6/7/2018
1
Training presented by:
Funded by:
Mental Health Act 2016
Clinician TrainingAdvance Health Directive
for Mental Health (AHD-MH)
AHD-MH training for Queensland Health
- health professionals & mental health services
NB: State-wide
version 31 May 2018
Welcome & Introductions
Welcome
Acknowledgement of Country
About “Advance Health Directives for
Mental Health (QLD, Australia)”
YouTube Video Resource [DURATION: 6min 41sec]
� Access via ADA Website:
https://adaaustralia.com.au/clinicians/
6/7/2018
2
Focus
� What is an Advance Health Directive for Mental Health (AHD-MH)
� Why complete
� Who can complete
� When it starts
� How to complete
MHA2016: Strengthening rights using least restrictive options
� Engage, equip and empower clinicians
� Identify if a person has an AHD-MH
� Assist a person to make or update an AHD-MH
� Storing, Review, Updating & Revoking
Clinician’s role
� Depending on your role, you may be responsible for:
� Checking the state-wide system (CIMHA/The Viewer)
� Following an AHD-MH to ensure less restrictive way
� Assisting a person to make an AHD-MH
� Liaising with a person’s GP, Allied Health Professionals, Attorney/s etc.
� Encouraging a person to make, review and/or update AHD-MH
� Maximising patient autonomy is everyone’s responsibility!
� Achieve the principles & objects of MHA2016
� Read & adhere to
� Chief Psychiatrist’s policy
� Guide to Advance Health Directives, Enduring Powers of Attorney, Guardians and Administrators (attachment to QH CPP Policy for AHD & Less Restrictive Way)
Patient autonomy is the ideal
6/7/2018
3
Chief Psychiatrist Policy: Advance Health Directives and ‘Less Restrictive Way’ of Treatment (March 2017)
https://www.health.qld.gov.au/__data/assets/pdf_file/0029/465176/cpp-advance-directives.pdf
� Policy – Section 5
� 5.1: Obligations of health practitioners
� 5.2: Requirement to consider less restrictive way of treatment
� 5.2.1: Presumption of Capacity; Principles of supported decision-making; rights to consent
� 5.2.2: Minors
� 5.2.3: Must take steps to identify if AHD exists; and/or appointed an attorney, or has guardian
� 5.2.4: Statutory Health Attorney (SHA)
� 5.2.5: Must document in record if being treated by AHD; or under consent of attorney / guardian
� 5.2.6: If less restrictive way becomes available at a future time
� 5.3: Use of physical restraint in providing treatment and care
� 5.4: Treatment as an inpatient
� 5.5: When requirement to treat in a less restrictive way does not apply
� 5.6: Ongoing lack of capacity
� 5.7: Making an AHD for future health care
� 5.8: Urgent health care
MHA2016 commenced 5 March 2017
� Objectives to be achieved in a way that:
� Safeguards the rights of persons
� Is the least restrictive of the rights and liberties of
a person who has a MI, and
� Promotes the recovery of a person who has a MI,
and the person’s ability to live in the community,
without the need for involuntary treatment and care
Mental Health Act 2016 (Qld)
MHA2016 Part 2 Principles for administration of Act https://www.legislation.qld.gov.au/browse/inforce
Principle of ‘less
restrictive way’
6/7/2018
4
MHA2016: Principles for persons with MISection 5
� Same human rights
� Matters to be considered in making decisions
� Support persons
� Provision of support and information
� Achievement of maximum potential and self-reliance
� Acknowledgement of needs
� Aboriginal and Torres Strait Islanders
� Persons from culturally and linguistically diverse backgrounds
� Minors
� Maintenance of supportive relationships and community participation
� Importance of recovery-oriented services and reduction of stigma
� Provision of treatment and care
� Privacy and confidentiality
Principles that apply to
administration of MHA2016
Future choices & consent for when unwell
� Treatment and care
� Attorney/s
� Inpatient stay? Physical restraint?
� Eligible Doctor certification required
Access the form (print version or online version)
health.qld.gov.au/mental-health-act
Optional
in QLD
6/7/2018
5
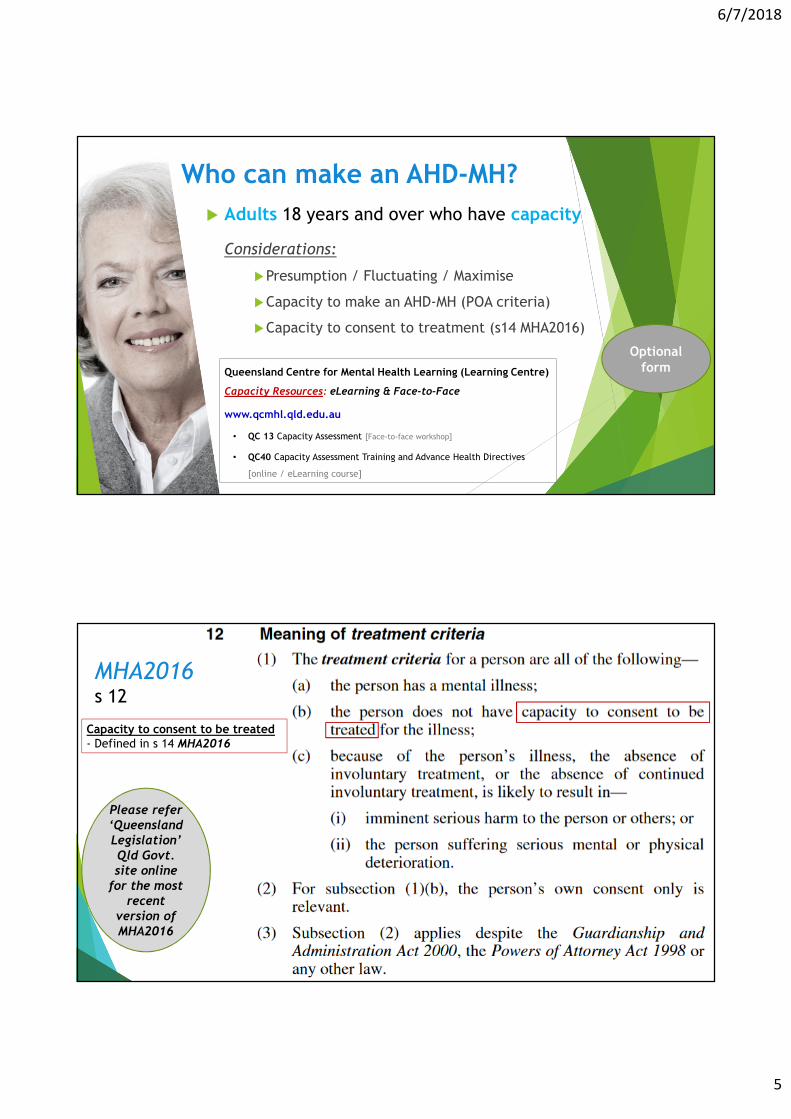
Who can make an AHD-MH?
