
CKD: The Story ofmy Seventy-Eight Year Old Patient
Ajay K. Singh, MB, FRCP
Renal Division
Brigham and Women’s Hospital
Senior Associate Dean, Postgraduate Medical Education
Harvard Medical School

Ajay K. Singh Bio
▪Attending Nephrologist, Brigham and Women’s Hospital
▪Senior Associate Dean for Postgraduate Medical Education, Harvard Medical School
▪Research interests: Anemia of CKD and CKDu
▪Clinical interests: managing patients with CKD

Disclosures
▪Gilead – stock ownership
▪GSK – Research Support

Case History
• 78 year old man
• T2DM, HTN
• Scr of 1.32 mg/dL. eGFR >60 ml/min/1.73m2.
• Otherwise healthy.
• PMH- hypertension ≈15 years duration, type 2 diabetes mellitus for 8 year; Hypercholesterolemia treated with atorvastatin.
• BP-- in the 150-160 mmHg range.
• Medications: lisinopril, ASA, hydrochlorthiazide, atorvastatin, metformin, glipizide.

Case History
• PE: BP 152/68 mmHg, HR 72 bpm. Weight 120 kg, Rest of the examination negative.
• Lab values
• Dipstick urinalysis shows SG 1015, pH 6.0, trace to 1+ alb, rest is negative
• BUN 28, Serum creatinine 1.32 mg/dL, HbA1C 7.8
• Does he have kidney disease?

We don’t want to call something a disease when it isn’t
Lindeman, R. D., J. D. Tobin, and N. W. Shock. Longitudinal
studies on the rate of decline in renal function with age. J.
Am. Geriatr. Soc. 33: 278–285, 1985.
xx

7
1. Does he have risk factors for CKD?
• Susceptibility Risk Factors
• Diabetes
• Hypertension
• Older age
• Family history of CKD
• Racial or ethnic minority
• Other: low income, minimal education, kidney-mass
reduction, known kidney disease
Levey et al. Ann Intern Med. 2003;139:137-147..

The Risk of Kidney Failure Is Not Uniform
Relative risks compared to Whites:
African Americans 4.45 X
Native Americans 3.57 X
Asians 1.59 X
Xue, et al., 2000

2. Obtain laboratory Data
b.) Renal USa.) UA dipstick /Sediment

Assess albuminuria – ACR
Risk for progression
or CVD

3. Evaluate Risk of Kidney FailureKidney Failure Risk Equation (KFRE)
▪Tangri’s laboratory based equation to predict CKD progression
▪Accurately predicts CKD stage 3-5 progression over 5 years (C statistic 0.84-0.91)
▪ 3 variable KFRE – Age, Sex, eGFR
▪ 4 variable KFRE – Age, Sex, eGFR, ACR
▪ 8 variable KFRE + Ca, Phos, Bicarb, alb
Tangri et al JAMA 2011, 2016

Rate of GFR Decline in Normals and CKD Patients
25 35 45 55 65 75
Age, years
GF
R m
l/m
in
0
10
20
30
40
50
60
70
80 9
0 1
00
ESRD
1ml/min/year starting at age 45yrs
(normal ageing)
Collister D,et al, Seminars in Nephrol 36, 273-282 2016
http://www.sciencedirect.com/science/article/pii/S027092951630033X
≈ 2-3 ml/min/year

Manage Progression factors for CKD?
• Susceptibility Risk Factors
• Progression Factors
• Diabetes
• Hypertension
• Older age
• Family history of CKD
• Racial or ethnic
minority
• Other: low income,
minimal education,
kidney-mass
reduction, known
kidney disease
• Higher level of
albuminuria
• Higher BP
• Poor glycemic
control
• Smoking
• Hyperlipidemia
• Drug use
Levey et al. Ann Intern Med. 2003;139:137-147.

Algorithm for this 78 year old man
eGFR ml/min/1.73m2
Does he have risk factors?
HTN, DM
High risk group
ACRRenal US
UA and sediment?
Does he have CKD? = YES
NEXT STEPS>>>>

Keys to managing patients with CKD
• Treat BP – goal BP <130/80, multiple agents will be needed
• SPRINT Trial <120/80 goal did not include T2D pts
• Manage diabetes, GLP1RA
• ACEI/ARB
• SGLT2 inhibitor (T2D and non-diabetic patients)
• MRA - Finerenone
• Consider other interventions: low protein diet, statin

