Conference on Therapy Case 1: Respiratory Problem
1
Mario, 30 y/o known asthmatic (in remission for past 10 yrs), presents w/
cough 2 mos. duration
Chief complaint: difficulty breathing
2
HPISeveral years PTC• Frequent sneezing, nasal stuffiness (esp. on
waking up in the morning)• Sx abate as day wears on
2 mos. PTC• Persistent nasal stuffiness (whole day),
more severe Sx at night when lying down• Wife says that he “snores loudly”• Started having productive cough and itchy
throat 3
2 mos. PTC (cont’d)• Px took cough and colds OTC w/ partial
relief of Sx
1 mo. PTC• Cough increased in severity esp. in a.m.,
disrupting sleep• paroxysms of retching cough soon after
going to bed• Wife noted “wheezing” sounds while px
is asleep
4
1 mo. PTC (cont’d)• Px complains of easy fatigability, cannot talk
long w/ clients; voice noted to be “hoarse”
1 wk PTC• Developed more severe colds w/ increased
mucopurulent discharge, anosmia, headache• Noted frequent regurgitation• Self medicated w/ amoxicillin 500 mg q 8 hrs
Few hours PTC• All Sx persistent, px developed difficulty
breathing, leading to ER consult5
Personal Hx
Dietheavy soda, tea, coffee & chocolate
consumption for years now
Environmentcarpeted home; indwelling dogs; 2nd
hand cigarette smoke at workplace
6
PE findingsVital signs
RR = 24/min HR = 100/min BP = 120/80
Gen survey• Wt = 90kg Ht = 170cm BMI = 31 (obese)• Ambulatory• Mild respiratory distress w/ loud deep throaty
tight cough
7
HEENT• + dark shadows on both lower lids• Tympanic membranes bulging w/ erythema &
opaque effusions• Nares w/ severe congestions, obstructed
passages, turbinates swollen & violaceous, w/ thick purulent disharge
PE findings (cont’d)
8
Respiratory• Symmetrical chest expansion• Mild suprasternal retractions• Fair air exchange w/ inspiratory & expiratory
wheezes• PFR = 200 L/min (ideal for age and ht = 600)
PE findings (cont’d)
9
Salient features (subjective)• 30 y/o, male• history of asthma• cough of 2 months duration• frequent sneezing & nasal stuffiness esp. in a.m.• snoring loudly• productive cough & itchy throat• easy fatigability• hoarse voice• severe colds w/ increased mucupurulent discharge• anosmia• paroxysms of retching cough soon after going to bed• frequent regurgitation• Heavy soda, coffee, tea, chocolate intake• carpeted home; indwelling dogs; 2nd hand cigarette smoke at
workplace
10
Salient features (objective)
Pertinent positives• obese (BMI=31)• mild respiratory distress (mild
suprasternal retractions)• loud deep throaty tight cough• PFR=200 L/min (normal=600)• + dark shadows on both lower
lids• tympanic membranes bulging w/
erythema & opaque effusions• inspiratory & expiratory wheezes• nares w/ severe congestion,
obstructed passages, turbinates swollen & violaceous, w/ thick purulent discharge
Pertinent negatives
• symmetrical chest expansion
• fair air exchange
11
Clinical impressionMario has the ff conditions:
•known asthmatic (10 yr remission)•Acute severe asthma•Allergic rhinitis (co-morbidity)•Sinusitis (bacterial)•Acute otitis media (bacterial)•GERD•Obesity (predisposing him to GERD and obstructive sleep apnea)
12
• Acute severe asthma– history of asthma– cough of 2 months duration– loud deep throaty tight cough– inspiratory & expiratory wheezes– easy fatigability, hoarse voice– mild respiratory distress (mild suprasternal
retractions)– PFR = 200 L/min (normal for age & height = 600)
13
Clinical impression
Evidences
-allergic rhinitis (early am sneezing, nasal stuffiness, postnasal drip, env. exposure; asthmatic)- sinusitis (anosmia, nares w/ severe congestion, obstructed passages, turbinates swollen & violaceous, w/ thick purulent discharge)
Clinical impression
14
Evidences
- acute otitis media (tympanic membranes bulging w/ erythema & opaque effusions) - GERD (paroxysms of retching cough soon after going to bed, frequent regurgitation)
15
Clinical impression
United Airway Disease Hypothesis
“any disease process that affects the upper airway is likely to affect the lower airway, and vice versa, by both direct and indirect means. It is postulated that rhinitis and asthma represent the manifestations of one syndrome in two parts of the respiratory tract, the upper and lower airways, respectively.”
What happened to our patient?