� Adults 18 years and over who have capacity
Considerations:
�Presumption / Fluctuating / Maximise
�Capacity to make an AHD-MH (POA criteria)
�Capacity to consent to treatment (s14 MHA2016)
Queensland Centre for Mental Health Learning (Learning Centre)
Capacity Resources: eLearning & Face-to-Face
www.qcmhl.qld.edu.au
• QC 13 Capacity Assessment [Face-to-face workshop]
• QC40 Capacity Assessment Training and Advance Health Directives
[online / eLearning course]
Optional form
MHA2016s 12
Capacity to consent to be treated - Defined in s 14 MHA2016
Please refer ‘Queensland Legislation’ Qld Govt. site online
for the most recent
version of MHA2016
6/7/2018
6
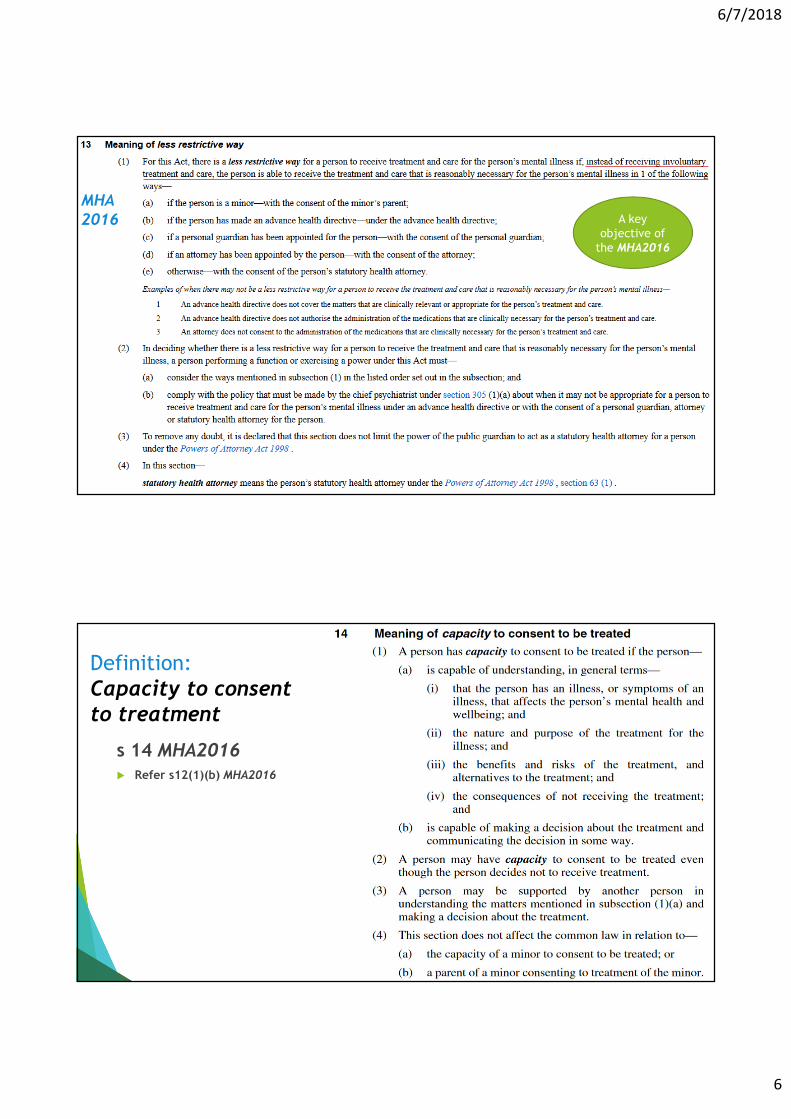
MHA2016 A key
objective of
the MHA2016
Definition:
Capacity to consent to treatment
s 14 MHA2016� Refer s12(1)(b) MHA2016
6/7/2018
7
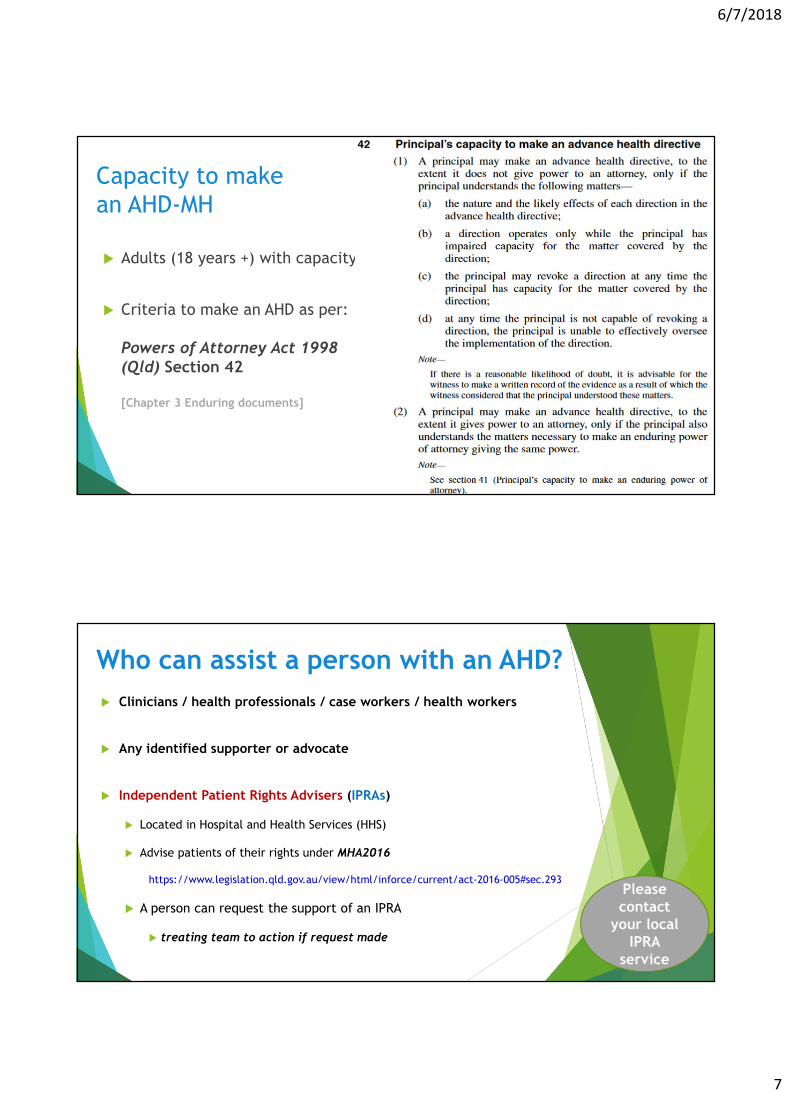
Capacity to make
an AHD-MH
� Adults (18 years +) with capacity
� Criteria to make an AHD as per:
Powers of Attorney Act 1998 (Qld) Section 42
[Chapter 3 Enduring documents]
Who can assist a person with an AHD?