ACEi and ARBs; CCBs
• ACEi and ARB have similar antiproteinuric effects
• Combination of ACEi and ARB: 20% reduction in albuminuria – over and above either agent alone
• Dual blockade not recommended
• CCBs - Strong antihypertensive agents
• Dihydropyridine CaCBs (e.g., amlodipine): No effect on CKD progression
• Non-dihydropyridine CaCBs (e.g., diltiazem): Reduces albuminuria, but not very effective for BP reduction

Newer therapy for renal progression in T2 Diabetics: YES… SGLT2 inhibitors
• Reduction in
HbA1c ≈0.5-1.5%
without inducing
hypoglycaemia
•Weight loss of ≈
2-3kg, (calorie loss
via renal glucose
excretion (loss of
80-85g glucose per
day) at around 6
months
•Decrease SBP ≈2-
5 mmHg

• Double blind RCT, N=4401
• T2D with CKD, eGFR 30-90, UACR 0.3 to 5 g alb/g cr
• Canagliflozin, (SGLT2 inhibitor), at a dose of 100 mg daily vs. placebo
• Median F/U 2.62 years
• Primary Outcome: Reduction ≈ 30% in RR of composite of ESRD
(dialysis, transplantation, or a sustained estimated GFR of <15 ml per
minute per 1.73 m2), a doubling Scr, or death from renal or CVD causes
• Components of Primary endpoint reduction ≈ 30%
• CVD and HF benefits
June 13, 2019
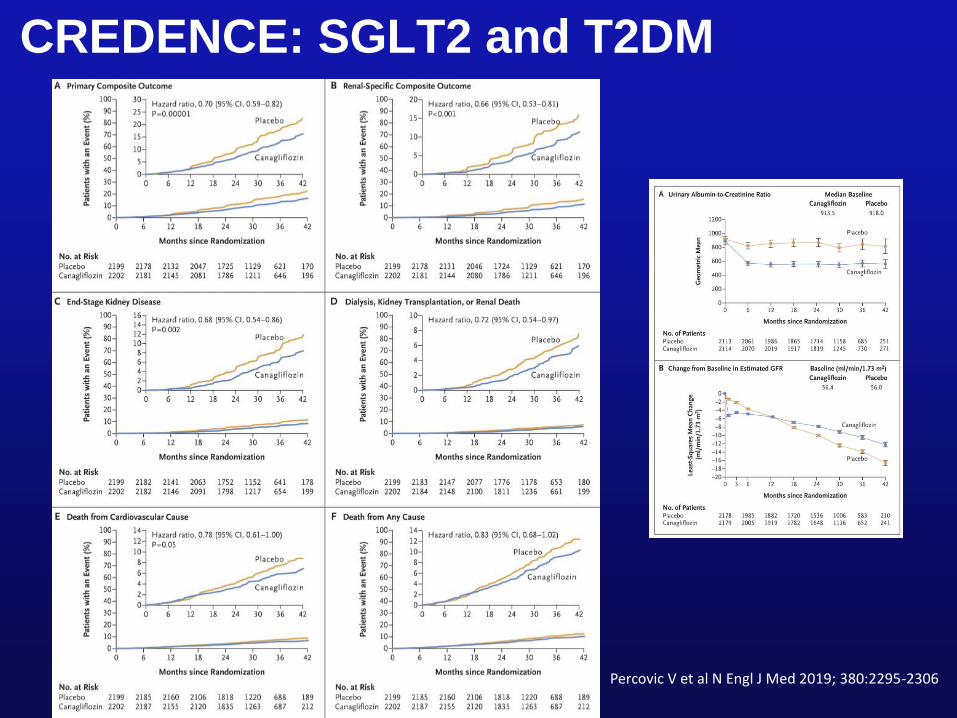
CREDENCE: SGLT2 and T2DM
Percovic V et al N Engl J Med 2019; 380:2295-2306

Both diabetics and non-diabetics benefit from SGLT2 inhibition
Oct 8, 2020
• RCT, N= 4304
• eGFR of 25 to 75 ml/min/1.73 m2, UACR 200 to 5000 mg/d, T2DM and
nonT2DM
• Dapagliflozin (10 mg once daily) vs. placebo.
• Primary outcome: composite of a sustained decline eGFR >50%, ESRD, or
death from renal or cardiovascular causes
• Median FU 2.4 years,
• Fewer primary outcomes in dapa (197 of 2152 participants (9.2%)) vs.
placebo (312 of 2152 participants (14.5%)) (hazard ratio, 0.61; 95% CI 0.51
to 0.72; P <0.001
• Number needed to treat to prevent primary=19

