Congenital Heart DiseaseCongenital Heart Disease
• Most common type of heart disease among children
a) ~ 1% of live birthsb) most causes unknown
i) ~ 10% genetic- e.g., trisomy 21 (Down
syndrome)- congenital defect in
parent or sibling is greatest risk factor
www.freelivedoctor.comwww.freelivedoctor.com

• Types:a) L to R shuntb) R to L shuntc) obstructions
1.- L to R shuntsL to R shuntsa) ASD, VSD, PDA
i) pulmonary blood flow (ASD)
- NO cyanosisb) RV pressures and Vol.
(VSD,PDA)i) hypertrophyii) PVR (vasoconstriction)
- to prevent edema
www.freelivedoctor.comwww.freelivedoctor.com

c) Over time PVR to that of SVRi) reverses shunt (cyanosis)
2.- R to L shuntR to L shunta) pulmonary blood flow
i) Cyanosis “blueness” of skinb) examples:
i) tetralogy of Fallot ii) great vessel transpositioniii) truncus arteriosusiv) tricuspid atresiav) anomalous pulmonary
venous connection
www.freelivedoctor.comwww.freelivedoctor.com

c) long standing cyanosis is associated with “clubbing”
of the tips of the fingers and toes
www.freelivedoctor.comwww.freelivedoctor.com

3.- Obstructions (of flow)Obstructions (of flow)a) coarctation of the aortab) valvular stenosis
i) aorticii) pulmonary
c) complete obstruction is called “Atresia”
www.freelivedoctor.comwww.freelivedoctor.com

Left to Right ShuntsLeft to Right Shunts
• Most common:a) VSD, ASD, PDA and AVSD
www.freelivedoctor.comwww.freelivedoctor.com

i) VSD most common- close spontaneously
(50%) ii) ASD usually not
symptomatic before 30 yrs
www.freelivedoctor.comwww.freelivedoctor.com

iii) DA remains open after birth- ~ 90% occur as isolated anomaly - reversal of flow with PVR causes cyanosis- PGE will maintain DA
cardiac defects such as obstructive disease
iv) complete atrioventricular canal defect
- all 4 chambers freely communicate (Down
syndrome)www.freelivedoctor.comwww.freelivedoctor.com

Right to Left ShuntsRight to Left Shunts
• Tetralogy of FallotTetralogy of Fallota) Most common form of cyanotic congenital heart disease
• Defects:a) VSDb) Pulmonary artery stenosis
i) determines clinical outcomec) aorta that overrides VSDd) RV hypertrophy
www.freelivedoctor.comwww.freelivedoctor.com

www.freelivedoctor.comwww.freelivedoctor.com

• Clinical Presentation:a) The onset and degree of
cyanosis depends on:i) severity of the pulmonary
obstruction ii) the size of the shunt.
b) Cyanosis is usually not seen until 3- 6 months of age.
c) The cyanosis is due to right ventricle outflow obstruction causing unoxygenated
blood through the VSD. www.freelivedoctor.comwww.freelivedoctor.com

• Transposition of the Great Transposition of the Great ArteriesArteries(TGA)(TGA)
a) aorta arises from RVi) is anterior and to the right
of the pulmonary arteryb) pulmonary artery arises from
LVc) total separation of pulmonary
and systemic circulationsi) need a shunt to survive following birth
- VSD stable shuntwww.freelivedoctor.comwww.freelivedoctor.com

- PDA, foramen ovale unstable shunt (close
quickly after birth) need surgery• the aorta originates from the right ventricle, so most of the blood returning to the heart from the body is pumped back out without first going to the lungs.
• the pulmonary artery originates from the left ventricle, so that most of the blood returning from the lungs goes back to the lungs again
www.freelivedoctor.comwww.freelivedoctor.com

www.freelivedoctor.comwww.freelivedoctor.com

www.freelivedoctor.comwww.freelivedoctor.com

Truncus ArteriosusTruncus Arteriosus
• Failure of separation into aorta and pulmonary artery
a) results in single great arteryi) receives blood from both ventricles
- early systemic cyanosisb) accompanying VSDc) pulmonary blood flow
i) danger of irreversible pulmonary hypertensionwww.freelivedoctor.comwww.freelivedoctor.com

www.freelivedoctor.comwww.freelivedoctor.com

Tricuspid AtresiaTricuspid Atresia
• Clinical Presentation:a) Cyanosis is almost always
present at birth and is progressive.
b) Etiology/Pathophysiology:i) Due to absence of the
tricuspid valve. This leads to an interatrial right to left shunt, usually through a patent foramen ovale. www.freelivedoctor.comwww.freelivedoctor.com

ii) It is classified by the absenceof tricuspid valve,pulmonary stenosis,and VSD.
iii)The most Common form is also associatedWith a hypoplastic right ventricle
www.freelivedoctor.comwww.freelivedoctor.com

