COPERNICUSCOPERNICUSandand
carvedilolcarvedilol
Background and Background and principal results slide kitprincipal results slide kit
December 2000December 2000

NorepinephrineNorepinephrineAngiotensin IIAngiotensin II
Hypertrophy, apoptosis, ischaemia,Hypertrophy, apoptosis, ischaemia,arrhythmia, remodelling, fibrosisarrhythmia, remodelling, fibrosis
ACE inhibitors in heart failureACE inhibitors in heart failure
Approximately 7,000 patients evaluated in Approximately 7,000 patients evaluated in placebo-controlled clinical trialsplacebo-controlled clinical trials
Consistent improvement in cardiac function, Consistent improvement in cardiac function, symptoms and clinical statussymptoms and clinical status
Decrease in all-cause mortality by 20-25% Decrease in all-cause mortality by 20-25% (p<(p<0.001)0.001)
Decrease in combined risk of death and Decrease in combined risk of death and hospitalisation by 20-25% (hospitalisation by 20-25% (pp<0.001)<0.001)
US Consensus Recommendations (1996)US Consensus Recommendations (1996)
ACE inhibitors in heart failureACE inhibitors in heart failure
Consensus recommendationsConsensus recommendations
All patients with heart failure due to left ventricular All patients with heart failure due to left ventricular
systolic dysfunction should receive an ACE inhibitor systolic dysfunction should receive an ACE inhibitor
unless they have a contraindication to its use or unless they have a contraindication to its use or
cannot tolerate treatment with the drugcannot tolerate treatment with the drug

SOLVD PreventionSOLVD Prevention(enalapril)(enalapril)
Class IClass I Class IVClass IV
SOLVD Treatment (enalapril)SOLVD Treatment (enalapril)V-HeFT II (enalapril)V-HeFT II (enalapril)
CONSENSUSCONSENSUS(enalapril)(enalapril)
Class IIClass IIClass IIIClass III

blockersblockers
Over 13,000 patients evaluated in placebo-Over 13,000 patients evaluated in placebo-controlled clinical trialscontrolled clinical trials
Consistent improvement in cardiac function, Consistent improvement in cardiac function, symptoms and clinical statussymptoms and clinical status
Decrease in all-cause mortality by 30–35% Decrease in all-cause mortality by 30–35% ((p<p<0.0001)0.0001)
Decrease in combined risk of death and Decrease in combined risk of death and hospitalisation by 25–30% (hospitalisation by 25–30% (p<p<0.0001)0.0001)

Carvedilol(n=696)
Placebo(n=398)
Survival
Days
0 50 100 150 200 250 300 350 400
1.0
0.9
0.8
0.7
0.6
0.5
Risk reduction = 65%Risk reduction = 65%p<0.001
Packer et al (1996)
Lancet (1999)0 200 400 600 800
1.0
0.8
0.6
0
Bisoprolol
Placebo
Time after inclusion (days)
p<0.0001
Survival
Risk reduction = 34%Risk reduction = 34%
The MERIT-HF Study Group (1999)
Months of follow-up
Mortality %
0 3 6 9 12 15 18 21
20
15
10
5
0
Placebo
Metoprolol CR/XL
p=0.0062
Risk reduction = 34%Risk reduction = 34%
US Carvedilol StudyUS Carvedilol Study
blockers in blockers in heart failure -heart failure -
all-cause mortalityall-cause mortality
CIBIS-IICIBIS-II MERIT-HFMERIT-HF

blockers in heart failureblockers in heart failure
Consensus recommendationsConsensus recommendations
All patients with stable class II or III heart failure due All patients with stable class II or III heart failure due
to left ventricular systolic dysfunction should to left ventricular systolic dysfunction should
receive a receive a blocker (in addition to an ACE inhibitor) blocker (in addition to an ACE inhibitor)
unless they have a contraindication to its use or unless they have a contraindication to its use or
cannot tolerate treatment with the drugcannot tolerate treatment with the drug
Why are the recommendations more restrictive than Why are the recommendations more restrictive than for ACE inhibitors despite the available evidence?for ACE inhibitors despite the available evidence?

Class IIClass IIClass IIIClass III
Class IClass I Class IVClass IV
US Carvedilol Programme (carvedilol)US Carvedilol Programme (carvedilol)CIBIS II (bisoprolol)CIBIS II (bisoprolol)
MERIT-HF (metoprolol)MERIT-HF (metoprolol)
?? ??
Packer, AHA 2000Packer, AHA 2000

blockers in NYHA class IV heart failureblockers in NYHA class IV heart failure
Proportion of patientsProportion of patientswith class IV heart failurewith class IV heart failure
US Carvedilol Programme US Carvedilol Programme 3% 3%
MERIT-HFMERIT-HF 4% 4%
CIBIS-IICIBIS-II 17%17%
BESTBEST 8% 8%

MERIT-HFMERIT-HF
CIBIS IICIBIS II
BESTBEST
Favours treatmentFavours treatment Favours placeboFavours placebo0.50.50.250.25 0.750.75 1.51.5 2.02.01.01.0
Survival effects of Survival effects of blockers in blockers inclass IV heart failureclass IV heart failure
Packer, AHA 2000Packer, AHA 2000

Effects of metoprolol inEffects of metoprolol inclass IV heart failureclass IV heart failure
0.50.50.250.25 0.750.75 1.51.5 2.02.01.01.0
Death or CHFDeath or CHFhospitalisationhospitalisation
Death or anyDeath or anyhospitalisationhospitalisation
Favours treatmentFavours treatment Favours placeboFavours placebo
Results of MERIT-HFResults of MERIT-HF
Packer, AHA 2000Packer, AHA 2000

??
Class IClass I Class IVClass IV
US Carvedilol (carvedilol)US Carvedilol (carvedilol)CIBIS II (bisoprolol)CIBIS II (bisoprolol)
MERIT-HF (metoprolol)MERIT-HF (metoprolol)
COPERNICUSCOPERNICUS(carvedilol)(carvedilol)
Class IIClass IIClass IIIClass III
Packer, AHA 2000Packer, AHA 2000

CCarvedilarvedilool l PProsprospeective ctive RRaanndomdomiizedzedCCumumuulative lative SSurvival Trialurvival Trial
COPERNICUSCOPERNICUS
Objectives and designObjectives and design
To determine the effect of carvedilol compared To determine the effect of carvedilol compared with placebo on all-cause mortality in patients with placebo on all-cause mortality in patients with severe chronic heart failurewith severe chronic heart failure
Randomised, placebo-controlled, parallel-group Randomised, placebo-controlled, parallel-group multicenter study in patients with ischaemic or multicenter study in patients with ischaemic or non-ischaemic cardiomyopathynon-ischaemic cardiomyopathy

COPERNICUSCOPERNICUS
Patient CharacteristicsPatient Characteristics
Symptoms of heart failure at rest or minimal exertion Symptoms of heart failure at rest or minimal exertion for at least 2 monthsfor at least 2 months
LV ejection fraction <25%LV ejection fraction <25%
Receiving diuretics and an ACE inhibitor Receiving diuretics and an ACE inhibitor (+ digitalis) (+ digitalis) 2 months. Diuretics optimised to achieve 2 months. Diuretics optimised to achieve euvolaemiaeuvolaemia
No need for intensive care and no treatment with IV No need for intensive care and no treatment with IV inotropic or IV vasodilator therapy within 4 days of inotropic or IV vasodilator therapy within 4 days of screeningscreening
Packer, AHA 2000Packer, AHA 2000

