Clinical Symptoms of Clinical Symptoms of Atrial Fibrillation Atrial Fibrillation according to QTc according to QTc Interval DurationInterval Duration
Kulik V.L., Yabluchansky N.I.Medical Clinics ChairNational University of Karazin (Kharkov, Ukraine)

Causes for the InvestigationCauses for the Investigation
QT shortening, less than 358 ms, or its QT shortening, less than 358 ms, or its prolongation, more than 437 ms, relate to a prolongation, more than 437 ms, relate to a high risk of AF development and sudden high risk of AF development and sudden cardiac death.cardiac death.
The patients with congenital short QT The patients with congenital short QT syndrome (2nd genotype) have a high risk of syndrome (2nd genotype) have a high risk of developing AF.developing AF.
There are no studies dedicated to the topic of There are no studies dedicated to the topic of the relationship between QTc and AF clinical the relationship between QTc and AF clinical symptomssymptoms..

Objective of the StudyObjective of the Study
To study the relationship between adjusted To study the relationship between adjusted QT interval and clinical symptoms in patients QT interval and clinical symptoms in patients with AF, with the goal of improving the with AF, with the goal of improving the quality of the diagnosis and management of quality of the diagnosis and management of this arrhythmia.this arrhythmia.

Investigated PopulationInvestigated Population
98 98 patients (67 men and 31 women), age patients (67 men and 31 women), age 6464±±1010 years years old.old.
Time of evolution of AF: Time of evolution of AF: 66..55±5±5 years oldyears old
Causes of AFCauses of AF:: CAD CAD (36 (36 patientspatients)) HBP HBP (83 (83 patientspatients)) CAD and HBP CAD and HBP (32 (32 patientspatients))
The relationship between the forms of AF (paroxysmal, The relationship between the forms of AF (paroxysmal, persistent, chronic) was 1:4:11, respectively.persistent, chronic) was 1:4:11, respectively.

Investigated PopulationInvestigated Population Classification according the Classification according the
characteristics of the patientscharacteristics of the patients
GenderGender - - malemale - - femalefemale Age: Age: –– adults adults ((men men 45-60 45-60 years oldyears old, , women women 45-55 45-55 years oldyears old)) - - older older adults adults ((men men 61-74 61-74 y.o.y.o., , women women 56-74 56-74 y.o.y.o.)) - - elderly elderly ((men and women men and women 75-87 75-87 y.o.y.o.)) AF characteristicsAF characteristics
– Time of evolution Time of evolution ((up to up to 10 years or more than 10 years10 years or more than 10 years))– FormForm ( (chronic, persistent, paroxysmalchronic, persistent, paroxysmal))– Classification by HR (bpm) Classification by HR (bpm) - - bradibradi- - (less than 60(less than 60), ), normonormo- (60-90) - (60-90) and and
tachycardia tachycardia ((more than more than 90)90) Degree of HF Degree of HF ((FC FC І-ІІІІ-ІІІ)) LV Ejection Fraction (EF) LV Ejection Fraction (EF) (20-43%, 44-66% (20-43%, 44-66% andand 67-88%) 67-88%) Stable chronic angina Stable chronic angina ((FC FC І-ІІІІ-ІІІ)) Systolic and diastolic pressure: normal BP – below 140/90 mm.Hg.Systolic and diastolic pressure: normal BP – below 140/90 mm.Hg. - - mild HBP (systolic pressure mild HBP (systolic pressure 140-159 140-159 mm.Hg., diastolic pressure mm.Hg., diastolic pressure 90-99 90-99 mm.Hg.mm.Hg.)) - - moderate HBP moderate HBP ((syst. pres.syst. pres.160-179160-179 mm.Hg. mm.Hg., , diast. pres. diast. pres. 100-109100-109 mm.Hg. mm.Hg.)) - - severe HBP severe HBP ((syst. pres. more than syst. pres. more than 180180 mm.Hg. mm.Hg., , diast. pres. more than diast. pres. more than 110110 mm.Hg. mm.Hg.)) History of AMIHistory of AMI History of strokeHistory of stroke