16
Rimmer, J. & Ruhno, J. (2006). Rhinitis and asthma: United airway disease. The Medical Journal of Australia. 185 (10): 565-571
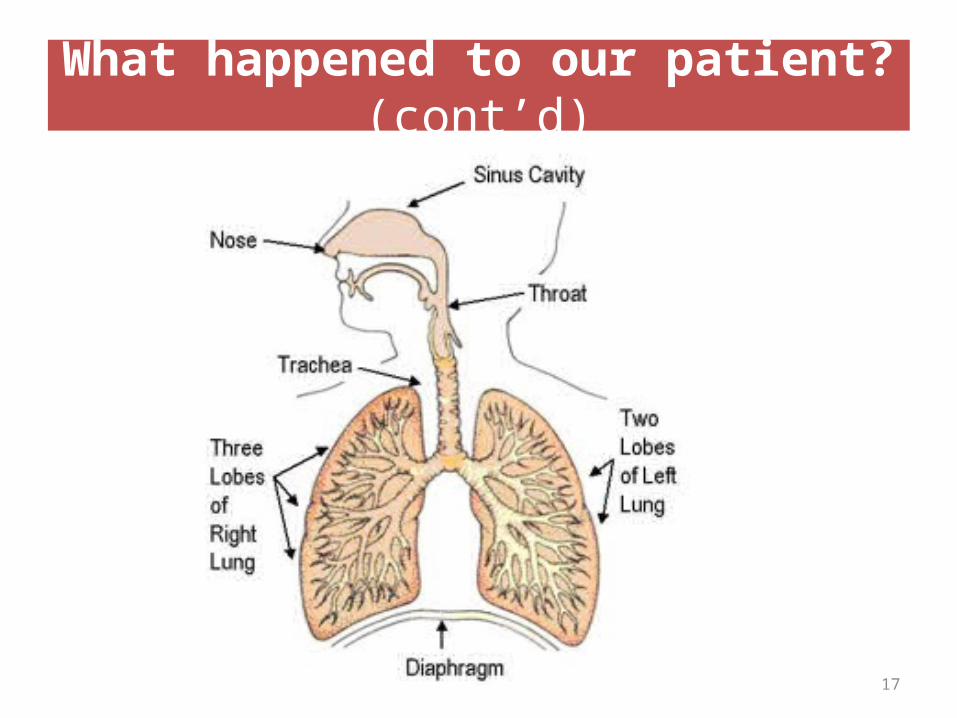
What happened to our patient? (cont’d)
17
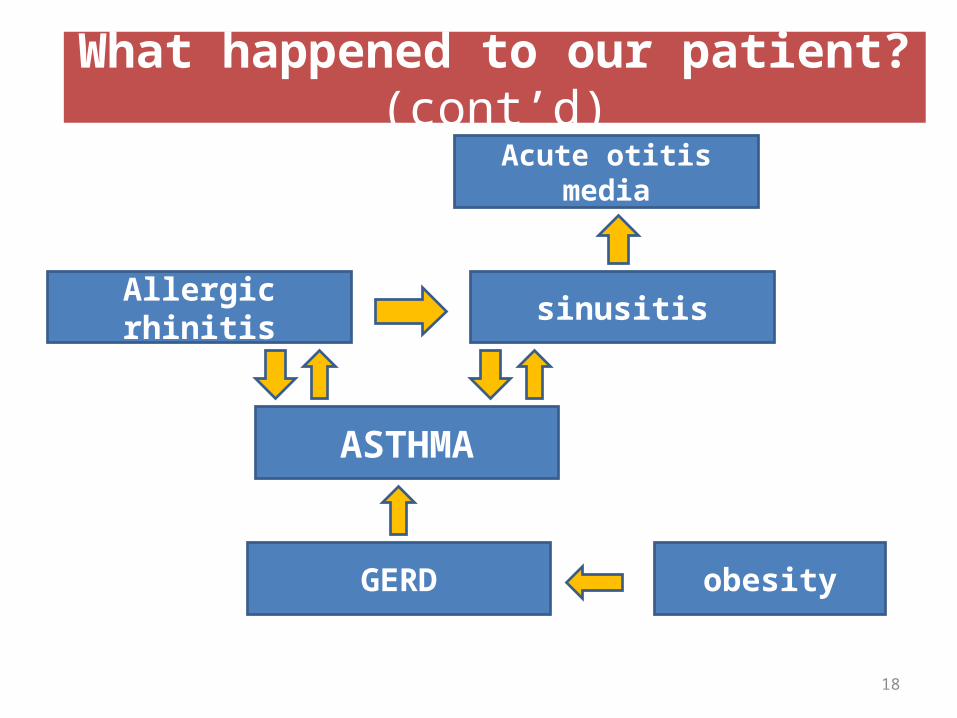
Allergic rhinitis sinusitis
ASTHMA
Acute otitis media
GERD obesity
What happened to our patient? (cont’d)
18
19
What happened to our patient? (cont’d)
Allergic rhinitis and asthma
• Allergic asthma and AR are often considered clinical manifestations of the same condition, the chronic allergic respiratory syndrome.
