PSYCHOANALYTIC THEORYSigmund Freud (1961), who has been called the father
of psychiatry, is credited as the first to identify development by stages. He considered the first 5 years of a child’s life to be the most important, because he believed that an individual’s basic character had been formed by the age of 5.
Freud’s personality theory can be conceptualized according to :
1.Structure and dynamics of the personality
2.Topography of the mind
3.stages of personality development.
2
PSYCHOANALYTIC THEORYStructure of the Personality : Freud organized the
structure of the personality into three major components:
Id The id is the locus of instinctual drives—the “pleasure
principle.” Present at birth, it endows the infant with instinctual drives that seek to satisfy needs and achieve immediate gratification. Id-driven behaviors are impulsive and may be irrational.
3
PSYCHOANALYTIC THEORYEgo The ego, also called the rational self or the “reality
principle,” begins to develop between the ages of 4 and 6 months. The ego experiences the reality of the external world, adapts to it, and responds to it , it seeks to bring the influences of the external world to bear upon the id, to substitute the reality principle for the pleasure principle . A primary function of the ego is one of mediator to maintain harmony among the external world, the id, and the superego.
4
PSYCHOANALYTIC THEORYSuperegoThe superego might be referred to as the “perfection
principle.” which develops between ages 3 and 6 years, internalizes the values and morals set forth by primary caregivers. Derived from a system of rewards and punishments.
The superego is composed of two major components: the ego-ideal and the conscience. When a child is consistently rewarded for “good” behavior, self-esteem is enhanced, and the behavior becomes part of the ego ideal. The conscience is formed when the child is consistently punished for “bad” behavior. The child learns what is considered morally right or wrong from feedback received from parental figures and from society or culture.
5
PSYCHOANALYTIC THEORYTopography of the Mind Freud classified all mental contents and operations into three
categories:
1- The conscious : all memories that remain within an individual’s awareness. Events and experiences that are easily remembered .Examples : telephone numbers, birthdays of self and significant others. The conscious mind is thought to be under the control of the ego, the rational and logical structure of the personality.
2- The preconscious : all memories that may have been forgotten or are not in present awareness but can be recalled into consciousness. Examples : telephone numbers or addresses once known but little used . It is thought to be partially under the control of the superego, which helps to suppress unacceptable thoughts and behaviors.
6
PSYCHOANALYTIC THEORY
Topography of the Mind
3- The unconscious: all memories that one is unable to bring to conscious awareness. Which consists of unpleasant or nonessential memories that have been repressed and can be retrieved only through therapy, hypnosis, and with certain substances that alter the awareness and have the capacity to restructure repressed memories. Unconscious material may also emerge in dreams and in seemingly incomprehensible behavior.
7
PSYCHOANALYTIC THEORYDynamics of the PersonalityFreud believed that psychic energy is the force or impetus
required for mental functioning. Originating in the id, it instinctually fulfills basic physiological needs. Freud called this psychic energy the libido.
As the child matures, psychic energy is diverted from the id to form the ego and then from the ego to form the superego. Psychic energy is distributed within these three components. If an excessive amount of psychic energy is stored in one of these personality components, behavior reflects that part of the personality. For instance, impulsive behavior prevails when excessive psychic energy is stored in the id. Overinvestment in the ego reflects self-absorbed, or narcissistic, behaviors; an excess within the superego results in rigid, self deprecating behaviors.
