25
Chapter 2
The Evolution of Ayurvedic Sector
The present chapter attempts to trace the evolution of Ayurveda, its
growth into an industry at global and national levels. The history of Ayurveda is the
history of a great civilisation. It is the part and parcel of culture, tradition and beliefs
that was transmitted from one generation to other, either verbally or vocally.
Ayurveda can be called the medical tradition of ancient culture. But Ayurveda has
stood the ravages of time. Ayurveda aims in healing body, relaxing mind, soothing
soul and renewing spirit. This system of medicine believed to have developed 5000
years ago, has its roots in India.
As in the case of any evolution, the origin of Ayurveda is widely
debated. These are several versions and interpretations regarding the origin of
Ayurveda. Some are logically consistent while others are mere folk stories. An
attempt to codify these varied views is done in the succeeding section.
2.1 Evolution of Ayurveda
History occupies a less significant spot in our thought process. We
have myths and legends in abundance but legendary accounts cannot be substitutes
for historical facts. This realisation led historians to trace the routes which the living
traditions have traversed.
According to age old belief Ayurveda, is „infinite’ and was revealed to
the sages. This notion gives spiritual sanctity to the science. For those who consider
that Ayurveda is complete in itself, any addition or deletion is an offence. This
approach discourages the spirit of enquiry, which in turn leads to decadence. The
protagonists of renaissance have realised this pitfall. To rejuvenate Ayurveda they
insisted on the study of its evolution. Search for roots thus became the prime concern

26
of the scholars during the first quarter of the last century. The main obstacles in the
study of history of the Ayurveda are the absence of reliable history of Indian society
and the lack of chronology of various movements (Varier, 2005).
2.1.1 Mythological Interpretations
According to Ashtangahridaya1, Ayurveda has no beginning. Lord
Brahma revealed it to Prajapathi. He passed it to Indra. But even these mythological
versions are mutually conflicting. For instance according to the Chraka samhita2
(5th
century), written by Charaka of Taxila University, during the end of Kratayuga3,
justice disappeared and selfish people began to accumulate more wealth. Gradually
they fell a prey, to evil passions and subsequently to illness. Sages pitied them and
assembled on the Himalayan slopes to find a remedy. They send sage Bharadvaja to
Lord Indra. Indra revealed to him the secrets of medicines. Bharadvaja later
transmitted it to their sages who developed their own samhitas3. But Sustruta (6
th to
5th
century B.C) of Varnasi University believed that Brahma created Ayurveda much
before he created man. Originally it had one lakh verses and one thousand chapters.
According to this interpretation, Brahma passed it to Prajapathi, he to Asvinis and
from him Indra got knowledge of Ayurveda, and finally Indra passed it on to
Divodosa (Dhanwanthari, 1920). The Kasyapa version takes another interpretation.
Vasistha and Atri learnt the secrets of Ayurveda from Indra. They passed it to their
sons and disciples. They received knowledge about all eight branches of Ayurveda.
2.1.2 Historical Overview
As it is not fair to trace the evolution of a civilization on the basis of
legendary myths, the modern researchers have started understanding history with the
help of material records. Their interpretations are more appealing. According to one

27
such finding, it is believed that Aryans who migrated from the Himalayan Ranges in
the northern and southern plains of river Ganges found the fertile land and moderate
climate good. They reduced their nomadic life and began to settle as an agricultural
society (Gowans, 2004). As civilization grew, a class of enthusiastic inquirers and
research scientists moved away from urban areas to rain forest areas to learn more
about plants, nature, animals and their relationship between human beings and
surroundings. These sages experimented and observed everything and these colonies
soon turned into universities of science and literature called Ashrams. They realised
specific role for all components of nature. Nature presents multifarious problems with
inherent solution. Pain and disease according to them occur due to inappropriate
imbalance with plants, animals, nature, fire and sun. At the same time healing and
happiness can be derived by using the same elements wisely. Every individual is
different, hence treatment is also different. Seemingly simple, this common sense
approach was systematically developed into comprehensive science of natural healing
called Ayurveda.
The roots of Ayurveda lie in ancient Hindu texts, called Vedas. The
history of Ayurveda lies spread over 50 centuries can be categorised into four
periods.
1. The Vedic Period
2. The Samhita Period
3. The Revival Period
4. The Present Period
Ayurveda is believed to be the Upaveda (meaning subdivision) of
Atharvaveda. There are about 160 hymns about medicines in the Atharvaveda. The
knowledge of life which was scattered in this book was well comprehended by the

