July
2016
CMANA
Haiti Missionparticipant testimonials page 7
Connection
NEWWEBSITE
CONFERENCE
2016Save the Date
NEWBOARD

edited and designed by Ramzy Lotfi
CMANA
CMANA
02 04 05
07
2216
22
tableof con -tents
02 President's Message
04 Board Introduction
05 New Website
07 Haiti MissionTestimonials
11 Upcoming Missions
22 Contributors wanted
22 Conference Save-the-Date
44 Michael DrOld Bethpage, New York 11804-1524
www.cmanamerica.org
cmanamerica.org/
13
06 6 Tips for Picking aSpeicalty
12 Med SchoolConfessionals
13 5 Deficiencies HealthProfessionals ShouldLook Out For
16 What to Wear: Professional Attire vs.Business Casual
20 Finding Balance inDaily Life
writerswanted
MICHAEL KARASS, MDNATIONAL PRESIDENT
'16 '17
JULY 2016CMANA
ealing was at the heart of Christ's ministry.In the 2nd century AD, Polycarp, Bishop ofSmyrna, identified care of the sick as aprincipal responsibility of church elders. "EarlyChristians nursed the sick to emulate thehealing ministry of Jesus, to express their faithin the ongoing healing power of Christ; and todistinguish Christian heroism in the face ofsickness and death from pagan fear."(Amanda Potterfield).
As Paul Offit, M.D., Chief of Infectious Diseasesand Director of the Vaccine Education Centerat the Children's Hospital of Philadelphia (andself proclaimed agnostic) writes "By the thirdcentury, no single entity had advancedhealing more than monasteries, which treatedthe sick, disable, and elderly..Christianmonasteries which put inpatient andoutpatient care into a single building gavebirth to the modern day hospital. By theMiddle Ages, Christians had created morehospitals that any other religious or secularentity"
H
2
Now in the 21st century, as young Christianhealthcare students, we are called to build onwhat we have received.
This year we are blessed with many newbeginnings starting with a new board andwebsite. We ended last year with a successfulconference with more than 150 attendeesfrom all around the USA and Canada whocame together in a spirit of fellowship andservice todig deeper into Spirituality and Healthcare.We were honored to have a slew of guestspeakers including our keynote speaker, Dr.Harold Koening, Director for the Center ofSpirituality, Theology, and Health at DukeUniversity, Dr. George Tadros, interventionalcardiologist and director of missions atCMANA, and Fr. Mena Attwa, who was calledto serve in Africa for 11 years. We are alsoactively building a strong student chapter inCanada and are in the process of organizingour annual conference which will be held inOrlando, Florida from December 16-19th. Wehope to be a light in a city that has recentlyseen a lot of darkness.

IT IS FORGOTTEN THAT MEDICINE OWNS ITSGREATEST DEBT NOT TO HIPPOCRATES, BUT TOJESUS. IT WAS THE HUMBLE GALILEAN WHOMORE THAN ANY OTHER FIGURE IN HISTORYBEQUEATHED TO THE HEALING ARTS ITS
ESSENTIAL MEANING AND SPIRIT. JESUS BRINGSTO METHODS AND CODES THE CORRECTIVELOVE WITHOUT WHICH TRUE HEALING IS
RARELY ACTUALLY POSSIBLE. THE SPIRITUAL"FATHER OF MEDICINE" WAS NOT HIPPOCRATESOF THE ISLAND OF COS, BUT JESUS OF THE
TOWN OF NAZARETH!
DR. JACK PROVONOSHA, PROFESSOR OF PHILOSOPHY ANDRELIGION AT LOMA LINDA UNIVERSITY
3
We are also excited to be coming out with this studentdriven newsletter; as a place where we can share thework God is doing, through personal experiences inour day to day lives, whether in a major hospital inNYC or in a rural clinic in Santa Cruz, Bolivia. We willalso be sharing articles to help us balance our variousroles as Christian young leaders in healthcare and wewelcome your submissions. We are also thrilled to bepartnering with Coptic Orphans through the Serve toLearn program; allowing healthcare students at thegraduate and undergraduate level to be involved inhealth education while serving our brothers andsisters in Egypt. We look forward to serving with you,through local and international service events, as wegrow into one body in Christ.
