Endoform® can help to improve healing and lower the cost of VLU management
• Endoform® can be used from day one in difficult-to-manage VLU’s.1, 2, 3, 4
• Endoform® does not need to be removed and requires fewer dressing changes than other products; which may lead to greater patient satisfaction and compliance.5
• Endoform® reduces the cost of VLU treatment because application can be carried out by a range of wound care practitioners (no suturing required) and subsequent applications can be carried out by the patient at home.5
• A case series using Endoform® was shown to result in 95.7% closure of VLUs in 12 weeks with an average closure time of 7.3 weeks (n=23 wounds, ranging in size from 0.2 – 23.4 cm2, in 14 patients).5
• Early reduction in wound area (20-40% in the first 2-4 weeks of treatment) is a good predictor of healing.6 In a clinical study, 4 weeks of Endoform® treatment resulted incomplete closure in 40% of cases (n=28). 1
Endoform® can be used at all phases of wound management
MKT.1436.01
CLINICAL EVIDENCE | Treatment of Venous Leg Ulcers (VLUs)
Stabilize
Hemostasis Inflammation Proliferation Remodelling
Correct Build Organize
Wound Closure
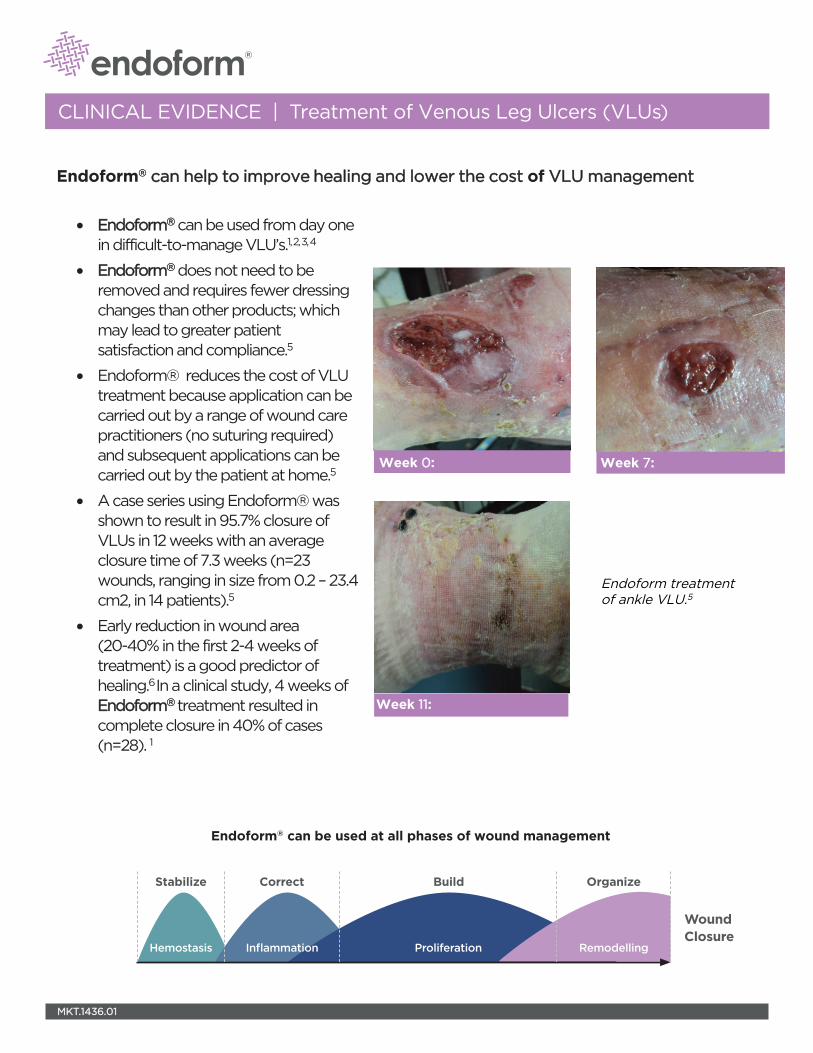
Week 0:
Week 11:
Week 7:
Endoform treatment of ankle VLU.5
References
1. Lullove, E. (2016). Use of Ovine Collagen Extracellular Matrix and Gentian Violet and Methylene Blue Antibacterial Foam Dressings to Help Improve Clinical Outcomes in Lower Extremity Wounds. Symposium on Advanced Wound Care - Fall, Las Vega, NA. 2. Liden BA, (2011). Case Study 1: Mixed Vascular Disease, from "Early Clinical Findings From The Use Of Endoform Dermal Template (Ovine Forestomach Matrix) To Treat Recalcitrant Wounds"; Presented at Symposium on Advanced Wound Care, April 14-17, 2011 Dallas, TX3. Liden BA, (2011). Case Study 3: Mixed Vascular Etiology, from "Early Clinical Findings From The Use Of Endoform Dermal Template (Ovine Forestomach Matrix) To Treat Recalcitrant Wounds"; Presented at Symposium on Advanced Wound Care, April 14-17, 2011 Dallas, TX. 4. Curran, M. (2013). Case Study 9: Venous Ulcer, Aroa Biosurgery.5. Bohn, G. A. and K. Gass (2014). "Leg ulcer treatment outcomes with new ovine collagen extracellular matrix dressing: a retrospective case series." Adv Skin Wound Care 27(10): 448-454. 6. Bohn, G. A., G. S. Schultz, B. A. Liden, M. N. Desvigne, E. J. Lullove, I. Zilberman, M. B. Regan, M. Ostler, K. Edwards, G. M. Arvanitis and J. F. Hartman (2017). "Proactive and Early Aggressive Wound Management: A Shift in Strategy Developed by a Consensus Panel Examining the Current Science, Prevention, and Management of Acute and Chronic Wounds." Wounds 29(11): S37-S42.
©2018 Aroa Biosurgery Limited
MKT 1436.01 | May 2018
Antimicrobial Dermal Template