28
great acharayas like Charaka, Susrutha and Vagbatha during the Samhita Period. In
the early days the science was learned in an individual manner in the traditional
gurukula system (from teacher to student and father to son). Each system had its own
techniques and formulae, which was unknown to the rest of the world. There was lot
of eminent vaidhyars (physicians) who were known in their family names. The
ashtavaidya4 tradition in Kerala is the best example. The only problem with this
tradition was that they never shared this traditional knowledge with anyone else. In
southern parts of India, Ayurvedic texts were written only in Sanskrit, the languages
of Gods. It was only studied by Brahmins (religious people who have the sole right
to pay offerings to Lord). They practiced it widely and jealously regarded it as their
family tradition. It was systematically well transmitted from father to son, and uncle
to nephew. Hence the learning and practicing of this noble healing system was
confined to this religion.
But with the starting of social reformation process and establishment
of Ayurvedic colleges this monopoly ended and Ayurveda got exposed. This
individualised education system was slowly institutionalised and history says that as
back as 2nd
century B.C., many students from different parts of the world used to
come to Nalanda University to learn Ayurveda. This finally led to modernisation and
decentralisation of Ayurveda (Trawck, 1993). Several Ayurvedic texts were
translated into Greek by Cnidos (300 B.C). The medical students from China, Tibet
and far Eastern countries traveled to India. They translated these writings to their
local languages. During Islamic period, Ayurvedic texts were translated into Persian
and Arabic. These processes though gradual and unsystematic finally led to the
widespread popularity of Ayurveda. Thus institutionalism augmented the
development of Ayurveda.

29
During this stage centers of knowledge were flourishing in Kasi and
Taxila under the guidance is of Buddhist. It was in this era that growth of Ayurveda
along with other sciences reached its acme. Ayurveda entered China, Ceylon
(present Srilanka) and South-East Asia along with Indian creeds. The knowledge that
liberated from the secretive Brahmins was exposed to the society, through open-
minded Buddhist monks. This became new upheaval and Ayurveda was considered
as an instrument of religious propaganda. When universities like Udantapuri and
Nalanda collapsed under heavy assault during the 10th
century, Ayurveda got
withered. The Mughal‟s destroyed many books and literature on Ayurveda and
subsequently it dwindled into a traditional family practice. Ayurveda could not
register any progress through observation, experimentation, discussion and
demonstration (Narayanan, 2002).
2.2 Ayurveda under British Rule
During the British rule the colonial needs of the people were largely,
met by Ayurveda, Unani Sidha & folk medicines. There was a proper interaction
between these systems of medicine. Even attempts to develop an integrated and
composite system were made during this period (Panikkar, 2002).
The introduction of western medicine was a major event during this
period. It was initially introduced for the benefit of Europeans in India and later
become a tool of the empire. The intelligent welcomed this with hesitation and
skepticism. Religious prejudices, unjustified rumors prevented the natives from
experimenting it. Raja Ram Mohan Roy was one of the pioneers who advocated and
preached the use of western medicine (Narayanan, 2003). But despite the initial
reservation the system was preferred and became attractive to the intelligentsia. It
was looked upon as a tool to embrace the modern and defy the old. Understanding

30
the possible threat, the British laid strong policy packages for the popularity of
western medicine.
During the course of the 19th
century the administrative and
institutional infrastructure necessary for the practice of western medicine was well
set by the state with the establishment of hospitals, dispensaries and colleges. This
led to the slow but steady marginalisation of the indigenous system. The colonial
authorities took it as administrative priority and made western medicine the officially
preferred system at the same time developed a hostile attitude towards all other
systems of healthcare.
The biggest challenge faced by western medicine was the existence of
irregularly qualified doctors who had received training in unorganised medical
institution or had no training at all. This endangered the hegemonic supremacy of
western medicine because its acceptance was based on its effectiveness and
effectiveness on the basis of its practice. Taking this aspect into consideration the
authorities established the Medical College in Mumbai in 1881 but came into force
only in 18875. Things changed thoroughly over the next thirty years with the passing
of Mumbai Medical Registration Act of 1912 which stressed that all medical
practitioners have to get registration. Initiated in the Province of Mumbai this was
later followed by other Presidencies also. This Act of 1912 indirectly became a big
blow to the indigenous medical practitioners who became irregularly unqualified
doctors. Thus they supplanted the indigenous system with western medicine and
excluded the indigenous system from the patronage of the state. Indigenous
practitioners were relegated to an interior status.
Despite the unlimited colonial patronage, the benefits of colonial
medicine were limited to a small section of population. The doctors were very few

