7/27/2019 case of 75 yr woman with chest pain,fever.pdf
http://slidepdf.com/reader/full/case-of-75-yr-woman-with-chest-painfeverpdf 1/9
case records of the massachusetts general hospital
The new england journal of
medicine
n engl j med 351;12
www.nejm.org september 16, 2004
1240
Founded by
Richard C. CabotNancy Lee Harris, m.d.,
Editor
Jo-Anne O. Shepard, m.d.
, Associate Editor
Stacey M. Ellender, Assistant Editor
Sally H. Ebeling, Assistant Editor
Christine C. Peters, Assistant Editor
Case 29-2004: A 75-Year-Old Woman with Acute Onset of Chest Pain
Followed by Fever
Adolf W. Karchmer, M.D., David F. Torchiana, M.D.,
Claudia U. Chae, M.D., M.P.H., Nadeem A. Afridi, M.D.,and Stuart L. Houser, M.D.
From the Division of Infectious Diseases,Beth Israel Deaconess Medical Center(A.W.K.); the Divisions of Cardiac Surgery(D.F.T.), and Cardiology (C.U.C., N.A.A.),and the Department of Pathology (S.L.H.),Massachusetts General Hospital; and theDepartments of Surgery (D.F.T.), Medicine(C.U.C., A.W.K., N.A.A.), and Pathology(S.L.H.), Harvard Medical School — all in
Boston.
N Engl J Med 2004;351:1240-8.
Copyright © 2004 Massachusetts Medical Society.
Dr. Claudia U. Chae:
A 75-year-old woman was admitted to the hospital because of chest
pain. One week before admission she had had an illness characterized by fever, head-ache, nausea, malaise, and anorexia. On the night before admission, she awoke witha sensation of heaviness in her chest, dyspnea, and sweating, without nausea, vomit-
ing, palpitations, or syncope. There was no improvement with the administration of sublingual nitroglycerin. She was admitted to the hospital.
The patient had had exertional chest pain for several years, which had been treated
and controlled with sublingual nitroglycerin. Forty months before admission, a cardiacultrasonographic study showed mild aortic stenosis. Eleven months before admission,she had had a non–Q-wave myocardial infarction. Cardiac catheterization revealed65 percent stenosis of the proximal right coronary artery and severe stenosis of a cir-
cumflex obtuse marginal branch; percutaneous transluminal coronary angioplasty wasperformed, with stent placement. A cardiac ultrasonographic examination disclosed
aortic stenosis with a valve area of 1 cm
2
and a mean gradient of 28 mm Hg; the left ven-tricular systolic function was normal. On the day after the placement of the stent, the
patient had episodes of tachycardia associated with dizziness; an electrophysiologicalstudy showed an easily inducible typical atrioventricular nodal tachycardia, and radio-frequency ablation was performed.
The patient had a history of hypothyroidism and in the past had had a transient ce-rebral ischemic attack, which had been managed by performing a left carotid endarter-
ectomy. Her medications were atenolol, lisinopril, fluvastatin, levothyroxine, prometh-azine, and aspirin. She drank alcohol occasionally and had smoked cigarettes in
previous years. Her mother had had diabetes mellitus and heart disease, and her fatherhad died at 67 years of age from a myocardial infarction.
On physical examination, the jugular venous pressure was normal. The tempera-
ture was 37°C, the heart rate 68 beats per minute, and the respiratory rate 16 breaths perminute. The blood pressure was 140/70 mm Hg. The carotid pulses were + bilaterally.
pres en t at i on of cas e
Copyright © 2004 Massachusetts Medical Society. All rights reserved.Downloaded from www.nejm.org on March 27, 2005 . This article is being provided free of charge for use in Indonesia.

7/27/2019 case of 75 yr woman with chest pain,fever.pdf
http://slidepdf.com/reader/full/case-of-75-yr-woman-with-chest-painfeverpdf 2/9
n engl j med 351;12
www.nejm.org september 16, 2004
case records of the massachusetts general hospital
1241
The lungs were clear. A systolic murmur, grade 2
of 6, was heard at the right upper sternal border, ra-diating to both carotid arteries; no pericardial rub was detected. The abdomen was unremarkable.
There was no peripheral edema; the femoral puls-es were + to ++ without bruits, and the pedal pulses
were ++. No focal neurologic deficit was detected.The urine was positive for protein (++), ketones
(+++), and bilirubin (+); the sediment contained50 to 100 white cells, 3 to 5 red cells, and moderate
amounts of bacteria per high-power field. The lev-els of urea nitrogen, creatinine, conjugated and to-tal bilirubin, phosphorus, magnesium, electrolytes,
aspartate aminotransferase, alanine aminotrans-ferase, amylase, lipase, creatine kinase, and crea-
tine kinase MB were all normal. Other laboratory values are shown in Tables 1 and 2.
An electrocardiogram showed a normal rhythmat a rate of 78 beats per minute and right bundle-
branch block with left anterior hemiblock; repeat-ed tracings revealed normal rhythm and right bun-dle-branch block, with ST-segment depression of
0.5 mm inferiorly and as much as 1 mm in leads V
4
through V
6
. A chest radiograph showed cardio-
megaly; the mediastinal contour was within normallimits, and the lungs were clear.
