Gwendolyn Ryals, Look at MeArtwork from The Creative Center
Julia Brown, Vice PresidentGovernment Affairs and Market Access
CADTH SymposiumApril 2015
RWE is the New Black: A Perspective from Industry

2
What is Real World Evidence (RWE)?
Generated using data from usual care setting in a range of non-interventional (observational) studies, including:
Primary data collections
Analyses of secondary data
RWE can be generated using so called “pragmatic” randomized trials that are conducted in more usual care settings that employ broad patient inclusion criteria and that investigate effectiveness (rather than efficacy) of different treatments.
A working definition of RWE…
3
Growing demand and increasing data availability moving RWE close to tipping point
RWE is growing in importance and relevance at accelerated pace
Growing demand – Focus on value and transparency
Increasing supply – Easier availability of data/analytics
Societal trends (e.g., reform, aging population, emerging middle class) increasing utilization
Markets becoming increasingly demanding as health care systems seek meaningful innovation, value and transparency
Substantial economic / pricing pressure; increased legal, regulatory, and business scrutiny
More data from new data sources, e.g., sensors, self-reported data
Better insights from structured and unstructured data
Governments (e.g., US, UK, Denmark) playing an active role making health data liquid
Engaged patients – more involved in care, sharing and generating data
4
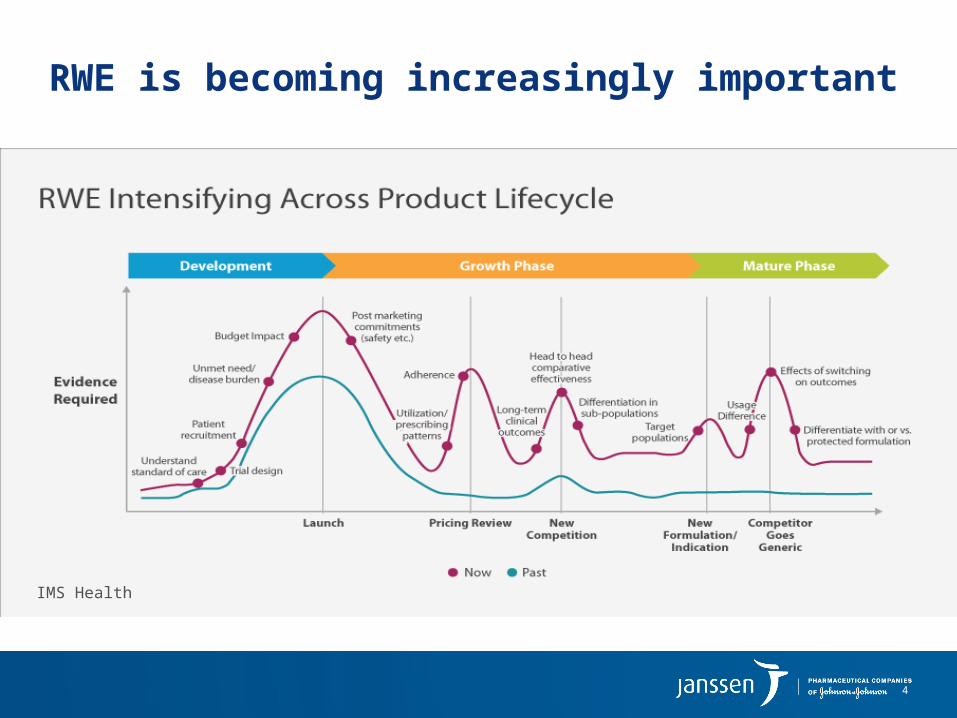
RWE is becoming increasingly important
IMS Health

5
Stakeholders responding globally
Regulators
▪ Mainly focused on pharmacovigilance
▪ Adaptive licensing concepts and corresponding use of RWE data
Payors
▪ Selected payers use RWE for formulary decisions (US) or cost/quality analyses (GER)
▪ Emerging outcomes based/risk-sharing contracts
Providers/clinicians
▪ Usage of internal RWE datasets for cost/quality monitoring and physician incentives
▪ Creating registries to generate RWE
HTA bodies