31
and hospitals and dispensaries could hardly cater the needs of the population. There
were only 2272 registered medical practitioners and 571 medical centers in Madras
Presidency (Narayanan, 2002). On an average each medical institution catered to
40,000 people (Usman, 1923). Since most of the medical centers were located in
urban areas, colonial medical facilities were unavailable to rural folk. Again there
was glaring disparity within each province.
In contrast there was more than one practitioner of indigenous
medicine for every village (Adam, 1941). There were 21,000 practitioners in Madras
presidency. More significant was that, indigenous medical knowledge was not the
preserve of any particular caste and had a popular character, acceptance and easy
accessibility. In Kerala for example, the practice of Ayurveda was not limited to
Ashtavaidya family. A large number of Ayurvedic vaidhyars belonged to the lower
untouchables who formulated several medicines and used Malayalam as the medium
of instruction (Warrier, 1980). Sree Narayana Guru6, the social reformer was initially
accepted for his ability to cure diseases (Chandra, 1998). The knowledge of
Ayurveda at least in Kerala was not the monopoly of upper castes; it transcended
caste and religious barriers (Panikkar, 2002). This may be cause for the widespread
acceptance and growth of Ayurveda in the state even in the present days.
Hence it was known to the colonial masters that it is impossible to
wipe away the indigenous system. The committee on the Indigenous System of
Medicine found indigenous medicine catered the needs of 9/10th
of the population
who were not provided the official medical aid (Usman, 1923). Even in urban areas
where western medical centers existed, indigenous medicine continued to be in good
demand. On a comparison while Ayurvedic dispensaries treated 1,22,238 patients in
1921-22, the western medicine dispensaries attracted only 37,626 patients (Panikkar,

32
2002). Thus it may be interpreted that even during the days of glorified patronage of
western medicine; Ayurveda had enough space to operate, particularly in rural areas.
In spite of this, insecurity gripped the minds of the Ayurvedic practitioners, due to
the unequal treatment confirmed and due to the challenge caused by western
medicine. They were in the complex amalgam of the pride in the past, dissatisfaction
with present and apprehension for the future. The efforts to revitalise the indigenous
system during the late 19th
century and early 20th
century began from this
discontentment.
2.2.1 Stagnation Decline and Revitalisation of Ayurveda
The state of development of Ayurveda is clear from the preceding
section. Although Ayurveda was the janani (mother) of all medical knowledge, it got
into very difficult state. Antiquity however was not the sole criterion in assessing the
past; the emphasis was equally on the state of knowledge in the ancient texts.
Ayurveda had attained a high level of perfection in the past as evident from the
works of Charaka, Susruta and Vagbhata. But the causes of decline were more
internal in nature and partially exogenous.
2.2.2 Stagnation of Knowledge and Ignorance of Practitioners
However excellent were the classic texts of Ayurveda, the knowledge
contained in them had remained stagnant as there were no efforts to improve them
through experimentation and relate knowledge with new experience. Thus the main
drawback of the system was that its knowledge became outdated. Ayurvedic
treatment lost the touch of reality. Ayurveda failed to keep pace with times and
laboured within the parameters of knowledge developed in the long past. To add, it
was doubtful whether the contemporary practitioners imbibed this knowledge
sufficiently. The classic texts were not available, if available most practitioners did

33
not have the necessary language expertise to assimilate the contents. Easily
accessible texts were also not adequately made use of. Most of the practitioners
preferred the easier method of oral learning than the arduous task of reading the text.
As a result, by the end of the nineteenth century an overwhelming majority of
Ayurvedic practitioners were ignorant of their art. Their only aim was their
livelihood and in their hands the system lost its effectiveness and creditability.
2.2.3 Non-availability of Quality Medicine
The method adopted for preparing medicine was another major
weakness of the indigenous system. Medicines in prepared form were very few and
hence the patients had to prepare medicines as per the ingredients prescribed by the
physicians. What the patient prepared did not measure up to the prescription either in
content or in method (Varier, 2005). Hence a wide gap between what the physician
intended and what was actually administered by the patient occurred. As a result the
treatment turned out to be ineffective. The physician blamed patients and patients
blamed physicians. The net result or effect was the complete neglect of Ayurvedic
treatment and switching on to western medicine.
2.2.4 Loss of Political Power and Social Support
Apart from the internal causes some external factors also played a
considerable role in the revitalisation of Ayurveda. The impact of the hostile attitude
of the colonial state was the most figured external reason for the decline of
Ayurveda. Ayurveda was deprived of the state patronage and was not given a chance
to compete with the western medicine. The reason for the success of the western
medicine in India was undoubtedly the support of the government (Nair, 1981).
During this period the social support to the system was also limited. A major source
from which the system drew appreciation was the Indian ruling classes

