COPD: MANAGEMENT OF STABLE DISEASEAND EXACERBATIONS
Dennis E. Doherty, M.D.
Professor of Medicine
Chief, Division of Pulmonary and Critical Care Medicine
Co-chairman, National Lung Health Education Program
University of Kentucky Medical Center
Lexington Veterans Administration Medical Center
OBJECTIVES
• Historical Perspective
• Mechanisms of Airflow Obstruction
• Treatment Modalities
MECHANISMS OF AIRFLOW OBSTRUCTION IN COPD

PERIPHERAL ADRENERGIC ACTIONS
BronchoconstrictionUrinary Retention
TachycardiaArrhythmias
BronchodilationUterine Relaxation
Tremor
DilatationHypertension
SmoothMuscle
Heart
SkeletalMuscle
Vascular
Alpha Beta1 Beta2

MECHANISMS OF BRONCHODILATIONBETA2-ADRENERGIC AGENTS
BRONCHODILATION
Adenylyl
Cyclase
cAMP cAMP
ATP
BRONCHODILATION
Beta2 -selectiveAdrenergic Agents
Drawing by Dennis E. Doherty, MD

MECHANISMS OF AIRWAY OBSTRUCTION
VagusNerve
Airway SmoothMuscle Cell
MediatorMast Cell
Antigen
Antibody
Classical Theory Reflex Theory
PATHWAYS OF ATOPIC ASTHMA
Drawing by Dennis E. Doherty, MD

Muscarinic Receptor Subtypes in Airways
M 3 RECEPTORS
M 2 RECEPTORSInhibit Ach Release
Acetylcholine
Acetylcholine
AIRWAY SMOOTH MUSCLE CELLS MUCUS GLANDS
CNS
Parasympathetic Nerves
Drawing by Dennis E. Doherty, MD
Vagal Parasympathetic (X)
.
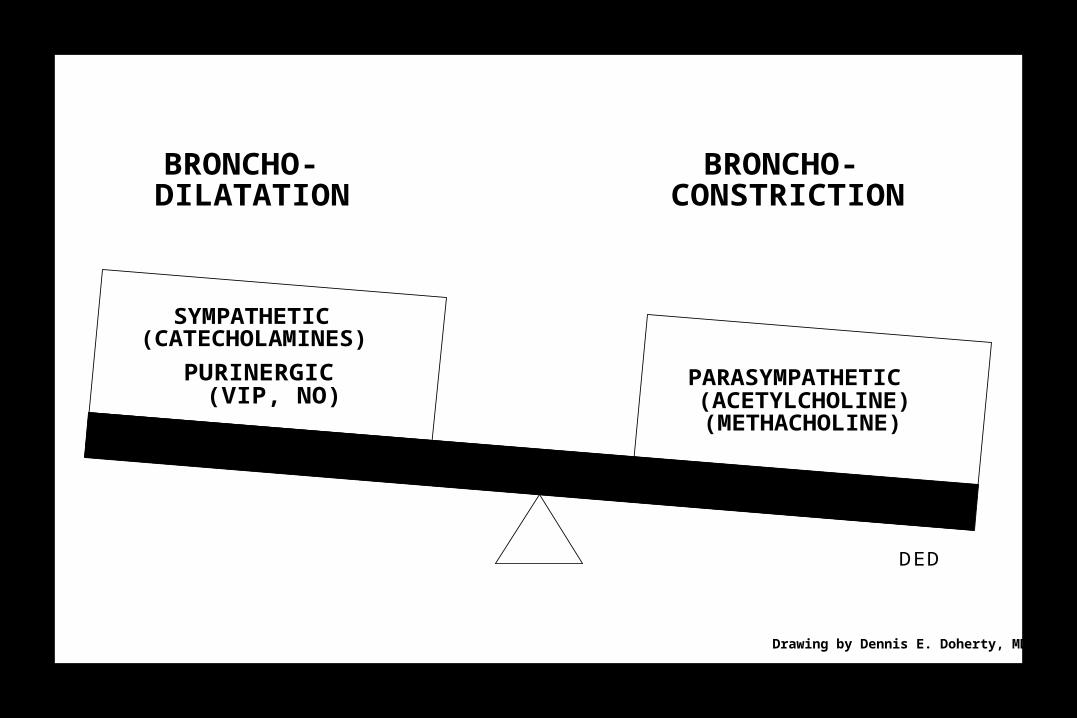
BRONCHO- DILATATION
BRONCHO- CONSTRICTION
SYMPATHETIC (CATECHOLAMINES)
PURINERGIC(VIP, NO)
PARASYMPATHETIC (ACETYLCHOLINE) (METHACHOLINE)
DED
Drawing by Dennis E. Doherty, MD

MECHANISMS OF BRONCHODILATIONANTICHOLINERGIC AGENTS
Increased Cyclic GMP
Calcium
Calcium
CHOLINERGICRECEPTOR
Acetyl-Choline (ACh)X
CHOLINERGIC M
Drawing by Dennis E. Doherty, MD
Decreased Smooth Muscle Constriction andMucus Gland Secretion
Ipratropium BromideAtropine
M3

Parasympathetic Sympathetic
DISTRIBUTION OF CHOLINERGIC AND ADRENERGIC RECEPTORS

CHRONICBRONCHITIS EMPHYSEMA
ASTHMA
AIRFLOWOBSTRUCTION
Treatment of COPD
American Thoracic Society. Am J Respir Crit Care Med. 1995.