▪ Broad variation of use, some systematic (e.g, UK, Italy) others more research focused (e.g., US)
Patients
▪ Interest in real-world evidence mixed with questions on data privacy
▪ Starting to “create” real-world data via forums
Academia
▪ Broad use of RWE as source of insight to medical research
▪ Partnerships with other stakeholders
6
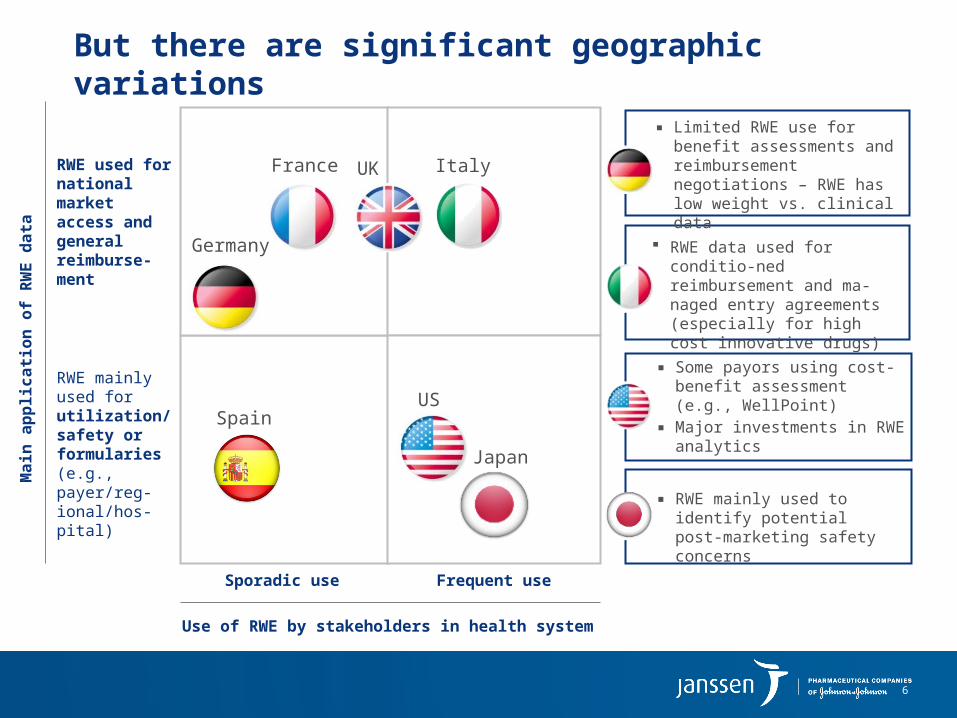
But there are significant geographic variations
RWE used for national market access and general reimburse-ment
RWE mainly used for utilization/ safety or formularies (e.g., payer/reg-ional/hos-pital)
Sporadic use Frequent use
▪ Limited RWE use for benefit assessments and reimbursement negotiations – RWE has low weight vs. clinical data
▪ Some payors using cost-benefit assessment (e.g., WellPoint)
▪ Major investments in RWE analytics
Use of RWE by stakeholders in health system
Main
ap
plicati
on
of
RW
E d
ata
France
Germany
ItalyUK
USSpain
RWE data used for conditio-ned reimbursement and ma-naged entry agreements (especially for high cost innovative drugs)
▪ RWE mainly used to identify potential post-marketing safety concerns
Japan

7
Going forward, RWE use will increase – albeit at different speeds
RWE used for national market access and general reimburse-ment
RWE mainly used for utilization/ safety or formularies (e.g., payer/reg-ional/hos-pital)
Sporadic use Frequent use
▪ Slower - RWE likely to play a somewhat larger role during drug re-evaluations post launch
▪ Faster - Higher number of payers and providers conducting HTA-type assessments (driven by data availability)
Use of RWE by stakeholders in health system
Main
ap
plicati
on
of
RW
E d
ata
▪ Faster - RWE expected to play significantly larger role during drug evaluations (3-5 yrs post launch)
Faster - RWE likely to be used more frequently at national level for access and during re-evaluations at regional level
▪ Faster - RWE use likely to increase due to increasing data availability
▪ Slower – role of HTA and RWE for market access and reimbur-sement likely to increase slowly
Outlook: At what speed will RWE usage increase?