8
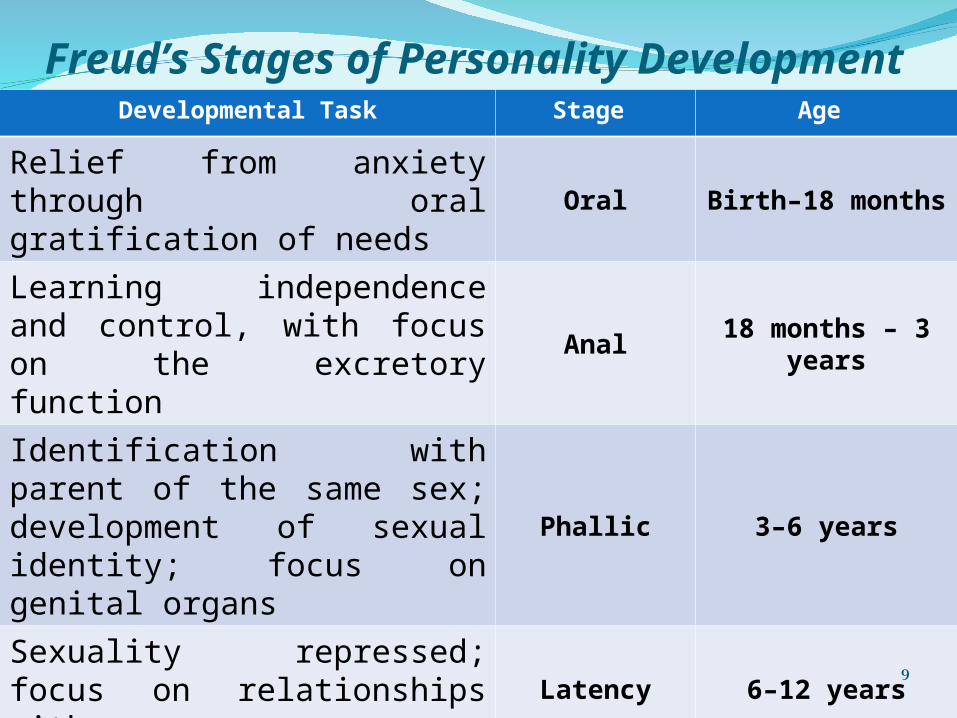
Freud’s Stages of Personality DevelopmentAge Stage Developmental Task
Birth–18 monthsOralRelief from anxiety through oral gratification of needs
18 months – 3 yearsAnalLearning independence and control, with focus on the excretory function
3–6 yearsPhallic
Identification with parent of the same sex; development of sexual identity; focus on genital organs
6–12 yearsLatencySexuality repressed; focus on relationships with same sex peers
13–20 yearsGenital
Libido reawakened as genital organs mature; focus on relationships with member of the opposite sex
9
Relevance of PsychoanalyticTheory to Nursing Practice
Knowledge of the structure of the personality can assist nurses who work in the mental health setting :
1. The ability to recognize behaviors associated with the id, the ego, and the superego .
2. Assists in the assessment of developmental level.
3. Understanding the use of ego defense mechanisms in making determinations about maladaptive behaviors.
4. Assist nurses in planning care for clients to assist in creating change (if desired), or in helping clients accept themselves as unique individuals.
10
INTERPERSONAL THEORYSullivan (1953) believed that individual behavior and
personality development are the direct result of interpersonal relationships. Sullivan embraced the concepts of Freud. Later, he changed the focus of his work from the intrapersonal view of Freud to one with a more interpersonal flavor in which human behavior could be observed in social interactions with others. His ideas, which were not universally accepted at the time, have been integrated into the practice of psychiatry through publication only since his death in 1949.
11
Sullivan’s major concepts include the following:
1.Anxiety is a feeling of emotional discomfort, toward the relief or prevention of which all behavior is aimed. Sullivan believed that anxiety is the “chief disruptive force in interpersonal relations and the main factor in the development of serious difficulties in living.” It arises out of one’s inability to satisfy needs or achieve interpersonal security.
2.Satisfaction of needs is the fulfillment of all requirements associated with an individual’s physiochemical environment. Sullivan identified examples of these requirements as oxygen, food, water, warmth, tenderness, rest, activity, sexual expression—virtually anything that, when absent, produces discomfort in the individual.
12
Sullivan’s major concepts include the following:
3. Interpersonal security is the feeling associated with relief from anxiety. When all needs have been met, one experiences a sense of total well-being, which Sullivan termed interpersonal security. He believed individuals have an innate need for interpersonal security.
4.Self-system is a collection of experiences, or security measures, adopted by the individual to protect against anxiety.
Sullivan identified three components of the self system, which are based on interpersonal experiences early in life:
13
Sullivan’s major concepts include the following:A.The “good me” is the part of the personality that develops in response
to positive feedback from the primary caregiver. Feelings of pleasure, contentment, and gratification are experienced. The child learns which behaviors elicit this positive response as it becomes incorporated into the self system.
