Challenging cases and risk assessment in clinical practice
Christian Spaulding MD, PhD, FESC, FACCCardiology DepartmentCochin HospitalParis Descartes UniversityParis, France

Trends in ACS
Inci
den
ce r
ate
(per
100
,000
)
Q-wave Non Q-wave
1975–1978
1981–1984
1986–1988
1990–1991
1993–1995
1997
ACS = acute coronary syndrome Reprinted with permission: Furman MI, et al. J Am Coll Cardiol 2001;37:1571–80
180
160
140
120
100
80
60
40
20
0

STEMI versus NSTEMI in-hospital versus 1-year-mortality
Mo
rtal
ity
(%)
9.3
7.1
5.7
10.8p<0.01
p<0.01
STEMI = ST segment elevation myocardial infarctionNSTEMI = non-ST segment elevation myocardial infarction
Adapted from: Furman MI, et al. J Am Coll Cardiol 2001;37:1571–80
STEMI
NSTEMI
14
12
10
8
6
4
2
0In-hospital mortality 1-year mortality

Months after discharge
Su
rviv
al (
MI
pat
ien
ts
dis
char
ged
ali
ve)
STEMI versus NSTEMI mortality after discharge
0 1 2 3 4 5 6 7 8 9 10 11 12
1.0
0.98
0.96
0.94
0.92
0.90
STEMI
NSTEMI
Adapted from: Furman MI, et al. J Am Coll Cardiol 2001;37:1571–80MI = myocardial infarction

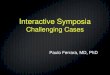
OASIS-5: mortality at days 30/180 in patients with major bleeds
Adapted from: Yusuf S. N Engl J Med 2006;354:1464–76
Major bleed 9 days
No major bleed 9 days
Days
Cu
mu
lati
ve h
azar
d
0.2
0.15
0.1
0.05
0 0 30 60 90 120 150 180

Treatment of NSTEMI: a balancing act
Clinical benefit of drugintervention
Bleeding complications

Single antiplatelet therapy
Dual antiplatelettherapy
Higher IPA
+ 60% + 38% + 32%
Relative reduction in
ischaemicevents
Relative increase
in major bleeding
The progression of antiplatelet therapy
100
80
60
40
20
0Placebo APTC1 CURE2 TRITON-TIMI 383
Aspirin–25%
Aspirin +clopidrogrel
–20% Aspirin +prasugrel
–19%
1Antiplatelet Trialists’ Collaboration. BMJ 1994;308:81–1062Yusuf S, et al. N Engl J Med 2001;345:494–502
3Wiviott SD, et al. N Engl J Med 2007;357:2001–15

A new concept was born
Bleeding carries a high risk of death, MI and stroke
Rate of major bleeding is as high as the rate of death at the acute phase of NSTE-ACS
Prevention of bleeding is equally as important as prevention of ischaemic events and results in a significant risk reduction for death, MI and stroke
Risk stratification for bleeding should be part of thedecision-making process
Bassand, JP et al. Eur Heart J 2007;28:1598–660

Risk factors for bleeding: the GRACE registry
Adjusted OR 95% CI P-value
Age (per 10-year increase) 1.28 1.21–1.37 <0.0001
Female 1.43 1.23–1.66 <0.0001
History of renal insufficiency 1.48 1.19–1.84 0.0004
History of bleeding 2.83 1.94–4.13 <0.0001
Mean arterial pressure 1.11 1.04–1.19 0.0016
Thrombolytics only 1.43 1.14–1.78 0.0017
GP IIb/IIIa blockers only 1.93 1.59–2.35 <0.0001
Thrombolytics and GP IIb/IIIa blockers 2.38 1.69–3.35 <0.0001
PCI 1.63 1.36–1.94 <0.0001
Right heart catheterisation 2.48 1.98–3.11 <0.0001
OR = odds ratio; CI = confidence interval GP = glycoprotein; PCI = percutaneous coronary intervention
Moscussi M, et al.Eur Heart J 2003;24:1815–23