Patients not in COPERNICUSPatients not in COPERNICUS
Hospitalised patients were allowed in the trial but Hospitalised patients were allowed in the trial but not if they were in the CCU/ICUnot if they were in the CCU/ICU
Patients receiving IV diuretics were allowed in the Patients receiving IV diuretics were allowed in the trial but not if they had received IV vasodilator or trial but not if they had received IV vasodilator or IV positive inotropic drugs within 4 days of IV positive inotropic drugs within 4 days of screeningscreening
Diuretics were to be titrated until patients were Diuretics were to be titrated until patients were euvolaemic. Those with marked fluid retention or euvolaemic. Those with marked fluid retention or overload were not randomizedoverload were not randomized
RandomisationRandomisation
2289 patients were randomized 1:12289 patients were randomized 1:1
PlaceboPlacebo
CarvedilolCarvedilol
Initial dose 3.125 mg bid with doubling of dose Initial dose 3.125 mg bid with doubling of dose every 2 weeks until target dose of 25 mg bid was every 2 weeks until target dose of 25 mg bid was reached. Patients received highest tolerated dosereached. Patients received highest tolerated dose
COPERNICUSCOPERNICUS

COPERNICUSCOPERNICUS
Protocol-specified endpointsProtocol-specified endpoints
Primary endpointPrimary endpoint
– All-cause mortalityAll-cause mortality
Secondary endpoints Secondary endpoints
– All-cause mortality or hospitalisations for any All-cause mortality or hospitalisations for any reasonreason
– All-cause mortality or cardiovascular All-cause mortality or cardiovascular hospitalisations hospitalisations
– All-cause mortality or CHF hospitalisations All-cause mortality or CHF hospitalisations
Packer, AHA 2000Packer, AHA 2000
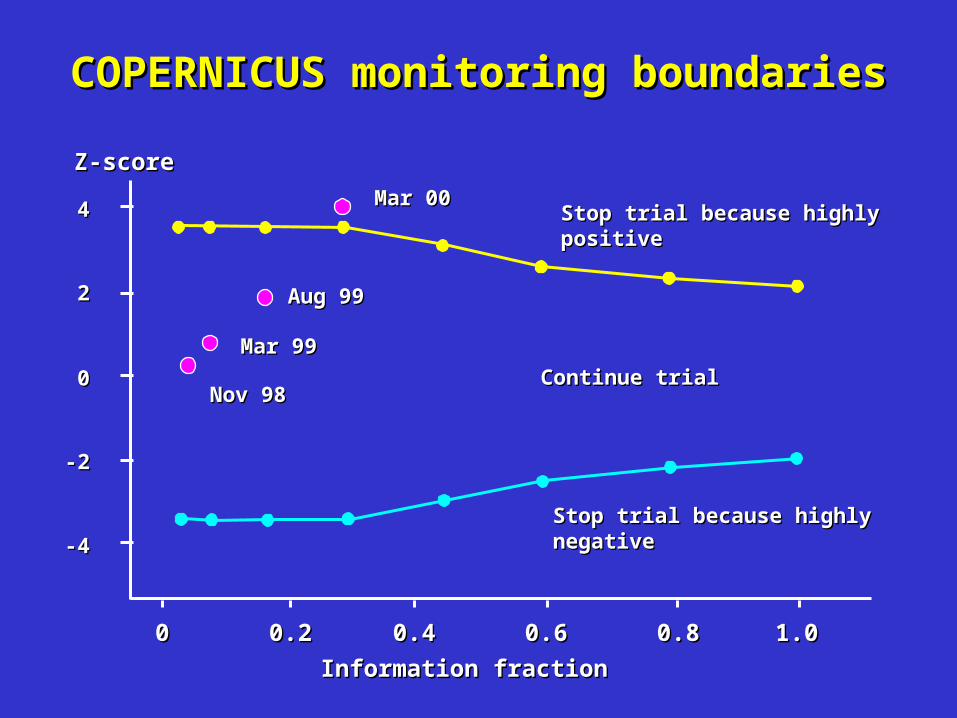
COPERNICUS monitoring boundariesCOPERNICUS monitoring boundaries
Stop trial because highly Stop trial because highly positivepositive
Continue trialContinue trial
Z-scoreZ-score
Information fractionInformation fraction
0.20.2
00
22
44
-2-2
-4-4
0.40.4 0.60.6 0.80.8 1.01.000
Stop trial because highly Stop trial because highly negativenegative
Mar 00Mar 00
Aug 99Aug 99
Mar 99Mar 99
Nov 98Nov 98

COPERNICUSCOPERNICUS
DSMB recommendations (14 March 2000)DSMB recommendations (14 March 2000)
Highly significant effect on mortalityHighly significant effect on mortality
Exceeded predefined criteria for early terminationExceeded predefined criteria for early termination
Consistent across all predefined subgroupsConsistent across all predefined subgroups
Serious adverse events more common on placeboSerious adverse events more common on placebo
Unanimous recommendation for early terminationUnanimous recommendation for early termination
All patients should be offered open-label carvedilolAll patients should be offered open-label carvedilol

0000
% S
urv
ival
% S
urv
ival
33 66 99 1212 1515 1818 2121MonthsMonths
100100
9090
8080
6060
7070
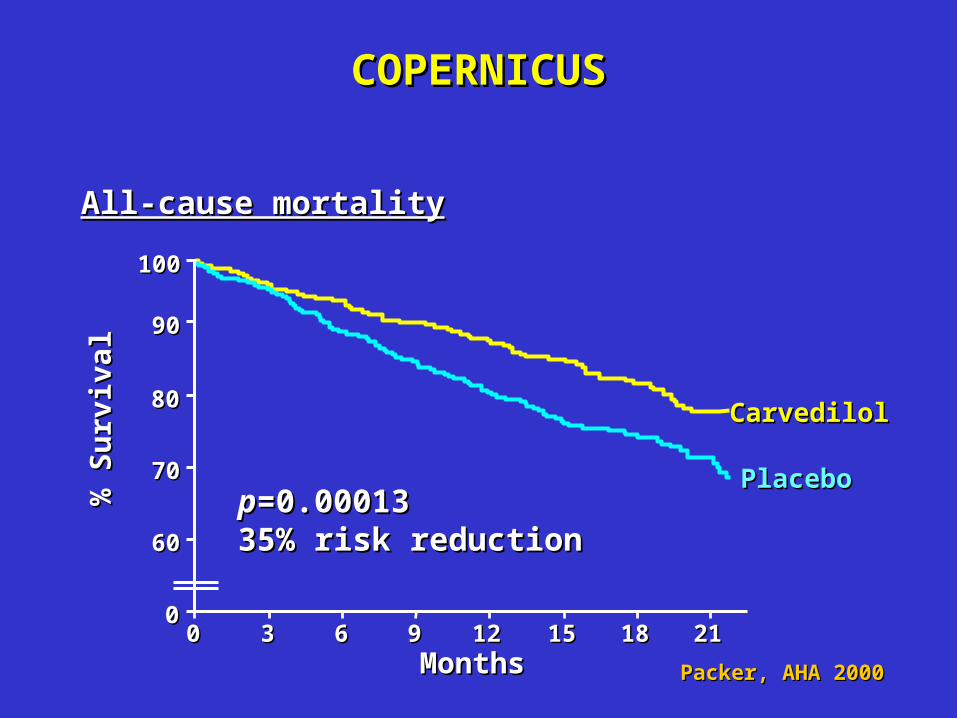
pp=0.00013=0.0001335% risk reduction35% risk reduction
CarvedilolCarvedilol
PlaceboPlacebo
COPERNICUSCOPERNICUS
All-cause mortalityAll-cause mortality
Packer, AHA 2000Packer, AHA 2000