Specimens of blood and urine were obtained
for culture, and levofloxacin was begun as treatment for a possible urinary tract infection. The patient
was treated with aspirin, beta-blockers, nitrates, andmorphine in the emergency room, and her initial
chest pain resolved over the course of four hours.
She had recurrent chest pain on the first hospitalday and two further episodes on the fourth hospital
day; the patient reported that the pain resembledthe angina she had had in the past, and it appeared
to respond to treatment with nitrates. The troponinT level was elevated, at 0.21 ng per milliliter, on ad-
mission; it decreased to 0.17 ng per milliliter onthe next day, was 0.19 ng per milliliter on the fourthhospital day, and then subsequently declined. The
levels of creatine kinase and creatine kinase MB re-mained normal. Minidose heparin was injected for
prophylaxis against deep venous thrombosis.Twelve hours after admission, the temperature
rose to 38.5°C, and a planned cardiac catheteriza-tion was aborted. The temperature rose daily there-after to between 38.4 and 39.3°C, accompanied
by shaking chills. Chest radiographs revealed that the heart and mediastinum were normal; there was
mild atelectasis in the right lower lobe but no evi-dence of pneumonia. On the third hospital day,
computed tomographic (CT) scanning of the ab-
domen and pelvis revealed no abnormalities.On the fifth hospital day, two of the six cultures
of blood drawn on the second hospital day yield-
ed gram-positive cocci in pairs and short chains, which were later identified as Streptococcus anginosus
(
S. milleri
group). Treatment with vancomycin wasbegun. A transthoracic ultrasonographic study dis-
closed valvular aortic stenosis with calcificationof all three leaflets. An echolucent area, 2.3 cm by 0.92 cm, was present anterior to the right coronary
cusp (Fig. 1A and Video Clip 1 in the Supplemen-tary Appendix, available with the full text of this
article at www.nejm.org), and several small mo-bile echodensities on the atrial and ventricular side
Table 1. Hematologic Laboratory Data.
Variable On Admission
Hematocrit (%) 34.4
White-cell count (per mm
3
) 11,400
Platelet count (per mm
3
) 117,000
Mean corpuscular volume (
m
m
3
) 85
Prothrombin time (sec) 13.5
Partial-thromboplastin time Normal
* To convert the value for glucose to millimoles per liter,multiply by 0.05551. To convert the value for calcium tomillimoles per liter, multiply by 0.02495. To convert thevalues for cholesterol to millimoles per liter, multiply by0.02586.
Table 2. Blood Chemical Values.*
Variable On Admission
Glucose (mg/dl) 143
Calcium (mg/dl) 8.1
Cholesterol (mg/dl)
Total 107
High-density lipoprotein 10
Low-density lipoprotein 71
Triglycerides (mg/dl) 129
Protein (g/dl)
Total 5.7
Albumin 1.9
Globulin 3.8
Alkaline phosphatase (U/liter) 201
Lactate dehydrogenase (U/liter) 284
Troponin T (ng/ml) 0.21
Copyright © 2004 Massachusetts Medical Society. All rights reserved.Downloaded from www.nejm.org on March 27, 2005 . This article is being provided free of charge for use in Indonesia.

7/27/2019 case of 75 yr woman with chest pain,fever.pdf
http://slidepdf.com/reader/full/case-of-75-yr-woman-with-chest-painfeverpdf 3/9
n engl j med 351;12
www.nejm.org september 16
, 2004
The
new england journal of
medicine
1242
of the cusps were seen (Fig. 1B and Video Clip 2 inthe Supplementary Appendix). The peak transaor-tic gradient was 36 mm Hg and the mean gradient
20 mm Hg. There was moderate aortic regurgita-tion as visualized on Doppler ultrasonography.
There was symmetrical left ventricular hypertro-phy; the size and systolic function of the left ven-
tricular cavity were normal. CT scanning of thebrain revealed no abnormalities. Treatment with in-travenous gentamicin and vancomycin was begun,
and levofloxacin was discontinued.On the sixth hospital day, a transesophageal car-
diac ultrasonographic study disclosed thickeningof the aortic root and a hypoechoic area anterior
to the aortic valve. Mobile, hyperechoic massesconsistent with vegetations were present on theright coronary cusp; the largest measured 0.75 cm
by 0.46 cm and was attached to the right aortic leaf-let (Fig. 1C and Video Clip 3 in the Supplementary
Appendix). No evidence of leaflet perforation orfistula formation was detected. There was Doppler
evidence of moderate aortic regurgitation (Fig. 1Dand Video Clip 4 in the Supplementary Appendix).Left ventricular size and systolic function were nor-
mal. There was a small pericardial effusion with ev-idence of right atrial inversion during a major por-
tion of the cardiac cycle, consistent with elevationof pericardial pressure. Another chest radiograph
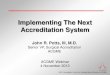
Figure 1. Echocardiograms.