PREVENT EMPHYSEMA

CHRONIC MANAGEMENT OF COPD(GOLD Guidelines Am J Respir Crit Care Med 2001;163:1256-1276)
DiagnoseDiagnose
Reduce Reduce RiskRisk
Smoking cessationImmunizeReduce other exposures
Reduce Reduce SymptomsSymptoms
Reduce Reduce ComplicationsComplications
BronchodilatorsConsider inhaled steroidsPulmonary rehabilitation
Consider oxygenTreat exacerbations
Spirometry
Education
Education
Education
Education

STEPWISE TREATMENT OF COPD BASED ON SEVERITY(GOLD Guidelines Am J Respir Crit Care Med 2001;163:1256-1276)
Stage 0:
At Risk
• Normal spirometry• Avoid Risks
• Vaccinate
Stage I:
Mild COPD
• FEV1/FVC < 70%
• FEV1 > 80% predicted
• Add a short-acting bronchodilator prn
– Anticholinergic or
– Beta2-agonist
Stage IIA:
Moderate COPD
• FEV1/FVC < 70%
• IIA: 50% < FEV1 < 80%
• Add one or more short-acting bronchodilators on a scheduled basis (Anticholinergic + Beta2-agonist)
Stage IIB:
Moderate COPD
• FEV1/FVC < 70%
• IIB: 30% < FEV1 < 50%
• Consider trial of inhaled steroids
• Add Pulmonary Rehabilitation
Stage III:
Severe COPD
•FEV1/FVC < 70%
•FEV1 < 30%
• Evaluate for adding oxygen
• Consider surgical options

NATIONAL LUNG HEALTHEDUCATION PROGRAM (NLHEP)
• TEST YOUR LUNGS
• KNOW YOUR NUMBERS
A new national healthcare initiative aimed at the diagnosis of early stages of COPD and related disorders.
www.nlhep.org

OFFICE SPIROMETERS

CHRONICBRONCHITIS EMPHYSEMA
ASTHMA
AIRFLOWOBSTRUCTION
Treatment of COPD
American Thoracic Society. Am J Respir Crit Care Med. 1995.

OBJECTIVES FOR INTERVENTIONSIN THE CHRONIC MANAGEMENT OF COPD
• Improvement in Lung Function
• Improve Quality of Life (Healthcare Status)
• Relieve Symptoms
• Decrease Exacerbations
• Decrease Hospitalizations
• Decelerate Decline in Lung Function
• Increase Life Expectancy
• Achieve Objectives in a Cost-Effective Manner

First Line Therapy in COPD is
Preventative
AVOID TOBACCO

GOLD Guidelines
Bronchodilation is first-line pharmacologic therapy in COPD
(GOLD Guidelines Am J Respir Crit Care Med 2001;163:1256-1276)
PHARMACOLOGIC ARMAMENTARIUM
• Anticholinergics (Parasympatholytic)• Short-acting inhaled (Ipratropium)
• Long-acting (Tiotropium)
• Beta Agonists (Sympathomimetic)• Short-acting inhaled (numerous available)
• Long-acting inhaled (Salmeterol, Formoterol)
• Methylxanthines (Sympathomimetic)
• Anti-Inflammatory• Oral Steroids
• Inhaled Steroids
• Other anti-inflammatory agents (data pending)

ANTICHOLINERGICS AND SHORT-ACTING BETA-AGONISTS ENHANCE FEV1 IN COPD
.
0
5
10
15
20
25
30
0 1 2 3 4 5 6 7 8
Hours After Test Dose
Test Day 85
Ipratroprium (N=176)
Albuterol (N=165)
Chest 105:1411, 1994
% C
han
ge
in m
ean
FE
V1
LONG-ACTING INHALED BETA AGONISTS
• Duration: Bronchodilation lasts for up to 12 hours
• Peak action: Fomoterol (30 min), onset within 5 min
Salmeterol (1-2hr), not indicated for exacerbations
• Most helpful:– Non-compliant patients (less frequent dosing)– Nocturnal component of COPD
• ? Of cost-benefit compared to short-acting beta-agonists

SALMETEROL IN COPD(Mahler et al, Chest 115:957, 1999)
Ch
ang
e fr
om
Bas
elin
eF
EV
1
PlaceboSalmeterolIpratopium
SALMETEROL IN COPD(Mahler et al, Chest 115:957, 1999)
• For patients ‘non-responsive’ to albuterol, (n=145, 35% ), ipratropium lead to greater bronchodilation compared to other treatments
• The mean transitional dyspnea index was significantly improved vs placebo and not significantly different for salmeterol vs ipratropium
• Ipratropium lead to a significantly improved 6 min walk vs placebo whereas salmeterol did not
• Night time dyspnea was improved with salmeterol treatment
• Overall, ipratropium lead to a greater reduction in dyspnea related to activities of daily living vs placebo or salmeterol
• The incidence of total lower respiratory tract adverse events (exacerbations) was different for salmeterol vs ipratropium, but both lead to fewer exacerbations vs placebo