� Clinicians / health professionals / case workers / health workers
� Any identified supporter or advocate
� Independent Patient Rights Advisers (IPRAs)
� Located in Hospital and Health Services (HHS)
� Advise patients of their rights under MHA2016
https://www.legislation.qld.gov.au/view/html/inforce/current/act-2016-005#sec.293
� A person can request the support of an IPRA
� treating team to action if request made
Please contact
your local IPRA
service
6/7/2018
8
MHA2016 Requirements: Role and Function of the IPRAs
IPRAs are required to work with the patient, and their nominated support persons, family, carers and
other support persons to:
Ensure that they are advised of their rights and responsibilities under the Act.
Help communicate the patient’s views, wishes and preferences about their treatment and care to
health practitioners.
Develop their understanding of the Mental Health Review Tribunal (MHRT) processes and their
rights at the hearing and organise a representative for the MHRT, including legal support or
advocacy, if requested.
Develop their understanding of the benefits of an AHD for mental health and the EPOA role for a
personal matter, if appropriate.
Additionally, IPRAs are required to:
Consult with authorised mental health practitioners, authorised doctors, administrators, and the
Chief Psychiatrist on the rights of patients under the Act, the Guardianship and Administration Act
2000 and the Powers of Attorney Act 1998.
Work cooperatively with any personal guardian or attorney to further the patient’s interests.
Work cooperatively with Community Visitors under the Public Guardian Act 2014.
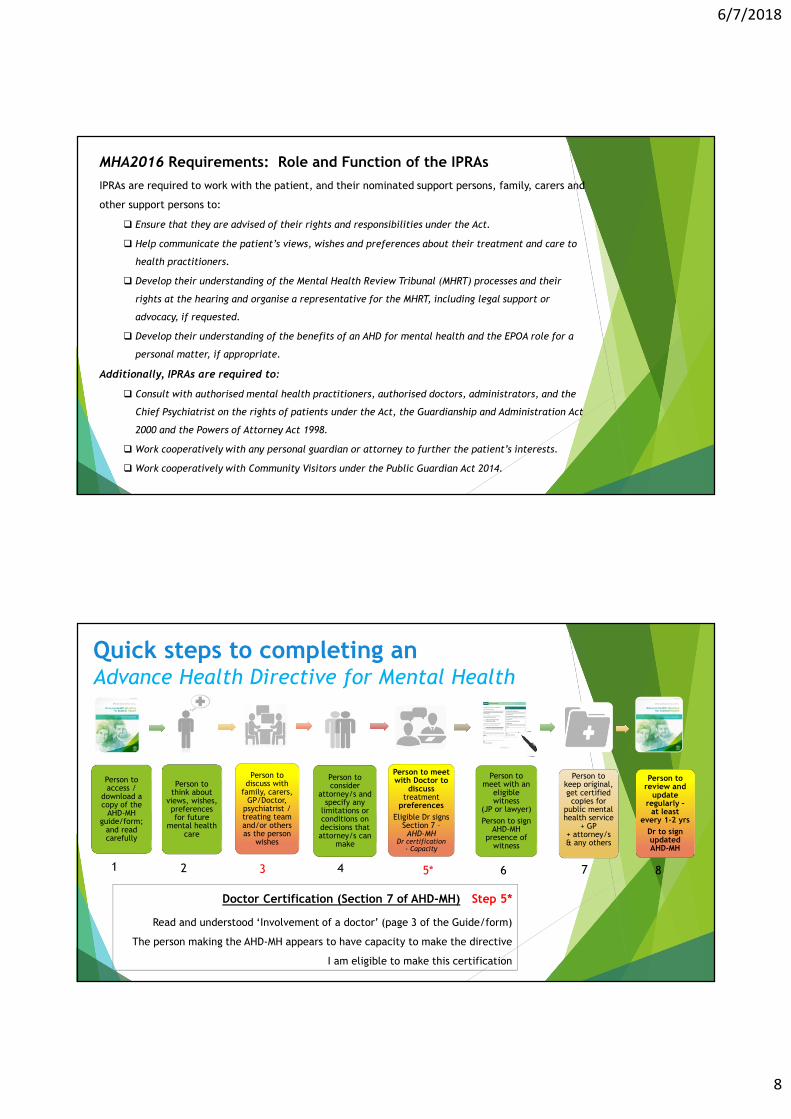
Person to access /
download a copy of the
AHD-MH guide/form;
and read carefully
Person to think about
views, wishes, preferences for future
mental health care
Person to discuss with
family, carers, GP/Doctor,
psychiatrist / treating team and/or others as the person
wishes
Person to consider
attorney/s and specify any
limitations or conditions on decisions that attorney/s can
make
Person to meet with Doctor to
discuss treatment
preferences
Eligible Dr signs Section 7 –AHD-MH
Dr certification - Capacity
Person to meet with an
eligible witness
(JP or lawyer)
Person to sign AHD-MH
presence of witness
Person to keep original, get certified copies for
public mental health service
+ GP+ attorney/s & any others
Person to review and
update regularly –
at least every 1-2 yrs
Dr to sign updated AHD-MH
Quick steps to completing an Advance Health Directive for Mental Health
Doctor Certification (Section 7 of AHD-MH) – Step 5*
Read and understood ‘Involvement of a doctor’ (page 3 of the Guide/form)
The person making the AHD-MH appears to have capacity to make the directive
I am eligible to make this certification
1 2 3 4 6 7 85*
6/7/2018
9
Best Practice TipsAdvance Health Directives for Mental Health
Conversation starters
� ENQUIRE
� Existing? Aware of?