A parasternal, long-axis view (Panel A) from the transthoracic echocardiogram shows a lucent area adjacent to the aorticroot, indicating an abscess of 2.3 cm by 0.92 cm (arrows). A color Doppler study (Panel B) shows a jet of aortic regurgi-
tation (yellow-orange) and aortic insufficiency (blue). A transesophageal echocardiographic view of the aortic-valve leaf-lets (Panel C) demonstrates a shaggy thickening consistent with valvular vegetations (arrows). A transesophageal
echocardiogram view of the aortic-valve leaflets as highlighted in a color-flow Doppler study (Panel D) shows evidenceof aortic insufficiency. LA denotes left atrium, Ao aorta, and AoV aortic valve.
A B
C D
Ao
LA
LA
AoV
AoV
AoV
Aov
Copyright © 2004 Massachusetts Medical Society. All rights reserved.Downloaded from www.nejm.org on March 27, 2005 . This article is being provided free of charge for use in Indonesia.

7/27/2019 case of 75 yr woman with chest pain,fever.pdf
http://slidepdf.com/reader/full/case-of-75-yr-woman-with-chest-painfeverpdf 4/9
n engl j med 351;12
www.nejm.org september 16, 2004
case records of the massachusetts general hospital
1243
disclosed mild cardiomegaly with clear lungs. Peni-
cillin G was substituted for vancomycin, in responseto results of tests to determine the sensitivity of theorganism. The spiking fevers and chills continued.
The results of cultures of blood from the fifth andsixth hospital days were negative.
On the seventh hospital day, chest radiographsshowed an enlarged cardiac silhouette and bilat-
eral pleural effusions with associated atelectasis.The temperature rose to 39.3°C, with rigor.
Dr. Chae:
This 75-year-old woman with a history of coronary artery disease and aortic stenosis came to
the hospital with chest pain of recent onset. The ini-tial impression of the cardiology team was that she
had unstable angina with a non–Q-wave myocar-dial infarction. As we were about to perform cardiac
catheterization, she had a shaking chill, and feverdeveloped. A chest radiograph showed no evidenceof pneumonia. Our differential diagnosis at this
point included subacute bacterial endocarditis, my-opericarditis, and, possibly, cardiac ischemia due
to increased physiological demand in the context of a febrile illness. On the fifth day, we received areport that two blood cultures were positive for
gram-positive cocci, which were later identified as
S. anginosus
(
S. milleri group). We then became very
concerned about endocarditis, changed her anti-biotic coverage, and obtained cardiac ultrasono-
graphic studies.
May we see the imaging studies?
Dr. Nadeem A. Afridi:
A transthoracic echocar-
diogram obtained in the parasternal long axis re- veals a pericardial effusion and an echolucent space,
consistent with an abscess cavity 2.3 cm by 0.92cm, in the anterior aortic-root wall (Fig. 1A and
Video Clip 1 in the Supplementary Appendix). Theaortic valve is thickened, with an attached substancesuspected to be vegetations. Color Doppler visuali-
zation shows moderate-to-severe aortic regurgita-tion with no flow in the space, suggesting no direct
communication between the abscess cavity and theaortic lumen (Fig. 1B and Video Clip 2 in the Sup-
plementary Appendix).A transesophageal echocardiogram again shows
the echolucent space with a mild pericardial effu-
sion, suggesting a diagnosis of pericarditis in thesetting of endocarditis. The valve leaflets are ragged
and thickened and prolapse slightly into the out-flow tract, affecting the integrity of the valve (Fig.
1C and Video Clip 3 in the Supplementary Appen-
dix) and inducing severe regurgitation (Fig. 1D andVideo Clip 4 in the Supplementary Appendix).
Dr. Chae:
At this point, we knew that the patient
had endocarditis; we believed she was receivingappropriate antibiotic therapy, and the blood cul-
tures became negative. However, the findings onthe transesophageal echocardiogram were highly
worrisome, and on the seventh day, her fever spikedagain, and a chest radiograph showed an enlarged
cardiac silhouette. At this point, I sought urgent consultation from my colleagues in infectious dis-eases and cardiothoracic surgery, who had been in-
volved in the patient’s care since the first echocar-diogram was performed. I would like to invite Dr.
Karchmer to give us his thoughts on further evalu-ation and management of this case.
Dr. Adolf W. Karchmer:
In a case such as this, the
infectious-disease consultant needs to address sev-
eral questions. What is the significance of the or-ganism isolated from the patient’s blood? Does thispatient have endocarditis, and if so, what would
be the optimal antimicrobial therapy? What is themeaning of the persistent fever and the echolucent
area in the upper septum anterior to the right coro-nary cusp? What adjunctive therapy would be indi-cated and why, and when should it begin?
This patient’s blood cultures grew S.
anginosus
,a member of the S.
milleri
group. This is the col-
lective designation for three species, S. intermedius,
S. constellatus,
andS. anginosus.
