Copyright © 2009 by Allyn & Bacon
Why Do Many People Eat Too Much?
Chapter 12Hunger, Eating, and Health

Copyright © 2009 by Allyn & Bacon
Control of Eating Is there a “set point” for the body’s energy
reserves that determines when we eat? The prevalence of eating disorders suggests
that this may not be the case Over half of the adult population in the U.S.
meets clinical criteria for obesity The average American consumes 3,800 calories
per day – about twice the average requirement

Copyright © 2009 by Allyn & Bacon
Digestion, Energy Storage, and Energy Utilization
Purpose of eating is to provide the body with molecular building blocks and energy
Digestion – breaking down food and absorbing its constituents
Energy storage in the body Lipids (fats) Amino acids (proteins) Glucose (carbohydrates)

Copyright © 2009 by Allyn & Bacon

Copyright © 2009 by Allyn & Bacon
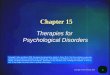
Energy Storage in the Body
Energy delivered to the body as lipids, amino acids, and glucose
Stored as fats, glycogen, and proteins Fats are most efficient for energy storage
One gram of fat stores twice as much energy as one gram of glycogen

Copyright © 2009 by Allyn & Bacon
Three Phases of Energy Metabolism
Energy metabolism: Chemical changes that make energy available for use
Cephalic phase – preparation for eating Absorptive phase – energy absorbed Fasting phase
Withdrawing energy from reserves Ends with next cephalic phase

Copyright © 2009 by Allyn & Bacon
Three Phases of Energy Metabolism (continued)
Controlled by two pancreatic hormones Insulin – high during cephalic and
absorptive phases triggers glucose use as fuel by body cells triggers conversion of bloodborne energy to fat,
glycogen, and protein triggers energy storage in adipose cells, liver, and
muscles Glucagon – high during fasting phase
triggers change of stored energy to usable fuel: fat to free fatty acids and then ketones; protein to glucose

Copyright © 2009 by Allyn & Bacon

Copyright © 2009 by Allyn & Bacon
Hunger and Eating: Set Points vs. Positive Incentives
The Set-Point Assumption: Despite lack of evidence, most believe that
hunger is a response to an energy need; we eat to maintain an energy set point Glucostatic and lipostatic theory
Positive Incentive Theory

Copyright © 2009 by Allyn & Bacon
Problems with Set-Point Theo-ries of Hunger and Eating
Epidemic of eating disorders Contrary to evolutionary pressures that
favored energy storage for survival Reductions in blood glucose or body fat do
not reliably induce eating Do not account for the influence of external
factors on eating and hunger

Copyright © 2009 by Allyn & Bacon
Physiological Research on Hunger and Satiety Role of blood glucose levels Myth of hypothalamic centers Role of the GI tract Hunger and satiety peptides Serotonin and satiety

Copyright © 2009 by Allyn & Bacon
Role of Blood Glucose Levels in Hunger and Satiety
Blood glucose drops prior to a meal as preparation to eat – not a cue to eat
Must decrease blood glucose by 50% to trigger feeding
Premeal glucose infusions often do not suppress eating
Reduced blood glucose may contribute to hunger, but changes in blood glucose do not prevent hunger or satiety

Copyright © 2009 by Allyn & Bacon
Myth of Hypothalamic Hunger and Satiety Centers Experiments suggested two hypo-
thalamic centers Ventromedial (VMH) – a satiety center Lateral (LH) – a hunger center
Lesions of VMH produce hyperphagia Lesions of LH produce aphagia and
adipsia

Copyright © 2009 by Allyn & Bacon

Copyright © 2009 by Allyn & Bacon
Myth of Hypothalamic Hunger and Satiety Centers (continued)
VMH lesion rats maintain a new higher weight
LH lesion rats will recover if kept alive by tube feeding
Hypothalamus – regulates energy metabolism

Copyright © 2009 by Allyn & Bacon
Myth of Hypothalamic Hunger and Satiety Centers (continued)
VMH lesions increase blood insulin Lipogenesis (fat production) increases Lipolysis (fat breakdown) decreases All calories are quickly stored so the rat
must eat more to meet immediate needs Same results seen with lesions of
noradrenergic bundle or paraventricular nuclei

Copyright © 2009 by Allyn & Bacon
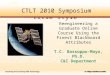
Location of hypothalamic
nuclei that impact feeding
behavior
Myth of HypothalamicHunger and SatietyCenters (continued)

Copyright © 2009 by Allyn & Bacon
Role of the Gastrointestinal Tract in Satiety
Cannon and Washburn (1912) Studies suggested stomach contractions led to
hunger, distension to satiety But – hunger is still experienced with no
stomach Blood borne satiety signals?