� ENCOURAGE
[1] What treatment would you prefer if you were unwell and could not make decisions?
[2] Who would you like helping you with personal decisions such as mail, paying bills?
[3] Who would you like to make decisions for you if you can’t make them for yourself?
� Right person? Had discussion? Trusted to make and follow wishes?
� EXPLAIN
� Choice of language + detail based on mental health history
*Reference: Questions modified from Decision Assist (VIC) – Webinar (Jan 2017)

6/7/2018
10
Conversation tips
� Have you done an AHD before?
� Do you know an AHD can help you have your say in future care if you were unwell?
� What has worked well in the past?
� What treatments/medications did or did not work?
� What do you want treatment and care to look like?
� What past experiences do you want to avoid in the future?
� If you were unwell, would you agree to a hospital stay for you own safety?
� Who would you like supporting you in a crisis? Anyone you do not want to help?
� What arrangements would you need to make to keep everything going at home?
(e.g. mail, bills, pets, kids, plants, work, emails)
� What other health professionals need to know you are unwell?
� Do you want to make changes to your AHD?
Key considerations …
� Episodic nature of MI / fluctuating capacity
� Impact of general medical health issues
� MI history
� Risks & patterns of behaviour
� Past presentations good indicator for future presentations
� Respecting choices & treating in the less restrictive way (when possible)
� Involving support person/s
� Transcultural mental health
� RANZCP Guidelines – Indigenous Mental Health
www.ranzcp.org/Publications/Indigenous-mental-health.aspx
AHDs are not a
demand for treatment –consider, respect, uphold where
possible
6/7/2018
11
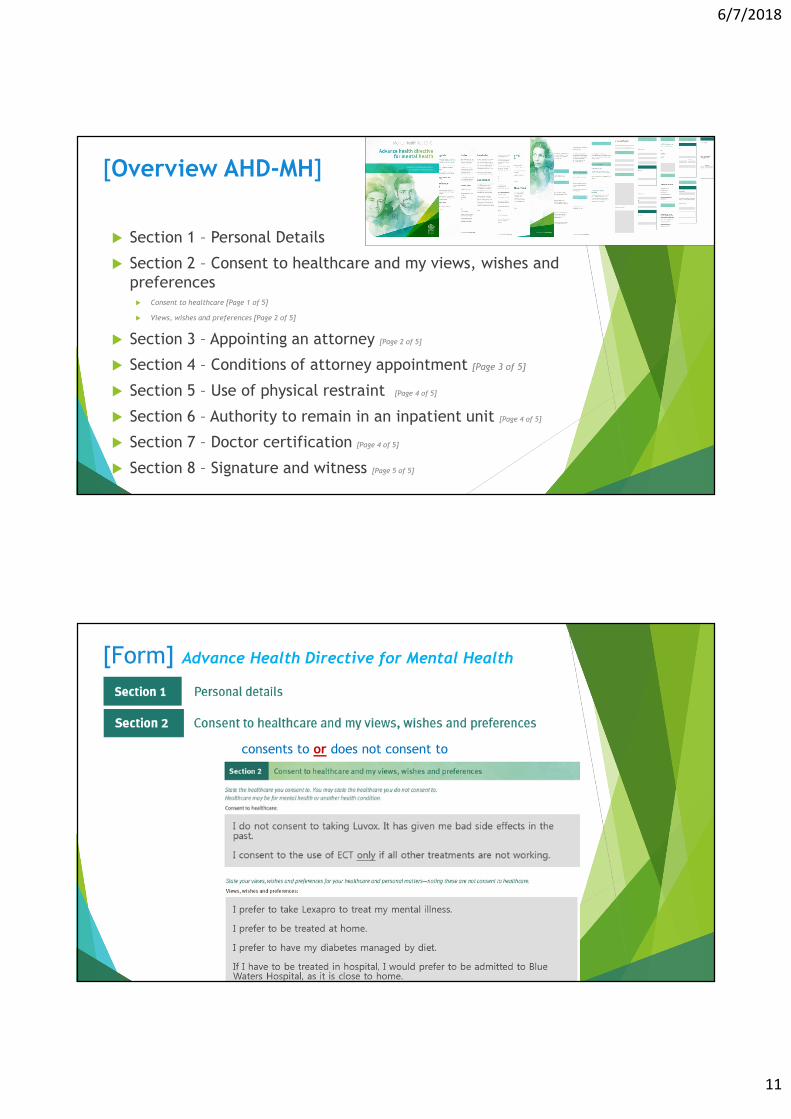
[Overview AHD-MH]
� Section 1 – Personal Details
� Section 2 – Consent to healthcare and my views, wishes and
preferences � Consent to healthcare [Page 1 of 5]
� Views, wishes and preferences [Page 2 of 5]
� Section 3 – Appointing an attorney [Page 2 of 5]