• approx 80% of asthmatics also have AR
What happened to our patient? (cont’d)
20
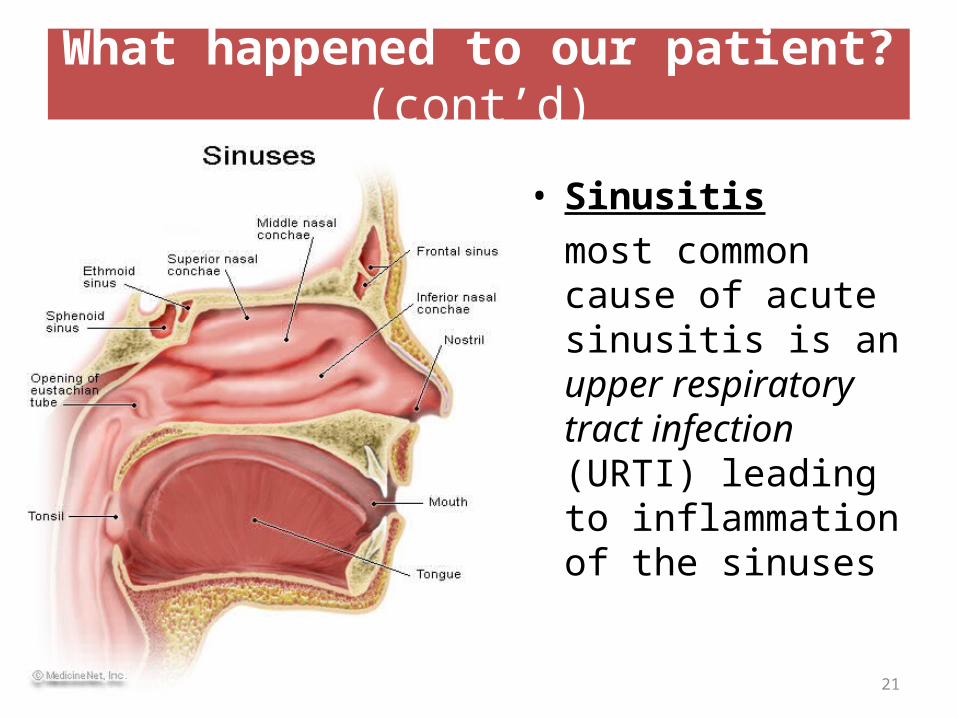
What happened to our patient? (cont’d)
• Sinusitismost common cause of acute sinusitis is an upper respiratory tract infection (URTI) leading to inflammation of the sinuses
21
Acute Otitis mediausually arises as a complication of a preceding upper respiratory infection (URI).The secretions and inflammation cause a relative obstruction of the eustachian tubes.
*infection due to sinusitis may be from S. pneumoniae, H. influenzae, or M. catarrhalis
What happened to our patient? (cont’d)
22
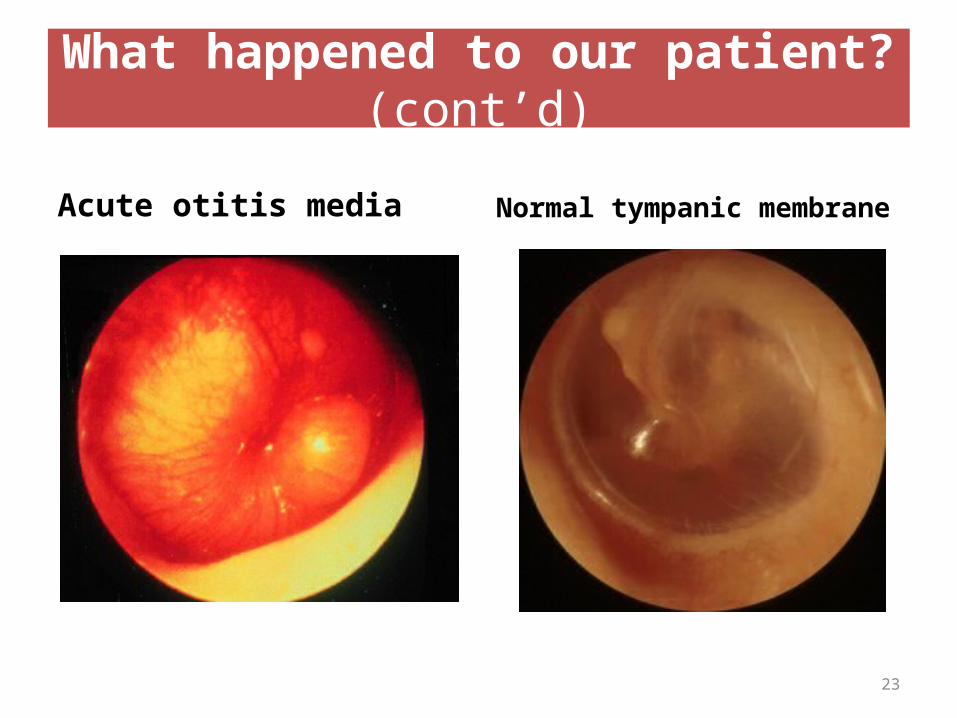
Acute otitis media Normal tympanic membrane
What happened to our patient? (cont’d)
23
GERD and Asthma• estimated that more than 75% of patients with
asthma also experience GERD. • People with asthma are twice as likely to have GERD
as those people who do not have asthma. • Of those people with asthma, those who have a
severe, chronic form that is resistant to treatment are most likely to also have GERD.
What happened to our patient? (cont’d)
Source: Cleveland Clinic health information website at http://my.clevelandclinic.org/disorders/gastroesophageal_reflux_gerd/hic_gerd_and_asthma.aspx
24
GERD and Asthma1. Acid flow causes injury to the lining of the
throat, airways and lungs, making inhalation difficult and often causing a persistent cough.
2. When acid enters the esophagus, a nerve reflex is triggered, causing the airways to narrow in order to prevent the acid from entering. This will cause a shortness of breath.