34
(Dhanwantari, 1920). The Ayurveda family received rent free lands from the royal
families. The displacement of power from these royal families to the colonial rule led
to the total neglect of patronage. Again the educated class during this period
preferred the systematic and professionally organised western medicine. Thus the
indigenous system got marginalised both in terms of political patronage and social
support.
But the process of revitalisation of Ayurveda began at national level
with the upsurge of nationalistic feelings against the British rule. Ayurveda was
taken as a symbol of nationalism and earnest attempts began from different circles to
revamp the indigenous health care system. Two major hurdles ahead of this task of
revitalisation were stagnation of the knowledge and the lack of knowledge among
the practitioners. The former happened due to the non-availability of texts and their
use. Many did not even know that there were versions of Ayurvedic texts written in
vernacular languages. By the time the practitioners came to know of this, the works
were lost. Hence the process of revitalisation began with the dissemination of
knowledge available. There were serious efforts undertaken by many scholars to
collect books, publish and distribute it among practitioners. They organised meetings
and arranged formal and informal gatherings to share the wisdom. Under their
initiative the science of life received a new breath. The end of this process was
manufacturing at household level which later led to the large scale industrialisation
of Ayurveda in India.
2.3 International Overview of Ayurvedic Industry
International trade in herbal medicines began with the growing
dissatisfaction with the western medicine. It was in the form of herbal plants in the
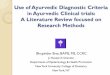
early period and later to plant extracts (Chaudhury, 1991). During the past decade

35
the global trade for medicinal plants has increased from 379.9 to 583.6 million
tonnes in 2002. During 1991 the international exports in value terms was U.S $ 1135
million and it came down to U.S $1034 million in the year 2002. In case of imports
which were U.S $ 1153 million in 1991, value fell to U.S $ 1128 million in 2002.
Thus in terms of volume, the export and import of medicinal plants are increasing
with the value of medicinal plants traded falling. This implies falling average unit
price of the medicinal plants (Lewington, 1993). This is shown in the figures given
below.
Figure 2.1
Volume of Export and Import of Medicinal Plants in the World (in MT)
0
100
200
300
400
500
600
700
1995 2000 2001 2002
Year
Vo
lum
e o
f E
xp
ort
an
d I
mp
ort
of
Med
icin
al
Pla
nts
Export Import
Source: Trade in Medicinal Plants, Raw Materials, Tropical and Horticultural Products
Service, Commodities and Trade (COMTRADE), Division Economic and Social Department,
Food and Agriculture Organization of the United Nations, Various Estimates

36
When we consider the contribution of direction of trade in herbal
plants we find China and India are the main players in this trade. But the volume of
herbs traded has declined in both the nations. The volume of exports of developed
countries as a whole increased from 60.8 million tonnes to 132.3 million tonnes. The
major exports of medicinal plants come from developing countries whose share
increased substantially from 311.1 million tonnes in 1991 to 451 million tonnes in
2002.
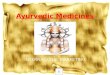
Figure 2.2
Value of Export and Import of Medicinal Plants in the World (in US $)
0
500
1000
1500
2000
2500
3000
3500
1995 2000 2001 2002
Year
Valu
e o
f E
xp
ort
an
d I
mp
ort
of
Med
icin
al
Pla
nts
Export Import
Source: COMTRADE & FAO, Various Estimates.

37
Table 2.1
Export Volume of Medicinal Plants Trade by Different Countries
(in MT)
1991 1995 2000 2001 2002
World 371.9 463.1 529.1 541.4 583.6
Developed 60.8 108.8 127.2 120.3 132.3
Developing 311.1 355.1 401.9 421.1 451.4
China 99 142.5 186.4 169.2 150.3
India 37.8 37.6 47.8 49.1 45.8
Source: COMTRADE & FAO Estimates, Various Years
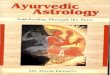
Fig. 2.3
Export Volume of Medicinal Plants by Different Countries in the World.
(in MT)
0
100
200
300
400
500
600
700
1991 1995 2000 2001 2002
Year
Ex
po
rt V
olu
me
of
Me
dic
ina
l P
lan
ts b
y
dif
fere
nt
co
un
trie
s
World Developed Developing China India
Source: COMTRADE & FAO, Estimates, 2002.
India‟s share in the global trade has remained rather inconsistent
with severe ups and downs. China‟s performance is rapidly falling in the past few
years.

