
Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 1
UNIT I: INTRODUCTION AND OVERVIEW OF THE COURSE
A. Definition and Scope of Clinical Pharmacy
Defined as the dimension of pharmacy concerned with the science and
practice of rational medication use
Health science discipline in which pharmacist provide patient care that:
o optimizes medication therapy
o promotes health and wellness and
o disease prevention
the practice embraces the philosophy of Health Care or Pharmaceutical Care;
it blends a caring orientation with specific therapeutic knowledge, experience
and judgment for the purpose of ensuring optimal patient outcomes
as a discipline, clinical pharmacy also has an obligation to contribute to the
generation of new knowledge that advances health and quality of life
Clinical Pharmacy encompasses the care for patient in Health Care settings:
they possess in-depth knowledge of medications that is integrated with a
foundational understanding of the biomedical, pharmaceutical, socio-
behavioral and clinical science
To achieve designed therapeutic goals, the clinical pharmacist applies:
o evidence-based therapeutic guidelines,
o evolving sciences
o emerging techniques and
o relevant, legal, ethical, social, cultural, economic and professional
principles
assume responsibility and accountability for managing medication
therapies in direct patient care settings whether practice independent on is
consultative/collaborative with other health care professions
In the USA, physicians do the diagnosis and pharmacists prescribe the
medication. Pharmacists should be familiarized with the different
diagnostic and screening tests and the interpretation of their corresponding
results.

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 2
B. Brief History and present status of Clinical Pharmacy
i. International Setting
1928
Pharmacists at the University of Iowa Hospital began
participating in patient rounds
1960 1st use of patient medication profiles in community pharmacy practice was done by Eugene White
1st office-based pharmacy practice opened in Berryville, VA by Eugene White
1962 University of Kentucky Medical Center opened the first
Drug Information Center
1965 University of Iowa Drug Info Service (DIS) was created
1971 University of Missouri – Kansas City began instructing medical students and residents in the safe, effective and
economical use of drugs
1972 Prescribing authority was granted to pharmacists in Indian
Health Service who completed Pharmacist Practitioner Training Program
1974 Pharmacist-conducted drug regimen reviews were required
every 30 days for all residents of skilled nursing facilities
1977 1st Clinical Pharmacokinetic service was recognized by
third-party player
1994 Pharmacists began training to administer immunizations in
Washington State
2001 Pharmacists were represented on epilepsy treatment teams
2004 United Network for Organ Sharing (UNOS) that a
pharmacist be on all transplant teams
2007 IDSA (Infectious Diseases Society of America) recommended that pharmacists be core members of antimicrobial stewardship teams
2008 Pharmacists began serving as medication safety officers
ii. Philippine Setting

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 3
1970 – Clinical Pharmacy Practice / Profession started at Makati Medical
Center founded by Dr. Siopin Co
1975 – Dr. Siopin Co’s “Clinical Pharmacy as a set up in a selected
medical center: An Assessment” was published at the Philippine Women’s
University
At present, University of Santo Tomas and Adamson University offer the
1-year post graduate course BS Clinical Pharmacy which includes
advanced internship, clinical experience and immunization
iii. Present Barriers to Clinical Pharmacy
Lack of interest of top management on the concept of higher cost
Other professionals are unhappy
Lack of incentives to pharmacists
Lack of training or specializing areas to develop

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 4
UNIT II: CONCEPTS IN CLINICAL PHARMACY
A. Evidence based medicine and therapeutic guidelines
Evidence-based medicine (EBM) emphasizes the use of evidence from
well designed and conducted research in healthcare decision-making. The term
was originally used to describe an approach to teaching the practice of medicine
and improving decisions by individual physicians. Use of the term rapidly
expanded to include a previously described approach that emphasized the use of
evidence in the design of guidelines and policies that apply to populations
("evidence-based practice policies"). It has subsequently spread to describe an
approach to decision making that is used at virtually every level of the healthcare
system.
Whether applied to medical education, decisions about individuals,
guidelines and policies applied to populations, or administration of health services
in general, evidence-based medicine advocates that to the greatest extent possible,
decisions and policies should be based on evidence, not just the beliefs of
practitioners, experts, or administrators. It promotes the use of formal, explicit
methods to analyze evidence and make it available to decision makers. It
promotes programs to teach the methods to medical students, practitioners, and
policy makers.
a. The 5 Step Process of Evidence Based Medication
1. Translation of uncertainty to an answerable question and includes critical
questioning, study design and levels of evidence.
2. Systematic retrieval of the best evidence available
3. Critical appraisal of evidence for internal validity that can be broken
down into aspects regarding:
Systematic errors as a result of selection bias, information bias and confounding
Quantitative aspects of diagnosis and treatment
The effect size and aspects regarding its precision
Clinical importance of results
External validity or generalizability
4. Application of results in practice
5. Evaluation of performance
b. Evidence Reviews

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 5
Once all the best evidence is assessed, treatment is categorized as:
1. likely to be beneficial,
2. likely to be harmful, or
3. evidence did not support either benefit or harm.
c. Assessing the Quality of Evidence
From the US Preventive Service Task Force
Level I: Evidence obtained from at least one properly
designed randomized controlled trial.
Level II-1: Evidence obtained from well-designed controlled trials
without randomization.
Level II-2: Evidence obtained from well-designed cohort or case-
control analytic studies, preferably from more than one center or research
group.
Level II-3: Evidence obtained from multiple time series designs with or
without the intervention. Dramatic results in uncontrolled trials might also
be regarded as this type of evidence.
Level III: Opinions of respected authorities, based on clinical experience,
descriptive studies, or reports of expert committees.
d. Therapeutic Guidelines
Reducing Medication Errors
o Read the prescription carefully and thoroughly. If in doubt of the
item, call the doctor to verify before dispensing. Always apply a
system of double checks
o Listen attentively. Certain brand names and generic names sound
alike
o Organize how products are stored in the pharmacy and storage. Use a
systematic labeling system if necessary and store common
medications with uncommonly used strengths/preparations separately
o Maintain a list of potential problematic drugs stored in the pharmacy.
Familiarize the personnel with the list and constantly update the list
1. Medication orders should be complete with regard to patient
information, drug name and dosage. It should be reviewed by the
prescriber for accuracy and legibility immediately after writing.
2. Instructions should be written out rather than using nonstandard or
ambiguous abbreviations

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 6
3. Vague instructions, such as “take as directed”, should not be used;
instead, more drug-specific instructions should be taken
4. Exact dosage strength (ex. 20mg) rather than dosage units (ex. 1
tablet) should be specified
5. Exact nomenclature for drug names (nonproprietary or proprietary)
should be used, rather than fabricated drug-name abbreviations
6. A leading zero should always precede a decimal expression of less
than 1 (ex. 0.5mL); conversely a terminal zero should never be used
(ex. 5.0mL), because failure to note the decimal would result in a ten-
fold error. When possible, avoid the use of decimals (ex. Prescribe
500mg instead of 0.5g)
7. The word units (ex. 10 units of regular insulin) should be spelled out
rather than abbreviated with a U, which could be misinterpreted as a
zero (misinterpreted as 100 units rather than the 10 units intended).
8. Use of the metric system should be required.
Medications are not used Correctly when:
o Improper Use – happens when consumers do not understand or
follow directions for taking medications, and often results in serious
consequences. For example, use of non-steroidal anti-inflammatory
drugs (NSAIDs) including aspirin and ibuprofen for pain, without
realizing that improve use of these medications can lead to kidney
failure or gastrointestinal bleeding
o Overuse – happens when too much of the wrong strength of a
medication is taken. For example, most people do not benefit from
taking antibiotics for colds and other respiratory problems, but more
than 23 million prescriptions a year are given to patients for these
conditions. Overuse of antibiotics can lead to drug-resistant strains of
bacteria and potentially life-threatening infections.

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 7
o Underuse – happens when a medication is not taken as it should be.
Skipping does of a medication or taking the wrong medication can
ultimately lead to hospitalization or other serious consequences. This
is a growing problem, especially among children. The majority of
medication errors reported in schools are due to children missing
doses.
Useful patient compliance aids
o Labeling – auxiliary labels that provide additional information
regarding the use, precautions and or storage of the medication will
contribute to the attainment of compliance
o Medication Calendars & Drug Reminder Charts – various forms
have been developed and are designed to assist patients in self-
administering drugs to help patients organize their medications and to
monitor self-administration of drugs
o Special Medication Containers, Caps and Systems – special
prescription containers, caps and systems may be effective in
achieving compliance by patients who forget doses or who are
confused by the complexity of the regimen
o Compliance Packing – a compliance package is defined as a
prepackaged until that provides one treatment cycle of the medication
to the patient in a ready-to-use package. It is designed to serve as a
patient-education tool for health professionals and to make it easier
for patients to understand in a ready-use package. It is designed to
serve as a patient-education tool for health-professionals and to make
it easier for patients to understand and remember to take their
medications correctly at home.
o Dosage forms – the development of longer-acting, controlled-release
dosage forms has permitted less frequent administration which
facilitates compliance. The use of transdermal drug delivery systems
permits less frequent administration of medications given by this
route.
Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 8
Recommendations for Pharmacists to advance prescription compliance
o Become proactive about gathering and providing medicine
information. Ask questions that stimulate dialogue, discuss care plans
with patients and use information about patient to make better
decisions
o Provide compliance monitoring and documentation for at least one at-
risk patient per month. Share findings with the patient and with
his/her other healthcare providers
o Work with management to redesign facilities to increase
pharmacist/patient contact, and to provide a private counseling area.
B. Physical Assessment Skills and Interpretation of Laboratory and Diagnostic Tests
results
a. Physical Assessment Skills
Usual Physical Assessment Sequence
a) Vital Signs
b) Appearance, behavior
c) Skin
d) Head
e) Eyes
f) Ears
g) Nose
h) Mouth
i) Neck
j) Breasts
k) Chest and lungs
l) Heart
m) Abdomen
n) Extremities
o) Back and spine
p) Nervous System
q) Mental Status
r) Genitalia and rectum
ii. Inspection, Palpation, Percussion and Ausculation Techniques
1. Inspection – denotes visual surveillance, i.e., inspect the skin
for color, presence of lesions, visible trauma or abnormalities.
2. Percussion – determines the density of a specific area or part
of the body, create a percussion note either by tapping the body
directly with the distal end of the finger (direct percussion) or
by tapping a finger placed on the body (indirect percussion);
only the finger being struck touches the body. The resultant
sound is described using one of four percussion notes:
resonant, dull, tympanic or flat.

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 9
Percussion notes are distinguishable with percussion over areas
of the body that normally produces the notes (percussion over
normal lung tissue produces a dull note; percussion over the
stomach produces and tympanic note; a percussion over large
muscles such as the thigh produces flat notes)
3. Palpation – using hand to feel areas that cannot be seen; can
be performed with the fingertips, palm or back or the hand; use
back of the hand to assess temperature and the fingertips to feel
the lower edge of the liver and the spleen tip.
4. Ausculation – consists of listening either directly with the ear
or indirectly with the aid of a device (typically a stethoscope)
to sounds that arise spontaneously from the body.
iii. Equipments
Equipment Purpose
Flashlight Assess pupillary reflexes; aid in the inspection of the
oropharynxand skin
Ophthalmoscope Perform fundoscopic examination
Otoscope Assess external ear canal and tympanic membrane
Tongue depressor Inspect oropharynx
Watch (digital or sweep
secondhand)
Assess heart and respiratory rate
Thermometer Obtain body temperature
Stethoscope Assess cardiovascular, pulmonary and abdominal
systems
Sphygmomanometer Obtain blood pressure
Reflex hammer Assess neurologic function
Tuning fork Asses neurologic function
iv. Skin
1. Inspection For:
Color (cyanosis, pallor, redness, yellowness)

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 10
Lesions
o Describe lesions according to location, type color,
shape, size, grouping and pattern
Trauma
Abnormalities
2. Palpation For:
Turgor (hydration status)
o Pulling up and quickly releasing a fold of skin
o In a well hydrated patient, the skin quickly returns to
normal
o Takes longer for skin to return if patient is dehydrate
Moistness
Temperature (warm, cool)
Texture (rough, smooth)
Thickness (thick, thin)
Mobility (immobile, mobile, hypermobile)
Edema
o Pressing the tips of one or two fingers into the skin and
noting how long the indentation remains after fingers
are removed.
o A plus scale (1+, 2+, 3+, 4+) to quantify edema, with
4+ for most long-lasting indentations

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 11
3. Lesions
Primary Lesions
Bulla a large (>1 cm),
circumscribed, elevated lesion containing serous
fluid, such as blistering from second-degree burns
Ecchymosis a large (>1 cm),
hemorrhage, bruise
Macule a small (<1 cm),
circumscribed, flat, discolored lesion, such as
a freckle or flat nevus)
Nodule a large (>1cm) solid lesion
that may be below, even with, or above the surface
of the skin
Papule a small (<1cm), elevated,
solid lesion, wart
Patch an area containing
discolored, circumscribed, and flat or elevated groups
of lesions, measles rash
Petechia a small (<2mm)
hemorrhage Plaque a large (>1cm),
circumscribed, elevated and solid lesion; ex: pityriasis rosea
Pustule a circumscribed, elevated
lesion of varying size containing pus; ex: impetigo
Vesicle a small (<1cm), circumscribed, elevated
lesion containing serous fluid; ex: herpes zoster
Wheal an edematous and transitory papule; ex:
hives Secondary Lesions

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 12
Crust mass of dried exudate; ex: impetigo
Excoriation scratch mark usually covered with blood or
serous crusts Fissure linear break in the skin
Keloid hypertrophic scar
Lichenification thickening and roughening
of the skin with increased visibility of normal skin lines
Scale dead epidermal cells; ex: dandruff
Scar area in which normal skin tissue has been replaced
by connective tissue
Ulcer irregularly sized and shaped excavation that
extends below dermal skin layer, ex: pressure sore
Other Lesions
comedo (black head)
pilosebaceous follicular plug of sebaceous and
keratinous material
milium (white head)
small (1-2mm) nodule with no visible opening
nevus (node) flat or elevated pigmented lesion
Osler's node small, raised, discolored, tender lesion on the pads
of the fingers and toes associated with bacterial endocarditis
telangiectasias dilated superficial blood vessels
4. Fingernail and Toenail Terms

