to 6months to detect middle ear effusion which would raisesuspicion for a nasopharyngeal mass are also recommended[6]
The outcome of CS patients with RMS has been compa-rable to that for patients without the syndrome with a 5-yearsurvival rate of 65 to 70 [19] but according to this reviewit could be worse than the general population Neoplasia wasnoted at the cause of death in five (22) patients with CS[4 15] but in our study the mortality associated with RMSwas 43 Because the long-term survival in RMS is basedon the histology of the tumor and the extent of disease atdiagnosis early diagnosis may alter the treatment regimenand improve prognosis This could be particularly importantin patients with CS who often are medically fragile [20]
The RasMAPK pathway is an attractive target in thetreatment of cancer utilizing small molecule therapeuticsthat specifically inhibits the pathway Ras pathway agentssuch as farnesyltransferase inhibitors (tipifarnib and lona-farnib) that prevent posttranslational modification of Rasare being evaluated for cancer treatment and may be oftherapeutic use for syndromes in this pathway especially CSIn addition B-Raf protooncogene serinethreonine kinase(BRAF) and mitogenextracellular signal-regulated kinase(MEK) inhibitors offer the same potential in the possibletreatment of CS Since the RasMAPK pathway has targets forinhibition in cancer treatment there aremany smallmoleculetherapeutics that are in development or undergoing clinicaltrials with some already FDA approval [43]
6 ConclusionsCS is a syndrome poorly known in oncology but theirpredisposition tomalignancies includingULRMS implies theneed for a new perspective on early diagnosis and aggressivemedical and surgical treatment
ConsentInformed consent was obtained from the new two individualparticipants included in the study and has been properlydocumented with the parental approval to the use of patientrsquosimages and complementary studies
12 Case Reports in Genetics
Competing Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
Special thanks are due to Israel Fernandez Pineda MDAssistantMember and Surgery Fellowship ProgramDirectorSt Jude Childrenrsquos Research Hospital (Memphis TN) for therecommendations and corrections to the manuscript
References
[1] E Quezada and K W Gripp ldquoCostello syndrome and relateddisordersrdquo Current Opinion in Pediatrics vol 19 no 6 pp 636ndash644 2007
[2] JM Costello ldquoA new syndromerdquoNewZealandMedical Journalvol 74 article 397 1971
[3] JMCostello ldquoAnew syndromemental subnormality andnasalpapillomatardquo Australian Paediatric Journal vol 13 no 2 pp114ndash118 1977
[4] K W Gripp and A E Lin ldquoCostello syndrome a Rasmitogenactivated protein kinase pathway syndrome (rasopathy) result-ing from HRAS germline mutationsrdquo Genetics in Medicine vol14 no 3 pp 285ndash292 2012
[5] B Kerr M-A Delrue S Sigaudy et al ldquoGenotype-phenotypecorrelation in Costello syndrome HRAS mutation analysis in43 casesrdquo Journal of Medical Genetics vol 43 no 5 pp 401ndash4052006
[6] N Ahmadi and E Harley ldquoCostello syndrome and the impor-tance of cancer screeningrdquo Archives of OtolaryngologymdashHeadand Neck Surgery vol 136 no 10 pp 1028ndash1029 2010
[7] B Kerr O B Eden R Dandamudi et al ldquoCostello syndrometwo cases with embryonal rhabdomyosarcomardquo Journal ofMedical Genetics vol 35 no 12 pp 1036ndash1039 1998
[8] K W Gripp C I Scott Jr L Nicholson et al ldquoFive additionalCostello syndrome patients with rhabdomyosarcoma proposalfor a tumor screening protocolrdquo American Journal of MedicalGenetics vol 108 no 1 pp 80ndash87 2002
[9] K W Gripp A E Lin D L Stabley et al ldquoHRAS mutationanalysis in Costello syndrome genotype and phenotype corre-lationrdquo American Journal of Medical Genetics Part A vol 140no 1 pp 1ndash7 2006
[10] M Feingold ldquoCostello syndrome and rhabdomyosarcomardquoJournal of Medical Genetics vol 36 no 7 pp 582ndash583 1999
[11] S M White J M Graham Jr B Kerr et al ldquoThe adultphenotype in Costello syndromerdquo American Journal of MedicalGenetics A vol 136 no 2 pp 128ndash135 2005
[12] G Bisogno A Murgia I Mammi M S Strafella and M CarlildquoRhabdomyosarcoma in a patient with cardio-facio-cutaneoussyndromerdquo Journal of Pediatric HematologyOncology vol 21no 5 pp 424ndash427 1999
[13] S Sigaudy G Vittu A David et al ldquoCostello syndrome reportof six patients including one with an embryonal rhabdomyosar-comardquoEuropean Journal of Pediatrics vol 159 no 3 pp 139ndash1422000
[14] A Hinek M A Teitell L Schoyer et al ldquoMyocardial storage ofchondroitin sulfate-containing moieties in Costello syndromepatients with severe hypertrophic cardiomyopathyrdquo AmericanJournal of Medical Genetics vol 133 no 1 pp 1ndash12 2005
[15] A E Lin P D Grossfeld R M Hamilton et al ldquoFurtherdelineation of cardiac abnormalities in Costello syndromerdquoAmerican Journal of Medical Genetics vol 111 no 2 pp 115ndash1292002
[16] A L Estep W E Tidyman M A Teitell P D Cotter and KA Rauen ldquoHRASmutations in Costello syndrome detection ofconstitutional activating mutations in codon 12 and 13 and lossof wild-type allele in malignancyrdquo American Journal of MedicalGenetics vol 140 no 1 pp 8ndash16 2006
[17] H KawameMMatsui K Kurosawa et al ldquoFurther delineationof the behavioral and neurologic features inCostello syndromerdquoAmerican Journal of Medical Genetics vol 118A no 1 pp 8ndash142003
[18] B Kerr M A Einaudi P Clayton et al ldquoIs growth hormonetreatment beneficial or harmful in Costello syndromerdquo Journalof medical genetics vol 40 no 6 article e74 2003
[19] J P OrsquoNeal J Ramdas W E Wood and P K PellitterildquoParameningeal rhabdomyosarcoma in a patient with Costellosyndromerdquo Journal of Pediatric HematologyOncology vol 26no 6 pp 389ndash392 2004
[20] K W Gripp ldquoTumor predisposition in Costello syndromerdquoAmerican Journal of Medical Genetics Part C Seminars inMedical Genetics vol 137C no 1 pp 72ndash77 2005
[21] Y Aoki T Niihori H Kawame et al ldquoGermline mutationsin HRAS proto-oncogene cause Costello syndromerdquo NatureGenetics vol 37 no 10 pp 1038ndash1040 2005
[22] Y Abe Y Aoki S Kuriyama et al ldquoPrevalence and clinicalfeatures of Costello syndrome and cardio-facio-cutaneous syn-drome in Japan findings from a nationwide epidemiologicalsurveyrdquo American Journal of Medical Genetics Part A vol 158no 5 pp 1083ndash1094 2012
[23] I F M Lo C Brewer N Shannon et al ldquoSevere neonatal man-ifestations of Costello syndromerdquo Journal of Medical Geneticsvol 45 no 3 pp 167ndash171 2008
[24] J Menke S Pauli M Sigler et al ldquoUniparental trisomy of amutated HRASproto-oncogene in embryonal rhabdomyosar-coma of a patient with costello syndromerdquo Journal of ClinicalOncology vol 33 no 13 pp e62ndashe65 2015
[25] C P Kratz L Franke H Peters et al ldquoCancer spectrum andfrequency among children with Noonan Costello and cardio-facio-cutaneous syndromesrdquo British Journal of Cancer vol 112no 8 pp 1392ndash1397 2015
[26] H K Ransom ldquoSarcoma of the urachus review of the literaturewith report of an additional caserdquo The American Journal ofSurgery vol 22 no 2 pp 187ndash191 1933
[27] E M L-T Fernandez N H Siverio R L Almaraz L MViota J R Luis and L D Flores ldquoRadical surgery and IVA-chemotherapeutic regimen to treat embryonal rhabdomyosar-coma of the urachus case reportrdquo Pediatric Hematology andOncology vol 24 no 7 pp 543ndash550 2007
[28] M Ishikawa T Nishi R Yamada et al ldquoA case of urachalsarcoma in childhood case report and review of the worldliteraturerdquo Journal of the Japanese Society of Pediatric Surgeonsvol 21 pp 128ndash135 1985
[29] S Yokoyama YHayashida J Nagahama et al ldquoRhabdomyosar-coma of the urachus a case reportrdquo Acta Cytologica vol 41 no4 pp 1293ndash1298 1997
[30] U Schulz and C P OrsquoLeary ldquoSpinal AVM epidermal nevusand rhabdomyosarcoma a rare neurocutaneous syndromerdquoNeurology vol 56 no 3 pp 395ndash397 2001
Case Reports in Genetics 13
[31] A Cheikhelard S Irtan D Orbach et al ldquoUrachal rhab-domyosarcoma in childhood a rare entity with a poor out-comerdquo Journal of Pediatric Surgery vol 50 no 8 pp 1329ndash13332015
[32] K W Gripp E Hopkins K Sol-Church et al ldquoPhenotypicanalysis of individuals with Costello syndrome due to HRASpG13Crdquo American Journal of Medical Genetics Part A vol 155no 4 pp 706ndash716 2011
[33] M Tarnowski G Schneider G Amann et al ldquoRasGRF1 reg-ulates proliferation and metastatic behavior of human alveolarrhabdomyosarcomasrdquo International Journal of Oncology vol 41no 3 pp 995ndash1004 2012
[34] J-S Yu K W Kim H-J Lee Y-J Lee C-S Yoon and M-J Kim ldquoUrachal remnant diseases spectrum of CT and USfindingsrdquo Radiographics vol 21 no 2 pp 451ndash461 2001
[35] C P Kratz S Rapisuwon H Reed H Hasle and P S Rosen-berg ldquoCancer in Noonan Costello cardiofaciocutaneous andLEOPARD syndromesrdquo American Journal of Medical GeneticsPart C Seminars in Medical Genetics vol 157 no 2 pp 83ndash892011
[36] B Kerr M L Mucchielli S Sigaudy et al ldquoIs the locus forCostello syndrome on 11prdquo Journal of Medical Genetics vol 40no 6 pp 469ndash471 2003
[37] TNiihori YAokiNOkamoto et al ldquoHRASmutants identifiedin Costello syndrome patients can induce cellular senescencepossible implications for the pathogenesis of Costello syn-dromerdquo Journal of Human Genetics vol 56 no 10 pp 707ndash7152011
[38] G Rosenberger S Meien and K Kutsche ldquoOncogenic HRASmutations cause prolonged PI3K signaling in response toepidermal growth factor in fibroblasts of patients with costellosyndromerdquo Human Mutation vol 30 no 3 pp 352ndash362 2009
[39] M R DeBaun ldquoScreening for cancer in children with Costellosyndromerdquo American Journal of Medical Genetics vol 108 no1 pp 88ndash90 2002
[40] K W Gripp H Kawame D H Viskochil and L NicholsonldquoElevated catecholamine metabolites in patients with Costellosyndromerdquo American Journal of Medical Genetics vol 128 no1 pp 48ndash51 2004
[41] M-ADelrue B Arveiler andD Lacombe ldquoCostello syndromeclinical features and tumoral riskrdquo Archives de Pediatrie vol 9no 10 pp 1059ndash1063 2002
[42] V Martınez-Gonzalez and P Lapunzina Sındrome de CostelloGrupodeTrabajo sobreCancer en SındromeGeneticos Polimar-formativos (GT-CSGP) httpswwworphanetdatapathoProesCSGP-Costello-3pdf
[43] K A Rauen A Banerjee W R Bishop et al ldquoCostello andcardio-facio-cutaneous syndromes moving toward clinical tri-als in RASopathiesrdquo American Journal of Medical Genetics PartC Seminars inMedical Genetics vol 157 no 2 pp 136ndash146 2011
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

4 Case Reports in Genetics
(a) (b) (c)
(d) (e) (f)
Figure 2 Patient 2 (a) Photograph of the physical features of the patient with prominent forehead low-set ears lower palpebral fissureshypertelorism broad nasal bridge thick lips and anteverted slightly nostrils (b) Initial abdominal ultrasound showing the presence ofa tubular image caliber of 56mm extending in the theoretical location of the right umbilical artery ((c) and (d)) Follow-up abdominalultrasound in themidline showing amultilobulated hypoechoic solid tumorwithmarked hypervascularization extending from the proximityof the abdominal wall to the right supravesical region (e) MRI onT2-weighted sequence confirms the presence of several nodular massesgrouped with thickening of both medial umbilical folds the right to 4mm proximal to the umbilicus and 8mm adjacent to the iliac vesselsparavesical region portion (f) Operative image indicating the presence of tumor originating in the right medial UL
most frequent encountered HRAS mutation associated withRMS was pG12S (712) Only 4 deaths were documented inpatients with change in codon 12 (2 patients G12S 1 patientG12A and 1 patient G12C) Chemotherapy that was appliedvaries based on the protocols of the countries where theywerediagnosed (Table 2) [5ndash10 12ndash14 16ndash25] Overall survival wasabout 43 (921) Mortality was observed in 12 out of 21individuals in nine of them associated with neoplasia andin three associated with surgery
Similarly the total number of reported cases of ULRMS in pediatric patients either in the obliterated umbilicalarteries (medial UL) or in urachus (median UL) is 17including these 2 new cases (Table 3) [5 7ndash9 24ndash31] Themean age of diagnosis was 3 years and 4 months (range 4monthsndash6 years) It is slightly more common in females thanin males (14 1) Themost common location was the urachus(1517) The most common histological type was embryonalRMS (1215) and one-fourth (312) of patients who died withreported histology showed embryonal RMS Chemotherapyvaries based on the protocols of the countries where theywerediagnosed (Table 4) [7 24 26ndash31] Overall survival was 69
(1116) overall mortality was 31 (516) two-year absolutesurvival rate was 69 (1116) and five-year absolute survivalrate was 19 (316)
5 Discussion
The prevalence of CS is estimated to be 1 1290000 individ-uals in Japan and at least 1 500000 in the United Kingdomthe incidence was estimated to be 1 60000ndash100000 [4 22]The overall tumor incidence is approximately 10ndash15 overthe lifetime of individuals with an identified HRASmutation[1 4 9] RMS accounting in about 60 of all neoplasia [1]Based on the 300 cases of CS currently known [4] we foundan incidence of 87 RMS in patients with CS
CS is the first disorder associated with germlinemutations in the Ras family of guanosine-51015840-triphosphate(GTP)ases [21] HRAS has six exons five exons are encodedfor a protein of 189 amino acids with a molecular weight of21 kDa [4] Missense mutations at codons 12 and 13 are inconstitutively active GTP-bound conformation and activatedownstream effectors such as MAPK phosphatidylinositol3-kinases (PI3K) and ral guanine nucleotide dissociation
Case Reports in Genetics 5
Table1Ch
aracteris
ticso
fpatientsw
ithCostello
synd
romea
ndrhabdo
myosarcom
a
PT number
Author
Year
Cou
ntry
Sex
Age
atdiagno
sis(yearsm
onths)
Symptom
sLo
catio
nHistolog
yMutation
AAC
(NS)
Therapy
Outcome
1Ke
rretal
[78]
1998
England
F2y
4mVo
miting
Con
stipatio
nRe
troperiton
ealleft
psoasm
ayor
muscle
Embryonal
G12S
(34GgtA)lowast
[9]
SCh
TRe
lapsetumor-fr
eeageo
f7years
2Ke
rretal
[78]
1998
England
F3y
2mAb
dominal
mass
Pelvis
urachu
s(m
edianUL)
adherent
tothe
bladder
Embryonal
G12A
(35GgtC)
[5]
SCh
T
Histologyshow
edextend
ingup
tothe
resectionmargin
Diedaged
5years
[59]
3Feingold
[810]
1999
USA
M6m
Tumor
Rightfoo
tAlveolar
NDF
SCh
TTu
mor-fr
eeageo
f20
years[11]
4Bisogn
oetal
[8912]
1999
Italy
M1y
8mCon
stipatio
nAb
dominal
pain
Lower
abdo
men
pelvis
abdo
minal
walllowast
Embryonal
NDF
SCh
TOnlybiop
syDiedaged
2yearsa
nd3mon
ths
5Sigaud
yetal
[813]
2000
France
M6y
NDF
Inguinalscrotal
Embryonal
NDF
NDF
NDF
6Grip
petal
[81415]
2002
USA
M5y
6mAb
dominal
pain
Pelvis
pulm
onary
metastasesw
aspresent
Embryonal
NDF
SCh
TDiedaft
errecurrence
[14]
7Grip
petal
[8]
2002
USA
F3y
7mAb
dominal
pain
Emesis
Upp
erabdo
men
masse
ncasingthe
superio
rmesenteric
anceliaca
rteries
Sing
lepu
lmon
ary
nodu
le
Pleomorph
icNDF
ChT
Diedaged
4years
8Grip
petal
[8]
2002
USA
F2y
6mAb
dominal
mass
Pelvis
bladder
Embryonal
NDF
ChT
RTS
Diedaged
7yearsfor
recurrency
ofRM
Sfib
rosarcom
a[16]
9Grip
petal
[8]
2002
USA
NDF
7mPerin
eal
grow
thPerin
eal
Embryonal
NDF
ChT
RTS
Tumor-fr
eeageo
f2years
10Grip
petal
[8]
2002
USA
NDF
1y11m
Prop
tosis
Leftorbit
Unk
nown
NDF
SRT
Tumor-fr
eeageo
f4years
11Ka
wam
eetal
[17]
2003
Japan
F1y
4mAb
dominal
mass
Pelvis
Spindlec
ell
NDF
SCh
TTu
mor-fr
eeageo
f7years
6 Case Reports in GeneticsTa
ble1Con
tinued
PT number
Author
Year
Cou
ntry
Sex
Age
atdiagno
sis(yearsm
onths)
Symptom
sLo
catio
nHistolog
yMutation
AAC
(NS)
Therapy
Outcome
12Ke
rretal
[18]
2003
UK
M2y
2mLargep
elvic
mass
Retro
vesic
ular
mass
byultrasou
ndEm
bryonal
NDF
ChT
Diedaged
2yearsa
nd4mon
ths
13OrsquoNealetal
[19]
2004
USA
F3y
Right-s
ided
cervicofacial
mass
Parameningeal
infratem
poralfossa
right
perip
arotid
mastic
ator
space
region
Alveolar
NDF
ChTS
RT
Clinicalgrou
p3T2
bN0stage3
Dieddu
ringsurgery
14Grip
p[20]
2005
USA
F3y
2mFacialmass
Rightinfratempo
ral
fossa
Mixed
alveolar
and
embryonal
NDF
ChTS
Dieddu
ringsurgery
byventric
ular
tachycardiafollowed
rapidlyby
lossof
heartrhythm
15Ao
kietal
[2122]
2005
Japan
F7y
2mNDF
NDF
NDF
G12S
(34GgtA)
NDF
NDF
16Grip
petal
[9]
2006
USA
M2y
NDF
NDF
NDF
G12S
(34GgtA)
NDF
Tumor-fr
eeageo
f11
yearslowast
17Ke
rretal[5]
2006
UK
NDF
7mNDF
Metastatic
arising
from
thep
rosta
teEm
bryonal
[23]
G12C
(34GgtT)
NDF
Diedaged
7mon
ths
18Ke
rretal[5]
2006
UK
NDF
NDF
NDF
NDF
NDF
G12S
(34GgtA)
NDF
Diedaged
7years
19Ke
rretal[5]
2006
UK
NDF
NDF
NDF
NDF
NDF
G12A
(35GgtC)
NDF
NDF
20Lo
etal[23]
2008
UK
M2y
3mRe
spira
tory
functio
ndeterio
rated
Rightlun
gNDF
G12S
(34GgtA)
SDiedfewweeks
later
surgery
21Ahm
adiand
Harley[6]
2010
USA
M2y
Increasedwork
ofbreathing
Nasop
haryngeal
Embryonal
NDF
SCh
TRT
Clinicalgrou
pIIA
(T1N
0M0)
Tumor-fr
eeageo
f3years
22Ab
eetal[22]
2012
Japan
NDF
NDF
NDF
NDF
NDF
NDF
NDF
Died
23Menke
etal
[2425]
2015
Germany
F3y
Abdo
minal
mass
Lower
anterio
rabdo
menabo
vethe
urinarybladderlowast
(urachus-m
edianUL
bylocatio
n)
Embryonal
G12C
(34GgtT)
SCh
T
R1resection
(marginaltum
orresid
ue)Tu
mor-fr
eeageo
f6years
24Kr
atze
tal
[25]
2015
Germany
M1y
NDF
NDF
Embryonal
G12S
(34GgtA)
NDF
NDF
25
Sanchez-
Mon
tenegro
etal(this
repo
rt)
2017
Spain
F2y
4mAs
ymptom
atic
LeftmedialU
LEm
bryonal
G12A
(35GgtC)
ChTS
RTTu
mor-fr
eeageo
f4yearsa
nd4mon
ths
26
Sanchez-
Mon
tenegro
etal(this
repo
rt)
2017
Spain
F3y
10m
Asym
ptom
atic
Rightm
edialU
LSpindlec
ell
G12S
(34GgtA)
SCh
TTu
mor-fr
eeageo
f5yearsa
nd4mon
ths
AAC
aminoacid
changeC
hTchemotherapyFfem
aleMm
aleNDFno
datafoun
dNSnu
cleotides
ubstitutio
nPT
patientR
TradiotherapySsurgeryU
Lum
bilicalligam
entlowastPerson
alcommun
icationby
author
Case Reports in Genetics 7
Table 2 Chemotherapy of patients with Costello syndrome and rhabdomyosarcoma
PTnumber Chemotherapy protocol
1Initially with VCR ACD and CTX After debulking continued on ChT using IFOS VCR and ACD After the second coursewhen she developed IFOS induced encephalopathy she was changed back to pulses of VCR ACD and CTX given every 3weeks for 9 courses [7]
2Initially IFOS ACD and VCR After 4 courses CTX was substituted for IFOS because hemorrhagic cystitis Tx complicatedby recurrent episodes of moderately severe diarrhoea and febrile neutropenia requiring readmission to hospital Tx wascompleted after six courses of ChT [7]
3 Tx consisted of below the knee amputation and ChT (DOX ACD VCR and CTX) [10]
4
Tx was implemented according to the Italian protocol for pediatric soft tissue sarcoma Three courses of ChT including VCR(0025mgkg day 1) IFOS (50mgkg days 1 and 2) and alternating ACD (0025mgkg day 1) and DOX (07mgkg day 1) wereadministered Symptoms regressed and the CT scan showed a reduction in tumor volume of more than two-thirds After 3more courses of ChT the patient experienced abdominal pain A repeat abdominal CT scan showed an increase in the pelvicmass Despite the administration of a different ChT with CBDCA (11mgkg day 1) and VP-16 (3mgkg for 3 doses) the tumorcontinued to grow and the child died 7 months after the diagnosis of RMS [12]
5 NDF [13]
6
The first cycle of ChT with VCR ACD and CTX and topotecan reduced the tumor size [16] The tumor was surgicallyremoved after the first ChT [8] Debulking S was required because of rapid growth and tumor necrosis The protocol wascontinued and was deemed sufficiently successful to withhold RT One month after completion of the first protocol tumorrecurrence necessitated a second round of ChT with irinotecan and DOXThe latter drug was administered about 1 weekbefore he died during which time he had tachycardia (heart rate 180ndash20 bpm) [14]
7 The tumor did not respond to ChT and she died shortly after her 4th birthday [8]8 Tx was a combination of S ChT and RT continued until age of 35 years [8]9-10 NDF [8]11 PT had later generalized tonic-clonic seizures during her Tx for RMS [17]12 Despite extensive ChT the tumor progressed rapidly and the PT died 2 months later [18]
13 Induction ChT was commenced with the initial 12-week course of VCR ACD and CTX based on the Intermediate RiskProtocol D9803 of the COG [19]
14 ChT did not result in tumor shrinkage therefore surgical resection was performed [20]15ndash22 NDF [5 6 9 21ndash23]23 ChT according to the cooperative soft tissue sarcoma protocol (CWS-2002 P) was well tolerated by the PT [24]24 NDF [25]
25 ChT in the standard risk group protocol EpSSG RMS 2005 subgroup D 3 preoperative cycles of IFOS (2 doses at 100mgkg)VCR (005mgkg) and ACD (005mgkg)
26 ChT (postoperative 15 days) in the standard risk group protocol EpSSG RMS 2005 subgroup B (Stage I) cycles of IFOS (2doses of 3 gm2d) VCR (15mgm2) and ACD (15mgm2) was initiated
ACD actinomycin D CBDCA carboplatin ChT chemotherapy COG childrenrsquos oncology group CTX cyclophosphamide CT computed tomography CWSCooperative Weichteilsarkom Studie (Cooperative Soft Tissue Sarcoma Study) DOX Doxorubicin EpSSG European pediatric Soft tissue sarcoma StudyGroup IFOS ifosfamide NDF no data found PT patient RMS rhabdomyosarcoma RT radiotherapy S surgery Tx treatment VCR vincristine VP-16etoposide
stimulator (RalGDS) [16 21] in signaling pathways control-ling cell proliferation and differentiation [9]
Themajority of patients with CS had 34GgtA transition incodon 12 (80) [4 16] More than 95 of the mutations arepredicted to result in substitution of the glycine in position12 or 13 of the protein product [1] All individuals withmalignancy had a codon 12 mutation (especially G12A 47patients) [5 21] The rare G12V mutation is associated witha more severe early lethal phenotype some patients diefrom respiratory distress hypertrophic cardiomyopathy ormalignant tachycardia prior to being diagnosed with CS [1]As far as we know no individual with G13C has developed amalignant tumor [4 32]
RMS is the most common soft tissue sarcoma of infancyIts incidence is between 4 and 7 cases per 1 million childrenyounger than 15 years [8 12] The age peak is between 2 and5 years with a slight male predominance (12ndash141) Thesetumors may arise anywhere in the body and fewer than 20are located in the pelvis [12]Most RMS tumors are originatedin the head and neck region urogenital tract and extremities[33] The most common histologic type seen in gt50 isembryonal followed by alveolar in 20ndash30 PleomorphicRMS is rare (1) and has a poor prognosis [8] AlveolarRMS is characterized by the translocation t(213)(q35q14) in70 of cases and the variant translocation t(113)(p36q14)in a smaller percentage of cases Evidence accumulates
8 Case Reports in Genetics
Table3Ch
aracteris
ticso
fPediatricPatie
ntsw
ithUmbilicalLigamentR
habd
omyosarcom
a
PT number
Author
Year
Cou
ntry
Sex
Age
atdiagno
sis(yearsm
onths)
Symptom
sLo
catio
nSize
(cm)
Histology
IRS
grou
pTh
erapy
Outcome
1Ra
nsom
[2627]
1933
USA
F4m
Massb
elowthe
umbilicus
and
extend
ing
somew
hattothe
right
Urachus
(medianUL)
attached
alon
gthea
nterior
wallfrom
theu
mbilicus
tothea
pexof
theb
ladd
er
115
Spindle
cell
ISM
AC
RT
Lastcheck-up
exam
ination(2
years)
show
edno
evidence
ofrecurrence
2Ishikawae
tal[28]
1985
Japan
F1y
4mAb
dominalmass
abdo
minalpain
hemop
erito
neum
Urachal(m
edianUL)
intra-abdo
minalruptureo
fthetum
or
Fist-
sized
NDF
IVSM
ACNDF
3Yo
koyamae
tal[2729]
1997
Japan
M2y
Episo
diclow
erabdo
minalpain
Urachus
(medianUL)
extraperito
neallocated
betweentheu
mbilicus
and
apex
oftheb
ladd
erandwas
adherin
gtig
htlyto
both
Theb
ilateralm
edialU
Lweres
eenenterin
gthe
tumorR
upturedwith
asm
alln
umbero
fdissem
inated
tumors
scatteredon
them
esentery
andDou
glas
pouch
12Em
bryonal
IVSM
AI
ChT
At2yearso
ffollo
w-upno
recurrence
hadbeen
detected
4lowastKe
rretal
[78]
1998
England
F3y
2mAb
dominalmass
Urachus
(medianUL)
adherent
totheb
ladd
erNDF
Embryonal
IIaSM
II
ChT
Histologyshow
edextend
ingup
tothe
resectionmargin
Diedaged
5years
[59]
5Schu
lzand
OrsquoLeary
[2730]
2001
Scotland
M2y
NDF
Urachus
(medianUL)
NDF
Embryonal
NDF
SCh
TRT
Tumor-fr
eeageo
f26
years
6Fernandeze
tal[27]
2007
Spain
F6y
Intractable
constip
ation
nauseaabd
ominal
painles
smass
Urachus
(medianUL)
infiltratingthev
entral
abdo
minalwalland
fixed
tothev
esicaldo
me
135
Embryonal
IbSM
IC
ChT
At4yearso
ffollo
w-upthep
atient
remains
welland
free
ofclinicald
isease
7lowastMenke
etal
[2425]
2015
Germany
F3y
Abdo
minalmass
Lower
anterio
rabd
omen
abovethe
urinarybladderamp
(urachusm
edianULby
locatio
n)
NDF
Embryonal
IIaSM
II
ChT
R1resection
(marginaltum
orresid
ue)Tu
mor-fr
eeageo
f6years
8Ch
eikh
elard
etal[31]
2015
Dx
1983
France
F5y
5mNDF
Urachus
(medianUL)
periton
ealm
etastasesa
ndhypo
gastric
lymph
nodes
5NDF
IVSM
AI
ChT
Died31
mon
thsa
fter
diagno
siswith
relap
sein
periton
ealliver
at11mon
ths
Case Reports in Genetics 9
Table3Con
tinued
PT number
Author
Year
Cou
ntry
Sex
Age
atdiagno
sis(yearsm
onths)
Symptom
sLo
catio
nSize
(cm)
Histology
IRS
grou
pTh
erapy
Outcome
9Ch
eikh
elard
etal[31]
2015
Dx
2003
France
F3y
3mPeriton
ealrup
ture
poor
generalstatus
Urachus
(medianUL)
lumbo
aorticandexternal
iliac
lymph
nodes
10Alveolar
IVSM
AI
ChTRT
Died57
mon
thsa
fter
diagno
siswith
relap
sein
periton
ealliver
at30
mon
ths
10Ch
eikh
elard
etal[31]
2015
Dx
2005
France
F2y
6mMasspo
orgeneral
statusdysuria
Urachus
(medianUL)
15Em
bryonal
III
SMII
ChTRT
Died37
mon
thsa
fter
diagno
siswith
periton
ealrelapse
at19
mon
ths
11Ch
eikh
elard
etal[31]
2015
Dx
2005
France
M4y
2mMasspo
orgeneral
statusdysuria
Urachus
(medianUL)
periton
ealm
etastasesa
ndiliac
lumbo
aorticlymph
nodes
10Em
bryonal
IVSM
II
ChTRT
Relapsed
multifocalat
82mon
thsfollo
w-up
100mon
ths
12Ch
eikh
elard
etal[31]
2015
Dx
2005
France
M5y
3mMasspo
orgeneral
status
Urachus
(medianUL)
periton
ealm
etastasesa
ndmesenteric
lymph
nodes
106
Embryonal
IVSM
IC
ChTRT
Tumor
freea
fter9
5mon
thssince
diagno
sis
13Ch
eikh
elard
etal[31]
2015
Dx
2006
France
M2y
5mMasspo
orgeneral
statusob
structiv
erenalinsuffi
ciency
Urachus
(medianUL)
periton
ealbon
emetastases
andhypo
gastric
lymph
nodes
21Em
bryonal
IVSM
II
ChTRT
Bone
progression
after
16mon
thsdied
18aft
erdiagno
sis
14Ch
eikh
elard
etal[31]
2015
Dx
2010
France
M4y
5mAb
dominalpain
Urachus
(medianUL)
7Em
bryonal
III
SMIC
ChT
Tumor
freea
fter18
mon
thssince
diagno
sis
15Ch
eikh
elard
etal[31]
2015
Dx
2010
France
M6y
Abdo
minalpain
Urachus
(medianUL)
periton
ealm
etastases
14Em
bryonal
IVSM
AI
ChTRT
Tumor
freea
fter4
5mon
thssince
diagno
sis
16lowast
Sanchez-
Mon
tenegro
etal(this
repo
rt)
2017
Dx
2015
Spain
F2y
4mAs
ymptom
atic
LeftmedialU
L5
Embryonal
IaCh
TSM
IC
RT
Tumor-fr
eeageo
f3yearsa
nd9mon
ths
17lowast
Sanchez-
Mon
tenegro
etal(this
repo
rt)
2017
Dx
2015
Spain
F3y
10m
Asym
ptom
atic
Rightm
edialU
L85
Spindle
cell
IIaSM
II
ChT
Tumor-fr
eeageo
f4yearsa
nd5mon
ths
ChT
chem
otherapyD
xdiagno
sed
Ffemale
IRS
intergroup
rhabdo
myosarcom
aMm
ale
NDF
nodata
foun
dRT
radiotherapy
Ssurgery
SMAIsurgerymacroscop
ically
incomplete
SMAC
surgery
macroscop
icallycompleteSM
ICsurgery
microscop
icallycompleteSM
IIsurgery
microscop
icallyincompleteULum
bilicalligam
ent
ampPerson
alcommun
icationby
authorlowast
Patientsw
ithCostello
synd
rome
10 Case Reports in Genetics
Table 4 Chemotherapy of pediatric patients with umbilical ligament rhabdomyosarcoma
PTnumber Chemotherapy protocol
1-2 No ChT [26 28]3 After establishment of the final diagnosis he was treated with combined ChT including VCR ACD and CTX [29]
4lowastInitially IFOS ACD and VCR After 4 courses CTX was substituted for IFOS because of hemorrhagic cystitis Tx complicatedby recurrent episodes of moderately severe diarrhoea and febrile neutropenia requiring readmission to hospital Tx wascompleted after six courses of ChT [7]
5 NDF [30]
6 PT started induction of ChT 2 weeks after S Induction regimen included 9 cycles of IVA (IFOS VCR and ACD) that were welltolerated with minimal systemic complications (Tx 953 of the MMT 95 SIOP protocol for RMS) [27]
7lowast ChT according to the cooperative soft tissue sarcoma protocol (CWS-2002 P) was well tolerated by the PT [24]8 Adjuvant ChT with 10 cycles of IFOS VCR and ACD [31]9 Adjuvant ChT with 6 cycles of IFOS VCR and VP-16 and 9 cycles of VCR ACD CTXACD and CTX [31]10 Neoadjuvant ChT with 6 cycles of IFOS VCR and ACD and adjuvant ChT with 3 cycles of IFOS VCR and ACD [31]
11 Neoadjuvant ChT with 1 cycle of CTX VCR and PRED 2 cycles IFOS VCR and ACD and 4 cycles of IFOS VCR ACD andDOX and adjuvant ChT with 3 cycles of IFOS VCR and ACD [31]
12 Neoadjuvant ChT with 1 cycle of CTX VCR and PRED and 5 cycles of IFOS VCR ACD and DOX and adjuvant ChT with 2cycles of IFOS VCR ACD and DOX and 1 cycle of IFOS VCR and ACD [31]
13 Neoadjuvant ChT with 2 cycles of VCR ACD and CTX + and 3 cycles of IFOS VCR ACD and DOX and adjuvant ChT with 3cycles of IFOS VCR and ACD [31]
14 Neoadjuvant ChT with 4 cycles of IFOS VCR ACD and DOX and adjuvant ChT with 5 cycles of IFOS VCR ACD [31]
15 Neoadjuvant ChT with 4 cycles of IFOS VCR ACD DOX 3 cycles of IFOS VCR ACD and adjuvant ChT with 1 cycle of IFOSVCR ACD 1 cycle of IFOS VCR [31]
16lowastChT in the standard risk group protocol EpSSG RMS 2005 subgroup D 3 preoperative cycles of IFOS (2 doses at 100mgkg)VCR (005mgkg) and ACD (005mgkg)
17lowastChT (postoperative 15 days) in the standard risk group protocol EpSSG RMS 2005 subgroup B (Stage I) cycles of IFOS (2 dosesof 3 gm2d) VCR (15mgm2) and ACD (15mgm2) was initiated