38
Table 2.2
Export Value of Medicinal Plants Trade by Different Countries
(in million US $)
Source: COMTRADE & FAO, Estimates, 2002.
Figure 2.4
Export Value of Medicinal Plants by Different Countries
(in U.S $)
0
200
400
600
800
1000
1200
1400
1600
1800
1991 1995 2000 2001 2002
Year
Exp
ort
Valu
e o
f M
ed
icin
al
Pla
nts
by
dif
fere
nt
Co
un
trie
s
World Developed Developing China India
Source: COMTRADE & FAO, Estimates, 2002
The medicinal plants exported are not used for the production of
traditional medicines alone but also in production of natural products, paints etc. It is
to be noted here that the value of medicinal plants traded have come down recent
1991 1995 2000 2001 2002
World 1135.8 1525.1 1097.0 1016.2 1034.8
Developed 338.0 481.5 417.2 381.7 407.9
Developing 797.8 1043.6 679.8 634.5 627.0
China 208.3 415.4 216.5 199.7 215.3
India 52.8 65.7 79.5 78.6 68.7

39
times but the share of developed nations is increasing consistently because they
mainly deal with medicinal plant extracts. The global trade in medicinal plants is
dominated by a few countries. About 80 percent of the medicinal trade comes from
12 leading countries which are Asian and European countries (COMTRADE, 2007).
The Asian countries account for 41percent of imports and 48 percent of exports. One
third of the global imports come from Europe. China‟s share is three times more
than that of Hong Kong and four times the size of India and Mexico. It is to be noted
that although India has the third place in the total export in terms of quantity traded,
the value of her exports are much lower than that of USA. This may be due to poor
value addition. USA mainly imports plant raw materials and very little processed
plant products but exports chiefly processed plant products only (Lange, 2006). But
India has a special place among the nations in trade. There are 95 trading partners in
India‟s medicinal plant trade. The major export destinations are USA and Europe.
India imports mainly from neighboring countries like Nepal, Afghanistan etc. From
a brief account of the dimensions in trade of medicinal plants certain broad
conclusions can be drawn.
The exports of medicinal plants are dominated by developing countries
whereas developed countries are the chief importers.
There are only a few players in this trade. 80 percent of the trade is in the
hands of 12 countries.
Japan, USA, Republic of Korea, Germany, Japan and France are the main
consumer countries whereas China, India, Mexico, Bulgaria, Chile,
Egypt, Morocco and Albania are the chief suppliers of this commodity.
The bulk of the botanicals trades are in their wild origin and not in the
processed form.

40
Export of medicinal plants in their raw form fetches less value than in
processed form and extracts.
The increase in the demand for medicinal plants led to the growing
preference for any health supplement based on plant material (FRLHT, 1999). The
safety, efficacy and cost effectiveness of Ayurveda has been accepted globally.
While medicinal plants are being utilised in the preparation of Ayurvedic drugs,
there is a global trend of using herbal medicines as a part of a movement which asks
for the use of natural or green products. World demand for herbal products has been
growing steadily at a rate of 10 to 15 percent per annum (EXIM Bank, 2002). Due to
the unorganised nature of the market, lack of availability of authentic data, the
nature in which the Ayurvedic medicines are classified in the data list of
international trade makes it very difficult to reach a definite conclusion. However
what is seen is a growing demand for Ayurvedic medicines, treatments, and
massages. The domestic market in India for indigenous medicines is dominated by
Ayurveda with a share of 84 percent while that of Sidha and Unani comes to a
negligible extent. If we take a quick look of the major trading partners for
Ayurvedic medicines, it can be seen that European Union is the largest importer of
herbal medicines from India with 45 percent and followed by ASEAN and Japan
with 17 percent and 16 percent respectively (EXIM Bank, 2002).

41
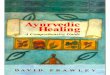
Fig 2.5
Exports of Ayurvedic Medicines from India
45%
17%
16%
11%
4%
7%
European Union ASEAN Japan N.America Rest of Europe Others
Table 2.3
Major Export Destinations of Ayurveda from India (Regions)
(US$ million)
Importing
Country
1999-2000
2000-01
Growth (%)
World 77.72 126.94 63.33
America 24.69 40.41 63.67
Europe 21.85 36.80 68.42
Africa 5.25 6.41 22.10
Source: DGCIS, 2001.
It has to be understood that the export market of Ayurveda products
have been to developed countries especially America and Europe. The growth of

42
exports to these regions has been explained in the table 2.3. The table shows that
there has been a robust growth in all these regions with rapidly increasing
exports to the African regions.
Further insight to this table can be had if we analyse the exports from
India to different nations. It can be found from the table given below that there is
tremendous improvement in the exports from India to all eight destinations. In
value terms USA happens to be the largest importer of Ayurvedic medicines
from India. But when we consider the percentage of growth we find that India‟s
export to Germany has increased by 157 percent.
Table 2.4
Major Export Destinations of Ayurvedic Medicines from India
(Countries) (US$ million)
Importing Country 1999-2000 2000-01 Growth (%)
USA 21.41 35.71 66.79
Germany 3.12 8.04 157.69
Russia 3.84 5.79 50.78
UK 2.76 4.83 75.00
Taiwan 1.95 4.24 117.44
UAE 1.75 2.95 68.57
Hong Kong 0.89 2.87 222.47
Malaysia 1.26 2.25 78.57
Source: DGCIS, Ministry of Commerce and Industry
Compiled by CMIE, India Trades Database, 2001.
2.4 An Outline of Ayurvedic Industry in India
The industrialisation of Ayurvedic industry in the country began
much before the establishment of Ayurvedic industry in Kerala. At national level the