What happened to our patient? (cont’d)
Source: Cleveland Clinic health information website at http://my.clevelandclinic.org/disorders/gastroesophageal_reflux_gerd/hic_gerd_and_asthma.aspx
25
Plan of Action (Therapy)
1. Address respiratory distress2. Address long term treatment for asthma3. Treat the nasal & ear infection4. Treat allergic rhinitis5. Treat GERD6. Non-pharmacologic measures
26
1. Address respiratory distress- Give reliever to immediately dilate narrowed airways (short acting β2 agonists)
- SALBUTAMOL recommended- Give supplemental O 2
Plan of Action (Therapy)
27
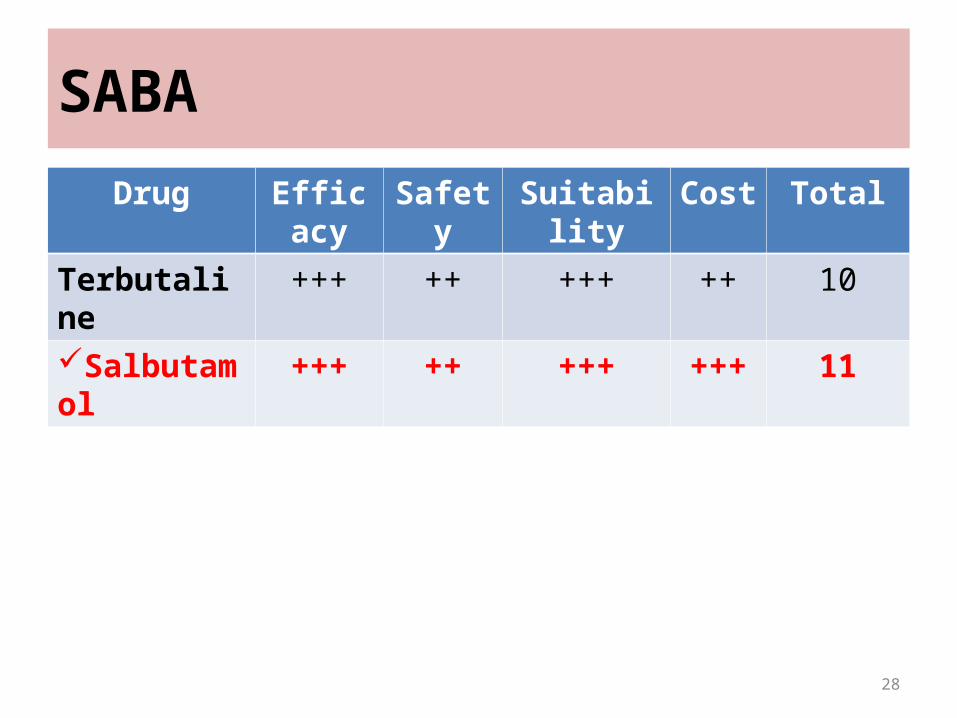
SABA
Drug Efficacy Safety Suitability Cost Total
Terbutaline +++ ++ +++ ++ 10
Salbutamol +++ ++ +++ +++ 11
28
Medicines for short term asthma relief
1. SABA (salbutamol or terbutaline)
MOA: activate β2 receptors; activate adenylyl cyclase; inc. cAMP; activate proein kinase A to phosphorylate several target proteins leading to cell muscle relaxation
29
β2 Agonists
Pharmacokinetics10% is deposited in the bronchial airway after inhalation Absorbed in systemic circulation Most of the inhaled dose is swallowed and absorbed from
GIT Rapidly metabolized Rapidly excreted in urine and stools A portion in the systemic circulation is excreted in the
kidneys unchanged
30
β2 Agonists
PharmacodynamicsActivation of β2 leads to activation of adenylyl cyclase
Activation of protein kinase A Phosphorylates target proteins within the cell Muscle relaxation thru :
– Activate uptake of Ca++ from cell into intracellular stores– Inhibition of phosphoinositide hydrolysis– Inhibition of myosin light chain kinase prevents interaction of myosin
with actin– Opening of large conductance Ca++ activated K+ channels that
repolarize
31
Drug interactions
• Effect of high doses may be exacerbated by concomitant administration of high doses of corticosteroids.
• effects are antagonized by propanolol or other beta- receptor blocking agents.
• Concomitant aminophylline or xanthine administration may enhance beta agonist effects.
• Hypokalemia associated with high doses may increase the susceptibility to digitalis-induced cardiac arrhythmias.