PRESIDENT:
MICHAEL KARASS
REGIONAL VICE PRESIDENTS:
MARK RAMZY (NORTH REGION)RAMZY LOTFI (SOUTH REGION)
SECRETARIES:
AMYE FARAGAMEER HALIM
ADDITIONAL BOARD MEMBERS:
JOHN SIDHOMDEMYANA AZEROLIVIA BASSILY MARIAN AWAD
JACQUELINE YOUSSEF
4
YOUNG PROFESSIONAL
STUDENT BOARD
iNTRODUCING YOUR CMANA NATIONAL

CMANAMERICA.ORG
5
NEWWEBSITE DESIGN
CHECK IT OUT AT

Some people walk in to medical school knowing
they’re going to be an orthopedic surgeon and
never waver in their calling. For others,
including myself, each new rotation brings more
to love and an even more difficult decision. Here
are some tips to help you search for the right
specialty!
Tips:
1. Seek feedback from those who know you best,
including yourself. Ask which rotations you
seemed happiest on, which rotation had patients
that affected you most, and which days were the
easiest to wake up for work. Ask mentors you
are comfortable with what they see as your
strengths/weaknesses and which specialties
compliment them.
2. Consider the patient population you want to
work with. For example, if you hate working
with old people, family medicine and
ophthalmology are probably not going to be good
fits for you.
TIPS FOR PICKING ASPECIALTY6
By Amye Farag , M.D .In te rn a t Phoen ix Chi ld ren 's Hosp i ta l
3. Lifestyle. While you shouldn’t do a specialty for
the money (or the lifestyle), it is definitely something
to consider. If you expect to have regular 9-5 work
hours, surgery probably won’t be in your future. If
you hate evening shifts, emergency medicine
probably won’t work for you either. Each specialty
has its pros and cons, but some may be incompatible
with your post-residency life- choose wisely.
4. Ask as many questions of residents and attendings
about their jobs and how they picked them as you
can. They probably have more insight into how their
field will be changing in the future and you’ll want
to know this to make an informed decision.
5. Make a list of pros and cons for the specialties
you’re deciding between. You may find a common
theme- ie. Patient population, procedure vs thinking
specialty, clinic vs hospital setting. This can help you
narrow it down.
6. Pray God will open doors you never imagined
would be possible and shut the ones you don’t belong
in.
6
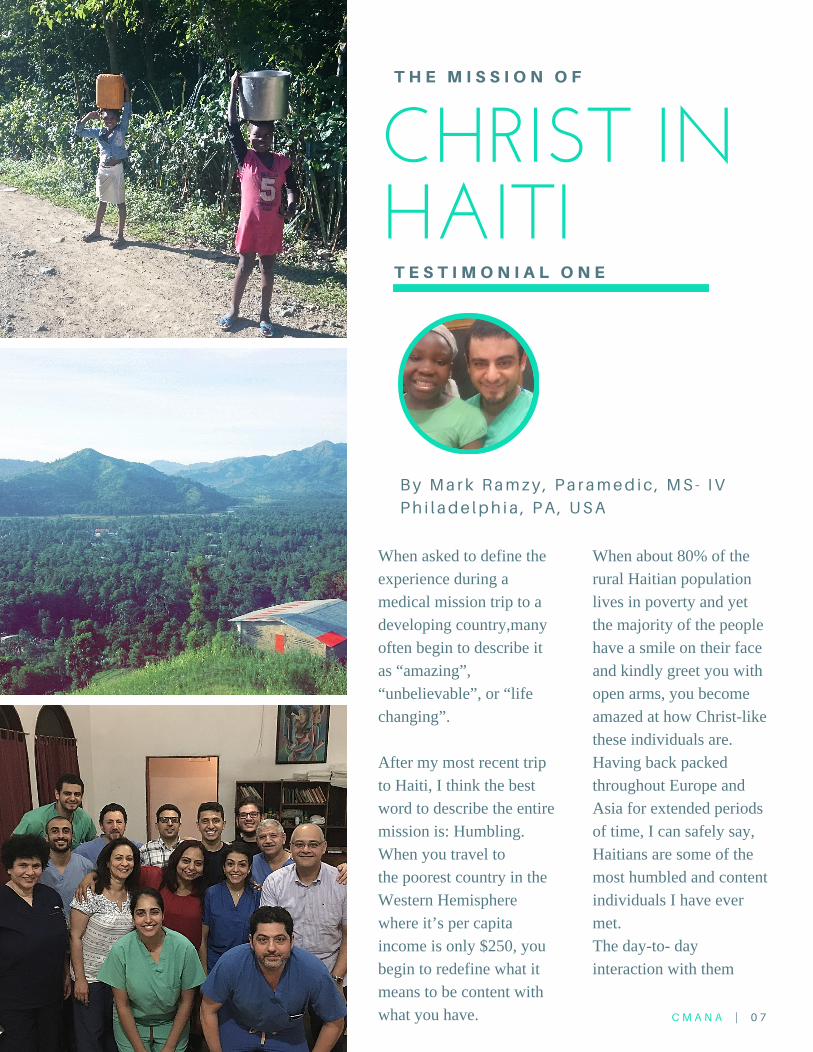
CHRIST INHAITI
By Mark Ramzy , Pa ramed ic , MS - I VPh i l ade lph i a , PA , USA
T H E M I S S I O N O F
When asked to define theexperience during amedical mission trip to adeveloping country,manyoften begin to describe itas “amazing”,“unbelievable”, or “lifechanging”.
After my most recent tripto Haiti, I think the bestword to describe the entiremission is: Humbling.When you travel tothe poorest country in theWestern Hemispherewhere it’s per capitaincome is only $250, youbegin to redefine what itmeans to be content withwhat you have.