� Section 4 – Conditions of attorney appointment [Page 3 of 5]
� Section 5 – Use of physical restraint [Page 4 of 5]
� Section 6 – Authority to remain in an inpatient unit [Page 4 of 5]
� Section 7 – Doctor certification [Page 4 of 5]
� Section 8 – Signature and witness [Page 5 of 5]
[Form] Advance Health Directive for Mental Health
consents to or does not consent to
6/7/2018
12
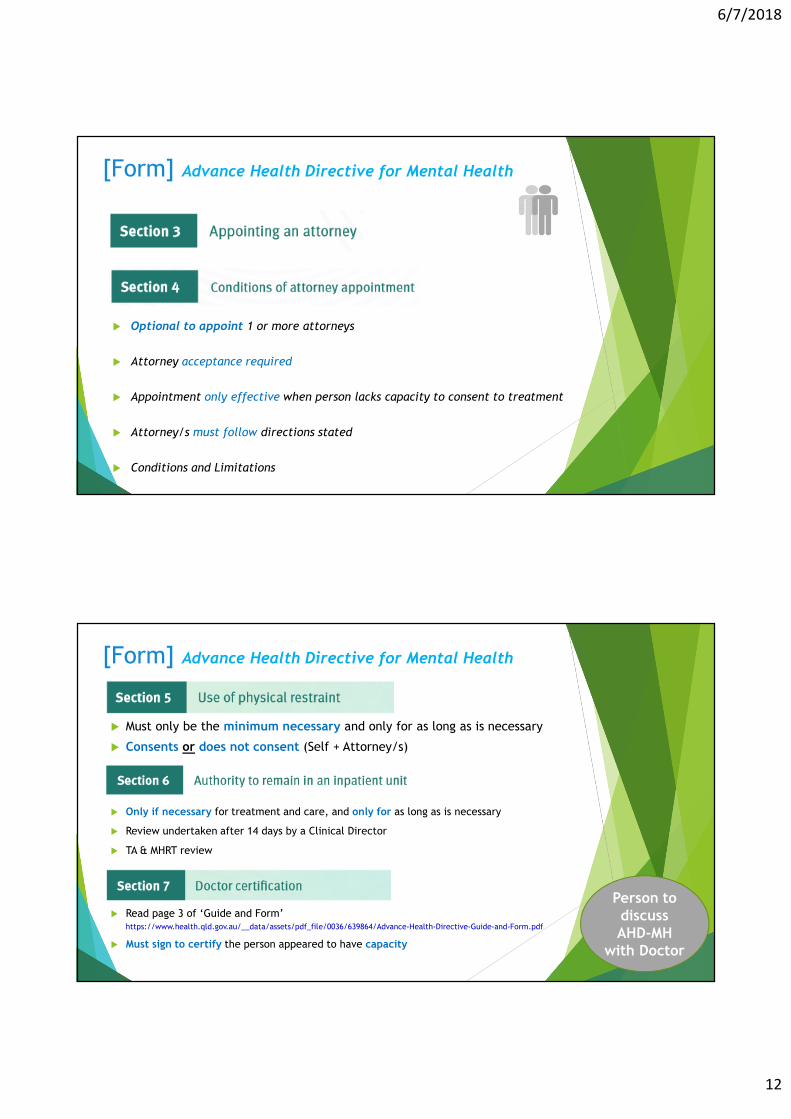
[Form] Advance Health Directive for Mental Health
� Optional to appoint 1 or more attorneys
� Attorney acceptance required
� Appointment only effective when person lacks capacity to consent to treatment
� Attorney/s must follow directions stated
� Conditions and Limitations
[Form] Advance Health Directive for Mental Health
� Must only be the minimum necessary and only for as long as is necessary
� Consents or does not consent (Self + Attorney/s)
� Only if necessary for treatment and care, and only for as long as is necessary
� Review undertaken after 14 days by a Clinical Director
� TA & MHRT review
� Read page 3 of ‘Guide and Form’ https://www.health.qld.gov.au/__data/assets/pdf_file/0036/639864/Advance-Health-Directive-Guide-and-Form.pdf
� Must sign to certify the person appeared to have capacity
Person to discuss AHD-MH
with Doctor
6/7/2018
13
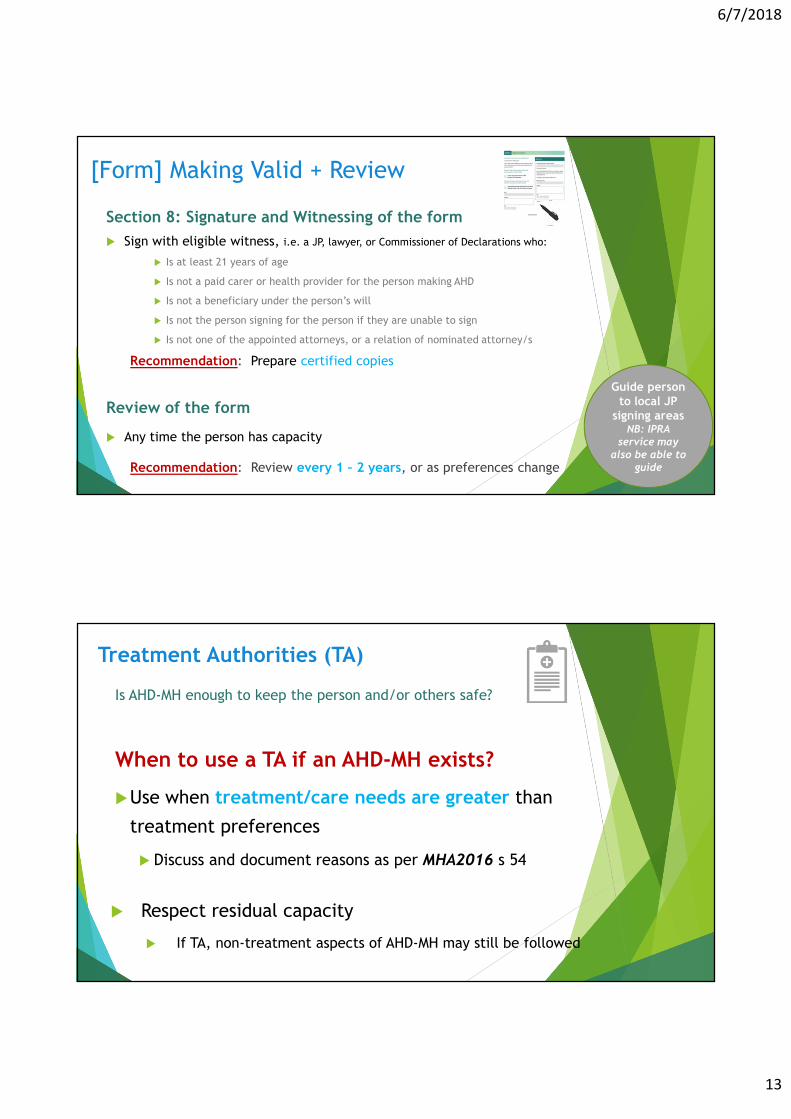
[Form] Making Valid + Review
Section 8: Signature and Witnessing of the form
� Sign with eligible witness, i.e. a JP, lawyer, or Commissioner of Declarations who:
� Is at least 21 years of age
� Is not a paid carer or health provider for the person making AHD
� Is not a beneficiary under the person’s will
� Is not the person signing for the person if they are unable to sign
� Is not one of the appointed attorneys, or a relation of nominated attorney/s
Recommendation: Prepare certified copies
Review of the form
� Any time the person has capacity
Recommendation: Review every 1 – 2 years, or as preferences change
Guide person to local JP
signing areas NB: IPRA
service may also be able to
guide
Treatment Authorities (TA)
Is AHD-MH enough to keep the person and/or others safe?