β2 Agonists
32
AE of β2 agonists
• Muscle cramps, arythmia, tachycardia, palpitaion, tremors
• inc. in: lactate, glucose, FFA, insulin• Inc. V-P mismatch (that’s why give O 2
nebulizer)• headache, restlessness, tension, dizziness,
nervousness, insomnia
33
2. Systemic oral corticosteriods (prednisone or prednisolone)
- Give for 5 to 10 days for treatment of acute severe asthma, no tapering of dose needed
MOA: anti-inflammatory effects due to inhib. of production of pro-inflammatory cytokines & chemokines; dec. lymphocytes & leukocytes in airways; dec. bronchial hyperreactivity; dec. mucus production; potentiate β2 agonist effect
Medicines for short term asthma relief (cont’d)
34
Corticosteroids in Asthma
• PharmacokineticsMajority of the ICS that are swallowed and absorbed from the GIT undergo extensive first pass effect in the liver ↓ systemic toxicity. ICS that are deposited into the respiratory system are absorbed systemically and may potentially cause adverse effect
• PharmacodynamicsAnti-inflammatory effects due to inhibition of
production of proinflammatory cytokines and chemokines ↓ trafficking of lymphocytes, eosinophils and other leukocytes into airways ↓ bronchial hyperreactivity
• Potentiates β2 agonist effect by ↑ synthesis of β2 receptors
• ↓ mucus production
Corticosteroids in Asthma
Some AE of sys. corticosteroids
• Truncal obesity, moon facies• Ulcers, striae, acne, hirsutism, alopecia, poor
wound healing, skin thinning• Osteoporosis, inc. risk of fractures, growth
stunting, muscular atrophy• Inc. susceptibility to infection• Hyperacidity, PUD• Inc. renal loss of calcium & dec. GIT
metabolism37
• NOTE: High doses of CS treatment of < 1 to 2 wks therapy unlikely to cause HPA axis suppression & adverse effects
• Tell px not to worry as systemic CS will only be 7 days duration
38
• Drug Interactions
Efficacy may be reduced by rifampicin, ephedrine, barbiturates, phenytoin, primidone. Corticosteroids may reduce effects of diuretics, hypoglycemics, anticholinesterases in myasthenia gravis, salicylates. May impair glucose tolerance when used with antidiabetics.
Corticosteroids in Asthma
2. Address long term treatment for asthma- Give Long acting β2 agonist with corticosteroid (inhalational)
Plan of Action (Therapy)
40
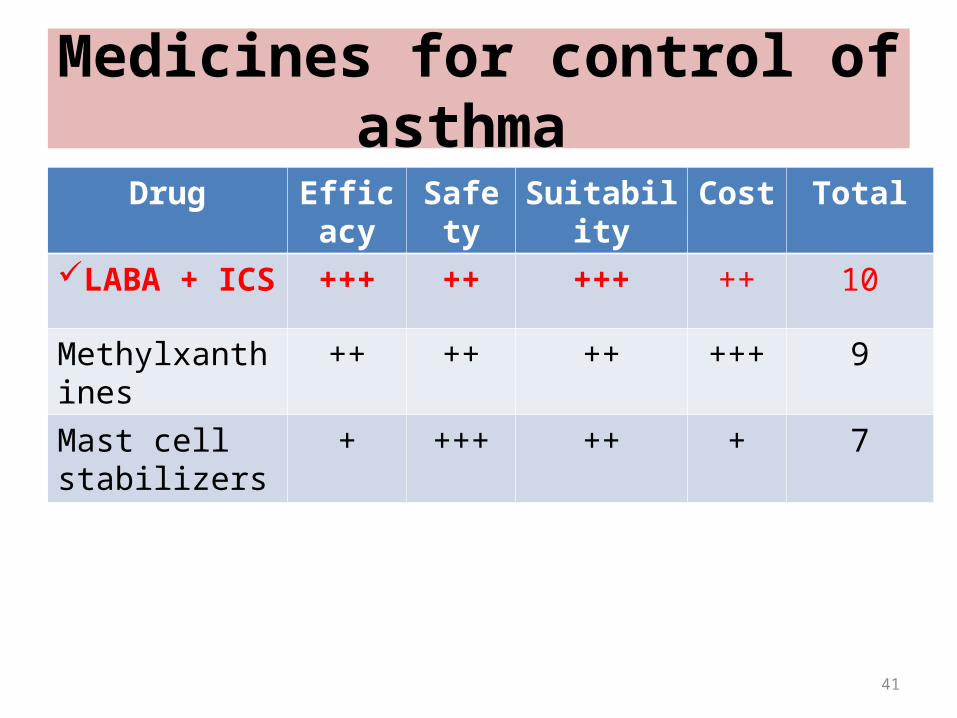