When about 80% of therural Haitian populationlives in poverty and yetthe majority of the peoplehave a smile on their faceand kindly greet you withopen arms, you becomeamazed at how Christ-likethese individuals are.Having back packedthroughout Europe andAsia for extended periodsof time, I can safely say,Haitians are some of themost humbled and contentindividuals I have evermet.The day-to- dayinteraction with them
C M A N A | 0 7
T E S T I M O N I A L O N E
A NEW COMMANDMENT I GIVE TO YOU,LOVE ONE ANOTHER. AS I HAVE LOVED
YOU, SO ALSO YOU MUST
LOVE ONE ANOTHER. BY THIS ALL MENWILL KNOW THAT YOU ARE MY
DISCIPLES, IF YOU LOVE ONE ANOTHER .
JOHN13:35
8
really helped me lookinward to my ownpersonal qualities andassess whether or notevery action and decisionI make is moving myselfcloser or away to Christ.Despite not knowing thelanguage and many ofthem not speakingEnglish, it was apparentthat our non-verbal
behavior communicatedsomething veryuniversally understood:Love.
For those who have neverbeen on a CMANAmedical mission trip,wherever you goremember Jesus’teaching: “A newcommandment I give to
you, Love one another.As I have loved you, soalso you mustlove one another. By thisall men will know thatyou are My disciples, ifyou love one another”(John 13:35).As an avidworld traveler (20+countries and counting)trust me when I say: InHaiti, regardless of their
poverty and the numberof possessions they don’thave, I truly felt loved byeveryone I treated.
And for those of you whoare about to go on a trip(especially if it’s yourfirst), prepare to encounter
Christ in some of the mostamazing people you’llever meet.

CHRIST INHAITI
By Amee r JosephA lbe r t E ins te in Co l l ege o f Med ic ineC las s o f 2020
T H E M I S S I O N O F
One of the things thatstruck me the most uponarrival in Haiti was theextreme level of povertythat the people lived in. Ihad witnessed povertybefore, but never to thisextent. I started to questionthe notions of justice andfairness, and wonderedhow God could allow Hischildren to live in thesedismal conditions. By theend of the mission Irealized that these peoplewere very rich in theirsimplicity, kindness, andcontentment, and that Iwas the poor one.
This realization made mequestion the purpose ofmy daily endeavors andthe goals that I strive for;if my whole life revolveson chasing goals in orderto become content whilethese people have nothingand yet are content, thenwhat am I doing with mylife? I discovered that thekey to their contentment istheir reliance on God. Dueto their poverty, they don'thave any material orwealth to put their hope
C M A N A | 0 9
T E S T I M O N I A L T W O
BY THE END OF THEMISSION I REALIZED THATTHESE PEOPLE WERE VERYRICH IN THEIR SIMPLICITY,
KINDNESS, ANDCONTENTMENT, AND THATI WAS THE POOR ONE.