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 13
Beau's Lines transverse horizontal depressions associated with severe illness
clubbing increased angle (>180 degrees) between the base of the nail and the nail bed; associated
with chronic arterial desaturation (ex: chronic obstructive pulmonary disease [COPD]
koilonychia spooning of the nails associated with iron deficiency anemia
onycholysis separation of the nail from the nail bed associated with trauma, malnutrition and
thyroid disease splinter hemorrhage red or brown linear streaks in the distal
extremity of the nail bed; nonspecific
v. Head and Neck
1. Skull
Inspection: size, contour, shape and evidence of trauma
Palpation: lumps, bumps and evidence of trauma
2. Hair
Inspection: quantity, texture and distribution
Palpation: texture (coarse, fine, dry, oily)
3. Scalp
Inspection: lesions and scales
4. Face
Inspection: expression, symmetry, movement, lesions and
edema
5. Neck
Inspection: symmetry, masses and enlargement of the
parotid and submaxillary gland and lymph nodes.
Note position and size of the sternomastoid muscles and the
carotid arteries and the position of the trachea
Ausculation: enlargement; thyroid bruit may be present
6. Nose
Inspection: symmetry, inflammation and lesions
Transluminate the maxillary sinuses by shining a bright
light in the mouth

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 14
Normal maxillary sinuses appear as dull-red crescent-
shaped glowing areas under each eye
Transluminate frontal sinuses by placing a light source
under the medial aspect of each eyebrow.
Normal frontal sinuses appear as glowing red areas above
each eye
7. Ears
Inspection: lesions, trauma, size and countour; edema,
color, insects, discharge, foreign bodies in the canal
Palpation: nodules
8. Hearing
Check hearing using tuning fork in one ear at a time
9. Mouth and Pharynx
Inspection:
o lips and mucosa for color, ulcerations, hydration and
lesions
o teeth and gums for color, bleedings, inflammation,
caries, missing teeth, ulcerations and lesions
o tongue for color, symmetry, ulcerations and lesions
o breath for odor
alcoholic – alcohol intoxication
ruinous – uremia
sweetish – diabetes with ketoacidosis
musty – sever parenchymal liver disease
10. Eyes
Inspection: visual acuity, eye movement, size, color,
lesions, bleeding, specks
11. Terminologies
acromegaly pituitary disorder characterized by amasive face with enlarged lower jaw, prominent nose
and eyebrows, and coarse facial features

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 15
astigmatism condition characterized by unequal curvatures of the cornea
AV nicking abnormality visualized on fundoscopic examination associated with hypertension; at
arteriovenous crossings the vein appears to stop abruptly on either side of the arteriole
AV tapering abnormality visualized on fundoscopic examination and associated with hypertension;
at arteriovenous crossings the veins appears to taper off on either side of the arteriole
Bell's palsy unilateral paralysis of the facial muscle
Chvostek sign contraction or spasm of the facial muscles associated with tetany and hypocalcemia;
elicited by tapping the face sharply with a finger just in front of the external auditory
meatus over the facial nerve
conjunctival injection dilated conjunctival vessels
copper wires abnormality visualized on fundoscopic examination and associated with hypertension;
coppery strip of light appears along the vessel
corneal arcus thin, gray-white circle around the cornea; associated with aging
deep hemorrhages abnormality visualized on fundoscopic examination and associated with diabetes;
appears as small irregular red spots in the retina
exophthalmos abnormal protrusion of the eyeball; associated with Grave's disease
fetor hepaticus musty odor of breath associated with parenchymal liver disease
fissured tongue increased tongue fissures; benign; sometimes associated with aging
flame hemorrhage abnormality visualized on fundoscopic examination associated with hypertension;
appears small, linear hemorrhages in the retina
geographic tongue denuded areas of papillae; benign
hairy tongue elongated papillae; benign; associated with antibiotic therapy
hirsutism increased hair growth in androgen-sensitive areas (ex: beard or mustache areas); associated
with ovarian, adrenal, thyroid and pituitary disorders and some medications

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 16
hyperopia Farsightedness
Klopik's spots small blue-white spots with red margins found on the mucous membranes near the parotid
duct; associated with measles; appear before skin lesions are visible
microaneurysms abnormality visualized on fundoscopic examination associated with diabetes; appear as
tiny red spots in the macular area
muddy sclera brownish sclera; benign; commonly found in dark-skinned individuals
myopia nearsightedness
normocephalic, atraumatic
physical examination finding meaning that the head is a normal size and shape and no
evidence of trauma is present
palpebral fissure the space, when the eyes are open, between the upper and lower eyelids
periorobital edema puffness of the upper and lower eyelids
Rinne test hearing test that compares air and bone conduction
smooth red tongue finding associated deficiencies of vitamin B12, niacin and iron
Weber's test hearing test that compares bone conduction in both ears
xanthelasma yellow, raised, well circumscribed plaques found in the skin around the eyelids; associated
with hypercholesterolemia
vi. Chest and Lungs
1. Inspection:
chest throughout at least one complete inspiratory-
expiratory cycle
chest wall abnormalities, accessory muscle use, the
anteroposterior diameter, and skeletal abnormalities
2. Percussion:
Intercostals spaces to assess lung density
Percussion over normal lung tissues create a loud, low-
pitched, resonant note
Percussion over areas of lung with increased air volume
(ex: emphysema) creates a very loud, low-pitched, hyper-
resonant note

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 17
Areas of consolidation (fluid) produce a dull or flat
percussion note
Shifting dullness is associated with freely moving fluid
within the pleural cavity
Assess all lobes, compare left and right lobes
Determine diaphragmatic location and excursion
Determine location of each diaphragm with lungs fully
expanded and emptied
Normal diaphragmatic excursion is about 3-5cm for
females and 5-6cm for males
Right diaphragm is slightly higher than the left
3. Palpation
Masses, pulsations, crepitation and tactile fremitus
Assess for tactile fremitus, place the palm of the hand on
the chest and have the patient say “ninety-nine” or “one-
two-three”
4. Ausculation
Ausculated with stethoscope
On posterior chest, ausculate between the scapulae and
vertebral column. Place the diaphragm of the stethoscope
flat against the chest wall and instruct patient to breathe
deeply and slowly through the mouth each time the
stethoscope touches skin
Assess at least one complete respiratory cycle over each
anterior and posterior lobe, comparing right and left sides;
assess more thoroughly if abnormalities are detected
Breath sounds are tracheal, bronchial, bronchovesicular or
vesicular
Breath sounds are distinguishable through auscultation over
areas of the lungs that normally produce the sounds
These breath sounds are considered abnormal if heard over
other areas of the lungs
Other abnormal breath sounds include wheezes, rhonchi,
stride and cackles
Pleural friction rub, created when the visceral and parietal
pleural rub together, sounds like creaking leather and is
heard best at the base of the lungs
Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 18
Voice sounds (egophony, whispered pectoriloquy) are
transmitted more clearly over areas of consolidation; vocal
resonance is decreased over areas of hyperinflation
5. Terminology
apnea absence of respiration
barrel chest anteroposterior diameter ratio of 1:1; associated
with diseases characterized with air trapping; ex: COPD
Biot's respiration irregular respiration; may occur in meningitis
bradypnea abnormally slow respiratory rate with regular
rhythm and normal depth of breathing; associated with CNS (central nervous system) depressants and elevated intracranial pressure
bronchial breath
sounds
loud, high-pitched, normal breath sounds heard
over the manabrium; normal inspiratory/expiratory ration of 1:3
bronchovesicular
breath sounds
normal breath sounds heard over the main stem
bronchi just distal to the central airways softer and lower pitched than tracheal breath sounds with equal inspiratory and expiratory duration
and pitch Cheyne-Stokes
respiration
cyclic, abnormal respiratory patter
characterized by a gradual increase in the depth and rate of respiration followed by a gradual decrease in the depth and rate of respiration
followed by gradual decrease in the depth and rate ending in apnea; characteristic of diseases
that affect the central respiratory centers
consolidation increased density
cackles discontinuous, short-duration, bubbling sounds
crepitation Cackling
dullness or flatness soft, medium-pitched percussion notes elicited
over areas of increase density
egophony altered vocal resonance over areas of
consolidation; the spoken "e-e-e-e" is transmitted as "a-a-a-a"
eupnea normal respiration
funnel chest (pectus
excavatum)
finding in which the lower part of the sternum
is depressed
hypernea increased depth and rate of respiration

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 19
hyperresonance loud, low-pitched percussion note elicited over areas of increased air volume
Kussmaul's breathing deep, rapid respiration; characteristic of coma and diabetic ketoacidosis
kyphoscoliosis combined kyphosis and scoliosis
kyphosis abnormal curvature of the spine with backward convexity
pigeon chest anterior displacement of the sternum
pleural friction rub abnormal, creaking leatherlike sound produced when the inflamed surfaces of the visceral and
parietal rub against one another
resonance loud, low-pitched percussion note elicited over normal lung tissue
rhonchi coarse, rattling, abnormal breath sounds; often change location after coughing
scoliosis abnormal lateral curvature of the spine
stridor abnormal, high-pitched, continuous lung sounds heard over the upper airway
tachypnea increased respiratory rate
tactile fremitus palpable vocal vibrations felt through the chest wall; increased over areas of consolidation;
decreased over obstructed areas and pleural abnormalities
tracheal breath sounds
very loud and high-pitched harsh normal breath sounds heard over the extrathoracic trachea
tracheobronchial breath sounds
loud-high pitched, normal breath sounds heard over large bronchi; slight pause occurs between
inspiratory and expiratory sounds; inspiratory duration shorter than expiratory duration
Tympanic loud, drum-like percussion notes elicited over hyper-inflated areas
vesicular breath sounds
slow, low-pitched, normal breath sounds heard over peripheral lung tissue; inspiratory duration
longer than expiratory duration
Wheezes abnormal, high-pitched, continuous breath sounds; associated with airway obstruction
whispered pectoriloquy
whispered voice sounds are transmitted more loudly and clearly than normal; associated with
areas of cavitation and consolidation
vii. Cardiovascular System

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 20
1. Inspection:
Chest: Visible cardiac motions
Estimated the jugular venous pressure (JVP
Jugular venous waveforms by observing pulsations in the
jugular vein with the patient supine and head of the bed
elevated to 15 to 30 degrees.
More generally, the right atrial pressure is high
(>15mmHg) if the jugular vein is distended to the jaw
when then patient is seated at a 90-degree angle
2. Palpation
Point of maximal impulse (PMI), local and general cardiac
motion and general cardiac motion and cardiac thrills
PMI normally has a diameter of about 2cm and is located
within about 10cm of the misternal line; use the fingertips
to locate PMI
PMI is easier to identify id the patient sits up and leans
forward than if the patient is supine
Palpate for local and general cardiac motion with the
fingertips with the patient in supine position
Pericardial friction rubs and thrills may be palpable
Radial, carotid, brachial, femoral, popliteal, posterior tibial,
and dorsalis, pedis peripheral pulses
Rate the strength of the pulse as:
o Normal
o Diminished or
o Absent
3. Ausculation
Use stethoscope
Use the diaphragm to assess higher-pitched sounds (S1, S2,
S3, S4)
Peripheral Vascular Pulse Rating Scale
Rating Meaning
0 No pulse palpable
1+ Markedly impaired pulse
2+ Normal pulse
3+ Increased pulse
4+ Bounding (markedly increased) pulse
Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 21
Apply diaphragm tightly to skin
Great deal of practice and experience is required to identify
and distinguish among the variety of normal and abnormal
heart sounds
Heart sounds are very soft; it may help to listen in a quiet
area or to close the eyes to reduce conflicting stimuli
4. Blood Pressure
Peripheral blood pressure is measured with a stethoscope,
blood pressure cuff and mercury or aneroid
sphygmomanometer
Both types of sphygmomanometers are accurate and easy to
use
The mercury column in mercury sphygmomanometers must
be kept vertical and the meniscus read at eye level.
Aneroid sphygmomanometers must be recalibrated
periodically
Use an appropriately sized cuffs
Cuffs that are too short or too narrow falsely elevate the
blood pressure
Cuff width should be about 40% of the limb circumference
and the cuff length should be about 80% of limb
circumference.
How to measure Blood Pressure:
a) Position cuff correctly
b) Place the arterial portion of the cuff directly over the
brachial artery with the bottom of the edge
approximately 2.5cm above the antecubital crease
c) Palpate for the brachial artery before positioning the
cuff to about 20-30 mmHg over the predicted systolic
blood pressure
d) Deflate cuff slowly (approximately 3mm Hg per
second)
e) There are no audible sounds (Korotkoff’s sounds) until
the cuff pressure approximates the systolic pressure

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 22
f) Systolic pressure is the pressure at which at least two
Korotkoff sounds are audible.
g) As pressure falls, the sounds become louder and then
slowly diminish before disappearing altogether
h) Diastolic pressure is the pressure at which the beats are
no longer audible
i) Depending on the clinical situation, it may be necessary
to obtain the blood pressure in both arms or in more
than one body position
j) Do not re-inflate the cuff after partial deflation; cuff re-
inflation causes venous congestion and inaccurate blood
pressure assessments

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 23
5. Terminology
bradycardia a slow (<50 beats per minute) heart rate
bruit abnormal ausculatory sound heard over a blood
vessel; associated with turbulent blood flow
crescendo,
decrescendo murmur
murmur that increases and then decreases in
intensity
diastolic murmur murmur heard during diastole
ejection clicks abnormal heart sounds caused by dilation of the
aorta and pulmonary arteries
gallop rhythms exaggerated diastolic heart sounds
holosystolic murmur murmur heard throughout systole
Hypertension elevated blood pressure
Hypotension low blood pressure
midsystolic clicks abnormal heart sounds caused by floppy mitral
valves
opening snap abnormal diastolic heart sound caused by the
opening of a stenotic mitral valve
orthostatic
hypotension
fall in systolic blood pressure of 15mmHg or
more when the patient assumes a more upright position
pansystolic murmur murmur heard throughout systole
pericardial friction rub
abnormal sound created when the visceral and parietal pericardial membranes rub against one another
PMI right ventricular thrust (apical impulse)
pulsus alternans regular alteration of high and low pulse beats; associated with heart failure
pulsus paradoxus decreased systolic blood pressure with inspiration; normally about 5 mmHg
regurgitant murmur murmur produces by backflow of blood across an incompetent valve
S1 first heart sound; produced by mitral and tricuspid valve closure
S2 second heart sound; produced by aortic and pulmonic valve closure
S3 third heart sound; produced by sudden distention of the ventricular wall during ventricular filling; associated with heart failure