0.95
1.00
1.05
1.10
1.15
1.20
1.25
1.30
1.35
-1 0 1 2 3 4 5 6 7 8 9 10 11 12
Time after administration (h)
Tiotropium (n = 202)
Placebo (n = 179)
Long-Acting Anticholinergic - TiotropiumChange in FEV1: Six Month Study
P < 0.001 for tiotropium vs placebo
FE
V1 (
L)
(DonohueJF, Chest 2002;122:47-55 )
Day 169
0.95
1.00
1.05
1.10
1.15
1.20
1.25
1.30
1.35
-1 0 1 2 3 4 5 6 7 8 9 10 11 12
Time after administration (h)
Tiotropium (n = 202)
Salmeterol (n = 203)
Placebo (n = 179)Day 169
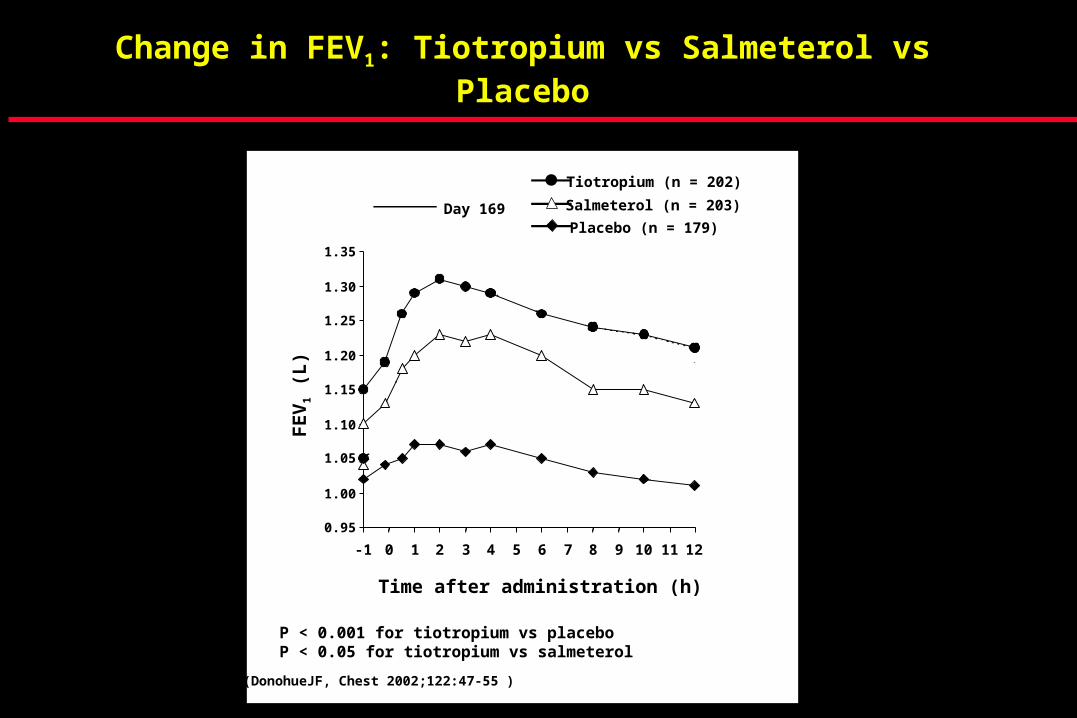
Change in FEV1: Tiotropium vs Salmeterol vs Placebo
P < 0.001 for tiotropium vs placeboP < 0.05 for tiotropium vs salmeterol
FE
V1 (
L)
(DonohueJF, Chest 2002;122:47-55 )
0.95
1.00
1.05
1.10
1.15
1.20
1.25
1.30
1.35
-1 0 1 2 3 4 5 6 7 8 9 10 11 12
Time after administration (h)
Tiotropium (n = 202)
Salmeterol (n = 203)
Placebo (n = 179)Day 169
Day 1
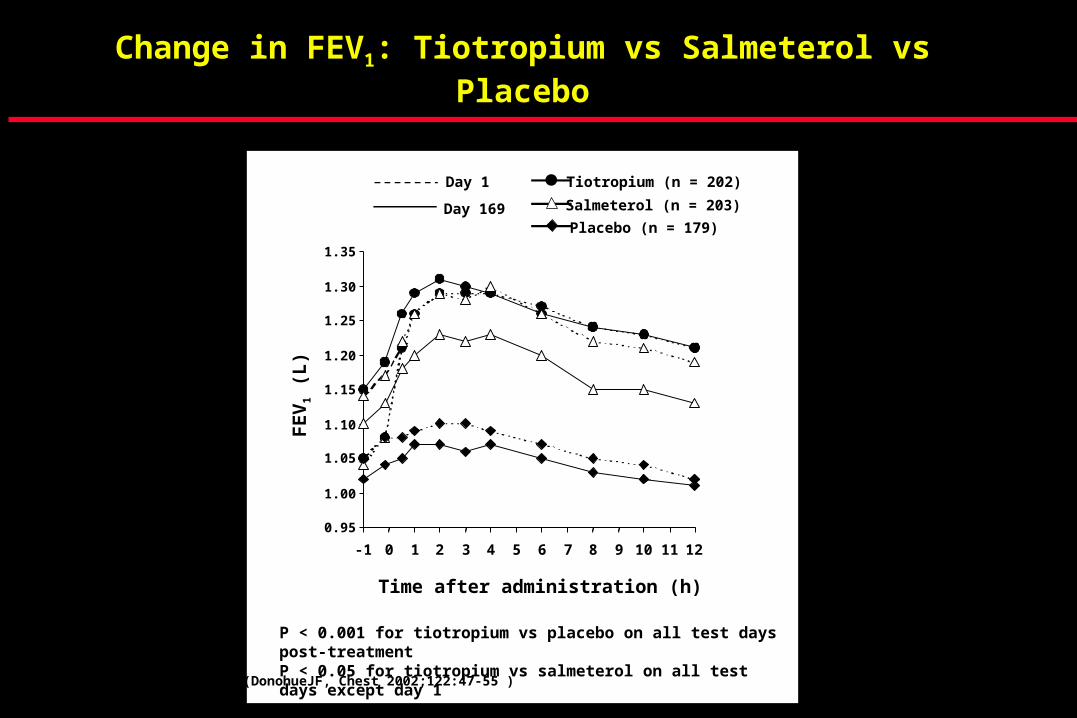
Change in FEV1: Tiotropium vs Salmeterol vs Placebo
P < 0.001 for tiotropium vs placebo on all test days post-treatmentP < 0.05 for tiotropium vs salmeterol on all test days except day 1
FE
V1 (
L)
(DonohueJF, Chest 2002;122:47-55 )