10
in; they have nothing orno one that they can relyon besides Him. Myproblem is that I rely onthe blessings as opposedto the One who hasprovided me with theblessings, only to realizethat I'm far from beingcontent. Overall theexperience was very eye-
opening and perspectivechanging, and I pray thatthe seed of missions thatwas planted in my heartduring this trip continuesto grow and multiply inmy life.

Bolivia: July 9 – 16Bolivia: August 20 – 27Egypt: November 5 – 12
REGISTER FOR OUR
UPCOMINGMISSIONS
NEXT MISSIONS
Where will Christ
take you NEXT?
11
The first semester of medical school was a very personal
experience for me, as it is for many students. It was filled
with an unimaginable number of highs and lows. As the
semester progressed and the workload got heavier, the
number of lows started to surpass and overshadow the
highs. I couldn’t figure out why I had suddenly started to
drown. Undergrad wasn’t easy, but I never felt the weight
of anxiety as I did in my first semester as a medical
student. Sometimes it was hard to breathe, sometimes
mom got an earful and/or tears over the phone, and
sometimes I got into bed feeling miserable and alone.
It felt isolating. Was I the only one struggling? Was I the
only one that was so lost? Suddenly, I was surrounded by
brilliant people with inspirational life stories, in addition to
incredible talent and skill. That was it. They call it imposter
syndrome. Why was I in medical school? How and why did
they choose me? I was obviously nothing compared to my
peers.
Everyone says, “No worries, everyone feels this way in
their first year!” Their words of comfort echoed in my head
and failed to fill the emptiness I felt. When I finally
recognized that I needed something more, I reached out to
my classmates. I hesitated though, I didn’t want them to
see or know that I was struggling.
Most people start medical school with a certain level of
pride. Proud that we’ve gotten this far, proud that our
parents are proud, and proud of the hard work we’ve done
to earn that spot next to our peers. It was a
humbling experience to recognize that I was struggling. It
was humbling to bring myself to talk to my classmates and
verbalize the emptiness I felt for months. Nothing made
me happier than that I did.
I took a leap of faith and entrusted my struggles to
individuals that I’m now proud to call friends. I didn’t feel
so alone anymore; they brought me back from the dark
hole I had hidden away in. Quiet prayers and words of
support replaced thoughts of inadequacy. I realized that I
was trying to make the journey without faith, which had
fallen by the wayside—along with my sense of self—as
the classes intensified.
Faith was something I grew up with. It wasn’t something I
cherished because it was old habit. Church on Sunday, a
few services during the week, youth meetings, rinse and
repeat. It wasn’t until medical school that I recognized the
treasure it actually was. It became my anchor, along with
the people that brought me back from the endless loop of
negative, selfdeprecating thoughts.
To the students who are struggling everyday, to those who
have lost sight of their goal, try and remember that
someone is out there who will listen to you. You are loved
by someone, no matter how much you feel that you’re
alone. Never think your problems are unimportant, but
always remember that your God is bigger.
“But may the God of all grace, who called us to His eternal
glory by Christ Jesus, after you have suffered a while,
perfect, establish, strengthen, and settle you. To Him be
the glory and dominion forever. Amen.” I Peter 5:1011
“I have taught you in the way of wisdom; I have led you in
the right paths. When you walk, your steps will not be
hindered, and when you run, you will not stumble.”
Proverbs 4:1112
Without An Anchor
Anonymous S tuden tSubmis s ion
MED SCHOOL CONFESSIONALS
12

By Saha ra So l imanRDN /LN , CLC
Iron deficiency could be for a number of reasons. Iron deficiency anemia is characterized by fatigue, dark circle under and around the eyes, feeling cold, and spoon shaped nails where the nails are concave and the edges are raised. Most people affected are woman of menstrual age, pregnant/post-partum, and children. Too muchcalcium, sweets beverages, and cruciferous vegetables(broccoli, cauliflower, cabbage) can decrease theabsorption of dietary iron.
