Chapter 12: Urologic Implications of AIDS and HIV Infection
C Fitzgerald GCH Uro 1

Overview
Epidemiology Pathogenesis Natural history Diagnosis Urologic Manifestations Occupational risk factors Anti-retroviral therapy

Epidemiology Diagnosed 1981 Prevalence: 34.6 to 42.3
million worldwide Incidence and mortality:
(2003) 4.8 M / 2.9 M -3 M /2.2 M Sub-saharan
Africa 2/3 all HIV-infected
individuals in Africa, reduced life expectancy by 15 yrs
#1 cause death men-2 women-largest African cities
Developed world deaths due to AIDS declining
US burden: 940,000 adults and children with HIV/AIDS
US incidence stable at 40,000 cases per year

Transmissionmodes of transmission contact with blood transmission from
mother to child unprotected
intercourseGlobally, unprotected
sexual intercourse between men and women is the predominant mode of HIV transmission (WHO, 2004).

Co-factors in transmission
STI Endocervix > vaginal epithelium Circumcision Sexual behaviors (see table 12-2) Anti-retroviral therapy and secretion

Table 12-2. HIV Infection Risk Associated with Sexual Behaviors Compared with Blood Exposure
Route/Type of Exposure Risk of Infection Mean/Range (%)
Transfusion of contaminated
blood 84-100
Intravenous drug use (needle sharing)
0.8
Receptive anal intercourse 0.3-0.8 Insertive anal intercourse 0.04-0.1 Occupational needlestick exposure
0.28-0.33
Insertive vaginal intercourse 0.03-0.09 Receptive vaginal intercourse 0.005-0.02Insertive oral intercourse 0.003-0.008 Receptive oral intercourse 0.006-0.02

HIV-1 or HIV-2HIV-1 Spherical shape Outer envelope Capsid with
ribonucleoprotein Glycoprotein
projections Catalytic enzymes
Reverse transcriptase Integrase Ss Viral RNA

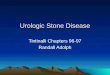
HIV Replication Glycoproteins
gp41, gp120 Co-receptors
CCR5 CXCR4 C-type lectin
Fusion Viral uncoating
protease

HIV Replication Viral RNA ds DNA
Reverse transcriptase
Transport Cytoplasm nuclei
Integration host DNA Integrase 3’ end
Shedding

Latent pool Invisible to modern
anti-retrovirals Inborn errors

Pathogenesis Primary infection
Chronic asymptomatic
Overt HIV
Transient nonspecific febrile illness, mimics mono
Incubation 2-4 weeks, self limiting 14 days, lab assays usually neg
Clinically stable, serum CD4 stable
Extracellular HIV levels elevated; trapped in lymphoid matrix
Rapid increase in viremia Rapid fall in CD4 Immunologic deterioration

Natural History Progression of disease~
time between detection and death HIV specific immune responses (without treatment) ~ 8-12 yrs (AIDS 2-3 yrs)
Median time conversion HIV AIDS
Typical 10-11 years; 60-70%
Rapid <5 years; 20% slow >15 years; 5-15% non-progressors never
progress; <1%

Diagnosis Hx: isolated 1983, first diagnostic test 1986 3 categories; diagnostic assays, viral load, drug
resistance assays (rare)
Diagnostic assays ELISA ~100% specificity (two stage)
Blood Saliva Urine
Confirmatory Immunoblotting ie. Western Blot HIV viral RNA load (day 12, others 6 weeks)

Question? + HIV Ab ELISA “-” Western Blot
Either false positive ELISA or acute infection

Diagnosis Viral monitoring; baseline before
HAART, clinical stage, risk of disease progression (De Gruttola et al 2001), increase in drug resistance
Drug-resistance assays genotypic or phenotypic predominant species only pregnancy, salvage therapy +/-
community standard

Urologic manifestations Primary infection:
viral exanthem (1-5 wks)
STI HSV – extended
course/increased severity, +/- resistance (Acyclovir parenteral, foscarnet, cidofovir)
HPV – unusual locations (lips, tongue..) higher risk recurrence after excision/treatment; CIN and SCC (see neoplasms)
Chanchroid – cofactor for HIV transmission; dx requires culture or painful ulcers supporative adenopathy and - HSV cx
Urethritis – STI vs Reiters syndrome
Molloscum contagiosum – pox virus found in10-20 % AIDS pt, CD4 < 250; dx histiologic

HSV

Urologic manifestations STI
HSV – extended course/increased severity, +/- resistance (Acyclovir parenteral, foscarnet, cidofovir)
HPV – unusual locations (lips, tongue..) higher risk recurrence after excision/treatment; CIN and SCC (see neoplasms)
Syphillis –chancre, expedited progression 2nd tertiary
Chanchroid – cofactor for HIV transmission; dx requires culture or painful ulcers supporative adenopathy and - HSV
Urethritis – STI vs Reiters syndrome
Molloscum contagiosum – pox virus found in10-20 % AIDS pt, CD4 < 250; dx histiologic

HSV

Urologic manifestations
STI HSV – extended
course/increased severity, +/- resistance (Acyclovir parenteral, foscarnet, cidofovir)
HPV – unusual locations (lips, tongue..) higher risk recurrence after excision/treatment; CIN and SCC
Syphillis –chancre, expedited progression 2nd tertiary
Chanchroid – cofactor for HIV transmission; dx requires culture or painful ulcers supporative adenopathy and - HSV
Urethritis – STI vs Reiters syndrome
Molloscum contagiosum – pox virus found in10-20 % AIDS pt, CD4 < 250; dx histiologic