B.The “bad me” is the part of the personality that develops in response to negative feedback from the primary caregiver. Anxiety is experienced, eliciting feelings of discomfort, displeasure, and distress. The child learns to avoid these negative feelings by altering certain behaviors.
C.The “not me” is the part of the personality that develops in response to situations that produce intense anxiety in the child. Feelings of horror, awe, to these situations, leading the child to deny these feelings in an effort to relieve anxiety. These feelings, having then been denied, become “not me,” but someone else. This withdrawal from emotions has serious implications for mental disorders in adult life.
14
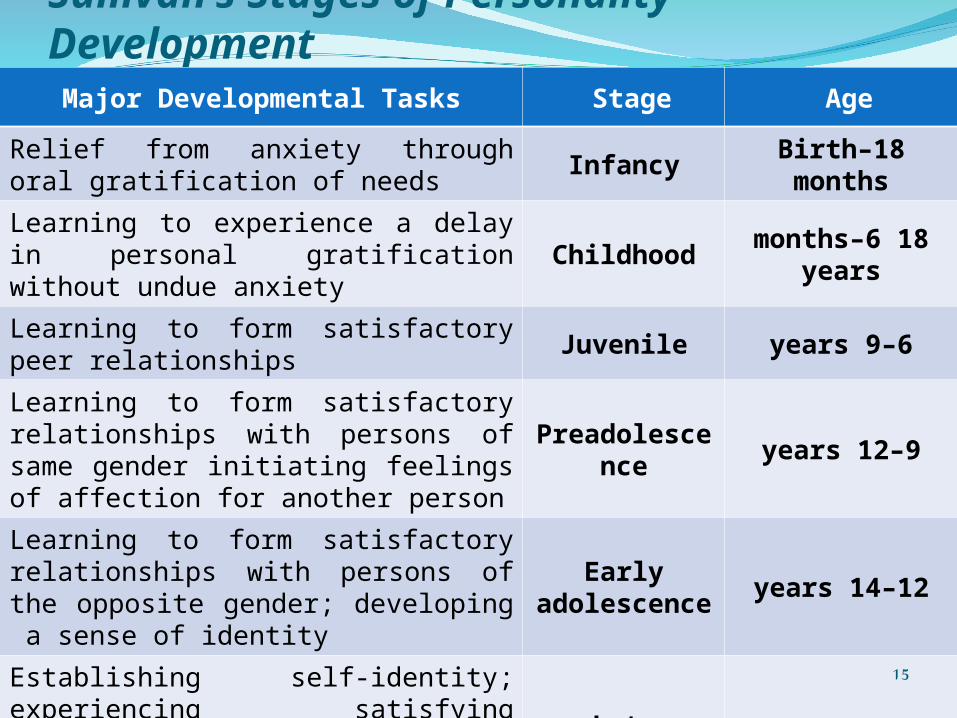
Sullivan’s Stages of Personality DevelopmentAge Stage Major Developmental Tasks
Birth–18 monthsInfancyRelief from anxiety through oral gratification of needs
18 months–6 yearsChildhoodLearning to experience a delay in personal gratification without undue anxiety
6–9 yearsJuvenileLearning to form satisfactory peer relationships
9–12 yearsPreadolescenceLearning to form satisfactory relationships with persons of same gender initiating feelings of affection for another person
12–14 yearsEarly
adolescence
Learning to form satisfactory relationships with persons of the opposite gender; developing a sense of identity
14–21 yearsLate
adolescence
Establishing self-identity; experiencing satisfying relationships; working to develop a lasting, intimate opposite-gender relationship
15
Relevance of InterpersonalTheory to Nursing PracticeRelationship development is a major concept of this
theory, and is also a major psychiatric nursing intervention.
Nurses develop therapeutic relationships with clients in an effort to help them generalize this ability to interact successfully with others.
With knowledge about the behaviors associated with all levels of anxiety nurses can help clients achieve interpersonal security and a sense of well-being.
Nurses use the concepts of Sullivan’s theory to help clients achieve a higher degree of independent and interpersonal functioning.
