Clinical Radiology (1996) 51, 737-739
Case Report: Sonographic Diagnosis of Biceps Tendon Dislocation N. PRATO, L. E. DERCHI* and C. MARTINOLI*
Department of Radiology, San Carlo Hospital, Genoa-Voltri, and *Institute of Radiology, University of Genoa, Genoa, Italy
We report the sonographic findings in a case of medial dislocation of the long head of biceps tendon. Sono- graphic signs included an empty bicipital groove and sulcus with medial dislocation of the long head of biceps tendon. This tendon was found below the bicipital groove and luxation was not reducible during internal rotation of the arm. It appeared swollen and surrounded by a hypoechogenic effusion within the tendon sheath. The rotator cuff had normal thickness and echogenicity. We conclude that dislocation of biceps tendon can be reliably diagnosed with ultrasound. The use of CT arthrography and MRI should be limited to supplement inconclusive sonographic studies.
Dislocation of the long head of biceps tendon out of the bicipital groove is an uncommon cause of shoulder pain. Clinical diagnosis may be difficult since biceps tendon dislocation is commonly associated with a rota- tor cuff tear and has a similar clinical presentation [1,2]. A variety of diagnostic imaging modalities, including arthrography, CT arthrography and magnetic resonance (MR) imaging has been used in identifying this condition [1 6]. Surprisingly, little attention has been paid to ultrasound (US) in this field, although US is considered one of the preferred diagnostic procedures in examining the shoulder. We report the US findings in a case of medial dislocation of the long head of biceps tendon diagnosed with US.
DISCUSSION
The long head of biceps tendon originates from the supraglenoid tubercle of the scapula, and traverses intra-articularly through the shoulder joint to enter the intertubercular groove of the humerus. The tendon is retained within the humeral sulcus by a large number of structures, including anterior capsule, supraspinatus tendon, coracohumeral ligament, trans- verse humeral ligament and subscapularis tendon [7]. Disruption of these structures, as often occurs in the impingement syndrome, is believed to make biceps tendon susceptible to dislocation [1,2]. This could explain the association of dislocations of biceps tendon in rotator cuff tears. Conversely, it is rare that
CASE REPORT
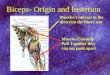
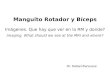
A 45-year-old left-handed man complained of left shoulder pain and functional disability following an effort to unscrew a bolt. Initial radiographs of the shoulder did not detect any traumatic lesion and a rotator cuff tear was hypothesized basing on physical examination. The patient refused shoulder arthrography and, after a short period of rest, underwent rehabilitative physiotherapy for a duration of four months which did not show any clinical improvement. Subsequently, he was referred for a US examination of the shoulder to assess status of the rotator cuff. During examination, the patient had tenderness at the anterior side of the shoulder with a reduced capability to abduct the arm. The US study, performed with a 7 .5MHz linear array transducer, showed an empty bicipital groove and sulcus with medial dislocation of the tendon (Fig. I a). The long head of biceps tendon was identified below the bicipital groove and tuxation was not reducible during internal rotation of the arm. The tendon appeared swollen, surrounded by a hypoechogenic effusion within the tendon sheath (Fig. 2a). The rotator cuff was of normal thickness and echogenicity. Then, CT arthrography was performed; it confirmed the US diagnosis through demonstration of both medial dislocation of the tendon (Fig. I b) and fluid in the tendon sheath (Fig. 2b). The patient refnsed surgery. Three months later he returned to the hospital complaining of acute left shoulder pain following sudden flexion of the forearm. Physical and US examination showed a complete rupture of the biceps tendon with distal retraction of the muscle (Fig. 3).
Correspondence to: Dr L. E. Derchi, Institute of Radiology, Uni- versity of Genoa. Viale Benedetto XV, 10. I-16132, Genova, Italy.