Binding and Dissociation
Disse B et al. Life Sci 1993
Apparent KD (nM)
Ipratropium 0.43 0.54 0.69
Tiotropium 0.27 0.12 0.33
Dissociation Half-Life (hours)
[3H]-Ipratropium 0.11 0.035 0.26
[3H]-Tiotropium 14.6 3.6 34.7
Human Muscarinic Receptors in CHO Cells
M1 M2 M3
KD = dissociation constant

CHRONICBRONCHITIS EMPHYSEMA
ASTHMA
AIRFLOWOBSTRUCTION
Combination Therapy in COPD
American Thoracic Society. Am J Respir Crit Care Med. 1995.
Bronchodilating Effects of CombinedTherapy With Clinical Dosages ofIpratropium Bromide and Salbutamol forStable COPD:Comparison With Ipratropium Bromide Alone
Akihiko Ikeda, MD, Koicht Nishimura
Bronchodilating Effects of CombinedTherapy With Clinical Dosages ofIpratropium Bromide and Salbutamol forStable COPD:Comparison With Ipratropium Bromide Alone
Akihiko Ikeda, MD, Koicht Nishimura
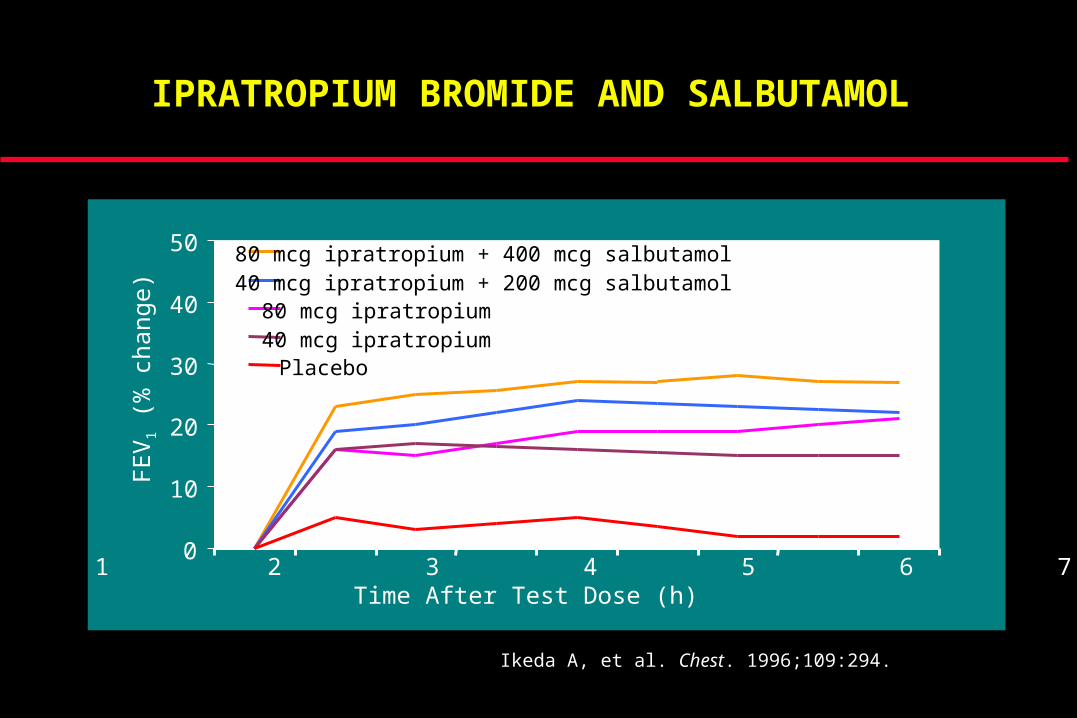
Ikeda A, et al. Chest. 1996;109:294.
0
10
20
30
40
50 80 mcg ipratropium + 400 mcg salbutamol40 mcg ipratropium + 200 mcg salbutamol80 mcg ipratropium40 mcg ipratropiumPlacebo
FE
V1
(% c
hang
e)
0 1 2 3 4 5 6 7 8 Time After Test Dose (h)
IPRATROPIUM BROMIDE AND SALBUTAMOL