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 24
S4 fourth heart sound; produced by increased left ventricular end-diastolic pressure and loss of
ventricular distensibility; associated with hypertension
split S2 finding in which both components of the second heart sound (aortic and pulmonic) are
distinguishable; may result from deep inspiration and any disease that delays the
closure of the pulmonic valve
stenosis murmur murmur produced by pathologic narrowing of the orifice of the valve
systolic ejection murmur
murmur produced by increased flow across a normal valve, valvular or subvalvular stenosis;
or other deformity of the valve
systolic murmur murmur heard during systol
tachycardia rapid (>100 beats per minute) heart rate
Thrill palpable variations produced by turbulent blood flow
viii. Breasts and Axillae
1. Inspection:
Breasts with the patient in sitting and supine position:
o Size
o Symmetry
o Contour
o Appearance of the skin
Abnormal findings:
o Visible masses
o Dimpling
o Localized flattening
o Rashes
o Ulcers
o Discharge from nipple
2. Palpation
Nodules, indurations and areas of tenderness or increased
warmth
Axillary lymph nodes, including the pector, subscapular
and lateral groups are located high in the axilla close to the
ribs
Palpate nodes for:

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 25
o Size
o Consistency
o Tenderness
3. Terminology
Gynecomastia hypertrophy of breast tissue; associated with
liver cirrhosis, Addison's disease, Klinefelter's syndrome and some medications (ex: spironolactone)
Mastodynia painful breasts
peau d'orange breast skin with an organge-peel appearance
(prominent pores); indication for lymphatic obstruction and is an important sign of malignancy
Retraction dimpling of the skin, nipple retraction or inversion
ix. Abdomen
1. Inspection
Appearance of the skin
umbilicus and
abdominal contour (scaphoid, protuberant)
note: visible aortic and hepatic pulsations, persistent waves,
and fluid shifts
Free fluid in the peritoneal cavity may shift with position,
causing bulging at the flanks when the patient is supine
2. Ausculation
Bowel sounds and abdominal bruits
o Produced by the movement of fluid of air in the bowel,
vary from low rumbles in loosely stretched intestines to
high-pitched tinkling sounds in tightly stretched
intestines

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 26
o Normal bowel sounds occur approximately every 10
seconds
o Ausculate for 2 minutes if normal bowel sounds are
present and for 3 minutes if bowel sounds are absent
Quadrant Structure
Right upper quadrant Liver, gallbladder, a portion of the ascending colon, a portion of the transverse colon,
pylorus, duodenum, head of pancreas, right adrenal gland, upper pole of the right kidney
Right lower quadrant Appendix, cecum, portion of the ascending colon, right ureter, lower pole of the right
kidney, bladder (if enlarged), right ovary, right fallopian tube, uterus (if enlarged), right
spermatic cord Left upper quadrant Liver, spleen, stomach, body of pancreas,
portion of transverse colon, portion of
descending colon, left adrenal gland
Left lower quadrant Sigmoid colon, portion of descending colon, lower pole of left kidneyy, left ureter, bladder
(if enlarged), left ovary, left fallopian tube, uterus (if enlarged), left spermatic cord
3. Percussion
Determine liver span and to differentiate between
abdominal fluid and air
Percussion over the liver produces a dull note
Percussion over air-filled loops of bowel produces a hollow
tympanic note
Normal liver span along the right midclavicular is about
10cm
Percuss each quadrant
o Shifting dullness indicated freely moving fluid
o Air-filled loops of bowel float to the surface of the
abdomen and may obscure abdominal fluid
4. Palpation
Palpate tender or rigid areas with light palpation; use pads
of fingertips with light pressure
Use deep palpation to determine the outlines of the
abdominal organs and to assess the size, shape, mobility
and tenderness of the lymph nodes
Palpate all four quadrants

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 27
5. Terminology
Ascites free fluid in peritoneal cavity
Borborygmi very loud gurgling and tinkling bowel sounds audible without a stethoscope; associated with
hyperperistalsis
caput medusa dilated veins radiating from the umbilicus; associated with portal vein obstruction
costal margin edge of the lower rib cage
costovertebral angle angle formed by the intersection of the rib cage and the vertebral column
epigastric region upper central abdominal area
fluid wave associated with free fluid in the abdominal cavity
hypogastric region lower central abdominal cavity
Peristalsis circular intestinal contractions that propel the intestinal contents forward
puddle sign gravity-dependent pooling of fluid at the surface of the abdomen
rebound tenderness pain elicited when abdominal hand pressure is abruptly removed; associated with parietal peritoneal membrane inflammation
Rovsing's sign right lower quadrant pain elicited by left-sided abdominal pressure; associated with appendicitis
Scaphoid concave-appearing abdomen
shifting dullness dull percussion notes that shift as the patient shifts position associated with free fluid in the
abdominal cavity
spider telangiectasia (spider angioma)
dilated small surface arteries that appear as small red spots with multiple radiating arms;
associated with portal hypertension
Striae discolored stripes of skin that result from ruptured elastic fibers; striae are pinkish or
bluish when relatively new and more whitish when older
suprapubic region abdominal area just above the pubic arch
umbilical region region around the umbilicus

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 28
x. Genitourinary System
1. Inspection
Sacrococcyeal and perianal areas for:
o Lumps
o Ulcerations
o Rashes
o Swelling
o External hemorrhoids
o Excoriations
Female external genitalia:
o Mons pubis
o Labia
o Perineum
o Labia minora
o Clitoris
o Urethral orifice
o Introitus
o For abnormalities:
Lumps
Ulcerations
Rashes
Swelling
Excoriations
Discharge
Female pelvic examination
o Vaginal wall and cervix for color, lesions and shape of
the cervix and cervical os
o Note position of cervix
o Cervical cells may be collected for cytologic evaluation
(Pap smear)
Male external genitalia
o Penis and scrotum
o Contour and abnormalities including lumps,
ulcerations, inflammations, excoriations and swelling
2. Palpation
Anus and rectal walls: tone and tenderness
Prostate: size, consistency and tenderness

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 29
Penis: indurations or other abnormalities and palpate the
scrotal structures (testis and epididymis) for size, shape,
consistency, tenderness
Inguinal and femoral areas: bulges that may indicate
hernias
Uterus and ovaries: size, shape, consistency, masses,
tenderness, mobility
Bimanual examination is performed by palpating the
internal structures between a hand placed on the abdominal
wall and a finger placed in the vagina
Combined rectovaginal examination is performed by
palpating the adnexa, cul-de-sac, and uterosacral ligaments
between a finger placed in the vagina and finger placed in
the rectum
3. Terminology
Angiokeratoma red, slightly raised, pipoint benign scrotal lesions; common after age 50 years
anteverted, anteflexed uterus
normal uterine position
Chancre hard infectious venereal ulcer
Chancroid soft infectious venereal ulcer
condylomata acuminatum
venereal warts
Gravid Pregnant
Hernia protrusion of an organ through the muscullar wall that normally contains the organ
Hydrocele serous fluid containing cavity
Papanicolau (Pap) smear
screening technique for cervical carcinoma
prostatic hypertrophy enlarged prostate
Varicocele enlarged spermatic cord
xi. Musculoskeletal System
1. Inspection
Symmetry, proportion, and muscular development
Note: curvature of the spine
Observe gait, stance, ability to stand, sit, rise from a sitting
position, and grasp objects

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 30
2. Palpation
Large and small joints
Assess joint range of motion
Decreased range of motion is associated with arthritis,
fibrosis in or around the joint, tissue inflammation around
the joint, and fixed (immobile) joints
Increased range of motion indicates increased joint motility
and may be a sign of joint instability
Assess the areas in and around the joints for abnormalities
such as warmth, tenderness, crepitation and deformities
3. Terminology
ADLs activities of daily living; routine activities
such as getting dressed, cleaning the teeth, combing or brushing the hair, bathing and feeding oneself
bouttonniere
deformity
flexion of the proximal interphalangeal
joint with hyperextension of the distal interphalangeal joint
crepitation audible or palpable crackling sounds
dorsiflexion inward flexion
eversion turning of the toes onto the great toe (foot flexed outward)
extension bending of the joint to bring the joint parallel to the long axis
flexion bending of the joint to bring the parts of joint into close approximation
Gait way a person walks
inversion turning of the toes onto the small toes (foot flexed inward)
kyphosis convex backward spinal curvature
List lateral deviation of the spine
lordosis anteroposterior curvature of the spine ex: accentuation of the normal lumbar curve
neutral range of motion
zero degrees
plantar flexion downward flexion of the foot

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 31
radial deviation deviation of the fingers toward the radial bone
rheumatoid nodules firm, nontender, unattached subcutaneous
nodules at pressure points on the extensor of the ulna; association with rheumatoid arthritis
scoliosis lateral curvature of the spine
station way person stands
ulnar deviation deviation of the fingers toward the ulnar
bone
xii. Neurologic System
1. Mental Status
Alertness – determine the patient’s level of consciousness
(awake, alert, confused, unresponsive)
Orientation – determine the patient’s orientation to person,
place, and time. Ask, “what is your name?” “where are
you?” and “what is today’s date?”
Affect – determine the patient’s affect (emotion or mood)
is appropriate to the situation
Speech and Vocabulary – Have the patient say “no ifs,
ands or buts” note patient’s vocabulary throughout the
interview. Ask patient to define a series of increasingly
difficult words
Memory (Immediate, Short-term and Long-term) – to
assess immediate memory, say a list of single-digit
numbers and have the patient immediately repeat the list.
To assess short-term memory, have the patient memorize
three unrelated words. Ask the patient to repeat the words
to ensure that the patient knows the words; then ask the
patient to repeat the words a few minutes later. To assess

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 32
long-term memory, ask patient about an age-appropriate,
well-known historical event
Judgment – ask patient to interpret a single problem that
involves judgment such as “what do you do if you noticed a
stamped, addressed envelope on the sidewalk near a
mailbox?”
Abstract Thinking – ask patient to interpret a common
proverb, such as “a bird in hand is worth two in a bush” or
“health is wealth”; ask patient to explain how items are
similar or dissimilar, “what do bananas, apples and oranges
have in common?”
Calculation – ask the patient to perform serial seven
subtractions, starting from 100 (ex: 100 minus 7 is 93, 93
minus 7 is 86, etc); ask patient to spell “world” backward
Object Recognition – ask the patient to identify several
well-known objects (ex: watch, eyeglasses)
Praxis – ask the patient to perform a multistep motor
activity motor activity (ex: pick up a piece of paper with
your left hand, crumple it and hand it to me)

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 33
2. Cranial Nerves
Cranial Nerve Function Assessment
I-Olfactory sense of smell evaluate olfactory nerve only if the
patient complains of loss of the sense of smell or if the patient has head injury. Ask patient to close his/her
eyes and identify (one nostril at a time) a familiar odor ex: toothpaste,
soap
II-Optic vision test the patient's visual fields and
ability to discriminate between colors
III-Oculomotor pupillary constriction;
upper eyelid elevation; most extraocular movement
evaluate the oculomotor, trochlear
and aducens nerves [III, IV, VI] (known collectively as ocular nerves) as agrpup. Observe the size and shape
of the pupil, pupillary reaction to light and accomodation and extraocular
movements
IV-Trochlear downward and inward
eye movements
V-Trigeminal temporal and masseter
muscles; lateral movement of the jaw
ask patient to clench teeth; test the
patient's ability to sense stimuli (sharp, dull, hot and cold) over the front half of the head
VI-Abducens lateral deviation of the
eye
VII-Facial facial muscle
movements; sense of taste on anterior two thirds of the tongue
assess motor function, observe facial
movements when the patient frowns, smiles, puffs out of the cheeks, whistles and raises the eyebrows;
assess sensory function, test the patient's ability to identify sweet, sour
and salty solutions placed on the tips of the sides of the tongue
VIII-Acoustic hearing and balance test hearing and balance

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 34
IX-
Glossopharyngeal
sensation of the
posterior position of the eardrum, ear, canal,
pharynx, and posterior tongue, including taste; motor activity of the
pharynx
assess quality of speech and the gag
reflex; observe the movement of the soft palate and uvula as the patient
says "aah"
X-Vagus sensation of the
pharynx and larynx; motor function of the palate, pharynx and
larynx XI-Accessory motor function of the
sternomastoid and upper portion of the trapezius muscle
test the patient's ability to shrug his or
her shoulders and turn the chin from side to side against resistance
XII-Hyglossal motor activity of the
tongue
ask the patient to stick our his or her
tongue; note abnormalities such as fasciculations, assymetry, deviations or atrophy
3. Sensory and Motor Function
Assess sensory function by testing the patient’s ability to
detect a variety of sensory stimuli
Ask the patient to close his/her eyes
Start distally and work proximally comparing left and right
sides
Ask the patient to identify when and where he/she is
touched
Use a variety of stimuli, including slight touch, pain and
vibration
Observe the patient for abnormal involuntary muscle
movements, resting muscle tone and strength against
restance
Muscle strength is evaluated using a plus scale, with 0
representing no muscle contraction (complete paralysis) to
5 representing normal muscle strength
Scale Meaning

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 35
0 No muscle contractility (complete paralysis)
1+ Barely detectable muscle contractility
2+ Active muscle contractility; unable to work against gravity
3+ Active muscle contractility; unable to work against gravity but not
against resistance
4+ Active muscle contractility; able to work against gravity and some
resistance
5+ Active muscle contractility; able to work against gravity and full
resistance
4. Cerebellar Function
Finger-to-nose test
Hold your finger about an arm’s length in front of the
patient; ask the patient to quickly and repeatedly touch
his or her nose and then your finger
heel-to-shin test
instruct patient to rub the heel down the shin of the
opposite leg
rapid alternating movements
performed by asking the patient to pronate and supinate
the hands rapidly and repeatedly
Romberg test
Performed by instructing patient to stand with the feet
together, arms extended with palms up, and eyes
closed. Patients with normal posterior column function
maintain the position without the moving their feer for
balance
Gait
Ask the patient to walk straight ahead, turn, return
walking on tiptoes, turn, walk away on the heels, turn,
and return walking heel-to-toe; observe the gait
5. Reflexes