Investigated PopulationInvestigated Population Inclusion and exclusion criteriaInclusion and exclusion criteria
Inclusion criteria:Inclusion criteria: AFAF CAD CAD ((CSA CSA FCFC I-IIII-III)) HBP HBP Endocarditis, myocarditis, pericarditisEndocarditis, myocarditis, pericarditis Valve diseasesValve diseases ExtrasystoleExtrasystole Conduction disordersConduction disorders Chronic heart failure Chronic heart failure (FC I-III(FC I-III))
Exclusion criteria:Exclusion criteria: Chronic stable angina, FCChronic stable angina, FC IVIV Acute coronary syndromesAcute coronary syndromes Heart failure FCHeart failure FC IVIV

Equipment Used and Evaluated Equipment Used and Evaluated ParametersParameters
““CardioLab+” computerized electrocardiographCardioLab+” computerized electrocardiographEvaluated parameters:Evaluated parameters: QTQT interval interval ((msms)) HR HR ((bpmbpm))
““Sim 5000 plusSim 5000 plus” echocardiograph” echocardiographEvaluated parameters: Evaluated parameters: LVEF LVEF (%)(%)
““Microlife” manual blood pressure cuffMicrolife” manual blood pressure cuff Systolic pressure Systolic pressure ((mm.Hg.mm.Hg.)) Diastolic pressure Diastolic pressure ((mm.Hg.mm.Hg.))

Measurement and Standardization Measurement and Standardization Method for the QT IntervalMethod for the QT Interval
The measurement of QT duration in 3 The measurement of QT duration in 3 consecutive complexes since the onset of consecutive complexes since the onset of the Q wave up to the end of T wave, in the the Q wave up to the end of T wave, in the DII, V5 and V6 leads, choosing the longest DII, V5 and V6 leads, choosing the longest QT.QT.
QTc estimationQTc estimation:: QTQTсс = QT + 0.154×(1 = QT + 0.154×(1000 000 − RR)− RR)
This formula was used in the Framingham study in patients with AFThis formula was used in the Framingham study in patients with AF**
* - * - Sagie A, Larson MG, Goldberg RJ, Bengston JR, Levy D. "An improved method for adjusting Sagie A, Larson MG, Goldberg RJ, Bengston JR, Levy D. "An improved method for adjusting the QTthe QT
interval for heart rate (the Framingham Heart Study)". Am J Cardiol 70 (7): 797–801interval for heart rate (the Framingham Heart Study)". Am J Cardiol 70 (7): 797–801, 1992., 1992.

Classification of QTc DurationClassification of QTc Duration
Classification of QTc duration:Classification of QTc duration:– Short Short ((less than less than 320 320 msms))– NormalNormal (320-440 (320-440 msms))– LongLong((more than more than 440 440 msms))
QTc interval divided each 30 msQTc interval divided each 30 ms

Statistical AnalysisStatistical Analysis
Data base in Data base in Microsoft ExcelMicrosoft Excel Statistical analysis with parametric Statistical analysis with parametric
methodsmethods Construction of graphs on QTc Construction of graphs on QTc
duration in different subsetsduration in different subsets

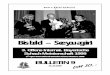
Distribution of QTc Duration Distribution of QTc Duration between Patientsbetween Patients
Most patients are in a range between 381 and 470 ms. The most frequent QTc duration was 381-410 ms. More than a third of the patients have prolonged QTc.
0
5
10
15
20
25
30
320 350 380 410 440 470 500 530 560
QTc (ms)

Ratio between QTc and GenderRatio between QTc and Gender
men
0
5
10
15
20
320 350 380 410 440 470 500 530 560
QTc (ms)
The ratio between men and women was 2:1.The QTc duration range in men was greater than in women. The ratio between the 381-410 and 441-470 ms intervals between men and women was similar.
women
0
2
4
6
8
10
320 350 380 410 440 470 500 530 560
QTc (ms)