ACD actinomycin D ChT chemotherapy CTX cyclophosphamide CWS Cooperative Weichteilsarkom Studie (Cooperative Soft Tissue Sarcoma Study)DOX Doxorubicin EpSSG European pediatric Soft tissue sarcoma Study Group IFOS ifosfamide MMT malignant mesenchymal tumor NDF no datafound PRED prednisone PT patient RMS rhabdomyosarcoma S surgery SIOP Societe Internationale DrsquoOncologie Pediatrique (International Society ofPediatric Oncology) Tx treatment VCR vincristine VP-16 etoposide lowastPatients with Costello syndrome
that alveolar RMS and embryonal RMS are two differentdisorders while alveolar RMS may originate from primitiveuncommitted mesodermal cells embryonal RMS originatesprobably from more differentiated myoblasts Ras protein-specific guanine nucleotide-releasing factor 1 (RasGRF1)plays an important role in alveolar RMS pathogenesis Theseinteresting concepts however need more evidence [33]
The umbilicus caudally originates the common ligamentwhich is divided into obliterated umbilical arteries (medialUL) and urachus (median UL) The urachus varies from3 to 10 cm in length and from 8 to 10mm in diameterIt is a three-layered tubular structure the innermost layerbeing lined with transitional epithelium in 70 of casesand with columnar epithelium in 30 The structure issurrounded by connective tissue and outermost muscularlayer in continuity with the detrusor muscle Along its pathfrom the bladder to the umbilicus the urachus lies betweenthe transverse fascia and the parietal peritoneum containedin the pyramidal retropubic perivesical preperitoneal spacecompartmentalized by umbilicovesical fascia along with themedial umbilical ligaments and the bladder Occasionallythe urachus may merge with one or both of the obliteratedumbilical arteries (medial UL) and there may be a slight
deviation to the right or left of the midline [34] The urachusis an embryological remnant resulting from the obliterationof the allantoic channel which attaches the bladder dome tothe umbilicus [31]
Urachal malignant tumors are extremely rare represent-ing less than 05 of all bladder cancers and 001 of alltumors They may arise from any portion of the urachus andare most commonly found in adults and males (60ndash70)Although sarcomas represent only 8 they are the mostfrequent urachal neoplasms reported in patients youngerthan 20 years of age (67) [27] Poor prognosis is a commonfeature in adults and pediatric urachalmalignancies with 50to 60 of 5-year survival In contrast the 5-year event-freesurvival in pelvic RMS was reported to be about 51 [31]
This indolent and rather large urachal tumor was mostlyrevealed by an uncomplicated progressing mass withoutprodromic urological symptomsThedelay of diagnosis couldbe explained by a long asymptomatic progression of thetumor in a preperitoneal location which allows an importantlocal spreading before diagnosis Even in patients withouttumor rupture peritoneal involvement appeared to be the keypoint in the prognosis of urachal RMS Systematic cytologyat diagnosis could be more accurate to evaluate peritoneal
Case Reports in Genetics 11
extension in order to avoid understaging and adjust adjuvantlocoregional treatment [31]
Previously only 12 patients with RMS arising from theurachus (median UL) in children without CS have beenreported in the English literature (Table 3) By 2011 therewere29 reported cases of cancer in patients withCS 19 RMS (meanage of 23 years 9 embryonal 1 alveolar 1 mixed histology1 pleomorphic 1 spindle cell type and 6 unclassified) 5neuroblastomas 4 bladder cancer and 1 fibrosarcoma [35]
Loss of heterozygosity for 11p155 in RMS from individu-als with CS suggests that loss of the wild-type allele is the sec-ond hit in tumor development [6 16 36] Whereas theHRASmutation in a sporadic malignancy in the general populationis present only within the tumor cells in CS an identicalmutation is present in every single cell of the individualthus accounting for the tumor predisposition [1] implicatingan alternate mechanism of rhabdomyosarcogenesis [16] Inaddition one patient with CS and uniparental trisomy dueto triplication of the mutated paternal HRAS gene was alsoreported RMS typically displays loss of heterozygosity ofthe 11p155 region because of paternal uniparental disomyand approximately 28 of cases harbor mutations in genesof growth signaling pathways In reports of uniparentaldisomy plus HRAS mutation the latter was heterozygousand therefore must have occurred after the developmentof uniparental disomy [24] The functional analysis alsorevealed that CS-causing mutant HRAS proteins causedoncogene-induced senescence in human fibroblasts [37]Theimportant role of PI3K-protein-kinase B (AKT) signalingin Ras-mediated transformation and tumorigenesis is high-lighted by constitutive AKT activation in RMS cell lines andclinical samples Thus prolonged PI3K-AKT signaling mightalso be implicated in the development of soft tissue sarcomain patients with CS [38]
Only four out of 11 patients were diagnosed with CS priorto the RMS diagnosis in 5 patients CS was diagnosed afterthe RMS and in the remaining 2 the order was unknown[20] In 2003 a further three unpublished cases of RMS inchildren with CS were known through the International CSSupport Group [18] and for that reason there is possiblyunderdiagnosis of RMS in patients with CS
A screening protocol was proposed consisting of ultra-sound examination of the abdomen and pelvis every 3ndash6 months until age of 8ndash10 years for RMS and abdomi-nal neuroblastoma urine catecholamine metabolite analysisevery 6ndash12 months until age of 5 years for neuroblastomaand urinalysis for hematuria annually for bladder carcinomaafter age of 10 years The prior diagnosis of CS was theprerequisite for the implementation of a tumor screeningprotocol [8] The recommendation based on the presumedfast doubling time of RMS was abdominal sonographyscreening for RMS that should be done in similar intervalsof every four months until stronger evidence would suggestotherwise [39] Screening for neuroblastoma is no longerrecommended becausemany CS patients without identifiabletumor show elevated catecholamine metabolites in urine itappears that in this patient group an elevation above thenormal limit defined as 2 standard deviations (SD) above themean for age is more likely to be a variant rather than a sign
of a neuroblastoma [1 40] A French monitoring protocolproposed the determination of catecholamines and theirmetabolites in urine every six months until the age of 5 yearsand ultrasound abdominopelvic every six months until theend of the puberty seeking hematuria dipstick from6monthsto the age of 10 [41] The protocol in our hospital for patientswith CS includes an abdominal and pelvic ultrasound 3times during the first year of life and in childhood every 6months until age of 10 [42] We believe that the best optionis to perform a pelvic abdominal ultrasound every 3 monthsduring the first eight years of life and then controls accordingto medical criteria This is even more necessary in patientswith possible UL RMS because diagnosis was usually done inadvanced stages with a poor survival It is possible that withclose monitoring after an early diagnosis will detect initialstages of the tumor in previously not described locations
Head and neck MRI scans can be performed less fre-quently Ear examination and tympanometry every 4 to 6months to detect middle ear effusion which would raisesuspicion for a nasopharyngeal mass are also recommended[6]
The outcome of CS patients with RMS has been compa-rable to that for patients without the syndrome with a 5-yearsurvival rate of 65 to 70 [19] but according to this reviewit could be worse than the general population Neoplasia wasnoted at the cause of death in five (22) patients with CS[4 15] but in our study the mortality associated with RMSwas 43 Because the long-term survival in RMS is basedon the histology of the tumor and the extent of disease atdiagnosis early diagnosis may alter the treatment regimenand improve prognosis This could be particularly importantin patients with CS who often are medically fragile [20]
The RasMAPK pathway is an attractive target in thetreatment of cancer utilizing small molecule therapeuticsthat specifically inhibits the pathway Ras pathway agentssuch as farnesyltransferase inhibitors (tipifarnib and lona-farnib) that prevent posttranslational modification of Rasare being evaluated for cancer treatment and may be oftherapeutic use for syndromes in this pathway especially CSIn addition B-Raf protooncogene serinethreonine kinase(BRAF) and mitogenextracellular signal-regulated kinase(MEK) inhibitors offer the same potential in the possibletreatment of CS Since the RasMAPK pathway has targets forinhibition in cancer treatment there aremany smallmoleculetherapeutics that are in development or undergoing clinicaltrials with some already FDA approval [43]
6 ConclusionsCS is a syndrome poorly known in oncology but theirpredisposition tomalignancies includingULRMS implies theneed for a new perspective on early diagnosis and aggressivemedical and surgical treatment
ConsentInformed consent was obtained from the new two individualparticipants included in the study and has been properlydocumented with the parental approval to the use of patientrsquosimages and complementary studies
12 Case Reports in Genetics
Competing Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
Special thanks are due to Israel Fernandez Pineda MDAssistantMember and Surgery Fellowship ProgramDirectorSt Jude Childrenrsquos Research Hospital (Memphis TN) for therecommendations and corrections to the manuscript
References
[1] E Quezada and K W Gripp ldquoCostello syndrome and relateddisordersrdquo Current Opinion in Pediatrics vol 19 no 6 pp 636ndash644 2007
[2] JM Costello ldquoA new syndromerdquoNewZealandMedical Journalvol 74 article 397 1971
[3] JMCostello ldquoAnew syndromemental subnormality andnasalpapillomatardquo Australian Paediatric Journal vol 13 no 2 pp114ndash118 1977
[4] K W Gripp and A E Lin ldquoCostello syndrome a Rasmitogenactivated protein kinase pathway syndrome (rasopathy) result-ing from HRAS germline mutationsrdquo Genetics in Medicine vol14 no 3 pp 285ndash292 2012
[5] B Kerr M-A Delrue S Sigaudy et al ldquoGenotype-phenotypecorrelation in Costello syndrome HRAS mutation analysis in43 casesrdquo Journal of Medical Genetics vol 43 no 5 pp 401ndash4052006
[6] N Ahmadi and E Harley ldquoCostello syndrome and the impor-tance of cancer screeningrdquo Archives of OtolaryngologymdashHeadand Neck Surgery vol 136 no 10 pp 1028ndash1029 2010
[7] B Kerr O B Eden R Dandamudi et al ldquoCostello syndrometwo cases with embryonal rhabdomyosarcomardquo Journal ofMedical Genetics vol 35 no 12 pp 1036ndash1039 1998
[8] K W Gripp C I Scott Jr L Nicholson et al ldquoFive additionalCostello syndrome patients with rhabdomyosarcoma proposalfor a tumor screening protocolrdquo American Journal of MedicalGenetics vol 108 no 1 pp 80ndash87 2002
[9] K W Gripp A E Lin D L Stabley et al ldquoHRAS mutationanalysis in Costello syndrome genotype and phenotype corre-lationrdquo American Journal of Medical Genetics Part A vol 140no 1 pp 1ndash7 2006
[10] M Feingold ldquoCostello syndrome and rhabdomyosarcomardquoJournal of Medical Genetics vol 36 no 7 pp 582ndash583 1999
[11] S M White J M Graham Jr B Kerr et al ldquoThe adultphenotype in Costello syndromerdquo American Journal of MedicalGenetics A vol 136 no 2 pp 128ndash135 2005
[12] G Bisogno A Murgia I Mammi M S Strafella and M CarlildquoRhabdomyosarcoma in a patient with cardio-facio-cutaneoussyndromerdquo Journal of Pediatric HematologyOncology vol 21no 5 pp 424ndash427 1999
[13] S Sigaudy G Vittu A David et al ldquoCostello syndrome reportof six patients including one with an embryonal rhabdomyosar-comardquoEuropean Journal of Pediatrics vol 159 no 3 pp 139ndash1422000
[14] A Hinek M A Teitell L Schoyer et al ldquoMyocardial storage ofchondroitin sulfate-containing moieties in Costello syndromepatients with severe hypertrophic cardiomyopathyrdquo AmericanJournal of Medical Genetics vol 133 no 1 pp 1ndash12 2005
[15] A E Lin P D Grossfeld R M Hamilton et al ldquoFurtherdelineation of cardiac abnormalities in Costello syndromerdquoAmerican Journal of Medical Genetics vol 111 no 2 pp 115ndash1292002
[16] A L Estep W E Tidyman M A Teitell P D Cotter and KA Rauen ldquoHRASmutations in Costello syndrome detection ofconstitutional activating mutations in codon 12 and 13 and lossof wild-type allele in malignancyrdquo American Journal of MedicalGenetics vol 140 no 1 pp 8ndash16 2006
[17] H KawameMMatsui K Kurosawa et al ldquoFurther delineationof the behavioral and neurologic features inCostello syndromerdquoAmerican Journal of Medical Genetics vol 118A no 1 pp 8ndash142003
[18] B Kerr M A Einaudi P Clayton et al ldquoIs growth hormonetreatment beneficial or harmful in Costello syndromerdquo Journalof medical genetics vol 40 no 6 article e74 2003
[19] J P OrsquoNeal J Ramdas W E Wood and P K PellitterildquoParameningeal rhabdomyosarcoma in a patient with Costellosyndromerdquo Journal of Pediatric HematologyOncology vol 26no 6 pp 389ndash392 2004
[20] K W Gripp ldquoTumor predisposition in Costello syndromerdquoAmerican Journal of Medical Genetics Part C Seminars inMedical Genetics vol 137C no 1 pp 72ndash77 2005
[21] Y Aoki T Niihori H Kawame et al ldquoGermline mutationsin HRAS proto-oncogene cause Costello syndromerdquo NatureGenetics vol 37 no 10 pp 1038ndash1040 2005
[22] Y Abe Y Aoki S Kuriyama et al ldquoPrevalence and clinicalfeatures of Costello syndrome and cardio-facio-cutaneous syn-drome in Japan findings from a nationwide epidemiologicalsurveyrdquo American Journal of Medical Genetics Part A vol 158no 5 pp 1083ndash1094 2012
[23] I F M Lo C Brewer N Shannon et al ldquoSevere neonatal man-ifestations of Costello syndromerdquo Journal of Medical Geneticsvol 45 no 3 pp 167ndash171 2008
[24] J Menke S Pauli M Sigler et al ldquoUniparental trisomy of amutated HRASproto-oncogene in embryonal rhabdomyosar-coma of a patient with costello syndromerdquo Journal of ClinicalOncology vol 33 no 13 pp e62ndashe65 2015
[25] C P Kratz L Franke H Peters et al ldquoCancer spectrum andfrequency among children with Noonan Costello and cardio-facio-cutaneous syndromesrdquo British Journal of Cancer vol 112no 8 pp 1392ndash1397 2015
[26] H K Ransom ldquoSarcoma of the urachus review of the literaturewith report of an additional caserdquo The American Journal ofSurgery vol 22 no 2 pp 187ndash191 1933
[27] E M L-T Fernandez N H Siverio R L Almaraz L MViota J R Luis and L D Flores ldquoRadical surgery and IVA-chemotherapeutic regimen to treat embryonal rhabdomyosar-coma of the urachus case reportrdquo Pediatric Hematology andOncology vol 24 no 7 pp 543ndash550 2007
[28] M Ishikawa T Nishi R Yamada et al ldquoA case of urachalsarcoma in childhood case report and review of the worldliteraturerdquo Journal of the Japanese Society of Pediatric Surgeonsvol 21 pp 128ndash135 1985
[29] S Yokoyama YHayashida J Nagahama et al ldquoRhabdomyosar-coma of the urachus a case reportrdquo Acta Cytologica vol 41 no4 pp 1293ndash1298 1997
[30] U Schulz and C P OrsquoLeary ldquoSpinal AVM epidermal nevusand rhabdomyosarcoma a rare neurocutaneous syndromerdquoNeurology vol 56 no 3 pp 395ndash397 2001
Case Reports in Genetics 13
[31] A Cheikhelard S Irtan D Orbach et al ldquoUrachal rhab-domyosarcoma in childhood a rare entity with a poor out-comerdquo Journal of Pediatric Surgery vol 50 no 8 pp 1329ndash13332015
[32] K W Gripp E Hopkins K Sol-Church et al ldquoPhenotypicanalysis of individuals with Costello syndrome due to HRASpG13Crdquo American Journal of Medical Genetics Part A vol 155no 4 pp 706ndash716 2011
[33] M Tarnowski G Schneider G Amann et al ldquoRasGRF1 reg-ulates proliferation and metastatic behavior of human alveolarrhabdomyosarcomasrdquo International Journal of Oncology vol 41no 3 pp 995ndash1004 2012
[34] J-S Yu K W Kim H-J Lee Y-J Lee C-S Yoon and M-J Kim ldquoUrachal remnant diseases spectrum of CT and USfindingsrdquo Radiographics vol 21 no 2 pp 451ndash461 2001
[35] C P Kratz S Rapisuwon H Reed H Hasle and P S Rosen-berg ldquoCancer in Noonan Costello cardiofaciocutaneous andLEOPARD syndromesrdquo American Journal of Medical GeneticsPart C Seminars in Medical Genetics vol 157 no 2 pp 83ndash892011
[36] B Kerr M L Mucchielli S Sigaudy et al ldquoIs the locus forCostello syndrome on 11prdquo Journal of Medical Genetics vol 40no 6 pp 469ndash471 2003
[37] TNiihori YAokiNOkamoto et al ldquoHRASmutants identifiedin Costello syndrome patients can induce cellular senescencepossible implications for the pathogenesis of Costello syn-dromerdquo Journal of Human Genetics vol 56 no 10 pp 707ndash7152011
[38] G Rosenberger S Meien and K Kutsche ldquoOncogenic HRASmutations cause prolonged PI3K signaling in response toepidermal growth factor in fibroblasts of patients with costellosyndromerdquo Human Mutation vol 30 no 3 pp 352ndash362 2009
[39] M R DeBaun ldquoScreening for cancer in children with Costellosyndromerdquo American Journal of Medical Genetics vol 108 no1 pp 88ndash90 2002
[40] K W Gripp H Kawame D H Viskochil and L NicholsonldquoElevated catecholamine metabolites in patients with Costellosyndromerdquo American Journal of Medical Genetics vol 128 no1 pp 48ndash51 2004
[41] M-ADelrue B Arveiler andD Lacombe ldquoCostello syndromeclinical features and tumoral riskrdquo Archives de Pediatrie vol 9no 10 pp 1059ndash1063 2002
[42] V Martınez-Gonzalez and P Lapunzina Sındrome de CostelloGrupodeTrabajo sobreCancer en SındromeGeneticos Polimar-formativos (GT-CSGP) httpswwworphanetdatapathoProesCSGP-Costello-3pdf
[43] K A Rauen A Banerjee W R Bishop et al ldquoCostello andcardio-facio-cutaneous syndromes moving toward clinical tri-als in RASopathiesrdquo American Journal of Medical Genetics PartC Seminars inMedical Genetics vol 157 no 2 pp 136ndash146 2011
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Case Reports in Genetics 5
Table1Ch
aracteris
ticso
fpatientsw
ithCostello
synd
romea
ndrhabdo
myosarcom
a
PT number
Author
Year
Cou
ntry
Sex
Age
atdiagno
sis(yearsm
onths)
Symptom
sLo
catio
nHistolog
yMutation
AAC
(NS)
Therapy
Outcome
1Ke
rretal
[78]
1998
England
F2y
4mVo
miting
Con
stipatio
nRe
troperiton
ealleft
psoasm
ayor
muscle
Embryonal
G12S
(34GgtA)lowast
[9]
SCh
TRe
lapsetumor-fr
eeageo
f7years
2Ke
rretal
[78]
1998
England
F3y
2mAb
dominal
mass
Pelvis
urachu
s(m
edianUL)
adherent
tothe
bladder
Embryonal
G12A
(35GgtC)
[5]
SCh
T
Histologyshow
edextend
ingup
tothe
resectionmargin
Diedaged
5years
[59]
3Feingold
[810]
1999
USA
M6m
Tumor
Rightfoo
tAlveolar
NDF
SCh
TTu
mor-fr
eeageo
f20
years[11]
4Bisogn
oetal
[8912]
1999
Italy
M1y
8mCon
stipatio
nAb
dominal
pain
Lower
abdo
men
pelvis
abdo
minal
walllowast
Embryonal
NDF
SCh
TOnlybiop
syDiedaged
2yearsa
nd3mon
ths
5Sigaud
yetal
[813]
2000
France
M6y
NDF
Inguinalscrotal
Embryonal
NDF
NDF
NDF
6Grip
petal
[81415]
2002
USA
M5y
6mAb
dominal
pain
Pelvis
pulm
onary
metastasesw
aspresent
Embryonal
NDF
SCh
TDiedaft
errecurrence
[14]
7Grip
petal
[8]
2002
USA
F3y
7mAb
dominal
pain
Emesis
Upp
erabdo
men
masse
ncasingthe
superio
rmesenteric
anceliaca
rteries
Sing
lepu
lmon
ary
nodu
le
Pleomorph
icNDF
ChT
Diedaged
4years
8Grip
petal
[8]
2002
USA
F2y
6mAb
dominal
mass
Pelvis
bladder
Embryonal
NDF
ChT
RTS
Diedaged
7yearsfor
recurrency
ofRM
Sfib
rosarcom
a[16]
9Grip
petal
[8]
2002
USA
NDF
7mPerin
eal
grow
thPerin
eal
Embryonal
NDF
ChT
RTS
Tumor-fr
eeageo
f2years
10Grip
petal
[8]
2002
USA
NDF
1y11m
Prop
tosis
Leftorbit
Unk
nown
NDF
SRT
Tumor-fr
eeageo
f4years
11Ka
wam
eetal
[17]
2003
Japan
F1y
4mAb
dominal
mass
Pelvis
Spindlec
ell
NDF
SCh
TTu
mor-fr
eeageo
f7years
6 Case Reports in GeneticsTa
ble1Con
tinued
PT number
Author
Year
Cou
ntry
Sex
Age
atdiagno
sis(yearsm
onths)
Symptom
sLo
catio
nHistolog
yMutation
AAC
(NS)
Therapy
Outcome
12Ke
rretal
[18]
2003
UK
M2y
2mLargep
elvic
mass
Retro
vesic
ular
mass
byultrasou
ndEm
bryonal
NDF
ChT
Diedaged
2yearsa
nd4mon
ths
13OrsquoNealetal
[19]
2004
USA
F3y
Right-s
ided
cervicofacial
mass
Parameningeal
infratem
poralfossa
right
perip
arotid
mastic
ator
space
region
Alveolar
NDF
ChTS
RT
Clinicalgrou
p3T2
bN0stage3
Dieddu
ringsurgery
14Grip
p[20]
2005
USA
F3y
2mFacialmass
Rightinfratempo
ral
fossa
Mixed
alveolar
and
embryonal
NDF
ChTS
Dieddu
ringsurgery
byventric
ular
tachycardiafollowed
rapidlyby
lossof
heartrhythm
15Ao
kietal
[2122]
2005
Japan
F7y
2mNDF
NDF
NDF
G12S
(34GgtA)
NDF
NDF
16Grip
petal
[9]
2006
USA
M2y
NDF
NDF
NDF
G12S
(34GgtA)
NDF
Tumor-fr
eeageo
f11
yearslowast
17Ke
rretal[5]
2006
UK
NDF
7mNDF
Metastatic
arising
from
thep
rosta
teEm
bryonal
[23]
G12C
(34GgtT)
NDF
Diedaged
7mon
ths
18Ke
rretal[5]
2006
UK
NDF
NDF
NDF
NDF
NDF
G12S
(34GgtA)
NDF
Diedaged
7years
19Ke
rretal[5]
2006
UK
NDF
NDF
NDF
NDF
NDF
G12A
(35GgtC)
NDF
NDF
20Lo
etal[23]
2008
UK
M2y
3mRe
spira
tory
functio
ndeterio
rated
Rightlun
gNDF
G12S
(34GgtA)
SDiedfewweeks
later
surgery
21Ahm
adiand
Harley[6]
2010
USA
M2y
Increasedwork
ofbreathing
Nasop
haryngeal
Embryonal
NDF
SCh
TRT
Clinicalgrou
pIIA
(T1N
0M0)
Tumor-fr
eeageo
f3years
22Ab
eetal[22]
2012
Japan
NDF
NDF
NDF
NDF
NDF
NDF
NDF
Died
23Menke
etal
[2425]
2015
Germany
F3y
Abdo
minal
mass
Lower
anterio
rabdo
menabo
vethe
urinarybladderlowast
(urachus-m
edianUL
bylocatio
n)
Embryonal
G12C
(34GgtT)
SCh
T
R1resection
(marginaltum
orresid
ue)Tu
mor-fr
eeageo
f6years
24Kr
atze
tal
[25]
2015
Germany
M1y
NDF
NDF
Embryonal
G12S
(34GgtA)
NDF
NDF
25
Sanchez-
Mon
tenegro
etal(this
repo
rt)
2017
Spain
F2y
4mAs
ymptom
atic
LeftmedialU
LEm
bryonal
G12A
(35GgtC)
ChTS
RTTu
mor-fr
eeageo
f4yearsa
nd4mon
ths
26
Sanchez-
Mon
tenegro
etal(this
repo
rt)
2017
Spain
F3y
10m
Asym
ptom
atic
Rightm
edialU
LSpindlec
ell
G12S
(34GgtA)
SCh
TTu
mor-fr
eeageo
f5yearsa
nd4mon
ths
AAC
aminoacid
changeC
hTchemotherapyFfem
aleMm
aleNDFno
datafoun
dNSnu
cleotides
ubstitutio
nPT
patientR
TradiotherapySsurgeryU
Lum
bilicalligam
entlowastPerson
alcommun
icationby
author
Case Reports in Genetics 7
Table 2 Chemotherapy of patients with Costello syndrome and rhabdomyosarcoma
PTnumber Chemotherapy protocol
1Initially with VCR ACD and CTX After debulking continued on ChT using IFOS VCR and ACD After the second coursewhen she developed IFOS induced encephalopathy she was changed back to pulses of VCR ACD and CTX given every 3weeks for 9 courses [7]
2Initially IFOS ACD and VCR After 4 courses CTX was substituted for IFOS because hemorrhagic cystitis Tx complicatedby recurrent episodes of moderately severe diarrhoea and febrile neutropenia requiring readmission to hospital Tx wascompleted after six courses of ChT [7]
3 Tx consisted of below the knee amputation and ChT (DOX ACD VCR and CTX) [10]
4
Tx was implemented according to the Italian protocol for pediatric soft tissue sarcoma Three courses of ChT including VCR(0025mgkg day 1) IFOS (50mgkg days 1 and 2) and alternating ACD (0025mgkg day 1) and DOX (07mgkg day 1) wereadministered Symptoms regressed and the CT scan showed a reduction in tumor volume of more than two-thirds After 3more courses of ChT the patient experienced abdominal pain A repeat abdominal CT scan showed an increase in the pelvicmass Despite the administration of a different ChT with CBDCA (11mgkg day 1) and VP-16 (3mgkg for 3 doses) the tumorcontinued to grow and the child died 7 months after the diagnosis of RMS [12]
5 NDF [13]
6
The first cycle of ChT with VCR ACD and CTX and topotecan reduced the tumor size [16] The tumor was surgicallyremoved after the first ChT [8] Debulking S was required because of rapid growth and tumor necrosis The protocol wascontinued and was deemed sufficiently successful to withhold RT One month after completion of the first protocol tumorrecurrence necessitated a second round of ChT with irinotecan and DOXThe latter drug was administered about 1 weekbefore he died during which time he had tachycardia (heart rate 180ndash20 bpm) [14]
7 The tumor did not respond to ChT and she died shortly after her 4th birthday [8]8 Tx was a combination of S ChT and RT continued until age of 35 years [8]9-10 NDF [8]11 PT had later generalized tonic-clonic seizures during her Tx for RMS [17]12 Despite extensive ChT the tumor progressed rapidly and the PT died 2 months later [18]
13 Induction ChT was commenced with the initial 12-week course of VCR ACD and CTX based on the Intermediate RiskProtocol D9803 of the COG [19]
14 ChT did not result in tumor shrinkage therefore surgical resection was performed [20]15ndash22 NDF [5 6 9 21ndash23]23 ChT according to the cooperative soft tissue sarcoma protocol (CWS-2002 P) was well tolerated by the PT [24]24 NDF [25]
25 ChT in the standard risk group protocol EpSSG RMS 2005 subgroup D 3 preoperative cycles of IFOS (2 doses at 100mgkg)VCR (005mgkg) and ACD (005mgkg)
26 ChT (postoperative 15 days) in the standard risk group protocol EpSSG RMS 2005 subgroup B (Stage I) cycles of IFOS (2doses of 3 gm2d) VCR (15mgm2) and ACD (15mgm2) was initiated
ACD actinomycin D CBDCA carboplatin ChT chemotherapy COG childrenrsquos oncology group CTX cyclophosphamide CT computed tomography CWSCooperative Weichteilsarkom Studie (Cooperative Soft Tissue Sarcoma Study) DOX Doxorubicin EpSSG European pediatric Soft tissue sarcoma StudyGroup IFOS ifosfamide NDF no data found PT patient RMS rhabdomyosarcoma RT radiotherapy S surgery Tx treatment VCR vincristine VP-16etoposide
stimulator (RalGDS) [16 21] in signaling pathways control-ling cell proliferation and differentiation [9]
Themajority of patients with CS had 34GgtA transition incodon 12 (80) [4 16] More than 95 of the mutations arepredicted to result in substitution of the glycine in position12 or 13 of the protein product [1] All individuals withmalignancy had a codon 12 mutation (especially G12A 47patients) [5 21] The rare G12V mutation is associated witha more severe early lethal phenotype some patients diefrom respiratory distress hypertrophic cardiomyopathy ormalignant tachycardia prior to being diagnosed with CS [1]As far as we know no individual with G13C has developed amalignant tumor [4 32]
RMS is the most common soft tissue sarcoma of infancyIts incidence is between 4 and 7 cases per 1 million childrenyounger than 15 years [8 12] The age peak is between 2 and5 years with a slight male predominance (12ndash141) Thesetumors may arise anywhere in the body and fewer than 20are located in the pelvis [12]Most RMS tumors are originatedin the head and neck region urogenital tract and extremities[33] The most common histologic type seen in gt50 isembryonal followed by alveolar in 20ndash30 PleomorphicRMS is rare (1) and has a poor prognosis [8] AlveolarRMS is characterized by the translocation t(213)(q35q14) in70 of cases and the variant translocation t(113)(p36q14)in a smaller percentage of cases Evidence accumulates
8 Case Reports in Genetics
Table3Ch
aracteris
ticso
fPediatricPatie
ntsw
ithUmbilicalLigamentR
habd
omyosarcom
a
PT number
Author
Year
Cou
ntry
Sex
Age
atdiagno
sis(yearsm
onths)
Symptom
sLo
catio
nSize
(cm)
Histology
IRS
grou
pTh
erapy
Outcome
1Ra
nsom
[2627]
1933
USA
F4m
Massb
elowthe
umbilicus
and
extend
ing
somew
hattothe
right
Urachus
(medianUL)
attached
alon
gthea
nterior
wallfrom
theu
mbilicus
tothea
pexof
theb
ladd
er
115
Spindle
cell
ISM
AC
RT
Lastcheck-up
exam
ination(2
years)
show
edno
evidence
ofrecurrence
2Ishikawae
tal[28]
1985
Japan
F1y
4mAb
dominalmass
abdo
minalpain
hemop
erito
neum
Urachal(m
edianUL)
intra-abdo
minalruptureo
fthetum
or
Fist-
sized
NDF
IVSM
ACNDF
3Yo
koyamae
tal[2729]
1997
Japan
M2y
Episo
diclow
erabdo
minalpain
Urachus
(medianUL)
extraperito
neallocated
betweentheu
mbilicus
and
apex
oftheb
ladd
erandwas
adherin
gtig
htlyto
both
Theb
ilateralm
edialU
Lweres
eenenterin
gthe
tumorR
upturedwith
asm
alln
umbero
fdissem
inated
tumors
scatteredon
them
esentery
andDou
glas
pouch
12Em
bryonal
IVSM
AI
ChT
At2yearso
ffollo
w-upno
recurrence
hadbeen
detected
4lowastKe
rretal
[78]
1998
England
F3y
2mAb
dominalmass
Urachus
(medianUL)
adherent
totheb
ladd
erNDF
Embryonal
IIaSM
II
ChT
Histologyshow
edextend
ingup
tothe
resectionmargin
Diedaged
5years
[59]
5Schu
lzand
OrsquoLeary
[2730]
2001
Scotland
M2y
NDF
Urachus
(medianUL)
NDF
Embryonal
NDF
SCh
TRT
Tumor-fr
eeageo
f26
years
6Fernandeze
tal[27]
2007
Spain
F6y
Intractable
constip
ation
nauseaabd
ominal
painles
smass
Urachus
(medianUL)
infiltratingthev
entral
abdo
minalwalland
fixed
tothev
esicaldo
me
135
Embryonal
IbSM
IC
ChT
At4yearso
ffollo
w-upthep
atient
remains
welland
free
ofclinicald
isease
7lowastMenke
etal
[2425]
2015
Germany
F3y
Abdo
minalmass
Lower
anterio
rabd
omen
abovethe
urinarybladderamp
(urachusm
edianULby
locatio
n)
NDF
Embryonal
IIaSM
II
ChT
R1resection
(marginaltum
orresid
ue)Tu
mor-fr
eeageo
f6years
8Ch
eikh
elard
etal[31]
2015
Dx
1983
France
F5y
5mNDF
Urachus
(medianUL)
periton
ealm
etastasesa
ndhypo
gastric
lymph
nodes
5NDF
IVSM
AI
ChT
Died31
mon
thsa
fter
diagno
siswith
relap
sein
periton
ealliver
at11mon
ths
Case Reports in Genetics 9
Table3Con
tinued
PT number
Author
Year
Cou
ntry
Sex
Age
atdiagno
sis(yearsm
onths)
Symptom
sLo
catio
nSize
(cm)
Histology
IRS
grou
pTh
erapy
Outcome
9Ch
eikh
elard
etal[31]
2015
Dx
2003
France
F3y
3mPeriton
ealrup
ture
poor
generalstatus
Urachus
(medianUL)
lumbo
aorticandexternal
iliac
lymph
nodes
10Alveolar
IVSM
AI
ChTRT
Died57
mon
thsa
fter
diagno
siswith
relap
sein
periton
ealliver
at30
mon
ths
10Ch
eikh
elard
etal[31]
2015
Dx
2005
France
F2y
6mMasspo
orgeneral
statusdysuria
Urachus
(medianUL)
15Em
bryonal
III
SMII
ChTRT
Died37
mon
thsa
fter
diagno
siswith
periton
ealrelapse
at19
mon
ths
11Ch
eikh
elard
etal[31]
2015
Dx
2005
France
M4y
2mMasspo
orgeneral
statusdysuria
Urachus
(medianUL)
periton
