
Dr. Lister de Lima Salgueiro
Focus Points
1. Ovarian Modern Physiology
2. Ovarian Reserve Evaluation
3. Basal Testosterone
4. Ovulation induction: Long Protocol
5. Embryo Transfer
6. Luteal Phase Support
7. OHSS management
8. Results
Modern Physiology
• Modern Physiology of the menstrual cycle
• Recruitment (window)
• Recruitment in induced cycles
• Polimorfism of FSH receptors
• Ovarian Response

Modern Physiology of Ovarian Cycle

Simple ovulation
Ovulation
Ovulation
Ovulation
Multiple ovulation – More follicles
Multiple Ovulation – Larger Window
(Two Cohorts)
Polymorphism of FSH
Receptors
FSHr Receptors – cromossome 2
Inactivating Mutations
○ Hipotalamic Amenorrea
○ Primary: homozygous
○ Secondary: heterozigous
○ Premature Ovarian failure
Activating Mutations
○ Spontaneous OHSS
○ Increase sensibility to FSH/HCG/TSH
○ Normal Espermatogênesis in the absense ofFSH

Effect of FSHr in natural
cycle
P4
SER
ASN
FSH
M
E2 < in cases with FSH

Ovarian Response ASN (Asparginine)
< number of follicles
Define cycle lenght
Decrease of negative E2 feedback
Recruitment increase
Cycle lenght increase
Higher FSH Treshold
SER (Serine) > follicle number
At least less 30 cycles
OBS: PCR determination
Polimorfism of FSH Receptors
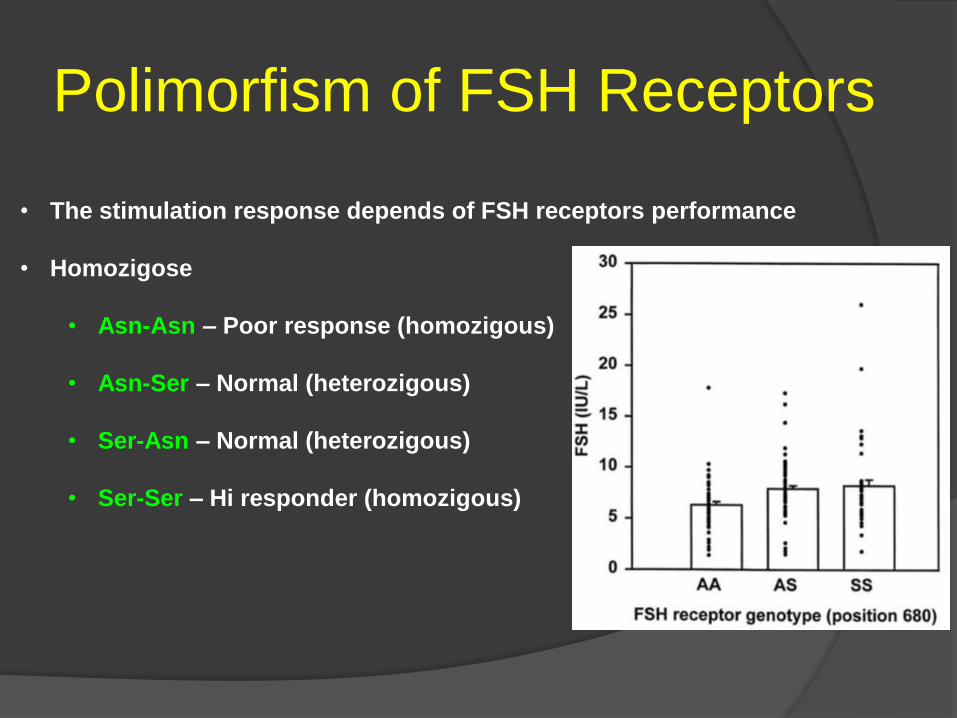
• The stimulation response depends of FSH receptors performance
• Homozigose
• Asn-Asn – Poor response (homozigous)
• Asn-Ser – Normal (heterozigous)
• Ser-Asn – Normal (heterozigous)
• Ser-Ser – Hi responder (homozigous)

Basic Concepts
• 50% From those with poor response
wil have porro response at the first cycle
• 50% increase the response in the second
cycle with the same stimulation protocol
• 70% will have better performance in the second cycle
Evaluation of Ovarian Reserve
• FSH basal
• Antral Follicle Count (AFC)
• AMH
• Basal Testosterone