16
THEORY OF PSYCHOSOCIALDEVELOPMENT
Erikson (1963) studied the influence of social processes on the development of the personality. He described eight stages of the life cycle during which individuals struggle with developmental “crises.” Specific tasks associated with each stage must be completed for resolution of the crisis and for emotional growth to occur.
17
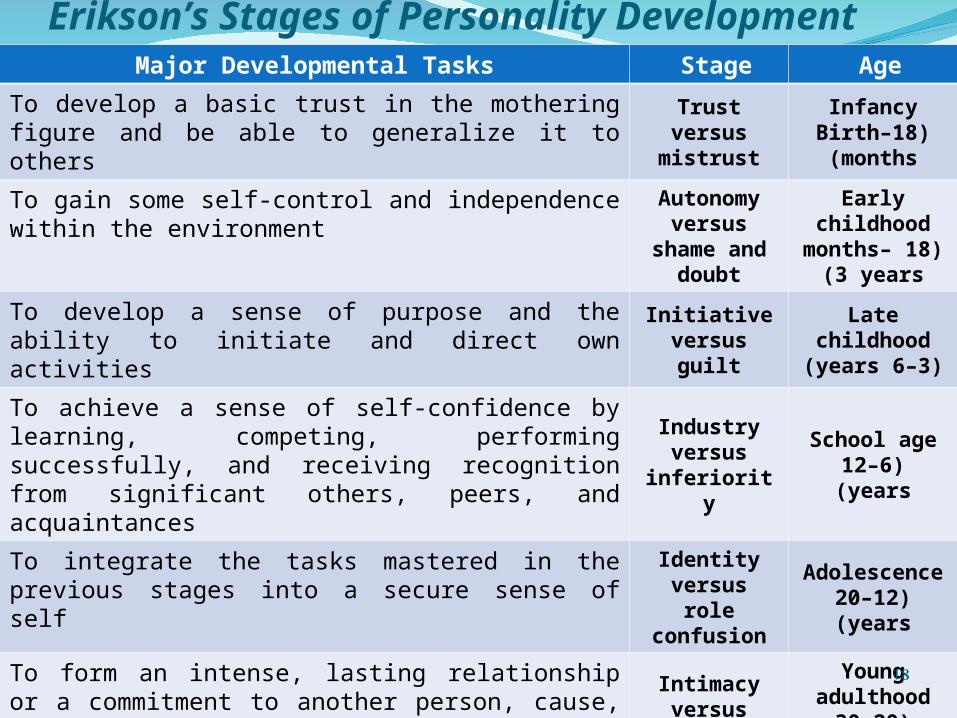
Erikson’s Stages of Personality DevelopmentAge Stage Major Developmental Tasks
Infancy(Birth–18
months)
Trust versus mistrust
To develop a basic trust in the mothering figure and be able to generalize it to others
Early childhood(18 months–3
years)
Autonomy versus shame
and doubt
To gain some self-control and independence within the environment
Late childhood(3–6 years)
Initiative versus guilt
To develop a sense of purpose and the ability to initiate and direct own activities
School age(6–12 years)
Industry versus
inferiority
To achieve a sense of self-confidence by learning, competing, performing successfully, and receiving recognition from significant others, peers, and acquaintances
Adolescence(12–20 years)
Identity versus role confusion
To integrate the tasks mastered in the previous stages into a secure sense of self
Young adulthood
(20–30 years)
Intimacy versus isolation
To form an intense, lasting relationship or a commitment to another person, cause, institution, or creative effort
Adulthood(30–65 years)
Generativity versus
stagnation
To achieve the life goals established for oneself, while also considering the welfare of future generations
Old age(65 years -
death)
Ego integrity versus despair
To review one’s life and derive meaning from both positive and negative events, while achieving a positive sense of self worth
18
THEORY OF OBJECT RELATIONS
Mahler (Mahler, Pine, & Bergman, 1975) formulated a theory that describes the separation–individuation process of the infant from the maternal figure (primary caregiver).
She described the process as progressing through three major phases, and further delineated phase III, the separation–individuation phase, into four subphases.