The organisms in this
group are often a
-hemolytic, but occasionally they
can be b
-hemolytic or nonhemolytic. They are foundamong the flora of the oral cavity and the gastro-
intestinal tract and are associated with abscessesand soft-tissue infections, which are often poly-
microbial, in the abdominal cavity, lower respirato-ry tract, orofacial and sinus area, and skin. In addi-
tion, they can cause hematogenous, monomicrobialabscesses in the brain, liver, spleen, subdural space,and bone, and occasionally endocarditis.
1
Does this patient have endocarditis? The modi-fied Duke criteria
2
require the presence of two ma-
jor criteria or one major and three minor criteria toestablish a definite clinical diagnosis of endocar-
ditis (Table 3). This case illustrates the value of echo-cardiography in making the diagnosis of endocar-ditis. Because neither peripheral manifestations
of endocarditis nor a diastolic murmur indicativeof new aortic regurgitation was detected on physi-
cal examination, it remained unclear until echocar-diography was performed whether the patient had
di fferen t i al di ag n os i s
Copyright © 2004 Massachusetts Medical Society. All rights reserved.Downloaded from www.nejm.org on March 27, 2005 . This article is being provided free of charge for use in Indonesia.

7/27/2019 case of 75 yr woman with chest pain,fever.pdf
http://slidepdf.com/reader/full/case-of-75-yr-woman-with-chest-painfeverpdf 5/9
n engl j med 351;12
www.nejm.org september 16
, 2004
The
new england journal of
medicine
1244
S. milleri
bacteremia and a focal extravascular in-fection or endocarditis. The echocardiographicfindings and the positive blood cultures meet ma-
jor criteria. If, for the sake of argument, the type of organism and the degree of bacteremia are not
considered sufficient for a major criterion to be met,the bacteremia would meet a minor criterion. Inthe latter case, the patient’s findings would satisfy
three minor criteria: bacteremia, a predisposingcondition (aortic stenosis), and persistent fever;
the echocardiographic findings would constitutea major criterion. Thus, by the Duke criteria, the
patient had definite endocarditis.
Is S. anginosus
a probable cause of this patient’sendocarditis? Viridans streptococci cause 30 to 50
percent of episodes of native-valve endocardi-tis,
3,4
and the S. milleri
group probably accounts
for 1 to 2 percent of cases overall. A study of infec-tive endocarditis caused by organisms of the S. mil-
leri
group
5
found that in 25 percent of the casesthere were extracardiac suppurative foci of infec-tion, 14 percent had intracardiac abscesses, and 90
percent had valvular regurgitation. These cardiacfindings are similar to those in the patient under
discussion.Organisms of the
S. milleri
group are generally
susceptible to penicillin, but they may be relative-ly penicillin-insensitive (with a minimal inhibitory concentration [MIC] of more than 0.1 µg per milli-
liter).
6,7
All of the organisms in the S. milleri
groupare susceptible to vancomycin. As was done in this
case, I would initiate therapy with vancomycin, es-tablish the MIC of penicillin, and — if the isolate
were susceptible — treat the infection with high-
dose penicillin in the range of 16 to 24 million Udaily. It is reasonable to add gentamicin, an amino-glycoside, to penicillin treatment in an attempt to
enhance the bactericidal activity of penicillin, aslong as the organism is not highly resistant to ami-
noglycosides. If the organism had been relatively resistant to penicillin, treatment with the combina-
tion of penicillin and gentamicin or with vancomy-cin should be considered.
This patient’s fever persisted after three days of adequate therapy. Without complications, the timeto defervescence in cases of endocarditis due to vir-
idans streptococci is usually three days; fever per-sists for more than five days in only 10 percent of
cases, and all patients should be afebrile by day 7.
8
Fever that persists after more than seven days of ap-
propriate antimicrobial therapy has been associ-ated with increased mortality.
8
In the context of persistent fever, there are sev-eral possibilities to consider: extensive intracardi-ac infection (intracardiac abscess accounts for 33
to 46 percent of such infections), embolic com-plications (15 to 20 percent), and drug hypersen-
sitivity (approximately 20 percent). Nosocomialevents, such as catheter-related bacteremia, diar-rhea induced by Clostridium difficile,
or pulmonary
emboli, can cause persistent fever, as can extracar-diac foci of infection, such as splenic abscesses, re-
nal abscesses, and abscesses in other areas that might require drainage or special attention.
9,10
The
latter would be an important consideration in this
patient with S. milleri
endocarditis. We also shouldbe concerned about inadequate therapy, either be-
cause the organism is resistant or because the ini-tial microbiologic data were not accurate.
Abscesses are more common with infection of the aortic valve than with infection of other valves,
and may be associated with new regurgitation, peri-carditis, and conduction abnormalities.
11-14
Con-duction abnormalities were present in this patient
but were preexisting and not progressive; however,the transthoracic echocardiogram showed an ab-
scess. Transesophageal echocardiography is mark-edly more sensitive than transthoracic echocardi-
ography for demonstrating intracardiac abscesses, with sensitivity rates of 87 to 100 percent and 28to 36 percent, respectively.