.
0
5
10
15
20
25
30
35
40
0 1 2 3 4 5 6 7 8
Hours After Test Dose
Test Day 85
Ipratroprium + Albuterol(N=173)
Ipratroprium (N=176)
Albuterol (N=165)
Chest 105:1411, 1994
% C
han
ge
in m
ean
FE
V1
Ipratropium and Albuterol per MDIis More Effective than Either Agent Alone

COMBINATION METERED DOSE INHALER(Ipratropium Bromide plus Albuterol Sulfate)
• Effective bronchodilation via two distinct mechanisms.
• Useful in the subset of patients who require both classes of agents to achieve maximal bronchodilation without potentiation of side effects over either single component alone.
• Useful in noncompliant (non-adherent) patients- can improve adherence and patient satisfaction- by decreasing their time, effort, and the number of puffs required to administer two efficacious drugs.
• Cost effective if restricted to these subsets of patients, and if the combination inhaler is properly priced.
COMBINATION THERAPY IN COPD
• Combination of ipratropium and long-acting beta-agonists have been shown to lead to significantly greater bronchodilation than that observed in response to either agent alone
– Ipratropium + Salmeterol (Van Noord, Eur Resp J 2000;15:878-885)
– Ipratropium + Formoterol (D’Urzo, Chest 2001;119:1347-1356)
• A new generation anticholinergic agent, tiotropium bromide, which is more selective, more potent, and has a longer duration of action compared to ipratropium bromide is currently in development (Litner, Am J Respir Crit Care Med 2000;161:1136-1142)

Combination Therapy with an Anticholinergicand a Long-Acting Beta-2 Agonist
-5
-2.5
0
2.5
5
7.5
10
12.5
0 0.5 1 2 3 4 5 6 7 8 9 10 11 12
Time (hours)
F
EV
1 (%
Pre
d.)
Salmeterol 50 µg + ipratropium 40 µg Salmeterol 50 µg Placebo
van Noord JA et al. Eur Respir J 2000;15:878-885
OBJECTIVES FOR INTERVENTIONSIN THE CHRONIC MANAGEMENT OF COPD
• Improvement in Lung Function
• Relieve Symptoms
• Decrease Exacerbations
• Decrease Hospitalizations
• Improve Quality of Life (Healthcare Status)
• Decelerate Decline in Lung Function
• Increase Life Expectancy
• Achieve Objectives in a Cost-Effective Manner