Copyright © 2009 by Allyn & Bacon

Copyright © 2009 by Allyn & Bacon
Hunger and Satiety Peptides
Gut peptides that decrease meal size: cholecystokinin (CCK), bombesin, glucacon,
alpha-melanocyte-stimulating hormone, somatostatin
Must first establish that peptide does not merely create illness
CCK causes nausea at high doses, but suppresses food intake at doses insufficient to induce taste aversions

Copyright © 2009 by Allyn & Bacon
Hunger Peptides Usually synthesized in the
hypothalamus – neuropeptide Y, galanin, orexin-A, ghrelin
Many different signals control eating (not just glucose and fat)
Hypothalamus plays a central role – microinjections of some peptides have major effects on eating

Copyright © 2009 by Allyn & Bacon
Serotonin and Satiety
Serotonin agonists consistently reduce rats’ food intake Even intake of palatable food is affected Reduces amount eaten per meal Preferences shift away from fatty foods
Similar effects seen in humans

Copyright © 2009 by Allyn & Bacon
Serotonin and Satiety: Prader-Willi Syndrome
Possible key to understanding neural basis of obesity
Symptoms Food-related: insatiable appetite, extremely slow
metabolism; eventual death in adulthood from obesity-related diseases
Other symptoms: weak muscles, small hands and feet, triangular mouth, stubbornness, feeding difficulties in infancy, tantrums, compulsivity, skin picking
Damage or absence of a section of chromosome 15

Copyright © 2009 by Allyn & Bacon
Why Is There an Epidemic of Obesity? Evolution favored preferring high-
calorie food, eating to capacity, storing fat, and using energy efficiently
Cultural practices and beliefs promote consumption

Copyright © 2009 by Allyn & Bacon
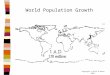
The five stages of a typical weight-loss program.

Copyright © 2009 by Allyn & Bacon
Why Do Some People Be-come Obese and Some Not?
Energy input differences Craving for high-calorie foods Cultural norms Large cephalic-phase response to sight and
smell of food Energy output differences
Exercise Diet-induced thermogenesis NEAT (nonexercise activity thermogenesis)

Copyright © 2009 by Allyn & Bacon
Leptin and the Regulation of Body Fat
Leptin – a negative feedback fat signal Hormone released by fat cells Leptin receptors found in the brain
ob/ob mice are three times normal weight Homozygous for a mutant gene ob Lack leptin Eat more, and store fat more efficiently than
controls Human leptin research
However, most obese humans have high leptin levels. Leptin injections help the few ob/ob humans

Copyright © 2009 by Allyn & Bacon
Insulin, Leptin, and the Arcuate Melanocortin System
Insulin brain levels reflect visceral fat; leptin levels reflect subcutaneous fat
Both insulin and leptin receptors found in the arcuate nucleus of the hypo-thalamus

Copyright © 2009 by Allyn & Bacon
Serotonergic Drugs and the Treatment of Obesity
Serotonin appears to increase short-term satiety signals associated with the consumption of a meal and decrease… urge to eat high-calorie foods consumption of fat intensity of hunger size of meals number of snacks and bingeing
Early serotonin agonists produced heart disease in some patients, was withdrawn, and not yet replaced

Copyright © 2009 by Allyn & Bacon
Anorexia Nervosa and Bulimia Nervosa
Anorexia Voluntary self-starvation Fatal in 10% of patients
Bulimia – bingeing and purging Similar symptoms, difficult to distinguish
Distorted body image Strike educated, affluent young females Associated with obsessive-compulsive disorder
and depression
Recommended