SGLT2 and CKD
Heerspink HJL et al N Engl J Med 2020;383:1436-46. DOI: 10.1056/NEJMoa2024816

Effect of non-steroidal mineralocorticoid receptor antagonist in CKD and T2DM
• Double blind RCT, N= 5734
• CKD and type 2 diabetes in a 1:1 ratio to receive finerenone or placebo.
• UACR 30 to <300 mg/g cre, eGFR 25 <60 ml /min/1.73 m2 and diabetic retinopathy,
or UACR 300 to 5000 and eGFR of 25 <75 ml /min/1.73 m2 . All treated with RAAS
inhibitor blockade
• Primary composite outcome: kidney failure, sustained decrease of >40% in the
eGFR from baseline, or death from renal causes.
• median follow-up of 2.6 years
• Fewer primary outcome event in finerenone (504 of 2833 (17.8%)) vs. Placebo (600
of 2841 patients (21.1%)) HR 0.82; 95% CI0.73 to 0.93; P=0.001
• Hyperkalemia-related discontinuation of the trial regimen was higher with finerenone
than with placebo (2.3% and 0.9%, respectively)
Dec 3, 2020

MRA for CKD and T2DM
Bakris GL, Agarwal R, Anker SD, et al. Effect of Finerenone on Chronic Kidney Disease Outcomes in Type 2 Diabetes. N Engl
J Med. 2020;383(23):2219-2229.\

GLP1-RAs and T2DM▪ Glucagon-like peptide-1 (GLP-1) regulates appetite and BS
• GLP-1 RAs mimic the actions GLP-1
– Slow stomach emptying
– Increase insulin production
– Reduce sugar released from the liver
▪ Short-acting (QD or BID)
– exenatide (Byetta)
– lixisenatide (Adlyxin)
– oral semaglutide (Rybelsus)
▪ Long-acting (QD-QW)
– dulaglutide (Trulicity) QW
– exenatide extended-release (Bydureon) QW
– liraglutide (Victoza) QD
– semaglutide (Ozempic) QW
▪ All GLP-1 RAs SC, except oral semaglutide

Slowing kidney progression in patients w/ CKD and T2DM
SOURCE: Sridhar VS et al, AJKD March 2021. https://doi.org/10.1053/j.ajkd.2021.02.324
SGLT2, sodium/glucose cotransporter 2; GLP-1RA, glucagon-like peptide 1 receptor agonist; MRA, mineralocorticoid
receptor antagonist; ERA, endothelin-1 receptor antagonist; ACE, angiotensin-converting enzyme; ARB, angiotensin
receptor blocker; RAAS, renin-angiotensin-aldosterone system.
👍🏿👍🏿
👍🏿
👍🏿👍🏿
👍🏿👍🏿
👍🏿

Summary
- Use GFR equations and albuminuria to make diagnosis of CKD
- Use a kidney failure risk equation
- Use multiple agents for BP control
- Use ACEi/ARB, but not in combination
- Add SGLT2 inhibitor and/or MRA for CKD+T2DN, but with modest-to-well preserved GFR
- Consider GLP1RA

References
▪ Lindeman, R. D., J. D. Tobin, and N. W. Shock. Longitudinal studies on the rate of decline in renal function with age. J. Am. Geriatr. Soc. 33: 278–285, 1985.
▪ Tangri N, Grams ME, Levey AS, et al. Multinational Assessment of Accuracy of Equations for Predicting Risk of Kidney Failure: A Meta-analysis [published correction appears in JAMA. 2016 Feb 23;315(8):822]. JAMA. 2016;315(2):164-174. doi:10.1001/jama.2015.1820
▪ Collister D, http://www.sciencedirect.com/science/article/pii/S027092951630033X
▪ Perkovic V, Jardine MJ, Neal B, et al. Canagliflozin and Renal Outcomes in Type 2 Diabetes and Nephropathy. N Engl J Med. 2019;380(24):2295-2306. doi:10.1056/NEJMoa1811744
▪ Bakris GL, Agarwal R, Anker SD, et al. Effect of Finerenone on Chronic Kidney Disease Outcomes in Type 2 Diabetes. N Engl J Med. 2020;383(23):2219-2229.\
▪ Heerspink H.J.L.Stefansson B.V.Correa-Rotter R.et al.Dapagliflozin in patients with chronic kidney disease.N Engl J Med. 2020; 383: 1436-1446
Recommended

