France
Germany
ItalyUK
USSpain
Japan
▪ Slower - opportunity to increase use of RWE via Public Know-ledge Assessment process
8
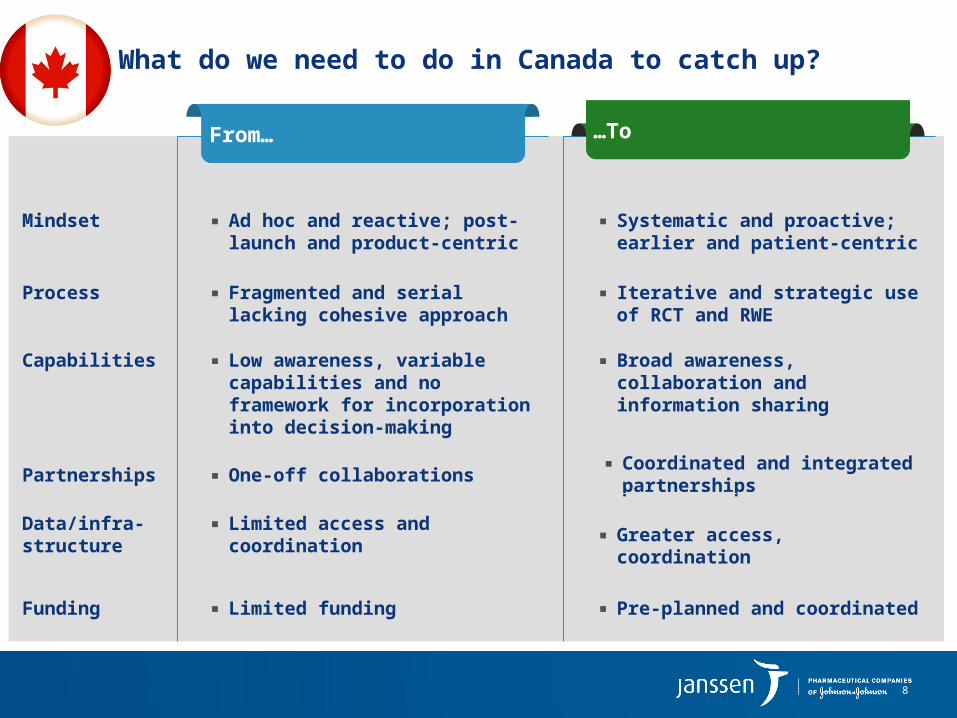
What do we need to do in Canada to catch up?
From… …To
Mindset ▪ Systematic and proactive; earlier and patient-centric
▪ Ad hoc and reactive; post-launch and product-centric
Capabilities ▪ Broad awareness, collaboration and information sharing
▪ Low awareness, variable capabilities and no framework for incorporation into decision-making
Process ▪ Iterative and strategic use of RCT and RWE
▪ Fragmented and serial lacking cohesive approach
Data/infra-structure ▪ Greater access, coordination ▪ Limited access and
coordination
Partnerships▪ Coordinated and integrated
partnerships▪ One-off collaborations
Funding ▪ Limited funding ▪ Pre-planned and coordinated

9
In Summary
Engagement and collaboration from all stakeholders:
– Patients, HTA bodies, payers, healthcare professionals, academia, industry…
Framework for RWE generation and incorporation into HTA reviews, public policy and formulary decision-making
Generation of data that balances commercial and public interests
Appropriate allocation of resources and willingness to risk-share
Prioritization of patient outcomes over short-term cost-containment
Recommended

