Syphillis

Urologic manifestationsSTI
HSV – extended course/increased severity, +/- resistance (Acyclovir parenteral, foscarnet, cidofovir)
HPV – unusual locations (lips, tongue..) higher risk recurrence after excision/treatment; CIN and SCC (see neoplasms)
Syphillis –chancre, expedited progression 2nd tertiary
Chanchroid – cofactor for HIV transmission; dx requires culture or painful ulcers supporative adenopathy and - HSV
Urethritis – STI vs Reiters syndrome
Molloscum contagiosum – pox virus found in10-20 % AIDS pt, CD4 < 250; dx histiologic

Chanchroid

Urologic manifestationsSTI
HSV – extended course/increased severity, +/- resistance (Acyclovir parenteral, foscarnet, cidofovir)
HPV – unusual locations (lips, tongue..) higher risk recurrence after excision/treatment; CIN and SCC (see neoplasms)
Syphillis –chancre, expedited progression 2nd tertiary
Chanchroid – cofactor for HIV transmission; dx requires culture or painful ulcers supporative adenopathy and - HSV
Urethritis – STI vs Reiters syndrome
Molloscum contagiosum – pox virus found in10-20 % AIDS pt, CD4 < 250; dx histiologic

Molloscum contagiosum

Urologic manifestations GU tract Infections
Renal ie Tb, CMV, aspergillosis, toxoplasmosis
Prostatitis (8%) aerobes, anaerobes, fungi, mycobac
Epididymitis and Orchitis (39%)
Skin manifestations ie staph, nec fasciitis – Fourniers Tx surgical
Voiding dysfunction CNS/peripheral in
advanced disease retention (54%) detrusor hyper-
reflexia (27%) outflow obstruction
(18%)- Tx: meds, CIC,
suprapubic, UDS if severe

Urologic manifestations Urolithiasis- Metabolic abnormalities Radiolucent stones
Indinavir - protease inhibitor; 2-24% nelfinavir and saquinavir can also cause
stones fluids, pain control, drug rest, +/- acidify urine (4.0)
Sulfadiazine for toxoplasmosis Tx: alkalinization

Urologic manifestations HIVAN
Epi: 3.5% clinic patients, blacks>whites, IV DU
Clinical: nephrosis, RI, low CD4, low alb., edema, HTN, hyperchol, +/- hematuria, sterile pyruria
Tx: antiretrovirals delay onset +/- ACE I, ARB, immunosuppress tx
Abnl Urinalysis Hematuria** Pyuria Bacteriuria Proteinuria
**hematuria secondary to GU tumors uncommon in young males

Neoplasms Kaposi’s Sarcoma
HSV 8 and HIV homosexual males
100,000:1 Decrease incidence w/
HAART Dx: Clinical or skin bx Tx: rad, laser, cryo,
chemo (Paclitaxel) avoid steroids
Rx: CD4 > 150 ~ 35 mo CD4 <150 ~ 12-13 mo

Neoplasms NHL and
lymphoreticular malignancies Clinical sxs: fever, wt
loss, night sweats Widespread disease,
poor Rx NHL decrease with
HAART Dx: excisional bx Tx: chemo Mortality ~ 5-10 mo

Neoplasms HPV
Anogenital pre/cancer
HPV 16, 18, 31, 45 Immunosuppression
correlates with occurrence and severity
Testicular Cancer 50:1 (Wilson et al) Germ cell and NGC Bilateral High grade
lymphoma Standard tx,
although tolerated poorly

Table 12-4 HIV infection risk r/t exposure
Type of exposure Percutaneous Mucous membrane
Number of studies
27 21
Number of exposures
6807 2761
Documented infections
21 0/1
Infection rate per exposure
0.031% 0-0.11%

HAART RTI nucleoside reverse
transcriptase inhibitors; competitive inhibition and block DNA elongation zidovudine, didanosine,zalcitabine, stavudine, lamivudine, abacavir
NRTI: Nucleotide reverse transcriptase inhibitor competitive inhibition and block DNA elongation tenovir disoproxil fumarate
NNRTI: Non Nucleotide reverse transcriptase inhibitor
competitive inhibition nevirapine, delavirdine, efavirenz
Protease Inhibitors block post translational processing saquinavir, ritonavir, indinavir, nelfinavir, amprenavir, lopinavir
HAART= RTI (x2) + PI or NNRTI
Combination therapies Combivir Trizivir Kaletra

Antiretroviral therapyDeaths declining rapidly in Western
Europe and North American cities; but eradication not possible with existing therapies
HAART virus eradication ~ 50-60 years secoandry to CD4 t½~4 mo

Antiretroviral therapy: side effects Zalcitabine:
peripheral neuropathy and painful penile ulcers
Ritonavir: high risk of bleeding
Indinavir: urolithiasis
Systemic SE: hypoglycemia, lactic acidosis, mitochondria toxicity
HAART Lipodystrophy
Atrophic: face and limbs
Hypertrophic: dorsocervical fat, breast

Future strategies: vaccine (preventative
OR therapeutic) immune based
strategies that boost inherent protective responses ie pooled immune sera or monoclonal antibody transfers
Vaccine trials underway

Questions
Recommended