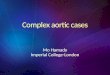
Non-CABG TIMI major bleeding: in selected subgroups of the TRITON TIMI 38 study
Prasugrel better Clopidogrel better
Kaplan-Meier event estimates for patients receiving 1 dose, within 7 days of discontinuation, or as determined locally to be related; †Tests hazard ratio = 1.0 within subgroups; ‡Tests equality of hazard ratio between subgroups; TIA = transit ischaemic attack
History of stroke or TIA Yes
No
At least one of: age 75 years, body weight <60kg, or history stroke/TIA
Yes
No
p† value
p‡
interaction
0.06 –
0.08 0.22
0.10 –
0.17 0.64
Adapted from: Wiviott S, et al. NEJM 2007;357:2001–15
Hazard ratio (95% CI)0.5 1.0 1.5 2.0 2.5 3.0 3.5 4.0 4.5 5.0 5.5 6.0 6.5

Any cause death, non-fatal MI, non-fatal stroke, non-CABG TIMI major bleeding in selected subgroups of the TRITON TIMI 38 study
Prasugrel better Clopidogrel better
History of stroke or TIA Yes
No
Yes
No
0.04 –
<0.001 0.006
0.43 –
<0.001 0.006
Hazard ratio (95% CI)0.5 0.8 1.0 1.3 1.5 1.8 2.0 2.3 2.6
Kaplan-Meier estimates intention-to-treat cohort†Tests hazard ratio = 1.0 within subgroups‡Tests equality of hazard ratio between subgroups
Adapted from: Wiviott S, et al. NEJM 2007;357:2001–15
p† value
p‡
interaction
At least one of: age 75 years, body weight <60kg, or history stroke/TIA

A difficult decision on a rainy Sunday afternoon in Paris
Male, 78 years of age
Past history– diabetes treated by insulin– haemorrhagic stroke with no sequellae 2 years ago – medical treatment: clopidogrel 75mg, atorvastatin 10mg
Chest pain on exertion for 2 weeks and at rest for 48 hours, lasting 20 minutes– last chest pain 2 hours before admission
Physical examination: 1.58m, 48kg (BMI: 19.2kg/m2)
ECG: ST segment depression in leads V1–V6
Troponin: 0.5 (normal <0.004)
Normal creatinine levelBMI = body mass index; ECG = electrocardiogram

Is this patient at low, moderate or high risk for ischaemic events?

Is this patient at low, moderate or high risk for bleeding complications?

A difficult decision on a rainy Sunday afternoon in Paris
High-risk for ischaemic events
– age
– diabetes
– ST segment depression in anterior leads
– elevated troponin
High risk for bleeding complications
– age
– past history of haemorrhagic stroke
– BMI: 19.2kg/m2

A difficult decision on a rainy Sunday afternoon in Paris
Treatment
– aspirin: 160mg followed by 100mg daily
– clopidogrel: reloading dose of 600mg, 75mg daily
– LMWH: fondaparinux 2.5mg daily
– atenolol: 100mg daily
– atorvastatin: 80mg
LMWH = low molecular weight heparin

Coronary angiogram

Coronary angiogram

Bare metal stent (2.75 x 15)

Two days later . . .

Would you initiate a GP IIb/IIIa inhibitor?

A difficult decision on a rainy Sunday afternoon in Paris
Because of the high risk profile for ischaemic events and bleeding complications, GP IIb/IIIa inhibitors were not administered and a coronary angiogram was performed 4 hours after admission via the radial artery

What would you do?

IVUS
Undersized stent (2.8mm; RVD 3.5mm)

Balloon inflation (3.5 X 12 at 22 atm)
Balloon 3.5 X 12 at 22atm

Stent thrombosis
Technical issues
Undersized stentUncovered dissection
Patient selection
Heavily calcified lesionsSmall vesselsLong lesions
Platelet aggregation
New therapeutic approaches

Treatment of NSTEMI: a balancing act
Careful patient selection– age, gender, past history of
bleeding, low weight, renal insufficiency
Clinical benefit of a drug– reduces mortality
Bleeding complications– increases mortality
Recommended