© 1996 The Roy~tl College of Radiologists, Clinical Radiology, 51,737-739
(a)
(b)
Fig. 1 (a) Transverse US image obtained at the bicipital groove level shows medial dislocation of the tendon (arrows) and an empty bicipital sulcus (arrowhead). (b) At the same level, CT arthrography shows the displaced biceps tendon as a slightly hypodense image (arrows). The biceps tendon sulcus is empty and contains air (arrowhead).

738 CLINICAL RADIOLOGY
(a)
(b)
Fig. 2 (a) Transverse US image obtained below the bicipital groove level demonstrates swelling of biceps tendon (arrows), which is sur- rounded by abundant effusion within its sheath. (b) At the same level, CT arthrography shows the tendon (arrows) within its dilated sheath, which is delineated by contrast medium.
a t r a u m a t i c e v e n t p r o d u c e s an i s o l a t e d t e n d o n d i s l o c a - t i o n [8].
T h e c l in ica l p r e s e n t a t i o n o f b iceps t e n d o n d i s l o c a t i o n is s imi la r to o t h e r m o r e c o m m o n s h o u l d e r a b n o r m a l i t i e s , p a r t i c u l a r l y r o t a t o r cuf f tears a n d r e c u r r e n t a n t e r i o r d i s l o c a t i o n [1]. C o n s e q u e n t l y , the r a d i o l o g i c d i agnos i s
of this abnormality is important given the difference in surgical management of these conditions. Conventional arthrography can show both the empty bicipital groove and the medial displacement of the tendon. However, a correct diagnosis cannot be established in some cases since the biceps tendon sheath may not fill with contrast medium; this finding can be encountered even in normal subjects, so it cannot be considered a specific sign of this disease [3,4]. CT arthrography optimally depicts the empty sulcus [6] but diagnostic difficulties remain when the tendon sheath fails to fill with contrast medium, because the displaced biceps tendon may be difficult to separate from the adjacent soft tissues (i.e. anterior portion of the capsule, cartilagineous glenoid labrum, subscapularis tendon) due to the similar CT density [5]. MR may have some advantages over CT arthrography in the evaluation of this abnormality, due to the multi- planar approach, and the capability to image directly the tendon, and to differentiate it from adjacent structures due to different signal intensity. In addition, MR can easily detect the tendon displacement with respect to subscapularis tendon [1,2].
In the US assessment of biceps tendon, an accurate examination technique has to be used. Transverse and longitudinal scans are acquired at the articular, inter- tuberosal and distal levels with the patient seated and the humerus in neutral position [9,10]. In this position the long head of biceps tendon is in full extension and easily assessed. When subluxation of the long head of biceps tendon is suspected, dynamic examination can demon- strate the subluxing tendon snapping in and out of the bicipital groove during internal and external rotation of the arm. When luxation does not reduce during dynamic study, transverse scans acquired medially to the bicipital sulcus can identify the biceps tendon displaced under the tendon of subscapularis muscle.
Although US is able to give direct identification of the biceps tendon and, as demonstrated in a comparative series, is superior to arthrography for the study of both normal and abnormal biceps tendon [9], little attention has been directed to the sonographic diagnosis of biceps tendon dislocation. It is conceivable that the main reason that US has not been used much in the diagnosis of this condition is because the diagnosis is generally not sus- pected on clinical grounds, and US does not play a significant role in the diagnosis of recurrent anterior dislocation of the shoulder, which is one of the more common clinical conditions mimicking this abnormality.
In conclusion, we believe that dislocation of biceps tendon should be included to the list of lesions which can be diagnosed in the US study of the shoulder. More invasive and expensive techniques, including CT arthrography and MRI, should be performed to supple- ment inconclusive sonographic studies.
Fig. 3 Longitudinal US image shows the complete rupture of the displaced biceps tendon occurring three month later. The distal segment of ruptures tendon is retracted (curved arrow) within the synovial sheath (straight arrows) filled with fluid.
REFERENCES
1 Cervitla V, Schweitzer ME, Ho C et al. Medial dislocation of the biceps brachii tendon: appearance at MR imaging. Radiology 1991;180:523 526.