43
beginning was a part of the greater revolt against the British hegemony than the
development of indigenous health care system. In India, Chandra Kishore Sen in
Bengal opened a dispensary in 1828 in Calcutta for selling Ayurvedic medicines at a
cheaper rate. His firm C. K. Sen & Co. started large scale production in 1898
followed by N. N. Sen & Co. in 1884 (Leslie, 1976).
As in the case of any industry the Ayurvedic manufacturing units
were carried out at household level where the process of production was primitive.
The chief physician was the main producer and his family members joined together
to produce medicines. There are no instances of use of any kind of machines in the
process of manufacturing. Ayurvedic industry in the country, record a vivid picture
of how a prolonged history of standardisation got materialised and how the
professional transformation happened in our medical health system. This was
attributed by large scale negotiations within the system and outside the system. The
process started with educational reform in different parts of the country and lobbying
with the central and state governments to divert policy attention towards qualified
practitioners of the indigenous systems of medicines (Harilal, 2009). This necessarily
resulted in a strong pluralistic health service delivery system, where people have
better choice, but under the conditions of unequal power relations between systems
of medicine (Prasad, 2007). Along with this, was the steep increase in the price of
western medicine which encouraged people to try indigenous health system and its
resultant success made the manufacturing of Ayurvedic medicines more popular.
This soon emerged as a global trend and the preference towards plant medicine and
natural medicines bolstered. In the Indian context of medical pluralism, Ayurveda
has been seen as an indigenous counterpart to biomedicine, but in the global health
market, it is one of the many alternatives to orthodox medicine, namely biomedicine.

44
In fact, developments in Ayurveda during the past two centuries
through organised production of medicine, institutionalisation of education and
professionalisation of clinical practice have often been parallel to, or a response to
developments in biomedicine in India. But the growth of the two systems of health
care has no comparison. As mentioned in the earlier section the manufacturing in
Ayurveda has passed from small-scale physician outlet to petty/cottage production
and later to the industrial enterprise, emerging as a competing alternative to the
biopharmaceutical market. Earlier, in the initial half of the 19th century, a number of
households produced and distributed Ayurvedic drugs. But the production and
distribution was not based on any pricing mechanism. This means that while raw
herbal, metal and mineral products were traded and marketed in a big way, ready-
made medicines were never considered as a “commodity” to be marketed for money
(Harilal, 2009).
Commercialisation was never thought of in those days and the
approach of the vaidhyars was holistic. The production of medicine was concentrated
in and around the physician‟s residence or locality and the service and production
costs were not clearly distinguished. Various reasons, including the inability of the
modern system to cater to the healthcare needs of a large number of villages and the
acceptance for the vaidhyars, helped the indigenous systems to remain significant
throughout the period. The transformation from household system to bulk production
began when the vaidhyars responded generously to the spread of epidemics like
cholera and small pox in the mid 19th
century (Varier, 2002; Bhattacharya, 2001).
The first initiatives in large-scale medicinal production were seen in the late 19th
century in Bengal by Kavirajas (Gupta, 1976; Bala, 1991; Kumar, 2001) and in
Kerala by P S Varier (Varier, 2002) and later, spread to different parts of the country.

45
The vaidya community launched mechanisation to make the drug more edible to the
users, to improve the shelf life and all the more too increase creditability by
providing information regarding the ingredients used in the formulation in the outer
label of the drug. In the production process, this was accompanied by centralised
manufacturing systems and some amount of mechanisation. By the end of the 20th
century, the turnover of the industry was more than government funding for
Ayurvedic and Unani education, treatment and research (Bode, 2004).
We may delineate a second phase of commercialisation of the
Ayurvedic medical sector in the end of the 20th century, marked by a move from
bulk to mass industrialised production. In this later phase, the process was not
necessarily under the control of the vaidhyars, but with the manufacturing firms.
This phase was governed by the dynamics of the market and state regulations on
drug development, and at this juncture, clinical testing and usage of scientific
methods became a necessity. Today there are hyper modern factories of Ayurvedic
medicine and the production process is completely mechanised, where the phases of
traditional medicine production are no longer visible, though this is not true in the
case of numerous small manufacturers. The revitalisation of Ayurveda revolved
around three issues; the retrieval, systematization and dissemination of knowledge;
the creation of institutional facilities for training physicians and the preparation and
distribution of medicines (Panikkar, 2002). Understanding the nature of growth and
the potentials for growth, the Government of India has incorporated several
initiatives to redirect the growth of the industry in the right direction.
To mention, there were three agents involved in the process of
industrialisation of Ayurveda in India- companies who aimed in reviving the sector,
non-government institutions who attempted a revitalisation and the government that