Natural Dermal Template
Manufactured for: AROA BIOSURGERY INC
340 Progress Drive, Manchester, CT 06042 1-860-337-7730
www.aroabio.com
RX Only. Prior to use, be sure to read the entire Instructions for Use package insert supplied with the product.
For product questions, sampling needs, or detailed clinical questions concerning our products in the US, please call 1-860-337-7730
HCPCS are for reference only and subject to change.
Endoform® is a registered trademark of Aroa Biosurgery Limited.
Endoform® Dermal Template is marketed in the USA by Appulse
CLINICAL EVIDENCE | Treatment of Venous Leg Ulcers (VLUs)
Purpose: To analyze our clinical outcomes with use of ovine collagenextracellular matrix (CECM)* and gentian violet/methylene blue (GV/MB) polyurethane (PU) antibacterial foam dressings** in treating chronic lower extremity wounds.
Introduction: Chronic lower extremity wounds are increasingly more prevalent and complex to treat, and are a significant cause of morbidity and drain on healthcare resources worldwide. Patient comorbid conditions such diabetes, peripheral vascular disease and obesity can delay wound healing, and must be clinically addressed to correct causes of tissue damage. In addition to underlying medical conditions, chronic wounds are characterized by a complex etiology that can include abnormal cell-extracellular matrix (ECM) interactions, elevated bioburden levels and bacterial biofilm, imbalances of matrix-metalloproteinases (MMP), and an unresolved inflammatory response—all of which can damage the wound ECM.1,2 Dressings that provide broad spectrum MMP reduction along with inherent aspects of an ECM may contribute to improved wound healing outcomes and shorter treatment times.3 Preliminary reports of a CECM dressing have demonstrated benefits in chronic wound healing.4,5
Methodology: • Retrospectivechartanalysiswasperformedonobservationaldata
of consecutive patients with chronic lower extremity ulcers whowere managed with CECM as a primary dressing and MB/GV PUantibacterial foam dressing to manage bioburden as a secondarydressing in an outpatient setting.
• Allpatientsweretreatedtwiceweeklyintheclinicforthefirstfourweeks.Duringthefirstvisit,woundswerecleansedwithsalineordermal cleanser, sharp debrided as needed, and a CECM dressingcoveredwithaMB/GVPUantibacterialfoamwasplaced.Atthemid-weekappointment,woundswereagaincleansedandexamined,butnotsharpdebrided.AnadditionalCECMdressingwas placed if the previous CECM dressing was fully integrated intothe wound and the MB/GV PU antibacterial foam was replaced.
• Aftertheinitialfourweekperiod,patientsreceivedonceweeklytreatment consisting of cleansing, sharp debridement as needed,and a CECM dressing covered with a GV/MB PU antibacterial foamuntil wound was healed.