19
Stages of Development in Mahler’s Theory of Object Relations
Age Phase/ SubphaseMajor Developmental Tasks
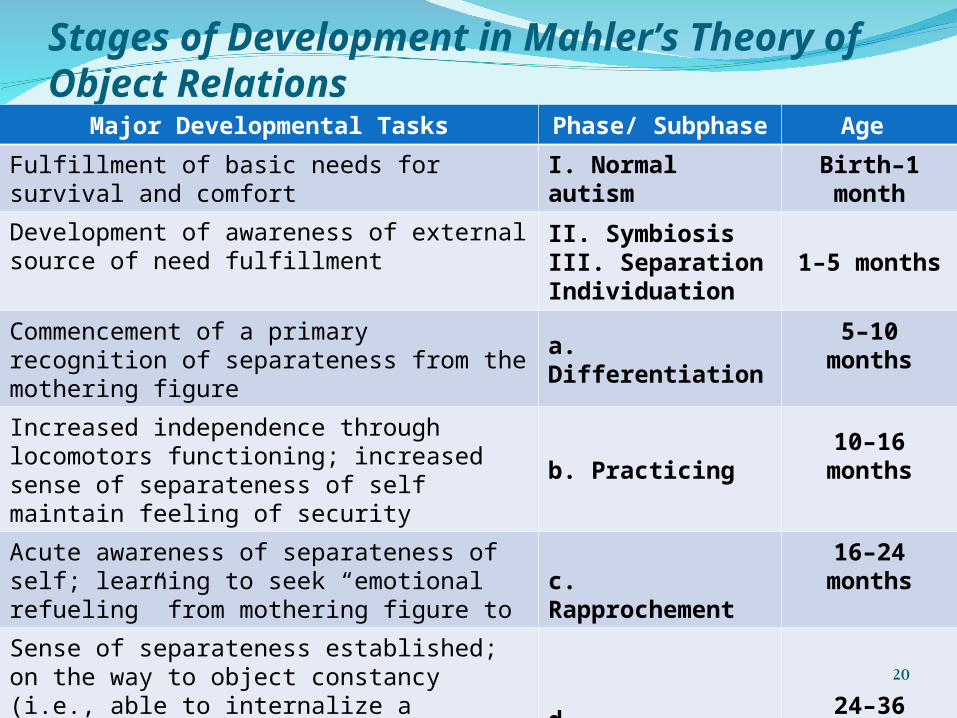
Birth–1 monthI. Normal autismFulfillment of basic needs for survival and comfort
1–5 monthsII. SymbiosisIII. Separation Individuation
Development of awareness of external source of need fulfillment
5–10 monthsa. Differentiation
Commencement of a primary recognition of separateness from the mothering figure
10–16 monthsb. Practicing
Increased independence through locomotors functioning; increased sense of separateness of self maintain feeling of security
16–24 monthsc. Rapprochement
Acute awareness of separateness of self; learning to seek “emotional refueling” from mothering figure to
24–36 monthsd. Consolidation
Sense of separateness established; on the way to object constancy (i.e., able to internalize a sustained image of loved object/person when it is out of sight); resolution of separation anxiety
20
A NURSING MODEL - HILDEGARD E. PEPLAUPeplau (1991) applied interpersonal theory to nursing practice
and, most specifically, to nurse–client relationship development. She established a framework for psychodynamic nursing, the interpersonal involvement of the nurse with a client in a given nursing situation.
Peplau correlated the stages of personality development in childhood to stages through which clients advance during the progression of an illness. She also viewed these interpersonal experiences as learning situations for nurses to facilitate forward movement in the development of personality. She believed that when there is fulfillment of psychological tasks associated with the nurse–client relationship, the personalities of both can be strengthened.