Ovarian Reserve Evaluation: Basal FSH
• When measure? : Cycle Day 3
• Always measure estradiol to avoid false negatives
• Can vary from cycle to cycle
• One alteraded value- poor prognosis
• Elevated FSH (>15)- Response almost never change
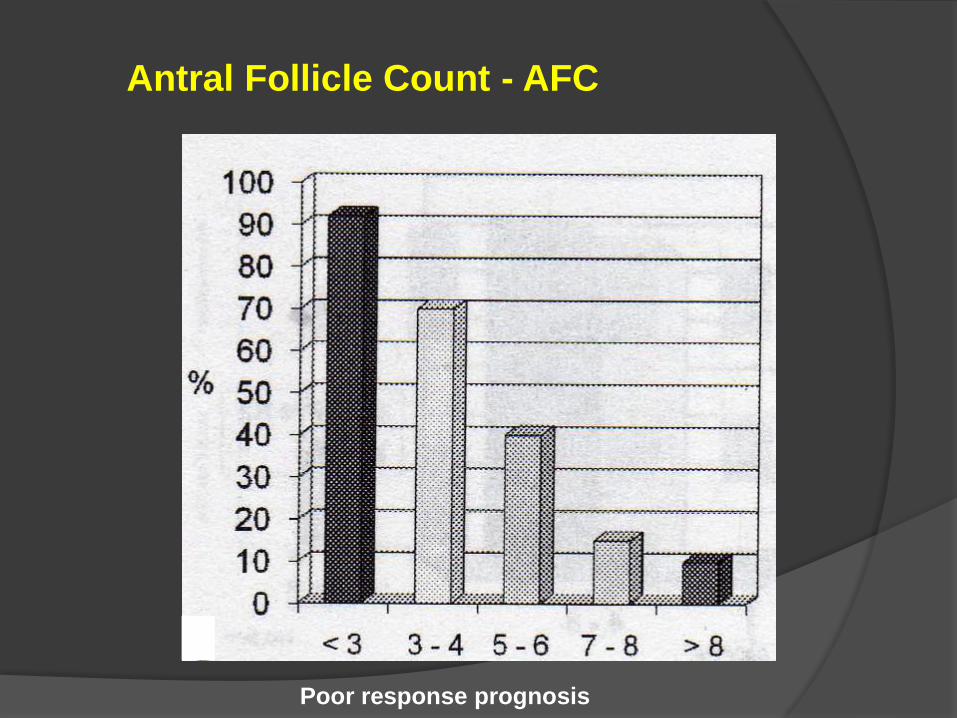
Antral Follicle Count - AFC
Poor response prognosis