Use of Ovine Collagen Extracellular Matrix and Gentian Violet and Methylene Blue Antibacterial Foam Dressings to Help Improve Clinical Outcomes in Lower Extremity Wounds
• Eric J. Lullove, DPM, CWS, FACCWSWestBocaCenterforWoundHealing,BocaRaton,FL
Results:
• Fifty-threepatientswith53woundsweretreated.• Typesofwoundstreatedwerediabeticfootulcers(n=22),venouslegulcers(n=28),andheelpressureulcers(n=3).
• AverageBMIforstudypopulationwas28.3usingastandardBMIformula with a BMI between 25 and 30 being overweight; averagepatient age was 75.9 years.
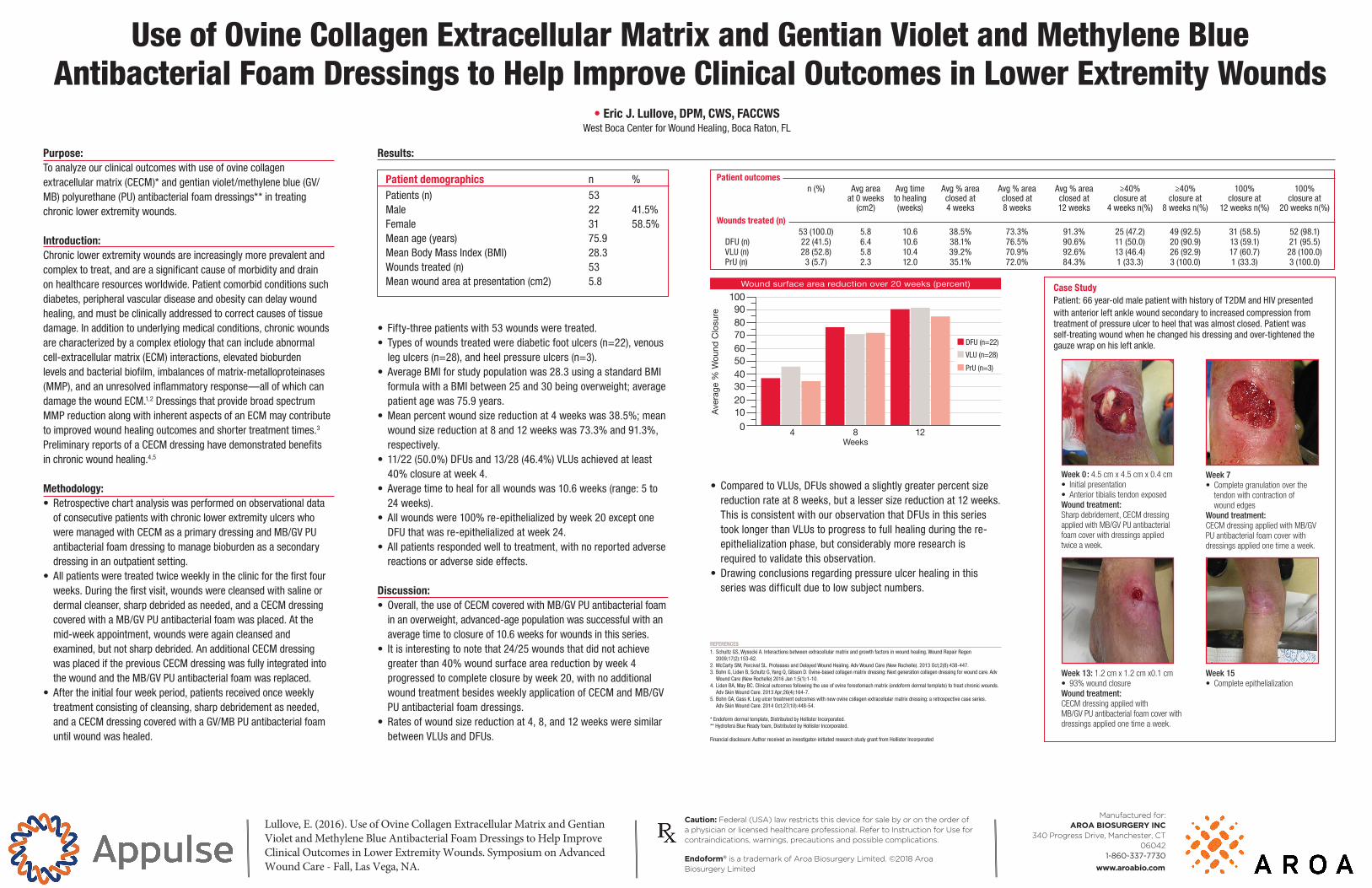
• Meanpercentwoundsizereductionat4weekswas38.5%;meanwoundsizereductionat8and12weekswas73.3%and91.3%,respectively.