5NUTRITIONDEFICIENCIES HEALTH PROFESSIONALS SHOULD LOOK FOR
Most American’s aren’t going to vitamin deficient regularly. There are some reasons withillness/disease, new growth, malabsorption, or even addiction can affect a person’s vitaminor mineral status. Here are 5 nutrients to be on the lookout for in the medical setting.cabbage) can decrease the absorption of dietary iron.
1 Fe 13
14
Thiamine B1 deficiency, is common among alcoholics, severe anorexics, and people in developing countries living mainly on white rice or refined carbohydrates. Treatment is adding thiamine back in the diet. Clinical manifestations present themselves as irritability, fatigue, Anorexia, abdominal irritability, dry beriberi- peripheral neurological deficits occurring bilaterally- burning in the feet, muscle cramps in the calves, Wernicke-korsakoff with alcoholics- psychomotor slowing, paralysis of the eye muscles, impaired balance,coma, death, wet beriberi-myocardial disease with vasodilation,tachycardia, warm skin, sweating, lactic acidosis, later heartfailure. Physically characterized by a round, swollen moon face,foot drop, weight loss, muscle weighting, jerky eye movementsand a staggering gait.
Vitamin A is a fat soluble vitamin that interacts with the eyes, skin and vision when too low. Decreased night vision is the first manifestation to happen, followed by the keratinization of the eyes (conjunctiva and cornea) and bitot spots. Dietary vitamin A is high in green leafy vegetables, colorfulorange and yellow fruits (color due to beta carotene),liver, egg yolk, fish liver oils.
23
AB1
15
Niacin B3 deficiency (pellagra) can be seen inalcoholism. The clinical manifestations include a localized pigmented rash that are usually bilaterally symmetrical, diarrhea, mucous membranes- easily seen in the mouth- become red, swollen and increased saliva production, anorexia and neurological deficits eventually to a cognitive decline. Very deficientpatients can show change in personalities. Foodsrich in tryptophan, dairy products, are metabolizedto niacin which can be used PO to increase levels.
Vitamin D deficiency has become more common and can affect anyone who is not exposed to enough sunlight. Depending on skin melanin, the patient needs direct sunlight for at least 20 minutes. The patient needs to be uncovered, no sun block and outside. In children, the clinical manifestation is called rickets causing bowing of the legs leading to delay in walking. Depending on how young the child is, the cranial bones are soft. In adults,it is called osteomalacia. It can cause muscle pain, weaknessand bone pain. Tentany, from low calcium as these twonutrients work together, can cause tingling of the lips, tongueand fingers. Milk has Vitamin D added in or supplements ofVitamin D3 will increase levels. This is a fat soluble vitamin.
45
B3
DReferenceshttp://www.nutrition411.com/content/vitamin-and-mineral-deficiencies-physical-assessmenthttp://www.merckmanuals.com/professional

What to Wear
Being in a professional setting often brings up the
question as to what clothes are professional and what
are not. Here are some tips on professional attire
versus casual professional attire!
Suits: •Jacket sleeve length should be 1/2 an in
under the wrist
•Neutral Colors: grey, navy, black, brown
Pants: •Should fall just at the knees when standing
If you have to tug on the skirt when sitting down,
they’re too tight!
•Avoid skirts with high slits
Shoes: •Avoid opentoed shoes, sandals, or shoes
with your heel showing
•No stilettos
•Use heels with a heel that’s 12 inches high
•Wear trouser socks or neutral hosiery
Shirts: •Use light, neutral colors; less patterns
•No cleavage ladies!
•Buttonups are widely acceptable
HEELS OR FLATS? TIE OR BOWTIE?