When to use a TA if an AHD-MH exists?
�Use when treatment/care needs are greater than
treatment preferences
� Discuss and document reasons as per MHA2016 s 54
� Respect residual capacity
� If TA, non-treatment aspects of AHD-MH may still be followed
6/7/2018
14
When requirement to treat in a less restrictive
way does not apply
� Refer to QH Chief Psychiatrist Policy “Advance Health Directives and ‘Less Restrictive Way’ of
Treatment”
� Section 5.5
� See also legislation: MHA2016 – Section 13 (extract below or refer to current version of MHA2016 online Qld Govt. Queensland Legislation site)
Queensland Consumer Resources & Videos:
Video: About the Advance Health Directive for Mental Health
Video: Completing the AHD-MH form
https://youtu.be/TSkP1xtlWBc
https://www.youtube.com/watch?v=U2MwR2h_F4Y
https://adaaustralia.com.au/clinicians/
health.qld.gov.au/mental-health-act
Guide people to watch videos
6/7/2018
15
GuidelinesThe RANZCP produces guidance to help psychiatrists and other mental health professionals in their work.
� Best Practice:
� The Royal Australian and New
Zealand College of Psychiatrists
(RANZCP)www.ranzcp.org/Publications/Guidelines-and-resources-for-practice.aspx
Discussion / ActivityEngage, Equip & Empower clinicians
Consider
� Would you feel confident assisting a person to complete their
AHD-MH if they approached you?
� Do you know where to locate the document?
� Have you engaged with IPRA roles?
� Have you encouraged the involvement of support person/s?
6/7/2018
16
Evidence suggests …
� Loss of capacity is likely to be episodic (3)
� Individual variation with decision-making (3)
� Directives allow a more informed and open dialogue
� Collaborative approach when drafting (4)
� Written directives usually indicates more stable preferences (1)
� Compliance improved with specific detail and attorney/s
� Review patient wishes over time (1)
E.g. UK Case [refer to Factsheet 7 https://adaaustralia.com.au/clinicians/]
Re E (Medical treatment: Anorexia) [2012] EWHC 1639 (COP)
Formal & detailed capacity assessment to be undertaken and documented
Evidence - References [1] Danis M et al., ‘Stability of Choices about Life-sustaining Treatments’ (1994) 120(7) American College of Physicians 567
[2] Loewy E, ‘Changing One’s Mind: When is Odysseus to Be Believed?’ (1988) 3 Journal of General Internal Medicine 54
[3] Ritchie J et al., ‘Advance Directives in Psychiatry – Resolving Issues of Autonomy and Competence’ (1998) 21(3) International Journal of Law and
Psychiatry 245
[4] Ryan C, ‘Betting your life: an argument against certain advance directives’ (1996) 22 Journal of Medical Ethics 95
[5] Winston M et al., ‘Can a Subject Consent to a ‘Ulysses Contract’?’ (1982) August The Hastings Center Report 26
[6] Loewy E, ‘Ethical Considerations in Executing and Implementing Advance Directives’ (1998) 158 (Feb 23) Archives of Internal Medicine 321
[7] Gross M, ‘What Do Patients Express as Their Preferences in Advance Directives?’ (1998) 158 (Feb 23) Archives of Internal Medicine 363
[8] Re E (Medical treatment: Anorexia) [2012] EWHC 1639 (COP)
[9] Del Villar, ‘The Enforceability of Mental Health Advance Directives: The Legal Limits of Personal Autonomy’ (PhD Thesis, Faculty of Law, QUT, in
progress) [2018/2019]