Medicines for control of asthma
Drug Efficacy Safety Suitability Cost Total
LABA + ICS +++ ++ +++ ++ 10
Methylxanthines ++ ++ ++ +++ 9
Mast cell stabilizers
+ +++ ++ + 7
41
Medicines for control of asthma
1. LABA- Pk, Pd, MOA, AE, drug interactions are same
as SABA- LABA lipophilicity, affinity, selectivity > SABA- LABA can be used vs. nocturnal asthma - Formoterol may be used for both control +
relief to fast onset of action
42
2. Give inhalational corticosteroid (Budesonide or Fluticasone)Pk, Pd, MOA: (same as sys. corticosteriod)
AE: usually hoarseness/dysphonia, oral candidiasis, throat irritation and cough
* Use spacer between MDI & mouth; ask px to gargle after inhalation
Medicines for long term asthma relief (cont’d)
43
3. Treat the nasal and ear infection- Antibiotic for the most likely causative pathogen (e.g. S. pneumoniae, H. influenzae, M. catarrhalis)
Plan of Action (Therapy)
44
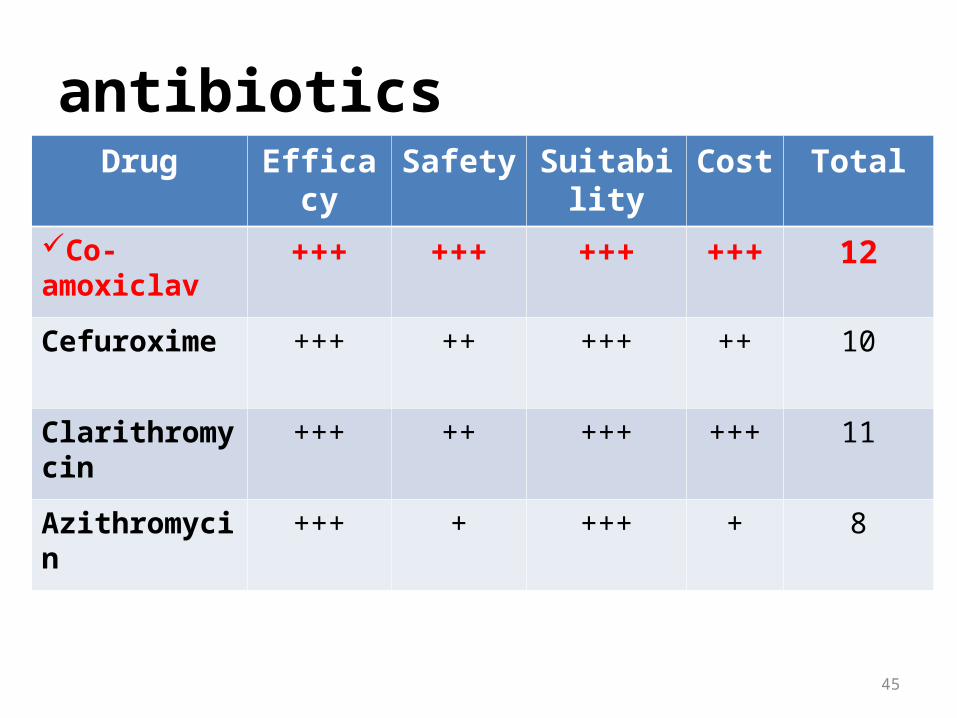
antibiotics
45
Drug Efficacy Safety Suitability Cost Total
Co-amoxiclav +++ +++ +++ +++ 12
Cefuroxime +++ ++ +++ ++ 10
Clarithromycin +++ ++ +++ +++ 11
Azithromycin +++ + +++ + 8
Co-amoxiclav
Pharmacokinetics• 75 % oral absorption with or without food• 20-30% protein boundPharmacodynamics, MOA• Binds irreversibly to the catalytic site of beta-lactamases
rendering them inactive• Binds with one or more PBPs causing selective inhibition
of transpeptidase, carboxypeptidase and endopeptidase reactions required for cross linkage between peptide chains in the synthesis of mucopeptide
• Activates endogenous autolytic enzymes in the cell wall
Co-amoxiclav
• Adverse ReactionsDiarrhea, nausea, skin rashes & urticaria, vaginitis,
abdominal discomfort, flatulence & headache• Drug interactionsConcomitant administration of probenecid may
result in increased & prolonged blood levels of amoxicillin. Increased incidence of skin rashes with allopurinol. Must not be given with disulfiram
4. Treat allergic rhinitis- Give oral 2nd Gen. H1 antagonist to control AR
- When px with co-morbid AR have AR controlled: LESS risk of hospitalizations or emergency department visits for asthma *
Plan of Action (Therapy)
*Bousquet J, Van Cauwenberge P, Khaltaev N. Allergic rhinitis and its impact on asthma. J Allergy Clin Immunol. 2001;108:S147–S334.
* Thomas M. Allergic rhinitis: evidence for impact on asthma. BMC Pulm Med. 2006;6:S4.