By Justine M. LatifPharm. D Candidate Class of 2017
Florida A&M University
Professional Attire
The Ladies
16
Suits: •Should be solid or have subtle pinstripes
•Jacket should be buttoned when standing and
unbuttoned when sitting
•Threepiece suites are unnecessary; this isn’t a
wedding
•Neutral Colors: grey, navy, black, brown
Pants: •Jackets and pants have to match
•Have your pants tailored to an appropriate length
•Tight jackets and pants are not recommended;
we’ll see your guns later
Tie: •Subtle colors are best
•Tie should reach your belt
Shoes: •Polished, leather shoes
•Should match belt color
Shirts: •Use light, neutral colors; less patterns
•Long sleeve shirts
•Sleeve of shirt should come out 1/2 an inch out
under the suit jacket sleeve
p. 16
Professional AttireThe Gents
17
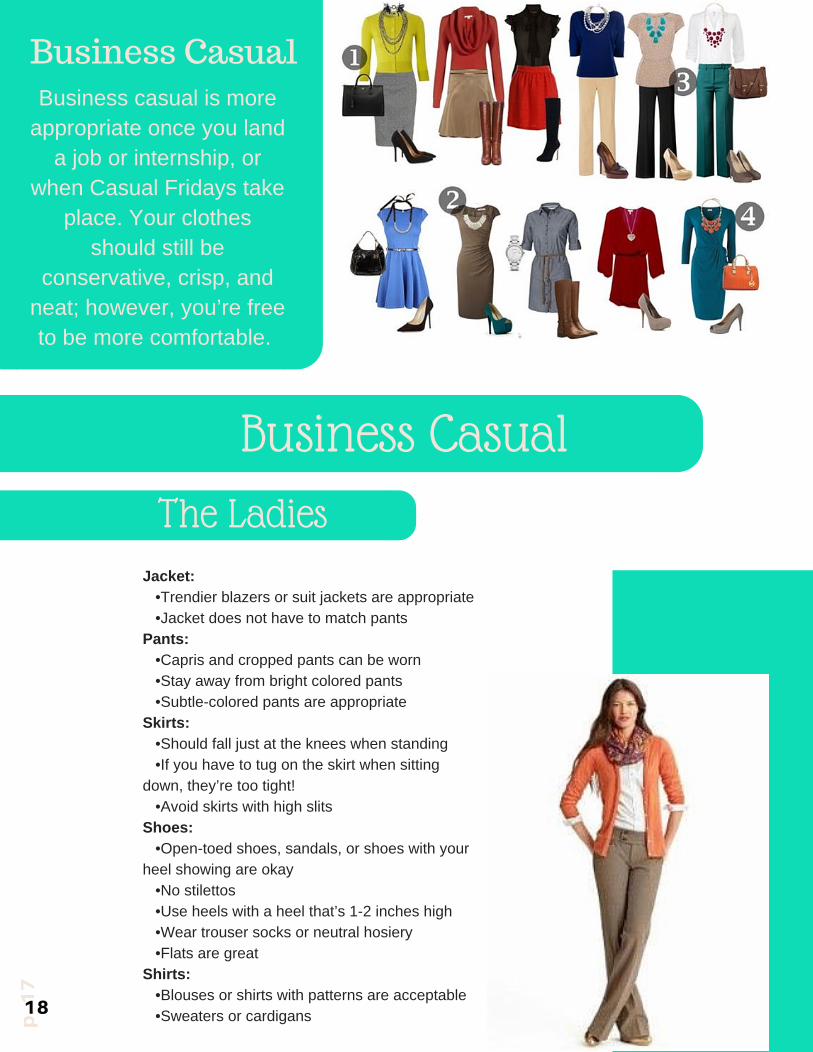
Business CasualBusiness casual is moreappropriate once you landa job or internship, or
when Casual Fridays takeplace. Your clothes
should still beconservative, crisp, andneat; however, you’re freeto be more comfortable.
Jacket: •Trendier blazers or suit jackets are appropriate
•Jacket does not have to match pants
Pants: •Capris and cropped pants can be worn
•Stay away from bright colored pants
•Subtlecolored pants are appropriate
Skirts: •Should fall just at the knees when standing
•If you have to tug on the skirt when sitting
down, they’re too tight!