[10] Ganzini MD et al., ‘Pitfalls in Assessment of Decision-Making Capacity’ (2003) 44:3 Psychosomatics 237
[11] Williams K, ‘Advance care directives in Queensland: Two sides of the coin’ (2017) July Proctor 22
[12] Simpson et al., ‘Recovery-focused care planning and coordination in England and Wales: a cross-national mixed methods comparative case study’
(2016) 16 BMC Psychiatry 147
[13] Kisely et al., ‘Motivational aftercare planning to better care: Applying the principles of advance directives and motivational interviewing to
discharge planning for people with mental illness’ (2016) 26(1) International Journal of Mental Health Nursing 41
[14] Sellars et al., ‘Australian Psychiatrists’ Support for Psychiatric Advance Directives: Responses to a Hypothetical Vignette’ (2017) 24(1) Psychiatry,
Psychology and Law 61
[15] Davidson et al., ‘Supported decision making: A review of the international literature’ (2015) 38 International Journal of Law and Psychiatry 61
[16] Davidson et al., ‘An international comparison of legal frameworks for supported and substitute decision-making in mental health services’ (2016)
44 International Journal of Law and Psychiatry 30
[17] Bellesheim K, ‘Ethical Challenges and Legal Issues for Mental Health Professionals Working with Family Caregivers of Individuals with Serious
Mental Illness’ (2016) 26(7) Ethics and Behavior 607
[18] Devi et al., ‘Moving towards substituted or supported decision-making? Article 12 of the Convention on the Rights of Persons with Disabilities’
(2011) 5 ALTER, European Journal of Disability Research 249
[19] State Government of Victoria, ‘Advance care planning: have the conversation – A strategy for Victorian health services 2014-2018’ (2014) Access
online https://www2.health.vic.gov.au/hospitals-and-health-services/patient-care/end-of-life-care/advance-care-planning
6/7/2018
17
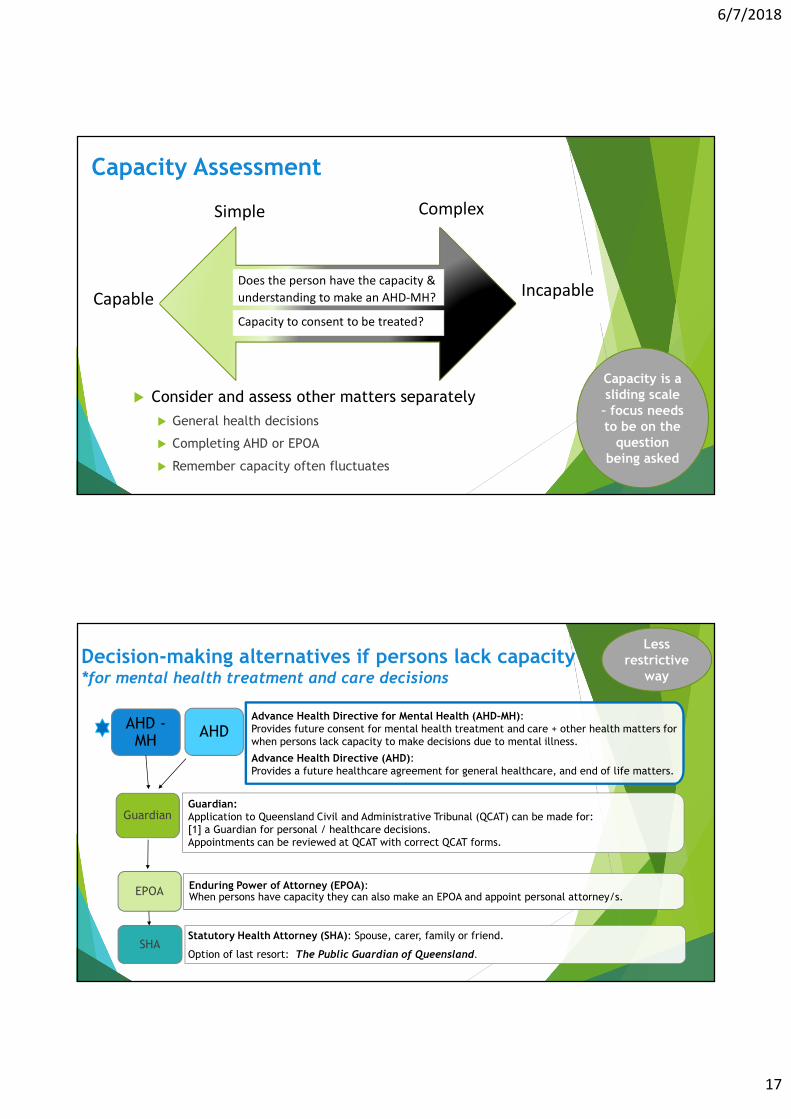
Capacity Assessment
CapableIncapable
Capacity to consent to be treated?
Simple Complex
� Consider and assess other matters separately
� General health decisions
� Completing AHD or EPOA
� Remember capacity often fluctuates
Does the person have the capacity &
understanding to make an AHD-MH?
Capacity is a sliding scale – focus needs to be on the
question being asked
Decision-making alternatives if persons lack capacity*for mental health treatment and care decisions
Guardian:Application to Queensland Civil and Administrative Tribunal (QCAT) can be made for:
[1] a Guardian for personal / healthcare decisions.
Appointments can be reviewed at QCAT with correct QCAT forms.
Enduring Power of Attorney (EPOA): When persons have capacity they can also make an EPOA and appoint personal attorney/s.
Statutory Health Attorney (SHA): Spouse, carer, family or friend.
Option of last resort: The Public Guardian of Queensland.
Advance Health Directive for Mental Health (AHD-MH): Provides future consent for mental health treatment and care + other health matters for
when persons lack capacity to make decisions due to mental illness.
Advance Health Directive (AHD): Provides a future healthcare agreement for general healthcare, and end of life matters.
AHDAHD -MH
Guardian
EPOA
SHA
Less restrictive
way
6/7/2018
18
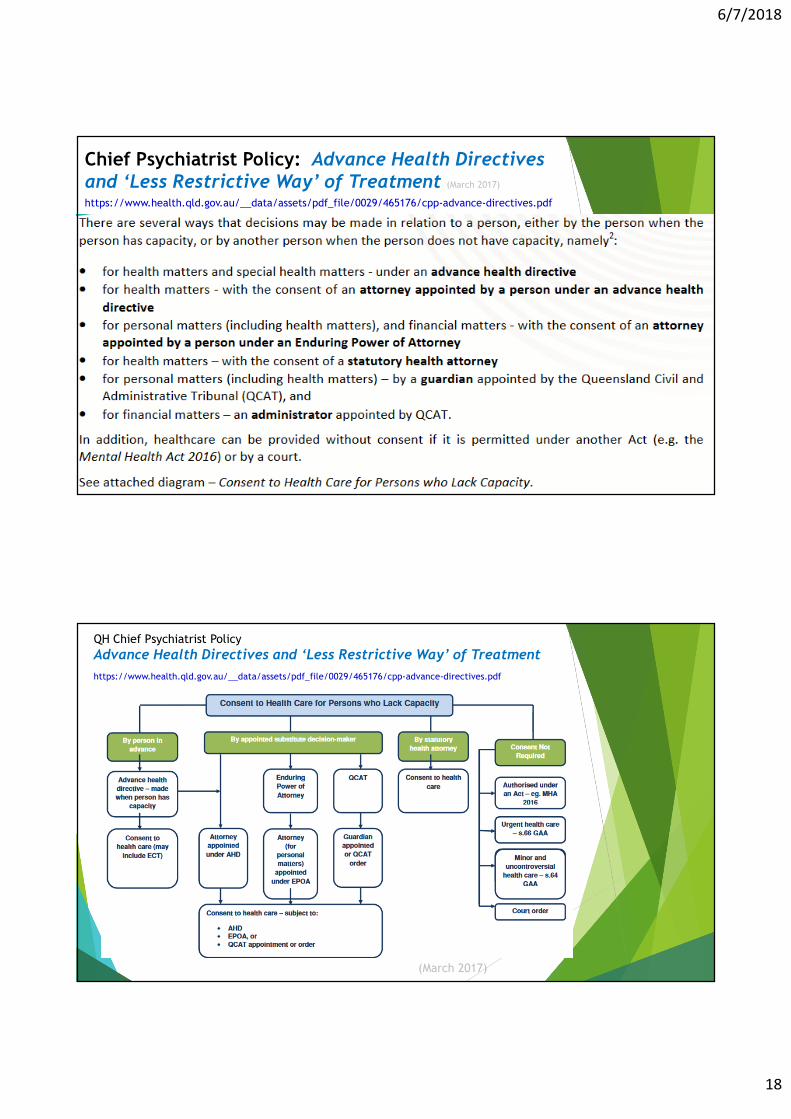