15,16
The echocardio-
gram revealed a newly dysfunctional aortic valve,continued normal left ventricular function, a peri-
valvular abscess, and a pericardial effusion withright atrial inversion during a substantial portion
* The presence of two major criteria or one major andthree minor criteria are necessary for a definitive clinicaldiagnosis of endocarditis.
Table 3. Modified Duke Criteria for Endocarditis.*
Major criteriaPositive blood cultures for typical organismValvular or endocardial involvementEchocardiographic findings of infective endocarditis
(vegetation, abscess, or new partial dehiscenceof prosthetic valve)
New valvular regurgitation
Minor criteriaPredisposing condition (predisposing heart condi-
tion or injection-drug use)Fever ≥38°CVascular phenomena (arterial emboli, septic in-
farcts) or immunologic phenomena (glomerulo-nephritis, Osler’s nodes, Roth spots, rheumatoidfactor)
Microbiologic evidence (not meeting major criteria)
Copyright © 2004 Massachusetts Medical Society. All rights reserved.Downloaded from www.nejm.org on March 27, 2005 . This article is being provided free of charge for use in Indonesia.

7/27/2019 case of 75 yr woman with chest pain,fever.pdf
http://slidepdf.com/reader/full/case-of-75-yr-woman-with-chest-painfeverpdf 6/9
n engl j med 351;12
www.nejm.org september 16, 2004
case records of the massachusetts general hospital
1245
of the cardiac cycle. A chest radiograph suggested
an increase in cardiomegaly or a pericardial effu-sion and bilateral pleural effusions. Taken togeth-er, these findings suggest an urgent need for car-
diac surgery to débride the abscess and restoreaortic-valve function.
Can this surgery be performed during active en-docarditis? Three recent studies show that for pa-
tients with active native-valve or prosthetic-valveendocarditis who were operated on during the
course of antibiotic therapy — often with recent positive cultures of blood or material from the siteof infection — there was relatively low operative
mortality.
17-19
Recurrent endocarditis was infre-quent. The timing of surgical intervention is very
important. It is the patient’s preoperative hemody-namic status that predicts postoperative mortality
rates (not the duration of preoperative antibiotictherapy), and this should be the chief consider-
ation in scheduling surgery. Delaying surgery whenthere is increasing ventricular decompensationmay lead to an increase in the rate of mortality. In-
tracardiac abscesses are rarely cured by antibiotictherapy, particularly in the context of persistent fe-
ver, and delay may allow more tissue destruction by uncontrolled infection. This patient’s abscess couldrupture into the pericardial space or form an in-
tracardiac fistula, or the aortic regurgitation could worsen. Finally, there is risk of an embolic com-
plication.In summary, this patient had intracardiac disease
that would not respond to antimicrobial therapy,
and the responsible organism, the S. milleri
group,can cause infection in other sites, such as the liver
and brain. Although surgery carries a small risk of death and of recurrent endocarditis, at this point
I would recommend urgent cardiac surgical inter- vention.
Dr. Chae:
I asked Dr. Torchiana to discuss how thedecision was made whether and when to take this
patient to surgery.
Dr. David F. Torchiana:
Most patients with native-
valve endocarditis are treated with antimicrobialtherapy and do not need surgery.
20,21
Surgery ismost clearly indicated when there has been destruc-
tion of tissue by infection and when valvular insuf-ficiency and congestive heart failure develop. Other
possible indications for surgery in endocarditis area resistant organism, persistent sepsis, extension
of infection beyond the valve, and recurrent emboli.
The term “complicated endocarditis” has been usedto differentiate those cases in which one or moreof these criteria are present.
21
This patient had
only modest aortic insufficiency, with little, if any,congestive heart failure. The infecting streptococ-
cal organism was relatively sensitive, but she hadextensive infection into the myocardium and per-
sistent sepsis.With a case of acute endocarditis and valvular
insufficiency, the temptation is to treat with anti-biotics and delay surgery if the patient’s conditioncan be managed safely in the interim. Gaining con-
trol of acute sepsis renders surgery and cardiopul-monary bypass less hazardous. Sterilization of the
field may reduce the risk of recurrent infection, es-pecially if foreign material such as a valve prosthe-
sis will be introduced. A sterilized field will havebetter tissue integrity, particularly if three or four
weeks of antibiotic therapy can be instituted beforesurgery, allowing time for scarring and fibrosis todevelop, which helps the valve sutures to hold.
There are pitfalls in delaying surgery, however,and vigilant follow-up is needed if this strategy is
undertaken. Patients with aortic insufficiency, par-ticularly younger patients, may appear to toleratea severe valve lesion with relatively little evidence of
clinical compromise, but their status may in reality be quite precarious. Recurrent emboli may be diffi-
cult to detect, particularly visceral emboli or centralnervous system emboli in patients who already have
an altered mental status. These issues must be kept
in mind when following a patient with endocardi-tis, and they must be factored into decisions on the
timing of surgery. As a general principle, patients with complicated endocarditis do better with sur-
gery than without it, and delay makes no sense if the patient’s health is deteriorating. In this pa-
tient, because of the extensive myocardial infectionand persistent sepsis, I thought that surgery wasindicated.