Mortality in Mortality in blocker heart failure trials blocker heart failure trials
Annual placeboAnnual placebomortality ratesmortality rates
MERIT-HFMERIT-HF 11.0%11.0%
US Carvedilol ProgrammeUS Carvedilol Programme 11.1%11.1%
CIBIS IICIBIS II 13.2%13.2%
BESTBEST 16.6%16.6%
COPERNICUSCOPERNICUS 19.7%19.7%
Class IV meta-analysisClass IV meta-analysis 20.7%20.7%
Packer, AHA 2000Packer, AHA 2000

StabilisedStabilisedclass IVclass IV
UnstableUnstableclass IVclass IV
Annual Annual placeboplacebomortalitymortality
raterate
24-29%24-29% 30%30%18-23%18-23%
PRAISE-1PRAISE-1PROMISEPROMISE
CONSENSUSCONSENSUSFIRSTFIRST
COPERNICUSCOPERNICUSRALESRALES
Spectrum of trials in severe heart failureSpectrum of trials in severe heart failure
Packer, AHA 2000Packer, AHA 2000

PlaceboPlacebo
CarvedilolCarvedilol
COPERNICUSCOPERNICUS
2424
00
66
1212
1818
1-year Kaplan-1-year Kaplan-Meier ratesMeier rates
Annual mortalityAnnual mortalityrates (per pt-year)rates (per pt-year)
19.719.7
12.812.8
18.518.5
11.411.4
All-cause mortalityAll-cause mortality
Packer, AHA 2000Packer, AHA 2000

Treatment EffectTreatment Effect pp-Value-Value
Death or hospitalisationsDeath or hospitalisations 24%24% <0.0001<0.0001for any reasonfor any reason
Death or hospitalisationsDeath or hospitalisations 27%27% <0.0001<0.0001for cardiovascular reasonfor cardiovascular reason
Death or hospitalisationsDeath or hospitalisations 31%31% <0.0001<0.0001for heart failurefor heart failure
COPERNICUSCOPERNICUS
Packer, AHA 2000Packer, AHA 2000

Favours treatmentFavours treatment Favours placeboFavours placebo
BESTBEST
COPERNICUSCOPERNICUS
Is the carvedilol benefit a class effect?Is the carvedilol benefit a class effect?
0.50.50.250.25 0.750.75 1.51.5 2.02.01.01.0
Effect in class IV patientsEffect in class IV patients
Packer, AHA 2000Packer, AHA 2000
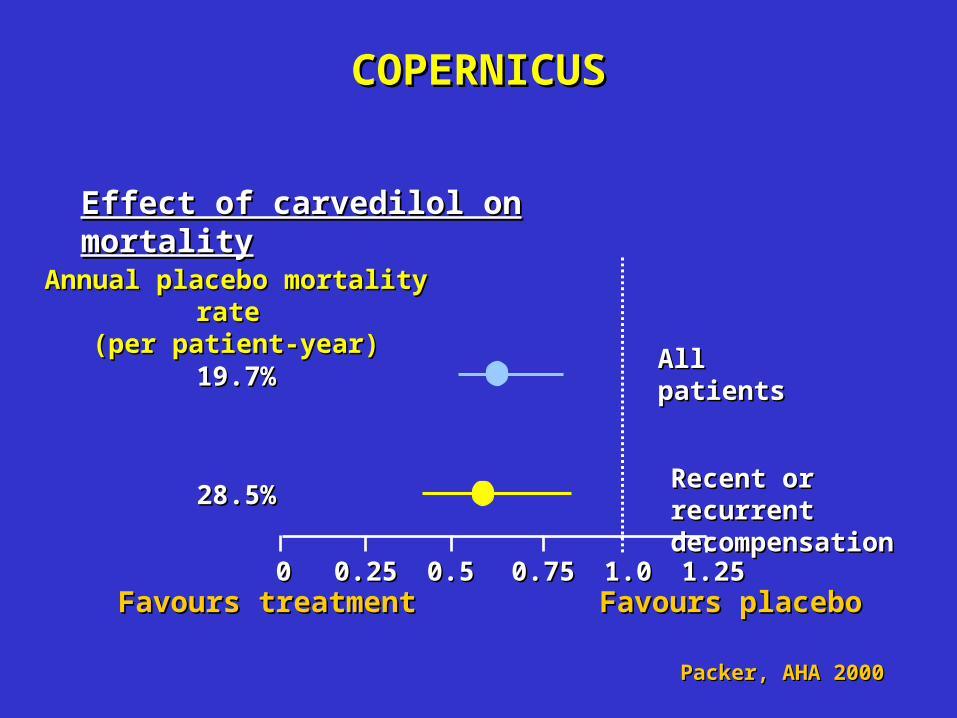
COPERNICUSCOPERNICUS
AllAllpatientspatients
Recent or recurrentRecent or recurrentdecompensationdecompensation
Annual placebo mortality rate Annual placebo mortality rate (per patient-year)(per patient-year)
19.7%19.7%
28.5%28.5%
0.50.50.250.25 0.750.75 1.251.251.01.000
Effect of carvedilol on mortalityEffect of carvedilol on mortality
Favours treatmentFavours treatment Favours placeboFavours placebo
Packer, AHA 2000Packer, AHA 2000

All patientsAll patients
Recent or Recent or recurrentrecurrentdecompensationdecompensation
Death or anyDeath or anyhospitalisationshospitalisations
Death or Death or cardiovascularcardiovascularhospitalisationshospitalisations
Death or CHFDeath or CHFhospitalisationshospitalisations
COPERNICUSCOPERNICUS
Effect of carvedilol on morbidity and mortalityEffect of carvedilol on morbidity and mortality
0.50.50.250.25 0.750.75 1.251.251.01.000Favours treatmentFavours treatment Favours placeboFavours placebo
Packer, AHA 2000Packer, AHA 2000
COPERNICUSCOPERNICUS
Effects on mortality in patient subgroupsEffects on mortality in patient subgroups
Consistent reductions in mortality across all patient Consistent reductions in mortality across all patient subgroups examined to date, e.g. in:subgroups examined to date, e.g. in:– patients <65 years and patients <65 years and 65 years65 years– men and womenmen and women– patients with ischaemic and non-ischaemic patients with ischaemic and non-ischaemic
cardiomyopathycardiomyopathy– patients with LVEF <0.20 and patients with LVEF <0.20 and 0.200.20
The benefits of carvedilol on mortality were apparent The benefits of carvedilol on mortality were apparent even in the highest-risk subgroups of the COPERNICUS even in the highest-risk subgroups of the COPERNICUS studystudy