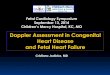
TRICUSPID ATRESIATRICUSPID ATRESIA1 - atrial septal defect2 - absent tricuspid valve3 - ventricular septal defectBlood is shunted through an atrial septal defect to the left atrium and through the ventricular septal defect to the pulmonary artery. The shaded arrows indicate mixing of the blood. www.freelivedoctor.comwww.freelivedoctor.com

Total Anomalous Pulmonary Total Anomalous Pulmonary Venous Connection (TAPVC)Venous Connection (TAPVC)
• No pulmonary veins directly join LAa) drain into left innominate vein
or coronary sinusb) PV drain into RA
• ASD or foramen ovale always present
a) allows PV blood to enter LAb) R to L shunt
• Volume and pressure hypertrophy of RV
www.freelivedoctor.comwww.freelivedoctor.com

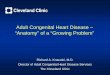
1 - superior vena cava2 - atrial septal defect3 - left innominate vein4 - pulmonary veinsOxygenated blood returning from the lungs is routed back into the superior vena cava, rather than the left atrium. The presence of an atrial septal defect is necessary to allow partially oxygenated blood to reach the left side of the heart.
Total Total Anomalous Anomalous Pulmonary Pulmonary Venous Venous Connection Connection (TAPVC)(TAPVC)
www.freelivedoctor.comwww.freelivedoctor.com

Obsttructive Congenital Obsttructive Congenital AnomaliesAnomalies
Coarctation of the Aorta• Narrowing• Males 2:1 vs. female
a) females with Turners frequently have coarctation
• 2 types:a) infantile (with PDA; poor
outcome)i) prior to PDA
- symptoms early in life- cyanosis of lower body
www.freelivedoctor.comwww.freelivedoctor.com

b) adult (without PDA)i) most children asymptomatic until late in lifeii) hypertension in upper
extremitiesiii) hypotension in lower
extremities• Murmurs
a) throughout systole• LV hypertrophy
www.freelivedoctor.comwww.freelivedoctor.com

1 - pinched or coarcted aorta flow patterns are normal but are reduced below the coarctation. Blood pressure is increased invessels leaving the aorta above the coarctation.The broken white arrow indicates diminishedblood flow through the aorta.
www.freelivedoctor.comwww.freelivedoctor.com

www.freelivedoctor.comwww.freelivedoctor.com

Pulmonary Stenosis and AtresiaPulmonary Stenosis and Atresia
• Obstruction at pulmonary valve• May occur as isolated defect or with:
a) Tetralogy of Fallot orb) TGA
• RV hypertrophya) usually there is poststenotic dilation
i) “jet” streaming• Relatively frequent defectwww.freelivedoctor.comwww.freelivedoctor.com

• Atresia of valvea) no communication between RV
and lungsb) hypoplastic RV with ASDc) flow enters lung through PDA
Aortic Stenosis and AtresiaAortic Stenosis and Atresia• 3 types:
a) valvularb) subvalvularc) supravalvular
• Systolic murmur• LV hypertrophywww.freelivedoctor.comwww.freelivedoctor.com

• Valvular (severe) aortic Valvular (severe) aortic stenosis orstenosis or atresiaatresia
a) outflow obstructioni) hypoplastic LV and
ascending aortab) PDA MUST be present to allow blood flow to:
i) aortaii) coronary arteriesiii) always fatal in first week of life
- when ductus closes !!www.freelivedoctor.comwww.freelivedoctor.com

Aortic stenosis (valvular)1 - narrowed aortic valveFlow patterns are normal but blood flow to the aortais reduced as indicated by the broken white arrows
www.freelivedoctor.comwww.freelivedoctor.com

• Subaortic stenosisSubaortic stenosisa) thickened ring below level of
cusps
• Supraventricular aortic stenosisSupraventricular aortic stenosisa) inherited defect
i) mutation of elastin gene causes this defect
b) ascending aorta is dysplastici) greatly thickened, causing
- narrowing of lumenwww.freelivedoctor.comwww.freelivedoctor.com