• 11/22(50.0%)DFUsand13/28(46.4%)VLUsachievedatleast40%closureatweek4.
• Averagetimetohealforallwoundswas10.6weeks(range:5to24weeks).
• Allwoundswere100%re-epithelializedbyweek20exceptoneDFUthatwasre-epithelializedatweek24.
• Allpatientsrespondedwelltotreatment,withnoreportedadversereactions or adverse side effects.
Discussion: • Overall,theuseofCECMcoveredwithMB/GVPUantibacterialfoam
in an overweight, advanced-age population was successful with anaveragetimetoclosureof10.6weeksforwoundsinthisseries.
• Itisinterestingtonotethat24/25woundsthatdidnotachievegreaterthan40%woundsurfaceareareductionbyweek4progressedtocompleteclosurebyweek20,withnoadditionalwoundtreatmentbesidesweeklyapplicationofCECMandMB/GVPU antibacterial foam dressings.
• Ratesofwoundsizereductionat4,8,and12weeksweresimilarbetweenVLUsandDFUs.
• ComparedtoVLUs,DFUsshowedaslightlygreaterpercentsizereductionrateat8weeks,butalessersizereductionat12weeks.ThisisconsistentwithourobservationthatDFUsinthisseriestooklongerthanVLUstoprogresstofullhealingduringthere-
epithelialization phase, but considerably more research is required to validate this observation.
• Drawingconclusionsregardingpressureulcerhealinginthisseries was difficult due to low subject numbers.
REFERENCES1.SchultzGS,WysockiA.Interactionsbetweenextracellularmatrixandgrowthfactorsinwoundhealing.WoundRepairRegen
2009;17(2):153-62.2.McCartySM,PercivalSL.ProteasesandDelayedWoundHealing.AdvWoundCare(NewRochelle).2013Oct;2(8):438-447.3. BohnG,LidenB,SchultzG,YangQ,GibsonD.Ovine-basedcollagenmatrixdressing:Nextgenerationcollagendressingforwoundcare.Adv
WoundCare(NewRochelle)2016Jan1;5(1):1-10.4. LidenBA,MayBC.Clinicaloutcomesfollowingtheuseofovineforestomachmatrix(endoformdermaltemplate)totreatchronicwounds.
AdvSkinWoundCare.2013Apr;26(4):164-7.5. BohnGA,GassK.Legulcertreatmentoutcomeswithnewovinecollagenextracellularmatrixdressing:aretrospectivecaseseries.
AdvSkinWoundCare.2014Oct;27(10):448-54.
* Endoform dermal template, Distributed by Hollister Incorporated.**HydroferaBlueReadyfoam,DistributedbyHollisterIncorporated.
Financialdisclosure:Authorreceivedaninvestigator-initiatedresearchstudygrantfromHollisterIncorporated
Wound surface area reduction over 20 weeks (percent)
010
50
90
30
70
20
60
100
40
80
8 12
VLU(n=28)
PrU(n=3)
DFU(n=22)
4
Ave
rage
% W
ound
Clo
sure
Weeks
Patient demographics n %Patients (n) 53 Male 22 41.5%Female 31 58.5%Mean age (years) 75.9 MeanBodyMassIndex(BMI) 28.3Wounds treated (n) 53 Meanwoundareaatpresentation(cm2) 5.8
Patient outcomesn(%) Avgarea Avgtime Avg%area Avg%area Avg%area ≥40% ≥40% 100% 100%
at0weeks tohealing closedat closedat closedat closureat closureat closureat closureat(cm2) (weeks) 4weeks 8weeks 12weeks 4weeksn(%) 8weeksn(%) 12weeksn(%) 20weeksn(%)
Wounds treated (n)53(100.0) 5.8 10.6 38.5% 73.3% 91.3% 25(47.2) 49(92.5) 31(58.5) 52(98.1)
DFU(n) 22(41.5) 6.4 10.6 38.1% 76.5% 90.6% 11(50.0) 20(90.9) 13(59.1) 21(95.5)VLU(n) 28(52.8) 5.8 10.4 39.2% 70.9% 92.6% 13(46.4) 26(92.9) 17(60.7) 28(100.0)PrU(n) 3(5.7) 2.3 12.0 35.1% 72.0% 84.3% 1(33.3) 3(100.0) 1(33.3) 3(100.0)
Case Study Patient:66year-oldmalepatientwithhistoryofT2DMandHIVpresentedwith anteriorleftanklewoundsecondarytoincreasedcompressionfromtreatment of pressure ulcer to heel that was almost closed. Patient was self-treating wound when he changed his dressing and over-tightened the gauzewraponhisleftankle.