•Avoid skirts with high slits
Shoes: •Opentoed shoes, sandals, or shoes with your
heel showing are okay
•No stilettos
•Use heels with a heel that’s 12 inches high
•Wear trouser socks or neutral hosiery
•Flats are great
Shirts: •Blouses or shirts with patterns are acceptable
•Sweaters or cardigans p. 17
Business Casual
The Ladies
18
p. 18
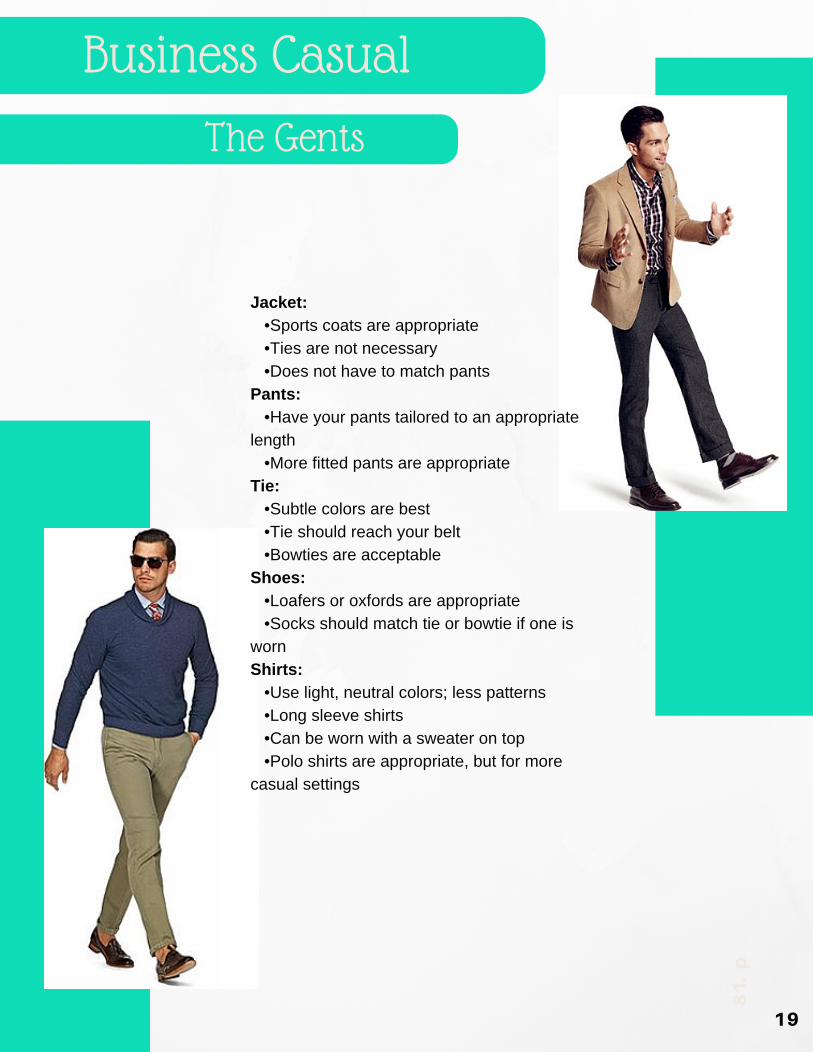
Jacket: •Sports coats are appropriate
•Ties are not necessary
•Does not have to match pants
Pants: •Have your pants tailored to an appropriate
length
•More fitted pants are appropriate
Tie: •Subtle colors are best
•Tie should reach your belt
•Bowties are acceptable
Shoes: •Loafers or oxfords are appropriate
•Socks should match tie or bowtie if one is
worn
Shirts: •Use light, neutral colors; less patterns
•Long sleeve shirts
•Can be worn with a sweater on top
•Polo shirts are appropriate, but for more
casual settings
Business Casual
The Gents
19
FINDINGBALANCE INDAILY LIFEBy John -Wi l l i am S idhomJohns Hopk ins Schoo l o f Med ic ine
I’ve heard there are two ‘types’ of people when it comes tothe time of day they best operate. The first type are called‘early birds.’ These individuals get up easily in the morningand are most productive early in the day. They have noproblem getting up and starting their day with full force. Thesecond type are called ‘night owls.’ These people seem toreach their full productive potential in the late hours of thenight. Conventional wisdom tells us that early birds tend to bereally good at making lists and accomplishing goals whilenight owls are the more creative type; instead of making a listof objectives to complete, they go with the flow untilsomething good comes from their work.To be quite honest, I’ve never been a morning person. Allthrough college, I found my most productive hours to be lateat night. It was as if it took the whole day for my brain towake up; but once it turned on, I found my creative juicesflowing and my best work would follow. As an engineeringstudent at the time, much of my work was either problemsolving or design. Tapping into the creative potential the nighthad to offer always seemed to result in my best work. Theirony is I ended up eventually choosing a career where notonly being a morning person is helpful but practicallynecessary. As a physician in training, days can start as earlyas 4 in the morning with shifts well over 12 hours in a day.Going through my surgery rotation in medical schooldefinitely highlighted for me the difficulty I had in workingthat early in the morning. So what is someone like me to doentering a profession where I’ll be called to be fullyfunctional in the wee hours of the morning?