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 36
Reflex Significance
Babinski's (plantar) extrapyramidal tract pathology
Snout diffuse brain disease
Sucking diffuse brain disease
Grasp prefrontal lobe lesions
Hoffman's corticospinal tract dysfunction
Oculocephalic brainstem pathology
Oculovestibular brainstem pathology
Scale Meaning
0 No response
1+ Diminished response
2+ Normal physiologic response
3+ Increased response
4+ Hyperactive; often associated with clonus
6. Terminology
Abduction movement away from the midline of the body
abstract reasoning ability to think beyond concrete terms
Acalcula inability to calculate
Adduction movement toward the midline of the body
Affect observed motion
Agraphia inability to write
Anosmia complete loss of the sense of smell
Anosognasia inability to recognize one's own impairment
Aphasia inability to speak
Aphonia loss of voice
Asterixis involuntary movements characterized by nonrhythmic flapping of the extremities
Athetosis involuntary movements characterized by slow, twisting irregular motions
Attention ability to focus on one activity
Blocking abnormal thought process characterized by sudden interruption of speech in midsentence

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 37
Chorea involuntary movement characterized by brief,
rapid, irregular, jerky motions
Circumstatiality abnormal thought process characterized by
unnecessary detail that delays reaching the point of the thought
Clanging abnormal thought process characterized by the
use of words on the basis of sound instead of meaning
Clonus rhythmic oscillation between extension and flexion
Coma altered state of consciousness characterized by
complete loss of consciousness, unresponsiveness and absence of voluntary
movement Confabulation abnormal thought process characterized by
fabrication of facts or events to fill gaps in the
memory
Confusion abnormality of consciousness characterized by mental slowness, inattentiveness, and incoherent
thought patterns
decerebrate rigidity abnormal body position observed in comatose patients characterized by clenched jaws,
extensions of the neck and legs, adduction of the arms, pronation of the forearms and flexion of
the wrists decorticate rigidity abnormal body position observed in comatose
patients characterized by flexion of the fingers
and wrists and extension and internal rotation of the legs
Delirium abnormality of consciousness characterized by confusion, agitation and hallucinations
Dementia acquired memory impairment
Dysarthria poorly coordinated, irregular speech
Dyscalculia difficulty calculating
Dysgraphia difficulty writing
Dyslexia difficulty reading
Dysphasia hesitancy and error in choosing words when speaking
Dysphonia Hoarseness
Dyspraxia difficulty coordinating body movements
Dystaxia difficulty with muscle coordination
Dystonia abnormal slow, twisting, irregular movements

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 38
Echolalia abnormal thought process characterized by
repetition of words or phrases spoken by others
Eversion turning of the toes onto the great toe (foot flexed
outward)
Extension bending of a joint to bring the joint parallel to
the long axis
Fasculation involuntary movements characterized by fine
twitching that rarely moves a joint
Flexion bending of a joint to bring the parts of the joint
into close approximation
flight of ideas abnormal thought process characterized by an
almost continuous flow of accelerated speech with quick changes of subject
Hemianopsia visual field defect associated with disorders of
the optic chiasm or tract
Hemiplegia paralysis of one side of the body
Incoherence abnormal thought process characterized by
illogical connections and quick changes of subject
intention tremor involuntary movements characterized by tremors that are absent at rest but appear with intentional movement
Inversion turning of the toes onto the small toes (foot flexed inward)
Judgment ability to compare and evaluate alternatives
loose associations abnormal thought processes characterized by repeated shifting to unrelated subjects
Mood sustained emotional state
Myoclonus involuntary movements characterized by sudden, brief, unpredictable jerks
Neologism abnormal thought process characterized but the use of invented words or the use of words with new meanings
Nystagmus involuntary oscillation of the eyeball; described as lateral if the eyeball oscillated from side to side, vertical if the eyeball oscillates up and
down, and rotatory if the eyeball oscillates in a circle
ophthalmoplegias optic eye movements
Paraparesis slight degree of lower extremity paralysis
Paraplegia paralysis of the lower extremities and trunk

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 39
Perserveration abnormal thought process characterized by
persistent repetion of words or phrases
postural tremor involuntary tremor that occurs when the affected
part maintains position
Pronation to place in a downward-facing position
Quadriplegia paralysis of the upper and lower extremities
recent memory memory of information of a few hours or days
remote memory memory of information from the distant past
resting or static
tremor
involuntary movement at rest
Scotoma a visual field defect associated with disorders of
the optic nerve
Stereognosis ability to identify, by touch, small objects placed
in the hand and physical activity and response to stimuli
Supination to place in a upward-facing position
thought content what a person thinks about
Tics involuntary movements characterized by brief,
repetitive movements at irregular intervals
b. Interpretation of Laboratory and Diagnostic Tests
Screening tests Diagnostic tests
Purpose To detect potential disease indicators
To establish presence/absence of disease
Target
population
Large numbers of asymptomatic,
but potentially at risk individuals
Symptomatic individuals to
establish diagnosis, or asymptomatic individuals with a
positive screening test
Test method Simple, acceptable to patients and staff
maybe invasive, expensive but justifiable as necessary to establish diagnosis
Positive
result
threshold
generally chosen towards high
sensitivity not to miss potential disease
Chosen towards high specificity
(true negatives). More weight given to accuracy and precision
than to patient acceptability
Positive
result
Essentially indicates suspicion of disease (often used in combination with other risk factors) that
warrants confirmation
Result provides a definite diagnosis
Cost Cheap, benefits should justify the costs since large numbers of people
will need to be screened to identify a small number of potential cases
Higher costs associated with diagnostic test maybe justified to
establish diagnosis.

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 40
Data from laboratory and diagnostic tests and procedures provide
important information about:
response to drug therapy
ability of patients to metabolize and eliminate specific
therapeutic agents
diagnosis of disease
progression and regression of disease
Laboratory and diagnostic tests are classified as either:
Invasive:
Requires penetration of the skin or insertion of instruments
or devices into a body orifice
Degree of risk involved varies from relatively minor risks
such as pain, bleeding and bruising associated with
venipuncture to the risk of death associated with more
invasive procedures, ex: coronary angiography
Examples: collection of blood, insertion of a central venous
catheter and collection of cerebrospinal fluid
Noninvasive
Do not penetrate the skin or involve insertion of
instruments to body orifices and pose little risk to the
patient
Examples: chest radiograph, analysis of spontaneously
voided urine and stool occult analysis
GENERAL ORGAN SYSTEM MONITORING
LABORATORY TESTS AND DIAGNOSTIC PROCEDURES
Test Description
Angiography Radiographic test used to evaluate blood vessels and the circulation. Radiopaque material is injected through a
catheter and images are recorded using standard radiographic techniques

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 41
Biopsy involves the removal and evaluation of a tissue
Computed Tomography (CT
Scan)
Computerized X-Ray system to produce detailed
sectional x-ray images. The system is very sensitive to differences in tissue density and produces detailed, two-dimensional planar images; contrast agents increase
attenuation. The spiral or helical CT takes pictures continuously, decreasing the time needed to obtain
images
Doppler Echography uses ultrasound technology
Endoscopy Examines the interior of a hollow viscus (digestive, respiratory and urogenital organs and the endocrine
system) or canal (bile ducts, pancreas). The endoscope, a flexible or inflexible tube with a camera and a light
source is inserted into a body orifice.
Fluoroscopy Uses a fluoroscope, a device that makes the shadows of x-ray films visible to provide real-time visualization of
procedures; exposes a patient to more radiation than routine radiography but often is used to guide needle biopsy procedures and nasogastric tube advancement
Magnetic Resonance Imaging
(MRI)
Uses an externally applied magnetic field to align the
axis of nuclear spin of cellular nuclei. The patient is surrounded by the magnetic field; brief radiofrequency
pulses are applied to displace the alignment. The energy emitted when the displacement ends is detected, resulting in finely detailed planar and three-dimensional
images; contrast agents increase the attenuation
Plethysmography measures changes in the size of vessels and hollow organs by measuring displacement of air or fluid from a
containment system; used to assess pulmonary function
Positron Emission
Tomography (PET)
Uses positron-emitting radionuclides to visualize organs
and tissues of the body. The radionuclides decay, producing positrons that collide with electrons. A special camera detects photons, released when the positrons and
electrons collide. PET imaging provides quantitative info regarding the structure and function of organs and tissues
Single-Photon Emission
Computed Tomography (SPECT)
Similar to PET but involves the administration of
radionuclides that emit gamma rays. SPECT is less expensive than PET but provides limited image
resolution

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 42
Standard Radiography (Plain Films, X-Ray Films)
Produces images on photographic plates by passing X-rays through the body. (these films are sometime difficult to interpret because of the three-dimensionality
is lost on the planar images)
CARDIOVASCULAR SYSTEM
LABORATORY TESTS
Cardiac Enzymes the pattern and time course of the appearance of enzymes in the blood after cardiac muscle cell damage
are used to diagnose myocardial infarction (MI)
Creatine Kinase (CK/Creatine
Phosphokinase)
Found in the skeletal muscle, cardiac muscle and the
brain, bladder, stomach and colon. Isoenzyme fractions identify the type of tissue damaged; detected in the blood
within 3-5 hours after a MI, levels peak in about 10-20 hours and normalize within about 3 days
Cholesterol Separated into lipoproteins by protein electrophoresis. Low-density lipoprotein (LDL) is strongly correlated
with coronary artery disease. High-density lipoprotein (HDL) is inversely correlated with coronary artery
disease
C-Reactive protein Biologic marker of systemic inflammation. Preliminary studies have linked an increased C-reactive protein concentration with an increased risk of MI, stroke, and
peripheral arterial disease
Myoglobin Small protein found in cardiac and skeletal muscle; the presence of myoglobin in the urine or plasm is relatively
sensitive indicator of cellular damage
Triglycerides Found in very-low-density lipoproteins (VLDLs) and
chylomicrons
Troponins Complex of proteins (troponins I, C, T) that mediate the actin and myosin interaction in muscle. Troponins I and
T are specific to cardiac muscle and are used to identify cardiac muscle injury. Troponin I and T concentrations increase within a few hours of cardiac muscle injury and
remain elevated for 5-7 days
DIAGNOSTIC TESTS AND PROCEDURES

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 43
Cardiac Catheterization Evaluate cardiac function; a catheter is passed into the right or left side of the heart. Transducers on the tip of the catheter record pressures in the vessels and chambers
of the heart.
Central Line Placement with Hemodynamic Monitoring
A catheter is placed into the central venous system and advanced into the right side of the heart. The right atrial,
right ventricular, pulmonary artery, and pulmonary artery occlusion pressures are measured, and cardiac
output is calculated. These parameters are used to monitor the hemodynamic status of the patient and to calculate the pulmonary and peripheral vascular
resistances.
Chest Radiography Chest x-ray films are used to diagnose cardiac disease and monitor the patient's response to drug and nondrug
therapy; determines the size and shape of the atria and ventricles to calculate the cardiothoracic ratio, and to detect abnormalities in the lung fields and pleural spaces
Cornoary Angiography cardiac vessels are visualized by injecting the vessel with
a contrast agent
Digital Subtraction Angiography (DSA)
background images are obtained before the contrast agent is injected, background images are then subtracted
from the images obtained after the injection of the contrast agent (improves image resolution)
Echocardiography used to evaluate the size, shape and motion of the valves,
septum and walls and changes in chamber size during the cardiac cycle, the beam is applied to the heart through the chest or esophagus
Contrast Echocardiography visualization of the right-sided chambers of the heart is
enhanced by the injection of contrast agents
Doppler Echocardiography evaluate cardiac blood flow patterns
Exercise Echocardiography compares echocardiograms obtained before and during
exercise
Two-Dimensional Echocardiography
(2D Echo) records 2D image of the heart, the spatial anatomic relationships can be determined by changing
the angle of the beam
Electrocardiogram (ECG) records the electrical activity of the heart, diagnose
cardiac disease, monitor the patient's response to drug therapy, and monitor for ADRs

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 44
ECG with stress recorded during a standardized exercise protocol with gradually increased levels of exercise or with the patient at rest after the administration of dobutamine or
dipyridamole
Thallium Stress Test Combines the parenteral administration of thallium-201, a radionuclide taken up by healthy myocardial tissue and
the stress test (either exercise or pharmacologic). A gamma camera is used to record serial images of the
myocardium
Intracardiac Electrophysiologic Studies (IEPSs)
tests in which special catheters with electrodes are used to stimulate the cardiac tissue to assess the nature and origin of cardiac arrythmias and the response to anti-
arrythmic drug therapy
Lymphoscintigraphy evaluates the patency and anatomy of peripheral lymph vessels by depositing a radioactive agent in the tissue
drained by the lymph system being evaluated; assesses lymphedema and tumor involvement of regional lymph nodes inaccessible to other imaging procedures
ENDOCRINE SYSTEM
LABORATORY TESTS
Dexamethesone Suppression
Test
Dexamethasone suppresses ACTH (Adenocorticotropic
Hormone) secretion
Human Chorionic Gonadotropin (hCG) test
hCG produced by the human placenta, it is detected in the urine as early as 10 days after missed menstrual cycle
and peaks at about 10 weeks
Insulin Tolerance Test Insulin (0.05-0.1 U/kg) is administered IV, serial blood
samples are obtained for 90 minutes. ACTH is released when the blood glucose falls to less than 40mg/dL
Fasting Serum Glucose test serum glucose concentrations are used to assess pancreatic function and the response to insulin
replacement to insulin replacement therapy; in this test, serum sample is obtained after 10-14 hrs of fasting, usually obtained before breakfast after an overnight fast
Glucose Tolerance test (GTT) used to diagnose diabetes mellitus (DM) and
gestational diabetes