48
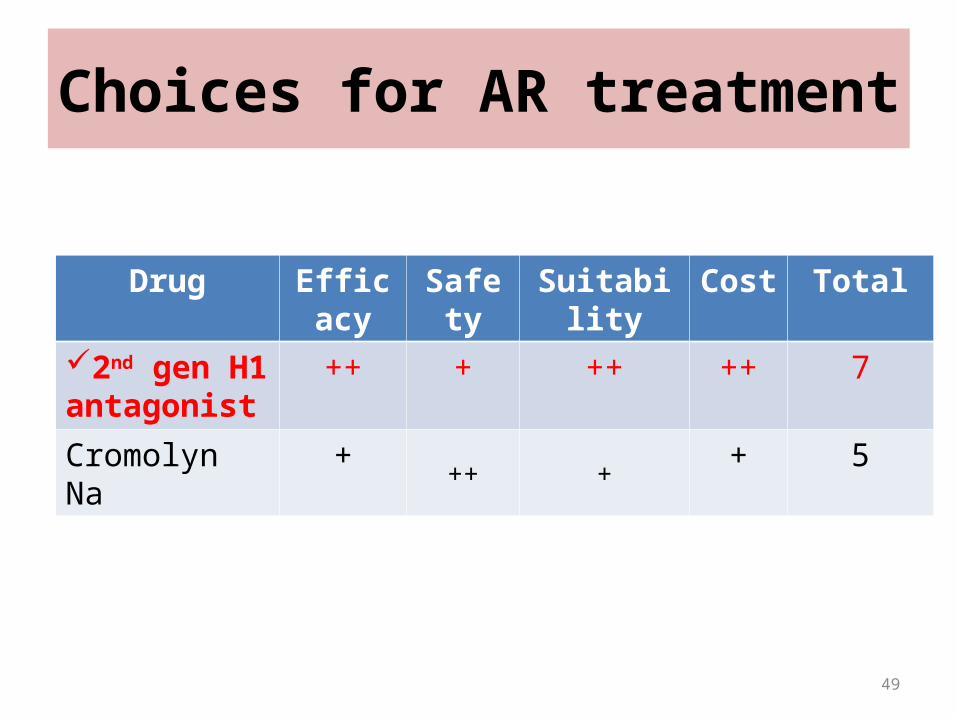
Choices for AR treatment
Drug Efficacy Safety Suitability Cost Total
2nd gen H1 antagonist
++ + ++ ++ 7
Cromolyn Na + ++ + + 5
49
Loratadine
• A second generation antihistamine (H1 blocker) drug
• Used to prevent or treat the symptoms of allergic reactions
Loratadine: MOA
Reversible competitive antagonism at the H1 receptor
Reversible competitive antagonism at the H1 receptor
Blocks action of histamineBlocks action of histamine
Loratadine: Pharmacokinetics
• Given orally, well absorbed from the GI tract, peak effect occurs in 1–2 hours, duration of action 12-24 hours
• Has rapid first-pass hepatic metabolism; metabolized by CYP450 (including CYP3A4)
• Less lipid soluble, acts as substrate of p-glycoprotein transporter in the brain
Loratadine: Pharmacokinetics
• Almost totally bound to plasma proteins
• Active metabolite: desloratadine – binds to plasma proteins only moderately
• About 40% is excreted as conjugated metabolites into the urine, and a similar amount is excreted into the feces.
Loratadine: Pharmacodynamics
• Competitive antagonism at the H1 receptor– Negligible potency at the H2 receptor, little at the
H3 receptor
• 2nd generation H1 antagonists have less sedating characteristics than the 1st generation– Less distribution in CNS
Loratadine: Adverse Effects
• Headache, fatigue, dry mouth, thirst, hoarseness– should lessen as your body adjusts to the
medication
• Rarer effects:– nervousness, rapid or pounding heartbeat,
unusual weakness, stomach pain, dizziness, diarrhea
Loratadine: Drug Interactions
• Drug interaction with CYP3A4 enzyme inhibitors can cause ventricular arrhythmia (Torsades de pointes)– Ketoconazole, macrolide antibiotics– Significant increase in the blood concentration of
loratadine
5. Treat GERD- give proton pump inhibitor to decrease HCl secretion
Plan of Action (Therapy)
57
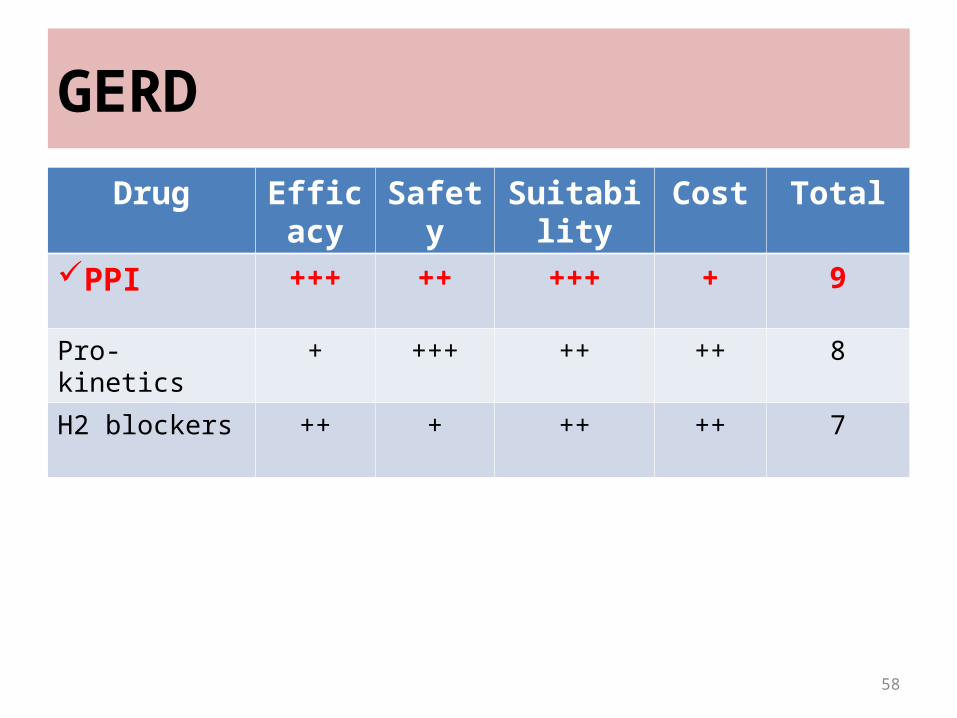
GERD
Drug Efficacy Safety Suitability Cost Total
PPI +++ ++ +++ + 9
Pro-kinetics + +++ ++ ++ 8
H2 blockers ++ + ++ ++ 7
58
Omeprazole
Proton Pump Inhibitor
MOA:suppresses gastric acid secretion by specific
inhibition of the enzyme system hydrogen/potassium adenosine triphosphatase (H+/K+ ATPase) present on the secretory surface of the gastric parietal cell.