ealm
etastasesa
ndiliac
lumbo
aorticlymph
nodes
10Em
bryonal
IVSM
II
ChTRT
Relapsed
multifocalat
82mon
thsfollo
w-up
100mon
ths
12Ch
eikh
elard
etal[31]
2015
Dx
2005
France
M5y
3mMasspo
orgeneral
status
Urachus
(medianUL)
periton
ealm
etastasesa
ndmesenteric
lymph
nodes
106
Embryonal
IVSM
IC
ChTRT
Tumor
freea
fter9
5mon
thssince
diagno
sis
13Ch
eikh
elard
etal[31]
2015
Dx
2006
France
M2y
5mMasspo
orgeneral
statusob
structiv
erenalinsuffi
ciency
Urachus
(medianUL)
periton
ealbon
emetastases
andhypo
gastric
lymph
nodes
21Em
bryonal
IVSM
II
ChTRT
Bone
progression
after
16mon
thsdied
18aft
erdiagno
sis
14Ch
eikh
elard
etal[31]
2015
Dx
2010
France
M4y
5mAb
dominalpain
Urachus
(medianUL)
7Em
bryonal
III
SMIC
ChT
Tumor
freea
fter18
mon
thssince
diagno
sis
15Ch
eikh
elard
etal[31]
2015
Dx
2010
France
M6y
Abdo
minalpain
Urachus
(medianUL)
periton
ealm
etastases
14Em
bryonal
IVSM
AI
ChTRT
Tumor
freea
fter4
5mon
thssince
diagno
sis
16lowast
Sanchez-
Mon
tenegro
etal(this
repo
rt)
2017
Dx
2015
Spain
F2y
4mAs
ymptom
atic
LeftmedialU
L5
Embryonal
IaCh
TSM
IC
RT
Tumor-fr
eeageo
f3yearsa
nd9mon
ths
17lowast
Sanchez-
Mon
tenegro
etal(this
repo
rt)
2017
Dx
2015
Spain
F3y
10m
Asym
ptom
atic
Rightm
edialU
L85
Spindle
cell
IIaSM
II
ChT
Tumor-fr
eeageo
f4yearsa
nd5mon
ths
ChT
chem
otherapyD
xdiagno
sed
Ffemale
IRS
intergroup
rhabdo
myosarcom
aMm
ale
NDF
nodata
foun
dRT
radiotherapy
Ssurgery
SMAIsurgerymacroscop
ically
incomplete
SMAC
surgery
macroscop
icallycompleteSM
ICsurgery
microscop
icallycompleteSM
IIsurgery
microscop
icallyincompleteULum
bilicalligam
ent
ampPerson
alcommun
icationby
authorlowast
Patientsw
ithCostello
synd
rome
10 Case Reports in Genetics
Table 4 Chemotherapy of pediatric patients with umbilical ligament rhabdomyosarcoma
PTnumber Chemotherapy protocol
1-2 No ChT [26 28]3 After establishment of the final diagnosis he was treated with combined ChT including VCR ACD and CTX [29]
4lowastInitially IFOS ACD and VCR After 4 courses CTX was substituted for IFOS because of hemorrhagic cystitis Tx complicatedby recurrent episodes of moderately severe diarrhoea and febrile neutropenia requiring readmission to hospital Tx wascompleted after six courses of ChT [7]
5 NDF [30]
6 PT started induction of ChT 2 weeks after S Induction regimen included 9 cycles of IVA (IFOS VCR and ACD) that were welltolerated with minimal systemic complications (Tx 953 of the MMT 95 SIOP protocol for RMS) [27]
7lowast ChT according to the cooperative soft tissue sarcoma protocol (CWS-2002 P) was well tolerated by the PT [24]8 Adjuvant ChT with 10 cycles of IFOS VCR and ACD [31]9 Adjuvant ChT with 6 cycles of IFOS VCR and VP-16 and 9 cycles of VCR ACD CTXACD and CTX [31]10 Neoadjuvant ChT with 6 cycles of IFOS VCR and ACD and adjuvant ChT with 3 cycles of IFOS VCR and ACD [31]
11 Neoadjuvant ChT with 1 cycle of CTX VCR and PRED 2 cycles IFOS VCR and ACD and 4 cycles of IFOS VCR ACD andDOX and adjuvant ChT with 3 cycles of IFOS VCR and ACD [31]
12 Neoadjuvant ChT with 1 cycle of CTX VCR and PRED and 5 cycles of IFOS VCR ACD and DOX and adjuvant ChT with 2cycles of IFOS VCR ACD and DOX and 1 cycle of IFOS VCR and ACD [31]
13 Neoadjuvant ChT with 2 cycles of VCR ACD and CTX + and 3 cycles of IFOS VCR ACD and DOX and adjuvant ChT with 3cycles of IFOS VCR and ACD [31]
14 Neoadjuvant ChT with 4 cycles of IFOS VCR ACD and DOX and adjuvant ChT with 5 cycles of IFOS VCR ACD [31]
15 Neoadjuvant ChT with 4 cycles of IFOS VCR ACD DOX 3 cycles of IFOS VCR ACD and adjuvant ChT with 1 cycle of IFOSVCR ACD 1 cycle of IFOS VCR [31]
16lowastChT in the standard risk group protocol EpSSG RMS 2005 subgroup D 3 preoperative cycles of IFOS (2 doses at 100mgkg)VCR (005mgkg) and ACD (005mgkg)
17lowastChT (postoperative 15 days) in the standard risk group protocol EpSSG RMS 2005 subgroup B (Stage I) cycles of IFOS (2 dosesof 3 gm2d) VCR (15mgm2) and ACD (15mgm2) was initiated
ACD actinomycin D ChT chemotherapy CTX cyclophosphamide CWS Cooperative Weichteilsarkom Studie (Cooperative Soft Tissue Sarcoma Study)DOX Doxorubicin EpSSG European pediatric Soft tissue sarcoma Study Group IFOS ifosfamide MMT malignant mesenchymal tumor NDF no datafound PRED prednisone PT patient RMS rhabdomyosarcoma S surgery SIOP Societe Internationale DrsquoOncologie Pediatrique (International Society ofPediatric Oncology) Tx treatment VCR vincristine VP-16 etoposide lowastPatients with Costello syndrome
that alveolar RMS and embryonal RMS are two differentdisorders while alveolar RMS may originate from primitiveuncommitted mesodermal cells embryonal RMS originatesprobably from more differentiated myoblasts Ras protein-specific guanine nucleotide-releasing factor 1 (RasGRF1)plays an important role in alveolar RMS pathogenesis Theseinteresting concepts however need more evidence [33]
The umbilicus caudally originates the common ligamentwhich is divided into obliterated umbilical arteries (medialUL) and urachus (median UL) The urachus varies from3 to 10 cm in length and from 8 to 10mm in diameterIt is a three-layered tubular structure the innermost layerbeing lined with transitional epithelium in 70 of casesand with columnar epithelium in 30 The structure issurrounded by connective tissue and outermost muscularlayer in continuity with the detrusor muscle Along its pathfrom the bladder to the umbilicus the urachus lies betweenthe transverse fascia and the parietal peritoneum containedin the pyramidal retropubic perivesical preperitoneal spacecompartmentalized by umbilicovesical fascia along with themedial umbilical ligaments and the bladder Occasionallythe urachus may merge with one or both of the obliteratedumbilical arteries (medial UL) and there may be a slight
deviation to the right or left of the midline [34] The urachusis an embryological remnant resulting from the obliterationof the allantoic channel which attaches the bladder dome tothe umbilicus [31]
Urachal malignant tumors are extremely rare represent-ing less than 05 of all bladder cancers and 001 of alltumors They may arise from any portion of the urachus andare most commonly found in adults and males (60ndash70)Although sarcomas represent only 8 they are the mostfrequent urachal neoplasms reported in patients youngerthan 20 years of age (67) [27] Poor prognosis is a commonfeature in adults and pediatric urachalmalignancies with 50to 60 of 5-year survival In contrast the 5-year event-freesurvival in pelvic RMS was reported to be about 51 [31]
This indolent and rather large urachal tumor was mostlyrevealed by an uncomplicated progressing mass withoutprodromic urological symptomsThedelay of diagnosis couldbe explained by a long asymptomatic progression of thetumor in a preperitoneal location which allows an importantlocal spreading before diagnosis Even in patients withouttumor rupture peritoneal involvement appeared to be the keypoint in the prognosis of urachal RMS Systematic cytologyat diagnosis could be more accurate to evaluate peritoneal
Case Reports in Genetics 11
extension in order to avoid understaging and adjust adjuvantlocoregional treatment [31]
Previously only 12 patients with RMS arising from theurachus (median UL) in children without CS have beenreported in the English literature (Table 3) By 2011 therewere29 reported cases of cancer in patients withCS 19 RMS (meanage of 23 years 9 embryonal 1 alveolar 1 mixed histology1 pleomorphic 1 spindle cell type and 6 unclassified) 5neuroblastomas 4 bladder cancer and 1 fibrosarcoma [35]
Loss of heterozygosity for 11p155 in RMS from individu-als with CS suggests that loss of the wild-type allele is the sec-ond hit in tumor development [6 16 36] Whereas theHRASmutation in a sporadic malignancy in the general populationis present only within the tumor cells in CS an identicalmutation is present in every single cell of the individualthus accounting for the tumor predisposition [1] implicatingan alternate mechanism of rhabdomyosarcogenesis [16] Inaddition one patient with CS and uniparental trisomy dueto triplication of the mutated paternal HRAS gene was alsoreported RMS typically displays loss of heterozygosity ofthe 11p155 region because of paternal uniparental disomyand approximately 28 of cases harbor mutations in genesof growth signaling pathways In reports of uniparentaldisomy plus HRAS mutation the latter was heterozygousand therefore must have occurred after the developmentof uniparental disomy [24] The functional analysis alsorevealed that CS-causing mutant HRAS proteins causedoncogene-induced senescence in human fibroblasts [37]Theimportant role of PI3K-protein-kinase B (AKT) signalingin Ras-mediated transformation and tumorigenesis is high-lighted by constitutive AKT activation in RMS cell lines andclinical samples Thus prolonged PI3K-AKT signaling mightalso be implicated in the development of soft tissue sarcomain patients with CS [38]
Only four out of 11 patients were diagnosed with CS priorto the RMS diagnosis in 5 patients CS was diagnosed afterthe RMS and in the remaining 2 the order was unknown[20] In 2003 a further three unpublished cases of RMS inchildren with CS were known through the International CSSupport Group [18] and for that reason there is possiblyunderdiagnosis of RMS in patients with CS
A screening protocol was proposed consisting of ultra-sound examination of the abdomen and pelvis every 3ndash6 months until age of 8ndash10 years for RMS and abdomi-nal neuroblastoma urine catecholamine metabolite analysisevery 6ndash12 months until age of 5 years for neuroblastomaand urinalysis for hematuria annually for bladder carcinomaafter age of 10 years The prior diagnosis of CS was theprerequisite for the implementation of a tumor screeningprotocol [8] The recommendation based on the presumedfast doubling time of RMS was abdominal sonographyscreening for RMS that should be done in similar intervalsof every four months until stronger evidence would suggestotherwise [39] Screening for neuroblastoma is no longerrecommended becausemany CS patients without identifiabletumor show elevated catecholamine metabolites in urine itappears that in this patient group an elevation above thenormal limit defined as 2 standard deviations (SD) above themean for age is more likely to be a variant rather than a sign
of a neuroblastoma [1 40] A French monitoring protocolproposed the determination of catecholamines and theirmetabolites in urine every six months until the age of 5 yearsand ultrasound abdominopelvic every six months until theend of the puberty seeking hematuria dipstick from6monthsto the age of 10 [41] The protocol in our hospital for patientswith CS includes an abdominal and pelvic ultrasound 3times during the first year of life and in childhood every 6months until age of 10 [42] We believe that the best optionis to perform a pelvic abdominal ultrasound every 3 monthsduring the first eight years of life and then controls accordingto medical criteria This is even more necessary in patientswith possible UL RMS because diagnosis was usually done inadvanced stages with a poor survival It is possible that withclose monitoring after an early diagnosis will detect initialstages of the tumor in previously not described locations
Head and neck MRI scans can be performed less fre-quently Ear examination and tympanometry every 4 to 6months to detect middle ear effusion which would raisesuspicion for a nasopharyngeal mass are also recommended[6]
The outcome of CS patients with RMS has been compa-rable to that for patients without the syndrome with a 5-yearsurvival rate of 65 to 70 [19] but according to this reviewit could be worse than the general population Neoplasia wasnoted at the cause of death in five (22) patients with CS[4 15] but in our study the mortality associated with RMSwas 43 Because the long-term survival in RMS is basedon the histology of the tumor and the extent of disease atdiagnosis early diagnosis may alter the treatment regimenand improve prognosis This could be particularly importantin patients with CS who often are medically fragile [20]
The RasMAPK pathway is an attractive target in thetreatment of cancer utilizing small molecule therapeuticsthat specifically inhibits the pathway Ras pathway agentssuch as farnesyltransferase inhibitors (tipifarnib and lona-farnib) that prevent posttranslational modification of Rasare being evaluated for cancer treatment and may be oftherapeutic use for syndromes in this pathway especially CSIn addition B-Raf protooncogene serinethreonine kinase(BRAF) and mitogenextracellular signal-regulated kinase(MEK) inhibitors offer the same potential in the possibletreatment of CS Since the RasMAPK pathway has targets forinhibition in cancer treatment there aremany smallmoleculetherapeutics that are in development or undergoing clinicaltrials with some already FDA approval [43]
6 ConclusionsCS is a syndrome poorly known in oncology but theirpredisposition tomalignancies includingULRMS implies theneed for a new perspective on early diagnosis and aggressivemedical and surgical treatment
ConsentInformed consent was obtained from the new two individualparticipants included in the study and has been properlydocumented with the parental approval to the use of patientrsquosimages and complementary studies
12 Case Reports in Genetics
Competing Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
Special thanks are due to Israel Fernandez Pineda MDAssistantMember and Surgery Fellowship ProgramDirectorSt Jude Childrenrsquos Research Hospital (Memphis TN) for therecommendations and corrections to the manuscript
References
[1] E Quezada and K W Gripp ldquoCostello syndrome and relateddisordersrdquo Current Opinion in Pediatrics vol 19 no 6 pp 636ndash644 2007
[2] JM Costello ldquoA new syndromerdquoNewZealandMedical Journalvol 74 article 397 1971
[3] JMCostello ldquoAnew syndromemental subnormality andnasalpapillomatardquo Australian Paediatric Journal vol 13 no 2 pp114ndash118 1977
[4] K W Gripp and A E Lin ldquoCostello syndrome a Rasmitogenactivated protein kinase pathway syndrome (rasopathy) result-ing from HRAS germline mutationsrdquo Genetics in Medicine vol14 no 3 pp 285ndash292 2012
[5] B Kerr M-A Delrue S Sigaudy et al ldquoGenotype-phenotypecorrelation in Costello syndrome HRAS mutation analysis in43 casesrdquo Journal of Medical Genetics vol 43 no 5 pp 401ndash4052006
[6] N Ahmadi and E Harley ldquoCostello syndrome and the impor-tance of cancer screeningrdquo Archives of OtolaryngologymdashHeadand Neck Surgery vol 136 no 10 pp 1028ndash1029 2010
[7] B Kerr O B Eden R Dandamudi et al ldquoCostello syndrometwo cases with embryonal rhabdomyosarcomardquo Journal ofMedical Genetics vol 35 no 12 pp 1036ndash1039 1998
[8] K W Gripp C I Scott Jr L Nicholson et al ldquoFive additionalCostello syndrome patients with rhabdomyosarcoma proposalfor a tumor screening protocolrdquo American Journal of MedicalGenetics vol 108 no 1 pp 80ndash87 2002
[9] K W Gripp A E Lin D L Stabley et al ldquoHRAS mutationanalysis in Costello syndrome genotype and phenotype corre-lationrdquo American Journal of Medical Genetics Part A vol 140no 1 pp 1ndash7 2006
[10] M Feingold ldquoCostello syndrome and rhabdomyosarcomardquoJournal of Medical Genetics vol 36 no 7 pp 582ndash583 1999
[11] S M White J M Graham Jr B Kerr et al ldquoThe adultphenotype in Costello syndromerdquo American Journal of MedicalGenetics A vol 136 no 2 pp 128ndash135 2005
[12] G Bisogno A Murgia I Mammi M S Strafella and M CarlildquoRhabdomyosarcoma in a patient with cardio-facio-cutaneoussyndromerdquo Journal of Pediatric HematologyOncology vol 21no 5 pp 424ndash427 1999
[13] S Sigaudy G Vittu A David et al ldquoCostello syndrome reportof six patients including one with an embryonal rhabdomyosar-comardquoEuropean Journal of Pediatrics vol 159 no 3 pp 139ndash1422000
[14] A Hinek M A Teitell L Schoyer et al ldquoMyocardial storage ofchondroitin sulfate-containing moieties in Costello syndromepatients with severe hypertrophic cardiomyopathyrdquo AmericanJournal of Medical Genetics vol 133 no 1 pp 1ndash12 2005
[15] A E Lin P D Grossfeld R M Hamilton et al ldquoFurtherdelineation of cardiac abnormalities in Costello syndromerdquoAmerican Journal of Medical Genetics vol 111 no 2 pp 115ndash1292002
[16] A L Estep W E Tidyman M A Teitell P D Cotter and KA Rauen ldquoHRASmutations in Costello syndrome detection ofconstitutional activating mutations in codon 12 and 13 and lossof wild-type allele in malignancyrdquo American Journal of MedicalGenetics vol 140 no 1 pp 8ndash16 2006
[17] H KawameMMatsui K Kurosawa et al ldquoFurther delineationof the behavioral and neurologic features inCostello syndromerdquoAmerican Journal of Medical Genetics vol 118A no 1 pp 8ndash142003
[18] B Kerr M A Einaudi P Clayton et al ldquoIs growth hormonetreatment beneficial or harmful in Costello syndromerdquo Journalof medical genetics vol 40 no 6 article e74 2003
[19] J P OrsquoNeal J Ramdas W E Wood and P K PellitterildquoParameningeal rhabdomyosarcoma in a patient with Costellosyndromerdquo Journal of Pediatric HematologyOncology vol 26no 6 pp 389ndash392 2004
[20] K W Gripp ldquoTumor predisposition in Costello syndromerdquoAmerican Journal of Medical Genetics Part C Seminars inMedical Genetics vol 137C no 1 pp 72ndash77 2005
[21] Y Aoki T Niihori H Kawame et al ldquoGermline mutationsin HRAS proto-oncogene cause Costello syndromerdquo NatureGenetics vol 37 no 10 pp 1038ndash1040 2005
[22] Y Abe Y Aoki S Kuriyama et al ldquoPrevalence and clinicalfeatures of Costello syndrome and cardio-facio-cutaneous syn-drome in Japan findings from a nationwide epidemiologicalsurveyrdquo American Journal of Medical Genetics Part A vol 158no 5 pp 1083ndash1094 2012
[23] I F M Lo C Brewer N Shannon et al ldquoSevere neonatal man-ifestations of Costello syndromerdquo Journal of Medical Geneticsvol 45 no 3 pp 167ndash171 2008
[24] J Menke S Pauli M Sigler et al ldquoUniparental trisomy of amutated HRASproto-oncogene in embryonal rhabdomyosar-coma of a patient with costello syndromerdquo Journal of ClinicalOncology vol 33 no 13 pp e62ndashe65 2015
[25] C P Kratz L Franke H Peters et al ldquoCancer spectrum andfrequency among children with Noonan Costello and cardio-facio-cutaneous syndromesrdquo British Journal of Cancer vol 112no 8 pp 1392ndash1397 2015
[26] H K Ransom ldquoSarcoma of the urachus review of the literaturewith report of an additional caserdquo The American Journal ofSurgery vol 22 no 2 pp 187ndash191 1933
[27] E M L-T Fernandez N H Siverio R L Almaraz L MViota J R Luis and L D Flores ldquoRadical surgery and IVA-chemotherapeutic regimen to treat embryonal rhabdomyosar-coma of the urachus case reportrdquo Pediatric Hematology andOncology vol 24 no 7 pp 543ndash550 2007
[28] M Ishikawa T Nishi R Yamada et al ldquoA case of urachalsarcoma in childhood case report and review of the worldliteraturerdquo Journal of the Japanese Society of Pediatric Surgeonsvol 21 pp 128ndash135 1985
[29] S Yokoyama YHayashida J Nagahama et al ldquoRhabdomyosar-coma of the urachus a case reportrdquo Acta Cytologica vol 41 no4 pp 1293ndash1298 1997
[30] U Schulz and C P OrsquoLeary ldquoSpinal AVM epidermal nevusand rhabdomyosarcoma a rare neurocutaneous syndromerdquoNeurology vol 56 no 3 pp 395ndash397 2001
Case Reports in Genetics 13
[31] A Cheikhelard S Irtan D Orbach et al ldquoUrachal rhab-domyosarcoma in childhood a rare entity with a poor out-comerdquo Journal of Pediatric Surgery vol 50 no 8 pp 1329ndash13332015
[32] K W Gripp E Hopkins K Sol-Church et al ldquoPhenotypicanalysis of individuals with Costello syndrome due to HRASpG13Crdquo American Journal of Medical Genetics Part A vol 155no 4 pp 706ndash716 2011
[33] M Tarnowski G Schneider G Amann et al ldquoRasGRF1 reg-ulates proliferation and metastatic behavior of human alveolarrhabdomyosarcomasrdquo International Journal of Oncology vol 41no 3 pp 995ndash1004 2012
[34] J-S Yu K W Kim H-J Lee Y-J Lee C-S Yoon and M-J Kim ldquoUrachal remnant diseases spectrum of CT and USfindingsrdquo Radiographics vol 21 no 2 pp 451ndash461 2001
[35] C P Kratz S Rapisuwon H Reed H Hasle and P S Rosen-berg ldquoCancer in Noonan Costello cardiofaciocutaneous andLEOPARD syndromesrdquo American Journal of Medical GeneticsPart C Seminars in Medical Genetics vol 157 no 2 pp 83ndash892011
[36] B Kerr M L Mucchielli S Sigaudy et al ldquoIs the locus forCostello syndrome on 11prdquo Journal of Medical Genetics vol 40no 6 pp 469ndash471 2003
[37] TNiihori YAokiNOkamoto et al ldquoHRASmutants identifiedin Costello syndrome patients can induce cellular senescencepossible implications for the pathogenesis of Costello syn-dromerdquo Journal of Human Genetics vol 56 no 10 pp 707ndash7152011
[38] G Rosenberger S Meien and K Kutsche ldquoOncogenic HRASmutations cause prolonged PI3K signaling in response toepidermal growth factor in fibroblasts of patients with costellosyndromerdquo Human Mutation vol 30 no 3 pp 352ndash362 2009
[39] M R DeBaun ldquoScreening for cancer in children with Costellosyndromerdquo American Journal of Medical Genetics vol 108 no1 pp 88ndash90 2002
[40] K W Gripp H Kawame D H Viskochil and L NicholsonldquoElevated catecholamine metabolites in patients with Costellosyndromerdquo American Journal of Medical Genetics vol 128 no1 pp 48ndash51 2004
[41] M-ADelrue B Arveiler andD Lacombe ldquoCostello syndromeclinical features and tumoral riskrdquo Archives de Pediatrie vol 9no 10 pp 1059ndash1063 2002
[42] V Martınez-Gonzalez and P Lapunzina Sındrome de CostelloGrupodeTrabajo sobreCancer en SındromeGeneticos Polimar-formativos (GT-CSGP) httpswwworphanetdatapathoProesCSGP-Costello-3pdf
[43] K A Rauen A Banerjee W R Bishop et al ldquoCostello andcardio-facio-cutaneous syndromes moving toward clinical tri-als in RASopathiesrdquo American Journal of Medical Genetics PartC Seminars inMedical Genetics vol 157 no 2 pp 136ndash146 2011
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

6 Case Reports in GeneticsTa
ble1Con
tinued
PT number
Author
Year
Cou
ntry
Sex
Age
atdiagno
sis(yearsm
onths)
Symptom
sLo
catio
nHistolog
yMutation
AAC
(NS)
Therapy
Outcome
12Ke
rretal
[18]
2003
UK
M2y
2mLargep
elvic
mass
Retro
vesic
ular
mass
byultrasou
ndEm
bryonal
NDF
ChT
Diedaged
2yearsa
nd4mon
ths
13OrsquoNealetal
[19]
2004
USA
F3y
Right-s
ided
cervicofacial
mass
Parameningeal
infratem
poralfossa
right
perip
arotid
mastic
ator
space
region
Alveolar
NDF
ChTS
RT
Clinicalgrou
p3T2
bN0stage3
Dieddu
ringsurgery
14Grip
p[20]
2005
USA
F3y
2mFacialmass
Rightinfratempo
ral
fossa
Mixed
alveolar
and
embryonal
NDF
ChTS
Dieddu
ringsurgery
byventric
ular
tachycardiafollowed
rapidlyby
lossof
heartrhythm
15Ao
kietal
[2122]
2005
Japan
F7y
2mNDF
NDF
NDF
G12S
(34GgtA)
NDF
NDF
16Grip
petal
[9]
2006
USA
M2y
NDF
NDF
NDF
G12S
(34GgtA)
NDF
Tumor-fr
eeageo
f11
yearslowast
17Ke
rretal[5]
2006
UK
NDF
7mNDF
Metastatic
arising
from
thep
rosta
teEm
bryonal
[23]
G12C
(34GgtT)
NDF
Diedaged
7mon
ths
18Ke
rretal[5]
2006
UK
NDF
NDF
NDF
NDF
NDF
G12S
(34GgtA)
NDF
Diedaged
7years
19Ke
rretal[5]
2006
UK
NDF
NDF
NDF
NDF
NDF
G12A
(35GgtC)
NDF
NDF
20Lo
etal[23]
2008
UK
M2y
3mRe
spira
tory
functio
ndeterio
rated
Rightlun
gNDF
G12S
(34GgtA)
SDiedfewweeks
later
surgery
21Ahm
adiand
Harley[6]
2010
USA
M2y
Increasedwork
ofbreathing
Nasop
haryngeal
Embryonal
NDF
SCh
TRT
Clinicalgrou
pIIA
(T1N
0M0)
Tumor-fr
eeageo
f3years
22Ab
eetal[22]
2012
Japan
NDF
NDF
NDF
NDF
NDF
NDF
NDF
Died
23Menke
etal
[2425]
2015
Germany
F3y
Abdo
minal
mass
Lower
anterio
rabdo
menabo
vethe
urinarybladderlowast
(urachus-m
edianUL
bylocatio
n)
Embryonal
G12C
(34GgtT)
SCh
T
R1resection
(marginaltum
orresid
ue)Tu
mor-fr
eeageo
f6years
24Kr
atze
tal
[25]
2015
Germany
M1y
NDF
NDF
Embryonal
G12S
(34GgtA)
NDF
NDF
25
Sanchez-
Mon
tenegro
etal(this
repo
rt)
2017
Spain
F2y
4mAs
ymptom
atic
LeftmedialU
LEm
bryonal
G12A
(35GgtC)
ChTS
RTTu
mor-fr
eeageo
f4yearsa
nd4mon
ths
26
Sanchez-
Mon
tenegro
etal(this
repo
rt)
2017
Spain
F3y
10m
Asym
ptom
atic
Rightm
edialU
LSpindlec
ell
G12S
(34GgtA)
SCh
TTu
mor-fr
eeageo
f5yearsa
nd4mon
ths
AAC
aminoacid
changeC
hTchemotherapyFfem
aleMm
aleNDFno
datafoun
dNSnu
cleotides
ubstitutio
nPT
patientR
TradiotherapySsurgeryU
Lum
bilicalligam
entlowastPerson
alcommun
icationby
author
Case Reports in Genetics 7
Table 2 Chemotherapy of patients with Costello syndrome and rhabdomyosarcoma
PTnumber Chemotherapy protocol
1Initially with VCR ACD and CTX After debulking continued on ChT using IFOS VCR and ACD After the second coursewhen she developed IFOS induced encephalopathy she was changed back to pulses of VCR ACD and CTX given every 3weeks for 9 courses [7]
2Initially IFOS ACD and VCR After 4 courses CTX was substituted for IFOS because hemorrhagic cystitis Tx complicatedby recurrent episodes of moderately severe diarrhoea and febrile neutropenia requiring readmission to hospital Tx wascompleted after six courses of ChT [7]
3 Tx consisted of below the knee amputation and ChT (DOX ACD VCR and CTX) [10]
4
Tx was implemented according to the Italian protocol for pediatric soft tissue sarcoma Three courses of ChT including VCR(0025mgkg day 1) IFOS (50mgkg days 1 and 2) and alternating ACD (0025mgkg day 1) and DOX (07mgkg day 1) wereadministered Symptoms regressed and the CT scan showed a reduction in tumor volume of more than two-thirds After 3more courses of ChT the patient experienced abdominal pain A repeat abdominal CT scan showed an increase in the pelvicmass Despite the administration of a different ChT with CBDCA (11mgkg day 1) and VP-16 (3mgkg for 3 doses) the tumorcontinued to grow and the child died 7 months after the diagnosis of RMS [12]
5 NDF [13]
6
The first cycle of ChT with VCR ACD and CTX and topotecan reduced the tumor size [16] The tumor was surgicallyremoved after the first ChT [8] Debulking S was required because of rapid growth and tumor necrosis The protocol wascontinued and was deemed sufficiently successful to withhold RT One month after completion of the first protocol tumorrecurrence necessitated a second round of ChT with irinotecan and DOXThe latter drug was administered about 1 weekbefore he died during which time he had tachycardia (heart rate 180ndash20 bpm) [14]
7 The tumor did not respond to ChT and she died shortly after her 4th birthday [8]8 Tx was a combination of S ChT and RT continued until age of 35 years [8]9-10 NDF [8]11 PT had later generalized tonic-clonic seizures during her Tx for RMS [17]12 Despite extensive ChT the tumor progressed rapidly and the PT died 2 months later [18]
13 Induction ChT was commenced with the initial 12-week course of VCR ACD and CTX based on the Intermediate RiskProtocol D9803 of the COG [19]
14 ChT did not result in tumor shrinkage therefore surgical resection was performed [20]15ndash22 NDF [5 6 9 21ndash23]23 ChT according to the cooperative soft tissue sarcoma protocol (CWS-2002 P) was well tolerated by the PT [24]24 NDF [25]
25 ChT in the standard risk group protocol EpSSG RMS 2005 subgroup D 3 preoperative cycles of IFOS (2 doses at 100mgkg)VCR (005mgkg) and ACD (005mgkg)
26 ChT (postoperative 15 days) in the standard risk group protocol EpSSG RMS 2005 subgroup B (Stage I) cycles of IFOS (2doses of 3 gm2d) VCR (15mgm2) and ACD (15mgm2) was initiated
ACD actinomycin D CBDCA carboplatin ChT chemotherapy COG childrenrsquos oncology group CTX cyclophosphamide CT computed tomography CWSCooperative Weichteilsarkom Studie (Cooperative Soft Tissue Sarcoma Study) DOX Doxorubicin EpSSG European pediatric Soft tissue sarcoma StudyGroup IFOS ifosfamide NDF no data found PT patient RMS rhabdomyosarcoma RT radiotherapy S surgery Tx treatment VCR vincristine VP-16etoposide
stimulator (RalGDS) [16 21] in signaling pathways control-ling cell proliferation and differentiation [9]
Themajority of patients with CS had 34GgtA transition incodon 12 (80) [4 16] More than 95 of the mutations arepredicted to result in substitution of the glycine in position12 or 13 of the protein product [1] All individuals withmalignancy had a codon 12 mutation (especially G12A 47patients) [5 21] The rare G12V mutation is associated witha more severe early lethal phenotype some patients diefrom respiratory distress hypertrophic cardiomyopathy ormalignant tachycardia prior to being diagnosed with CS [1]As far as we know no individual with G13C has developed amalignant tumor [4 32]
RMS is the most common soft tissue sarcoma of infancyIts incidence is between 4 and 7 cases per 1 million childrenyounger than 15 years [8 12] The age peak is between 2 and5 years with a slight male predominance (12ndash141) Thesetumors may arise anywhere in the body and fewer than 20are located in the pelvis [12]Most RMS tumors are originatedin the head and neck region urogenital tract and extremities[33] The most common histologic type seen in gt50 isembryonal followed by alveolar in 20ndash30 PleomorphicRMS is rare (1) and has a poor prognosis [8] AlveolarRMS is characterized by the translocation t(213)(q35q14) in70 of cases and the variant translocation t(113)(p36q14)in a smaller percentage of cases Evidence accumulates
8 Case Reports in Genetics
Table3Ch
aracteris
ticso
fPediatricPatie
ntsw
ithUmbilicalLigamentR
habd
omyosarcom
a
PT number
Author
Year
Cou
ntry
Sex
Age
atdiagno
sis(yearsm
onths)
Symptom
sLo
catio
nSize
(cm)
Histology
IRS
grou
pTh
erapy
Outcome
1Ra
nsom
[2627]
1933
USA
F4m
Massb
elowthe
umbilicus
and
extend
ing
somew
hattothe
right
Urachus
(medianUL)
attached
alon
gthea
nterior
wallfrom
theu
mbilicus
tothea
pexof
theb
ladd
er
115
Spindle
cell
ISM
AC
RT
Lastcheck-up
exam
ination(2
years)
show
edno
evidence
ofrecurrence
2Ishikawae
tal[28]
1985
Japan