Week 0 : 4.5 cm x 4.5 cm x 0.4 cm• Initial presentation• AnteriortibialistendonexposedWound treatment:Sharpdebridement,CECMdressingappliedwithMB/GVPUantibacterialfoamcoverwithdressingsappliedtwiceaweek.
Week 15 • Completeepithelialization
Week 13: 1.2 cm x 1.2 cm x0.1 cm• 93%woundclosureWound treatment:CECMdressingappliedwithMB/GVPUantibacterialfoamcoverwithdressingsappliedonetimeaweek.
Week 7 • Completegranulationoverthetendonwithcontractionofwoundedges
Wound treatment:CECMdressingappliedwithMB/GVPUantibacterialfoamcoverwithdressingsappliedonetimeaweek.
Lullove, E. (2016). Use of Ovine Collagen Extracellular Matrix and Gentian Violet and Methylene Blue Antibacterial Foam Dressings to Help Improve Clinical Outcomes in Lower Extremity Wounds. Symposium on Advanced Wound Care - Fall, Las Vega, NA.
Caution: Federal (USA) law restricts this device for sale by or on the order of a physician or licensed healthcare professional. Refer to Instruction for Use for contraindications, warnings, precautions and possible complications.
Endoform® is a trademark of Aroa Biosurgery Limited. ©2018 Aroa Biosurgery Limited
Manufactured for: AROA BIOSURGERY INC
340 Progress Drive, Manchester, CT 06042
1-860-337-7730
www.aroabio.com
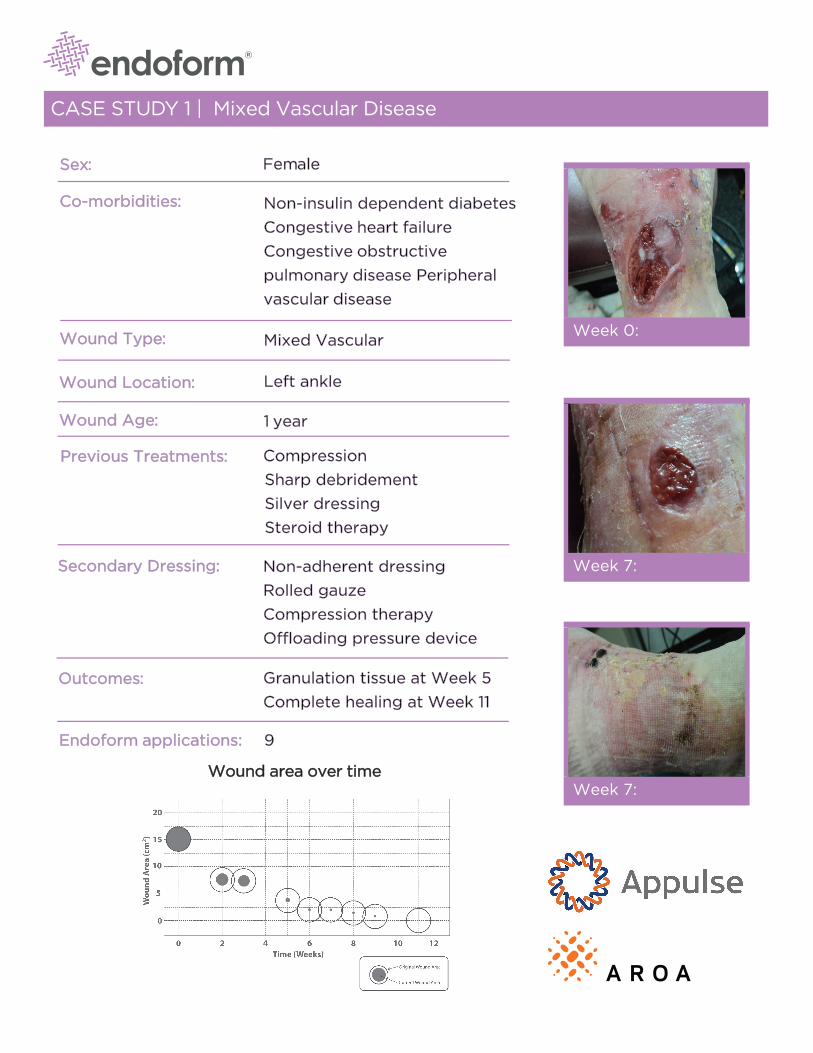
CASE STUDY 1 | Mixed Vascular Disease
Sex:
Co-morbidities:
Wound Type:
Wound Location:
Wound Age:
Previous Treatments:
Secondary Dressing:
Outcomes:
Endoform applications:
Female
Non-insulin dependent diabetes
Congestive heart failure
Congestive obstructive
pulmonary disease Peripheral
vascular disease
Mixed Vascular
Left ankle
1 year
Compression
Sharp debridement
Silver dressing
Steroid therapy
Non-adherent dressing
Rolled gauze
Compression therapy
Offloading pressure device
Granulation tissue at Week 5
Complete healing at Week 11
9
Wound area over time
Week 0:
Week 7:
Week 7:

Initial PreparationThe wound was surgically debrided down to viable tissue and irrigated with hypochlorous acid
solution and treated with a silver dressing and compression. The wound was assessed for visible
signs of infection (i.e., absence of swelling, pain, purulent drainage, or tracking into the deep tissue
planes). The wound had to remain free of infection to start using the Endoform dermal template.