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 45
Insulin test fasting serum insulin is sometimes obtained during the assessment of pancreatic function
Lipase test specific marker for acute pancreatic disease; increases in
serum lipase parallel increases in serum amylase, in chronic pancreatitis the pancreas may be "burned out" and unable to secrete lipase
ACTH Stimulation test ACTH stimulates adrenal cortisol production, a baseline
plasma cortisol level is obtained and then 250 mcg of cosyntropin is injected IV, plasma cortisol levels peak in
30-60 mins
Thyroid tests used to establish the level of thyroid function and the response to suppressant evaluating the serum concentrationsof the free hormones thyroxine and
triiodothyronine
GASTROINTESTINAL SYSTEM
LABORATORY TESTS
Alkaline Phosphatase test elevated in biliary cirrhosis, cirrhosis, and intrahepatic
bile duct disease
Direct bilirubin test water-soluble conjugated posthepatic bilirubin, increases with biliary disease
Indirect bilirubin test indirect bilirubin is unconjugated bilirubin, increased
with hemolytic anemia and liver disease
Delta bilirubin albumin-bound conjugated bilirubin, is increased by biliary obstruction and liver disease
Total biliribin sum of all three forms of bilirubin, increased with
hepatic and hemolytic disease

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 46
Hepatic Synthetic Function many drugs are hepatically metabolized, one way of assessing the liver's ability to metabolize these agents is to assess the synthetic function of the liver by evaluating
the quantity of specific products produces or processed by the liver
Hepatocellular Enzymes hepatocyte contain numerous enzymes that leak into the
serum when liver cells die or are damaged
Alanine Aminotransferase (ALT)
found in high concentration in hepatocytes and is considered a specific marker of hepatocellular damage
Aspartate Aminotransferase
(AST)
found in hepatocytes, myocardial muscles, skeletal
muscle, the brain and the kidneys, nonspecific marker of hepatocellular damage
Lactic Dehydrogenase (LDH) found in the heart, brain, RBCs, kidneys, liver, skeletal muscle and ileum, elevations occur during shock
syndrome (marked changes in circulation) and diseases associated with hepatocellular damage (hepatitis, cirrhosis, inflammatory disease, and infiltrative diseases)
Stool test Stool is evaluated for color, consistency, and the
presence of obvious or occult blood, fat, ova and parasites, microorganisms and WBCs. The color of the
stool provides diagnostic and monitoring information
Carcinoembryonic Antigen (CEA)
tumor marker found in the blood, associated with rapid multiplication of digestive system epithelial cells and is used to monitor recurrence
DIAGNOSTIC TESTS AND PROCEDURES
Barium Studies patient swallows contrast material and x-ray films are taken to visualize esophagus, stomach and small intestine, barium enemas are used to visualize colon
Capsule Endoscopy relatively new method used to visualize the GIT (gastrointestinal tract), patient swallows a disposable
capsule about the size of a large vitamin tablet that contains a miniature video camera, a light source, a
miniature transmitter an antenna and a battery, images are transmitted to an external receiver in a belt worn around the patient's waist; peristalsis moves the capsule
through the GI system; the capsule is excreted rectally

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 47
Cholecytosomography used to detect gallstones and evaluate the gallbladder, biliary system, and adjacent organs
Colonoscopy used to evaluate gallbladder function and anatomy;
orally administered iopanoic acid concentrates in the gallbladder, opacifying it
p-Xylose Test used to screen for carbohydrate malabsorption; a dose of 25g of D-xylose is administered with water and the urine is collected for a 5-hour period; normally more than 3g
of D-xylose is excreted in the urine during this period, lower amounts indicate impaired carbohydrate
absorption
Endosopic Retrograde Cholangiopancreatography
(ERCP) combines endoscopy and x-ray films to visualize the biliary system and pancreas; the endoscope is inserted in the esophagus and advanced to where the
bile ducts and pancreas open in the duodenum; contrast dye is injected into the ducts
Endoscopy flexible fiberoptic tube is inserted orally to visualize the
lining of the upper and lower GI system
Esophagogastroduodenoscopy an endoscope is inserted into the esophagus to visualize the inside of the esophagus, stomach and duodenum
Intragastric pH the pH of gastric secretions is sometimes measured to
monitor the effectiveness of antacid or H2-receptor antagonist therapy
Manometry evaluates esophageal contractions and esophageal sphincter pressures, pressures are measured by pressure
transduces on a tube inserted orally
pH Stimulation tests test involving pH stimulation are sued to determine the
response of gastric acid secretion to a chemical stimulus; they are sometimes used to diagnose hyposecretory and hypersecretory gastric acid disorders. Gastric secretions
are collected from the stomach by aspiration through a nasogastric tube; secretions are collected at baseline and
after stimulation with betazole or pentagastrin
SchillingTest used to evaluate the absorption of vitamin B12 (cyanocobalamin)
Stigmoidoscopy Endoscope is used to evaluate the GIT from the anus to
about 60 cm of the terminal colon. The rigid sigmoidoscope is used to screen for rectosigmoid cancer,

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 48
to obtain large mucosal biopsies and to evaluate patients with inflammatory disease of the rectum or distal sigmoid colon
HEMATOLOGIC SYSTEM
GENERAL LABORATORY TESTS
ABO Blood Typing antigen properties of blood are typed to avoid potentially lethal transfusion reactions (Blood types include A, B,
AB, O)
Blood Smear produced by smearing a drop of peripheral blood on a slide and examining the smear microscopically
Coagulation Tests common tests of coagulation include bleeding time,
Bleeding Test duration of bleeding after a standardized skin incision,
used to evaluate platelet quantity and function
Thrombin Time thrombin time is used to evaluate the effect of heparin and thrombolytic drug therapy and coagulation
abnormalities
Cross-matching determines compatibility between donor and recipient
blood, agglutination between the donor's RBCs and the recipient's serum indicates incompatibility
Fibrinogen increased in disseminated intravascular coagulation, used to evaluate bleeding disorders
Fibrin Degradation Products (FDPs) are released when fibrin is broken down,
assessed in the diagnosis and monitoring of disseminated intravascular coagulation
Hemoglobin Electrophoresis immunoelectrophoresis uses electrophoretic separation and immunodiffusion to screen for the presence of
abnormal proteins such as Bence Jones and myeloma proteins.
Serum protein electrophoresis (SPEP) is used to screen for serum protein abnormalities, proteins (albumin, globulin) are identified by different
migration patterns when subjected to an electric field

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 49
LABORATORY TESTS BY SPECIFIC CELL TYPE
Platelets initiate hemostasis; risk for spontaneous bleeding is
greatly increased if the platelet count is less than 20,000 cells/mm3; estimated from the peripheral blood smear (manually or electronically)
RBCs
Carboxyhemoglobin Forms in the presence of CO (house fires, smoke). Carbon Monoxide attaches to hemoglobin rendering the
hemoglobin incapable of carrying oxygen
Coomb's test performed by using an antiserum containing antibodies
that act o bridge antibody or complement-coated RBCs; agglutination occurs when the cells are bridged
Eythrocyte Sedimentation Rate
(ESR) is a nonspecific indicator of inflammation, this test measures the rate at which RBCs settle out of mixed
venous blood
Folate decreased serum folate levels are associated with
megaloblastic anemias
Hemoglobin oxygen-carryign RBC protein, reference vary wih age, gender, and elevation above sea level; decreased in
blood loss and iron deficiency anemia, used to diagnose anemia, assess the patient's response to replacement therapy, and estimate oxygen content
Hematocrit the number of RBCs in 100mL of blood reported as a
percentage, reference ranges vary with age, gender ad elevation above sea level, it increased in vitamin B12
and folic acid deficiencies and is decreased in iron deficiency, used to diagnose anemia and assess the patient's response to replacement therapy
RBC Appearance size, shape, and color of RBCs are influenced by many
diseases
Acanthosytes RBCs with long, thin, irregularly placed spines on the membrane, are associated with alcoholic cirrhosis and
heparin therapy and may appear after splenectomy
Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 50
Anisocytosis variably sized RBCs is associated with early iron replacement therapy
Burr Cells RBCs with evenly distributed spicules on the membrane,
associated with uremia
Elliptocytes rod-shaped RBCs, are associated with sickle cell trait and thalassemia
Hypochromia decrease in the hemoglobin content of RBCs, produces pale RBCs and is associated with folic acid and vitamin
B12 deficiency anemias
Macrocytes larger than normal RBCs
Microcytes smaller than normal RBCS
Normachromia normal RBC color
Ovalocytes oval-shaped RBCs, are associated with microcytic and megaloblastic anemias
Schistocytes RBC fragments, associated with microcytic and
megaloblastic anemias
Spherocytes small, round RBC fragments are associated with anemias and hemolytic transfusion reactions
Stomatocytes RBCs with central slitlike areas of pallor, are associated
with neoplastic, liver and cardiac disease
Target Cells RBCs with dark centers surrounded by light rings are associated with sickle cell anemia, iron deficiency and
liver disease; they also may occur after splenectomy
RBC count the number of RBCSs per 1mL of blood, used to
diagnose anemias, and to assess the patient's repsonse to replacement therapy, serves as an indicator of chronic hypoxemia
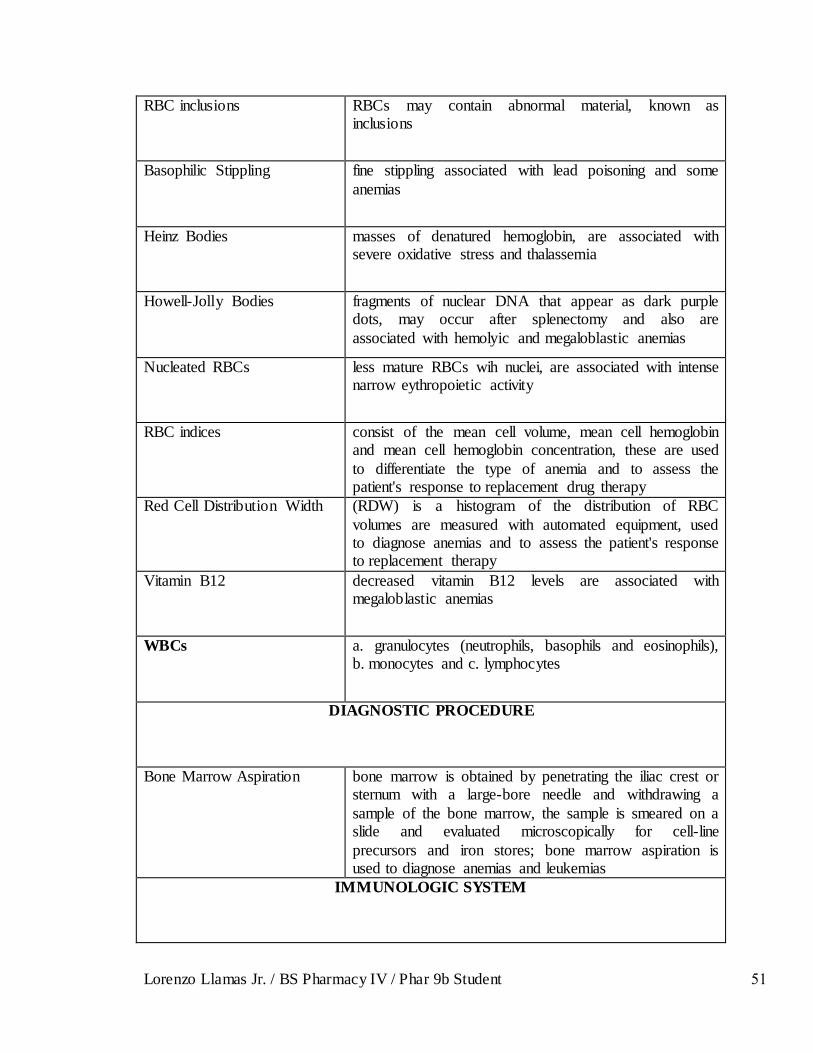
Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 51
RBC inclusions RBCs may contain abnormal material, known as inclusions
Basophilic Stippling fine stippling associated with lead poisoning and some
anemias
Heinz Bodies masses of denatured hemoglobin, are associated with severe oxidative stress and thalassemia
Howell-Jolly Bodies fragments of nuclear DNA that appear as dark purple dots, may occur after splenectomy and also are
associated with hemolyic and megaloblastic anemias
Nucleated RBCs less mature RBCs wih nuclei, are associated with intense narrow eythropoietic activity
RBC indices consist of the mean cell volume, mean cell hemoglobin and mean cell hemoglobin concentration, these are used
to differentiate the type of anemia and to assess the patient's response to replacement drug therapy
Red Cell Distribution Width (RDW) is a histogram of the distribution of RBC
volumes are measured with automated equipment, used to diagnose anemias and to assess the patient's response to replacement therapy
Vitamin B12 decreased vitamin B12 levels are associated with megaloblastic anemias
WBCs a. granulocytes (neutrophils, basophils and eosinophils), b. monocytes and c. lymphocytes
DIAGNOSTIC PROCEDURE
Bone Marrow Aspiration bone marrow is obtained by penetrating the iliac crest or sternum with a large-bore needle and withdrawing a
sample of the bone marrow, the sample is smeared on a slide and evaluated microscopically for cell-line
precursors and iron stores; bone marrow aspiration is used to diagnose anemias and leukemias
IMMUNOLOGIC SYSTEM

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 52
LABORATORY TESTS
Antineutrophil Cytoplasmic
Antibodies
(ANCA) are autoantibodes against neutrophil granules
and monocyte lysosomes, p-ANCA reactivity is associated with angiitis, rheumatoid arthritis, inflammatory bowel disease and vasculitis
Antinuclear Antibodies (ANAs) often associated with systemic lupus
erythematosus (SLE), although they may be present in rheumatoid collagen diseases, mixed connective tissue
disease, and systemic sclerosis
Anti-DNA Antibodies Antibodies against double-stranded DNA (dsDNA) and with single-stranded DNA (ssDNA). Anti-dsDNA antibodies often are found patients with SLE
Extractable Nuclear Antigens May be present against specific extractable nuclear
antigens (ENAs). Systemic sclerosis and SLE are associated with high titers of anti-SS-A and anti-SS-B antibodies. Antibodies against histones may be found in
patients with drug-induced SLE
Rheumatoid Factor Against immunoglobulin E and G (IgE and IgM) may be found in patients with rheumatoid arthritis (RA)
Cold Agglutinins antibodies that bind to the surface of RBCs,
agglutination occurs when the blood sample is cooled, associated with a variety of infections and inflammatory disorders
Coomb'sTest uses an antiserum containing antibodies that bridge antibody or complement-coated RBCs; bridging causes agglutination (clumping)
Direct coomb's test uses antibodies directed against human proteins to detect whether these proteins are attached to the surface of
RBCs, used to differentiate between immunologic and non-immunologic
Indirect coomb's test detects antibodies against human RBCs in the patient's
serum, used in cross-matching before transfusion
C-Reactive protein nonspecific indicator of inflammation, is acutely elevated in RA, acute bacterial infections and viral hepatitis and viral hepatitis
Erythtocyte Sedimentation
Rate
(ESR) is a nonspecific indicator of inflammation, this
test measures the rate at which RBCs settle out of mixed venous blood, rate of settling is influenced by the shape of the RBCs and charges on the membrane, a nonspecific