COPD EXACERBATION - DEFINITION
Acute Worsening of Respiratory Symptoms (72hr)
• Increased Dyspnea
• Increased Quantity of Sputum
• Increased Purulence of Sputum
Anthonisen NR 1987 Ann Int Med 106:196-204
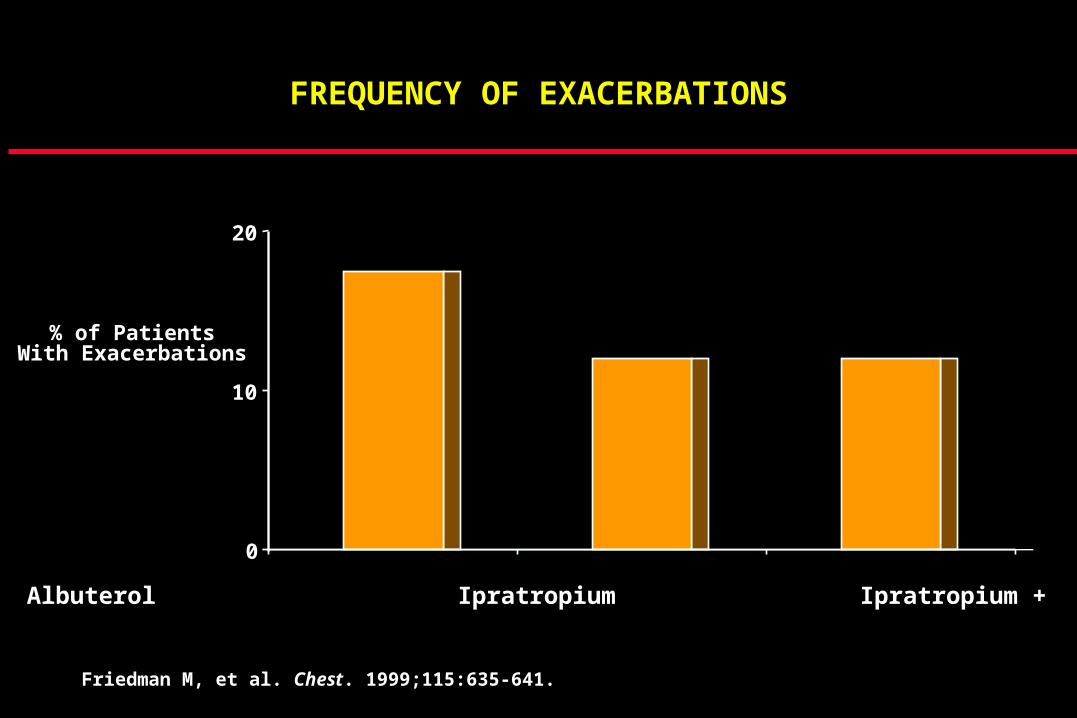
0
10
20
Albuterol Ipratropium Ipratropium + Albuterol
% of PatientsWith Exacerbations
Friedman M, et al. Chest. 1999;115:635-641.
FREQUENCY OF EXACERBATIONS
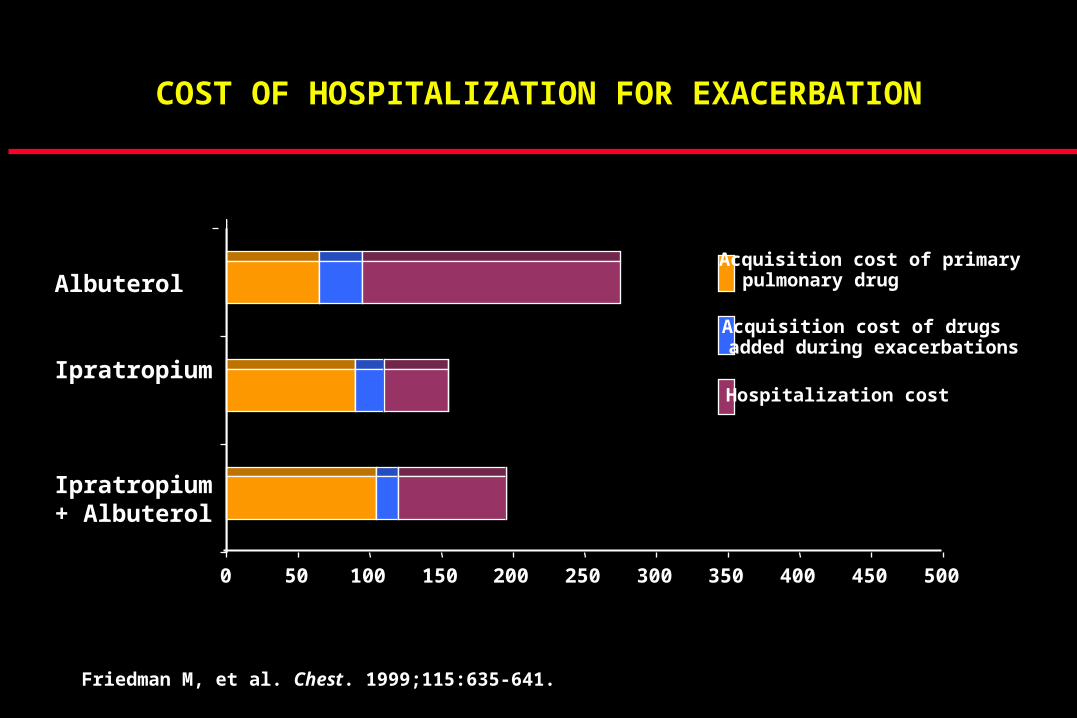
0 50 100 150 200 250 300 350 400 450 500
Acquisition cost of primarypulmonary drug
Acquisition cost of drugsadded during exacerbations
Hospitalization cost
Albuterol
Ipratropium
Ipratropium + Albuterol
Friedman M, et al. Chest. 1999;115:635-641.
COST OF HOSPITALIZATION FOR EXACERBATION

PHARMACOLOGIC ARMAMENTARIUM
• Anticholinergics (Parasympatholytic)• Short-acting inhaled (Ipratropium)
• Long-acting (Tiotropium)
• Beta Agonists (Sympathomimetic)• Short-acting inhaled (numerous available)
• Long-acting inhaled (Salmeterol, Fomoterol)
• Methylxanthines (Sympathomimetic)
• Anti-Inflammatory• Oral Steroids
• Inhaled Steroids
• Other anti-inflammatory agents (data pending)