Silver dressing treatments were stopped at this time.
Endoform dermal template ApplicationUsing aseptic technique, Endoform dermal template was trimmed to roughly overlap the wound
margins, placed on the wound bed and rehydrated with sterile saline. Following hydration, the
color of the dressing changed from white to opaque. Light pressure was applied to the dressing to
ensure that it conformed to the underlying wound bed. The dressing was covered with a non-
adherent secondary dressing. Compression stockings, exudate control and offloading were used as
required.
Follow-UpThe patient received weekly follow-up, during which time the wound was debrided as required and
irrigated to remove loose material. The Endoform dermal template was reapplied on a weekly basis.
Changes in the wound granulation tissue, epithelial tissue and wound dimensions were monitored
and recorded using digital photography.
ObservationsIn approximately three days, the dressing had adhered to the underlying wound bed. After seven
days, the dressing was completely integrated into the wound bed. In some cases, only remnants of
the dressing remained as an off-white gel that was allowed to remain in place during subsequent
applications of Endoform dermal template.
Case provided by:
Liden BA, Ward BR, May BCH; Early Clinical Findings From The Use Of Endoform Dermal Template (Ovine Forestomach Matrix) To Treat Recalcitrant Wounds; Presented at Symposium on Advanced Wound Care, April 14-17, 2011 Dallas, TX.
Manufactured for: AROA BIOSURGERY INC
340 Progress Drive, Manchester, CT 06042 1-860-337-7730
www.aroabio.com
©2018 Aroa Biosurgery Limited
RX Only. Prior to use, be sure to read the entire Instructions for Use package insert supplied with the product.
For product questions, sampling needs, or detailed clinical questions concerning our products in the US, please call 1-860-337-7730
HCPCS are for reference only and subject to change.
Endoform® is a registered trademark of Aroa Biosurgery Limited.
Endoform® Dermal Template is marketed in the USA by Appulse
CASE STUDY 3 | Mixed Vascular Etiology
Sex:
Co-morbidities:
Wound Type:
Wound Location:
Wound Age:
Previous Treatments:
Secondary Dressing:
Outcomes:
Female
Diabetes
Congestive heart failure
Venous reflux
Mixed vascular
Left lower medial leg, anterior ankle
1+ year
Compression
Sharp debridement
Enzymatic debrider
Growth factos
Skin substitute (x4)
Silver dressing
Non-adherent dressing
Rolled gauze
Granulation tissue at week 4Complete Healing at week 9
Endoform applications:
Wound area over time
Week 0:
Week 4:
Week 9:
6

Case provided by:
Liden BA, Ward BR, May BCH; Early Clinical Findings From The Use Of Endoform Dermal Template (Ovine Forestomach Matrix) To Treat Recalcitrant Wounds; Presented at Symposium on Advanced Wound Care, April 14-17, 2011 Dallas, TX.
Manufactured for: AROA BIOSURGERY INC
340 Progress Drive, Manchester, CT 06042 1-860-337-7730
www.aroabio.com
©2018 Aroa Biosurgery Limited
RX Only. Prior to use, be sure to read the entire Instructions for Use package insert supplied with the product.