2 Chan TW, Dalinka MK, Kneeland JB et al. Biceps tendon disloca- tion: evaluation with MR imaging. Radiology 1991;179:649-652.
3 Arndt RD. Clinical arthrography, 2nd ed. Baltimore: Williams and Wilkins, 1985.
4 Goldman AB, Ghelman B. The double-contrast shoulder arthrogram. Radiology 1978;127:655-663.
5 Rafii M, Firooznia H, Gotimbu C et al. CT arthrography of
© 1996 The Royal College of Radiologists, Clinical Radiology, 51, 737-739-

CASE REPORTS 739
capsular structures of the shoulder. American Journal of Roentgen- ology 1986;146:361-367.
6 Beltran J, Gray LA, Bools JC et al. Rotator cuff lesions of the shoulder: evaluation by direct sagittal CT arthrography. Radiology 1986;160:161-165.
7 Cone RO, Danzig L, Resnick D et al. The bicipital groove: radio- graphic anatomic and pathologic study. American Journal of Roent- genology 1983;141:781 788.
8 Neer CS. Cuff tears, biceps lesions and impingement. In: Neer CS, ed. Shoulder reconstruction. Philadelphia: Saunders, 1990:73 84.
9 Middleton WD, Reinus WR, Totty WG et al. Ultrasonographic evaluation of the rotator cuff and biceps tendon. Journal of Bone and Joint Surgery 1986;68:440 450.
10 Middleton WD, Reinus WR, Totty WG et al. US of the biceps tendon apparatus. Radiology 1985; 157:211-215.
Clinical Radiology (1996) 51, 739 740
Case Report: Spinal Cord
S. G R A N D , E. M O V E T a n d J -F . L E B A S
UnitO I R M , Grenoble , F r a n c e
Schistosomiasis: MRI Findings
We r e p o r t a p a t i e n t p r e s e n t i n g w i t h a n e u r o l o g i c a l def ic i t due to i n v o l v e m e n t o f t h e c o n u s m e d u l l a r i s b y S c h i s t o - s o m a M a n s o n i . B a s e d o n a n u m b e r o f e p i d e m i o l o g i c a l , l a b o r a t o r y , a n d M R ! f i nd ings , a p p r o p r i a t e c u r a t i v e che - m o t h e r a p y w a s b e g u n v e r y r ap id ly . C l i n i c a l a n d r a d i - o log ica l p r o g r e s s w a s f a v o u r a b l e .
CASE R E P O R T
A 20-year-old white male, with no significant medical history, was
hospitalized for acute urinary retention. Upon questioning it was revealed that a month before he had travelled to Burkina Fasso and had gone swimming in a river on several occasions.
The physical examination on admission revealed a normal body temperature and a palpable bladder. Rapidly the patient presented saddle anesthesia, anal incontinence, and a slight motor deficit of both lower limbs associated with pyramidal signs and tactile hypoesthesia suggesting involvement of the conus medullaris and the cauda equina. Splenomegaly was also noted.
Laboratory findings revealed an erythrocyte sedimentation rate at 20, a complete blood count showing 11 900 leucocytes/mm 3 with 29% eosinophils, and a haemoglobin of 132 g/l urine and cerebrospinal fluid (CSF) cultures were normal. Analysis of the CSF showed 60 predomi- nantly lymphocytic cells/mm 3, but there were also many eosinophils. The protein concentration was 0.985 g/t. The bilharzia indirect immuno
Fig. 1 Sagit talT2weightedimageatl .5T(TR:2780ms;TE: 150ms). Enlargement of the conus medullaris with hyper-intense signal.
Correspondence to: Dr S. Grand, Unit6 1RM, Centre Hospitalier Universitaire, Grenoble BP 217-38043, Grenoble, Cedex, France.
© 1996 The Roya] College of Radiologists, Clinical Radiology, 51, 739 -740.
Fig. 2 - Sagittal T1 weighted image after injection of Gadolinium at 0.5 T (TR: 450ms; TE: 20ms). Enlargement and enhancement of the conus medullaris.
Recommended