F1y
4mAb
dominalmass
abdo
minalpain
hemop
erito
neum
Urachal(m
edianUL)
intra-abdo
minalruptureo
fthetum
or
Fist-
sized
NDF
IVSM
ACNDF
3Yo
koyamae
tal[2729]
1997
Japan
M2y
Episo
diclow
erabdo
minalpain
Urachus
(medianUL)
extraperito
neallocated
betweentheu
mbilicus
and
apex
oftheb
ladd
erandwas
adherin
gtig
htlyto
both
Theb
ilateralm
edialU
Lweres
eenenterin
gthe
tumorR
upturedwith
asm
alln
umbero
fdissem
inated
tumors
scatteredon
them
esentery
andDou
glas
pouch
12Em
bryonal
IVSM
AI
ChT
At2yearso
ffollo
w-upno
recurrence
hadbeen
detected
4lowastKe
rretal
[78]
1998
England
F3y
2mAb
dominalmass
Urachus
(medianUL)
adherent
totheb
ladd
erNDF
Embryonal
IIaSM
II
ChT
Histologyshow
edextend
ingup
tothe
resectionmargin
Diedaged
5years
[59]
5Schu
lzand
OrsquoLeary
[2730]
2001
Scotland
M2y
NDF
Urachus
(medianUL)
NDF
Embryonal
NDF
SCh
TRT
Tumor-fr
eeageo
f26
years
6Fernandeze
tal[27]
2007
Spain
F6y
Intractable
constip
ation
nauseaabd
ominal
painles
smass
Urachus
(medianUL)
infiltratingthev
entral
abdo
minalwalland
fixed
tothev
esicaldo
me
135
Embryonal
IbSM
IC
ChT
At4yearso
ffollo
w-upthep
atient
remains
welland
free
ofclinicald
isease
7lowastMenke
etal
[2425]
2015
Germany
F3y
Abdo
minalmass
Lower
anterio
rabd
omen
abovethe
urinarybladderamp
(urachusm
edianULby
locatio
n)
NDF
Embryonal
IIaSM
II
ChT
R1resection
(marginaltum
orresid
ue)Tu
mor-fr
eeageo
f6years
8Ch
eikh
elard
etal[31]
2015
Dx
1983
France
F5y
5mNDF
Urachus
(medianUL)
periton
ealm
etastasesa
ndhypo
gastric
lymph
nodes
5NDF
IVSM
AI
ChT
Died31
mon
thsa
fter
diagno
siswith
relap
sein
periton
ealliver
at11mon
ths
Case Reports in Genetics 9
Table3Con
tinued
PT number
Author
Year
Cou
ntry
Sex
Age
atdiagno
sis(yearsm
onths)
Symptom
sLo
catio
nSize
(cm)
Histology
IRS
grou
pTh
erapy
Outcome
9Ch
eikh
elard
etal[31]
2015
Dx
2003
France
F3y
3mPeriton
ealrup
ture
poor
generalstatus
Urachus
(medianUL)
lumbo
aorticandexternal
iliac
lymph
nodes
10Alveolar
IVSM
AI
ChTRT
Died57
mon
thsa
fter
diagno
siswith
relap
sein
periton
ealliver
at30
mon
ths
10Ch
eikh
elard
etal[31]
2015
Dx
2005
France
F2y
6mMasspo
orgeneral
statusdysuria
Urachus
(medianUL)
15Em
bryonal
III
SMII
ChTRT
Died37
mon
thsa
fter
diagno
siswith
periton
ealrelapse
at19
mon
ths
11Ch
eikh
elard
etal[31]
2015
Dx
2005
France
M4y
2mMasspo
orgeneral
statusdysuria
Urachus
(medianUL)
periton
ealm
etastasesa
ndiliac
lumbo
aorticlymph
nodes
10Em
bryonal
IVSM
II
ChTRT
Relapsed
multifocalat
82mon
thsfollo
w-up
100mon
ths
12Ch
eikh
elard
etal[31]
2015
Dx
2005
France
M5y
3mMasspo
orgeneral
status
Urachus
(medianUL)
periton
ealm
etastasesa
ndmesenteric
lymph
nodes
106
Embryonal
IVSM
IC
ChTRT
Tumor
freea
fter9
5mon
thssince
diagno
sis
13Ch
eikh
elard
etal[31]
2015
Dx
2006
France
M2y
5mMasspo
orgeneral
statusob
structiv
erenalinsuffi
ciency
Urachus
(medianUL)
periton
ealbon
emetastases
andhypo
gastric
lymph
nodes
21Em
bryonal
IVSM
II
ChTRT
Bone
progression
after
16mon
thsdied
18aft
erdiagno
sis
14Ch
eikh
elard
etal[31]
2015
Dx
2010
France
M4y
5mAb
dominalpain
Urachus
(medianUL)
7Em
bryonal
III
SMIC
ChT
Tumor
freea
fter18
mon
thssince
diagno
sis
15Ch
eikh
elard
etal[31]
2015
Dx
2010
France
M6y
Abdo
minalpain
Urachus
(medianUL)
periton
ealm
etastases
14Em
bryonal
IVSM
AI
ChTRT
Tumor
freea
fter4
5mon
thssince
diagno
sis
16lowast
Sanchez-
Mon
tenegro
etal(this
repo
rt)
2017
Dx
2015
Spain
F2y
4mAs
ymptom
atic
LeftmedialU
L5
Embryonal
IaCh
TSM
IC
RT
Tumor-fr
eeageo
f3yearsa
nd9mon
ths
17lowast
Sanchez-
Mon
tenegro
etal(this
repo
rt)
2017
Dx
2015
Spain
F3y
10m
Asym
ptom
atic
Rightm
edialU
L85
Spindle
cell
IIaSM
II
ChT
Tumor-fr
eeageo
f4yearsa
nd5mon
ths
ChT
chem
otherapyD
xdiagno
sed
Ffemale
IRS
intergroup
rhabdo
myosarcom
aMm
ale
NDF
nodata
foun
dRT
radiotherapy
Ssurgery
SMAIsurgerymacroscop
ically
incomplete
SMAC
surgery
macroscop
icallycompleteSM
ICsurgery
microscop
icallycompleteSM
IIsurgery
microscop
icallyincompleteULum
bilicalligam
ent
ampPerson
alcommun
icationby
authorlowast
Patientsw
ithCostello
synd
rome
10 Case Reports in Genetics
Table 4 Chemotherapy of pediatric patients with umbilical ligament rhabdomyosarcoma
PTnumber Chemotherapy protocol
1-2 No ChT [26 28]3 After establishment of the final diagnosis he was treated with combined ChT including VCR ACD and CTX [29]
4lowastInitially IFOS ACD and VCR After 4 courses CTX was substituted for IFOS because of hemorrhagic cystitis Tx complicatedby recurrent episodes of moderately severe diarrhoea and febrile neutropenia requiring readmission to hospital Tx wascompleted after six courses of ChT [7]
5 NDF [30]
6 PT started induction of ChT 2 weeks after S Induction regimen included 9 cycles of IVA (IFOS VCR and ACD) that were welltolerated with minimal systemic complications (Tx 953 of the MMT 95 SIOP protocol for RMS) [27]
7lowast ChT according to the cooperative soft tissue sarcoma protocol (CWS-2002 P) was well tolerated by the PT [24]8 Adjuvant ChT with 10 cycles of IFOS VCR and ACD [31]9 Adjuvant ChT with 6 cycles of IFOS VCR and VP-16 and 9 cycles of VCR ACD CTXACD and CTX [31]10 Neoadjuvant ChT with 6 cycles of IFOS VCR and ACD and adjuvant ChT with 3 cycles of IFOS VCR and ACD [31]
11 Neoadjuvant ChT with 1 cycle of CTX VCR and PRED 2 cycles IFOS VCR and ACD and 4 cycles of IFOS VCR ACD andDOX and adjuvant ChT with 3 cycles of IFOS VCR and ACD [31]
12 Neoadjuvant ChT with 1 cycle of CTX VCR and PRED and 5 cycles of IFOS VCR ACD and DOX and adjuvant ChT with 2cycles of IFOS VCR ACD and DOX and 1 cycle of IFOS VCR and ACD [31]
13 Neoadjuvant ChT with 2 cycles of VCR ACD and CTX + and 3 cycles of IFOS VCR ACD and DOX and adjuvant ChT with 3cycles of IFOS VCR and ACD [31]
14 Neoadjuvant ChT with 4 cycles of IFOS VCR ACD and DOX and adjuvant ChT with 5 cycles of IFOS VCR ACD [31]
15 Neoadjuvant ChT with 4 cycles of IFOS VCR ACD DOX 3 cycles of IFOS VCR ACD and adjuvant ChT with 1 cycle of IFOSVCR ACD 1 cycle of IFOS VCR [31]
16lowastChT in the standard risk group protocol EpSSG RMS 2005 subgroup D 3 preoperative cycles of IFOS (2 doses at 100mgkg)VCR (005mgkg) and ACD (005mgkg)
17lowastChT (postoperative 15 days) in the standard risk group protocol EpSSG RMS 2005 subgroup B (Stage I) cycles of IFOS (2 dosesof 3 gm2d) VCR (15mgm2) and ACD (15mgm2) was initiated
ACD actinomycin D ChT chemotherapy CTX cyclophosphamide CWS Cooperative Weichteilsarkom Studie (Cooperative Soft Tissue Sarcoma Study)DOX Doxorubicin EpSSG European pediatric Soft tissue sarcoma Study Group IFOS ifosfamide MMT malignant mesenchymal tumor NDF no datafound PRED prednisone PT patient RMS rhabdomyosarcoma S surgery SIOP Societe Internationale DrsquoOncologie Pediatrique (International Society ofPediatric Oncology) Tx treatment VCR vincristine VP-16 etoposide lowastPatients with Costello syndrome
that alveolar RMS and embryonal RMS are two differentdisorders while alveolar RMS may originate from primitiveuncommitted mesodermal cells embryonal RMS originatesprobably from more differentiated myoblasts Ras protein-specific guanine nucleotide-releasing factor 1 (RasGRF1)plays an important role in alveolar RMS pathogenesis Theseinteresting concepts however need more evidence [33]
The umbilicus caudally originates the common ligamentwhich is divided into obliterated umbilical arteries (medialUL) and urachus (median UL) The urachus varies from3 to 10 cm in length and from 8 to 10mm in diameterIt is a three-layered tubular structure the innermost layerbeing lined with transitional epithelium in 70 of casesand with columnar epithelium in 30 The structure issurrounded by connective tissue and outermost muscularlayer in continuity with the detrusor muscle Along its pathfrom the bladder to the umbilicus the urachus lies betweenthe transverse fascia and the parietal peritoneum containedin the pyramidal retropubic perivesical preperitoneal spacecompartmentalized by umbilicovesical fascia along with themedial umbilical ligaments and the bladder Occasionallythe urachus may merge with one or both of the obliteratedumbilical arteries (medial UL) and there may be a slight
deviation to the right or left of the midline [34] The urachusis an embryological remnant resulting from the obliterationof the allantoic channel which attaches the bladder dome tothe umbilicus [31]
Urachal malignant tumors are extremely rare represent-ing less than 05 of all bladder cancers and 001 of alltumors They may arise from any portion of the urachus andare most commonly found in adults and males (60ndash70)Although sarcomas represent only 8 they are the mostfrequent urachal neoplasms reported in patients youngerthan 20 years of age (67) [27] Poor prognosis is a commonfeature in adults and pediatric urachalmalignancies with 50to 60 of 5-year survival In contrast the 5-year event-freesurvival in pelvic RMS was reported to be about 51 [31]
This indolent and rather large urachal tumor was mostlyrevealed by an uncomplicated progressing mass withoutprodromic urological symptomsThedelay of diagnosis couldbe explained by a long asymptomatic progression of thetumor in a preperitoneal location which allows an importantlocal spreading before diagnosis Even in patients withouttumor rupture peritoneal involvement appeared to be the keypoint in the prognosis of urachal RMS Systematic cytologyat diagnosis could be more accurate to evaluate peritoneal
Case Reports in Genetics 11
extension in order to avoid understaging and adjust adjuvantlocoregional treatment [31]
Previously only 12 patients with RMS arising from theurachus (median UL) in children without CS have beenreported in the English literature (Table 3) By 2011 therewere29 reported cases of cancer in patients withCS 19 RMS (meanage of 23 years 9 embryonal 1 alveolar 1 mixed histology1 pleomorphic 1 spindle cell type and 6 unclassified) 5neuroblastomas 4 bladder cancer and 1 fibrosarcoma [35]
Loss of heterozygosity for 11p155 in RMS from individu-als with CS suggests that loss of the wild-type allele is the sec-ond hit in tumor development [6 16 36] Whereas theHRASmutation in a sporadic malignancy in the general populationis present only within the tumor cells in CS an identicalmutation is present in every single cell of the individualthus accounting for the tumor predisposition [1] implicatingan alternate mechanism of rhabdomyosarcogenesis [16] Inaddition one patient with CS and uniparental trisomy dueto triplication of the mutated paternal HRAS gene was alsoreported RMS typically displays loss of heterozygosity ofthe 11p155 region because of paternal uniparental disomyand approximately 28 of cases harbor mutations in genesof growth signaling pathways In reports of uniparentaldisomy plus HRAS mutation the latter was heterozygousand therefore must have occurred after the developmentof uniparental disomy [24] The functional analysis alsorevealed that CS-causing mutant HRAS proteins causedoncogene-induced senescence in human fibroblasts [37]Theimportant role of PI3K-protein-kinase B (AKT) signalingin Ras-mediated transformation and tumorigenesis is high-lighted by constitutive AKT activation in RMS cell lines andclinical samples Thus prolonged PI3K-AKT signaling mightalso be implicated in the development of soft tissue sarcomain patients with CS [38]
Only four out of 11 patients were diagnosed with CS priorto the RMS diagnosis in 5 patients CS was diagnosed afterthe RMS and in the remaining 2 the order was unknown[20] In 2003 a further three unpublished cases of RMS inchildren with CS were known through the International CSSupport Group [18] and for that reason there is possiblyunderdiagnosis of RMS in patients with CS
A screening protocol was proposed consisting of ultra-sound examination of the abdomen and pelvis every 3ndash6 months until age of 8ndash10 years for RMS and abdomi-nal neuroblastoma urine catecholamine metabolite analysisevery 6ndash12 months until age of 5 years for neuroblastomaand urinalysis for hematuria annually for bladder carcinomaafter age of 10 years The prior diagnosis of CS was theprerequisite for the implementation of a tumor screeningprotocol [8] The recommendation based on the presumedfast doubling time of RMS was abdominal sonographyscreening for RMS that should be done in similar intervalsof every four months until stronger evidence would suggestotherwise [39] Screening for neuroblastoma is no longerrecommended becausemany CS patients without identifiabletumor show elevated catecholamine metabolites in urine itappears that in this patient group an elevation above thenormal limit defined as 2 standard deviations (SD) above themean for age is more likely to be a variant rather than a sign
of a neuroblastoma [1 40] A French monitoring protocolproposed the determination of catecholamines and theirmetabolites in urine every six months until the age of 5 yearsand ultrasound abdominopelvic every six months until theend of the puberty seeking hematuria dipstick from6monthsto the age of 10 [41] The protocol in our hospital for patientswith CS includes an abdominal and pelvic ultrasound 3times during the first year of life and in childhood every 6months until age of 10 [42] We believe that the best optionis to perform a pelvic abdominal ultrasound every 3 monthsduring the first eight years of life and then controls accordingto medical criteria This is even more necessary in patientswith possible UL RMS because diagnosis was usually done inadvanced stages with a poor survival It is possible that withclose monitoring after an early diagnosis will detect initialstages of the tumor in previously not described locations
Head and neck MRI scans can be performed less fre-quently Ear examination and tympanometry every 4 to 6months to detect middle ear effusion which would raisesuspicion for a nasopharyngeal mass are also recommended[6]
The outcome of CS patients with RMS has been compa-rable to that for patients without the syndrome with a 5-yearsurvival rate of 65 to 70 [19] but according to this reviewit could be worse than the general population Neoplasia wasnoted at the cause of death in five (22) patients with CS[4 15] but in our study the mortality associated with RMSwas 43 Because the long-term survival in RMS is basedon the histology of the tumor and the extent of disease atdiagnosis early diagnosis may alter the treatment regimenand improve prognosis This could be particularly importantin patients with CS who often are medically fragile [20]
The RasMAPK pathway is an attractive target in thetreatment of cancer utilizing small molecule therapeuticsthat specifically inhibits the pathway Ras pathway agentssuch as farnesyltransferase inhibitors (tipifarnib and lona-farnib) that prevent posttranslational modification of Rasare being evaluated for cancer treatment and may be oftherapeutic use for syndromes in this pathway especially CSIn addition B-Raf protooncogene serinethreonine kinase(BRAF) and mitogenextracellular signal-regulated kinase(MEK) inhibitors offer the same potential in the possibletreatment of CS Since the RasMAPK pathway has targets forinhibition in cancer treatment there aremany smallmoleculetherapeutics that are in development or undergoing clinicaltrials with some already FDA approval [43]
6 ConclusionsCS is a syndrome poorly known in oncology but theirpredisposition tomalignancies includingULRMS implies theneed for a new perspective on early diagnosis and aggressivemedical and surgical treatment
ConsentInformed consent was obtained from the new two individualparticipants included in the study and has been properlydocumented with the parental approval to the use of patientrsquosimages and complementary studies
12 Case Reports in Genetics
Competing Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
Special thanks are due to Israel Fernandez Pineda MDAssistantMember and Surgery Fellowship ProgramDirectorSt Jude Childrenrsquos Research Hospital (Memphis TN) for therecommendations and corrections to the manuscript
References
[1] E Quezada and K W Gripp ldquoCostello syndrome and relateddisordersrdquo Current Opinion in Pediatrics vol 19 no 6 pp 636ndash644 2007
[2] JM Costello ldquoA new syndromerdquoNewZealandMedical Journalvol 74 article 397 1971
[3] JMCostello ldquoAnew syndromemental subnormality andnasalpapillomatardquo Australian Paediatric Journal vol 13 no 2 pp114ndash118 1977
[4] K W Gripp and A E Lin ldquoCostello syndrome a Rasmitogenactivated protein kinase pathway syndrome (rasopathy) result-ing from HRAS germline mutationsrdquo Genetics in Medicine vol14 no 3 pp 285ndash292 2012
[5] B Kerr M-A Delrue S Sigaudy et al ldquoGenotype-phenotypecorrelation in Costello syndrome HRAS mutation analysis in43 casesrdquo Journal of Medical Genetics vol 43 no 5 pp 401ndash4052006
[6] N Ahmadi and E Harley ldquoCostello syndrome and the impor-tance of cancer screeningrdquo Archives of OtolaryngologymdashHeadand Neck Surgery vol 136 no 10 pp 1028ndash1029 2010
[7] B Kerr O B Eden R Dandamudi et al ldquoCostello syndrometwo cases with embryonal rhabdomyosarcomardquo Journal ofMedical Genetics vol 35 no 12 pp 1036ndash1039 1998
[8] K W Gripp C I Scott Jr L Nicholson et al ldquoFive additionalCostello syndrome patients with rhabdomyosarcoma proposalfor a tumor screening protocolrdquo American Journal of MedicalGenetics vol 108 no 1 pp 80ndash87 2002
[9] K W Gripp A E Lin D L Stabley et al ldquoHRAS mutationanalysis in Costello syndrome genotype and phenotype corre-lationrdquo American Journal of Medical Genetics Part A vol 140no 1 pp 1ndash7 2006
[10] M Feingold ldquoCostello syndrome and rhabdomyosarcomardquoJournal of Medical Genetics vol 36 no 7 pp 582ndash583 1999
[11] S M White J M Graham Jr B Kerr et al ldquoThe adultphenotype in Costello syndromerdquo American Journal of MedicalGenetics A vol 136 no 2 pp 128ndash135 2005
[12] G Bisogno A Murgia I Mammi M S Strafella and M CarlildquoRhabdomyosarcoma in a patient with cardio-facio-cutaneoussyndromerdquo Journal of Pediatric HematologyOncology vol 21no 5 pp 424ndash427 1999
[13] S Sigaudy G Vittu A David et al ldquoCostello syndrome reportof six patients including one with an embryonal rhabdomyosar-comardquoEuropean Journal of Pediatrics vol 159 no 3 pp 139ndash1422000
[14] A Hinek M A Teitell L Schoyer et al ldquoMyocardial storage ofchondroitin sulfate-containing moieties in Costello syndromepatients with severe hypertrophic cardiomyopathyrdquo AmericanJournal of Medical Genetics vol 133 no 1 pp 1ndash12 2005
[15] A E Lin P D Grossfeld R M Hamilton et al ldquoFurtherdelineation of cardiac abnormalities in Costello syndromerdquoAmerican Journal of Medical Genetics vol 111 no 2 pp 115ndash1292002
[16] A L Estep W E Tidyman M A Teitell P D Cotter and KA Rauen ldquoHRASmutations in Costello syndrome detection ofconstitutional activating mutations in codon 12 and 13 and lossof wild-type allele in malignancyrdquo American Journal of MedicalGenetics vol 140 no 1 pp 8ndash16 2006
[17] H KawameMMatsui K Kurosawa et al ldquoFurther delineationof the behavioral and neurologic features inCostello syndromerdquoAmerican Journal of Medical Genetics vol 118A no 1 pp 8ndash142003
[18] B Kerr M A Einaudi P Clayton et al ldquoIs growth hormonetreatment beneficial or harmful in Costello syndromerdquo Journalof medical genetics vol 40 no 6 article e74 2003
[19] J P OrsquoNeal J Ramdas W E Wood and P K PellitterildquoParameningeal rhabdomyosarcoma in a patient with Costellosyndromerdquo Journal of Pediatric HematologyOncology vol 26no 6 pp 389ndash392 2004
[20] K W Gripp ldquoTumor predisposition in Costello syndromerdquoAmerican Journal of Medical Genetics Part C Seminars inMedical Genetics vol 137C no 1 pp 72ndash77 2005
[21] Y Aoki T Niihori H Kawame et al ldquoGermline mutationsin HRAS proto-oncogene cause Costello syndromerdquo NatureGenetics vol 37 no 10 pp 1038ndash1040 2005
[22] Y Abe Y Aoki S Kuriyama et al ldquoPrevalence and clinicalfeatures of Costello syndrome and cardio-facio-cutaneous syn-drome in Japan findings from a nationwide epidemiologicalsurveyrdquo American Journal of Medical Genetics Part A vol 158no 5 pp 1083ndash1094 2012
[23] I F M Lo C Brewer N Shannon et al ldquoSevere neonatal man-ifestations of Costello syndromerdquo Journal of Medical Geneticsvol 45 no 3 pp 167ndash171 2008
[24] J Menke S Pauli M Sigler et al ldquoUniparental trisomy of amutated HRASproto-oncogene in embryonal rhabdomyosar-coma of a patient with costello syndromerdquo Journal of ClinicalOncology vol 33 no 13 pp e62ndashe65 2015
[25] C P Kratz L Franke H Peters et al ldquoCancer spectrum andfrequency among children with Noonan Costello and cardio-facio-cutaneous syndromesrdquo British Journal of Cancer vol 112no 8 pp 1392ndash1397 2015
[26] H K Ransom ldquoSarcoma of the urachus review of the literaturewith report of an additional caserdquo The American Journal ofSurgery vol 22 no 2 pp 187ndash191 1933
[27] E M L-T Fernandez N H Siverio R L Almaraz L MViota J R Luis and L D Flores ldquoRadical surgery and IVA-chemotherapeutic regimen to treat embryonal rhabdomyosar-coma of the urachus case reportrdquo Pediatric Hematology andOncology vol 24 no 7 pp 543ndash550 2007
[28] M Ishikawa T Nishi R Yamada et al ldquoA case of urachalsarcoma in childhood case report and review of the worldliteraturerdquo Journal of the Japanese Society of Pediatric Surgeonsvol 21 pp 128ndash135 1985
[29] S Yokoyama YHayashida J Nagahama et al ldquoRhabdomyosar-coma of the urachus a case reportrdquo Acta Cytologica vol 41 no4 pp 1293ndash1298 1997
[30] U Schulz and C P OrsquoLeary ldquoSpinal AVM epidermal nevusand rhabdomyosarcoma a rare neurocutaneous syndromerdquoNeurology vol 56 no 3 pp 395ndash397 2001
Case Reports in Genetics 13
[31] A Cheikhelard S Irtan D Orbach et al ldquoUrachal rhab-domyosarcoma in childhood a rare entity with a poor out-comerdquo Journal of Pediatric Surgery vol 50 no 8 pp 1329ndash13332015
[32] K W Gripp E Hopkins K Sol-Church et al ldquoPhenotypicanalysis of individuals with Costello syndrome due to HRASpG13Crdquo American Journal of Medical Genetics Part A vol 155no 4 pp 706ndash716 2011
[33] M Tarnowski G Schneider G Amann et al ldquoRasGRF1 reg-ulates proliferation and metastatic behavior of human alveolarrhabdomyosarcomasrdquo International Journal of Oncology vol 41no 3 pp 995ndash1004 2012
[34] J-S Yu K W Kim H-J Lee Y-J Lee C-S Yoon and M-J Kim ldquoUrachal remnant diseases spectrum of CT and USfindingsrdquo Radiographics vol 21 no 2 pp 451ndash461 2001
[35] C P Kratz S Rapisuwon H Reed H Hasle and P S Rosen-berg ldquoCancer in Noonan Costello cardiofaciocutaneous andLEOPARD syndromesrdquo American Journal of Medical GeneticsPart C Seminars in Medical Genetics vol 157 no 2 pp 83ndash892011
[36] B Kerr M L Mucchielli S Sigaudy et al ldquoIs the locus forCostello syndrome on 11prdquo Journal of Medical Genetics vol 40no 6 pp 469ndash471 2003
[37] TNiihori YAokiNOkamoto et al ldquoHRASmutants identifiedin Costello syndrome patients can induce cellular senescencepossible implications for the pathogenesis of Costello syn-dromerdquo Journal of Human Genetics vol 56 no 10 pp 707ndash7152011
[38] G Rosenberger S Meien and K Kutsche ldquoOncogenic HRASmutations cause prolonged PI3K signaling in response toepidermal growth factor in fibroblasts of patients with costellosyndromerdquo Human Mutation vol 30 no 3 pp 352ndash362 2009
[39] M R DeBaun ldquoScreening for cancer in children with Costellosyndromerdquo American Journal of Medical Genetics vol 108 no1 pp 88ndash90 2002
[40] K W Gripp H Kawame D H Viskochil and L NicholsonldquoElevated catecholamine metabolites in patients with Costellosyndromerdquo American Journal of Medical Genetics vol 128 no1 pp 48ndash51 2004
[41] M-ADelrue B Arveiler andD Lacombe ldquoCostello syndromeclinical features and tumoral riskrdquo Archives de Pediatrie vol 9no 10 pp 1059ndash1063 2002
[42] V Martınez-Gonzalez and P Lapunzina Sındrome de CostelloGrupodeTrabajo sobreCancer en SındromeGeneticos Polimar-formativos (GT-CSGP) httpswwworphanetdatapathoProesCSGP-Costello-3pdf
[43] K A Rauen A Banerjee W R Bishop et al ldquoCostello andcardio-facio-cutaneous syndromes moving toward clinical tri-als in RASopathiesrdquo American Journal of Medical Genetics PartC Seminars inMedical Genetics vol 157 no 2 pp 136ndash146 2011
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Case Reports in Genetics 7
Table 2 Chemotherapy of patients with Costello syndrome and rhabdomyosarcoma
PTnumber Chemotherapy protocol
1Initially with VCR ACD and CTX After debulking continued on ChT using IFOS VCR and ACD After the second coursewhen she developed IFOS induced encephalopathy she was changed back to pulses of VCR ACD and CTX given every 3weeks for 9 courses [7]
2Initially IFOS ACD and VCR After 4 courses CTX was substituted for IFOS because hemorrhagic cystitis Tx complicatedby recurrent episodes of moderately severe diarrhoea and febrile neutropenia requiring readmission to hospital Tx wascompleted after six courses of ChT [7]
3 Tx consisted of below the knee amputation and ChT (DOX ACD VCR and CTX) [10]
4
Tx was implemented according to the Italian protocol for pediatric soft tissue sarcoma Three courses of ChT including VCR(0025mgkg day 1) IFOS (50mgkg days 1 and 2) and alternating ACD (0025mgkg day 1) and DOX (07mgkg day 1) wereadministered Symptoms regressed and the CT scan showed a reduction in tumor volume of more than two-thirds After 3more courses of ChT the patient experienced abdominal pain A repeat abdominal CT scan showed an increase in the pelvicmass Despite the administration of a different ChT with CBDCA (11mgkg day 1) and VP-16 (3mgkg for 3 doses) the tumorcontinued to grow and the child died 7 months after the diagnosis of RMS [12]
5 NDF [13]
6
The first cycle of ChT with VCR ACD and CTX and topotecan reduced the tumor size [16] The tumor was surgicallyremoved after the first ChT [8] Debulking S was required because of rapid growth and tumor necrosis The protocol wascontinued and was deemed sufficiently successful to withhold RT One month after completion of the first protocol tumorrecurrence necessitated a second round of ChT with irinotecan and DOXThe latter drug was administered about 1 weekbefore he died during which time he had tachycardia (heart rate 180ndash20 bpm) [14]
7 The tumor did not respond to ChT and she died shortly after her 4th birthday [8]8 Tx was a combination of S ChT and RT continued until age of 35 years [8]9-10 NDF [8]11 PT had later generalized tonic-clonic seizures during her Tx for RMS [17]12 Despite extensive ChT the tumor progressed rapidly and the PT died 2 months later [18]
13 Induction ChT was commenced with the initial 12-week course of VCR ACD and CTX based on the Intermediate RiskProtocol D9803 of the COG [19]
14 ChT did not result in tumor shrinkage therefore surgical resection was performed [20]15ndash22 NDF [5 6 9 21ndash23]23 ChT according to the cooperative soft tissue sarcoma protocol (CWS-2002 P) was well tolerated by the PT [24]24 NDF [25]
25 ChT in the standard risk group protocol EpSSG RMS 2005 subgroup D 3 preoperative cycles of IFOS (2 doses at 100mgkg)VCR (005mgkg) and ACD (005mgkg)
26 ChT (postoperative 15 days) in the standard risk group protocol EpSSG RMS 2005 subgroup B (Stage I) cycles of IFOS (2doses of 3 gm2d) VCR (15mgm2) and ACD (15mgm2) was initiated
ACD actinomycin D CBDCA carboplatin ChT chemotherapy COG childrenrsquos oncology group CTX cyclophosphamide CT computed tomography CWSCooperative Weichteilsarkom Studie (Cooperative Soft Tissue Sarcoma Study) DOX Doxorubicin EpSSG European pediatric Soft tissue sarcoma StudyGroup IFOS ifosfamide NDF no data found PT patient RMS rhabdomyosarcoma RT radiotherapy S surgery Tx treatment VCR vincristine VP-16etoposide
stimulator (RalGDS) [16 21] in signaling pathways control-ling cell proliferation and differentiation [9]
Themajority of patients with CS had 34GgtA transition incodon 12 (80) [4 16] More than 95 of the mutations arepredicted to result in substitution of the glycine in position12 or 13 of the protein product [1] All individuals withmalignancy had a codon 12 mutation (especially G12A 47patients) [5 21] The rare G12V mutation is associated witha more severe early lethal phenotype some patients diefrom respiratory distress hypertrophic cardiomyopathy ormalignant tachycardia prior to being diagnosed with CS [1]As far as we know no individual with G13C has developed amalignant tumor [4 32]
RMS is the most common soft tissue sarcoma of infancyIts incidence is between 4 and 7 cases per 1 million childrenyounger than 15 years [8 12] The age peak is between 2 and5 years with a slight male predominance (12ndash141) Thesetumors may arise anywhere in the body and fewer than 20are located in the pelvis [12]Most RMS tumors are originatedin the head and neck region urogenital tract and extremities[33] The most common histologic type seen in gt50 isembryonal followed by alveolar in 20ndash30 PleomorphicRMS is rare (1) and has a poor prognosis [8] AlveolarRMS is characterized by the translocation t(213)(q35q14) in70 of cases and the variant translocation t(113)(p36q14)in a smaller percentage of cases Evidence accumulates
8 Case Reports in Genetics
Table3Ch
aracteris
ticso
fPediatricPatie
ntsw
ithUmbilicalLigamentR
habd
omyosarcom
a
PT number
Author
Year
Cou
ntry
Sex
Age
atdiagno
sis(yearsm
onths)
Symptom
sLo
catio
nSize
(cm)
Histology
IRS
grou
pTh
erapy
Outcome
1Ra
nsom
[2627]
1933
USA
F4m
Massb
elowthe
umbilicus
and
extend
ing
somew
hattothe
right
Urachus
(medianUL)
attached
alon
gthea
nterior
wallfrom
theu
mbilicus
tothea
pexof
theb
ladd
er
115
Spindle
cell
ISM
AC
RT
Lastcheck-up
exam
ination(2
years)
show
edno
evidence