Once we decided that this patient would proba-bly require surgery, a decision needed to be made
whether to perform coronary angiography. In thiscase, the patient had two indications for coronary
angiography. The first was known coronary artery disease and a prior coronary intervention. Obvious-ly, the potential for new or progressive occlusive
disease made coronary angiography beneficial insurgical planning. Second, this patient had an aor-
tic-root abscess; knowledge of the relative size andcourse of the coronary arteries can be helpful in
di s cus s i on of m an ag em en t
Copyright © 2004 Massachusetts Medical Society. All rights reserved.Downloaded from www.nejm.org on March 27, 2005 . This article is being provided free of charge for use in Indonesia.

7/27/2019 case of 75 yr woman with chest pain,fever.pdf
http://slidepdf.com/reader/full/case-of-75-yr-woman-with-chest-painfeverpdf 7/9
n engl j med 351;12
www.nejm.org september 16
, 2004
The
new england journal of
medicine
1246
planning a complex aortic-root reconstruction. In
the absence of risk factors for coronary disease andin younger patients, echocardiography is sufficient preoperative imaging. The necessity of administer-
ing a contrast agent to an already sick patient andthe risk of causing embolization of aortic-valve
vegetations are relative contraindications to angi-ography. Newer techniques for noninvasive coro-
nary imaging, such as CT or magnetic resonanceangiography, may have a role in management in the
future. In this patient, we opted to do preoperativecoronary angiography, which disclosed a 40 per-cent stenosis of the left main coronary artery and
a 50 percent stenosis of the proximal right coro-nary artery.
The principles of valve surgery in endocarditishave changed relatively little since the first reported
surgery in 1965.
22
Infected tissue should be thor-oughly débrided and cultured. There is no clear ad-
vantage in terms of the risk of recurrent infection with either mechanical or tissue prostheses.
18,23-25
The lack of a need for anticoagulant treatment may
make a tissue prosthesis a safer choice early on incomplicated cases, in sick patients, and in intrave-
nous-drug users in whom noncompliance increas-es the risks associated with warfarin.
The choice of prosthesis for patients with en-
docarditis is based on the same criteria as are usedin the absence of infection. Valves that can be re-
paired should be repaired. When replacement isnecessary, tissue valves are used in older patients
and mechanical prostheses in younger patients. In
cases of complicated infection of the aortic root,such as this, implantation of an aortic homograft
(a nonviable, cryopreserved human aortic root) ap-pears to be associated with better early results and
a lower risk of recurrent infection.
26
Both the pli-ability of the homograft tissue and the fact that the
infected field is radically excluded from the blood-stream in this procedure probably contribute to itssuccess rate in spite of the greater associated tech-
nical complexity.At surgery, we found a large aortic-root abscess
extending from the left main artery around to theorigin of the right coronary artery, with purulent
destruction of part of the interventricular septum.Because of the extent of tissue destruction, we useda homograft for root replacement. The left main
coronary artery was reimplanted. The origin of theright coronary artery was surrounded by inflamma-
tory tissue and induration, which precluded mo-bilization. This vessel was ligated proximally and
bypassed with a saphenous-vein graft. The patient
recovered uneventfully, was discharged on the sixthpostoperative day, and went on to complete a six- week course of intravenous antibiotics. She is alive
and well a year later, with no recurrence of endo-carditis.
Acute bacterial endocarditis due to S. anginosus
(
S.
milleri group), with myocardial abscess.
Dr. Stuart L. Houser:
The trileaflet aortic valve was
thickened and had focal areas of calcification
27
(Fig. 2A). Vegetations were present that contained
fibrin, platelets, neutrophils, and invading coloniesof bacteria, findings that are characteristic of acute
bacterial endocarditis (Fig. 2B). The organisms weregram-positive cocci, consistent with the S. angino-
sus
(
S. milleri group) cultured in the patient’s blood.
This patient’s aortic-root abscess indicated tis-sue destruction by a virulent organism. In a study
cli n i cal di ag n os i s
pat h olog i cal di s cus s i on
Figure 2. Resected Aortic Valve.
An aortic-valve leaflet (Panel A) is thickened and contains
blue areas of dystrophic calcification (hematoxylin and
eosin). There is acute endocarditis (Panel B), with neutro-phils and gram-positive bacteria (Brown–Hopps stain).
A
B
Copyright © 2004 Massachusetts Medical Society. All rights reserved.Downloaded from www.nejm.org on March 27, 2005 . This article is being provided free of charge for use in Indonesia.

7/27/2019 case of 75 yr woman with chest pain,fever.pdf
http://slidepdf.com/reader/full/case-of-75-yr-woman-with-chest-painfeverpdf 8/9
n engl j med 351;12
www.nejm.org september 16, 2004
case records of the massachusetts general hospital
1247
of the pathogenesis of abscess formation in infec-
tions by S. milleri
, Wanahita et al.
28
observed that
S. milleri
stimulated neutrophil migration to a less-er extent than other viridans streptococci and than
Staphylococcus aureus
and survived better within hu-man neutrophils.