For product questions, sampling needs, or detailed clinical questions concerning our products in the US, please call 1-860-337-7730
HCPCS are for reference only and subject to change.
Endoform® is a registered trademark of Aroa Biosurgery Limited.
Endoform® Dermal Template is marketed in the USA by Appulse
Initial PreparationThe wound was surgically debrided down to viable tissue and irrigated with hypochlorous acid
solution and treated with enzymatic debriding agent and compression. The wound was assessed
for visible signs of infection (i.e., absence of swelling, pain, purulent drainage, or tracking into the
deep tissue planes). The wound had to remain free of infection to start using the Endoform dermal
template. Previously used dressings and enzymatic debriding treatments were stopped at this time.
Endoform dermal template ApplicationUsing aseptic technique, the Endoform dermal template was trimmed to roughly overlap the
wound margins, placed on the wound bed and rehydrated with sterile saline. Following hydration,
the color of the dressing changed from white to opaque. Light pressure was applied to the dressing
to ensure that it conformed to the underlying wound bed. The dressing was covered with a non-
adherent secondary dressing. Compression stockings, exudate control and offloading were used as
required.
Follow-UpThe patient received weekly follow-up, during which time the wound was debrided as required and
irrigated to remove loose material. The Endoform dermal template was reapplied on a weekly basis.
Changes in the wound granulation tissue, epithelial tissue and wound dimensions were monitored
and recorded using digital photography. The wound was monitored for a further four weeks.
ObservationsIn approximately three days, the dressing had adhered to the underlying wound bed. After seven
days, the dressing was completely integrated into the wound bed. In some cases, only remnants of
the dressing remained as an off-white gel that was allowed to remain in place during subsequent
applications of Endoform dermal template.

Patient: 53-year-old male, presented with a
venous ulcer wound to the left ankle
Results:
• Initial wound measurement after debridement was 1.0cm x1.0cm x 0.2cm
• After seven weeks of treatment, wound had decreased to0.2cm x 0.2cm x 0.1cm
CASE STUDY 9 Venous Ulcer
Wound characteristics and prior treatment:
The wound was treated initially with zinc-paste-impregnated gauze and an alginate dressing
After debridement, wound measures 1 cm x 1 cm x 0.2 cm. Endoform dermaltemplate treatment begun
Treatment:
• Wound cleansed with normal saline
• Sharp debridement to remove devitalized wound base
tissue
• Endoform dermal template was applied, covered with a
secondary foam dressing, and secured with tape
Week 3, wound measures 0.7 cm 0.8 cm x 0.1 cm
Week 4, wound measures 0.6 cm 0.9 cm x 0.2 cm
Week 5, wound measures 0.4 cm 0.8 cm x 0.2 cm
Week 7, wound measures 0.2 cm 0.2 cm x 0.1 cm

Case provided by:
Maeve Curran, PT, CWS, CLT; Desert Regional Medical Center, Palm Springs, CA
©2018 Aroa Biosurgery Limited
Manufactured for: AROA BIOSURGERY INC
340 Progress Drive, Manchester, CT 06042 1-860-337-7730
www.aroabio.com
RX Only. Prior to use, be sure to read the entire Instructions for Use package insert supplied with the product.
For product questions, sampling needs, or detailed clinical questions concerning our products in the US, please call 1-860-337-7730
HCPCS are for reference only and subject to change.
Endoform® is a registered trademark of Aroa Biosurgery Limited.
Endoform® Dermal Template is marketed in the USA by Appulse
CASE STUDY 9 Venous Ulcer

Pub�,, USh-.llbl'l'ol ..... .,.
PubMed �--------------------�--H .... , ....... H,, If> Advanced
Foonat: Abstract .. Send to ...
� 2017 Nav;29(11) $37--$42
Proactive and Early Aggressive Wound Management: A Shift in Strategy Developed by a
Consensus Panel Examining the Current Science, Prevention, and Management of Acute and
Chronic Wounds.
illlllll.GA.��.Qmjgl!Ulll,�.Zill1amallJ.�.=·��.liilllm,llUf.