ofrecurrence
2Ishikawae
tal[28]
1985
Japan
F1y
4mAb
dominalmass
abdo
minalpain
hemop
erito
neum
Urachal(m
edianUL)
intra-abdo
minalruptureo
fthetum
or
Fist-
sized
NDF
IVSM
ACNDF
3Yo
koyamae
tal[2729]
1997
Japan
M2y
Episo
diclow
erabdo
minalpain
Urachus
(medianUL)
extraperito
neallocated
betweentheu
mbilicus
and
apex
oftheb
ladd
erandwas
adherin
gtig
htlyto
both
Theb
ilateralm
edialU
Lweres
eenenterin
gthe
tumorR
upturedwith
asm
alln
umbero
fdissem
inated
tumors
scatteredon
them
esentery
andDou
glas
pouch
12Em
bryonal
IVSM
AI
ChT
At2yearso
ffollo
w-upno
recurrence
hadbeen
detected
4lowastKe
rretal
[78]
1998
England
F3y
2mAb
dominalmass
Urachus
(medianUL)
adherent
totheb
ladd
erNDF
Embryonal
IIaSM
II
ChT
Histologyshow
edextend
ingup
tothe
resectionmargin
Diedaged
5years
[59]
5Schu
lzand
OrsquoLeary
[2730]
2001
Scotland
M2y
NDF
Urachus
(medianUL)
NDF
Embryonal
NDF
SCh
TRT
Tumor-fr
eeageo
f26
years
6Fernandeze
tal[27]
2007
Spain
F6y
Intractable
constip
ation
nauseaabd
ominal
painles
smass
Urachus
(medianUL)
infiltratingthev
entral
abdo
minalwalland
fixed
tothev
esicaldo
me
135
Embryonal
IbSM
IC
ChT
At4yearso
ffollo
w-upthep
atient
remains
welland
free
ofclinicald
isease
7lowastMenke
etal
[2425]
2015
Germany
F3y
Abdo
minalmass
Lower
anterio
rabd
omen
abovethe
urinarybladderamp
(urachusm
edianULby
locatio
n)
NDF
Embryonal
IIaSM
II
ChT
R1resection
(marginaltum
orresid
ue)Tu
mor-fr
eeageo
f6years
8Ch
eikh
elard
etal[31]
2015
Dx
1983
France
F5y
5mNDF
Urachus
(medianUL)
periton
ealm
etastasesa
ndhypo
gastric
lymph
nodes
5NDF
IVSM
AI
ChT
Died31
mon
thsa
fter
diagno
siswith
relap
sein
periton
ealliver
at11mon
ths
Case Reports in Genetics 9
Table3Con
tinued
PT number
Author
Year
Cou
ntry
Sex
Age
atdiagno
sis(yearsm
onths)
Symptom
sLo
catio
nSize
(cm)
Histology
IRS
grou
pTh
erapy
Outcome
9Ch
eikh
elard
etal[31]
2015
Dx
2003
France
F3y
3mPeriton
ealrup
ture
poor
generalstatus
Urachus
(medianUL)
lumbo
aorticandexternal
iliac
lymph
nodes
10Alveolar
IVSM
AI
ChTRT
Died57
mon
thsa
fter
diagno
siswith
relap
sein
periton
ealliver
at30
mon
ths
10Ch
eikh
elard
etal[31]
2015
Dx
2005
France
F2y
6mMasspo
orgeneral
statusdysuria
Urachus
(medianUL)
15Em
bryonal
III
SMII
ChTRT
Died37
mon
thsa
fter
diagno
siswith
periton
ealrelapse
at19
mon
ths
11Ch
eikh
elard
etal[31]
2015
Dx
2005
France
M4y
2mMasspo
orgeneral
statusdysuria
Urachus
(medianUL)
periton
ealm
etastasesa
ndiliac
lumbo
aorticlymph
nodes
10Em
bryonal
IVSM
II
ChTRT
Relapsed
multifocalat
82mon
thsfollo
w-up
100mon
ths
12Ch
eikh
elard
etal[31]
2015
Dx
2005
France
M5y
3mMasspo
orgeneral
status
Urachus
(medianUL)
periton
ealm
etastasesa
ndmesenteric
lymph
nodes
106
Embryonal
IVSM
IC
ChTRT
Tumor
freea
fter9
5mon
thssince
diagno
sis
13Ch
eikh
elard
etal[31]
2015
Dx
2006
France
M2y
5mMasspo
orgeneral
statusob
structiv
erenalinsuffi
ciency
Urachus
(medianUL)
periton
ealbon
emetastases
andhypo
gastric
lymph
nodes
21Em
bryonal
IVSM
II
ChTRT
Bone
progression
after
16mon
thsdied
18aft
erdiagno
sis
14Ch
eikh
elard
etal[31]
2015
Dx
2010
France
M4y
5mAb
dominalpain
Urachus
(medianUL)
7Em
bryonal
III
SMIC
ChT
Tumor
freea
fter18
mon
thssince
diagno
sis
15Ch
eikh
elard
etal[31]
2015
Dx
2010
France
M6y
Abdo
minalpain
Urachus
(medianUL)
periton
ealm
etastases
14Em
bryonal
IVSM
AI
ChTRT
Tumor
freea
fter4
5mon
thssince
diagno
sis
16lowast
Sanchez-
Mon
tenegro
etal(this
repo
rt)
2017
Dx
2015
Spain
F2y
4mAs
ymptom
atic
LeftmedialU
L5
Embryonal
IaCh
TSM
IC
RT
Tumor-fr
eeageo
f3yearsa
nd9mon
ths
17lowast
Sanchez-
Mon
tenegro
etal(this
repo
rt)
2017
Dx
2015
Spain
F3y
10m
Asym
ptom
atic
Rightm
edialU
L85
Spindle
cell
IIaSM
II
ChT
Tumor-fr
eeageo
f4yearsa
nd5mon
ths
ChT
chem
otherapyD
xdiagno
sed
Ffemale
IRS
intergroup
rhabdo
myosarcom
aMm
ale
NDF
nodata
foun
dRT
radiotherapy
Ssurgery
SMAIsurgerymacroscop
ically
incomplete
SMAC
surgery
macroscop
icallycompleteSM
ICsurgery
microscop
icallycompleteSM
IIsurgery
microscop
icallyincompleteULum
bilicalligam
ent
ampPerson
alcommun
icationby
authorlowast
Patientsw
ithCostello
synd
rome
10 Case Reports in Genetics
Table 4 Chemotherapy of pediatric patients with umbilical ligament rhabdomyosarcoma
PTnumber Chemotherapy protocol
1-2 No ChT [26 28]3 After establishment of the final diagnosis he was treated with combined ChT including VCR ACD and CTX [29]
4lowastInitially IFOS ACD and VCR After 4 courses CTX was substituted for IFOS because of hemorrhagic cystitis Tx complicatedby recurrent episodes of moderately severe diarrhoea and febrile neutropenia requiring readmission to hospital Tx wascompleted after six courses of ChT [7]
5 NDF [30]
6 PT started induction of ChT 2 weeks after S Induction regimen included 9 cycles of IVA (IFOS VCR and ACD) that were welltolerated with minimal systemic complications (Tx 953 of the MMT 95 SIOP protocol for RMS) [27]
7lowast ChT according to the cooperative soft tissue sarcoma protocol (CWS-2002 P) was well tolerated by the PT [24]8 Adjuvant ChT with 10 cycles of IFOS VCR and ACD [31]9 Adjuvant ChT with 6 cycles of IFOS VCR and VP-16 and 9 cycles of VCR ACD CTXACD and CTX [31]10 Neoadjuvant ChT with 6 cycles of IFOS VCR and ACD and adjuvant ChT with 3 cycles of IFOS VCR and ACD [31]
11 Neoadjuvant ChT with 1 cycle of CTX VCR and PRED 2 cycles IFOS VCR and ACD and 4 cycles of IFOS VCR ACD andDOX and adjuvant ChT with 3 cycles of IFOS VCR and ACD [31]
12 Neoadjuvant ChT with 1 cycle of CTX VCR and PRED and 5 cycles of IFOS VCR ACD and DOX and adjuvant ChT with 2cycles of IFOS VCR ACD and DOX and 1 cycle of IFOS VCR and ACD [31]
13 Neoadjuvant ChT with 2 cycles of VCR ACD and CTX + and 3 cycles of IFOS VCR ACD and DOX and adjuvant ChT with 3cycles of IFOS VCR and ACD [31]
14 Neoadjuvant ChT with 4 cycles of IFOS VCR ACD and DOX and adjuvant ChT with 5 cycles of IFOS VCR ACD [31]
15 Neoadjuvant ChT with 4 cycles of IFOS VCR ACD DOX 3 cycles of IFOS VCR ACD and adjuvant ChT with 1 cycle of IFOSVCR ACD 1 cycle of IFOS VCR [31]
16lowastChT in the standard risk group protocol EpSSG RMS 2005 subgroup D 3 preoperative cycles of IFOS (2 doses at 100mgkg)VCR (005mgkg) and ACD (005mgkg)
17lowastChT (postoperative 15 days) in the standard risk group protocol EpSSG RMS 2005 subgroup B (Stage I) cycles of IFOS (2 dosesof 3 gm2d) VCR (15mgm2) and ACD (15mgm2) was initiated
ACD actinomycin D ChT chemotherapy CTX cyclophosphamide CWS Cooperative Weichteilsarkom Studie (Cooperative Soft Tissue Sarcoma Study)DOX Doxorubicin EpSSG European pediatric Soft tissue sarcoma Study Group IFOS ifosfamide MMT malignant mesenchymal tumor NDF no datafound PRED prednisone PT patient RMS rhabdomyosarcoma S surgery SIOP Societe Internationale DrsquoOncologie Pediatrique (International Society ofPediatric Oncology) Tx treatment VCR vincristine VP-16 etoposide lowastPatients with Costello syndrome
that alveolar RMS and embryonal RMS are two differentdisorders while alveolar RMS may originate from primitiveuncommitted mesodermal cells embryonal RMS originatesprobably from more differentiated myoblasts Ras protein-specific guanine nucleotide-releasing factor 1 (RasGRF1)plays an important role in alveolar RMS pathogenesis Theseinteresting concepts however need more evidence [33]
The umbilicus caudally originates the common ligamentwhich is divided into obliterated umbilical arteries (medialUL) and urachus (median UL) The urachus varies from3 to 10 cm in length and from 8 to 10mm in diameterIt is a three-layered tubular structure the innermost layerbeing lined with transitional epithelium in 70 of casesand with columnar epithelium in 30 The structure issurrounded by connective tissue and outermost muscularlayer in continuity with the detrusor muscle Along its pathfrom the bladder to the umbilicus the urachus lies betweenthe transverse fascia and the parietal peritoneum containedin the pyramidal retropubic perivesical preperitoneal spacecompartmentalized by umbilicovesical fascia along with themedial umbilical ligaments and the bladder Occasionallythe urachus may merge with one or both of the obliteratedumbilical arteries (medial UL) and there may be a slight
deviation to the right or left of the midline [34] The urachusis an embryological remnant resulting from the obliterationof the allantoic channel which attaches the bladder dome tothe umbilicus [31]
Urachal malignant tumors are extremely rare represent-ing less than 05 of all bladder cancers and 001 of alltumors They may arise from any portion of the urachus andare most commonly found in adults and males (60ndash70)Although sarcomas represent only 8 they are the mostfrequent urachal neoplasms reported in patients youngerthan 20 years of age (67) [27] Poor prognosis is a commonfeature in adults and pediatric urachalmalignancies with 50to 60 of 5-year survival In contrast the 5-year event-freesurvival in pelvic RMS was reported to be about 51 [31]
This indolent and rather large urachal tumor was mostlyrevealed by an uncomplicated progressing mass withoutprodromic urological symptomsThedelay of diagnosis couldbe explained by a long asymptomatic progression of thetumor in a preperitoneal location which allows an importantlocal spreading before diagnosis Even in patients withouttumor rupture peritoneal involvement appeared to be the keypoint in the prognosis of urachal RMS Systematic cytologyat diagnosis could be more accurate to evaluate peritoneal
Case Reports in Genetics 11
extension in order to avoid understaging and adjust adjuvantlocoregional treatment [31]
Previously only 12 patients with RMS arising from theurachus (median UL) in children without CS have beenreported in the English literature (Table 3) By 2011 therewere29 reported cases of cancer in patients withCS 19 RMS (meanage of 23 years 9 embryonal 1 alveolar 1 mixed histology1 pleomorphic 1 spindle cell type and 6 unclassified) 5neuroblastomas 4 bladder cancer and 1 fibrosarcoma [35]
Loss of heterozygosity for 11p155 in RMS from individu-als with CS suggests that loss of the wild-type allele is the sec-ond hit in tumor development [6 16 36] Whereas theHRASmutation in a sporadic malignancy in the general populationis present only within the tumor cells in CS an identicalmutation is present in every single cell of the individualthus accounting for the tumor predisposition [1] implicatingan alternate mechanism of rhabdomyosarcogenesis [16] Inaddition one patient with CS and uniparental trisomy dueto triplication of the mutated paternal HRAS gene was alsoreported RMS typically displays loss of heterozygosity ofthe 11p155 region because of paternal uniparental disomyand approximately 28 of cases harbor mutations in genesof growth signaling pathways In reports of uniparentaldisomy plus HRAS mutation the latter was heterozygousand therefore must have occurred after the developmentof uniparental disomy [24] The functional analysis alsorevealed that CS-causing mutant HRAS proteins causedoncogene-induced senescence in human fibroblasts [37]Theimportant role of PI3K-protein-kinase B (AKT) signalingin Ras-mediated transformation and tumorigenesis is high-lighted by constitutive AKT activation in RMS cell lines andclinical samples Thus prolonged PI3K-AKT signaling mightalso be implicated in the development of soft tissue sarcomain patients with CS [38]
Only four out of 11 patients were diagnosed with CS priorto the RMS diagnosis in 5 patients CS was diagnosed afterthe RMS and in the remaining 2 the order was unknown[20] In 2003 a further three unpublished cases of RMS inchildren with CS were known through the International CSSupport Group [18] and for that reason there is possiblyunderdiagnosis of RMS in patients with CS
A screening protocol was proposed consisting of ultra-sound examination of the abdomen and pelvis every 3ndash6 months until age of 8ndash10 years for RMS and abdomi-nal neuroblastoma urine catecholamine metabolite analysisevery 6ndash12 months until age of 5 years for neuroblastomaand urinalysis for hematuria annually for bladder carcinomaafter age of 10 years The prior diagnosis of CS was theprerequisite for the implementation of a tumor screeningprotocol [8] The recommendation based on the presumedfast doubling time of RMS was abdominal sonographyscreening for RMS that should be done in similar intervalsof every four months until stronger evidence would suggestotherwise [39] Screening for neuroblastoma is no longerrecommended becausemany CS patients without identifiabletumor show elevated catecholamine metabolites in urine itappears that in this patient group an elevation above thenormal limit defined as 2 standard deviations (SD) above themean for age is more likely to be a variant rather than a sign
of a neuroblastoma [1 40] A French monitoring protocolproposed the determination of catecholamines and theirmetabolites in urine every six months until the age of 5 yearsand ultrasound abdominopelvic every six months until theend of the puberty seeking hematuria dipstick from6monthsto the age of 10 [41] The protocol in our hospital for patientswith CS includes an abdominal and pelvic ultrasound 3times during the first year of life and in childhood every 6months until age of 10 [42] We believe that the best optionis to perform a pelvic abdominal ultrasound every 3 monthsduring the first eight years of life and then controls accordingto medical criteria This is even more necessary in patientswith possible UL RMS because diagnosis was usually done inadvanced stages with a poor survival It is possible that withclose monitoring after an early diagnosis will detect initialstages of the tumor in previously not described locations
Head and neck MRI scans can be performed less fre-quently Ear examination and tympanometry every 4 to 6months to detect middle ear effusion which would raisesuspicion for a nasopharyngeal mass are also recommended[6]
The outcome of CS patients with RMS has been compa-rable to that for patients without the syndrome with a 5-yearsurvival rate of 65 to 70 [19] but according to this reviewit could be worse than the general population Neoplasia wasnoted at the cause of death in five (22) patients with CS[4 15] but in our study the mortality associated with RMSwas 43 Because the long-term survival in RMS is basedon the histology of the tumor and the extent of disease atdiagnosis early diagnosis may alter the treatment regimenand improve prognosis This could be particularly importantin patients with CS who often are medically fragile [20]
The RasMAPK pathway is an attractive target in thetreatment of cancer utilizing small molecule therapeuticsthat specifically inhibits the pathway Ras pathway agentssuch as farnesyltransferase inhibitors (tipifarnib and lona-farnib) that prevent posttranslational modification of Rasare being evaluated for cancer treatment and may be oftherapeutic use for syndromes in this pathway especially CSIn addition B-Raf protooncogene serinethreonine kinase(BRAF) and mitogenextracellular signal-regulated kinase(MEK) inhibitors offer the same potential in the possibletreatment of CS Since the RasMAPK pathway has targets forinhibition in cancer treatment there aremany smallmoleculetherapeutics that are in development or undergoing clinicaltrials with some already FDA approval [43]
6 ConclusionsCS is a syndrome poorly known in oncology but theirpredisposition tomalignancies includingULRMS implies theneed for a new perspective on early diagnosis and aggressivemedical and surgical treatment
ConsentInformed consent was obtained from the new two individualparticipants included in the study and has been properlydocumented with the parental approval to the use of patientrsquosimages and complementary studies
12 Case Reports in Genetics
Competing Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
Special thanks are due to Israel Fernandez Pineda MDAssistantMember and Surgery Fellowship ProgramDirectorSt Jude Childrenrsquos Research Hospital (Memphis TN) for therecommendations and corrections to the manuscript
References
[1] E Quezada and K W Gripp ldquoCostello syndrome and relateddisordersrdquo Current Opinion in Pediatrics vol 19 no 6 pp 636ndash644 2007
[2] JM Costello ldquoA new syndromerdquoNewZealandMedical Journalvol 74 article 397 1971
[3] JMCostello ldquoAnew syndromemental subnormality andnasalpapillomatardquo Australian Paediatric Journal vol 13 no 2 pp114ndash118 1977
[4] K W Gripp and A E Lin ldquoCostello syndrome a Rasmitogenactivated protein kinase pathway syndrome (rasopathy) result-ing from HRAS germline mutationsrdquo Genetics in Medicine vol14 no 3 pp 285ndash292 2012
[5] B Kerr M-A Delrue S Sigaudy et al ldquoGenotype-phenotypecorrelation in Costello syndrome HRAS mutation analysis in43 casesrdquo Journal of Medical Genetics vol 43 no 5 pp 401ndash4052006
[6] N Ahmadi and E Harley ldquoCostello syndrome and the impor-tance of cancer screeningrdquo Archives of OtolaryngologymdashHeadand Neck Surgery vol 136 no 10 pp 1028ndash1029 2010
[7] B Kerr O B Eden R Dandamudi et al ldquoCostello syndrometwo cases with embryonal rhabdomyosarcomardquo Journal ofMedical Genetics vol 35 no 12 pp 1036ndash1039 1998
[8] K W Gripp C I Scott Jr L Nicholson et al ldquoFive additionalCostello syndrome patients with rhabdomyosarcoma proposalfor a tumor screening protocolrdquo American Journal of MedicalGenetics vol 108 no 1 pp 80ndash87 2002
[9] K W Gripp A E Lin D L Stabley et al ldquoHRAS mutationanalysis in Costello syndrome genotype and phenotype corre-lationrdquo American Journal of Medical Genetics Part A vol 140no 1 pp 1ndash7 2006
[10] M Feingold ldquoCostello syndrome and rhabdomyosarcomardquoJournal of Medical Genetics vol 36 no 7 pp 582ndash583 1999
[11] S M White J M Graham Jr B Kerr et al ldquoThe adultphenotype in Costello syndromerdquo American Journal of MedicalGenetics A vol 136 no 2 pp 128ndash135 2005
[12] G Bisogno A Murgia I Mammi M S Strafella and M CarlildquoRhabdomyosarcoma in a patient with cardio-facio-cutaneoussyndromerdquo Journal of Pediatric HematologyOncology vol 21no 5 pp 424ndash427 1999
[13] S Sigaudy G Vittu A David et al ldquoCostello syndrome reportof six patients including one with an embryonal rhabdomyosar-comardquoEuropean Journal of Pediatrics vol 159 no 3 pp 139ndash1422000
[14] A Hinek M A Teitell L Schoyer et al ldquoMyocardial storage ofchondroitin sulfate-containing moieties in Costello syndromepatients with severe hypertrophic cardiomyopathyrdquo AmericanJournal of Medical Genetics vol 133 no 1 pp 1ndash12 2005
[15] A E Lin P D Grossfeld R M Hamilton et al ldquoFurtherdelineation of cardiac abnormalities in Costello syndromerdquoAmerican Journal of Medical Genetics vol 111 no 2 pp 115ndash1292002
[16] A L Estep W E Tidyman M A Teitell P D Cotter and KA Rauen ldquoHRASmutations in Costello syndrome detection ofconstitutional activating mutations in codon 12 and 13 and lossof wild-type allele in malignancyrdquo American Journal of MedicalGenetics vol 140 no 1 pp 8ndash16 2006
[17] H KawameMMatsui K Kurosawa et al ldquoFurther delineationof the behavioral and neurologic features inCostello syndromerdquoAmerican Journal of Medical Genetics vol 118A no 1 pp 8ndash142003
[18] B Kerr M A Einaudi P Clayton et al ldquoIs growth hormonetreatment beneficial or harmful in Costello syndromerdquo Journalof medical genetics vol 40 no 6 article e74 2003
[19] J P OrsquoNeal J Ramdas W E Wood and P K PellitterildquoParameningeal rhabdomyosarcoma in a patient with Costellosyndromerdquo Journal of Pediatric HematologyOncology vol 26no 6 pp 389ndash392 2004
[20] K W Gripp ldquoTumor predisposition in Costello syndromerdquoAmerican Journal of Medical Genetics Part C Seminars inMedical Genetics vol 137C no 1 pp 72ndash77 2005
[21] Y Aoki T Niihori H Kawame et al ldquoGermline mutationsin HRAS proto-oncogene cause Costello syndromerdquo NatureGenetics vol 37 no 10 pp 1038ndash1040 2005
[22] Y Abe Y Aoki S Kuriyama et al ldquoPrevalence and clinicalfeatures of Costello syndrome and cardio-facio-cutaneous syn-drome in Japan findings from a nationwide epidemiologicalsurveyrdquo American Journal of Medical Genetics Part A vol 158no 5 pp 1083ndash1094 2012
[23] I F M Lo C Brewer N Shannon et al ldquoSevere neonatal man-ifestations of Costello syndromerdquo Journal of Medical Geneticsvol 45 no 3 pp 167ndash171 2008
[24] J Menke S Pauli M Sigler et al ldquoUniparental trisomy of amutated HRASproto-oncogene in embryonal rhabdomyosar-coma of a patient with costello syndromerdquo Journal of ClinicalOncology vol 33 no 13 pp e62ndashe65 2015
[25] C P Kratz L Franke H Peters et al ldquoCancer spectrum andfrequency among children with Noonan Costello and cardio-facio-cutaneous syndromesrdquo British Journal of Cancer vol 112no 8 pp 1392ndash1397 2015
[26] H K Ransom ldquoSarcoma of the urachus review of the literaturewith report of an additional caserdquo The American Journal ofSurgery vol 22 no 2 pp 187ndash191 1933
[27] E M L-T Fernandez N H Siverio R L Almaraz L MViota J R Luis and L D Flores ldquoRadical surgery and IVA-chemotherapeutic regimen to treat embryonal rhabdomyosar-coma of the urachus case reportrdquo Pediatric Hematology andOncology vol 24 no 7 pp 543ndash550 2007
[28] M Ishikawa T Nishi R Yamada et al ldquoA case of urachalsarcoma in childhood case report and review of the worldliteraturerdquo Journal of the Japanese Society of Pediatric Surgeonsvol 21 pp 128ndash135 1985
[29] S Yokoyama YHayashida J Nagahama et al ldquoRhabdomyosar-coma of the urachus a case reportrdquo Acta Cytologica vol 41 no4 pp 1293ndash1298 1997
[30] U Schulz and C P OrsquoLeary ldquoSpinal AVM epidermal nevusand rhabdomyosarcoma a rare neurocutaneous syndromerdquoNeurology vol 56 no 3 pp 395ndash397 2001
Case Reports in Genetics 13
[31] A Cheikhelard S Irtan D Orbach et al ldquoUrachal rhab-domyosarcoma in childhood a rare entity with a poor out-comerdquo Journal of Pediatric Surgery vol 50 no 8 pp 1329ndash13332015
[32] K W Gripp E Hopkins K Sol-Church et al ldquoPhenotypicanalysis of individuals with Costello syndrome due to HRASpG13Crdquo American Journal of Medical Genetics Part A vol 155no 4 pp 706ndash716 2011
[33] M Tarnowski G Schneider G Amann et al ldquoRasGRF1 reg-ulates proliferation and metastatic behavior of human alveolarrhabdomyosarcomasrdquo International Journal of Oncology vol 41no 3 pp 995ndash1004 2012
[34] J-S Yu K W Kim H-J Lee Y-J Lee C-S Yoon and M-J Kim ldquoUrachal remnant diseases spectrum of CT and USfindingsrdquo Radiographics vol 21 no 2 pp 451ndash461 2001
[35] C P Kratz S Rapisuwon H Reed H Hasle and P S Rosen-berg ldquoCancer in Noonan Costello cardiofaciocutaneous andLEOPARD syndromesrdquo American Journal of Medical GeneticsPart C Seminars in Medical Genetics vol 157 no 2 pp 83ndash892011
[36] B Kerr M L Mucchielli S Sigaudy et al ldquoIs the locus forCostello syndrome on 11prdquo Journal of Medical Genetics vol 40no 6 pp 469ndash471 2003
[37] TNiihori YAokiNOkamoto et al ldquoHRASmutants identifiedin Costello syndrome patients can induce cellular senescencepossible implications for the pathogenesis of Costello syn-dromerdquo Journal of Human Genetics vol 56 no 10 pp 707ndash7152011
[38] G Rosenberger S Meien and K Kutsche ldquoOncogenic HRASmutations cause prolonged PI3K signaling in response toepidermal growth factor in fibroblasts of patients with costellosyndromerdquo Human Mutation vol 30 no 3 pp 352ndash362 2009
[39] M R DeBaun ldquoScreening for cancer in children with Costellosyndromerdquo American Journal of Medical Genetics vol 108 no1 pp 88ndash90 2002
[40] K W Gripp H Kawame D H Viskochil and L NicholsonldquoElevated catecholamine metabolites in patients with Costellosyndromerdquo American Journal of Medical Genetics vol 128 no1 pp 48ndash51 2004
[41] M-ADelrue B Arveiler andD Lacombe ldquoCostello syndromeclinical features and tumoral riskrdquo Archives de Pediatrie vol 9no 10 pp 1059ndash1063 2002
[42] V Martınez-Gonzalez and P Lapunzina Sındrome de CostelloGrupodeTrabajo sobreCancer en SındromeGeneticos Polimar-formativos (GT-CSGP) httpswwworphanetdatapathoProesCSGP-Costello-3pdf
[43] K A Rauen A Banerjee W R Bishop et al ldquoCostello andcardio-facio-cutaneous syndromes moving toward clinical tri-als in RASopathiesrdquo American Journal of Medical Genetics PartC Seminars inMedical Genetics vol 157 no 2 pp 136ndash146 2011
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

8 Case Reports in Genetics
Table3Ch
aracteris
ticso
fPediatricPatie
ntsw
ithUmbilicalLigamentR
habd
omyosarcom
a
PT number
Author
Year
Cou
ntry
Sex
Age
atdiagno
sis(yearsm
onths)
Symptom
sLo
catio
nSize
(cm)
Histology
IRS
grou
pTh
erapy
Outcome
1Ra
nsom
[2627]
1933
USA
F4m
Massb
elowthe
umbilicus
and
extend
ing
somew
hattothe
right
Urachus
(medianUL)
attached
alon
gthea
nterior
wallfrom
theu
mbilicus
tothea
pexof
theb
ladd
er
115
Spindle
cell
ISM
AC
RT
Lastcheck-up
exam
ination(2
years)
show
edno
evidence
ofrecurrence
2Ishikawae
tal[28]
1985
Japan
F1y
4mAb
dominalmass
abdo
minalpain
hemop
erito
neum
Urachal(m
edianUL)
intra-abdo
minalruptureo
fthetum
or
Fist-
sized
NDF
IVSM
ACNDF
3Yo
koyamae
tal[2729]
1997
Japan
M2y
Episo
diclow
erabdo
minalpain
Urachus
(medianUL)
extraperito
neallocated
betweentheu
mbilicus
and
apex
oftheb
ladd
erandwas
adherin
gtig
htlyto
both
Theb
ilateralm
edialU
Lweres
eenenterin
gthe
tumorR
upturedwith
asm
alln
umbero
fdissem
inated
tumors
scatteredon
them
esentery
andDou
glas
pouch
12Em
bryonal
IVSM
AI
ChT
At2yearso
ffollo
w-upno
recurrence
hadbeen
detected
4lowastKe
rretal
[78]
1998
England
F3y
2mAb
dominalmass
Urachus
(medianUL)
adherent
totheb
ladd
erNDF
Embryonal
IIaSM
II
ChT
Histologyshow
edextend
ingup
tothe
resectionmargin
Diedaged
5years
[59]
5Schu
lzand
OrsquoLeary
[2730]
2001
Scotland
M2y
NDF
Urachus
(medianUL)
NDF
Embryonal
NDF
SCh
TRT
Tumor-fr
eeageo
f26
years
6Fernandeze
tal[27]
2007
Spain
F6y
Intractable
constip
ation
nauseaabd
ominal
painles
smass
Urachus
(medianUL)
infiltratingthev
entral
abdo
minalwalland
fixed
tothev
esicaldo
me
135
Embryonal
IbSM
IC
ChT
At4yearso
ffollo
w-upthep
atient
remains
welland
free
ofclinicald
isease
7lowastMenke
etal
[2425]
2015
Germany
F3y
Abdo
minalmass
Lower
anterio
rabd
omen
abovethe
urinarybladderamp
(urachusm
edianULby
locatio
n)
NDF
Embryonal
IIaSM
II
ChT
R1resection
(marginaltum
orresid
ue)Tu
mor-fr
eeageo
f6years
8Ch
eikh
elard
etal[31]
2015
Dx
1983
France
F5y
5mNDF
Urachus
(medianUL)
periton
ealm
etastasesa
ndhypo
gastric
lymph
nodes
5NDF
IVSM
AI
ChT
Died31
mon
thsa
fter
diagno
siswith
relap
sein
periton
ealliver
at11mon
ths
Case Reports in Genetics 9
Table3Con
tinued
PT number
Author
Year
Cou
ntry
Sex
Age
atdiagno
sis(yearsm
onths)
Symptom
sLo
catio
nSize
(cm)
Histology
IRS
grou
pTh
erapy
Outcome
9Ch
eikh
elard
etal[31]
2015
Dx
2003
France
F3y
3mPeriton
ealrup
ture
poor
generalstatus
Urachus
(medianUL)
lumbo
aorticandexternal
iliac
lymph
nodes
10Alveolar
IVSM
AI
ChTRT
Died57
mon
thsa
fter
diagno
siswith
relap
sein
periton
ealliver
at30
mon
ths
10Ch
eikh
elard
etal[31]
2015
Dx
2005
France
F2y
6mMasspo
orgeneral
statusdysuria
Urachus
(medianUL)
15Em
bryonal
III
SMII
ChTRT
Died37
mon
thsa
fter
diagno
siswith
periton
ealrelapse
at19
mon
ths
11Ch
eikh
elard
etal[31]
2015
Dx
2005
France
M4y
2mMasspo
orgeneral
statusdysuria
Urachus
(medianUL)
periton
ealm
etastasesa
ndiliac
lumbo
aorticlymph
nodes
10Em
bryonal
IVSM
II
ChTRT
Relapsed
multifocalat
82mon
thsfollo
w-up
100mon
ths
12Ch
eikh
elard
etal[31]
2015
Dx
2005
France
M5y
3mMasspo
orgeneral
status
Urachus
(medianUL)
periton
ealm
etastasesa
ndmesenteric
lymph
nodes
106
Embryonal
IVSM
IC
ChTRT
Tumor
freea
fter9
5mon
thssince
diagno
sis
13Ch
eikh
elard
etal[31]
2015
Dx
2006
France
M2y
5mMasspo
orgeneral
statusob
structiv
erenalinsuffi
ciency
Urachus
(medianUL)
periton
ealbon
emetastases
andhypo
gastric
lymph
nodes
21Em
bryonal
IVSM
II
ChTRT
Bone
progression
after
16mon
thsdied
18aft
erdiagno
sis
14Ch
eikh
elard
etal[31]
2015
Dx
2010
France
M4y
5mAb
dominalpain
Urachus
(medianUL)
7Em
bryonal
III
SMIC
ChT
Tumor
freea
fter18
mon
thssince
diagno
sis
15Ch
eikh
elard
etal[31]
2015
Dx
2010
France
M6y
Abdo
minalpain
Urachus
(medianUL)
periton
ealm
etastases
14Em
bryonal
IVSM
AI
ChTRT
Tumor
freea
fter4
5mon
thssince
diagno
sis
16lowast
Sanchez-
Mon
tenegro
etal(this
repo
rt)
2017
Dx
2015
Spain
F2y
4mAs
ymptom
atic
LeftmedialU
L5
Embryonal
IaCh
TSM
IC
RT
Tumor-fr
eeageo
f3yearsa
nd9mon
ths
17lowast
Sanchez-
Mon
tenegro
etal(this
repo
rt)
2017
Dx
2015
Spain
F3y
10m
Asym
ptom
atic
Rightm
edialU
L85
Spindle
cell
IIaSM
II
ChT
Tumor-fr
eeageo
f4yearsa
nd5mon
ths
ChT
chem
otherapyD
xdiagno
sed
Ffemale
IRS
intergroup
rhabdo
myosarcom
aMm
ale
NDF
nodata
foun
dRT
radiotherapy
Ssurgery
SMAIsurgerymacroscop
ically
incomplete
SMAC
surgery
macroscop
icallycompleteSM
ICsurgery
microscop
icallycompleteSM
IIsurgery
microscop
icallyincompleteULum
bilicalligam
ent
ampPerson
alcommun
icationby
authorlowast
Patientsw
ithCostello
synd
rome
10 Case Reports in Genetics
Table 4 Chemotherapy of pediatric patients with umbilical ligament rhabdomyosarcoma
PTnumber Chemotherapy protocol
1-2 No ChT [26 28]3 After establishment of the final diagnosis he was treated with combined ChT including VCR ACD and CTX [29]
4lowastInitially IFOS ACD and VCR After 4 courses CTX was substituted for IFOS because of hemorrhagic cystitis Tx complicatedby recurrent episodes of moderately severe diarrhoea and febrile neutropenia requiring readmission to hospital Tx wascompleted after six courses of ChT [7]
5 NDF [30]
6 PT started induction of ChT 2 weeks after S Induction regimen included 9 cycles of IVA (IFOS VCR and ACD) that were welltolerated with minimal systemic complications (Tx 953 of the MMT 95 SIOP protocol for RMS) [27]