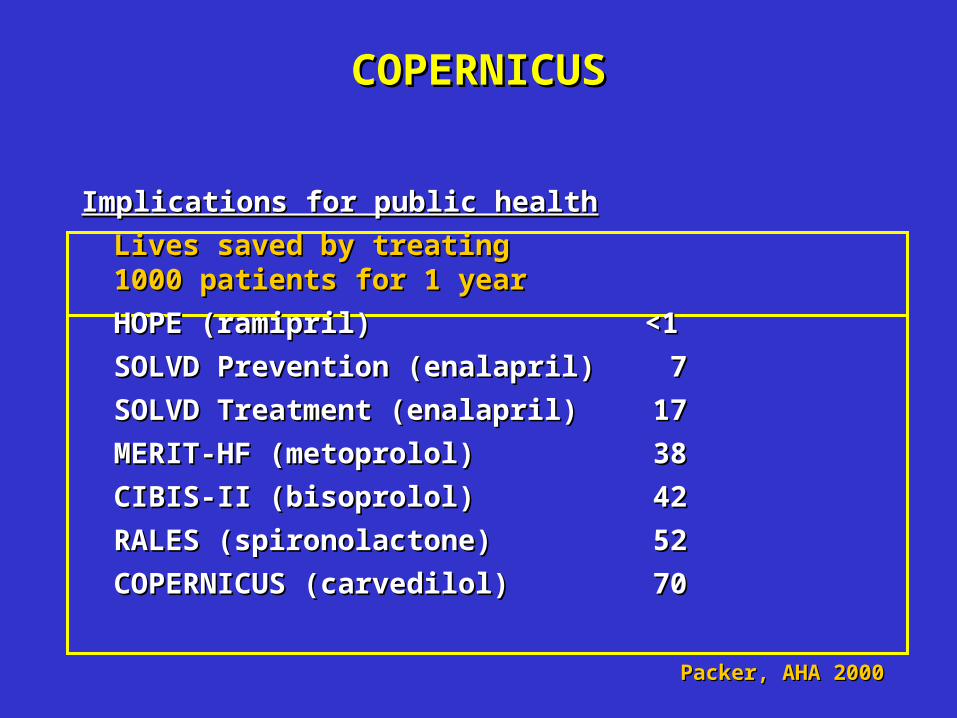
COPERNICUSCOPERNICUS
Implications for public healthImplications for public health
Lives saved by treatingLives saved by treating1000 patients for 1 year1000 patients for 1 year
HOPE (ramipril)HOPE (ramipril) <1<1
SOLVD Prevention (enalapril)SOLVD Prevention (enalapril) 7 7
SOLVD Treatment (enalapril)SOLVD Treatment (enalapril) 17 17
MERIT-HF (metoprolol)MERIT-HF (metoprolol) 38 38
CIBIS-II (bisoprolol)CIBIS-II (bisoprolol) 42 42
RALES (spironolactone)RALES (spironolactone) 52 52
COPERNICUS (carvedilol)COPERNICUS (carvedilol) 70 70
Packer, AHA 2000Packer, AHA 2000

COPERNICUSCOPERNICUS
SafetySafety
DizzinessDizziness
Bradycardia and heart blockBradycardia and heart block
FatigueFatigue
Worsening heart failureWorsening heart failure
Packer, AHA 2000Packer, AHA 2000

CirculationCirculation 2000; 101:378-84 2000; 101:378-84
RESOLVDRESOLVD
426 patients with class II-III heart failure were 426 patients with class II-III heart failure were randomized to placebo or metoprolol CR/XL for 24 randomized to placebo or metoprolol CR/XL for 24 weeks, added to ACE inhibitor or AT antagonistweeks, added to ACE inhibitor or AT antagonist
PlaceboPlacebo MetoprololMetoprolol
Worsening CHF leading to:Worsening CHF leading to:
Decrease in doseDecrease in dose 44 1111
DiscontinuationDiscontinuation 33 66
HospitalisationHospitalisation 55 1515

pp=NS=NS
% P
atie
nts
per
man
entl
y%
Pat
ien
ts p
erm
anen
tly
wit
hd
raw
n w
ith
dra
wn
00 33 66 99 1212 1515 1818 2121
MetoprololMetoprolol
PlaceboPlacebo
MonthsMonths
4040
3030
1010
2020
00
MERIT-HFMERIT-HF
Permanent withdrawalsPermanent withdrawals
Packer, AHA 2000Packer, AHA 2000

pp=0.02=0.02
COPERNICUSCOPERNICUS
4040
3030
1010
2020
0000 33 66 99 1212 1515 1818 2121
CarvedilolCarvedilol
PlaceboPlacebo
MonthsMonths
% P
atie
nts
per
man
entl
y%
Pat
ien
ts p
erm
anen
tly
wit
hd
raw
n w
ith
dra
wn
Permanent withdrawalsPermanent withdrawals
Packer, AHA 2000Packer, AHA 2000

COPERNICUS – Summary COPERNICUS – Summary
COPERNICUS establishes the efficacy of carvedilol COPERNICUS establishes the efficacy of carvedilol in severe heart failure and extends the benefits of in severe heart failure and extends the benefits of this drug first observed in patients with mild and this drug first observed in patients with mild and moderate symptoms to those with advanced diseasemoderate symptoms to those with advanced disease
COPERNICUS does not settle the question as to COPERNICUS does not settle the question as to whether all other whether all other blockers are effective in patients blockers are effective in patients with severe heart failure.with severe heart failure.
The effects of other The effects of other blockers in this patient blockers in this patient population remain to be determinedpopulation remain to be determined

CAPRICORNCAPRICORN(carvedilol)(carvedilol)
Class IClass I Class IVClass IV
US Carvedilol (carvedilol)US Carvedilol (carvedilol)CIBIS II (bisoprolol)CIBIS II (bisoprolol)
MERIT-HF (metoprolol)MERIT-HF (metoprolol)
COPERNICUSCOPERNICUS(carvedilol)(carvedilol)
Class IIClass IIClass IIIClass III
Packer, AHA 2000Packer, AHA 2000
CAPRICORNCAPRICORN
Study characteristicsStudy characteristics 1958 patients with acute myocardial infarction within 1958 patients with acute myocardial infarction within
21 days21 days LV ejection fraction <40%, receiving an ACE inhibitorLV ejection fraction <40%, receiving an ACE inhibitor Randomized to placebo or carvedilol (target 25 mg Randomized to placebo or carvedilol (target 25 mg
BID)BID) Endpoints: combined risk of death or cardiovascular Endpoints: combined risk of death or cardiovascular
hospitalisations, all-cause mortalityhospitalisations, all-cause mortality Data analysis ongoingData analysis ongoing
Carvedilol Post Infarct Survival Controlin Left Ventricular Dysfunction
Packer, AHA 2000Packer, AHA 2000
Why do we need another Why do we need another blocker trial in blocker trial in post-infarction patients?post-infarction patients?
Earlier post-MI trials with Earlier post-MI trials with blockers were performed blockers were performed in a different era and enrolled patients who generally in a different era and enrolled patients who generally were not receiving other agents that reduce mortality:were not receiving other agents that reduce mortality:
– No use of thrombolytic drugs No use of thrombolytic drugs
– Little use of aspirin or heparinLittle use of aspirin or heparin
– No use of ACE inhibitorsNo use of ACE inhibitors
– Did not have LV systolic dysfunctionDid not have LV systolic dysfunction
Are Are blockers still effective in the modern era? blockers still effective in the modern era?
Packer, AHA 2000Packer, AHA 2000
CAPRICORNCAPRICORN(carvedilol)(carvedilol)
Class IClass I Class IVClass IV
US Carvedilol (carvedilol)US Carvedilol (carvedilol)CIBIS II (bisoprolol)CIBIS II (bisoprolol)
MERIT-HF (metoprolol)MERIT-HF (metoprolol)
COPERNICUSCOPERNICUS(carvedilol)(carvedilol)
Class IIClass IIClass IIIClass III
Packer, AHA 2000Packer, AHA 2000