Chief Psychiatrist Policy: Advance Health Directives and ‘Less Restrictive Way’ of Treatment (March 2017)
https://www.health.qld.gov.au/__data/assets/pdf_file/0029/465176/cpp-advance-directives.pdf
QH Chief Psychiatrist Policy
Advance Health Directives and ‘Less Restrictive Way’ of Treatment
https://www.health.qld.gov.au/__data/assets/pdf_file/0029/465176/cpp-advance-directives.pdf
(March 2017)
6/7/2018
19
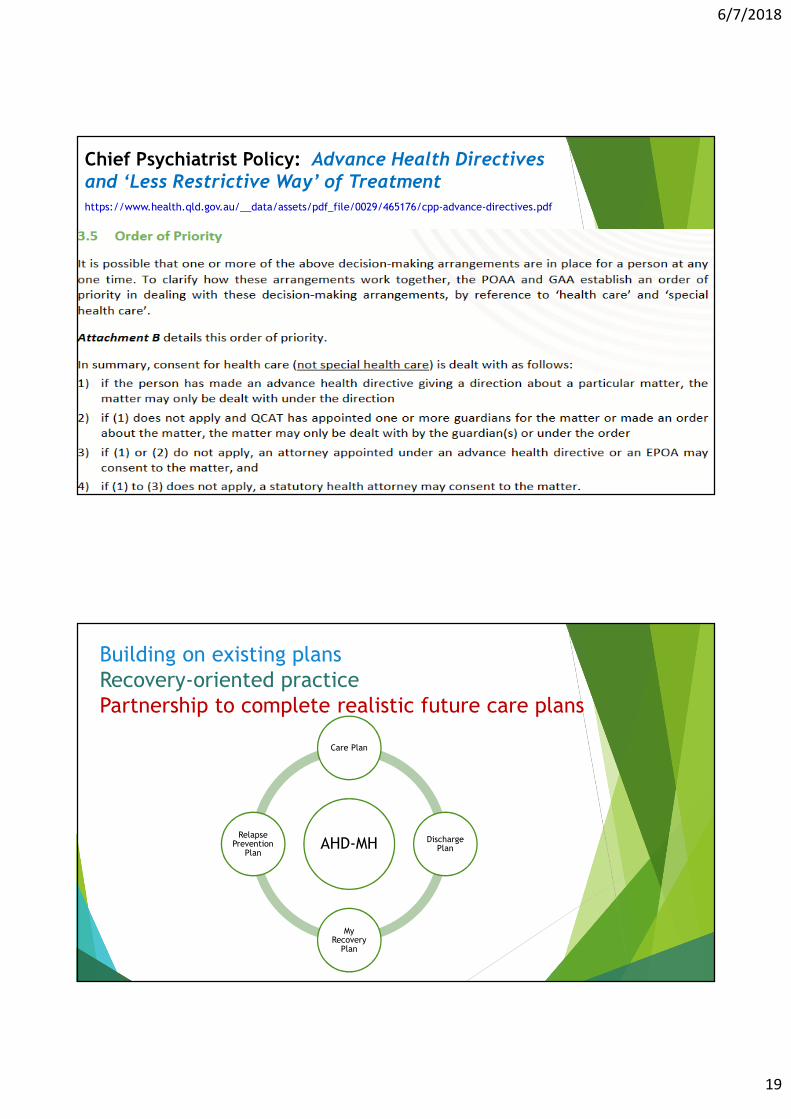
Chief Psychiatrist Policy: Advance Health Directives and ‘Less Restrictive Way’ of Treatmenthttps://www.health.qld.gov.au/__data/assets/pdf_file/0029/465176/cpp-advance-directives.pdf
Building on existing plans
Recovery-oriented practice
Partnership to complete realistic future care plans
AHD-MH
Care Plan
Discharge Plan
My Recovery
Plan
Relapse Prevention
Plan
6/7/2018
20
AHD-MH Training Resources
https://adaaustralia.com.au/clinicians/� Fact sheets
� Factsheet 1: About Advance Health Directives for Mental Health (AHD-MH)
� Factsheet 2: Decision-making and Capacity
� Factsheet 3: Frequently Asked Questions
� Factsheet 4: Glossary
� Factsheet 5: Useful Resources and Information
� Factsheet 6: Empowering 8 Steps for consumers to make an AHD-MH
� Factsheet 7: International Case Note
� QLD Health Checklist
https://www.health.qld.gov.au/__data/assets/pdf_file/0027/641169/Checklist_AHD_signing.pdf
MHA2016 Evaluation
Opportunities to provide feedback on the Mental Health Act 2016
https://www.health.qld.gov.au/clinical-practice/guidelines-
procedures/clinical-staff/mental-health/act/evaluation
More information about the Mental Health Act 2016 (Qld)
health.qld.gov.au/mental-health-act
More information on AHD-MH?
adaaustralia.com.au/clinicians
6/7/2018
21
Summary for AHD-MH
� Ask about existing
� Assist people with making
� Check state-wide system/s (i.e. CIMHA / The Viewer)
� Read and consider
� Remember section 54 MHA2016 – When an AHD not followed
� Review the AHD-MH regularly with the person
� AHD-MH Resources for Clinicians: https://adaaustralia.com.au/clinicians/
QC40 Capacity Assessment Training and Advance Health Directives – Module 2
Principle of ‘less
restrictive way’
Mental Health Act 2016 resources
Queensland Health resources and information:
health.qld.gov.au/mental-health-act
• Chief Psychiatrist policies and guidelines
Consumer resources
adaaustralia.com.au/education/advance-health-directives-mh
Online Learning & Face-to-Face courses
Queensland Centre for Mental Health Learning
qcmhl.qld.edu.au
• Online: QC40 Capacity Assessment Training and
Advance Health Directives
• Face-to-face: QC 13 Capacity Assessment
iLearn ilearn.health.qld.gov.au
More information:
• IPRA/s available - Queensland public hospitals
Queensland Health Documents for Consumers*
Guides and Forms
Guide to Patient Rights
Advance health directive for mental health (Guide & Form)
Nominated Support Persons (Guide & Form)
Factsheets
Statement of Rights – Your rights under the Mental Health Act 2016
Patient Rights
Role of Nominated Support Persons
Rights of Family, Carers and Other Support Persons
Advance Health Directives and Less Restrictive Way of Treatment
Brochures
Advance Health Directives
Support Persons
Your Rights
Revocation Forms
Revocation of AHD and Attorney Form
Revocation of Nominated Support Person
Recommended

