N O M A D I C | 2 420
A few months ago, under the influence ofseveral people, I began to think about takingcontrol of my mornings. Even though I felt Iwas a ‘night owl,’ I began to see the value ofbecoming an ‘early bird.’ If not for just mycareer, I began to learn about all the benefits ofstarting my morning early and with purpose. Ideveloped a morning ritual as a way to set thetone for the rest of my day. I made a schedulefor myself that I began to follow each morningto the minute. I set aside time in the morning toexercise, eat a filling and healthy breakfast,pray, read the Bible, and take a few minutes towrite in a gratitude journal before I got off tostart the rest of my day. I realized being amorning person was not just a matter ofpreference but a very effective way to make themost of my entire day. Instead of rushing out ofmy apartment in the morning feeling like acomplete mental train wreck, I took an extra 30-45 minutes in the morning to gather myself andprepare for the upcoming day. As a result, I wasable to establish an inner peace and calmbefore tackling the challenges that were aheadof me. By making my morning ritual a routine,I’ve been able to build habits that have hadresounding and disruptive effects in all otheraspects of my life. In the word of CharlesDuhigg, the author of the book The Power ofHabit, “Some habits matter more than others inremaking lives. These are ‘keystone habits,’and they can influence how people work, eat,play, live, spend, and communicate. Keystonehabits start a process that, over time, transformseverything.”But what about my creative side? Pursuing acareer in medicine often calls for life ofregimen and routine: the essence of medicinecalls it to be ‘practiced’ until that routine can beexecuted to the highest proficiency to providereliable and good care of patients. There reallyis little room for creativity in the practice ofmedicine. After all, would you want yourphysician to be creatively experimenting withyour next surgery? Not at all. You want yourphysician to be doing for you what he/she hasdone for countless of patients before you; somuch so they can do it in their sleep. As aresult, the practice of medicine can trulybecome boring as one perfects their craft. Tomaintain an outlet for my creative side, I beganto pick up music more during my graduateyears. I learned how to play the guitar andbegan to write/produce music as a means tomaintain my sanity outside of medicine. After along day where my mind has been whirlingfrom work, it’s relaxing and relieving to let mymind go in singing, playing, and writing music.
While a good conclusion is an importantingredient for newspaper articles, theimmediacy of a deadline environment meansthat copy editing often takes the form ofdeleting everything past an arbitrary point inthe story corresponding to the dictates ofavailable space on a page.
Therefore, newspaper reporters are trained towrite in inverted pyramid style, with all themost important information in the firstparagraph or two. If the less vital details arepushed towards the end of the story, then thepotentially destructive impact of draconiancopy editing will be minimized.
At one point, I thought a life of routine/regimenand one of creativity/art were at odds with eachother. Either you were someone who could knockout a to-do list before 9 am easily or you were thetype of person who would spend countless hourswithout a real goal in mind in order to freelyexpress their creative side. It turns out, for me,both were invaluable to maintain balance in mylife: they just occupied different parts of my day.“To everything there is a season, a time for everypurpose under heaven” (Eccles. 3:1). A morningroutine sets the tempo for my day and musicalexpression ends my night on the perfectunwinding note.A news article discusses current or recent newsof either general interest (i.e. daily newspapers)or of a specific topic (i.e. political or trade newsmagazines, club newsletters, or technology newswebsites).
A news article can include accounts ofeyewitnesses to the happening event. It cancontain photographs, accounts, statistics, graphs,recollections, interviews, polls, debates on thetopic, etc. Headlines can be used to focus thereader’s attention on a particular (or main) part ofthe article. The writer can also give facts anddetailed information following answers to generalquestions like who, what, when, where, why andhow.
21

If you are interested in submittingan article for our publication
please contact us [email protected]
22
-Contributors Wanted-
Recommended