7lowast ChT according to the cooperative soft tissue sarcoma protocol (CWS-2002 P) was well tolerated by the PT [24]8 Adjuvant ChT with 10 cycles of IFOS VCR and ACD [31]9 Adjuvant ChT with 6 cycles of IFOS VCR and VP-16 and 9 cycles of VCR ACD CTXACD and CTX [31]10 Neoadjuvant ChT with 6 cycles of IFOS VCR and ACD and adjuvant ChT with 3 cycles of IFOS VCR and ACD [31]
11 Neoadjuvant ChT with 1 cycle of CTX VCR and PRED 2 cycles IFOS VCR and ACD and 4 cycles of IFOS VCR ACD andDOX and adjuvant ChT with 3 cycles of IFOS VCR and ACD [31]
12 Neoadjuvant ChT with 1 cycle of CTX VCR and PRED and 5 cycles of IFOS VCR ACD and DOX and adjuvant ChT with 2cycles of IFOS VCR ACD and DOX and 1 cycle of IFOS VCR and ACD [31]
13 Neoadjuvant ChT with 2 cycles of VCR ACD and CTX + and 3 cycles of IFOS VCR ACD and DOX and adjuvant ChT with 3cycles of IFOS VCR and ACD [31]
14 Neoadjuvant ChT with 4 cycles of IFOS VCR ACD and DOX and adjuvant ChT with 5 cycles of IFOS VCR ACD [31]
15 Neoadjuvant ChT with 4 cycles of IFOS VCR ACD DOX 3 cycles of IFOS VCR ACD and adjuvant ChT with 1 cycle of IFOSVCR ACD 1 cycle of IFOS VCR [31]
16lowastChT in the standard risk group protocol EpSSG RMS 2005 subgroup D 3 preoperative cycles of IFOS (2 doses at 100mgkg)VCR (005mgkg) and ACD (005mgkg)
17lowastChT (postoperative 15 days) in the standard risk group protocol EpSSG RMS 2005 subgroup B (Stage I) cycles of IFOS (2 dosesof 3 gm2d) VCR (15mgm2) and ACD (15mgm2) was initiated
ACD actinomycin D ChT chemotherapy CTX cyclophosphamide CWS Cooperative Weichteilsarkom Studie (Cooperative Soft Tissue Sarcoma Study)DOX Doxorubicin EpSSG European pediatric Soft tissue sarcoma Study Group IFOS ifosfamide MMT malignant mesenchymal tumor NDF no datafound PRED prednisone PT patient RMS rhabdomyosarcoma S surgery SIOP Societe Internationale DrsquoOncologie Pediatrique (International Society ofPediatric Oncology) Tx treatment VCR vincristine VP-16 etoposide lowastPatients with Costello syndrome
that alveolar RMS and embryonal RMS are two differentdisorders while alveolar RMS may originate from primitiveuncommitted mesodermal cells embryonal RMS originatesprobably from more differentiated myoblasts Ras protein-specific guanine nucleotide-releasing factor 1 (RasGRF1)plays an important role in alveolar RMS pathogenesis Theseinteresting concepts however need more evidence [33]
The umbilicus caudally originates the common ligamentwhich is divided into obliterated umbilical arteries (medialUL) and urachus (median UL) The urachus varies from3 to 10 cm in length and from 8 to 10mm in diameterIt is a three-layered tubular structure the innermost layerbeing lined with transitional epithelium in 70 of casesand with columnar epithelium in 30 The structure issurrounded by connective tissue and outermost muscularlayer in continuity with the detrusor muscle Along its pathfrom the bladder to the umbilicus the urachus lies betweenthe transverse fascia and the parietal peritoneum containedin the pyramidal retropubic perivesical preperitoneal spacecompartmentalized by umbilicovesical fascia along with themedial umbilical ligaments and the bladder Occasionallythe urachus may merge with one or both of the obliteratedumbilical arteries (medial UL) and there may be a slight
deviation to the right or left of the midline [34] The urachusis an embryological remnant resulting from the obliterationof the allantoic channel which attaches the bladder dome tothe umbilicus [31]
Urachal malignant tumors are extremely rare represent-ing less than 05 of all bladder cancers and 001 of alltumors They may arise from any portion of the urachus andare most commonly found in adults and males (60ndash70)Although sarcomas represent only 8 they are the mostfrequent urachal neoplasms reported in patients youngerthan 20 years of age (67) [27] Poor prognosis is a commonfeature in adults and pediatric urachalmalignancies with 50to 60 of 5-year survival In contrast the 5-year event-freesurvival in pelvic RMS was reported to be about 51 [31]
This indolent and rather large urachal tumor was mostlyrevealed by an uncomplicated progressing mass withoutprodromic urological symptomsThedelay of diagnosis couldbe explained by a long asymptomatic progression of thetumor in a preperitoneal location which allows an importantlocal spreading before diagnosis Even in patients withouttumor rupture peritoneal involvement appeared to be the keypoint in the prognosis of urachal RMS Systematic cytologyat diagnosis could be more accurate to evaluate peritoneal
Case Reports in Genetics 11
extension in order to avoid understaging and adjust adjuvantlocoregional treatment [31]
Previously only 12 patients with RMS arising from theurachus (median UL) in children without CS have beenreported in the English literature (Table 3) By 2011 therewere29 reported cases of cancer in patients withCS 19 RMS (meanage of 23 years 9 embryonal 1 alveolar 1 mixed histology1 pleomorphic 1 spindle cell type and 6 unclassified) 5neuroblastomas 4 bladder cancer and 1 fibrosarcoma [35]
Loss of heterozygosity for 11p155 in RMS from individu-als with CS suggests that loss of the wild-type allele is the sec-ond hit in tumor development [6 16 36] Whereas theHRASmutation in a sporadic malignancy in the general populationis present only within the tumor cells in CS an identicalmutation is present in every single cell of the individualthus accounting for the tumor predisposition [1] implicatingan alternate mechanism of rhabdomyosarcogenesis [16] Inaddition one patient with CS and uniparental trisomy dueto triplication of the mutated paternal HRAS gene was alsoreported RMS typically displays loss of heterozygosity ofthe 11p155 region because of paternal uniparental disomyand approximately 28 of cases harbor mutations in genesof growth signaling pathways In reports of uniparentaldisomy plus HRAS mutation the latter was heterozygousand therefore must have occurred after the developmentof uniparental disomy [24] The functional analysis alsorevealed that CS-causing mutant HRAS proteins causedoncogene-induced senescence in human fibroblasts [37]Theimportant role of PI3K-protein-kinase B (AKT) signalingin Ras-mediated transformation and tumorigenesis is high-lighted by constitutive AKT activation in RMS cell lines andclinical samples Thus prolonged PI3K-AKT signaling mightalso be implicated in the development of soft tissue sarcomain patients with CS [38]
Only four out of 11 patients were diagnosed with CS priorto the RMS diagnosis in 5 patients CS was diagnosed afterthe RMS and in the remaining 2 the order was unknown[20] In 2003 a further three unpublished cases of RMS inchildren with CS were known through the International CSSupport Group [18] and for that reason there is possiblyunderdiagnosis of RMS in patients with CS
A screening protocol was proposed consisting of ultra-sound examination of the abdomen and pelvis every 3ndash6 months until age of 8ndash10 years for RMS and abdomi-nal neuroblastoma urine catecholamine metabolite analysisevery 6ndash12 months until age of 5 years for neuroblastomaand urinalysis for hematuria annually for bladder carcinomaafter age of 10 years The prior diagnosis of CS was theprerequisite for the implementation of a tumor screeningprotocol [8] The recommendation based on the presumedfast doubling time of RMS was abdominal sonographyscreening for RMS that should be done in similar intervalsof every four months until stronger evidence would suggestotherwise [39] Screening for neuroblastoma is no longerrecommended becausemany CS patients without identifiabletumor show elevated catecholamine metabolites in urine itappears that in this patient group an elevation above thenormal limit defined as 2 standard deviations (SD) above themean for age is more likely to be a variant rather than a sign
of a neuroblastoma [1 40] A French monitoring protocolproposed the determination of catecholamines and theirmetabolites in urine every six months until the age of 5 yearsand ultrasound abdominopelvic every six months until theend of the puberty seeking hematuria dipstick from6monthsto the age of 10 [41] The protocol in our hospital for patientswith CS includes an abdominal and pelvic ultrasound 3times during the first year of life and in childhood every 6months until age of 10 [42] We believe that the best optionis to perform a pelvic abdominal ultrasound every 3 monthsduring the first eight years of life and then controls accordingto medical criteria This is even more necessary in patientswith possible UL RMS because diagnosis was usually done inadvanced stages with a poor survival It is possible that withclose monitoring after an early diagnosis will detect initialstages of the tumor in previously not described locations
Head and neck MRI scans can be performed less fre-quently Ear examination and tympanometry every 4 to 6months to detect middle ear effusion which would raisesuspicion for a nasopharyngeal mass are also recommended[6]
The outcome of CS patients with RMS has been compa-rable to that for patients without the syndrome with a 5-yearsurvival rate of 65 to 70 [19] but according to this reviewit could be worse than the general population Neoplasia wasnoted at the cause of death in five (22) patients with CS[4 15] but in our study the mortality associated with RMSwas 43 Because the long-term survival in RMS is basedon the histology of the tumor and the extent of disease atdiagnosis early diagnosis may alter the treatment regimenand improve prognosis This could be particularly importantin patients with CS who often are medically fragile [20]
The RasMAPK pathway is an attractive target in thetreatment of cancer utilizing small molecule therapeuticsthat specifically inhibits the pathway Ras pathway agentssuch as farnesyltransferase inhibitors (tipifarnib and lona-farnib) that prevent posttranslational modification of Rasare being evaluated for cancer treatment and may be oftherapeutic use for syndromes in this pathway especially CSIn addition B-Raf protooncogene serinethreonine kinase(BRAF) and mitogenextracellular signal-regulated kinase(MEK) inhibitors offer the same potential in the possibletreatment of CS Since the RasMAPK pathway has targets forinhibition in cancer treatment there aremany smallmoleculetherapeutics that are in development or undergoing clinicaltrials with some already FDA approval [43]
6 ConclusionsCS is a syndrome poorly known in oncology but theirpredisposition tomalignancies includingULRMS implies theneed for a new perspective on early diagnosis and aggressivemedical and surgical treatment
ConsentInformed consent was obtained from the new two individualparticipants included in the study and has been properlydocumented with the parental approval to the use of patientrsquosimages and complementary studies
12 Case Reports in Genetics
Competing Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
Special thanks are due to Israel Fernandez Pineda MDAssistantMember and Surgery Fellowship ProgramDirectorSt Jude Childrenrsquos Research Hospital (Memphis TN) for therecommendations and corrections to the manuscript
References
[1] E Quezada and K W Gripp ldquoCostello syndrome and relateddisordersrdquo Current Opinion in Pediatrics vol 19 no 6 pp 636ndash644 2007
[2] JM Costello ldquoA new syndromerdquoNewZealandMedical Journalvol 74 article 397 1971
[3] JMCostello ldquoAnew syndromemental subnormality andnasalpapillomatardquo Australian Paediatric Journal vol 13 no 2 pp114ndash118 1977
[4] K W Gripp and A E Lin ldquoCostello syndrome a Rasmitogenactivated protein kinase pathway syndrome (rasopathy) result-ing from HRAS germline mutationsrdquo Genetics in Medicine vol14 no 3 pp 285ndash292 2012
[5] B Kerr M-A Delrue S Sigaudy et al ldquoGenotype-phenotypecorrelation in Costello syndrome HRAS mutation analysis in43 casesrdquo Journal of Medical Genetics vol 43 no 5 pp 401ndash4052006
[6] N Ahmadi and E Harley ldquoCostello syndrome and the impor-tance of cancer screeningrdquo Archives of OtolaryngologymdashHeadand Neck Surgery vol 136 no 10 pp 1028ndash1029 2010
[7] B Kerr O B Eden R Dandamudi et al ldquoCostello syndrometwo cases with embryonal rhabdomyosarcomardquo Journal ofMedical Genetics vol 35 no 12 pp 1036ndash1039 1998
[8] K W Gripp C I Scott Jr L Nicholson et al ldquoFive additionalCostello syndrome patients with rhabdomyosarcoma proposalfor a tumor screening protocolrdquo American Journal of MedicalGenetics vol 108 no 1 pp 80ndash87 2002
[9] K W Gripp A E Lin D L Stabley et al ldquoHRAS mutationanalysis in Costello syndrome genotype and phenotype corre-lationrdquo American Journal of Medical Genetics Part A vol 140no 1 pp 1ndash7 2006
[10] M Feingold ldquoCostello syndrome and rhabdomyosarcomardquoJournal of Medical Genetics vol 36 no 7 pp 582ndash583 1999
[11] S M White J M Graham Jr B Kerr et al ldquoThe adultphenotype in Costello syndromerdquo American Journal of MedicalGenetics A vol 136 no 2 pp 128ndash135 2005
[12] G Bisogno A Murgia I Mammi M S Strafella and M CarlildquoRhabdomyosarcoma in a patient with cardio-facio-cutaneoussyndromerdquo Journal of Pediatric HematologyOncology vol 21no 5 pp 424ndash427 1999
[13] S Sigaudy G Vittu A David et al ldquoCostello syndrome reportof six patients including one with an embryonal rhabdomyosar-comardquoEuropean Journal of Pediatrics vol 159 no 3 pp 139ndash1422000
[14] A Hinek M A Teitell L Schoyer et al ldquoMyocardial storage ofchondroitin sulfate-containing moieties in Costello syndromepatients with severe hypertrophic cardiomyopathyrdquo AmericanJournal of Medical Genetics vol 133 no 1 pp 1ndash12 2005
[15] A E Lin P D Grossfeld R M Hamilton et al ldquoFurtherdelineation of cardiac abnormalities in Costello syndromerdquoAmerican Journal of Medical Genetics vol 111 no 2 pp 115ndash1292002
[16] A L Estep W E Tidyman M A Teitell P D Cotter and KA Rauen ldquoHRASmutations in Costello syndrome detection ofconstitutional activating mutations in codon 12 and 13 and lossof wild-type allele in malignancyrdquo American Journal of MedicalGenetics vol 140 no 1 pp 8ndash16 2006
[17] H KawameMMatsui K Kurosawa et al ldquoFurther delineationof the behavioral and neurologic features inCostello syndromerdquoAmerican Journal of Medical Genetics vol 118A no 1 pp 8ndash142003
[18] B Kerr M A Einaudi P Clayton et al ldquoIs growth hormonetreatment beneficial or harmful in Costello syndromerdquo Journalof medical genetics vol 40 no 6 article e74 2003
[19] J P OrsquoNeal J Ramdas W E Wood and P K PellitterildquoParameningeal rhabdomyosarcoma in a patient with Costellosyndromerdquo Journal of Pediatric HematologyOncology vol 26no 6 pp 389ndash392 2004
[20] K W Gripp ldquoTumor predisposition in Costello syndromerdquoAmerican Journal of Medical Genetics Part C Seminars inMedical Genetics vol 137C no 1 pp 72ndash77 2005
[21] Y Aoki T Niihori H Kawame et al ldquoGermline mutationsin HRAS proto-oncogene cause Costello syndromerdquo NatureGenetics vol 37 no 10 pp 1038ndash1040 2005
[22] Y Abe Y Aoki S Kuriyama et al ldquoPrevalence and clinicalfeatures of Costello syndrome and cardio-facio-cutaneous syn-drome in Japan findings from a nationwide epidemiologicalsurveyrdquo American Journal of Medical Genetics Part A vol 158no 5 pp 1083ndash1094 2012
[23] I F M Lo C Brewer N Shannon et al ldquoSevere neonatal man-ifestations of Costello syndromerdquo Journal of Medical Geneticsvol 45 no 3 pp 167ndash171 2008
[24] J Menke S Pauli M Sigler et al ldquoUniparental trisomy of amutated HRASproto-oncogene in embryonal rhabdomyosar-coma of a patient with costello syndromerdquo Journal of ClinicalOncology vol 33 no 13 pp e62ndashe65 2015
[25] C P Kratz L Franke H Peters et al ldquoCancer spectrum andfrequency among children with Noonan Costello and cardio-facio-cutaneous syndromesrdquo British Journal of Cancer vol 112no 8 pp 1392ndash1397 2015
[26] H K Ransom ldquoSarcoma of the urachus review of the literaturewith report of an additional caserdquo The American Journal ofSurgery vol 22 no 2 pp 187ndash191 1933
[27] E M L-T Fernandez N H Siverio R L Almaraz L MViota J R Luis and L D Flores ldquoRadical surgery and IVA-chemotherapeutic regimen to treat embryonal rhabdomyosar-coma of the urachus case reportrdquo Pediatric Hematology andOncology vol 24 no 7 pp 543ndash550 2007
[28] M Ishikawa T Nishi R Yamada et al ldquoA case of urachalsarcoma in childhood case report and review of the worldliteraturerdquo Journal of the Japanese Society of Pediatric Surgeonsvol 21 pp 128ndash135 1985
[29] S Yokoyama YHayashida J Nagahama et al ldquoRhabdomyosar-coma of the urachus a case reportrdquo Acta Cytologica vol 41 no4 pp 1293ndash1298 1997
[30] U Schulz and C P OrsquoLeary ldquoSpinal AVM epidermal nevusand rhabdomyosarcoma a rare neurocutaneous syndromerdquoNeurology vol 56 no 3 pp 395ndash397 2001
Case Reports in Genetics 13
[31] A Cheikhelard S Irtan D Orbach et al ldquoUrachal rhab-domyosarcoma in childhood a rare entity with a poor out-comerdquo Journal of Pediatric Surgery vol 50 no 8 pp 1329ndash13332015
[32] K W Gripp E Hopkins K Sol-Church et al ldquoPhenotypicanalysis of individuals with Costello syndrome due to HRASpG13Crdquo American Journal of Medical Genetics Part A vol 155no 4 pp 706ndash716 2011
[33] M Tarnowski G Schneider G Amann et al ldquoRasGRF1 reg-ulates proliferation and metastatic behavior of human alveolarrhabdomyosarcomasrdquo International Journal of Oncology vol 41no 3 pp 995ndash1004 2012
[34] J-S Yu K W Kim H-J Lee Y-J Lee C-S Yoon and M-J Kim ldquoUrachal remnant diseases spectrum of CT and USfindingsrdquo Radiographics vol 21 no 2 pp 451ndash461 2001
[35] C P Kratz S Rapisuwon H Reed H Hasle and P S Rosen-berg ldquoCancer in Noonan Costello cardiofaciocutaneous andLEOPARD syndromesrdquo American Journal of Medical GeneticsPart C Seminars in Medical Genetics vol 157 no 2 pp 83ndash892011
[36] B Kerr M L Mucchielli S Sigaudy et al ldquoIs the locus forCostello syndrome on 11prdquo Journal of Medical Genetics vol 40no 6 pp 469ndash471 2003
[37] TNiihori YAokiNOkamoto et al ldquoHRASmutants identifiedin Costello syndrome patients can induce cellular senescencepossible implications for the pathogenesis of Costello syn-dromerdquo Journal of Human Genetics vol 56 no 10 pp 707ndash7152011
[38] G Rosenberger S Meien and K Kutsche ldquoOncogenic HRASmutations cause prolonged PI3K signaling in response toepidermal growth factor in fibroblasts of patients with costellosyndromerdquo Human Mutation vol 30 no 3 pp 352ndash362 2009
[39] M R DeBaun ldquoScreening for cancer in children with Costellosyndromerdquo American Journal of Medical Genetics vol 108 no1 pp 88ndash90 2002
[40] K W Gripp H Kawame D H Viskochil and L NicholsonldquoElevated catecholamine metabolites in patients with Costellosyndromerdquo American Journal of Medical Genetics vol 128 no1 pp 48ndash51 2004
[41] M-ADelrue B Arveiler andD Lacombe ldquoCostello syndromeclinical features and tumoral riskrdquo Archives de Pediatrie vol 9no 10 pp 1059ndash1063 2002
[42] V Martınez-Gonzalez and P Lapunzina Sındrome de CostelloGrupodeTrabajo sobreCancer en SındromeGeneticos Polimar-formativos (GT-CSGP) httpswwworphanetdatapathoProesCSGP-Costello-3pdf
[43] K A Rauen A Banerjee W R Bishop et al ldquoCostello andcardio-facio-cutaneous syndromes moving toward clinical tri-als in RASopathiesrdquo American Journal of Medical Genetics PartC Seminars inMedical Genetics vol 157 no 2 pp 136ndash146 2011
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Case Reports in Genetics 9
Table3Con
tinued
PT number
Author
Year
Cou
ntry
Sex
Age
atdiagno
sis(yearsm
onths)
Symptom
sLo
catio
nSize
(cm)
Histology
IRS
grou
pTh
erapy
Outcome
9Ch
eikh
elard
etal[31]
2015
Dx
2003
France
F3y
3mPeriton
ealrup
ture
poor
generalstatus
Urachus
(medianUL)
lumbo
aorticandexternal
iliac
lymph
nodes
10Alveolar
IVSM
AI
ChTRT
Died57
mon
thsa
fter
diagno
siswith
relap
sein
periton
ealliver
at30
mon
ths
10Ch
eikh
elard
etal[31]
2015
Dx
2005
France
F2y
6mMasspo
orgeneral
statusdysuria
Urachus
(medianUL)
15Em
bryonal
III
SMII
ChTRT
Died37
mon
thsa
fter
diagno
siswith
periton
ealrelapse
at19
mon
ths
11Ch
eikh
elard
etal[31]
2015
Dx
2005
France
M4y
2mMasspo
orgeneral
statusdysuria
Urachus
(medianUL)
periton
ealm
etastasesa
ndiliac
lumbo
aorticlymph
nodes
10Em
bryonal
IVSM
II
ChTRT
Relapsed
multifocalat
82mon
thsfollo
w-up
100mon
ths
12Ch
eikh
elard
etal[31]
2015
Dx
2005
France
M5y
3mMasspo
orgeneral
status
Urachus
(medianUL)
periton
ealm
etastasesa
ndmesenteric
lymph
nodes
106
Embryonal
IVSM
IC
ChTRT
Tumor
freea
fter9
5mon
thssince
diagno
sis
13Ch
eikh
elard
etal[31]
2015
Dx
2006
France
M2y
5mMasspo
orgeneral
statusob
structiv
erenalinsuffi
ciency
Urachus
(medianUL)
periton
ealbon
emetastases
andhypo
gastric
lymph
nodes
21Em
bryonal
IVSM
II
ChTRT
Bone
progression
after
16mon
thsdied
18aft
erdiagno
sis
14Ch
eikh
elard
etal[31]
2015
Dx
2010
France
M4y
5mAb
dominalpain
Urachus
(medianUL)
7Em
bryonal
III
SMIC
ChT
Tumor
freea
fter18
mon
thssince
diagno
sis
15Ch
eikh
elard
etal[31]
2015
Dx
2010
France
M6y
Abdo
minalpain
Urachus
(medianUL)
periton
ealm
etastases
14Em
bryonal
IVSM
AI
ChTRT
Tumor
freea
fter4
5mon
thssince
diagno
sis
16lowast
Sanchez-
Mon
tenegro
etal(this
repo
rt)
2017
Dx
2015
Spain
F2y
4mAs
ymptom
atic
LeftmedialU
L5
Embryonal
IaCh
TSM
IC
RT
Tumor-fr
eeageo
f3yearsa
nd9mon
ths
17lowast
Sanchez-
Mon
tenegro
etal(this
repo
rt)
2017
Dx
2015
Spain
F3y
10m
Asym
ptom
atic
Rightm
edialU
L85
Spindle
cell
IIaSM
II
ChT
Tumor-fr
eeageo
f4yearsa
nd5mon
ths
ChT
chem
otherapyD
xdiagno
sed
Ffemale
IRS
intergroup
rhabdo
myosarcom
aMm
ale
NDF
nodata
foun
dRT
radiotherapy
Ssurgery
SMAIsurgerymacroscop
ically
incomplete
SMAC
surgery
macroscop
icallycompleteSM
ICsurgery
microscop
icallycompleteSM
IIsurgery
microscop
icallyincompleteULum
bilicalligam
ent
ampPerson
alcommun
icationby
authorlowast
Patientsw
ithCostello
synd
rome
10 Case Reports in Genetics
Table 4 Chemotherapy of pediatric patients with umbilical ligament rhabdomyosarcoma
PTnumber Chemotherapy protocol
1-2 No ChT [26 28]3 After establishment of the final diagnosis he was treated with combined ChT including VCR ACD and CTX [29]
4lowastInitially IFOS ACD and VCR After 4 courses CTX was substituted for IFOS because of hemorrhagic cystitis Tx complicatedby recurrent episodes of moderately severe diarrhoea and febrile neutropenia requiring readmission to hospital Tx wascompleted after six courses of ChT [7]
5 NDF [30]
6 PT started induction of ChT 2 weeks after S Induction regimen included 9 cycles of IVA (IFOS VCR and ACD) that were welltolerated with minimal systemic complications (Tx 953 of the MMT 95 SIOP protocol for RMS) [27]
7lowast ChT according to the cooperative soft tissue sarcoma protocol (CWS-2002 P) was well tolerated by the PT [24]8 Adjuvant ChT with 10 cycles of IFOS VCR and ACD [31]9 Adjuvant ChT with 6 cycles of IFOS VCR and VP-16 and 9 cycles of VCR ACD CTXACD and CTX [31]10 Neoadjuvant ChT with 6 cycles of IFOS VCR and ACD and adjuvant ChT with 3 cycles of IFOS VCR and ACD [31]
11 Neoadjuvant ChT with 1 cycle of CTX VCR and PRED 2 cycles IFOS VCR and ACD and 4 cycles of IFOS VCR ACD andDOX and adjuvant ChT with 3 cycles of IFOS VCR and ACD [31]
12 Neoadjuvant ChT with 1 cycle of CTX VCR and PRED and 5 cycles of IFOS VCR ACD and DOX and adjuvant ChT with 2cycles of IFOS VCR ACD and DOX and 1 cycle of IFOS VCR and ACD [31]
13 Neoadjuvant ChT with 2 cycles of VCR ACD and CTX + and 3 cycles of IFOS VCR ACD and DOX and adjuvant ChT with 3cycles of IFOS VCR and ACD [31]
14 Neoadjuvant ChT with 4 cycles of IFOS VCR ACD and DOX and adjuvant ChT with 5 cycles of IFOS VCR ACD [31]
15 Neoadjuvant ChT with 4 cycles of IFOS VCR ACD DOX 3 cycles of IFOS VCR ACD and adjuvant ChT with 1 cycle of IFOSVCR ACD 1 cycle of IFOS VCR [31]
16lowastChT in the standard risk group protocol EpSSG RMS 2005 subgroup D 3 preoperative cycles of IFOS (2 doses at 100mgkg)VCR (005mgkg) and ACD (005mgkg)
17lowastChT (postoperative 15 days) in the standard risk group protocol EpSSG RMS 2005 subgroup B (Stage I) cycles of IFOS (2 dosesof 3 gm2d) VCR (15mgm2) and ACD (15mgm2) was initiated
ACD actinomycin D ChT chemotherapy CTX cyclophosphamide CWS Cooperative Weichteilsarkom Studie (Cooperative Soft Tissue Sarcoma Study)DOX Doxorubicin EpSSG European pediatric Soft tissue sarcoma Study Group IFOS ifosfamide MMT malignant mesenchymal tumor NDF no datafound PRED prednisone PT patient RMS rhabdomyosarcoma S surgery SIOP Societe Internationale DrsquoOncologie Pediatrique (International Society ofPediatric Oncology) Tx treatment VCR vincristine VP-16 etoposide lowastPatients with Costello syndrome
that alveolar RMS and embryonal RMS are two differentdisorders while alveolar RMS may originate from primitiveuncommitted mesodermal cells embryonal RMS originatesprobably from more differentiated myoblasts Ras protein-specific guanine nucleotide-releasing factor 1 (RasGRF1)plays an important role in alveolar RMS pathogenesis Theseinteresting concepts however need more evidence [33]
The umbilicus caudally originates the common ligamentwhich is divided into obliterated umbilical arteries (medialUL) and urachus (median UL) The urachus varies from3 to 10 cm in length and from 8 to 10mm in diameterIt is a three-layered tubular structure the innermost layerbeing lined with transitional epithelium in 70 of casesand with columnar epithelium in 30 The structure issurrounded by connective tissue and outermost muscularlayer in continuity with the detrusor muscle Along its pathfrom the bladder to the umbilicus the urachus lies betweenthe transverse fascia and the parietal peritoneum containedin the pyramidal retropubic perivesical preperitoneal spacecompartmentalized by umbilicovesical fascia along with themedial umbilical ligaments and the bladder Occasionallythe urachus may merge with one or both of the obliteratedumbilical arteries (medial UL) and there may be a slight
deviation to the right or left of the midline [34] The urachusis an embryological remnant resulting from the obliterationof the allantoic channel which attaches the bladder dome tothe umbilicus [31]
Urachal malignant tumors are extremely rare represent-ing less than 05 of all bladder cancers and 001 of alltumors They may arise from any portion of the urachus andare most commonly found in adults and males (60ndash70)Although sarcomas represent only 8 they are the mostfrequent urachal neoplasms reported in patients youngerthan 20 years of age (67) [27] Poor prognosis is a commonfeature in adults and pediatric urachalmalignancies with 50to 60 of 5-year survival In contrast the 5-year event-freesurvival in pelvic RMS was reported to be about 51 [31]
This indolent and rather large urachal tumor was mostlyrevealed by an uncomplicated progressing mass withoutprodromic urological symptomsThedelay of diagnosis couldbe explained by a long asymptomatic progression of thetumor in a preperitoneal location which allows an importantlocal spreading before diagnosis Even in patients withouttumor rupture peritoneal involvement appeared to be the keypoint in the prognosis of urachal RMS Systematic cytologyat diagnosis could be more accurate to evaluate peritoneal
Case Reports in Genetics 11
extension in order to avoid understaging and adjust adjuvantlocoregional treatment [31]
Previously only 12 patients with RMS arising from theurachus (median UL) in children without CS have beenreported in the English literature (Table 3) By 2011 therewere29 reported cases of cancer in patients withCS 19 RMS (meanage of 23 years 9 embryonal 1 alveolar 1 mixed histology1 pleomorphic 1 spindle cell type and 6 unclassified) 5neuroblastomas 4 bladder cancer and 1 fibrosarcoma [35]
Loss of heterozygosity for 11p155 in RMS from individu-als with CS suggests that loss of the wild-type allele is the sec-ond hit in tumor development [6 16 36] Whereas theHRASmutation in a sporadic malignancy in the general populationis present only within the tumor cells in CS an identicalmutation is present in every single cell of the individualthus accounting for the tumor predisposition [1] implicatingan alternate mechanism of rhabdomyosarcogenesis [16] Inaddition one patient with CS and uniparental trisomy dueto triplication of the mutated paternal HRAS gene was alsoreported RMS typically displays loss of heterozygosity ofthe 11p155 region because of paternal uniparental disomyand approximately 28 of cases harbor mutations in genesof growth signaling pathways In reports of uniparentaldisomy plus HRAS mutation the latter was heterozygousand therefore must have occurred after the developmentof uniparental disomy [24] The functional analysis alsorevealed that CS-causing mutant HRAS proteins causedoncogene-induced senescence in human fibroblasts [37]Theimportant role of PI3K-protein-kinase B (AKT) signalingin Ras-mediated transformation and tumorigenesis is high-lighted by constitutive AKT activation in RMS cell lines andclinical samples Thus prolonged PI3K-AKT signaling mightalso be implicated in the development of soft tissue sarcomain patients with CS [38]
Only four out of 11 patients were diagnosed with CS priorto the RMS diagnosis in 5 patients CS was diagnosed afterthe RMS and in the remaining 2 the order was unknown[20] In 2003 a further three unpublished cases of RMS inchildren with CS were known through the International CSSupport Group [18] and for that reason there is possiblyunderdiagnosis of RMS in patients with CS