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 53
marker of inflammatory and malignant disease
Immunoelectrophoresis uses electrophoretic separation and immunodiffusion
techniques to separate proteins, used to screen for diseases associated with Ig abnormalities
Immunoglobulin E serum IgE is elevated in patients with allergic disorders
Lupus Anticoagulant is a circulating Immunoglobulin found in patients with autoimmune disease, prolongs in vitro clotting time by
inhibiting phospholipid interactions but is not associated with an increased risk of bleeding in vivo
Uric Acid uric acid is the end product of purine metabolism, low
serum levels are associated with Wilson's disease and some malabsorption syndromes, high levels are
associated with rapid cellular destruction (as in chemotherapy or malignancies) and disorders of metabolism as gout
Venereal Disease Research
Laboratory Test
(VDLR) used to diagnose syphilis, is sometimes falsely
positive in connective tissue disease
DIAGNOSTIC PROCEDURES
Allergy Panel Test the patient's reactivity to a variety of antigens
(purified protein derivative antigen, mumps antigen, Streptococcus antigen, Candida, Trichophyton antigen,
histoplasmin); antigens are injected intradermally and the skin is evaluated for redness and swelling at the injection site. Response to one or more of the antigens
indicates a responsive immune system. Response to a specific antigen indicates that the patient has antibodies
to a specific antigen
Scratch or Patch Testing used to evaluate patient sensitivity to specific allergens, each allergen is applied to the skin by scratching the skin; the skin is then evaluated for swelling and redness
INFECTIOUS DISEASE

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 54
LABORATORY TESTS
Acid-Fast Stain used to screen for the presence of Mycobacterium,
Nocardia, and Legionella species in body tissues and fluids; some oocytes such as Cryptosporidium can be detected with the acid-fast stain
Cerebrospinal Fluid (CSF)
Analysis
CSF is analyzed for the presence and quantity of RBCs,
WBCs, glucose, and protein; if indicated, stains (Gram's stain and acid-fast stain) and potassium hydroxide and
India ink preparations are used to evaluate the fluid; the CSF glucose is normally about two-thirds the serum blood glucose. Viral meningitis is characterized by a
negative Gram's stain and normal protein and glucose; fungal and tuberculous meningititis is characterized by a
negative Gram's stain, normal protein, and low glucose; bacterial meningitis is characterized by cloudy CSF, increased WBCs, elevated protein and frequently a
positive Gram's stain
Cold Agglutinins antibodies that bind to the surface of RBCs and agglutinate when the blood sample is cooled; about 50%
of patients with Mycoplasma pneumoniae have cold addlutinin titers
C-Reactive protein a nonspecific indicator of inflammation, is acutely
elevated in RA, acute bacterial infections and viral hepatitis; sometimes used to differentiate between bacterial and viral meningitis
Culture and Sensitivity
Testing
cultures of body fluids and tissue identify specific
infecting organisms; in vitro testing is used to determine antibiotic susceptibilities
Gram's Stain evaluates a body fluid or specimen for the presence of microorganisms; organisms are characterized according
to their gram-positive or gram-negative characteristics, morphology and other characteristics
India Ink Preparation used to detect Cryptococcus neoformans in a variety of body fluids; carbons in India ink are unable to penetrate
the organism, enabling the microscopic identification of the organism by its lack of staining
Minimal Bactericidal
Concentration
(MBC) lowest antibiotic concentration that kills at least
9.9% of the bacteria in the original inoculum; used to determine the susceptibility of the organism to
antibiotics

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 55
Minimum Inhibitory Concentration
(MIC) lowest antibiotic concentration that completely inhibits the visible growth of a microorganism; determine the susceptibility of the organism to
antibiotics
Potassium Hydroxide Preparation
(KOH) 10-20% is used to detect fungi in body fluids and skin scrapings
Rapid Plasma Reagin Test (RPR test) is used to screen for syphilis; tests for
antibodies against antigens from damaged host cells
Serologic Tests used to indentify an antigen or antibody to help diagnose infectious disease and to monitor the immunologic
response to the microorganism; acute-phase titers and convalescent titers are sometimes compared
Venereal Disease Research
Laboratory Test
(VDLR) used to diagnose syphilis and neurosyphillis,
test for antibodies against antigens from damaged host cells; not as sensitive as RPR test
Wet Mounts body fluid specimensare examined microscopically for the presence of parasites and fungi
WBC Count and Differential the WBC count is often elevated in patients with bacterial and viral infections; a left shift (increased bands
and segmented neutrophils) indicate a bacterial infection; lymphocyte count may be elevated in viral infections;
eosinophil count may be elevated in parasitic infections; elderly patients and those with impaired immune systems or very sever infectious disease may not be able
to mount a white cell response to infection
NEUROLOGIC SYSTEM
DIAGNOSTIC PROCEDURES
Cold Calorics assesses brain stem function in comatose patients; the intact external auditory canal is filled with ice-cold
water; both eyes move toward the cold ear and then snap back to the center if brainstem function is normal
Edrophonium (Tensilon) Test diagnose myasthenia gravis and to determione whether
the maintenance acetycholinesterase inhiitor dosage is appropriate; endrophonium is administered parenterally, and the muscle strength of the patient is evaluated
subjectively

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 56
Electroencephalography (EEG) records the electrical activity of the brain from electrodes attached to the scalp; used to diagnose seizures and to assess the patient's response to therapy
Peripheral Nerve Stimulation assesses the depth of neuromuscular blockade
Nerve Conduction Studies rate of nerve conduction is evaluated by stimulating the nerve and recording the rate fo conduction to electrodes placed over the muscle; nerve conduction studies are
used to diagnose nerve injuries and neuromuscular disease
NUTRITIONAL STUDIES
LABORATORY TESTS
Albumin indicator of visceral protein reserves and nutritional
status; protein malnutrition is associated with a serum albumin level of less than 3.5 g/dL if liver function is normal
Bilirubin conjugation of bilirubin requires energy; starvation may
cause mild hyperbilirubinemia
Calcium decreased serum albumin decreases total calcium; the serum calcium does not reflect body stores
Creatinine the 24-hour urinary excretion of creatinine is used to
estimate muscle catabolism; serum creatinine is not a useful indicator of nutritional status, very low serum
creatinine levels may reflect poor nutrional status
Glucose monitored during nutrional supplementation or total nutrional replacement therapy to assess overall metabolic balancel not a useful indicator of nutritional status
Immunologic Status malnutrition may be associated with altered
immunologic status; lymphocyte production may be diminished, resulting in a decreased total lymphocyte count; patients may not be able to mount an
immunologic response to skin test antigens
Magnesium decreased serum albumin levels decrease total magnesium; the serum magnesium does not reflect total
body stores

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 57
Partial Thromboplastin Time poor nutritional status may be associated with inadequate intake of vitamin K, resulting in a deficiency of vitamin K-dependent clotting factors and prolonged clotting time
Phosphorus Phosphorus is a metabolic cofactor and intermediate;
refeeding hypophosphatemia may occur in patients with low levels of phosphorus who receive nutritional supplementation or total nutrional replacement therapy
Transaminases starvation compromises cellular membrane integrity and
may be associated with increased transaminases (AST and ALT)
Transferrin Transferrin is an iron transport protein with a shorted half-life than albumin (1week versus 3weeks); serum
transferrin responds more quickly to changes in nutritional status than does albumin and is a useful indicator of nutritional status
Urea Nitrogen, Blood (BUN) is a useful indicator of protein breakdown
DIAGNOSTIC PROCEDURES
Anthropometrics comparative body measurements assess nutrional status; parameters such as skin-fold thickness of the upper
portion of the nondominant arm, midupper arm circumferene (MUAC) and arm muscle circumference
(AMC) are assessed;20%-40% decrease compared with normal values is associated with moderate malnutrition; greater than 40% is associated with severe malnutrition
RENAL SYSTEMS
LABORATORY TESTS
Arterial Blood Gas arterial blood gas assesses acid-base balance and
ventialtion; used to diagnose acid-base disturbances and to monitor the patient's response to drug and nondrug
interventions

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 58
Arterial pH arterial pH is a quantitative measure of the degree of acidity or alkalinity of the arterial blood (reference range: 7.35 - 7.45)
Base Excess (BE) is quantitative measurement of the combined
buffering capacity of all body buffering systems, including the bicarbonate system and hemoglobin (-2 to +2)
Bicarbonate Quantitative measurement of net bicarbonate production
and elimination
Carbon Dioxide Tension partial pressure of dissolved carbon dioxide is quantitative measure of net carbon dioxide production
and elimination (35-45 mmHg)
Oxygen Saturation oxygen saturation of the blood (SaO2) is a quantitative
measurement of the percentage of hemoglobin combined with oxygen; can be measured noninvasively with pulse
oximetry
Oxygen Tension partial pressure of oxygen dissolved in the blood is a quantitative measure of oxygen concentration (75-100 mmHg)
Creatinine filtered by glomeruli, is a useful indicator of renal function
Electrolytes and Minerals electrolytes and minerals that are useful when assessing the renal system include calcium, chloride, magnesium, phosphorus, potassium and sodium; the serum
concentration of these electrolytes and minerals is variable and does not reflect total body stores
Calcium (ionized) ionized (free) calcium is the physiologic active portion
of total serum calcium; ionized calcium is used to assess calcium status in patients with or at risk of secondary hyperparathyroidism and in patients with hypomagnesia,
sepsis and pancreatitis (4.6-5.1 mg/dL)
Calcium (total) approximately 40% of serum calcium is bound to albumin in a ratio of 0.8 mg/dL of calcium per 1.0 g/dL
albumin; approximately 15% of serum calcium is bound to albumin; the remaining 45% of serum is unbound ionized calcium; total serum calcium, the sum of bound
and free calcium is used to assess calcium metabolism and to screen for and evaluate the response to therapy in
bone tumors, primary and secondary hyperparathyroidism and hypoparathyroidism, renal failure and acute pancreatitis (8.5-10.0 mg/dL)

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 59
Chloride extracellular electrolyte; increased in renal tubular acidosis and primary hyperthyroidism; decreased by the administration of drugs such as thiazide, loop diuretics
and corticosteriods (100-108 mEq/L)
Magnesium intracellular electrolyte; assessment of magnesium deficiency and for monitoring of replacement therapy
(1.5-2.0 mEq/L)
Phosphorus present in bone (about 85% of the total) and skeletal
muscle (about 10% of the total); serum phosphorus concentration is always in a 1:1 ratio with the serum
calcium concentration; used in the diagnosis of hypoparathyriodism and the assessment of bone metabolism (2.5-4.5 mg/dL)
Potassium intracellular electrolyte; serum concentration is sensitive
to changes in acid-base status; increased in acidosis, dehydration and renal insufficiency and with the
administration of some drugs, such as spironolactone; decreased in overhydration and alkalosis and with the administration of drugs such as corticosteroids,
amphotericin, and lithium carbonate (3.5-5.0 mEq/dL)
Sodium extracellular electrolyte; used to assess water and sodium balance, increased in dehydration; decreased in
Addison's disease and by diuretic administration, dilution in ascites, congestive heart failure, renal
insufficiency and excessive water intake (135-145 mEq/L)
Gram's Stain and Culture normal urine contains no bacteriaor yeasts; bacteriaare present in UTIs and pyelonephritis. Gram's stain and
culture identify the cause of the infection and aid in monitoring the patient's response to drug therapy; yeasts
are found in the immunocompromised host and sometimes are associated with braod-spectrum antibiotic therapy
Osmolality measured and compared to assess the kidnet's ability to
concentrate the urine; normal urine-to-serum osmolality ratio is 1:3; Ratios less than 1:1 indicate distal tubular
disease; ratios greater than 1:1 indicate glomerular disease
Blood Urea Nitrogen (BUN) low BUN signify liver disease; high BUN indicated renal disease, other than glomerular function readily affect
BUN levels, sometimes making interpretation of resultant difference
Urinary Sodium differentiate between renal failurefrom prerenal causes
and from parenchymal renal insufficiency; in renal disease the kidneys are unable to conserve sodium,
resilting in elevated urine sodium levels; used to

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 60
diagnose the syndrome of inappropriate antidiuretic hormone secretion (SIADH); in SIADH the serum sodium is low but the urine sodium is elevated
Urine Toxicology detect the presence of drugs in patients with suspected
drug overdoses, patients experiencing altered mental status and patients in drug rehabilitation programs
Urinalysis used to screen for renal and nonrenal disease and to monitor the patient's repsonse to drug and nondrug therapy; consists of macroscopic assessment, chemical
screening by dipsteick and microscopic assessment of the urine sedimient
Dipstick Screening
Bilirubin not normally present in the urine; excreted in the urine in the presence of severe liver disease or obstructive biliray
disease; urine appears dark yellow to brown if bilirubin is present
Blood not normally present in the urine; may be visibly be bloody or blood may be found on dipstick examination;
a variety of renal and non-renal diseases including UTIs, renal stones, sickle cell anemia, glomerulonephritis, and
malignant hypertension, are associated with blood in urine
Glucose not normally present in urine; may be present in diabetes miletus
Ketones not normally found in urine; present before serum ketones are detectable in diabetic ketoacids and may be found in patients with who are dieting or are
malnourished
Lueukocyte Esterase not normally found in urine; present in WBCs and may be found in urine during urinary tract and vaginal
infections
Nitrites not normally found in urine; E. converts dietary nitrates
to nitrites are associated with E. coli urinary tract infections but may only be found if the urine is retained in the bladder for at least 4 hours
pH Urinary pH reflects the overall acid-base balance of the
body and the kidney's ability to handle acids and bases; formation of kidney stones is pH dependent. An alkaline
pH (pH .7.0) is commonly associated with the presence of urea-splitting organisms such as Proteus mirabilis