Key messagesKey messages
Carvedilol is the only drug with Carvedilol is the only drug with -blocking activity that -blocking activity that provides comprehensive adrenergic blockadeprovides comprehensive adrenergic blockade
Carvedilol is more beneficial than conventional Carvedilol is more beneficial than conventional -blocking agents in mild-to-moderate heart failure-blocking agents in mild-to-moderate heart failure
Carvedilol is the only drug with Carvedilol is the only drug with -blocking activity -blocking activity proven to be effective at lower doses proven to be effective at lower doses
COPERNICUS enrolled the most severely affected heart COPERNICUS enrolled the most severely affected heart failure population of any trial of failure population of any trial of blockade blockade
Carvedilol significantly reduces mortality in severe heart Carvedilol significantly reduces mortality in severe heart failure patientsfailure patients

11 receptors receptors 22 receptors receptors
Myocyte hypertrophy & death,Myocyte hypertrophy & death,dilatation, ischaemia & arrhythmia'sdilatation, ischaemia & arrhythmia's
11 receptors receptors
CardiacCardiacsympathetic activitysympathetic activity
SympatheticSympatheticactivity to kidneysactivity to kidneys& blood vessels& blood vessels
VasoconstrictionVasoconstrictionSodium retentionSodium retention
CNS sympatheticCNS sympatheticoutflowoutflow
Adrenergic activationAdrenergic activation
Packer, AHA 2000Packer, AHA 2000
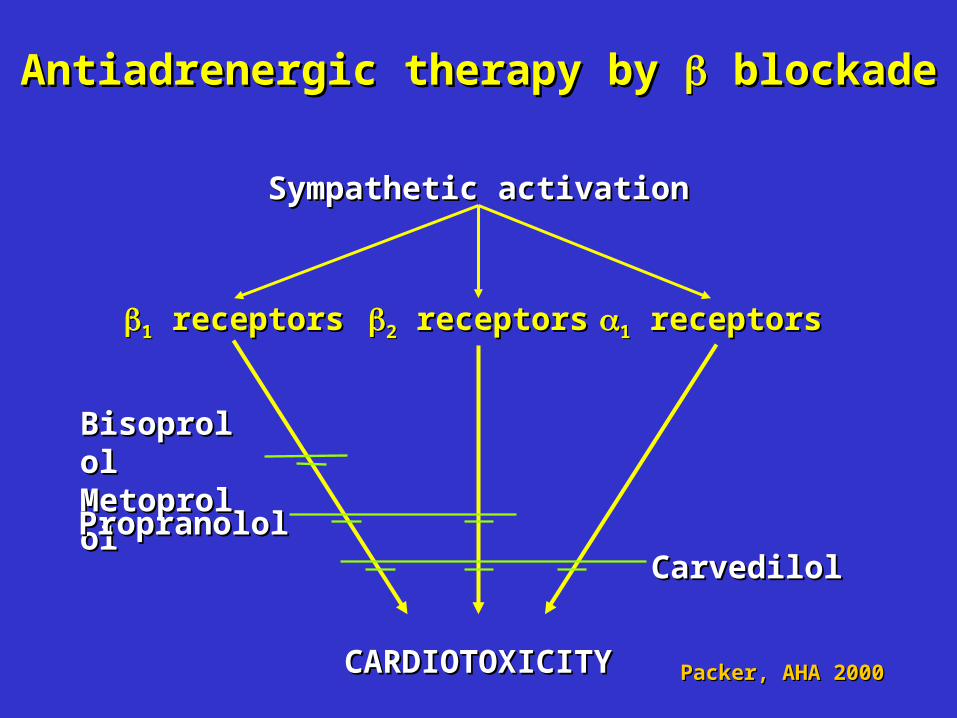
11 receptors receptors 11 receptors receptors
CARDIOTOXICITYCARDIOTOXICITY
22 receptors receptors
Sympathetic activationSympathetic activation
BisoprololBisoprololMetoproloMetoprolollPropranololPropranolol
CarvedilolCarvedilol
Antiadrenergic therapy by Antiadrenergic therapy by blockade blockade
Packer, AHA 2000Packer, AHA 2000
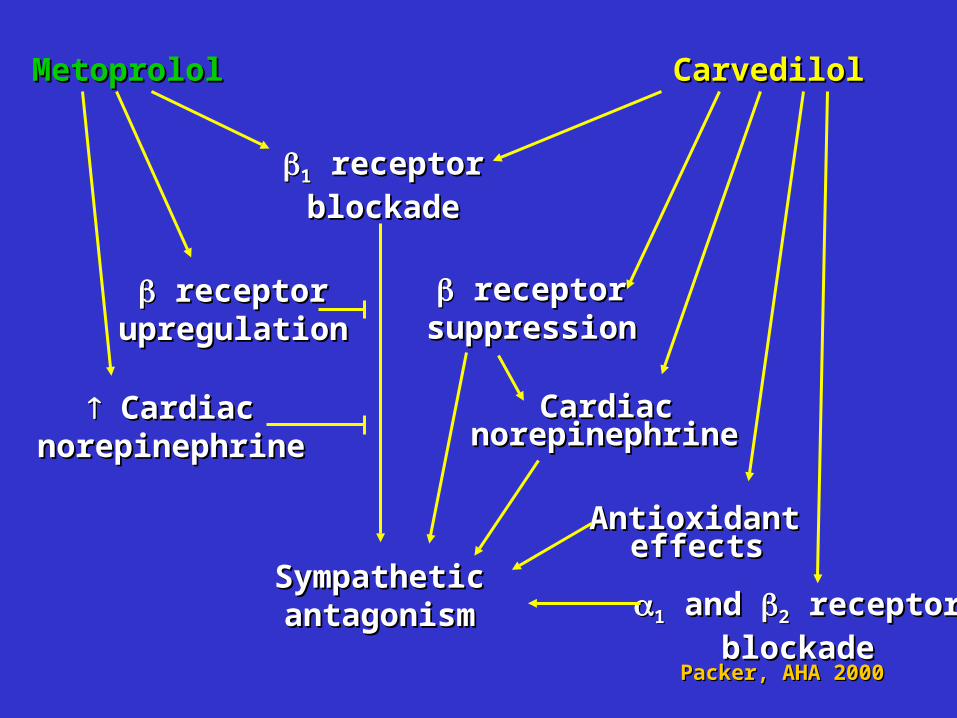
MetoprololMetoprolol
CardiacCardiacnorepinephrinenorepinephrine
AntioxidantAntioxidanteffectseffects
CarvedilolCarvedilol
CardiacCardiacnorepinephrinenorepinephrine
SympatheticSympatheticantagonismantagonism
11 receptor receptor
blockadeblockade
11 and and 22 receptor receptor
blockadeblockade
receptorreceptorupregulationupregulation
receptorreceptorsuppressionsuppression
Packer, AHA 2000Packer, AHA 2000