AMH
Produced by Granulosa céls
From follicle primary to antral
Low or no dependence to FSH
Best ovarian age marker
< AMH can have precocious menopause
AMH not change with sequencial cycles
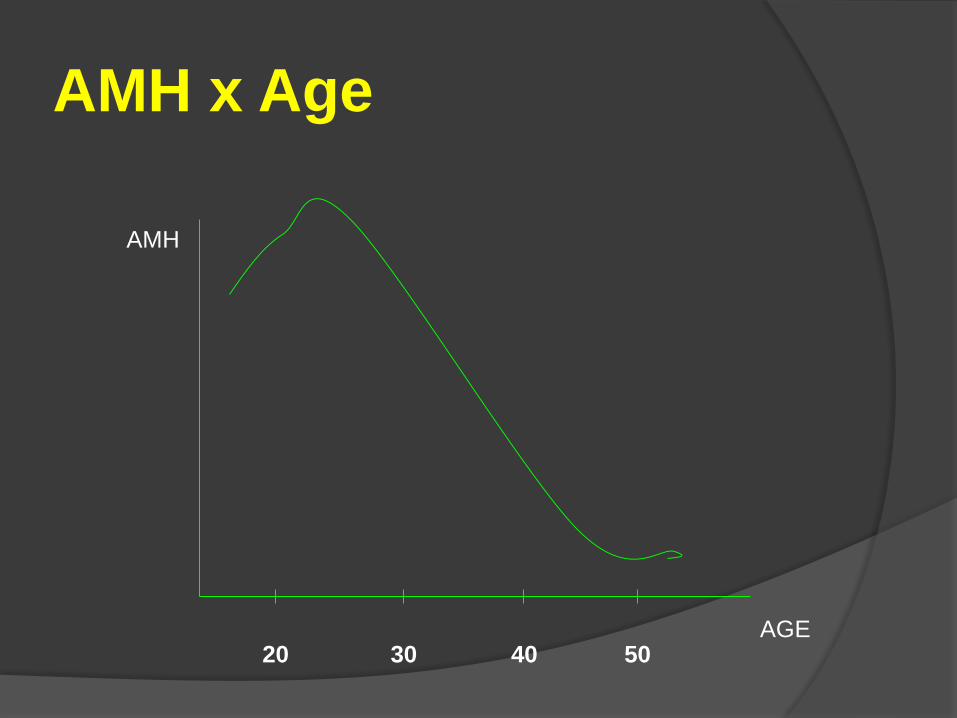
AMH x Age
20 30 40 50
AMH
AGE
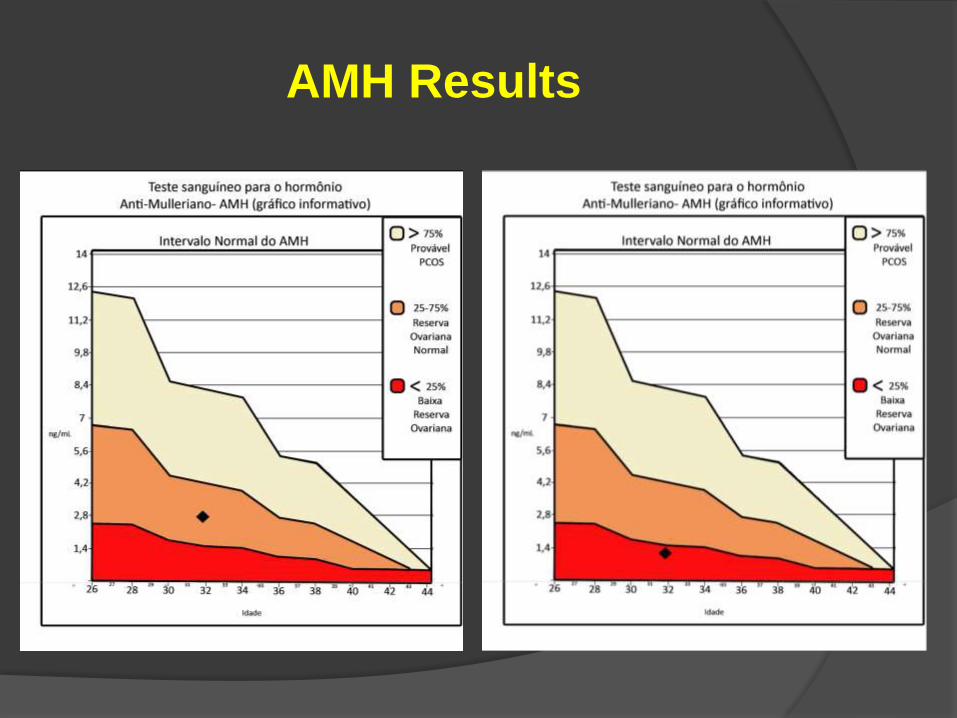
AMH Results
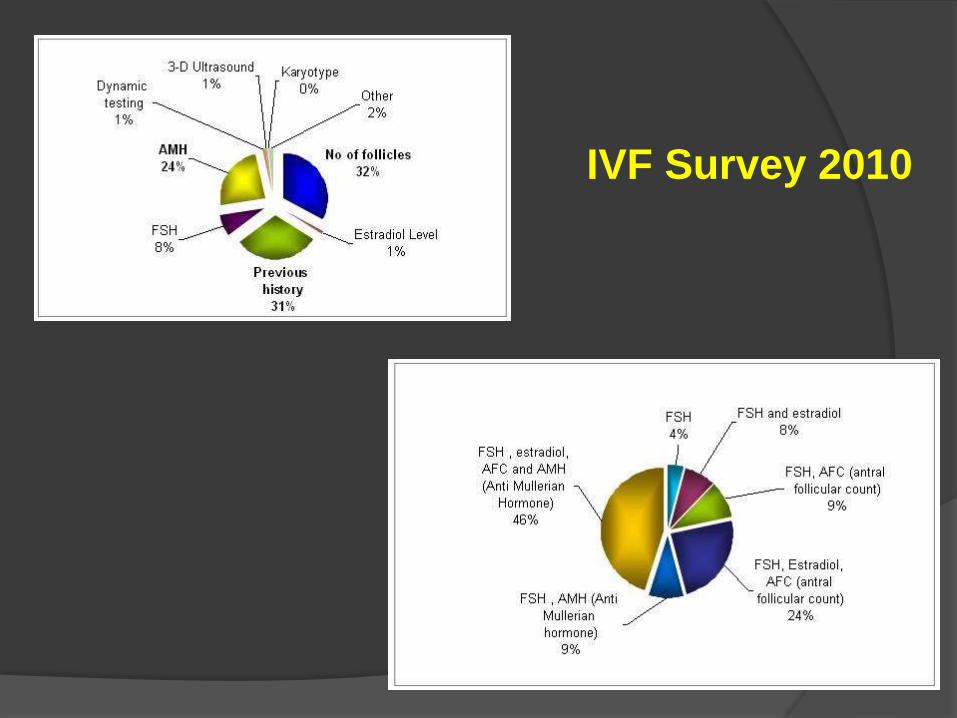