Ratio between QTc and the Age of Ratio between QTc and the Age of MenMen
With age, the QTc dispersion range shifts toward higher values.
45-60-year-old men
0
2
4
6
8
10
12
320 350 380 410 440 470 500 530 560
QTc (ms)
61-74-year-old men
0
1
2
3
4
5
6
320 350 380 410 440 470 500 530 560
QTc (ms)
75-89-year-old men
0
1
2
3
4
5
320 350 380 410 440 470 500 530 560
QTc (ms)

Ratio between QTc and the Age of Ratio between QTc and the Age of WomenWomen
With age, the QTc range shifts toward higher values.
45-55-year-old women
0
0,5
1
1,5
2
2,5
350 380 410 440 470 500
QTc (ms)
75-89-year-old women
0
0,5
1
1,5
2
2,5
350 380 410 440 470 500
QTc (ms)
56-74-year-old women
0
1
2
3
4
5
6
350 380 410 440 470 500
QTc (ms)

Ratio between QTc and AF FormRatio between QTc and AF Form
The ratio between persistent and paroxysmal AF subsets was 1:2.
The ranges of QTc duration in both subsets showed no significant differences.
Paroxysmal and persistent AF
0
5
10
15
320 350 380 410 440 470 500 530 560
QTc (ms)
Chronic AF
0
5
10
15
20
320 350 380 410 440 470 500 530 560
QTc (ms)

Ratio between QTc and HRRatio between QTc and HR
The ratio between patients with tachy-, normo-, and bradycardic AF was 13:6:1, respectively.In tachycardic AF, QTc duration is distributed over the whole range.With the decrease of HR the range is narrowed. In the bradycardic form, the distribution of QTc duration is shifted toward higher values.
Bradysystolic AF
012345
320 350 380 410 440 470 500 530 560
QTc (ms)
Normosystolic AF
0
5
10
15
320 350 380 410 440 470 500 530 560
QTc (ms)
Tachysystolic AF
0
5
10
15
320 350 380 410 440 470 500 530 560
QTc (ms)

Ratio between QTc and the Time of Ratio between QTc and the Time of AF EvolutionAF Evolution
The ratio between the subsets with less than 10 years of evolution and more than 10 years was 4:1.
In the subset of less than 10 years, the QTc duration range is wider; in the subset of more than 10 years, narrower.
Time of AF evolution of less than 10 years
05
10152025
320 350 380 410 440 470 500 530 560
QTc (ms)
Time of AF evolution of more than 10 years
0
1
2
3
4
5
6
320 350 380 410 440 470 500 530 560
QTc (ms)

Ratio between QTc and LVEFRatio between QTc and LVEF
LVEF 20-41%
00,5
11,5
22,5
33,5
320 350 380 410 440 470 500 530 560
QTc (ms)
LVEF 42-63%
0
5
10
15
20
320 350 380 410 440 470 500 530 560
QTc (ms)
LVEF 64-86%
0
2
4
6
8
10
12
320 350 380 410 440 470 500 530 560
QTc (ms)
The ratio between patients with LVEF 20-43%, 44-66%, and 67-88% was 1:4:2, respectively.With the decrease of LVEF, the QTc duration range is wider.