A screening protocol was proposed consisting of ultra-sound examination of the abdomen and pelvis every 3ndash6 months until age of 8ndash10 years for RMS and abdomi-nal neuroblastoma urine catecholamine metabolite analysisevery 6ndash12 months until age of 5 years for neuroblastomaand urinalysis for hematuria annually for bladder carcinomaafter age of 10 years The prior diagnosis of CS was theprerequisite for the implementation of a tumor screeningprotocol [8] The recommendation based on the presumedfast doubling time of RMS was abdominal sonographyscreening for RMS that should be done in similar intervalsof every four months until stronger evidence would suggestotherwise [39] Screening for neuroblastoma is no longerrecommended becausemany CS patients without identifiabletumor show elevated catecholamine metabolites in urine itappears that in this patient group an elevation above thenormal limit defined as 2 standard deviations (SD) above themean for age is more likely to be a variant rather than a sign
of a neuroblastoma [1 40] A French monitoring protocolproposed the determination of catecholamines and theirmetabolites in urine every six months until the age of 5 yearsand ultrasound abdominopelvic every six months until theend of the puberty seeking hematuria dipstick from6monthsto the age of 10 [41] The protocol in our hospital for patientswith CS includes an abdominal and pelvic ultrasound 3times during the first year of life and in childhood every 6months until age of 10 [42] We believe that the best optionis to perform a pelvic abdominal ultrasound every 3 monthsduring the first eight years of life and then controls accordingto medical criteria This is even more necessary in patientswith possible UL RMS because diagnosis was usually done inadvanced stages with a poor survival It is possible that withclose monitoring after an early diagnosis will detect initialstages of the tumor in previously not described locations
Head and neck MRI scans can be performed less fre-quently Ear examination and tympanometry every 4 to 6months to detect middle ear effusion which would raisesuspicion for a nasopharyngeal mass are also recommended[6]
The outcome of CS patients with RMS has been compa-rable to that for patients without the syndrome with a 5-yearsurvival rate of 65 to 70 [19] but according to this reviewit could be worse than the general population Neoplasia wasnoted at the cause of death in five (22) patients with CS[4 15] but in our study the mortality associated with RMSwas 43 Because the long-term survival in RMS is basedon the histology of the tumor and the extent of disease atdiagnosis early diagnosis may alter the treatment regimenand improve prognosis This could be particularly importantin patients with CS who often are medically fragile [20]
The RasMAPK pathway is an attractive target in thetreatment of cancer utilizing small molecule therapeuticsthat specifically inhibits the pathway Ras pathway agentssuch as farnesyltransferase inhibitors (tipifarnib and lona-farnib) that prevent posttranslational modification of Rasare being evaluated for cancer treatment and may be oftherapeutic use for syndromes in this pathway especially CSIn addition B-Raf protooncogene serinethreonine kinase(BRAF) and mitogenextracellular signal-regulated kinase(MEK) inhibitors offer the same potential in the possibletreatment of CS Since the RasMAPK pathway has targets forinhibition in cancer treatment there aremany smallmoleculetherapeutics that are in development or undergoing clinicaltrials with some already FDA approval [43]
6 ConclusionsCS is a syndrome poorly known in oncology but theirpredisposition tomalignancies includingULRMS implies theneed for a new perspective on early diagnosis and aggressivemedical and surgical treatment
ConsentInformed consent was obtained from the new two individualparticipants included in the study and has been properlydocumented with the parental approval to the use of patientrsquosimages and complementary studies
12 Case Reports in Genetics
Competing Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
Special thanks are due to Israel Fernandez Pineda MDAssistantMember and Surgery Fellowship ProgramDirectorSt Jude Childrenrsquos Research Hospital (Memphis TN) for therecommendations and corrections to the manuscript
References
[1] E Quezada and K W Gripp ldquoCostello syndrome and relateddisordersrdquo Current Opinion in Pediatrics vol 19 no 6 pp 636ndash644 2007
[2] JM Costello ldquoA new syndromerdquoNewZealandMedical Journalvol 74 article 397 1971
[3] JMCostello ldquoAnew syndromemental subnormality andnasalpapillomatardquo Australian Paediatric Journal vol 13 no 2 pp114ndash118 1977
[4] K W Gripp and A E Lin ldquoCostello syndrome a Rasmitogenactivated protein kinase pathway syndrome (rasopathy) result-ing from HRAS germline mutationsrdquo Genetics in Medicine vol14 no 3 pp 285ndash292 2012
[5] B Kerr M-A Delrue S Sigaudy et al ldquoGenotype-phenotypecorrelation in Costello syndrome HRAS mutation analysis in43 casesrdquo Journal of Medical Genetics vol 43 no 5 pp 401ndash4052006
[6] N Ahmadi and E Harley ldquoCostello syndrome and the impor-tance of cancer screeningrdquo Archives of OtolaryngologymdashHeadand Neck Surgery vol 136 no 10 pp 1028ndash1029 2010
[7] B Kerr O B Eden R Dandamudi et al ldquoCostello syndrometwo cases with embryonal rhabdomyosarcomardquo Journal ofMedical Genetics vol 35 no 12 pp 1036ndash1039 1998
[8] K W Gripp C I Scott Jr L Nicholson et al ldquoFive additionalCostello syndrome patients with rhabdomyosarcoma proposalfor a tumor screening protocolrdquo American Journal of MedicalGenetics vol 108 no 1 pp 80ndash87 2002
[9] K W Gripp A E Lin D L Stabley et al ldquoHRAS mutationanalysis in Costello syndrome genotype and phenotype corre-lationrdquo American Journal of Medical Genetics Part A vol 140no 1 pp 1ndash7 2006
[10] M Feingold ldquoCostello syndrome and rhabdomyosarcomardquoJournal of Medical Genetics vol 36 no 7 pp 582ndash583 1999
[11] S M White J M Graham Jr B Kerr et al ldquoThe adultphenotype in Costello syndromerdquo American Journal of MedicalGenetics A vol 136 no 2 pp 128ndash135 2005
[12] G Bisogno A Murgia I Mammi M S Strafella and M CarlildquoRhabdomyosarcoma in a patient with cardio-facio-cutaneoussyndromerdquo Journal of Pediatric HematologyOncology vol 21no 5 pp 424ndash427 1999
[13] S Sigaudy G Vittu A David et al ldquoCostello syndrome reportof six patients including one with an embryonal rhabdomyosar-comardquoEuropean Journal of Pediatrics vol 159 no 3 pp 139ndash1422000
[14] A Hinek M A Teitell L Schoyer et al ldquoMyocardial storage ofchondroitin sulfate-containing moieties in Costello syndromepatients with severe hypertrophic cardiomyopathyrdquo AmericanJournal of Medical Genetics vol 133 no 1 pp 1ndash12 2005
[15] A E Lin P D Grossfeld R M Hamilton et al ldquoFurtherdelineation of cardiac abnormalities in Costello syndromerdquoAmerican Journal of Medical Genetics vol 111 no 2 pp 115ndash1292002
[16] A L Estep W E Tidyman M A Teitell P D Cotter and KA Rauen ldquoHRASmutations in Costello syndrome detection ofconstitutional activating mutations in codon 12 and 13 and lossof wild-type allele in malignancyrdquo American Journal of MedicalGenetics vol 140 no 1 pp 8ndash16 2006
[17] H KawameMMatsui K Kurosawa et al ldquoFurther delineationof the behavioral and neurologic features inCostello syndromerdquoAmerican Journal of Medical Genetics vol 118A no 1 pp 8ndash142003
[18] B Kerr M A Einaudi P Clayton et al ldquoIs growth hormonetreatment beneficial or harmful in Costello syndromerdquo Journalof medical genetics vol 40 no 6 article e74 2003
[19] J P OrsquoNeal J Ramdas W E Wood and P K PellitterildquoParameningeal rhabdomyosarcoma in a patient with Costellosyndromerdquo Journal of Pediatric HematologyOncology vol 26no 6 pp 389ndash392 2004
[20] K W Gripp ldquoTumor predisposition in Costello syndromerdquoAmerican Journal of Medical Genetics Part C Seminars inMedical Genetics vol 137C no 1 pp 72ndash77 2005
[21] Y Aoki T Niihori H Kawame et al ldquoGermline mutationsin HRAS proto-oncogene cause Costello syndromerdquo NatureGenetics vol 37 no 10 pp 1038ndash1040 2005
[22] Y Abe Y Aoki S Kuriyama et al ldquoPrevalence and clinicalfeatures of Costello syndrome and cardio-facio-cutaneous syn-drome in Japan findings from a nationwide epidemiologicalsurveyrdquo American Journal of Medical Genetics Part A vol 158no 5 pp 1083ndash1094 2012
[23] I F M Lo C Brewer N Shannon et al ldquoSevere neonatal man-ifestations of Costello syndromerdquo Journal of Medical Geneticsvol 45 no 3 pp 167ndash171 2008
[24] J Menke S Pauli M Sigler et al ldquoUniparental trisomy of amutated HRASproto-oncogene in embryonal rhabdomyosar-coma of a patient with costello syndromerdquo Journal of ClinicalOncology vol 33 no 13 pp e62ndashe65 2015
[25] C P Kratz L Franke H Peters et al ldquoCancer spectrum andfrequency among children with Noonan Costello and cardio-facio-cutaneous syndromesrdquo British Journal of Cancer vol 112no 8 pp 1392ndash1397 2015
[26] H K Ransom ldquoSarcoma of the urachus review of the literaturewith report of an additional caserdquo The American Journal ofSurgery vol 22 no 2 pp 187ndash191 1933
[27] E M L-T Fernandez N H Siverio R L Almaraz L MViota J R Luis and L D Flores ldquoRadical surgery and IVA-chemotherapeutic regimen to treat embryonal rhabdomyosar-coma of the urachus case reportrdquo Pediatric Hematology andOncology vol 24 no 7 pp 543ndash550 2007
[28] M Ishikawa T Nishi R Yamada et al ldquoA case of urachalsarcoma in childhood case report and review of the worldliteraturerdquo Journal of the Japanese Society of Pediatric Surgeonsvol 21 pp 128ndash135 1985
[29] S Yokoyama YHayashida J Nagahama et al ldquoRhabdomyosar-coma of the urachus a case reportrdquo Acta Cytologica vol 41 no4 pp 1293ndash1298 1997
[30] U Schulz and C P OrsquoLeary ldquoSpinal AVM epidermal nevusand rhabdomyosarcoma a rare neurocutaneous syndromerdquoNeurology vol 56 no 3 pp 395ndash397 2001
Case Reports in Genetics 13
[31] A Cheikhelard S Irtan D Orbach et al ldquoUrachal rhab-domyosarcoma in childhood a rare entity with a poor out-comerdquo Journal of Pediatric Surgery vol 50 no 8 pp 1329ndash13332015
[32] K W Gripp E Hopkins K Sol-Church et al ldquoPhenotypicanalysis of individuals with Costello syndrome due to HRASpG13Crdquo American Journal of Medical Genetics Part A vol 155no 4 pp 706ndash716 2011
[33] M Tarnowski G Schneider G Amann et al ldquoRasGRF1 reg-ulates proliferation and metastatic behavior of human alveolarrhabdomyosarcomasrdquo International Journal of Oncology vol 41no 3 pp 995ndash1004 2012
[34] J-S Yu K W Kim H-J Lee Y-J Lee C-S Yoon and M-J Kim ldquoUrachal remnant diseases spectrum of CT and USfindingsrdquo Radiographics vol 21 no 2 pp 451ndash461 2001
[35] C P Kratz S Rapisuwon H Reed H Hasle and P S Rosen-berg ldquoCancer in Noonan Costello cardiofaciocutaneous andLEOPARD syndromesrdquo American Journal of Medical GeneticsPart C Seminars in Medical Genetics vol 157 no 2 pp 83ndash892011
[36] B Kerr M L Mucchielli S Sigaudy et al ldquoIs the locus forCostello syndrome on 11prdquo Journal of Medical Genetics vol 40no 6 pp 469ndash471 2003
[37] TNiihori YAokiNOkamoto et al ldquoHRASmutants identifiedin Costello syndrome patients can induce cellular senescencepossible implications for the pathogenesis of Costello syn-dromerdquo Journal of Human Genetics vol 56 no 10 pp 707ndash7152011
[38] G Rosenberger S Meien and K Kutsche ldquoOncogenic HRASmutations cause prolonged PI3K signaling in response toepidermal growth factor in fibroblasts of patients with costellosyndromerdquo Human Mutation vol 30 no 3 pp 352ndash362 2009
[39] M R DeBaun ldquoScreening for cancer in children with Costellosyndromerdquo American Journal of Medical Genetics vol 108 no1 pp 88ndash90 2002
[40] K W Gripp H Kawame D H Viskochil and L NicholsonldquoElevated catecholamine metabolites in patients with Costellosyndromerdquo American Journal of Medical Genetics vol 128 no1 pp 48ndash51 2004
[41] M-ADelrue B Arveiler andD Lacombe ldquoCostello syndromeclinical features and tumoral riskrdquo Archives de Pediatrie vol 9no 10 pp 1059ndash1063 2002
[42] V Martınez-Gonzalez and P Lapunzina Sındrome de CostelloGrupodeTrabajo sobreCancer en SındromeGeneticos Polimar-formativos (GT-CSGP) httpswwworphanetdatapathoProesCSGP-Costello-3pdf
[43] K A Rauen A Banerjee W R Bishop et al ldquoCostello andcardio-facio-cutaneous syndromes moving toward clinical tri-als in RASopathiesrdquo American Journal of Medical Genetics PartC Seminars inMedical Genetics vol 157 no 2 pp 136ndash146 2011
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

10 Case Reports in Genetics
Table 4 Chemotherapy of pediatric patients with umbilical ligament rhabdomyosarcoma
PTnumber Chemotherapy protocol
1-2 No ChT [26 28]3 After establishment of the final diagnosis he was treated with combined ChT including VCR ACD and CTX [29]
4lowastInitially IFOS ACD and VCR After 4 courses CTX was substituted for IFOS because of hemorrhagic cystitis Tx complicatedby recurrent episodes of moderately severe diarrhoea and febrile neutropenia requiring readmission to hospital Tx wascompleted after six courses of ChT [7]
5 NDF [30]
6 PT started induction of ChT 2 weeks after S Induction regimen included 9 cycles of IVA (IFOS VCR and ACD) that were welltolerated with minimal systemic complications (Tx 953 of the MMT 95 SIOP protocol for RMS) [27]
7lowast ChT according to the cooperative soft tissue sarcoma protocol (CWS-2002 P) was well tolerated by the PT [24]8 Adjuvant ChT with 10 cycles of IFOS VCR and ACD [31]9 Adjuvant ChT with 6 cycles of IFOS VCR and VP-16 and 9 cycles of VCR ACD CTXACD and CTX [31]10 Neoadjuvant ChT with 6 cycles of IFOS VCR and ACD and adjuvant ChT with 3 cycles of IFOS VCR and ACD [31]
11 Neoadjuvant ChT with 1 cycle of CTX VCR and PRED 2 cycles IFOS VCR and ACD and 4 cycles of IFOS VCR ACD andDOX and adjuvant ChT with 3 cycles of IFOS VCR and ACD [31]
12 Neoadjuvant ChT with 1 cycle of CTX VCR and PRED and 5 cycles of IFOS VCR ACD and DOX and adjuvant ChT with 2cycles of IFOS VCR ACD and DOX and 1 cycle of IFOS VCR and ACD [31]
13 Neoadjuvant ChT with 2 cycles of VCR ACD and CTX + and 3 cycles of IFOS VCR ACD and DOX and adjuvant ChT with 3cycles of IFOS VCR and ACD [31]
14 Neoadjuvant ChT with 4 cycles of IFOS VCR ACD and DOX and adjuvant ChT with 5 cycles of IFOS VCR ACD [31]
15 Neoadjuvant ChT with 4 cycles of IFOS VCR ACD DOX 3 cycles of IFOS VCR ACD and adjuvant ChT with 1 cycle of IFOSVCR ACD 1 cycle of IFOS VCR [31]
16lowastChT in the standard risk group protocol EpSSG RMS 2005 subgroup D 3 preoperative cycles of IFOS (2 doses at 100mgkg)VCR (005mgkg) and ACD (005mgkg)
17lowastChT (postoperative 15 days) in the standard risk group protocol EpSSG RMS 2005 subgroup B (Stage I) cycles of IFOS (2 dosesof 3 gm2d) VCR (15mgm2) and ACD (15mgm2) was initiated
ACD actinomycin D ChT chemotherapy CTX cyclophosphamide CWS Cooperative Weichteilsarkom Studie (Cooperative Soft Tissue Sarcoma Study)DOX Doxorubicin EpSSG European pediatric Soft tissue sarcoma Study Group IFOS ifosfamide MMT malignant mesenchymal tumor NDF no datafound PRED prednisone PT patient RMS rhabdomyosarcoma S surgery SIOP Societe Internationale DrsquoOncologie Pediatrique (International Society ofPediatric Oncology) Tx treatment VCR vincristine VP-16 etoposide lowastPatients with Costello syndrome
that alveolar RMS and embryonal RMS are two differentdisorders while alveolar RMS may originate from primitiveuncommitted mesodermal cells embryonal RMS originatesprobably from more differentiated myoblasts Ras protein-specific guanine nucleotide-releasing factor 1 (RasGRF1)plays an important role in alveolar RMS pathogenesis Theseinteresting concepts however need more evidence [33]
The umbilicus caudally originates the common ligamentwhich is divided into obliterated umbilical arteries (medialUL) and urachus (median UL) The urachus varies from3 to 10 cm in length and from 8 to 10mm in diameterIt is a three-layered tubular structure the innermost layerbeing lined with transitional epithelium in 70 of casesand with columnar epithelium in 30 The structure issurrounded by connective tissue and outermost muscularlayer in continuity with the detrusor muscle Along its pathfrom the bladder to the umbilicus the urachus lies betweenthe transverse fascia and the parietal peritoneum containedin the pyramidal retropubic perivesical preperitoneal spacecompartmentalized by umbilicovesical fascia along with themedial umbilical ligaments and the bladder Occasionallythe urachus may merge with one or both of the obliteratedumbilical arteries (medial UL) and there may be a slight
deviation to the right or left of the midline [34] The urachusis an embryological remnant resulting from the obliterationof the allantoic channel which attaches the bladder dome tothe umbilicus [31]
Urachal malignant tumors are extremely rare represent-ing less than 05 of all bladder cancers and 001 of alltumors They may arise from any portion of the urachus andare most commonly found in adults and males (60ndash70)Although sarcomas represent only 8 they are the mostfrequent urachal neoplasms reported in patients youngerthan 20 years of age (67) [27] Poor prognosis is a commonfeature in adults and pediatric urachalmalignancies with 50to 60 of 5-year survival In contrast the 5-year event-freesurvival in pelvic RMS was reported to be about 51 [31]
This indolent and rather large urachal tumor was mostlyrevealed by an uncomplicated progressing mass withoutprodromic urological symptomsThedelay of diagnosis couldbe explained by a long asymptomatic progression of thetumor in a preperitoneal location which allows an importantlocal spreading before diagnosis Even in patients withouttumor rupture peritoneal involvement appeared to be the keypoint in the prognosis of urachal RMS Systematic cytologyat diagnosis could be more accurate to evaluate peritoneal
Case Reports in Genetics 11
extension in order to avoid understaging and adjust adjuvantlocoregional treatment [31]
Previously only 12 patients with RMS arising from theurachus (median UL) in children without CS have beenreported in the English literature (Table 3) By 2011 therewere29 reported cases of cancer in patients withCS 19 RMS (meanage of 23 years 9 embryonal 1 alveolar 1 mixed histology1 pleomorphic 1 spindle cell type and 6 unclassified) 5neuroblastomas 4 bladder cancer and 1 fibrosarcoma [35]
Loss of heterozygosity for 11p155 in RMS from individu-als with CS suggests that loss of the wild-type allele is the sec-ond hit in tumor development [6 16 36] Whereas theHRASmutation in a sporadic malignancy in the general populationis present only within the tumor cells in CS an identicalmutation is present in every single cell of the individualthus accounting for the tumor predisposition [1] implicatingan alternate mechanism of rhabdomyosarcogenesis [16] Inaddition one patient with CS and uniparental trisomy dueto triplication of the mutated paternal HRAS gene was alsoreported RMS typically displays loss of heterozygosity ofthe 11p155 region because of paternal uniparental disomyand approximately 28 of cases harbor mutations in genesof growth signaling pathways In reports of uniparentaldisomy plus HRAS mutation the latter was heterozygousand therefore must have occurred after the developmentof uniparental disomy [24] The functional analysis alsorevealed that CS-causing mutant HRAS proteins causedoncogene-induced senescence in human fibroblasts [37]Theimportant role of PI3K-protein-kinase B (AKT) signalingin Ras-mediated transformation and tumorigenesis is high-lighted by constitutive AKT activation in RMS cell lines andclinical samples Thus prolonged PI3K-AKT signaling mightalso be implicated in the development of soft tissue sarcomain patients with CS [38]
Only four out of 11 patients were diagnosed with CS priorto the RMS diagnosis in 5 patients CS was diagnosed afterthe RMS and in the remaining 2 the order was unknown[20] In 2003 a further three unpublished cases of RMS inchildren with CS were known through the International CSSupport Group [18] and for that reason there is possiblyunderdiagnosis of RMS in patients with CS
A screening protocol was proposed consisting of ultra-sound examination of the abdomen and pelvis every 3ndash6 months until age of 8ndash10 years for RMS and abdomi-nal neuroblastoma urine catecholamine metabolite analysisevery 6ndash12 months until age of 5 years for neuroblastomaand urinalysis for hematuria annually for bladder carcinomaafter age of 10 years The prior diagnosis of CS was theprerequisite for the implementation of a tumor screeningprotocol [8] The recommendation based on the presumedfast doubling time of RMS was abdominal sonographyscreening for RMS that should be done in similar intervalsof every four months until stronger evidence would suggestotherwise [39] Screening for neuroblastoma is no longerrecommended becausemany CS patients without identifiabletumor show elevated catecholamine metabolites in urine itappears that in this patient group an elevation above thenormal limit defined as 2 standard deviations (SD) above themean for age is more likely to be a variant rather than a sign
of a neuroblastoma [1 40] A French monitoring protocolproposed the determination of catecholamines and theirmetabolites in urine every six months until the age of 5 yearsand ultrasound abdominopelvic every six months until theend of the puberty seeking hematuria dipstick from6monthsto the age of 10 [41] The protocol in our hospital for patientswith CS includes an abdominal and pelvic ultrasound 3times during the first year of life and in childhood every 6months until age of 10 [42] We believe that the best optionis to perform a pelvic abdominal ultrasound every 3 monthsduring the first eight years of life and then controls accordingto medical criteria This is even more necessary in patientswith possible UL RMS because diagnosis was usually done inadvanced stages with a poor survival It is possible that withclose monitoring after an early diagnosis will detect initialstages of the tumor in previously not described locations
Head and neck MRI scans can be performed less fre-quently Ear examination and tympanometry every 4 to 6months to detect middle ear effusion which would raisesuspicion for a nasopharyngeal mass are also recommended[6]
The outcome of CS patients with RMS has been compa-rable to that for patients without the syndrome with a 5-yearsurvival rate of 65 to 70 [19] but according to this reviewit could be worse than the general population Neoplasia wasnoted at the cause of death in five (22) patients with CS[4 15] but in our study the mortality associated with RMSwas 43 Because the long-term survival in RMS is basedon the histology of the tumor and the extent of disease atdiagnosis early diagnosis may alter the treatment regimenand improve prognosis This could be particularly importantin patients with CS who often are medically fragile [20]
The RasMAPK pathway is an attractive target in thetreatment of cancer utilizing small molecule therapeuticsthat specifically inhibits the pathway Ras pathway agentssuch as farnesyltransferase inhibitors (tipifarnib and lona-farnib) that prevent posttranslational modification of Rasare being evaluated for cancer treatment and may be oftherapeutic use for syndromes in this pathway especially CSIn addition B-Raf protooncogene serinethreonine kinase(BRAF) and mitogenextracellular signal-regulated kinase(MEK) inhibitors offer the same potential in the possibletreatment of CS Since the RasMAPK pathway has targets forinhibition in cancer treatment there aremany smallmoleculetherapeutics that are in development or undergoing clinicaltrials with some already FDA approval [43]
6 ConclusionsCS is a syndrome poorly known in oncology but theirpredisposition tomalignancies includingULRMS implies theneed for a new perspective on early diagnosis and aggressivemedical and surgical treatment
ConsentInformed consent was obtained from the new two individualparticipants included in the study and has been properlydocumented with the parental approval to the use of patientrsquosimages and complementary studies
12 Case Reports in Genetics
Competing Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
Special thanks are due to Israel Fernandez Pineda MDAssistantMember and Surgery Fellowship ProgramDirectorSt Jude Childrenrsquos Research Hospital (Memphis TN) for therecommendations and corrections to the manuscript
References
[1] E Quezada and K W Gripp ldquoCostello syndrome and relateddisordersrdquo Current Opinion in Pediatrics vol 19 no 6 pp 636ndash644 2007
[2] JM Costello ldquoA new syndromerdquoNewZealandMedical Journalvol 74 article 397 1971
[3] JMCostello ldquoAnew syndromemental subnormality andnasalpapillomatardquo Australian Paediatric Journal vol 13 no 2 pp114ndash118 1977
[4] K W Gripp and A E Lin ldquoCostello syndrome a Rasmitogenactivated protein kinase pathway syndrome (rasopathy) result-ing from HRAS germline mutationsrdquo Genetics in Medicine vol14 no 3 pp 285ndash292 2012
[5] B Kerr M-A Delrue S Sigaudy et al ldquoGenotype-phenotypecorrelation in Costello syndrome HRAS mutation analysis in43 casesrdquo Journal of Medical Genetics vol 43 no 5 pp 401ndash4052006
[6] N Ahmadi and E Harley ldquoCostello syndrome and the impor-tance of cancer screeningrdquo Archives of OtolaryngologymdashHeadand Neck Surgery vol 136 no 10 pp 1028ndash1029 2010
[7] B Kerr O B Eden R Dandamudi et al ldquoCostello syndrometwo cases with embryonal rhabdomyosarcomardquo Journal ofMedical Genetics vol 35 no 12 pp 1036ndash1039 1998
[8] K W Gripp C I Scott Jr L Nicholson et al ldquoFive additionalCostello syndrome patients with rhabdomyosarcoma proposalfor a tumor screening protocolrdquo American Journal of MedicalGenetics vol 108 no 1 pp 80ndash87 2002
[9] K W Gripp A E Lin D L Stabley et al ldquoHRAS mutationanalysis in Costello syndrome genotype and phenotype corre-lationrdquo American Journal of Medical Genetics Part A vol 140no 1 pp 1ndash7 2006
[10] M Feingold ldquoCostello syndrome and rhabdomyosarcomardquoJournal of Medical Genetics vol 36 no 7 pp 582ndash583 1999
[11] S M White J M Graham Jr B Kerr et al ldquoThe adultphenotype in Costello syndromerdquo American Journal of MedicalGenetics A vol 136 no 2 pp 128ndash135 2005
[12] G Bisogno A Murgia I Mammi M S Strafella and M CarlildquoRhabdomyosarcoma in a patient with cardio-facio-cutaneoussyndromerdquo Journal of Pediatric HematologyOncology vol 21no 5 pp 424ndash427 1999
[13] S Sigaudy G Vittu A David et al ldquoCostello syndrome reportof six patients including one with an embryonal rhabdomyosar-comardquoEuropean Journal of Pediatrics vol 159 no 3 pp 139ndash1422000
[14] A Hinek M A Teitell L Schoyer et al ldquoMyocardial storage ofchondroitin sulfate-containing moieties in Costello syndromepatients with severe hypertrophic cardiomyopathyrdquo AmericanJournal of Medical Genetics vol 133 no 1 pp 1ndash12 2005
[15] A E Lin P D Grossfeld R M Hamilton et al ldquoFurtherdelineation of cardiac abnormalities in Costello syndromerdquoAmerican Journal of Medical Genetics vol 111 no 2 pp 115ndash1292002
[16] A L Estep W E Tidyman M A Teitell P D Cotter and KA Rauen ldquoHRASmutations in Costello syndrome detection ofconstitutional activating mutations in codon 12 and 13 and lossof wild-type allele in malignancyrdquo American Journal of MedicalGenetics vol 140 no 1 pp 8ndash16 2006
[17] H KawameMMatsui K Kurosawa et al ldquoFurther delineationof the behavioral and neurologic features inCostello syndromerdquoAmerican Journal of Medical Genetics vol 118A no 1 pp 8ndash142003
[18] B Kerr M A Einaudi P Clayton et al ldquoIs growth hormonetreatment beneficial or harmful in Costello syndromerdquo Journalof medical genetics vol 40 no 6 article e74 2003
[19] J P OrsquoNeal J Ramdas W E Wood and P K PellitterildquoParameningeal rhabdomyosarcoma in a patient with Costellosyndromerdquo Journal of Pediatric HematologyOncology vol 26no 6 pp 389ndash392 2004
[20] K W Gripp ldquoTumor predisposition in Costello syndromerdquoAmerican Journal of Medical Genetics Part C Seminars inMedical Genetics vol 137C no 1 pp 72ndash77 2005
[21] Y Aoki T Niihori H Kawame et al ldquoGermline mutationsin HRAS proto-oncogene cause Costello syndromerdquo NatureGenetics vol 37 no 10 pp 1038ndash1040 2005
[22] Y Abe Y Aoki S Kuriyama et al ldquoPrevalence and clinicalfeatures of Costello syndrome and cardio-facio-cutaneous syn-drome in Japan findings from a nationwide epidemiologicalsurveyrdquo American Journal of Medical Genetics Part A vol 158no 5 pp 1083ndash1094 2012
[23] I F M Lo C Brewer N Shannon et al ldquoSevere neonatal man-ifestations of Costello syndromerdquo Journal of Medical Geneticsvol 45 no 3 pp 167ndash171 2008
[24] J Menke S Pauli M Sigler et al ldquoUniparental trisomy of amutated HRASproto-oncogene in embryonal rhabdomyosar-coma of a patient with costello syndromerdquo Journal of ClinicalOncology vol 33 no 13 pp e62ndashe65 2015
[25] C P Kratz L Franke H Peters et al ldquoCancer spectrum andfrequency among children with Noonan Costello and cardio-facio-cutaneous syndromesrdquo British Journal of Cancer vol 112no 8 pp 1392ndash1397 2015
[26] H K Ransom ldquoSarcoma of the urachus review of the literaturewith report of an additional caserdquo The American Journal ofSurgery vol 22 no 2 pp 187ndash191 1933
[27] E M L-T Fernandez N H Siverio R L Almaraz L MViota J R Luis and L D Flores ldquoRadical surgery and IVA-chemotherapeutic regimen to treat embryonal rhabdomyosar-coma of the urachus case reportrdquo Pediatric Hematology andOncology vol 24 no 7 pp 543ndash550 2007