Relationship Between Plasma Theophylline Concentrations and Clinical Effects
mg/liter
EfficacyToxicityConcentration
5
10
20
40
60
}Minimal
Optimal
Gastrointestinal Upset
Nervousness
Arrhythmias
Convulsions
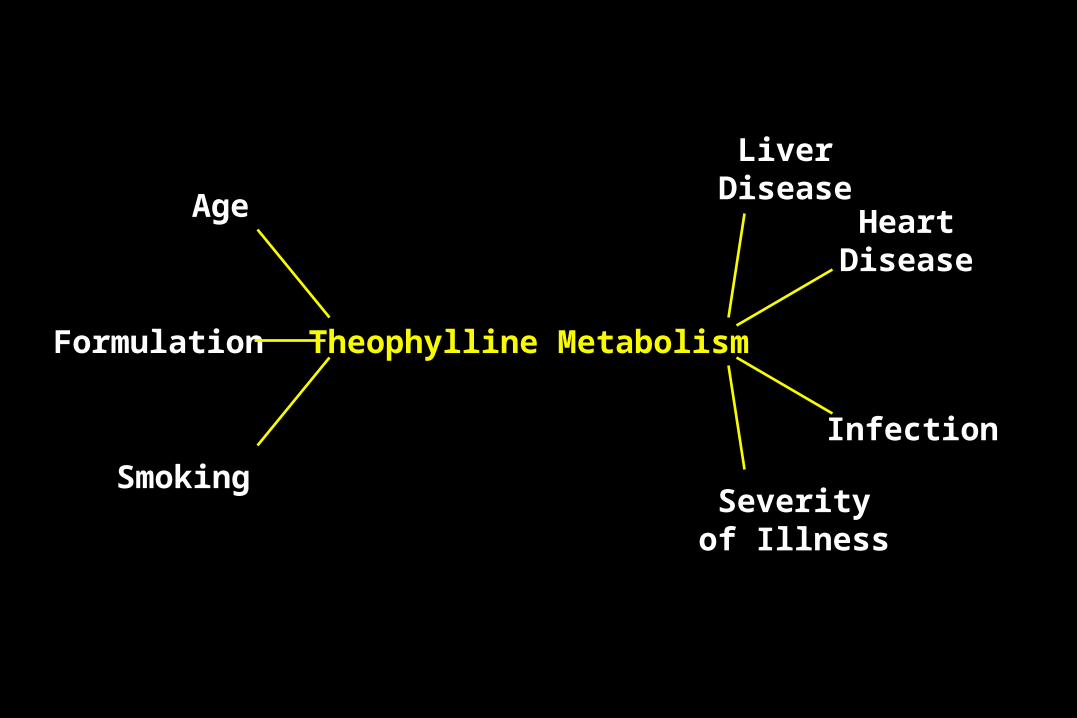
Theophylline Metabolism
Age
Smoking
Formulation
LiverDisease
HeartDisease
Infection
Severityof Illness

PHARMACOLOGIC ARMAMENTARIUM
• Anticholinergics (Parasympatholytic)• Short-acting inhaled (Ipratropium)
• Long-acting (Tiotropium)
• Beta Agonists (Sympathomimetic)• Short-acting inhaled (numerous available)
• Long-acting inhaled (Salmeterol, Fomoterol)
• Methylxanthines (Sympathomimetic)
• Anti-Inflammatory• Oral Steroids
• Inhaled Steroids
• Other anti-inflammatory agents (data pending)

• The inflammation of asthma is responsive to steroids
– Mast cells, eosinophils, TH2-like lymphocytes (CD4)
– IL-4, IL-5, IL-13, ECP, LTC4
• The chronic inflammation in COPD is not responsive to steroids
– Macrophages, Neutrophils, T-Lymphocytes (CD8)
– LTB4, TNF, IL-8, Chemokines
LUNG INFLAMMATION IN ASTHMA IS DIFFERENT THAN THE LUNG INFLAMMATION IN COPD

GOLD Guidelines
• Trial of inhaled corticosteroids (6 wks – 3 mo) given only if patient with moderate to severe COPD (defined by spirometry) continues with significant symptoms and frequent exacerbations (3 - 4 per yr) despite maximal bronchodilation.
• If symptoms or the frequency of exacerbations are not improved, steroids should be discontinued.
(GOLD Guidelines Am J Respir Crit Care Med 2001;163:1256-1276)

INHALED CORTICOSTEROIDS IN COPD
• Copenhagen City Heart Study (Lancet 1999;353:1819-23)
• Mild-Moderate COPD (n=290)
• Budesonide 1200-800 micrograms/day
• No difference vs placebo in rate of decline in FEV1 over 3 years
• EUROSCOP Trial (N Engl J Med 1999;340:1948-53)
• Mild COPD (n=1277)
• Budesonide 800 micrograms/day
• No difference vs placebo in rate of decline in FEV1 over 3 years
• Increase of 30-40ml FEV1 in treatment group early on which was sustained throughout the study

INHALED CORTICOSTEROIDS IN COPD
• Lung Health Study (N Engl J Med 2000;343:1902-1909)
• Moderate COPD, FEV1 of 2L (n=1116)
• Triamcinolone 1200 micrograms/day
• No difference vs placebo in rate of decline in FEV1 over 3.5 years
• Modest improvement in dyspnea and onset of severe symptoms
• Increased risk of osteoporosis
• ISOLDE Trial (BMJ 2000;320:1297-303)
• Moderate to severe COPD , FEV1 of 1.5L (n=751)
• Fluticasone 1000 micrograms/day
• No difference vs placebo in rate of decline in FEV1 over 3 years
• Increase of 100ml FEV1 in treatment group early on which was sustained throughout the study
• Exacerbations decreased by 25% in treatment group