IVF Survey 2010
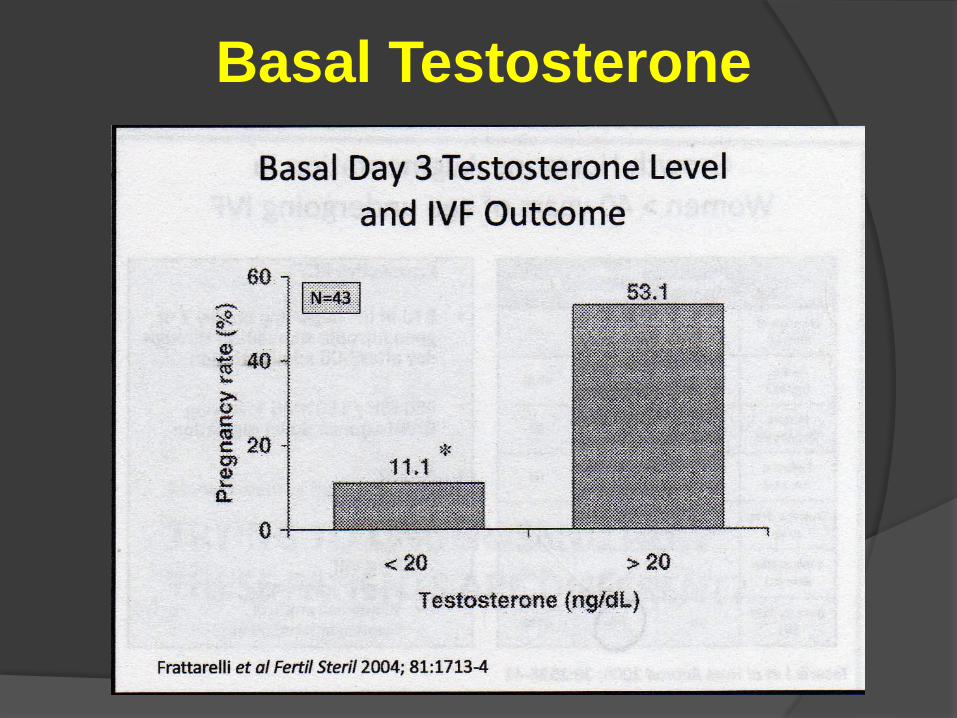
Basal Testosterone

Cycle Preparing
• Estrógens
• Andrógens
• Testosterone
• DHEA
• Aromatase Inhibitors
• Dexametasone
• LH
• GH
• ACO
• Crash IVF

Luteal Phase Supression
Estradiol:
D20 D2
E2 - 4 mg/day Gonadotrophins
Short Protocol
• E2 supress FSH
• Decresase last cycle stimulation