46
eagerly attempted to reposition the sector (Banerjee, 2002).The legal foundation for
this was laid by the Bhore Committee in 1943. The committee was appointed by the
Colonial Government to make recommendation on the health condition of the
country and reported that it could not value the indigenous system. This remark
which became hostile to the growth of Ayurveda was widely criticized by the All
India Medical Conference held at Mumbai in 1946.
The meeting of health ministers recommended the application and
development of scientific methods to value Ayurveda, starting Ayurvedic colleges
and appointing Ayurvedic physicians in states health sector. Soon after independence
the Government of India appointed the Chopra Committee on Indigenous System of
Medicine in 1948 which became a land mark. It accepted all the above proposals and
recommended the establishment of the Drugs Enquiry Committee in 1946.
The Drugs Enquiry Committee recommended mass production. But the
situation prevailing was not indicative for the industry as such. The manufacturers
were aware of only small scale production laid down in the classical texts. The
present system did not link the possibility of linking technology with production.
The recommendations of the committee were primarily focused on the
commercialisation, standardisation of the industry. It was well realised that mass
production was possible only through mechanisation. The mechanised production
was resorted by majority of the companies and this prevented the preparation of
medicines by hand by vaidhyars. This was a serious handicap for the sector. But the
lack of standardisation was still a problem. Different texts followed different
methods and included different ingredients.

47
Table 2.5
Milestones in the Industrialisation of Ayurveda in India
Institution/ Attempt Year of
Establishment Impact
C.K SEN‟S
DISPENSARY, BENGAL 1828
first production and sale of
Ayurvedic medicines at a reduced
rate.
AYURVEDA MEDICAL
COLLEGE 1887
first Institutional
teaching of Ayurveda
BOMBAY MEDICAL
REGISTRATION
ACT
1912
all medical practitioners
needed registration
BHORE COMMITTEE 1943
legal foundation for
production of Ayurvedic
medicines
DRUGS ENQUIRY
COMMITTEE 1946
checking quality of drugs
and authenticity of
formulations
CHOPRA COMMITTEE 1948
guidelines for mass
production of Ayurvedic
medicines
AYURVEDIC
FORMULATORY INDIA 1978
framing an official
common formulation
for Ayurvedic
medicines in India
DEPARTMENT OF
INDIAN SYSTEM OF
MEDICINE AND
HOMEOPATHY
(ISM&H)
1995
Department for the
special care and
development of ISM
&H
NATIONAL
MEDICINAL PLANT
BOARD
2000 Conservation, cultivation of
medicinal plants
GOOD
MANUFCTURING
PRACTICE ( GMP)
2000
Guidelines for
requirements for
infrastructure,
quality control,
manpower and
absence of
contamination
TRADITIONAL
KNOWLEDGE DIGITAL
LIBRARY7
2002
For safeguarding the
patent and treasuring our
knowledge
Source: Compiled from 1. Narayanan (2002) 2. ISM & H (2001).
3. Report of the Expert Committee on Ayurveda, 1963

48
Hence experts in the field joined together to the launch of the
Ayurvedic Formulatory of India in 1978. The Formulatory laid down following
guidelines
1. preparation of official formulary
2. providing standards for drugs
3. laying down tests for identity
4. ensuring uniformity in physical properties and active constituents and
providing all information regarding the methods of preparation dosage
etc.
Based on these governmental efforts, several Ayurvedic medicine
manufacturing units were established in the country. many leading manufacturers
of the present day had already established their strength in market.
Dabur India limited is the largest Ayurvedic supplier and the fourth
largest fast moving consumer goods industry in India. It was established in 1884
with its headquarters at Utter Pradesh and had a turnover of more than 650 million
dollars in 2003. 15 percent of their sales volume comes from pharmaceuticals and
85 percent from cosmetic and food items. The Ayurvedic section of Dabur has 260
medicines for common ailments like cold and cough to paralysis. These materials
constitute 7 percent of the total revenue of Dabur. Other popular branded items
include Dabur Chyawanaprash, Dabur lal dandmanjan, Chewable Hajmola, Dabur
hair oil, Vatika Shampoo etc.
Sri Baidyanath Ayurvedic Bhawan Ltd (henceforth Baidyanath) was
founded in 1917 at Calcutta and specialises in Ayurvedic formulations although it
has entered into FMCG products and cosmetic products such as hair care recently.
Baidyanath had a sales turnover of 350 million dollars in 2003. They produce over