[28] M Ishikawa T Nishi R Yamada et al ldquoA case of urachalsarcoma in childhood case report and review of the worldliteraturerdquo Journal of the Japanese Society of Pediatric Surgeonsvol 21 pp 128ndash135 1985
[29] S Yokoyama YHayashida J Nagahama et al ldquoRhabdomyosar-coma of the urachus a case reportrdquo Acta Cytologica vol 41 no4 pp 1293ndash1298 1997
[30] U Schulz and C P OrsquoLeary ldquoSpinal AVM epidermal nevusand rhabdomyosarcoma a rare neurocutaneous syndromerdquoNeurology vol 56 no 3 pp 395ndash397 2001
Case Reports in Genetics 13
[31] A Cheikhelard S Irtan D Orbach et al ldquoUrachal rhab-domyosarcoma in childhood a rare entity with a poor out-comerdquo Journal of Pediatric Surgery vol 50 no 8 pp 1329ndash13332015
[32] K W Gripp E Hopkins K Sol-Church et al ldquoPhenotypicanalysis of individuals with Costello syndrome due to HRASpG13Crdquo American Journal of Medical Genetics Part A vol 155no 4 pp 706ndash716 2011
[33] M Tarnowski G Schneider G Amann et al ldquoRasGRF1 reg-ulates proliferation and metastatic behavior of human alveolarrhabdomyosarcomasrdquo International Journal of Oncology vol 41no 3 pp 995ndash1004 2012
[34] J-S Yu K W Kim H-J Lee Y-J Lee C-S Yoon and M-J Kim ldquoUrachal remnant diseases spectrum of CT and USfindingsrdquo Radiographics vol 21 no 2 pp 451ndash461 2001
[35] C P Kratz S Rapisuwon H Reed H Hasle and P S Rosen-berg ldquoCancer in Noonan Costello cardiofaciocutaneous andLEOPARD syndromesrdquo American Journal of Medical GeneticsPart C Seminars in Medical Genetics vol 157 no 2 pp 83ndash892011
[36] B Kerr M L Mucchielli S Sigaudy et al ldquoIs the locus forCostello syndrome on 11prdquo Journal of Medical Genetics vol 40no 6 pp 469ndash471 2003
[37] TNiihori YAokiNOkamoto et al ldquoHRASmutants identifiedin Costello syndrome patients can induce cellular senescencepossible implications for the pathogenesis of Costello syn-dromerdquo Journal of Human Genetics vol 56 no 10 pp 707ndash7152011
[38] G Rosenberger S Meien and K Kutsche ldquoOncogenic HRASmutations cause prolonged PI3K signaling in response toepidermal growth factor in fibroblasts of patients with costellosyndromerdquo Human Mutation vol 30 no 3 pp 352ndash362 2009
[39] M R DeBaun ldquoScreening for cancer in children with Costellosyndromerdquo American Journal of Medical Genetics vol 108 no1 pp 88ndash90 2002
[40] K W Gripp H Kawame D H Viskochil and L NicholsonldquoElevated catecholamine metabolites in patients with Costellosyndromerdquo American Journal of Medical Genetics vol 128 no1 pp 48ndash51 2004
[41] M-ADelrue B Arveiler andD Lacombe ldquoCostello syndromeclinical features and tumoral riskrdquo Archives de Pediatrie vol 9no 10 pp 1059ndash1063 2002
[42] V Martınez-Gonzalez and P Lapunzina Sındrome de CostelloGrupodeTrabajo sobreCancer en SındromeGeneticos Polimar-formativos (GT-CSGP) httpswwworphanetdatapathoProesCSGP-Costello-3pdf
[43] K A Rauen A Banerjee W R Bishop et al ldquoCostello andcardio-facio-cutaneous syndromes moving toward clinical tri-als in RASopathiesrdquo American Journal of Medical Genetics PartC Seminars inMedical Genetics vol 157 no 2 pp 136ndash146 2011
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Case Reports in Genetics 11
extension in order to avoid understaging and adjust adjuvantlocoregional treatment [31]
Previously only 12 patients with RMS arising from theurachus (median UL) in children without CS have beenreported in the English literature (Table 3) By 2011 therewere29 reported cases of cancer in patients withCS 19 RMS (meanage of 23 years 9 embryonal 1 alveolar 1 mixed histology1 pleomorphic 1 spindle cell type and 6 unclassified) 5neuroblastomas 4 bladder cancer and 1 fibrosarcoma [35]
Loss of heterozygosity for 11p155 in RMS from individu-als with CS suggests that loss of the wild-type allele is the sec-ond hit in tumor development [6 16 36] Whereas theHRASmutation in a sporadic malignancy in the general populationis present only within the tumor cells in CS an identicalmutation is present in every single cell of the individualthus accounting for the tumor predisposition [1] implicatingan alternate mechanism of rhabdomyosarcogenesis [16] Inaddition one patient with CS and uniparental trisomy dueto triplication of the mutated paternal HRAS gene was alsoreported RMS typically displays loss of heterozygosity ofthe 11p155 region because of paternal uniparental disomyand approximately 28 of cases harbor mutations in genesof growth signaling pathways In reports of uniparentaldisomy plus HRAS mutation the latter was heterozygousand therefore must have occurred after the developmentof uniparental disomy [24] The functional analysis alsorevealed that CS-causing mutant HRAS proteins causedoncogene-induced senescence in human fibroblasts [37]Theimportant role of PI3K-protein-kinase B (AKT) signalingin Ras-mediated transformation and tumorigenesis is high-lighted by constitutive AKT activation in RMS cell lines andclinical samples Thus prolonged PI3K-AKT signaling mightalso be implicated in the development of soft tissue sarcomain patients with CS [38]
Only four out of 11 patients were diagnosed with CS priorto the RMS diagnosis in 5 patients CS was diagnosed afterthe RMS and in the remaining 2 the order was unknown[20] In 2003 a further three unpublished cases of RMS inchildren with CS were known through the International CSSupport Group [18] and for that reason there is possiblyunderdiagnosis of RMS in patients with CS
A screening protocol was proposed consisting of ultra-sound examination of the abdomen and pelvis every 3ndash6 months until age of 8ndash10 years for RMS and abdomi-nal neuroblastoma urine catecholamine metabolite analysisevery 6ndash12 months until age of 5 years for neuroblastomaand urinalysis for hematuria annually for bladder carcinomaafter age of 10 years The prior diagnosis of CS was theprerequisite for the implementation of a tumor screeningprotocol [8] The recommendation based on the presumedfast doubling time of RMS was abdominal sonographyscreening for RMS that should be done in similar intervalsof every four months until stronger evidence would suggestotherwise [39] Screening for neuroblastoma is no longerrecommended becausemany CS patients without identifiabletumor show elevated catecholamine metabolites in urine itappears that in this patient group an elevation above thenormal limit defined as 2 standard deviations (SD) above themean for age is more likely to be a variant rather than a sign
of a neuroblastoma [1 40] A French monitoring protocolproposed the determination of catecholamines and theirmetabolites in urine every six months until the age of 5 yearsand ultrasound abdominopelvic every six months until theend of the puberty seeking hematuria dipstick from6monthsto the age of 10 [41] The protocol in our hospital for patientswith CS includes an abdominal and pelvic ultrasound 3times during the first year of life and in childhood every 6months until age of 10 [42] We believe that the best optionis to perform a pelvic abdominal ultrasound every 3 monthsduring the first eight years of life and then controls accordingto medical criteria This is even more necessary in patientswith possible UL RMS because diagnosis was usually done inadvanced stages with a poor survival It is possible that withclose monitoring after an early diagnosis will detect initialstages of the tumor in previously not described locations
Head and neck MRI scans can be performed less fre-quently Ear examination and tympanometry every 4 to 6months to detect middle ear effusion which would raisesuspicion for a nasopharyngeal mass are also recommended[6]
The outcome of CS patients with RMS has been compa-rable to that for patients without the syndrome with a 5-yearsurvival rate of 65 to 70 [19] but according to this reviewit could be worse than the general population Neoplasia wasnoted at the cause of death in five (22) patients with CS[4 15] but in our study the mortality associated with RMSwas 43 Because the long-term survival in RMS is basedon the histology of the tumor and the extent of disease atdiagnosis early diagnosis may alter the treatment regimenand improve prognosis This could be particularly importantin patients with CS who often are medically fragile [20]
The RasMAPK pathway is an attractive target in thetreatment of cancer utilizing small molecule therapeuticsthat specifically inhibits the pathway Ras pathway agentssuch as farnesyltransferase inhibitors (tipifarnib and lona-farnib) that prevent posttranslational modification of Rasare being evaluated for cancer treatment and may be oftherapeutic use for syndromes in this pathway especially CSIn addition B-Raf protooncogene serinethreonine kinase(BRAF) and mitogenextracellular signal-regulated kinase(MEK) inhibitors offer the same potential in the possibletreatment of CS Since the RasMAPK pathway has targets forinhibition in cancer treatment there aremany smallmoleculetherapeutics that are in development or undergoing clinicaltrials with some already FDA approval [43]
6 ConclusionsCS is a syndrome poorly known in oncology but theirpredisposition tomalignancies includingULRMS implies theneed for a new perspective on early diagnosis and aggressivemedical and surgical treatment
ConsentInformed consent was obtained from the new two individualparticipants included in the study and has been properlydocumented with the parental approval to the use of patientrsquosimages and complementary studies
12 Case Reports in Genetics
Competing Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
Special thanks are due to Israel Fernandez Pineda MDAssistantMember and Surgery Fellowship ProgramDirectorSt Jude Childrenrsquos Research Hospital (Memphis TN) for therecommendations and corrections to the manuscript
References
[1] E Quezada and K W Gripp ldquoCostello syndrome and relateddisordersrdquo Current Opinion in Pediatrics vol 19 no 6 pp 636ndash644 2007
[2] JM Costello ldquoA new syndromerdquoNewZealandMedical Journalvol 74 article 397 1971
[3] JMCostello ldquoAnew syndromemental subnormality andnasalpapillomatardquo Australian Paediatric Journal vol 13 no 2 pp114ndash118 1977
[4] K W Gripp and A E Lin ldquoCostello syndrome a Rasmitogenactivated protein kinase pathway syndrome (rasopathy) result-ing from HRAS germline mutationsrdquo Genetics in Medicine vol14 no 3 pp 285ndash292 2012
[5] B Kerr M-A Delrue S Sigaudy et al ldquoGenotype-phenotypecorrelation in Costello syndrome HRAS mutation analysis in43 casesrdquo Journal of Medical Genetics vol 43 no 5 pp 401ndash4052006
[6] N Ahmadi and E Harley ldquoCostello syndrome and the impor-tance of cancer screeningrdquo Archives of OtolaryngologymdashHeadand Neck Surgery vol 136 no 10 pp 1028ndash1029 2010
[7] B Kerr O B Eden R Dandamudi et al ldquoCostello syndrometwo cases with embryonal rhabdomyosarcomardquo Journal ofMedical Genetics vol 35 no 12 pp 1036ndash1039 1998
[8] K W Gripp C I Scott Jr L Nicholson et al ldquoFive additionalCostello syndrome patients with rhabdomyosarcoma proposalfor a tumor screening protocolrdquo American Journal of MedicalGenetics vol 108 no 1 pp 80ndash87 2002
[9] K W Gripp A E Lin D L Stabley et al ldquoHRAS mutationanalysis in Costello syndrome genotype and phenotype corre-lationrdquo American Journal of Medical Genetics Part A vol 140no 1 pp 1ndash7 2006
[10] M Feingold ldquoCostello syndrome and rhabdomyosarcomardquoJournal of Medical Genetics vol 36 no 7 pp 582ndash583 1999
[11] S M White J M Graham Jr B Kerr et al ldquoThe adultphenotype in Costello syndromerdquo American Journal of MedicalGenetics A vol 136 no 2 pp 128ndash135 2005
[12] G Bisogno A Murgia I Mammi M S Strafella and M CarlildquoRhabdomyosarcoma in a patient with cardio-facio-cutaneoussyndromerdquo Journal of Pediatric HematologyOncology vol 21no 5 pp 424ndash427 1999
[13] S Sigaudy G Vittu A David et al ldquoCostello syndrome reportof six patients including one with an embryonal rhabdomyosar-comardquoEuropean Journal of Pediatrics vol 159 no 3 pp 139ndash1422000
[14] A Hinek M A Teitell L Schoyer et al ldquoMyocardial storage ofchondroitin sulfate-containing moieties in Costello syndromepatients with severe hypertrophic cardiomyopathyrdquo AmericanJournal of Medical Genetics vol 133 no 1 pp 1ndash12 2005
[15] A E Lin P D Grossfeld R M Hamilton et al ldquoFurtherdelineation of cardiac abnormalities in Costello syndromerdquoAmerican Journal of Medical Genetics vol 111 no 2 pp 115ndash1292002
[16] A L Estep W E Tidyman M A Teitell P D Cotter and KA Rauen ldquoHRASmutations in Costello syndrome detection ofconstitutional activating mutations in codon 12 and 13 and lossof wild-type allele in malignancyrdquo American Journal of MedicalGenetics vol 140 no 1 pp 8ndash16 2006
[17] H KawameMMatsui K Kurosawa et al ldquoFurther delineationof the behavioral and neurologic features inCostello syndromerdquoAmerican Journal of Medical Genetics vol 118A no 1 pp 8ndash142003
[18] B Kerr M A Einaudi P Clayton et al ldquoIs growth hormonetreatment beneficial or harmful in Costello syndromerdquo Journalof medical genetics vol 40 no 6 article e74 2003
[19] J P OrsquoNeal J Ramdas W E Wood and P K PellitterildquoParameningeal rhabdomyosarcoma in a patient with Costellosyndromerdquo Journal of Pediatric HematologyOncology vol 26no 6 pp 389ndash392 2004
[20] K W Gripp ldquoTumor predisposition in Costello syndromerdquoAmerican Journal of Medical Genetics Part C Seminars inMedical Genetics vol 137C no 1 pp 72ndash77 2005
[21] Y Aoki T Niihori H Kawame et al ldquoGermline mutationsin HRAS proto-oncogene cause Costello syndromerdquo NatureGenetics vol 37 no 10 pp 1038ndash1040 2005
[22] Y Abe Y Aoki S Kuriyama et al ldquoPrevalence and clinicalfeatures of Costello syndrome and cardio-facio-cutaneous syn-drome in Japan findings from a nationwide epidemiologicalsurveyrdquo American Journal of Medical Genetics Part A vol 158no 5 pp 1083ndash1094 2012
[23] I F M Lo C Brewer N Shannon et al ldquoSevere neonatal man-ifestations of Costello syndromerdquo Journal of Medical Geneticsvol 45 no 3 pp 167ndash171 2008
[24] J Menke S Pauli M Sigler et al ldquoUniparental trisomy of amutated HRASproto-oncogene in embryonal rhabdomyosar-coma of a patient with costello syndromerdquo Journal of ClinicalOncology vol 33 no 13 pp e62ndashe65 2015
[25] C P Kratz L Franke H Peters et al ldquoCancer spectrum andfrequency among children with Noonan Costello and cardio-facio-cutaneous syndromesrdquo British Journal of Cancer vol 112no 8 pp 1392ndash1397 2015
[26] H K Ransom ldquoSarcoma of the urachus review of the literaturewith report of an additional caserdquo The American Journal ofSurgery vol 22 no 2 pp 187ndash191 1933
[27] E M L-T Fernandez N H Siverio R L Almaraz L MViota J R Luis and L D Flores ldquoRadical surgery and IVA-chemotherapeutic regimen to treat embryonal rhabdomyosar-coma of the urachus case reportrdquo Pediatric Hematology andOncology vol 24 no 7 pp 543ndash550 2007
[28] M Ishikawa T Nishi R Yamada et al ldquoA case of urachalsarcoma in childhood case report and review of the worldliteraturerdquo Journal of the Japanese Society of Pediatric Surgeonsvol 21 pp 128ndash135 1985
[29] S Yokoyama YHayashida J Nagahama et al ldquoRhabdomyosar-coma of the urachus a case reportrdquo Acta Cytologica vol 41 no4 pp 1293ndash1298 1997
[30] U Schulz and C P OrsquoLeary ldquoSpinal AVM epidermal nevusand rhabdomyosarcoma a rare neurocutaneous syndromerdquoNeurology vol 56 no 3 pp 395ndash397 2001
Case Reports in Genetics 13
[31] A Cheikhelard S Irtan D Orbach et al ldquoUrachal rhab-domyosarcoma in childhood a rare entity with a poor out-comerdquo Journal of Pediatric Surgery vol 50 no 8 pp 1329ndash13332015
[32] K W Gripp E Hopkins K Sol-Church et al ldquoPhenotypicanalysis of individuals with Costello syndrome due to HRASpG13Crdquo American Journal of Medical Genetics Part A vol 155no 4 pp 706ndash716 2011
[33] M Tarnowski G Schneider G Amann et al ldquoRasGRF1 reg-ulates proliferation and metastatic behavior of human alveolarrhabdomyosarcomasrdquo International Journal of Oncology vol 41no 3 pp 995ndash1004 2012
[34] J-S Yu K W Kim H-J Lee Y-J Lee C-S Yoon and M-J Kim ldquoUrachal remnant diseases spectrum of CT and USfindingsrdquo Radiographics vol 21 no 2 pp 451ndash461 2001
[35] C P Kratz S Rapisuwon H Reed H Hasle and P S Rosen-berg ldquoCancer in Noonan Costello cardiofaciocutaneous andLEOPARD syndromesrdquo American Journal of Medical GeneticsPart C Seminars in Medical Genetics vol 157 no 2 pp 83ndash892011
[36] B Kerr M L Mucchielli S Sigaudy et al ldquoIs the locus forCostello syndrome on 11prdquo Journal of Medical Genetics vol 40no 6 pp 469ndash471 2003
[37] TNiihori YAokiNOkamoto et al ldquoHRASmutants identifiedin Costello syndrome patients can induce cellular senescencepossible implications for the pathogenesis of Costello syn-dromerdquo Journal of Human Genetics vol 56 no 10 pp 707ndash7152011
[38] G Rosenberger S Meien and K Kutsche ldquoOncogenic HRASmutations cause prolonged PI3K signaling in response toepidermal growth factor in fibroblasts of patients with costellosyndromerdquo Human Mutation vol 30 no 3 pp 352ndash362 2009
[39] M R DeBaun ldquoScreening for cancer in children with Costellosyndromerdquo American Journal of Medical Genetics vol 108 no1 pp 88ndash90 2002
[40] K W Gripp H Kawame D H Viskochil and L NicholsonldquoElevated catecholamine metabolites in patients with Costellosyndromerdquo American Journal of Medical Genetics vol 128 no1 pp 48ndash51 2004
[41] M-ADelrue B Arveiler andD Lacombe ldquoCostello syndromeclinical features and tumoral riskrdquo Archives de Pediatrie vol 9no 10 pp 1059ndash1063 2002
[42] V Martınez-Gonzalez and P Lapunzina Sındrome de CostelloGrupodeTrabajo sobreCancer en SındromeGeneticos Polimar-formativos (GT-CSGP) httpswwworphanetdatapathoProesCSGP-Costello-3pdf
[43] K A Rauen A Banerjee W R Bishop et al ldquoCostello andcardio-facio-cutaneous syndromes moving toward clinical tri-als in RASopathiesrdquo American Journal of Medical Genetics PartC Seminars inMedical Genetics vol 157 no 2 pp 136ndash146 2011
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

12 Case Reports in Genetics
Competing Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
Special thanks are due to Israel Fernandez Pineda MDAssistantMember and Surgery Fellowship ProgramDirectorSt Jude Childrenrsquos Research Hospital (Memphis TN) for therecommendations and corrections to the manuscript
References
[1] E Quezada and K W Gripp ldquoCostello syndrome and relateddisordersrdquo Current Opinion in Pediatrics vol 19 no 6 pp 636ndash644 2007
[2] JM Costello ldquoA new syndromerdquoNewZealandMedical Journalvol 74 article 397 1971
[3] JMCostello ldquoAnew syndromemental subnormality andnasalpapillomatardquo Australian Paediatric Journal vol 13 no 2 pp114ndash118 1977
[4] K W Gripp and A E Lin ldquoCostello syndrome a Rasmitogenactivated protein kinase pathway syndrome (rasopathy) result-ing from HRAS germline mutationsrdquo Genetics in Medicine vol14 no 3 pp 285ndash292 2012
[5] B Kerr M-A Delrue S Sigaudy et al ldquoGenotype-phenotypecorrelation in Costello syndrome HRAS mutation analysis in43 casesrdquo Journal of Medical Genetics vol 43 no 5 pp 401ndash4052006
[6] N Ahmadi and E Harley ldquoCostello syndrome and the impor-tance of cancer screeningrdquo Archives of OtolaryngologymdashHeadand Neck Surgery vol 136 no 10 pp 1028ndash1029 2010
[7] B Kerr O B Eden R Dandamudi et al ldquoCostello syndrometwo cases with embryonal rhabdomyosarcomardquo Journal ofMedical Genetics vol 35 no 12 pp 1036ndash1039 1998
[8] K W Gripp C I Scott Jr L Nicholson et al ldquoFive additionalCostello syndrome patients with rhabdomyosarcoma proposalfor a tumor screening protocolrdquo American Journal of MedicalGenetics vol 108 no 1 pp 80ndash87 2002
[9] K W Gripp A E Lin D L Stabley et al ldquoHRAS mutationanalysis in Costello syndrome genotype and phenotype corre-lationrdquo American Journal of Medical Genetics Part A vol 140no 1 pp 1ndash7 2006
[10] M Feingold ldquoCostello syndrome and rhabdomyosarcomardquoJournal of Medical Genetics vol 36 no 7 pp 582ndash583 1999
[11] S M White J M Graham Jr B Kerr et al ldquoThe adultphenotype in Costello syndromerdquo American Journal of MedicalGenetics A vol 136 no 2 pp 128ndash135 2005
[12] G Bisogno A Murgia I Mammi M S Strafella and M CarlildquoRhabdomyosarcoma in a patient with cardio-facio-cutaneoussyndromerdquo Journal of Pediatric HematologyOncology vol 21no 5 pp 424ndash427 1999
[13] S Sigaudy G Vittu A David et al ldquoCostello syndrome reportof six patients including one with an embryonal rhabdomyosar-comardquoEuropean Journal of Pediatrics vol 159 no 3 pp 139ndash1422000
[14] A Hinek M A Teitell L Schoyer et al ldquoMyocardial storage ofchondroitin sulfate-containing moieties in Costello syndromepatients with severe hypertrophic cardiomyopathyrdquo AmericanJournal of Medical Genetics vol 133 no 1 pp 1ndash12 2005
[15] A E Lin P D Grossfeld R M Hamilton et al ldquoFurtherdelineation of cardiac abnormalities in Costello syndromerdquoAmerican Journal of Medical Genetics vol 111 no 2 pp 115ndash1292002
[16] A L Estep W E Tidyman M A Teitell P D Cotter and KA Rauen ldquoHRASmutations in Costello syndrome detection ofconstitutional activating mutations in codon 12 and 13 and lossof wild-type allele in malignancyrdquo American Journal of MedicalGenetics vol 140 no 1 pp 8ndash16 2006
[17] H KawameMMatsui K Kurosawa et al ldquoFurther delineationof the behavioral and neurologic features inCostello syndromerdquoAmerican Journal of Medical Genetics vol 118A no 1 pp 8ndash142003
[18] B Kerr M A Einaudi P Clayton et al ldquoIs growth hormonetreatment beneficial or harmful in Costello syndromerdquo Journalof medical genetics vol 40 no 6 article e74 2003
[19] J P OrsquoNeal J Ramdas W E Wood and P K PellitterildquoParameningeal rhabdomyosarcoma in a patient with Costellosyndromerdquo Journal of Pediatric HematologyOncology vol 26no 6 pp 389ndash392 2004
[20] K W Gripp ldquoTumor predisposition in Costello syndromerdquoAmerican Journal of Medical Genetics Part C Seminars inMedical Genetics vol 137C no 1 pp 72ndash77 2005
[21] Y Aoki T Niihori H Kawame et al ldquoGermline mutationsin HRAS proto-oncogene cause Costello syndromerdquo NatureGenetics vol 37 no 10 pp 1038ndash1040 2005
[22] Y Abe Y Aoki S Kuriyama et al ldquoPrevalence and clinicalfeatures of Costello syndrome and cardio-facio-cutaneous syn-drome in Japan findings from a nationwide epidemiologicalsurveyrdquo American Journal of Medical Genetics Part A vol 158no 5 pp 1083ndash1094 2012
[23] I F M Lo C Brewer N Shannon et al ldquoSevere neonatal man-ifestations of Costello syndromerdquo Journal of Medical Geneticsvol 45 no 3 pp 167ndash171 2008
[24] J Menke S Pauli M Sigler et al ldquoUniparental trisomy of amutated HRASproto-oncogene in embryonal rhabdomyosar-coma of a patient with costello syndromerdquo Journal of ClinicalOncology vol 33 no 13 pp e62ndashe65 2015
[25] C P Kratz L Franke H Peters et al ldquoCancer spectrum andfrequency among children with Noonan Costello and cardio-facio-cutaneous syndromesrdquo British Journal of Cancer vol 112no 8 pp 1392ndash1397 2015
[26] H K Ransom ldquoSarcoma of the urachus review of the literaturewith report of an additional caserdquo The American Journal ofSurgery vol 22 no 2 pp 187ndash191 1933
[27] E M L-T Fernandez N H Siverio R L Almaraz L MViota J R Luis and L D Flores ldquoRadical surgery and IVA-chemotherapeutic regimen to treat embryonal rhabdomyosar-coma of the urachus case reportrdquo Pediatric Hematology andOncology vol 24 no 7 pp 543ndash550 2007
[28] M Ishikawa T Nishi R Yamada et al ldquoA case of urachalsarcoma in childhood case report and review of the worldliteraturerdquo Journal of the Japanese Society of Pediatric Surgeonsvol 21 pp 128ndash135 1985
[29] S Yokoyama YHayashida J Nagahama et al ldquoRhabdomyosar-coma of the urachus a case reportrdquo Acta Cytologica vol 41 no4 pp 1293ndash1298 1997
[30] U Schulz and C P OrsquoLeary ldquoSpinal AVM epidermal nevusand rhabdomyosarcoma a rare neurocutaneous syndromerdquoNeurology vol 56 no 3 pp 395ndash397 2001
Case Reports in Genetics 13
[31] A Cheikhelard S Irtan D Orbach et al ldquoUrachal rhab-domyosarcoma in childhood a rare entity with a poor out-comerdquo Journal of Pediatric Surgery vol 50 no 8 pp 1329ndash13332015
[32] K W Gripp E Hopkins K Sol-Church et al ldquoPhenotypicanalysis of individuals with Costello syndrome due to HRASpG13Crdquo American Journal of Medical Genetics Part A vol 155no 4 pp 706ndash716 2011
[33] M Tarnowski G Schneider G Amann et al ldquoRasGRF1 reg-ulates proliferation and metastatic behavior of human alveolarrhabdomyosarcomasrdquo International Journal of Oncology vol 41no 3 pp 995ndash1004 2012
[34] J-S Yu K W Kim H-J Lee Y-J Lee C-S Yoon and M-J Kim ldquoUrachal remnant diseases spectrum of CT and USfindingsrdquo Radiographics vol 21 no 2 pp 451ndash461 2001
[35] C P Kratz S Rapisuwon H Reed H Hasle and P S Rosen-berg ldquoCancer in Noonan Costello cardiofaciocutaneous andLEOPARD syndromesrdquo American Journal of Medical GeneticsPart C Seminars in Medical Genetics vol 157 no 2 pp 83ndash892011
[36] B Kerr M L Mucchielli S Sigaudy et al ldquoIs the locus forCostello syndrome on 11prdquo Journal of Medical Genetics vol 40no 6 pp 469ndash471 2003
[37] TNiihori YAokiNOkamoto et al ldquoHRASmutants identifiedin Costello syndrome patients can induce cellular senescencepossible implications for the pathogenesis of Costello syn-dromerdquo Journal of Human Genetics vol 56 no 10 pp 707ndash7152011
[38] G Rosenberger S Meien and K Kutsche ldquoOncogenic HRASmutations cause prolonged PI3K signaling in response toepidermal growth factor in fibroblasts of patients with costellosyndromerdquo Human Mutation vol 30 no 3 pp 352ndash362 2009
[39] M R DeBaun ldquoScreening for cancer in children with Costellosyndromerdquo American Journal of Medical Genetics vol 108 no1 pp 88ndash90 2002
[40] K W Gripp H Kawame D H Viskochil and L NicholsonldquoElevated catecholamine metabolites in patients with Costellosyndromerdquo American Journal of Medical Genetics vol 128 no1 pp 48ndash51 2004
[41] M-ADelrue B Arveiler andD Lacombe ldquoCostello syndromeclinical features and tumoral riskrdquo Archives de Pediatrie vol 9no 10 pp 1059ndash1063 2002
[42] V Martınez-Gonzalez and P Lapunzina Sındrome de CostelloGrupodeTrabajo sobreCancer en SındromeGeneticos Polimar-formativos (GT-CSGP) httpswwworphanetdatapathoProesCSGP-Costello-3pdf
[43] K A Rauen A Banerjee W R Bishop et al ldquoCostello andcardio-facio-cutaneous syndromes moving toward clinical tri-als in RASopathiesrdquo American Journal of Medical Genetics PartC Seminars inMedical Genetics vol 157 no 2 pp 136ndash146 2011
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Case Reports in Genetics 13
[31] A Cheikhelard S Irtan D Orbach et al ldquoUrachal rhab-domyosarcoma in childhood a rare entity with a poor out-comerdquo Journal of Pediatric Surgery vol 50 no 8 pp 1329ndash13332015
[32] K W Gripp E Hopkins K Sol-Church et al ldquoPhenotypicanalysis of individuals with Costello syndrome due to HRASpG13Crdquo American Journal of Medical Genetics Part A vol 155no 4 pp 706ndash716 2011
[33] M Tarnowski G Schneider G Amann et al ldquoRasGRF1 reg-ulates proliferation and metastatic behavior of human alveolarrhabdomyosarcomasrdquo International Journal of Oncology vol 41no 3 pp 995ndash1004 2012
[34] J-S Yu K W Kim H-J Lee Y-J Lee C-S Yoon and M-J Kim ldquoUrachal remnant diseases spectrum of CT and USfindingsrdquo Radiographics vol 21 no 2 pp 451ndash461 2001
[35] C P Kratz S Rapisuwon H Reed H Hasle and P S Rosen-berg ldquoCancer in Noonan Costello cardiofaciocutaneous andLEOPARD syndromesrdquo American Journal of Medical GeneticsPart C Seminars in Medical Genetics vol 157 no 2 pp 83ndash892011
[36] B Kerr M L Mucchielli S Sigaudy et al ldquoIs the locus forCostello syndrome on 11prdquo Journal of Medical Genetics vol 40no 6 pp 469ndash471 2003
[37] TNiihori YAokiNOkamoto et al ldquoHRASmutants identifiedin Costello syndrome patients can induce cellular senescencepossible implications for the pathogenesis of Costello syn-dromerdquo Journal of Human Genetics vol 56 no 10 pp 707ndash7152011
[38] G Rosenberger S Meien and K Kutsche ldquoOncogenic HRASmutations cause prolonged PI3K signaling in response toepidermal growth factor in fibroblasts of patients with costellosyndromerdquo Human Mutation vol 30 no 3 pp 352ndash362 2009
[39] M R DeBaun ldquoScreening for cancer in children with Costellosyndromerdquo American Journal of Medical Genetics vol 108 no1 pp 88ndash90 2002
[40] K W Gripp H Kawame D H Viskochil and L NicholsonldquoElevated catecholamine metabolites in patients with Costellosyndromerdquo American Journal of Medical Genetics vol 128 no1 pp 48ndash51 2004
[41] M-ADelrue B Arveiler andD Lacombe ldquoCostello syndromeclinical features and tumoral riskrdquo Archives de Pediatrie vol 9no 10 pp 1059ndash1063 2002
[42] V Martınez-Gonzalez and P Lapunzina Sındrome de CostelloGrupodeTrabajo sobreCancer en SındromeGeneticos Polimar-formativos (GT-CSGP) httpswwworphanetdatapathoProesCSGP-Costello-3pdf
[43] K A Rauen A Banerjee W R Bishop et al ldquoCostello andcardio-facio-cutaneous syndromes moving toward clinical tri-als in RASopathiesrdquo American Journal of Medical Genetics PartC Seminars inMedical Genetics vol 157 no 2 pp 136ndash146 2011
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
Recommended