SYSTEMIC CORTICOSTEROIDS SHOULD BE USED DURING ACUTE EXACERBATIONS OF COPD
Two studies have shown efficacy for the use of systemic steroids during acute COPD exacerbations
• Niewoehner DE et al, NEJM 340:1941, 1999
• Davies L et al, Lancet 354:456, 1999
Once daily Solumedrol (60 mg iv) or
Once daily Prednisone (30 - 40mg po)
Taper off in 5-7 days

CORTICOSTEROIDS DURINGACUTE EXACERBATIONS OF COPD
Niewoehner et al NEJM 1999;340:1941

OBJECTIVES FOR INTERVENTIONSIN THE CHRONIC MANAGEMENT OF COPD
• Improvement in Lung Function
• Relieve Symptoms
• Decrease Exacerbations
• Decrease Hospitalizations
• Improve Quality of Life (Healthcare Status)
• Decelerate Decline in Lung Function
• Increase Life Expectancy
• Achieve Objectives in a Cost-Effective Manner

MONTHLY ACQUISITION COSTS FOR COPD DRUGS (AWP)(REDBOOK, 2002 Edition)
0 25 50 75 100 1250 25 50 75 100 125
Albuterol
AWP/month (Dollars)
No. MDIs/Month
Ipratropium
Albuterol +Ipratropium
Albuterol +Ipratropium(single MDI)
Formoterol
Salmeterol
Salmeterol +Albuterol
1.2
1.2
1.2 + 1.2
1.2
1.0
1.0
1.0 + 1.2

MONTHLY ACQUISITION COSTS FOR COPD DRUGS (AWP)(REDBOOK, 2002 Edition)
0 25 50 75 100 125 150 175 2000 25 50 75 100 125 150 175 200
AWP/month (Dollars)
No. MDIs/MonthAlbuterol
Ipratropium
Albuterol +Ipratropium(Single MDI)
Salmeterol + Albuterol
Formoterol + Albuterol
Beclomethasone
Fluticasone 110
Fluticasone 220
Flunisolide
Budesonide
Fluticasone 500+ Salmeterol 50
Combination
1.2
1.2
1.2
1.0 + 1.2
1.0 + 1.2
1.2
1.0
1.0
1.2
0.6
1.0
OBJECTIVES FOR INTERVENTIONSIN THE CHRONIC MANAGEMENT OF COPD
• Improvement in Lung Function
• Relieve Symptoms
• Decrease Exacerbations
• Decrease Hospitalizations
• Improve Quality of Life (Healthcare Status)
• Decelerate Decline in Lung Function
• Increase Life Expectancy
• Achieve Objectives in a Cost-Effective Manner

MODALITIES IMPROVING SURVIVAL IN COPD
• Successful Smoke Cessation (Behavioral Modification Required)
• Oxygen Therapy (Minimum of 15-18 hr qd)

NON-PHARMACOLOGIC ARMAMENTARIUM
• Successful Smoke Cessation
• Pulmonary Rehabilitation (formal/informal)
• Overall Education
• Exercise Program (home program)
• Nutrition
• Vaccination
• Pulmonary Hygiene (?mucolytic agents)
• Antibiotics
• Transplantation (Single Lung)
• Oxygen, Noninvasive Ventilation
• Experimental (LVRS, Anti-oxidants/Vitamins)
• Carol Boland (Nurse Practitioner)• Dick D. Briggs (Pulmonary)• Dennis E. Doherty (Pulmonary)• Harold Hedges III (Family Medicine)• Louis Kuritzky (Family Medicine)• Ron Levine (Internal Medicine)• Kenneth Pellegrino (Family Medicine)• Alan Radin (Internal Medicine)• Steven A. Sahn (Pulmonary)
THE NATIONAL COPD AWARENESS PANEL (NCAP)Journal of Respiratory Diseases 21:S1-21, Sept 2000
Journal of Respiratory Diseases 23:S1-52, Sept 2002

COPD Management in Primary CareNCAP- Journal of Respiratory Diseases 23:S1-52, Sept 2002
GOLD Guidelines Am J Respir Crit Care Med 2001;163:1256-1276
• Sustained Smoking Cessation
• First-line Therapy is to Maximize Bronchodilation• Anticholinergics (short- or long-acting)
• Beta-2 Agonists (short- or long-acting)
• Methylxanthines
• After Maximal Bronchodilation with multiple agents in patients with severe COPD and frequent exacerbations• A trial of Inhaled Corticosteroids can be considered
– 6 week to 3 month trial– Monitor Spirometry and Symptoms– Discontinue if no improvement in that time period

VACCINNATION IN COPD
• Pneumococcal
• In all COPD Patients
• Patients > 65 vaccinated more than 5 years previously should be revaccinated, if unsure - revaccinate
• Evidence for efficacy is inconclusive (some studies show a 65-85% efficacy amongst high-risk populations)
• Influenza
• Administer annually unless there is a history of severe anaphylaxis to egg protein
• 30-80% effective in preventing illness, complications, and death in high-risk populations
• Can be administered concurrently with pneumococcal vaccine if administered at different sites
For more information on COPD
National Lung Health Education Program
www.nlhep.org
U.S. COPD Coalition
www.uscopd.com
Recommended