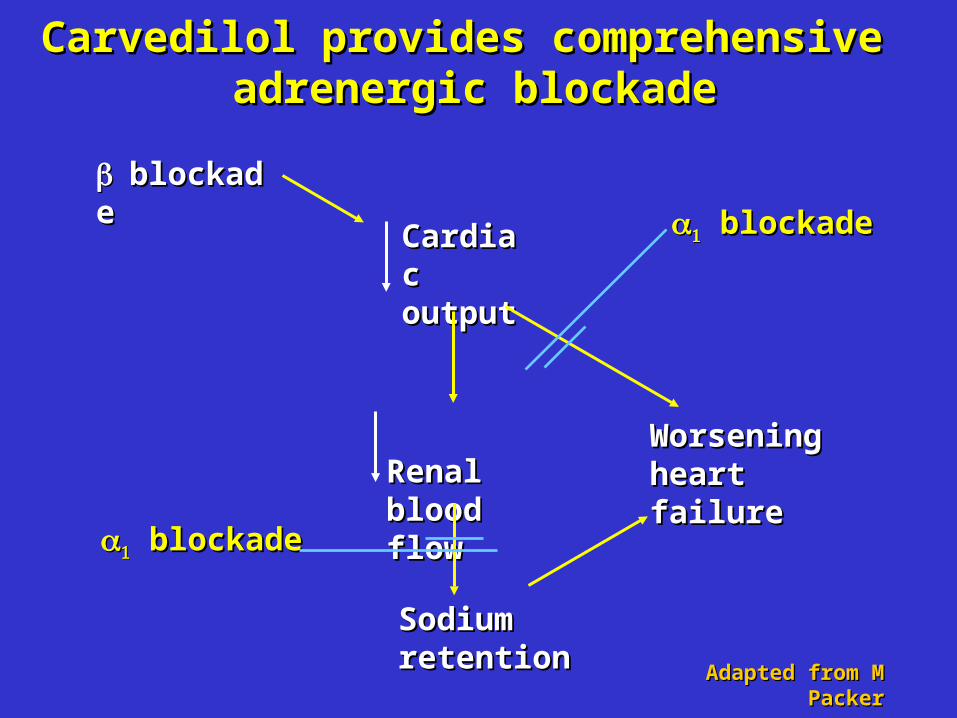
Carvedilol provides comprehensive Carvedilol provides comprehensive adrenergic blockadeadrenergic blockade
Adapted from M PackerAdapted from M Packer
blockadeblockade
Cardiac Cardiac outputoutput
Renal Renal blood flowblood flow
Worsening Worsening heart failureheart failure
Sodium Sodium retentionretention
Carvedilol provides comprehensive Carvedilol provides comprehensive adrenergic blockadeadrenergic blockade
Adapted from M PackerAdapted from M Packer
blockadeblockade
blockadeblockade
blockadeblockade
Cardiac Cardiac outputoutput
Renal Renal blood flowblood flow
Worsening Worsening heart failureheart failure
Sodium Sodium retentionretention
Key messagesKey messages
Carvedilol is the only drug with Carvedilol is the only drug with -blocking activity that -blocking activity that provides comprehensive adrenergic blockadeprovides comprehensive adrenergic blockade
Carvedilol is more beneficial than conventional Carvedilol is more beneficial than conventional -blocking agents in mild-to-moderate heart failure-blocking agents in mild-to-moderate heart failure
Carvedilol is the only drug with Carvedilol is the only drug with -blocking activity -blocking activity proven to be effective at lower dosesproven to be effective at lower doses
COPERNICUS enrolled the most severely affected heart COPERNICUS enrolled the most severely affected heart failure population of any trial of failure population of any trial of blockade blockade
Carvedilol significantly reduces mortality in severe heart Carvedilol significantly reduces mortality in severe heart failure patientsfailure patients

Randomized trials directly comparing Randomized trials directly comparing metoprolol with carvedilolmetoprolol with carvedilol
DiLenarda et alDiLenarda et al J Am Coll Cardiol, 1999J Am Coll Cardiol, 1999– Open-label for 12 months (n=30)Open-label for 12 months (n=30)
Kukin et al Kukin et al Circulation, 1999Circulation, 1999– Open-label for 6 months (n=67)Open-label for 6 months (n=67)
Sanderson et alSanderson et al J Am Coll Cardiol, 1999J Am Coll Cardiol, 1999– Double-blind for 3 months (n=51)Double-blind for 3 months (n=51)
Metra et alMetra et al Circulation, 2000Circulation, 2000– Double-blind for 12–15 months (n=150)Double-blind for 12–15 months (n=150)
Packer, AHA 2000Packer, AHA 2000
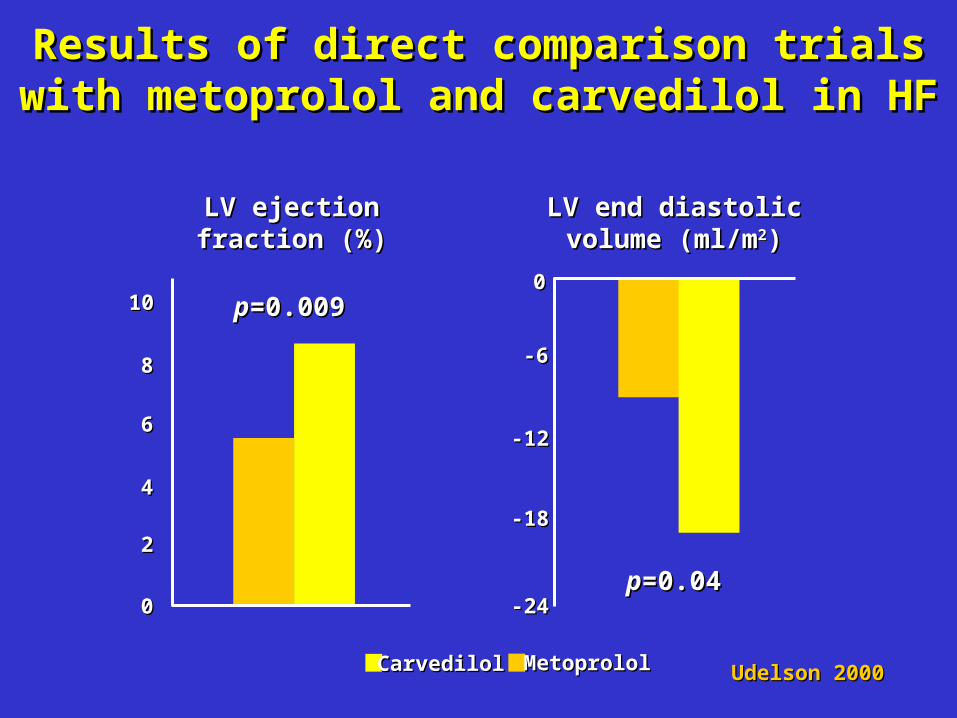
Udelson 2000Udelson 2000
LV ejectionLV ejectionfraction (%)fraction (%)
pp=0.009=0.009
00
22
44
66
88
1010
LV end diastolicLV end diastolicvolume (ml/mvolume (ml/m22))
pp=0.04=0.04-24-24
-18-18
-12-12
-6-6
00
CarvedilolCarvedilol MetoprololMetoprolol
Results of direct comparison trials with Results of direct comparison trials with metoprolol and carvedilol in HFmetoprolol and carvedilol in HF