49
700 Ayurvedic products, at ten manufacturing centers and employees 1600
labourers. Most popular internationally acclaimed product is Shikkakai Shampoo,
herbal tea, massage oils and Chyawanaprash.
Zandu Pharmaceutical Works was incorporated in Bombay in 1919.
The primary focus of the company is Ayurvedic products. However, today Zandu
has a chemical division and cosmetics division. Its total sales volume is about 45
million dollars. One of its current projects is to develop a dopamine drug from a
plant extract, applying for new drug status in the U.S.
The Himalaya Drug Company was established in 1934 in Bangalore.
It currently has a business level of about 500 million dollars and has a U.S. distribution
division (Himalaya USA). It is known in the U.S. for the product Liv-52, marketed as
a liver protector and therapy for liver diseases like viral hepatitis, the product was first
marketed in India in 1955.
Charak Pharmaceuticals was founded in 1947, and currently has
three distribution centers in India; it produces liquids, tablets, and veterinary
supplies. It has gained a large advantage with its new product Evanova, a preparation
containing 33 herbs and minerals and non-hormonal active ingredients used as a
menopause treatment. The Emami Group, founded in 1974, provides a diverse range
of products, doing 110 million dollars of business annually, though only a portion is
involved with Ayurvedic products, through its Himani line; the company is mainly
involved with toiletries and cosmetics, but also provides Chyawanprash and other
health products.

50
Table 2.6
Ayurvedic Manufacturers in India on the Basis of Turnover
Number of
Units
Annual Turnover
10 large Units >12.5 $ Million ( Rs. 50 crores)
25 Medium Units
Between $1.23 Million and $12.5
Million
965 small Units $ 250,000and $ 125 Million
6000 tiny units < $ 250,000 Million ( Rs. 1 crore)
Source: Ministry of Health and Family Welfare, Government of India, 2001.
As per the records of the Indian System of Medicine and
Homeopathy(ISM&H) there are 7621 registered manufacturing units in India. The
number of unregistered manufacturers will be more than half the number of the
registered units. The state wise data on the number of manufacturing units is given
in the Appendix. Uttar Pradesh has the largest number of manufacturing units in
India followed by Kerala. Kerala accounts to16 percent of the total units in India.
Among the 7621 Ayurvedic manufacturers in India there are 15 firms which have a
turnover of more than Rs.50 crores. Around 45 companies have an annual turnover
between Rs. 5 crore and Rs. 50 crores and while remaining companies have a turn
over of less than Rs. 5 crore (EXIM Bank, 2002) Nonetheless the Ayurveda industry
is highly unorganised and mostly in small scale sector. The global demand for herbal
medicines is growing steadily at a rate of 10 percent to 15 percent in the last decade
(WHO, 2002). The revival may be attributed to the belief that green medicine is safe
and more dependable than the allopathic drug which has lot of side effects. As per
the WHO records, the 80 percent of the world population depend directly or
indirectly on herbal medicines. The herbal market includes medicines, food

51
supplements, and beauty care products which has a market of US $ 62 billion. Out of
this the market for herbal medicine is alone reported to be US$ 5 billion (EXIM
Bank, 2002). In India there is inadequate information regarding the total market for
Ayurvedic drugs. According to one such estimate, India‟s share is less than two
percent i.e., about Rs 2000-Rs 2500 crores. Out of this, the share of Kerala is Rs.
230 crores (Harilal, 2002). Of late the recent discussions with industry related
professionals revealed that the share of Kerala is around Rs. 400 crores (Survey
Data, 2008).
Endnotes
1. Basic text on Ayurvedic drug formulation
2. Charaka, Sustruta, Vagbata and Kasyapa –four versatile sages and masters of Ayurveda
3. Samhita meaning a book.
4. Ashta meaning eight, Ashtavaidya form eight nambudiri families who were gifted with
the knowledge of Ayurvda. Only they had the right to practice Ayurveda.
5. First Ayurveda course was started in Government Sanskrit College, Calcutta in 1827,
and the British discontinued it after six years)
6. Sree Narayana Guru, the most popular social reformer who preached that man has only
one caste and one religion and that whatever be the caste, man should be good.
7. The basic idea of TKDL is to make all documented information on Ayurveda available to
patent examiners so as to prevent grant of patents on non-original inventions and to
retrieve about 35,000 formulations of Ayurveda, 30 Ayurvedic experts and scientists
and five patent examiners have provided the expertise for setting up of the facility and
AYUSH works as a nodal agency.
Recommended