Omeprazole
Pharmacokinetics:Administered as inactive prodrug Lipophilic weak bases, that diffuse readily across
lipid membranes becomes protonated in gastric parietal cell
canaliculusReactivates to thiophilic sulfonamideIrreversibly inactivates H+/K+ ATPase
Omeprazole
Pharmacodynamics:
Inhibits both fasting and meal-stimulated secretion
Blocks the final common pathway of acid secretion, the Proton Pump
Omeprazole
Indication:• Most effective agent for treatment of erosive
and non-erosive reflux disease• Peptic ulcer disease• Non-ulcer dyspepsia• Stress-related mucosal bleeding
Omeprazole
Dosage :• 20-40mg should be administered 1 hr before
meal ( usually breakfast or dinner)
Omeprazole
Adverse effect:• PPI are extremely safe, however diarrhea,
headache, and abdominal pain are reported (1-5%)
Omeprazole
Drug interactions:• Metabolized by hepatic P450 cytochromes• Inhibits the metabolism of Coumadin,
Diazepam and Phenytoin
6. Non-pharmacological treatment (asthma & AR)- remove all carpeting at home- place dogs outside the home or get rid of them- keep home clean by using air cleaners; vacuum well (minimize dust, molds, pollen)- be mindful to avoid 2nd hand cigarette exposure
Plan of Action (Therapy)
66
6. Non-pharmacological treatment (GERD)- cease soda, chocolate, tea, coffee intake- small frequent feedings (no heavy meals)- ask px not to lie down shortly after a meal- lie semi-upright or left lateral recumbent- reduce weight (diet and exercise) as obesity worsens GI reflux & may predispose to obstructive sleep apnea
Plan of Action (Therapy)
67
6. Non-pharmacological treatment (obesity)– Control diet– After asthma has been controlled, start
exercising (i.e. swimming – may also be good for his asthma)
68
Plan of Action (Therapy)
*Obese px w/ loud snoring
• May use continuous positive airway pressure (CPAP) machine to control loud snoring during sleep (esp. if he is eventually diagnosed with obstructive sleep apnea since he is obese)
69
Prescriptions
• Prednisone (salbutamol at ER only)• Formoterol + Budesonide (Symbicort)• Co-amoxiclav• Loratadine• Omeprazole
70
Juan Dela Cruz, M.D.Internal Medicine
MAB Rm. 2012Santo Tomas University Hospital
España, Manila
Name: ___Mario_Silvestre_______ ____ Date: _Feb. 26, 2009__Address: __ Quezon City_ ___________ Age: _30_Sex: _M__
_ Juan dela Cruz_____ M.D.
License no. 2003001234
PTR no. 12051986
Prednisone 30 mg tab
Dispense 7 tablets
Sig. Take 1 tablet by mouth after breakfast daily for 7 days.
For asthma
Juan Dela Cruz, M.D.Internal Medicine
MAB Rm. 2012Santo Tomas University Hospital
España, Manila
Name: ___Mario_Silvestre____________ Date: _Feb. 26, 2009__Address: __ Quezon City_ ___________ Age: 30__Sex: _M ___
_ Juan dela Cruz_____ M.D.
License no. 2003001234
PTR no. 12051986
Budesonide + formoterol fumarate 80/4.5 mcg turbuhaler
Dispense 1 turbuhaler
Sig. Take 2 puffs by mouth twice daily, in the morning and evening everyday
For asthma
Juan Dela Cruz, M.D.Internal Medicine
MAB Rm. 2012Santo Tomas University Hospital
España, Manila
Name: ___Mario_Silvestre_______ Date: __Feb. 26, 2010_Address: ____Quezon City_ Age: _30__Sex: _M__
Juan dela Cruz___M.D.
License no. 2003001234PTR no. 12051986
Co- Amoxiclav 1 g tab
Dispense 20 tablets
Sig. Take 1 tablet by mouth before meals twice a day for 10 days
For acute sinusitis and otitis media
Juan Dela Cruz, M.D.Internal Medicine
MAB Rm. 2012Santo Tomas University Hospital
España, Manila
Name: ___Mario_Silvestre____________ Date: __Feb. 26, 2010_Address: __ Quezon City_ ___________ Age: _30__Sex: _M__
Juan dela Cruz___M.D.
License no. 2003001234PTR no. 12051986
Loratadine 10 mg tab
Dispense 30 tablets
Sig. Take 1 tablet by mouth after a meal once a day for 4 weeks.
For allergic rhinitis
Juan Dela Cruz, M.D.Internal Medicine
MAB Rm. 2012Santo Tomas University Hospital
España, Manila
Name: ___Mario_Silvestre_________ Date: _Feb. 26, 2010__Address: ___Quezon City__________ Age: _30_Sex: _M__
_ Juan dela Cruz_ __M.D.
License no. 2003001234PTR no. 12051986
Omeprazole 20 mg capsule
Dispense 30 tablets
Sig. Take 1 tablet by mouth before meals once daily for 4 weeks
For Gastroesophageal reflux disease
Recommended

