Androgens and Follicular
Stimulation
Synergic action of Testosterone with FSH
Prolonged Ovulation Stimulation
Association with small follicles
Can predict the ovarian response

Suplementation
Testosterone
Testogen
○ Poor responder
○ During 15-20 days
○ Without significative disfunction
○ No effect in: Number of basal follicles
Mature follicles
Oocytes
Embriyos
Pregnancy rate
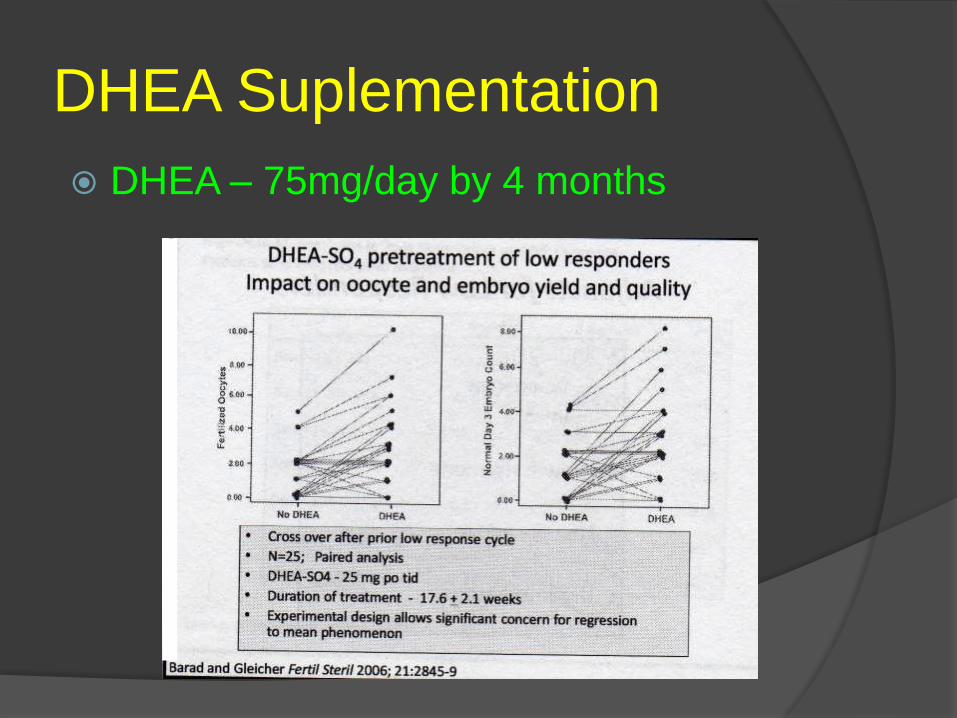
DHEA Suplementation
DHEA – 75mg/day by 4 months

DHEA Suplementation
DHEA – 75mg/day for 4 months
Benefit effect on eggs and embryos: Improve pregnancy chances
Decrease abortment rate
Improve integrity of cromossomes
Improve endometrial conditions
Reduce the aneuplydy incidence
Used by 1/3 of the clinics
Aneuplidy Origens:
- Eggs 90%
- Espermatozoa 9%
- Embryos 2%
Aromatase Inhibitors
Block transition T-DHT increasing
Testosterone
Increase of:
Antral follicles
Oocytes
Implantation rate
3 to 7 days during the cycle

Dexametasona
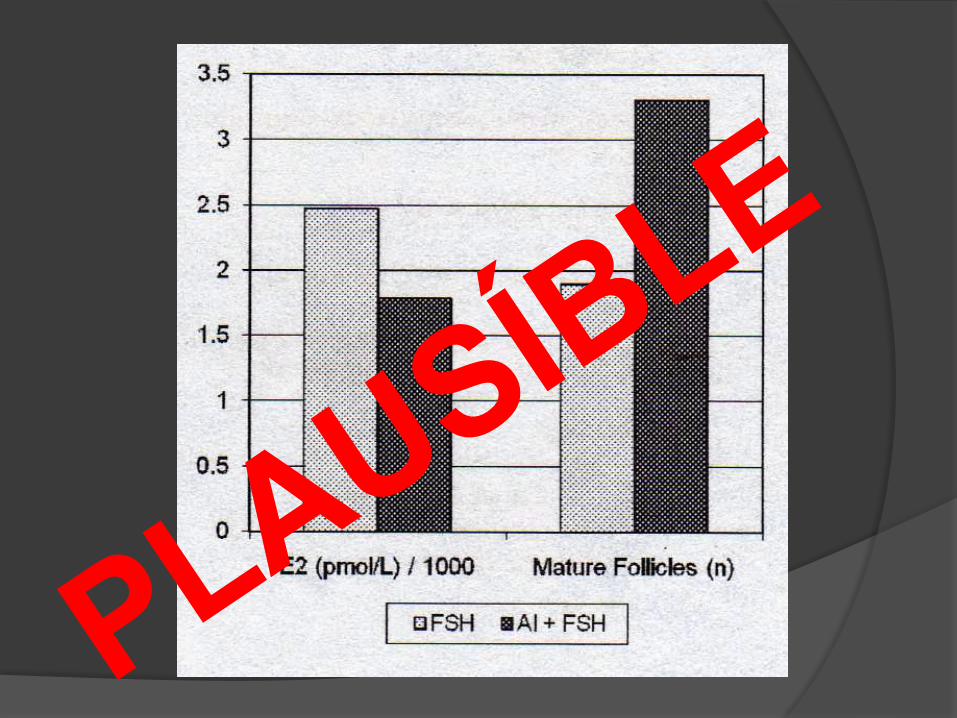
LH
Before the cycle
300 IU/day
Bloqueia com Triptorelina Depot
200 UI FSH dia
HCG com fol > 12 mm
Reduz risco de SHO
Dim. número de folículos pequenos