Dr. Chae
: The patient’s chest pain, positive tro-ponin levels, and electrocardiographic changes on
admission have several possible causes. Because of her known coronary artery disease, she may have
had subendocardial ischemia in the setting of in-creased physiological demand from her infection.Alternatively, if the aortic-root abscess had already
formed, her acute presentation could have beendue to infectious perimyocarditis. There are several
complications of endocarditis that may result incoronary ischemia. Rarely, an aortic-root abscess
can cause coronary-artery compression.
29
The most commonly described complication is septic coro-
nary embolism. This occurs in 22 to 50 percent of cases of endocarditis; whereas the majority (up to65 percent) involve the central nervous system,
other major arterial beds may be involved, includ-
ing the coronary arteries.
30
Septic emboli are morefrequent with mitral-valve infections (25 percent)than with aortic-valve infections (10 percent), and
with other organisms (such as S. aureus
and can-dida species) than with S. milleri
.
30
In streptococ-
cal endocarditis, larger vegetations are more likely to embolize, whereas with staphylococcal or fun-
gal endocarditis, the risk is independent of vege-tation size.
31
Another rare complication is the for-
mation of a mycotic coronary aneurysm with in situthrombosis and embolization,
32
although this typeof aneurysm most commonly involves the intracra-
nial arteries.
30
This case illustrates the need for continued vigi-
lance by clinicians with respect to the diagnosis of endocarditis and its possible complications.
Acute bacterial endocarditis with aortic-root abscess,due to infection by S. anginosus (
S. milleri group).
an at om i cal di ag n os i s
references
1.
Clarridge JE III, Attorri S, Musher DM,Hebert J, Dunbar S. Streptococcus intermedius,Streptococcus constellatus,
and Streptococcus angi-nosus
(“
Streptococcus milleri
group”) are of dif-ferent clinical importance and are not equally associated with abscess. Clin Infect Dis 2001;32:1511-5.
2.
Li JS, Sexton DJ, Mick N, et al. Proposedmodifications to the Duke criteria for thediagnosis of infective endocarditis. Clin In-
fect Dis 2000;30:633-8.
3.
Roberts RB, Krieger AG, Schiller NL,Gross KC. Viridans streptococcal endocar-ditis: the role of various species, includingpyridoxal-dependent streptococci. Rev Infect Dis 1979;1:955-66.
4.
Tuazon CU, Gill V, Gill F. Streptococcalendocarditis: single vs. combination antibi-otic therapy and role of various species. Rev Infect Dis 1986;8:54-60.
5.
Lefort A, Lortholary O, Casassus P, et al.Comparison between adult endocarditis dueto beta-hemolytic streptococci (serogroupsA, B, C, and G) and Streptococcus milleri:
a mul-ticenter study in France. Arch Intern Med2002;162:2450-6.
6.
Tracy M, Wanahita A, Shuhatovich Y,
Goldsmith EA, Clarridge JE III, Musher DM.Antibiotic susceptibilities of genetically char-acterized Streptococcus milleri
group strains.Antimicrob Agents Chemother 2001;45:1511-4.
7.
Doern GV, Ferraro MJ, Brueggemann AB,Ruoff KL. Emergence of high rates of anti-microbial resistance among viridans groupstreptococci in the United States. Antimi-crob Agents Chemother 1996;40:891-4.
8.
Lederman MM, Sprague L, Wallis RS,Ellner JJ. Duration of fever during treat-ment of infective endocarditis. Medicine(Baltimore) 1992;71:52-7.
9.
Douglas A, Moore-Gillon J, Eykyn S.Fever during treatment of infective endocar-ditis. Lancet 1986;1:1341-3.
10.
Blumberg EA, Robbins N, Adimora A,Lowy FD. Persistent fever in association withinfective endocarditis. Clin Infect Dis 1992;
15:983-90.11. Arnett EN, Roberts WC. Valve ring ab-scess in active infective endocarditis: fe-quency, location, and clues to clinical diag-nosis from the study of 95 necropsy patients.Circulation 1976;54:140-5.12. Blumberg EA, Karalis DA, Chandraseka-ran K, et al. Endocarditis-associated para-
valvular abscess: do clinical parameters pre-dict the presence of abscess? Chest 1995;107:898-903.13. DiNubile MJ, Calderwood SB, Stein-haus DM, Karchmer AW. Cardiac conduc-tion abnormalities complicating native valveactive infective endocarditis. Am J Cardiol1986;58:1213-7.14. Meine TJ, Nettles RE, Anderson DJ, et al.