Ratio between QTc and FC of Ratio between QTc and FC of Chronic Stable Angina (CSA)Chronic Stable Angina (CSA)
The ratio between FC I, II, and III of CSA was 1:3:2, respectively.In the FC I and II subsets, the QTc range was between 351 and 470 ms.With the increase of FC, the QTc range shifts toward higher values.
Chronic HF, FC I
0
1
2
3
4
5
320 350 380 410 440 470 500 530 560
QTc (ms)
Chronic HF, FC II
0
2
4
6
8
10
12
320 350 380 410 440 470 500 530 560
QTc (ms)
Chronic HF, FC III
0
2
4
6
8
10
12
320 350 380 410 440 470 500 530 560
QTc (ms)

Ratio between QTc and systolic Ratio between QTc and systolic BPBP
Systolic BP <139 mm.Hg.
0
5
10
15
320 350 380 410 440 470 500 530 560
QTc (ms)
Systolic BP 140-159 mm.Hg.
0
2
4
6
8
320 350 380 410 440 470 500 530 560
QTc (ms)
Systolic BP 160-179 mm.Hg.
0
2
4
6
8
10
320 350 380 410 440 470 500 530 560
QTc (ms)
The ratio between patients without HBP, with mild, moderate, and severe HBP (in regard to systolic BP) was 5:3:2:1.With the increase of systolic BP, the QTc range shifts toward higher values.In the subset of severe HBP, the range of QTc duration is narrower and is concentrated between 381 and 500 ms.
Systolic BP >180 mm.Hg.
012345
320 350 380 410 440 470 500 530 560
QTc (ms)

Ratio between QTc and Ratio between QTc and Diastolic BPDiastolic BP
Diastolic BP <89 mm.Hg.
0246
8101214
320 350 380 410 440 470 500 530 560
QTc (ms)
Diastolic BP 90-99 mm.Hg.
0
2
4
6
8
320 350 380 410 440 470 500 530 560
QTc (ms)
The ratio between patients without HBP, with mild, moderate, and severe HBP (in regard to diastolic BP) was 5:2:2:1.With the increase of diastolic BP, the range of QTc shifts toward higher values.In the subset of severe HBP, the range of QTc duration is narrower and is concentrated between 381 and 470 ms.
Diastolic BP >110
0
1
2
3
4
5
320 350 380 410 440 470 500 530 560
QTc (ms)
Diastolic BP 100-109 mm.Hg.
0
2
4
6
8
10
320 350 380 410 440 470 500 530 560
QTc (ms)

Ratio between QTc Duration and Ratio between QTc Duration and History of AMIHistory of AMI
Patients with history of AMI
00,5
11,5
22,5
33,5
320 350 380 410 440 470 500 530 560
QTс (ms)
The ratio between patients with history of AMI and without AMI, was 1:8.
The QTc range in the subsets with history of AMI and without AMI, was similar.
Patients without history of AMI
0
5
10
15
20
25
320 350 380 410 440 470 500 530 560
QTc (ms)

Ratio between QTc and History of Ratio between QTc and History of StrokeStroke
Patients with history of stroke
00,5
11,5
22,5
33,5
320 350 380 410 440 470 500 530 560
QTc (ms)
The ratio between the subsets with history of stroke and without stroke, was 1:8.In the subset with stroke, the range of QTc duration was lower.
Patients without history of stroke
0
5
10
15
20
25
320 350 380 410 440 470 500 530 560
QTc (ms)

ConclusionsConclusions
In the patients studied, the range of QTc duration was between 290 and 560 ms. The ratio between the patients with short, normal, and prolonged QTc was 1:16:7,
respectively. The most frequent QTc duration was between 381 and 410 ms. The range of the QTc interval in men was greater than in women. The QTc range in subsets with persistent or paroxysmal and chronic AF was similar. With the decrease of HR, the QTc range decreased. In the subset with AF evolution of less than 10 years, the range of QTc was wider
than in the subset of more than 10 years. As LVEF decreased, the QTc range became wider. With the increase of age, heart failure functional class, HBP degree, and HR
decrease, the QTc range shifts to higher values. QTc range in the subsets with history of AMI or without AMI was similar. In the subset of patients with history of stroke, the range of QTc duration was lower
than in the subset without history of stroke. For the diagnosis of AF, it is important to consider the QTc interval duration. The changes in QTc duration may be useful as a marker of therapeutic measures
effectiveness.
Recommended