GH Hormônio do
Crescimento
• Cochrane Review
• Without impact on stimulation parameters:
• E2 Peak
• Stimulation Lenght
• Gonadotrophins Requirements
• Only 3 studies reported births

Oral Contraceptives
• Previous use to the cycle
• At least 15 days
• Bleeding occurs between 48 and 72h
• Stimulation must start between days 1 and 5
• Endocrinology alteration
• Follicle growth rate alterated
• Increase in FSH dose
• Increase in stimulation lenght

Luteal Phase Supression
GnRHant: Crash
D23 ou 25 D2
Gonadotrophins
Short protocol
• GnRHant supress previous cycle stimulation
• Luteólisys
3.0 g GnRHant
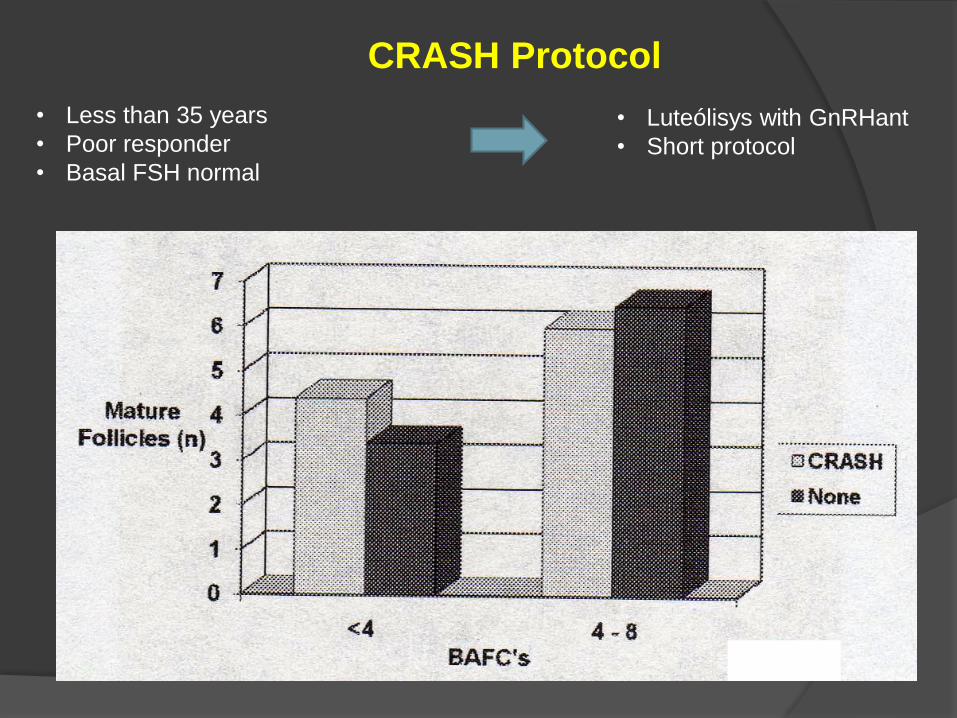
CRASH Protocol
• Less than 35 years
• Poor responder
• Basal FSH normal
• Luteólisys with GnRHant
• Short protocol
Ovulation Induction
• LH
• Less is More
• Cohort
• Choosing agonists/antagonists

LH During the cycle
Indications:
> 35 years
Suboptimal response to FSH
How Much LH?
○ 75 UI
○ LH ceiling = atresia (> 375 UI)
○ Filicori used 200 UI without problems
Use in Hipogonadotrófic/Hipogonadism

LH Window: Follicular
Phase
Agonist
Antagonist
S0 S 5-8 S - HCG

LH
LH alto no day8 – aum abortamento
Triptorelina
Leuprolida
Buserelina
Nafarelina
Incremento
na potência
do antagonista
Potência
confunde
Bosch 2008: > 35 anos
• Com e sem LH
• Taxa de gravidez igual
• Tx de implantação igual
• Taxa de abortamento igual
LH use:
• Earlier:
• Increase Androgen synthesis
• Stimulates the Recruitment
• Late
• Physiological Manutention
• Increase of E2 synthesis
• Control of the follicular growth

LH = More Euploidy
Weghofer 2008

OVULATION INDUCTION
GnRH Agonist
Individualised Dose FSH rec®1
Lupron® 1.0 mg/day/for 14 days 0.5 or 1.0mg / day
150/225 IU
per day
day1
of FSH rec®
Day7
of FSH rec® HCG rec®
day21
Down regulation
Long Protocol
Why only two Ultrassound
exams?
• First Exam day 7:
• Follicle count
• Follicle Measurement
• Endometrium classification
• Endometrium measure

Why only two Ultrassound
exams?
• Second Exam day 10 or 11:
• Follicle count
• Follicle Measurement (Growth rate)
• Endometrium classification
• Endometrium measure
• Calculate the HCG day
Follicular Cohort
• Same cohort per patient
• Dose independent
• Less is more
• Actual recommendations:
• < 30 years 150 IU/day
• > 30 years 225 IU/day

LESS IS MORE• Lower Dose of FSHr:
• Smaller Cohort
• More Syncrony
• Higher number of MII
• Less incidence of Aneuploidy
• Higher Fertilization Rate
• Higher Pregnancy Rate
Increased gonadotrophin stimulation does not improve IVF
outcomes in patients with predicted poor ovarian reserve
Dharmawijaya N Lekamge & Michelle Lane &
Robert B Gilchrist & Kelton P Tremellen