Cardiac conduction abnormalities in endo-carditis defined by the Duke criteria. AmHeart J 2001;142:280-5.15. Daniel WG, Mügge A, Martin RP, et al.Improvement in the diagnosis of abscessesassociated with endocarditis by transesoph-ageal echocardiography. N Engl J Med 1991;324:795-800.16. Leung DYC, Cranney GB, Hopkins AP,Walsh WF. Role of transoesophageal echo-
cardiography in the diagnosis and manage-ment of aortic root abscess. Br Heart J 1994;72:175-81.17. d’Udekem Y, David TE, Feindel CM,Armstrong S, Sun Z. Long-term results of operation for paravalvular abscess. Ann Tho-rac Surg 1996;62:48-53.18. Alexiou C, Langley SM, Stafford H,Lowes JA, Livesey SA, Monro JL. Surgery foractive culture-positive endocarditis: determi-
nants of early and late outcome. Ann ThoracSurg 2000;69:1448-54.19. Baumgartner FJ, Omari BO, Robertson
JM, Nelson RJ, Pandya A, Miliken JC. Annu-lar abscesses in surgical endocarditis: ana-tomic, clinical, and operative features. AnnThorac Surg 2000;70:442-7.20. Mylonakis E, Calderwood SB. Infectiveendocarditis in adults. N Engl J Med 2001;345:1318-30.21. Hasbun R, Vikram HR, Barakat LA,Buenconsejo J, Quagliarello VJ. Complicatedleft-sided native valve endocarditis in adults:risk classification for mortality. JAMA 2003;15:1933-40.22. Wallace AG, Young WG Jr, Osterhout S.Treatment of acute bacteria endocarditis by
valve excision and replacement. Circulation1965;31:450-3.23. Sweeney MS, Reul GJ Jr, Cooley DA, et al.Comparison of bioprosthetic and mechanical
valve replacement for active endocarditis. J Thorac Cardiovasc Surg 1985;90:676-80.24. Grover FL, Cohen DJ, Oprian C, Hend-erson WG, Sethi G, Hammermeister KE.Determinants of occurrence of and survivalfrom prosthetic valve endocarditis: experi-
Copyright © 2004 Massachusetts Medical Society. All rights reserved.Downloaded from www.nejm.org on March 27, 2005 . This article is being provided free of charge for use in Indonesia.

7/27/2019 case of 75 yr woman with chest pain,fever.pdf
http://slidepdf.com/reader/full/case-of-75-yr-woman-with-chest-painfeverpdf 9/9
n engl j med 351;12 www.nejm.org september 16 , 20041248
case records of the massachusetts general hospital
ence of the Veterans Affairs CooperativeStudy on Valvular Heart Disease. J ThoracCardiovasc Surg 1994;108:207-14.25. Haydock D, Barratt-Boyes B, Macedo T,Kirklin JW, Blackstone E. Aortic valve replace-ment for active infectious endocarditis in108 patients: a comparison of freehand allo-graft valves with mechanical prosthesesand bioprostheses. J Thorac Cardiovasc Surg1992;103:130-9.26. Dossche KM, Defauw JJ, Ernst SM,Craenen TW, De Jongh BM, de la RiviereAB. Allograft aortic root replacement inprosthetic aortic valve endocarditis: a re-
view of 32 patients. Ann Thorac Surg 1997;63:1644-9.27. Horstkotte D, Loogen F. The naturalhistory of aortic valve stenosis. Eur Heart
J 1988;9:Suppl E:57-64.28. Wanahita A, Goldsmith EA, MusherDM, et al. Interaction between human poly-morphonuclear leukocytes and Streptococ-cus milleri group bacteria. J Infect Dis 2002;185:85-90.29. Clarke NRA, Forfar JC. Aortic root ab-scess presenting as unstable angina due toextrinsic compression of the left coronary artery. Postgrad Med J 2002;78:168-9.
30. Bayer AS, Bolger AF, Taubert KA, et al.Diagnosis and management of infective en-docarditis and its complications. Circula-tion 1998;98:2936-48.31. Steckelberg JM, Murphy JG, Ballard D,et al. Emboli in infective endocarditis: theprognostic value of echocardiography. AnnIntern Med 1991;114:635-40.32. Herzog CA, Henry TD, Zimmer SD.Bacterial endocarditis presenting as acutemyocardial infarction: a cautionary note forthe era of reperfusion. Am J Med 1991;90:392-7.Copyright © 2004 Massachusetts Medical Society.
35-millimeter slides for the case records
Any reader of the Journal who uses the Case Records of the Massachusetts General Hospital as a medical teaching
exercise or reference material is eligible to receive 35-mm slides, with identifying legends, of the pertinent x-ray films,
electrocardiograms, gross specimens, and photomicrographs of each case. The slides are 2 in. by 2 in., for use with a
standard 35-mm projector. These slides, which illustrate the current cases in the Journal, are mailed from the Department
of Pathology to correspond to the week of publication and may be retained by the subscriber. Each year approximately
250 slides from 40 cases are sent to each subscriber. The cost of the subscription is $450 per year. Application forms for
the current subscription year, which began in January, may be obtained from Lantern Slides Service, Department of
Pathology, Massachusetts General Hospital, Boston, MA 02114 (telephone 617-726-2974).
Slides from individual cases may be obtained at a cost of $35 per case.
Copyright © 2004 Massachusetts Medical Society All rights reservedDownloaded from www.nejm.org on March 27, 2005 . This article is being provided free of charge for use in Indonesia.
Recommended