21
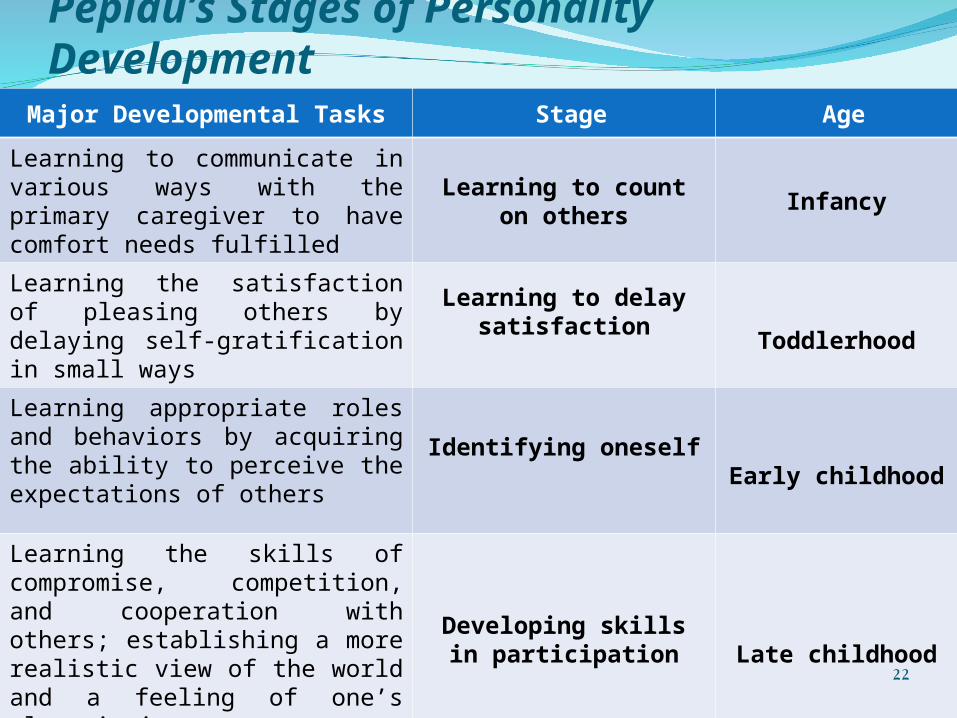
Peplau’s Stages of Personality DevelopmentAge Stage Major Developmental Tasks
InfancyLearning to count on
others
Learning to communicate in various ways with the primary caregiver to have comfort needs fulfilled
Toddlerhood
Learning to delay satisfaction
Learning the satisfaction of pleasing others by delaying self-gratification in small ways
Early childhoodIdentifying oneself
Learning appropriate roles and behaviors by acquiring the ability to perceive the expectations of others
Late childhoodDeveloping skills in
participation
Learning the skills of compromise, competition, and cooperation with others; establishing a more realistic view of the world and a feeling of one’s place in it
22
Beck’s Cognitive Theory
Early observation of negative content of depressed people’s dreams
Beck's background was in psychoanalytic psychiatry. He developed theories and inventories instrumental to
cognitive therapy research and practice, particularly for the treatment of depression through challenging faulty attributions or unhelpful thinking patterns.
23
Beck’s TheoryDepressed people have a negative view of:ThemselvesThe worldThe futureDepressed people have negative schemas or frames
of reference through which they interpret all events and experiences .
Schemas in psychology and cognitive science, is a mental structure that represents some aspect of the world.
24
Beck’s Cognitive Therapy: Sessions
Identify and changing maladaptive thoughtsFirst sessions: therapist explains cognitive theory of
emotional disorders (negative cognitions contribute to distress).
Middle Sessions: Client is taught to identify, evaluate and replace negative automatic thoughts were more positive cognitions.
Therapist is a collaborator (fellow scientists in therapy)Final Sessions: solidify gains, focus on prevention of
recurrence.
25
Behavioral Component
1. Behavioral coping strategies .
2. Problem solving skills
3. Assertiveness training
26
Cognitive Behavioral Therapy:Efficacy/Effectiveness (old question)
Identified as a well established treatment for the treatment of unipolar depression.
As effective (and sometimes more effective than) alternate forms of treatment for depression including antidepressant medication.
However (despite focus on prevention of relapse) 2/3 of patients who receive cognitive therapy have another episode of depression within two years.
27
CBT Effective for which type of patients (new question)
Outcome not predicted by level of intelligence
1.Patient with lower levels of dysfunctional thinking benefit the most (paradoxically)
2.Interpersonally avoidant patients do better in CBT (rather than interpersonal psychotherapy)
3.Patients with more obsessional styles do better in Interpersonal Psychotherapy
28
CBT: Effective for Which Disorders?
Empirically supported treatment for :
1.Depression
2.Generalized anxiety disorder
3.Obsessive compulsive disorder
4.Panic disorder
29
Recommended