Less Than 30 years
• Low Responders: Upgrade to 30/37 years protocol
• Normal Responders:
• Gonal-F 150 IU for seven days
• Step-down to 75 IU
• Keep untill the day before HcG
• High Responders:
• Gonal-F 150 IU for 3 days
• Step-down to 75 IU
• Keep untill the day before HcG

From 30 to 37 years
• Low Responders: Upgrade to >37 years protocol
• Normal Responders:
• Gonal-F 225 IU for seven days
• Step-down to 150 IU (one day)
• Step-down to 75 IU
• Keep untill the day before HcG
• High Responders:
• Gonal-F 225 IU for 3 days
• Step-down to 150 IU (day 4)
• Step-down to 75 IU
• Keep untill the day before HcG

More Than 37 years
• Low Responders: Do not Upgrade the dose
• Normal Responders:
• Gonal-F 300 IU for seven days
• Step-down to 225 IU (one day)
• Step-down to 150 IU (one day)
• Step-down to 75 IU
• Keep untill the day before HcG
• High Responders:
• Gonal-F 300 IU for 3 days
• Step-down to 225 IU (day 4)
• Step-down to 150 IU (day 5)
• Step-down to 75 IU
• Keep untill the day before HcG

Why use Step-down
Protocol?
• Respect the Physiology
• Avoid the second cohort recruitment
• Prevent Assincrony
• More Mature follicles


Why choose Agonist
Protocol?• Better response
• Possibility to use almost fix protocol
• Less FSHr dose
• Less Assincrony
• Less Aneuploidy
• Higher number of mature eggs (MII)
• Higher Fertilization Rate
• Less incidence of moderate OHSS (2%)
• Higher Pregancy Rate
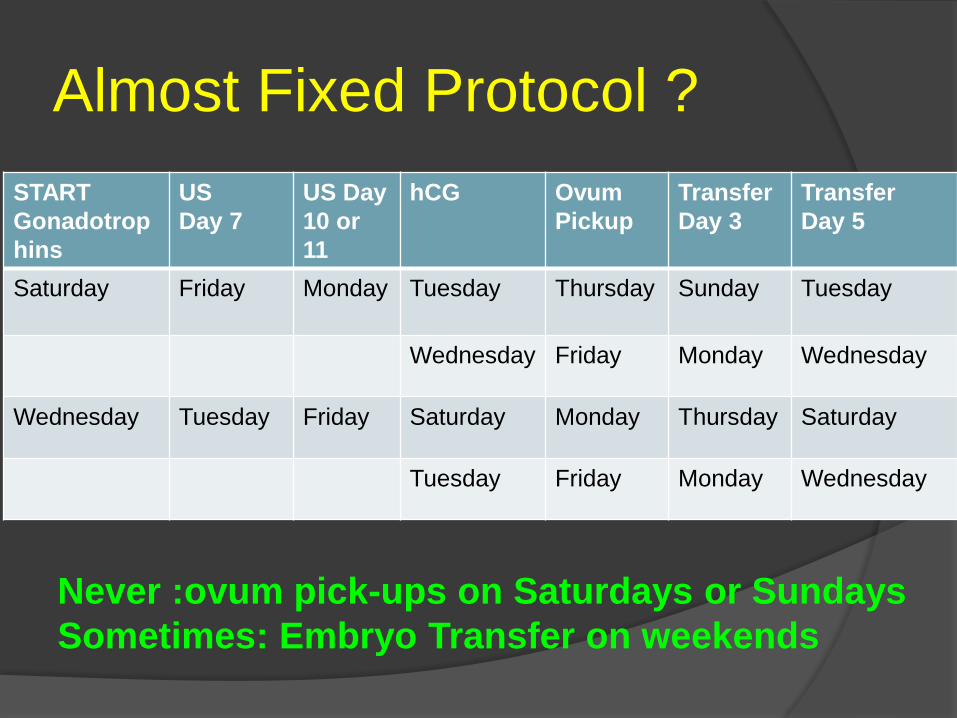
Almost Fixed Protocol ?
START
Gonadotrop
hins
US
Day 7
US Day
10 or
11
hCG Ovum
Pickup
Transfer
Day 3
Transfer
Day 5
Saturday Friday Monday Tuesday Thursday Sunday Tuesday
Wednesday Friday Monday Wednesday
Wednesday Tuesday Friday Saturday Monday Thursday Saturday
Tuesday Friday Monday Wednesday
Never :ovum pick-ups on Saturdays or Sundays
Sometimes: Embryo Transfer on weekends
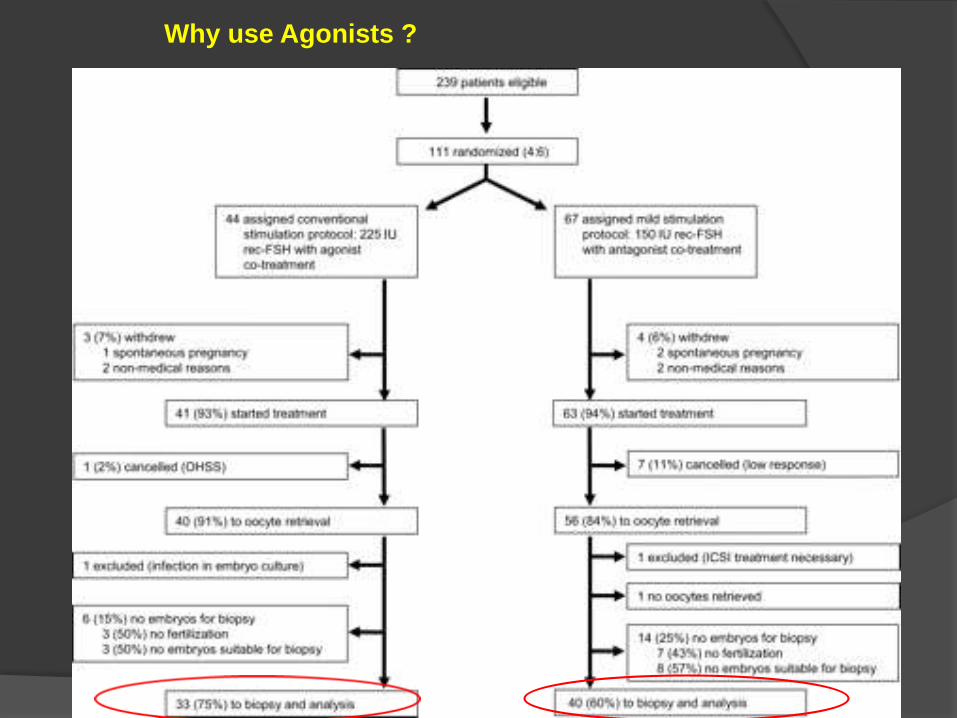
Why use Agonists ?
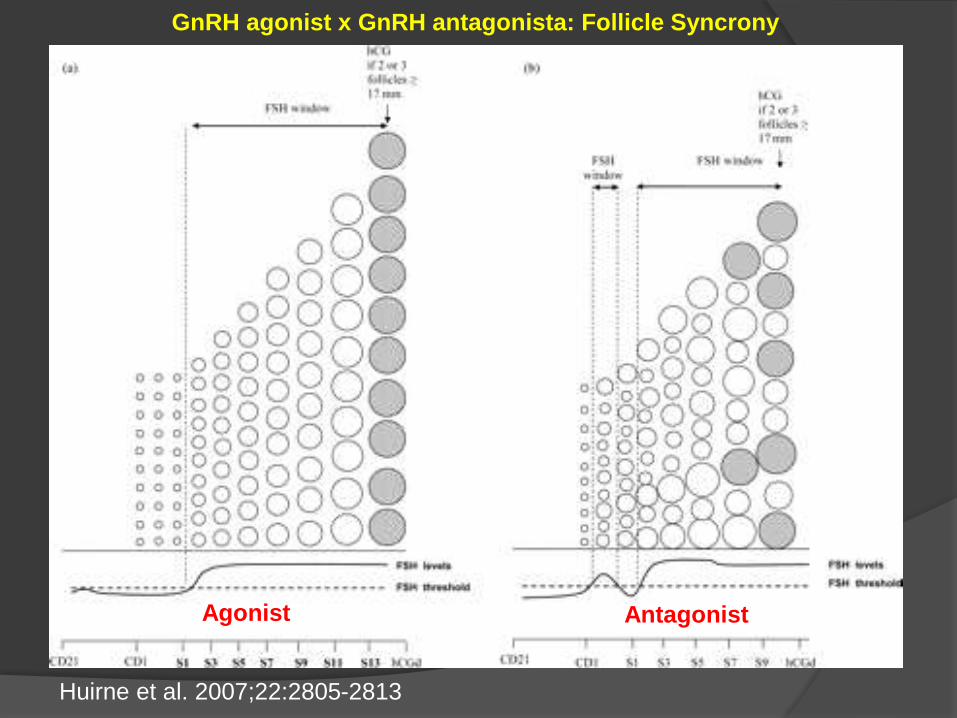
Huirne et al. 2007;22:2805-2813
GnRH agonist x GnRH antagonista: Follicle Syncrony
Agonist Antagonist