Subaortic StenosisSubaortic Stenosis
www.freelivedoctor.comwww.freelivedoctor.com

www.freelivedoctor.comwww.freelivedoctor.com

Heart Failure (i.e.,Congestive)Heart Failure (i.e.,Congestive)
• Heart cannot eject volume which is being returned to it
a) failure to perfuse tissues effectivelyb) usually slowly progressive
i) acute forms- MI- Volume overload- valvular dysfunction
www.freelivedoctor.comwww.freelivedoctor.com

• Compensatory mechanisms:a) Frank-Starling mechanism
i) stretch contractionb) cardiac structural changes
i) hypertrophyc) activation of neurohumoral
systemi) sympathetic tone (NE)
- HR- contractility
ii) renin-angiotensin- aldosterone systemiii) ANP
www.freelivedoctor.comwww.freelivedoctor.com

• Most frequent causes for failure of these compensatory mechanisms are:
a) ischemiab) hypertensionc) whatever the reason for the failure CHF
i) CO (systolic failure) or,ii) CO (diastolic failure)
www.freelivedoctor.comwww.freelivedoctor.com

• Cardiac HypertrophyCardiac Hypertrophy a) cardiac myocyte is terminally differentiated cell
i) no in cell # (i.e., hyperplasia)
ii) load on cells causes cells to in size (i.e., hypertrophy)
- pressure or volume overload- trophic hormones (e.g.,
T4)b) pressure overload
i) “concentric hypertrophy”
www.freelivedoctor.comwww.freelivedoctor.com

ii) wall thicknessiii) cavity diameter
c) volume overloadi) “eccentric hypertrophy”ii) chamber dilationiii) ventricular diameteriv) wall thickness may not
change- owing to simultaneous
hypertrophyd) capillary density with hypertrophy
i) demands ischemia !!
www.freelivedoctor.comwww.freelivedoctor.com

Left Sided Heart FailureLeft Sided Heart Failure
• Most often caused by:a) ischemic heart diseaseb) hypertensionc) aortic and mitral valve diseased) nonischemic myocardial
disease• Major effect is “damming” of blood within the lungs• LV hypertrophy and often dilation• LA secondary dilation
a) stasis, arrhythmia, thrombuswww.freelivedoctor.comwww.freelivedoctor.com

• Lungs major problema) pulmonary vein pressure
i) pulmonary congestion and edema- heavy and wet
b) iron containing proteins in edema fluid and Hb from RBC
i) phagocytosed by macrophages
- converted to “Hemosiderin”
- “heart failure cells”c) dyspnea
i) early sign
www.freelivedoctor.comwww.freelivedoctor.com

d) orthopnea i) dyspnea on lying down and
relieved by sitting upright
e) cough is common with Left sided failure
• Kidneysa) COb) renin-angiotensin-aldosterone
i) retention of salt and water- contribute to edema- counteracted by ANP
www.freelivedoctor.comwww.freelivedoctor.com

Right Sided Heart FailureRight Sided Heart Failure
• Major cause is LEFT heart failure• Occurs as isolated failure in only few diseases
a) chronic pulmonary hypertension
i) “ Cor Pulmonale”• Minimal pulmonary congestion• Major areas of edema are systemic, peripheral
a) liver and portal system i) “congestive hepatomegaly”
www.freelivedoctor.comwww.freelivedoctor.com

ii) when Left heart failure is present, hypoxic liver
shows signs of “centrilobular necrosis”
iii) long standing Right failure- cardiac cirrhosis
iv) portal hypertension- congestive splenomegaly
v) ascites vi) pleural and pericardial effusions accompany Right heart failurewww.freelivedoctor.comwww.freelivedoctor.com

Cardiac TransplantationCardiac Transplantation• 2 major causes:
a) DCMb) IHD
• Major success due to:a) careful selection of patientsb) drug therapyc) sequential biopsies
• Major problemsa) stenosis (coronary arteries)
i) silent MI (no pain !)- CHF or sudden deathwww.freelivedoctor.comwww.freelivedoctor.com

b) infectionsc) malignancies
i) lymphomas- Ebstein-Barr virus
www.freelivedoctor.comwww.freelivedoctor.com
Recommended