Abstract
Full text links
I �, .. ,,_ti:: I .WOUNDS
Save items
Add to Favorites
Similar 8rticles
Help
Normal wound healing is aocotnplished th1ough a series of well-eoordinat&d , ptogressive events wi1h overlapping phases. Chronic wounds are desaibed as not progressing lo healing or nol being responsive lo mal\agement in a timely manner. A consensus panel 01 multidisciplinary wound care professionals was assembled to (1) educate wound ca.re practitioners by identifying key principles of the basic science of chroni<: wound pathophy-$iology, highlighting the impact of metalloproleKlases and biofitms, as well 8$ the role of the e�racellular matrix; and (2) equip practitioners with a syslematic strategy for lhe prevention and heating ol acule injuries and chronic wounds based upon scientific evidence and the panel members' expertise. An algorithm is presen1ed that represents a shifl in strategy to proactive and earty agg,essive wound management Wit11 proactive maMgement. adjuncl therapies a,e applied preemptively to acute injuries to reduce wound duration and risk ol ctironicity. For existi� chronic wounds. earty aggressive wound management is emplOyEtd to bleak the pattioptiysiology cycle and drive wounds Ioward healing. Reducing biol>urden through debridernent and bioburden managemenl and using collagen dressings to balance protease activity prior to lhe use of advanced modalities may enhance their effectivefless. This earty aggressive wound management slrategy is reoommend&d for patients at high risk lor chronic: wound development al a minimum. In their own practices. lhe panel members apply lhis systemalic stralegy for aJI patients presenting with acute injuries or Chronic wounds.
Community-based care lor chroniC wound management: [Ont Health Temnol Assess ser.
PMID 29166254 Free full text
Management ot chronic pressure �s: an evidence-baS< [Ont Health Temnol Assess Ser.
EWMA Documenl: Nogative Pressure Woond Therapy. IJ -.nc1 ca,e. 20111
cmmm Systematic revie'NS ol womd caie management: (3) , !Health Tect,nol Assess. 2000)
C!ll'ElJ Recommenclalions f"' the management of biofilm: a consenSU$ do< IJ _,ncl care 2016)
see ,ev1ews ...
Seeal ...
WOUNDS •la.A\\l '7 < � I 11 I q JCll ;,r., \L in
HCI.IE SUBSCRIBE l'BUE� \1ULT1MECIA EDLIC)TlON U0UlU3
Proaclive and Early Aggressive Wound Management A Shifl in Strategy Developed by a Consensus Panel Examining tho Current Science, Prevention, and Management of Acute and Chronic Wounds
!IIGN JP LCG M
1-W'IU OOMMI.JNl(.;,\110�
!{emote errperature Moortonng 1n mati.�c i=oot UlcN C•c-tcc-J"'1
----------------------------ill 11'11.�01/1,?"l�I �Orwc;�
PROACTIVE AN a EARLY AGGRESSIVE WOUND MANAGEMENT: A Shift in Strategy Des eloped tiy a Consensus Panel
E<ilmining the Current Science, P,e,ent,on and Management of Acute and Chronic Wound,
Abstrut l11bodud.iur1. i:l.llQh; r�ll Llu:Mi. (OF Ji.: i:41'::i ass:dated \\'itt ioa..at,a,d 1101:,d ::y. n'IOl'talir,'. ;md resource utilization. Rerrcte f�raftlU! rrvdiulnn :RT\11"1 :'I H <!\1,1rm,�r. t'i::rM :md r<'!N'lrrrnr.ndr.£1 w1n1,1u11�11l L•f �-li.111U,11J p1::vt11lt.1liv.: ·L•ul c,ara torhi3h-<i�•: p�Llations :hat car dGt;;ct lhe i111f amr· a;:ion poeceding and IIN'.:-, ..... r;;n·lfl!] 11FIJ� r.:-.'lini1P r!'.=o,1inf1
MOST roruLAR ARTl::.�s
tlnrfor�i;ndln!J Ol!'ll'W'!tk.lndur.Tlon nf Cdl•JliJ1 Si.:m.:�i.:cm;i:; A Cund:.c R•.:vi�w ■-OJUay:Q'V/101-li?�
Chairaderiitic!o ot �U19ical Site l11�ction rcllo·1oin!=j Cclon-ctal Surge,r/ in o TErtief'l c.,mrP.r! F:rriP.:rwiP.il�'lflF:r:rrum fU nr.10mr.•�P.-1J1Uth.n:i11f 8ai.;Lc1i;:, Culiitit:. in Dbt.•c::;t.• ■ -.. �.., '.&nflnl "'"""""'•
Edito,iol Meg�e: Yoo U'fom to Spit on r.tyWr,un:t'? ■ ---:sa,,1·2111s1r1 ni,lid!;
tdiluti;:11 MY6ti,i,t\J�; Huv, Ou Yoo t1;-.11rJI� Adl"&ft.ity'i'
Recommended