Di Lenarda et al (1999)Di Lenarda et al (1999)
Change inChange inLV ejectionLV ejectionfraction (%)fraction (%)
Change inChange inend-diastolicend-diastolicvolume (ml)volume (ml)
Continued onContinued on
Switched toSwitched to
Metoprolol (n=16)Metoprolol (n=16)
Carvedilol (n=14)Carvedilol (n=14)
-20-20
-15-15
-10-10
-5-5
00
+5+5
+10+10
+15+15
**
**
pp=0.053=0.053
pp=0.045=0.045
Effect of switching patients from metoprolol Effect of switching patients from metoprolol to carvedilol for 12 monthsto carvedilol for 12 months

Metra et al (2000)Metra et al (2000)-20-20
-15-15
-10-10
-5-5
00
+6+6
+12+12
+18+18**
**
pp=0.002=0.002
pp<0.05<0.05
Double-blind comparison of effects of Double-blind comparison of effects of metoprolol and carvedilol for 13-15 monthsmetoprolol and carvedilol for 13-15 months
Change inChange inLV ejectionLV ejectionfraction (%)fraction (%)
Change inChange inpulmonary wedgepulmonary wedgepressure (mm Hg)pressure (mm Hg)
Metoprolol (n=75)Metoprolol (n=75)
Carvedilol (n=75)Carvedilol (n=75)

CAPRICORNCAPRICORN(carvedilol)(carvedilol)
Class IClass I Class IVClass IV
COMETCOMET(carvedilol vs metoprolol)(carvedilol vs metoprolol)
COPERNICUSCOPERNICUS(carvedilol)(carvedilol)
Class IIClass IIClass IIIClass III
Packer, AHA 2000Packer, AHA 2000

COMETCOMET
Objectives and designObjectives and design
To compare the effects of carvedilol with those of To compare the effects of carvedilol with those of metoprolol on the risk of death and hospitalisation metoprolol on the risk of death and hospitalisation in patients with chronic heart failurein patients with chronic heart failure
Randomised, double-blind, parallel-group, Randomised, double-blind, parallel-group, multicenter study of more than 3 years in durationmulticenter study of more than 3 years in duration
CCarvedilarvedilool l OOr r MMetoprolol etoprolol EEuropean uropean TTrialrial

COMETCOMET
>3000 patients with class II-IV heart failure due>3000 patients with class II-IV heart failure dueto ischaemic or non-ischaemic cardiomyopathyto ischaemic or non-ischaemic cardiomyopathy
Randomized to carvedilol or metoprolol (in addition to Randomized to carvedilol or metoprolol (in addition to usual therapy) for up to 3 yearsusual therapy) for up to 3 years
Pre-specified endpoints:Pre-specified endpoints:
– all-cause mortalityall-cause mortality
– death and hospitalisationdeath and hospitalisation
– all-cause mortality/all-cause hospitalisationall-cause mortality/all-cause hospitalisation
Packer, AHA 2000Packer, AHA 2000

Key messagesKey messages
Carvedilol is the only drug with Carvedilol is the only drug with -blocking activity that -blocking activity that provides comprehensive adrenergic blockadeprovides comprehensive adrenergic blockade
Carvedilol is more beneficial than conventional Carvedilol is more beneficial than conventional -blocking agents in mild-to-moderate heart failure-blocking agents in mild-to-moderate heart failure
Carvedilol is the only drug with Carvedilol is the only drug with -blocking activity -blocking activity proven to be effective at lower dosesproven to be effective at lower doses
COPERNICUS enrolled the most severely affected heart COPERNICUS enrolled the most severely affected heart failure population of any trial of failure population of any trial of blockade blockade
Carvedilol significantly reduces mortality in severe heart Carvedilol significantly reduces mortality in severe heart failure patientsfailure patients
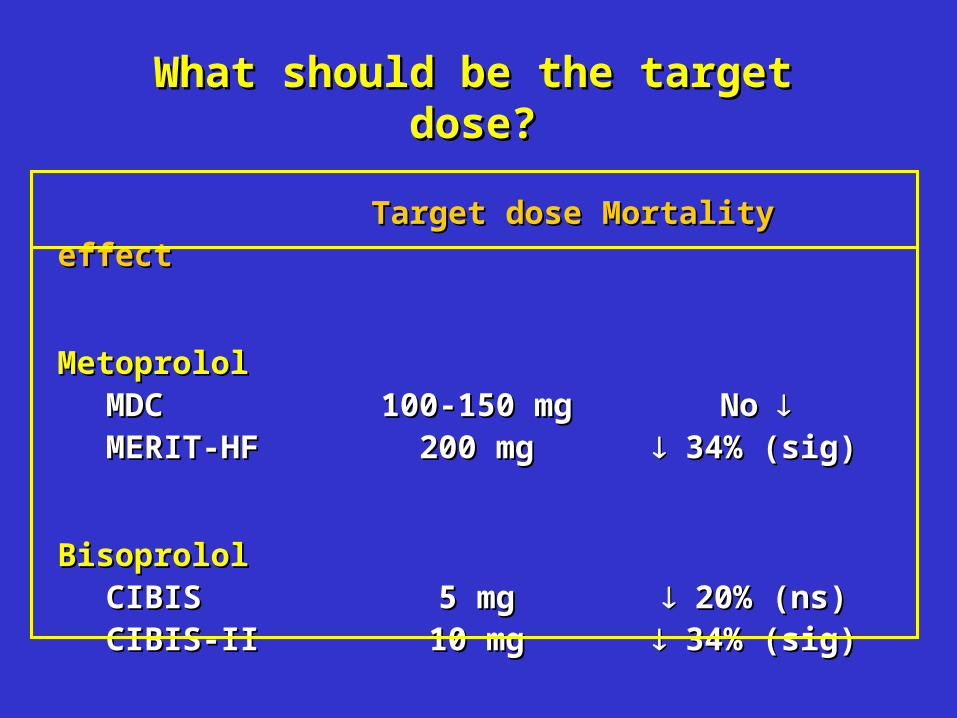
Target doseTarget dose Mortality effectMortality effect
MetoprololMetoprololMDCMDC 100-150 mg100-150 mg No No MERIT-HFMERIT-HF 200 mg200 mg 34% (sig) 34% (sig)
BisoprololBisoprololCIBISCIBIS 5 mg5 mg 20% (ns) 20% (ns)CIBIS-IICIBIS-II 10 mg10 mg 34% (sig) 34% (sig)
What should be the target dose?What should be the target dose?
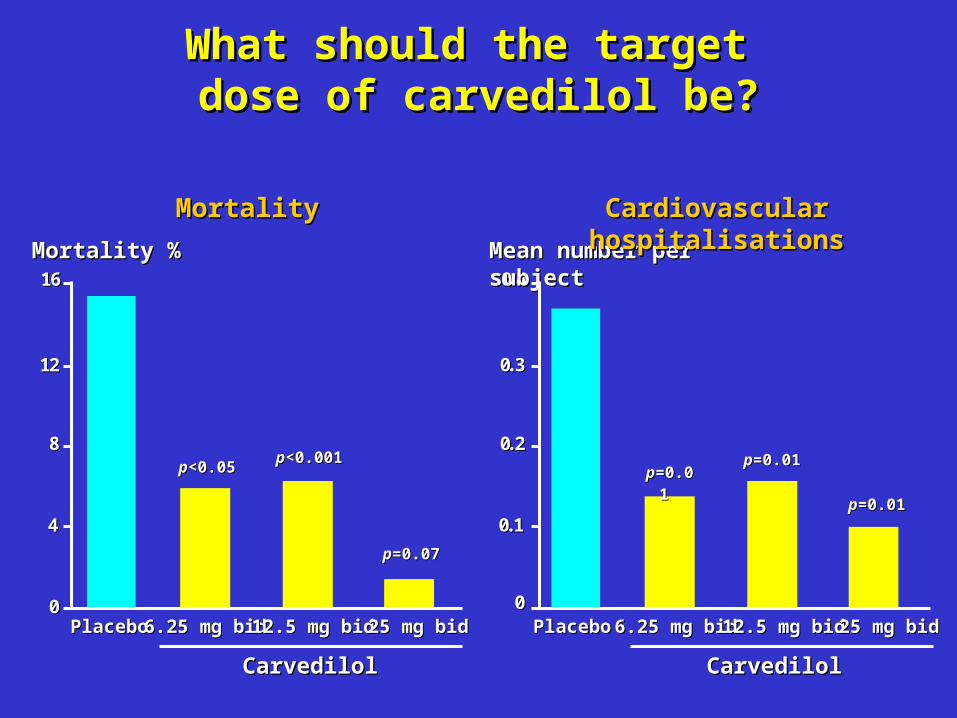
What should the target What should the target dose of carvedilol be?dose of carvedilol be?
..
00
00..11
00..22
00..33
00..44
CarvedilolCarvedilol
00
44
88
1122
1166
pp<0.05<0.05
pp=0.07=0.07
pp=0.01=0.01 pp=0.01=0.01
pp=0.01=0.01
Mortality %Mortality % Mean number per subjectMean number per subject
MortalityMortality Cardiovascular hospitalisationsCardiovascular hospitalisations
PlaceboPlacebo 6.25 mg bid6.25 mg bid 12.5 mg bid12.5 mg bid 25 mg bid25 mg bid PlaceboPlacebo 6.25 mg bid6.25 mg bid 12.5 mg bid12.5 mg bid 25 mg bid25 mg bid
CarvedilolCarvedilol
pp<0.001<0.001