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 61
Protein small amounts of protein are normally present in the urine (as much as 0.5g/day); urinary protein is increased in a variety of renal diseases
Specific Gravity reflects the kidney's ability to concentrate urine and the
overall state of hydration; the greater the concentration of the urine, the higher the specific gravity
Urobilinogen not normally present in the urine; may be excreted in the urine in the presence of severe liver disease or obstructive biliary disease
Macroscopic Assessment
Color freshly voided urine is normally pale yellow; normal urine may range in color from nearly colorless if very dilute to orange if very concentrated
Turbidity Freshly voided urine is normally clear; urine is turbid if bacteria, WBCs, RBCs, yeast or crystals are present
Microscopic Assessment
Casts "poor man's renal biopsy" are objects formed and molded within renal tubules; are cylindrical and
composed mostly of protein and cells, may be convoluted (spiral) if formed in distal convoluted
tubules, broad if formed in dilated collecting ducts and narrow if formed in narrow lumens
Bile casts acellular casts that contain bile; associated with liver disease
Hyaline casts acellular casts that consists of a protein matrix; an
occasional hyaline cast may may normally be presen; the number of hyaline casts increases with renal disease
Mixed cellular casts may contain RBCs, WBCs, and renal tubular epithelial cells; are associated with mixed tubular and interstitial
renal diseases
RBC casts RBC casts are formed if the glomerular basement
membrane is damaged; may be found in acute and focal glomerulonephritis, lupus nephritis, and trauma

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 62
Waxy casts acellular casts formed by the breakdome of cellular casts; associated wuth chronic renal disease
Cells
RBCs normally, as many as two RBCs per high-power field may be present in the urine; number of RBCs in the urine increases with UTI, stones and tumors and with
strenuous exercise
Renal tubular epithelial cells shed from the renal tubules, are normally present in the urine
Squamous epithelial cells normally present in the urine, shed from the urethra and
vagina
WBCs normally, as many as five WBCs in the urine, increases with renal and urinary tract disease and strenuous
exercise
Crystals found in acidic and basic urine; amorphous phosphate
crystals and triple phosphate crystals, calcium oxalate and uric acid crystals are normally present in acidic urine; a variety of pathologic crystals may be found in
alkaline urine
Bilirubin crystals reddish brown needles, plates and cubes associated with jaundice and bilirubinemia
Cholesterol crystals flat plates with notched corners associated with the
nephrotic syndromes
Cysteine crystals hexagonal plates associated with congenital cystinuria
Leucine crystals round, oily appearing crystals associated with severe
hepatic disease
Tyrosine crystals fine needles grouped in sheaves that are associated with severe hepatic disease

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 63
DIAGNOSTIC PROCEDURES
Intravenous Pyelogram (IVP) test used to visualize the entire urinary tract; parenteral
contrast medium cleared by glomerular filtratrion is used to detect ureteral obstruction, masses, tumors and cysts
used to visualize te urine-collecting systems independent of renal function; contrast media are instilled through a catheter placed in the bladder
RESPIRATORY SYSTEM
LABORATORY TESTS
Arterial Blood Gas used to assess the acid-base balance and level of
ventilation, to diagnose acid-base disturbances and to monitor the patient's response to drug and nondrug interventions
Sputum Analysis used to screen for disease and to monitor the patient's
response to drug and nondrug therapy; consists of macroscopic and microscopic assessment
Macroscopic Assessment
Color Normally mucoid and clear; purulent sputum contains
pus and is associated with bacterial infection; yellow sputum is indicative of inflammation. Uniformly rusty-
appearing purulent sputum is indicative of Pneumonococcal pneumoniae pneumonia; bright red streaks in viscid sputum indicates Klesiella pneumoniae
pneumonia. Greenish black sputum is indicative of gram-negative bacilli infection
Odor normal sputum is odorless; foul-smelling sputum is
indicative of a bacterial infection
Viscosity normal sputum is thin and watery, asthmatic patients have a very thick, sticky, tenacious sputum

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 64
Volume very little sputum is produced normally; volume of sputum is increased in a variety of diseases including bronchitis, pneumonia, and tuberculosis
Microscopic Assessment
Charcot-Leyden Crystals elongated double pyramid-shaped masses of eosinophils associated with lupus
Curschmann's Spirals casts of small bronchi present in diseases associated with bronchial obstruction, such as asthma
Eosinophils present in asthma and other hypersenstivity disorders
Neutrophils found in bacterial and fungal pneumonia and chronic bronchitis
DIAGNOSTICS PROCEDURES
Bronchoscopy visualize the tracheobronchial tree; flexible bronchoscope is introduced into the tracheobronchial
free through the nose, mouth or endotracheal or tracheotomy tube; samples of fluid and tissue may be
obtained for Gram's stain, culture and cytologic examination
Chest Radiography Chest x-ray films aid in the diagnosis of pulmonary and cardiac disease and the assessment of the patient's
response to drug and nondrug intervention
Pulmonary Function Testing Used to diagnose pulmonary disease to monitor
progression of disease, to predict response to bronchodilators and to monitor the patient's response to
drug and nondrug therapy; performed using a spirometer or body plethysmography. A spirometer detects and records changes in lung volume and flow. Body
plethysmography detects changes in intrathoracic pressure and volume; normal values vary with age,
gender, height, and weight. In general, decreases of 20% or more from predicted values are considered significant

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 65
Forced Vital Capacity FVC is the volume of air (in liters) blown out of the lungs during forced exhalation after maximal inspiration
Peak Expiratory Flow Rate PEFR measures the forced expiratory flow in liters per
minute; used to monitor the progression and response to therapy of patients with bronchospastic diseases such as asthma; asthmatic patients monitor their PEFR at home
inexpensive handheld peak flow meters; PEFR variability of greater than 30% indicates moderate to
severe persistent asthma
Tidal Volume (VT) is the volume of air inspired or expired with normal breathing
Pulse Oximetry noninvasive, transcutaneous technique used to assess oxygen saturation
Quanitative Pilocarpine Iontophoresis (Sweat Test)
Concentration of sodium in sweat is measured after stimulation of the sweat glands with topical pilocarpine; low-voltage current is applied to aid in the absorption of
the pilocarpine. The sweat test is used in the diagnosis of cystic fibrosis
Ventilation/Perfusion
Scanning
(V/Q) scanning is used to compare ventilation and
perfusion; images of the airways taken after the inhalation of radiolabeled tracers are compared with images of the pulmonary vasculature taken after the
injection of contrast agents; normally ventilated and perfuse areas match. This test is commonly used to
identify pulmonary emboli
SEROUS BODY FLUIDS
LABORATORY AND DIAGNOSTIC TESTS
Calcium Pyrophosphate Crystals
may be rod-shaped, needle-shaped or rhombic; have positive birefringence and are found intra-cellularly and extra-cellularly; associated with pseudo-gout
Monosodium Urate Crystals needle-shaped, have negative bifringence and are found intra-cellularly and extra-cellularly; associated with gout
1. Biochemical Data

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 66
Typical Normal Adult References Values measure in serum
Laboratory test Reference Range
Urea and electrolytes
Sodium 135-145 mmol/L
Potassium 3.4-50 mmol/L
Calcium (total) 2.12-2.60 mmol/L
Calcium (ionized) 1.19-1.37 mmol/L
Phosphate 0.80-1.44 mmol/L
Magnesium 0.70-1.00 mmol/L
Creatine 75-155 mol/L
Urea 3.1-7.9 mmol/L
Estimated glomerular filtration rate (eGFR)
>90mL/min/1.73m2
Glucose
Fasting 3.3-60 mmol/L
Non-Fasting <11.1 mmol/L
Glycated hemoglobin Non-diabetic subjects <42mmol/mol; Inadequate
control >58mmol/mol
Liver function Test
Albumin 34-50g/L
Bilirubin (total) <19 mol/L
Enzymes
Alanine transaminase (ALT) <45U/L
Aspartate transaminase (ASP) <35U/L
gamma-Glutamyl transpeptidase
35-120U/L
Ammonia
Male 15-50 mol/L
Female 10-40 mol/L
Amylase <100U/L
Cardiac markers
Troponin I (99th percentile of upper reference limit) 0.04 mcg/L

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 67
Other tests
C-reactive protein (CRP) 0.5mg/L
Osmolality 282-295 mOsmol/kg
Uric acid 0.15-0.47 mmol/L
Parathyroid hormone (adult with normal calcium)
10-65 ng/L
25-hydroxyvitamin D >75 nmol/L (optimal)
>50 nmol/L (sufficient)
30-50 nmol/L (insufficient)
12-30 nmol/L (deficient)
<12 nmol/L (severely deficient)
Water
Water Depletion
Occurs if intake is inadequate or loss excessive
Excessive loss of water through the kidney is unusual except in
diabetes insipidus or overuse of diuretics
Patients with fever will lose water through the skin
Ventilated patients lose it via lungs
Underlying cause for water depletion should be identified and
treated
Replacement of water should be given orally, where possible, or by
nasogastric tube, intravenously or subcutaneously with 5%
dextrose in water or isotonic saline in patients with sodium
deficiency
Water excess
Impairment of water excretion such as caused by renal failure or
syndrome of inappropriate secretion of the antidiuretic hormone
(SIADH)
Chest infections and tumors (small cell carcinoma of the lung)
Cerebral overhydration
Hyponatremia
Excess intake is rare since a healthy adult kidney can excrete water
at a rate of 2mL/min
Sodium (Na+)
Sodium Depletion
Inadequate oral intake is rarely the cause of Na depletion
More common on inadequate parenteral treatment of sodium

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 68
Occurs with water depletion, resulting in dehydration
Normal response of the body to the hypovolemia includes an
increase in aldosterone secretion (stimulates renal reabsorption)
Sodium Excess
Can be due to either increased intake or decreased excretion
Excessive intake is not a common cause but can be associated with
excessive intravenous saline depletion due to impaired access to
free water or impair thirst
Usually due to impaired excretion, mineralocorticoid excess
(Cushing’s syndrome or Conn’s syndrome), secondary
hyperaldosteronism ex: congestive cardiac failure, nephritic
syndrome, hepatic cirrhosis with ascites or renal artery stenosis
Hypernatremia
Muscle weakness and confusion
Often drug-induced
Lithium and phenytoin; diabetes insipidus- like syndrome with
lithium has been reported after 2 weeks of therapy, syndrome is
reversible with discontinuation
Demeclocycline can cause diabestes insipidus and can be used
in patients with SIADH
Phenytoin has less pronounced effect on urinary volume than
litium or demeclocycline; inhibits ADH secretion
Hyponatremia
Fall in Na level can result of Na loss, water retention in excess of
sodium resulting from defects in free water
Drugs known to cause hyponatremia
Amitryptyline and other TCAs (tricyclic antidepressants)
Amphotericin
Angiotensin converting enzyme (ACE) inhibitors [Captopril]
NSAIDs (non-steroidal anti-inflammatory drugs)
Opiates
Vincristine
Potassium
Hypokalemia
Moderate hypokalemia may be asymptomatic
Severe hypokalema = muscle weakness, hypotonia, paralytic ileus,
depression and confusion, arrhythmias
Drugs known to cause hypokalemia: ampotericin, aspirin,
corticosteroids, insulin, laxatives, diuretics (except K-sparing),
sodium bicarbonate, sodium chloride, penicillin G, salicylates

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 69
Hyperkalema
May arise from excessive intake, decreased elimination or shift of
potassium from cells to the extracellular fluid (ECF)
Hyperkalemia can be asymptomatic but fatal
An elevated potassium level has many effects on the heart: notably
resting membrane potential is lowered and action potential
shortened
Calcium
Hypercalcemia
May be caused by variety of disorders, most common being
primary hyperparathyroidism
Thiazide diuretics, lithium, tamoxifen and calcium supplements
used in management of osteoporosis are examples of some drugs
that cause hypercalcemia
Hypocalcemia
Caused by a variety of disorders including severe malnutrition,
hypoalbuminemia, hypoparathyroidism, pancreatitis and those that
cause vitamin D deficiency
Drugs that cause hypocalcemia include: bisphonates, phenytoin,
Phenobarbital, aminoglycosides, phosphate edemas, calcitonin,
cisplatin, mithramycin and furosemide
Phosphate
Hypophosphatemia
Severe cases can cause general delebility, anorexia, anemia,
muscle weakness and watering and some bone pain and skeletal
wasting
Inadequate phosphorus intake requires near starvation
Hyperphosphatemia
Occurs in chronic renal failure
Less common causes are secondary to rhabdomyolysis, tumor lysis
or severe hemolysis and hyperphosphatemia
Magnesium
Hypomagnesemia
Frequently seen in critically ill patients
Causes include: excess GI (gastro-intestinal) losses, renal losses,
surgery, trauma, infection, malnutrion and sepsis

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 70
Drugs that induce hypomagnesemia include: amikacin,
amphotericin B, cisplatin, gentamicin, tacrolimus, carboplatin,
digoxin
Hypermagnesemia
Caused by renal insufficiency and excess iatrogenic magnesium
administration
Creatinine
Good indicator of the glomerular filtration rate (GFR)
Serum creatine can be transiently elevated by meat ingestion, urea or
strenuous exercise
Overall measure of kidney function
Allows estimation of GFR
Urea
Elevation of serum urea
High protein intake from diet
Tissue breakdown
Major hemorrhage in the gut
Consequent absorption of the protein from blood
Corticosteroid therapy
Production is decreased where there is a low protein intake and in
some patients with liver disease
Glucose
Normal ranges for serum glucose for nonfasting: <11.1 mmol/L;
fasting: 3.3-6.0mmol/L
Fasting serum glucose levels between 6.1 – 7.0 mmol/L indicate
impaired glucose tolerance
Fasting serum glucose levels above 7.0 mmol/L indicate diabetes
Uric acid
Elevated serum nitric acid level
Increased rate of formation
Reduced excretion
2. Liver Function Tests
Albumin
Low serum concentration
Volume of albumin increases
In cirrhosis with ascites, fluid retention such as pregnancy
Bilirubin
Elevation of serum bilirubin
Reveal as jaundice, seen best in the skin and sclera