Implantation Window

Progesterone on hCG Day
• Measure P4 on hCG day
• > 1,5 cycle lost (?)
• Antagonist 4/7/before hCG

TOTAL
P4 Level Number BhCG + % Ongoing % Abortion % Ong Pregn Rate
P4 <1,00 303 158 52,1% 109 69,0% 49 29,0% 36,0%
P4 1,0 a 2,0 310 131 42,2% 84 64,1% 47 25,9% 27,1%
P4 2,0 a 3,0 31 9 29,0% 7 77,7% 2 28,5% 22,5%
P4 3,0 a 4,0 7 2 28,5% 1 50,0% 1 50,0% 14,3%
P4 > 4,0 14 2 14,3% 1 50,0% 1 50,0% 7,1%
LESS THAN 35 YEARS
P4 Level Number BhCG + % Ongoing % Abortion % Ong Pregn Rate
P4 <1,00 173 111 64,1% 14 12,6%
P4 1,0 a 2,0 195 87 44,6% 15 17,2%
P4 2,0 a 3,0 20 5 25,0% 0 0,0%
P4 3,0 a 4,0 5 2 40,0% 0 0,0%
P4 > 4,0 9 1 11,1% 0 0,0%
Progesterone limitation
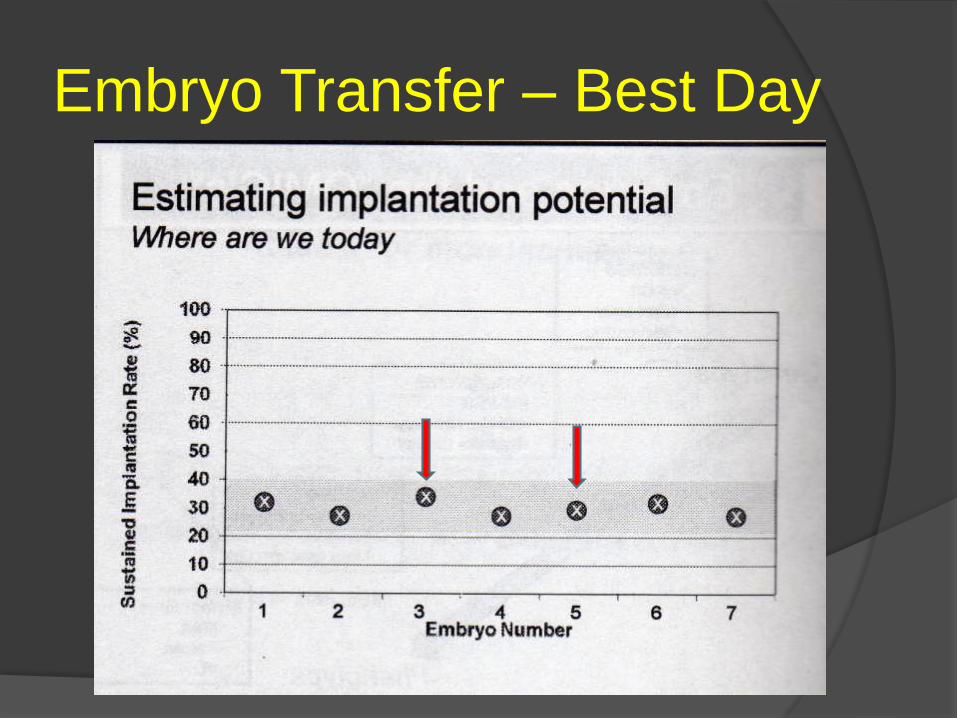
Embryo Transfer – Best Day

Aspirin
• Low dose: Aspirin prevent 100
• Increase:
• Ovarian Response
• Ovarian and Uterine blood influx
• Implantation Rate
• Pregnancy Rate (15%)
• Risk of Haemorragic accidents

OHSS (Old)
• Coasting: maximun 2 days
• Renin/angiotensin Blockers:
• Dostinex 1 pill/VO/day/7 days
• Losartana 10 mg 1 pill/VO/day/7 days
+
• Enalapril 8 mg ½ pill/VO/2x day/ 7 days
• Quinagolide 100 mg 1 cp/VO/day/ 7 days

OHSS (New)
• Normal Ovum Pickup
• Presence of Symptoms:
• Ovarian enlargement
• Slow Intestinal transit.
• Ascitis
• Frezze All (Eggs or Embryos)
• Aplication of 4 Cetrotide Syringes (At the same time)
• Regression of the symptoms in 4 days
• Transfer in the next cycle
• OHSS incidence : 2% of the cycles
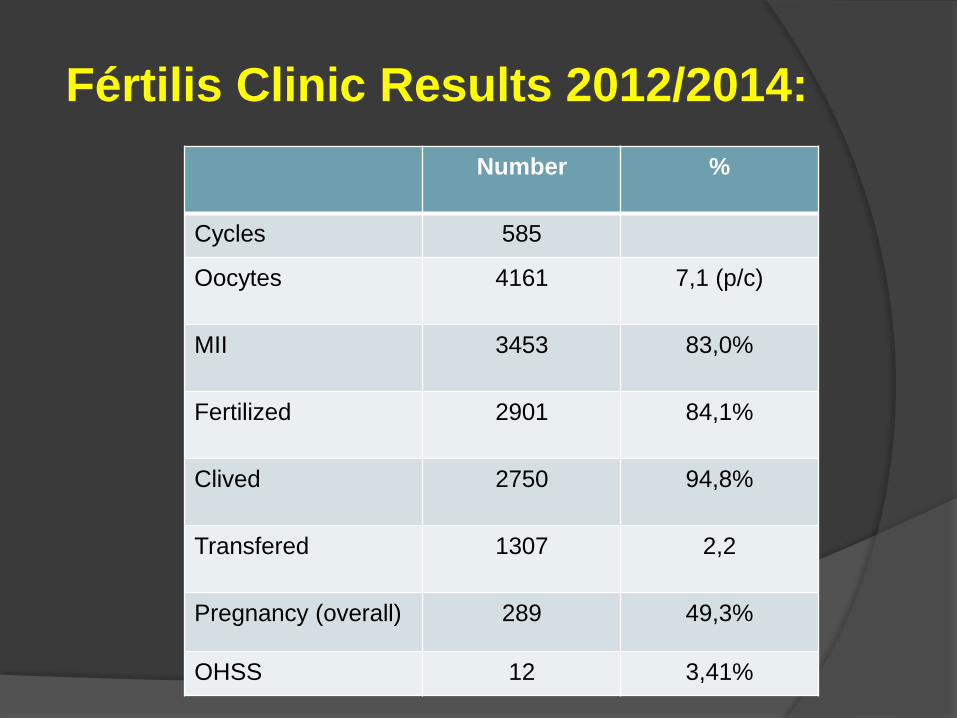
Fértilis Clinic Results 2012/2014:
Number %
Cycles 585
Oocytes 4161 7,1 (p/c)
MII 3453 83,0%
Fertilized 2901 84,1%
Clived 2750 94,8%
Transfered 1307 2,2
Pregnancy (overall) 289 49,3%
OHSS 12 3,41%

Fértilis Clinic Results Per
Age:
Age Number of
Cases
% Positive
<35 259 60,5%
36-40 111 50,5%
>41 54 39,0%
Why should I change to Antagonists???

END
WWW.FERTILIS.COM.BR
Recommended

