Dosing for Dosing for blockers in heart failure blockers in heart failure
DrugDrug Starting doseStarting dose Target Target dosedose
BisoprololBisoprolol 1.25 mg qd1.25 mg qd 10 mg qd10 mg qd
CarvedilolCarvedilol 3.125 mg bid3.125 mg bid 6.256.25––25 mg 25 mg bidbid
MetoprololMetoprolol 12.512.5––25 mg qd25 mg qd 200 mg qd200 mg qd(extended-release)(extended-release)
The Medical Letter, June 26, 2000The Medical Letter, June 26, 2000

Key messagesKey messages
Carvedilol is the only drug with Carvedilol is the only drug with -blocking activity that -blocking activity that provides comprehensive adrenergic blockadeprovides comprehensive adrenergic blockade
Carvedilol is more beneficial than conventional Carvedilol is more beneficial than conventional -blocking agents in mild-to-moderate heart failure-blocking agents in mild-to-moderate heart failure
Carvedilol is the only drug with Carvedilol is the only drug with -blocking activity -blocking activity proven to be effective at lower dosesproven to be effective at lower doses
COPERNICUS enrolled the most severely affected heart COPERNICUS enrolled the most severely affected heart failure population of any trial of failure population of any trial of blockade blockade
Carvedilol significantly reduces mortality in severe heart Carvedilol significantly reduces mortality in severe heart failure patientsfailure patients

Mortality in Mortality in blocker heart failure trials blocker heart failure trials
Annual placeboAnnual placebomortality ratesmortality rates
MERIT-HFMERIT-HF 11.0%11.0%
US Carvedilol ProgrammeUS Carvedilol Programme 11.1%11.1%
CIBIS IICIBIS II 13.2%13.2%
BESTBEST 16.6%16.6%
COPERNICUSCOPERNICUS 19.7%19.7%
Class IV meta-analysisClass IV meta-analysis 20.7%20.7%
Packer, AHA 2000Packer, AHA 2000
Key messagesKey messages
Carvedilol is the only drug with Carvedilol is the only drug with -blocking activity that -blocking activity that provides comprehensive adrenergic blockadeprovides comprehensive adrenergic blockade
Carvedilol is more beneficial than conventional Carvedilol is more beneficial than conventional -blocking agents in mild-to-moderate heart failure-blocking agents in mild-to-moderate heart failure
Carvedilol is the only drug with Carvedilol is the only drug with -blocking activity -blocking activity proven to be effective at lower dosesproven to be effective at lower doses
COPERNICUS enrolled the most severely affected heart COPERNICUS enrolled the most severely affected heart failure population of any trial of failure population of any trial of blockade blockade
Carvedilol significantly reduces mortality in severe heart Carvedilol significantly reduces mortality in severe heart failure patientsfailure patients
0000
% S
urv
ival
% S
urv
ival
33 66 99 1212 1515 1818 2121MonthsMonths
100100
9090
8080
6060
7070
pp=0.00013=0.0001335% risk reduction35% risk reduction
CarvedilolCarvedilol
PlaceboPlacebo
COPERNICUSCOPERNICUS
All-cause mortalityAll-cause mortality
Packer, AHA 2000Packer, AHA 2000
COPERNICUSCOPERNICUS
Implications for public healthImplications for public health
Lives saved by treatingLives saved by treating1000 patients for 1 year1000 patients for 1 year
HOPE (ramipril)HOPE (ramipril) <1<1
SOLVD Prevention (enalapril)SOLVD Prevention (enalapril) 7 7
SOLVD Treatment (enalapril)SOLVD Treatment (enalapril) 17 17
MERIT-HF (metoprolol)MERIT-HF (metoprolol) 38 38
CIBIS-II (bisoprolol)CIBIS-II (bisoprolol) 42 42
RALES (spironolactone)RALES (spironolactone) 52 52
COPERNICUS (carvedilol)COPERNICUS (carvedilol) 70 70
Packer, AHA 2000Packer, AHA 2000

Implications for public healthImplications for public health
If 1000 patients are treated per year If 1000 patients are treated per year
approximately 70 lives would be savedapproximately 70 lives would be saved
Packer, AHA 2000Packer, AHA 2000

Key messagesKey messages
Carvedilol is the only drug with Carvedilol is the only drug with -blocking activity that -blocking activity that provides comprehensive adrenergic blockadeprovides comprehensive adrenergic blockade
Carvedilol is more beneficial than conventional Carvedilol is more beneficial than conventional -blocking agents in mild-to-moderate heart failure-blocking agents in mild-to-moderate heart failure
Carvedilol is the only drug with Carvedilol is the only drug with -blocking activity -blocking activity proven to be effective at lower dosesproven to be effective at lower doses
COPERNICUS enrolled the most severely affected heart COPERNICUS enrolled the most severely affected heart failure population of any trial of failure population of any trial of blockade blockade
Carvedilol significantly reduces mortality in severe heart Carvedilol significantly reduces mortality in severe heart failure patientsfailure patients
Recommended