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 71
Caused by increased production of bilirubin (ex: hemolysis,
ineffective erythropoesis), impaired transport into hepatoctes
Enzymes
Alkaline phosphatase (ASP)
Enzyme which transports metabolites across cell membranes
Pathological increase in serum ASP
Caused by: disorders of the liver ex: hepatitis, drug-induced ex:
ACE inhibitors, estrogens; pregnancy; osteomalacia
Transaminase
Elevated serum AST
Variety of disorders including liver diseases, crush injuries, severe
tissue hypoxia, myocardial infarction, surgery, trauma, muscle
disease pacreatitis
Elevated serum ALT
Similar to agents that caused serum AST elevation but at a lesser
extent
Raised by viral and non-viral acute and chronic liver disease, drug
induced (ex: paracetamol poisoning), alcohol and ischemic liver
damage
Gamma-Glutamyl transpeptidase (Gamma GT)
Elevated levels in alcoholic liver disease, hepatitis, cirrhosis and non-
hepatic disease such as pancreatitis, congestive cardiac failure, COPD
and renal failure
Ammonia
Hyperammonemia occur at concentrations >60 mmol/L
Clinical features: anorexia, irritability, lethargy, vomiting,
somnolence, disorientation, asterixis, cerebral edema, coma and death
Cause include: genetic defects in urea, hepatic dysfunction
Amylase
Produced in the pancreas and salivary glands
Serum amylase elevation
Caused by pancreatitis
Loss of bowel integrity though infarction
Perforation
chronic alcoholism
post-operative states and
renal failure
3. Hematology data

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 72
Hemotology Data: Typical Normal Adult Reference Values
Hemoglobin 11.5 - 16.5 g/dL
Red Blood Cell (RBC) count 3.8 - 4.8 x 1012/L
Reticulocyte count 50 - 100 x 106/L
Packed cell volume (PCV) 0.36 - 0.46 L/L
Mean cell volume (MCV) 83 - 101 fL
Mean cell hemoglobin 27-34 pg
Mean cell hemoglobin concentration (MCHC)
31.5 - 34.5 g/dL
White Blood Cell Count 4.0 - 11.0 x 109/L
Neutrophils (30-75%) 2.0 - 7.0 x 109/L
Lymphocytes (5-15%) 1.5 - 4.0 x 109/L
Monocytes (2-10%) 0.2 - 0.8 x 109/L
Basophils (<1%) <0.1 x 109/L
Eosinophils (1-6%) 0.04 - 0.4 x 109/L
Platelets 150 - 450 x 109/L
Erythrocyte Sedimentation Rate (ESR)
1 - 35 mm/h
D-dimers 0 - 230 ng/mL
Ferritin 15 - 300 mcg/L
Total iron binding capacity (TBC)
47 - 70 mol/L
Serum B12 170 - 700 ng/L
Red cell folate 160 - 600 mcg/L
Iron 11 - 29 mol/L
Transferrin 1.7 - 3.4 g/L
RBC count
High RBC count (erythrocytosis or polycythemia) = increased
production by bone marrow, response to hypoxia; malignant condition
of red cells such as in polycythemia rubra vera
Reticulocytes
Assessing response of the marrow to iron, folate or vitamin B12
therapy (count peaks at about 7-10 days after starting such therapy and
then subsides)
Mean Cell Volume (MCV)
Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 73
Useful in the process of identification of various types of anemias such
as caused iron deficiency (microcytic) or vitamin B12 or folic acid
deficiency (megaloblastic or macrocytic)
Packed Cell Volume (PCV)
Ratio of volume occupied by RBCs to the total volume of blood
Measured by centrifugation of a capillary tube and then expressing the
volume packed in the bottom as a percentage
Calculated as product of MCV and RBC and reflects RBC
Low values = anemia; raised values = polycythemia
Mean Cell Hemoglobin (MCV)
Dependent of the size of the RBCs and concentration of hemoglobin in
cells
Usually low in iron-deficiency anemia
Raised in macrocytic anemia
Mean Cell Hemoglobin Concentration (MCHC)
Measure of average concentration of hemoglobin in 100ml or RBCs
Expressed in gram per liter
Low MCHC values in iron-deficiency anemia
High MCHC values in prolonged dehydration
Platelets
Thrombocytosis = low levels of platelets; occurs in pregnancy, viral
infections, spontaneous bleeding, intravascular coagulation
Thrombocytosis = high levels of platelets; occurs in malignancy,
inflammatory disease and in response to blood loss
White Blood Cell Count
Neutrophils / Polymorphonucleocytes (PMNs)
Most abundant type of WBC
Have phagocytic action
Counts increase (Neutrophilia) in: infection, tissue damage
(infarction) and inflammation (ex: acute gout)
Neutropenia (decrease in neutrophils) is associated with
malignancy and drug toxicity; also occur in infections such as
influenza, infectious mononucleosis and hepatitis
Basophils
Normally constitute small percent of WBC count
Elevated numbers (basophilia) occur in various malignant and
premalignant disorders ex: leukemia and myelofibrosis
Eosinophils
Constitute 6% of WBCs
Acts in inactivation of mediators released from mast cells

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 74
Eosinophilia is apparent in allergic reactions such as asthma, hay
fever; worm infestation and drug sensitivity
Lymphocytes
2nd most abundant WBCs
Formed in bone marrow
Increase in lymphocyte occurs particularly in viral infections such
as rubella, mumps, infectious hepatitis and infectious
mononucleosis
Monocytes
Increased in infections ex: typhpoid, subacture bacterial
endocarditis, infectious mononucleosis and tuberculosis
Coagulation
Process by which a platelet and fibrin plug is formed to seal a site of
injury or rupture in a blood vessel
4. Monitoring anticoagulant therapy
One stage Prothrombin Time (PT)
Measuring the PT is the most commonly used method for monitoring
oral anticoagulation activity
PT is responsive to depression of three of the four vitamin K
dependent factors (II, VII and X)
PT is measured by adding calcium and thromboplastin (phospholipid-
protein extract of tissue that promotes the activation of factor X by
factor VIII) to citrated plasma
International Normalized Ratio (INR)
Results are expressed as a ratio of the PT time of the patient compared
with that of the normal control
D-dimers
Degradation products of fibrin clots
formed by the sequential action of three enzymes = thrombin, factor
VIIIa and plasmin; which degrades cross-linked fibrin to release fibrin
degradation products and expose the D-dimer antigen
Xanthochromia
Yellow discoloration of cerebrospinal fluid caused by hemoglobin
catabolism
Arise within several hours of subarachnoid hemorrhage (SAH) and can
help to distinguish the elevated red cell count observed after traumatic
lumbar puncture from that observed following SAH
Spectrophotometry – detects the presence of both oxyhemoglobin and
bilirubin which contribute to xanthochromia
Iron, transferring and iron binding

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 75
Iron important in production of hemoglobin and myoglobin
Iron circulating in the serum is bound to transferring
Leaves the serum pool and enters the bone marrow where it becomes
incorporated into hemoglobin in developing red cells
Serum iron levels are extremely labile and fluctuate throughout the day
and provide little useful info about iron status
Iron balance is regulated by hepdicin, a circulating peptide hormone,
which aims to provide iron as needed, while avoiding excess iron
promoting formation of toxic oxygen tradicals.
Iron overload causes high concentrations of serum ferritin as can liver
disease and some forms of cancer
Vitamin B12 and folate
Liver disease tends to increase B12 levels and may be reduced in folate
deficient patients
Malabsorption of B12 may result from long-term ingestion of antacids
such as proton pump inhibitors or H2-antagonists or biguanides
(metformin)
Serum folate levels tend to increase in B12 deficiencies and alcohol
can reduce levels
C. Complimentary and Medicinal Interventions
a. Alternative Medical Systems
Alternative medical systems are built upon complete systems of theory
and practice. Often, these systems have evolved apart from and earlier than the
conventional medical approach used in the United States. Examples of alternative
medical systems include: Acupuncture, Ayurveda, Homeopathy.
b. Mind-Body Interventions
Mind-body medicine uses a variety of techniques designed to enhance the
mind's capacity to affect bodily function and symptoms. Some techniques that
were considered alternative in the past have become mainstream (for example,
patient support groups and cognitive-behavioral therapy).
c. Biologically-based Therapies
Biologically based therapies in complementary and alternative medicine
use substances found in nature, such as herbs, foods, and vitamins. Some
examples include: Diet, Dietary supplements

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 76
D. Therapeutic planning and patient counseling
a. Therapeutic Planning/ Drug Use Process
i. Need for a Drug
Ensure there is an appropriate indication for each drug and
that all medical problems are address therapeutically
ii. Select drug
Select a recommend the most appropriate drug based upon
the ability to reach the therapeutic goals
iii. Select regimen
Select the most appropriate drug regimen for
accomplishing the therapeutic goals
iv. Provide drug
Facilitate dispensing of the drug and ensure the drug is
accurately prepared and delivered to the right patient and
administration site and time basis
v. Drug administration
Ensure that appropriate devices and techniques are used for
drug administration
vi. Monitor drug therapy
Monitor drug therapy for effectives or adverse effects in
order to determine to maintain, modify or discontinue
vii. Counsel patient
Educate patient or caregiver about the patient’s therapy to
ensure proper use of medicines
viii. Evaluate effectiveness
Evaluate patient’s drug therapy by reviewing previous steps
of the drug use process and take appropriate steps to ensure
the therapeutic goals are achieved.
b. Patient Counseling
i. Exercise active listening
Allow patient to state the problem completely, and the
pharmacist should provide undivided attention to minimize

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 77
misperception and misunderstanding. Then the pharmacist
must be able to summarize mentally what the patient has
said and provide positive feedback that conveys
understanding of the problem
ii. Question the patient thoroughly
The patient often provides incomplete or contradictory
information, with experience, the pharmacist should be able
to gather the needed information in a period of minutes.
This will be easy if the proper medications are asked to the
patient. If the situation is more complex and time-
consuming, the pharmacist can ask the patient to return at a
mutually agreeable time, contact them by telephone or refer
directly to physician
iii. Interpret verbal and nonverbal communication
Every question asked to the patient should be phrased
carefully to facilitate interpretation. The pharmacist should
be able to convey his interest to be of help to the patient. It
is important to be aware of the patient’s nonverbal cues.
The pharmacist should assess the patient physically,
through observation or inspection. This would provide
clues to the overall state of health of the patient, and these
provide insight to the seriousness of the problem.
E. Monitoring of Drug Therapy and Utilization
Patient Monitoring Format
Current Medications
Start Date Medication/
Route
Dose/Schedule Stop Date Start Date
F. Monitoring and Report of Adverse Drug Reactions and Interactions
Several countries in the world conduct national reporting programs for ADRs. Most programs rely on voluntary reporting by physicians, and in some
cases, reporters are appointed to coordinate this activity in hospitals. This is one
Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 78
of the responsibilities of the PTC (Pharmacy and Therapeutics Committee). However, a subcommittee can be organized to work closely with the PTC.
The PTC should be the repository for adverse drug reaction reports since the committee is the one responsible for accepting and deleting drugs in the
hospital formulary. As such, the committee should be provided with continuing feedback of significant drug therapy problems in the hospital. These reports can in turn be reported to the entire medical staff through the
pharmacy bulletin or other hospital publications. Problems related to drug administration can be solved through close coordination with the nursing staff in
establishing parameters for monitoring drug therapy, collaborating in-patient education and discharge planning, and providing routine drug information.
G. Drug Use Review
With the abundance of drug products which do not reflect the actual health
needs of patients in hospitals and considering the limited financial and manpower resources, it is important to improve the quality ofdrug usewithin a health care
organization. The development of an evaluation process would lead to corrective measures in drug utilization for patients and reduction in cost of care.
Drug utilization is defined as an authorized, structured, and continuing program which reviews, analyzes and interprets patterns of drug use in a given
health care delivery system against a predetermined standard. The predetermination of standards of care provides both scientific validity to the work and acceptability by the hospital staff.
H. Monitoring and Reporting of Medication errors and Pharmacovigilance
consideration
If an error occurs in the administration or application of medication, the proper official should be informed immediately. Medication errors should not be
discussed with the patient. A detailed account of the error, whether of omission or commission, should be prepared with duplicate and forwarded to the proper official.
I. Pharmacoeconomics
Pharmacoeconomics refers to the scientific discipline that compares the value of one pharmaceutical drug or drug therapy to another. It is a sub-discipline of health economics. A pharmacoeconomic study evaluates the cost (expressed in
monetary terms) and effects (expressed in terms of monetary value, efficacy or enhanced quality of life) of a pharmaceutical product. There are several types of pharmacoeconomic evaluation: cost-minimization analysis, cost-benefit
analysis, cost-effectiveness analysis and cost-utility analysis. Pharmacoeconomic

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 79
studies serve to guide optimal healthcare resource allocation, in a standardized and scientifically grounded manner.
One important consideration in a pharmacoeconomic evaluation is to
decide the perspective from which the analysis should be conducted (such as
institutional or societal).
J. Dose adjustment
Under most circumstances provided the preceding criteria observed, adjusting the
dose of a drug is relatively simple, since a linear relationship exists between the
dose and concentration if a drug follows firs-order elimination
a. Factors involved:
i. Patient factors (ex: severity of disease, age)
ii. Concentrations achievable at the site of action
iii. Level of sensitivity to the drug
b. Criteria
i. Capacity limited clearance
If a drug is eliminated by the liver, it is possible for the
metabolic pathway to become saturated, since it is an
enzymatic system
Initially, elimination is the first-order, but saturation of the
system occurs, elimination becomes zero-order.
For the majority of drugs
ii. Increasing clearance
iii. Therapeutic clearance
c. Dose Calculations
i. Young’s rule:
Age X Adult dose = dose for child
Age + 12
ii. Cowling’s rule
Age at next birthday (in years) X Adult dose = dose for child
24
iii. Fried’s rule for infants:
Age (in months) X Adult dose = dose for child

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 80
150
iv. Clark’s rule:
Weight in pounds X Adult dose = dose for child
150
v. Dose Based on Body Weight
Patient’s weight (kg) x Drug dose (mg) = Patient’s dose (mg)
1(kg)
vi. Dose Based on Body Surface Area (BSA)
Patient’s BSA = √ (Patient’s height (cm) x Patient’s weight (kg)
3600
Patient’s BSA (m2) X Drug dose (mg) = Patient’s dose (mg)
1.73m2
K. Nutrition
Nutrition is the act or process of being nourished.

Lorenzo Llamas Jr. / BS Pharmacy IV / Phar 9b Student 81
UNIT III: Disease Orientation and Management
A. Definition
B. Classification
C. Etiology
D. Clinical features
E. Treatment and monitoring
Recommended

















