By BASALINGAPPA B G
MSC MEDICAL BIOCHEMISTRYDEPT OF BIOCHEMISTRY
JSS MEDICAL COLLEGE
1. To study the importance of creatine in muscle as a storage form of energy
2. To understand the biosynthesis of creatine
3. To study the process of creatine degradation and formation of creatinine as an end product
4. To understand the clinical importance of creatinine as a sensitive indicator of kidney function
5. To study different types of creatine kinase (CK) and their clinical importance
Objectives
What’s Creatine and Creatinine
• Creatine and creatinine are not the samesubstance!• Creatine is found in the muscles…….• Creatinine is a break-down product (a waste product) of creatine phosphate. creatine in muscles, and is usually produced at a fairly constant rate by the body depending on muscle mass.
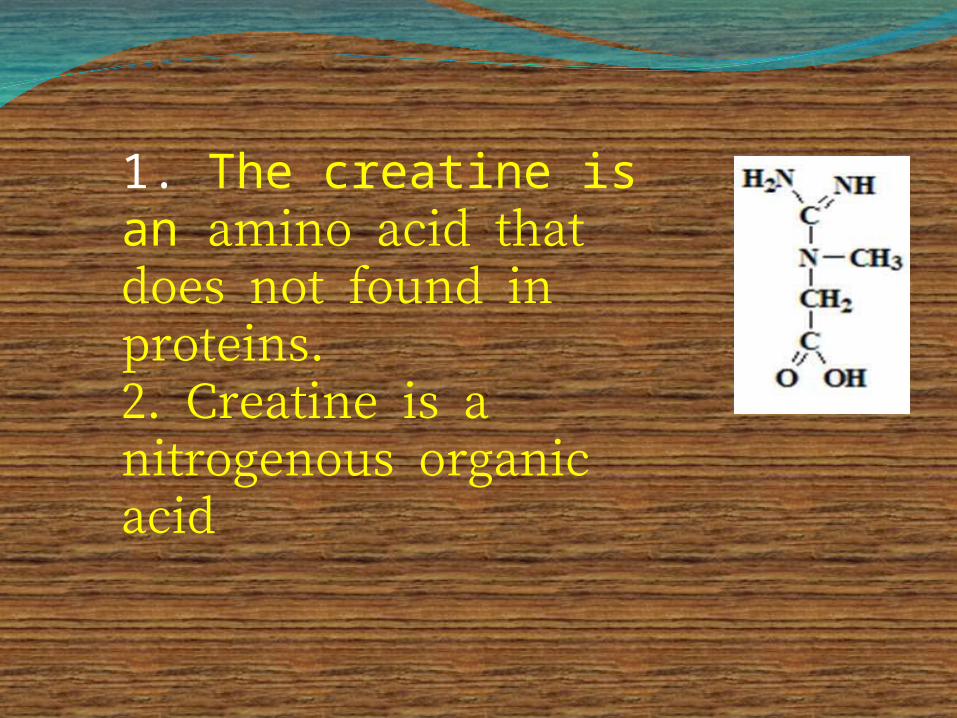
1. The creatine is an amino acid that does not found in proteins.2. Creatine is a nitrogenous organic acid
Creatine is a naturally occurring amino acid found in the body (primarily muscle tissue)
The daily requirement of creatine is about 2-3 grams/day
About half of the daily needs are obtained from the diet (primarily meat and fish)
The remaining daily need for creatine is synthesized from the amino acids glycine, arginine, and methionine primarily in the liver
Where is Creatine Found?
Distribution of body creatineFrom liver, transported to other tissues98% are present in skeletal and heart
musclesIn Muscle, gets converted to the high
energy source creatine phosphate (phosphocreatine)Creatine
Creatine phosphate
ATP
ADP + H+
ATP
ADP
Creatine Kinase
Three amino acids are required:GlycineArginineMethionine (as S-
adenosylmethionine)
Site of biosynthesis:Step 1: KidneysStep 2: Liver
Creatine Biosynthesis
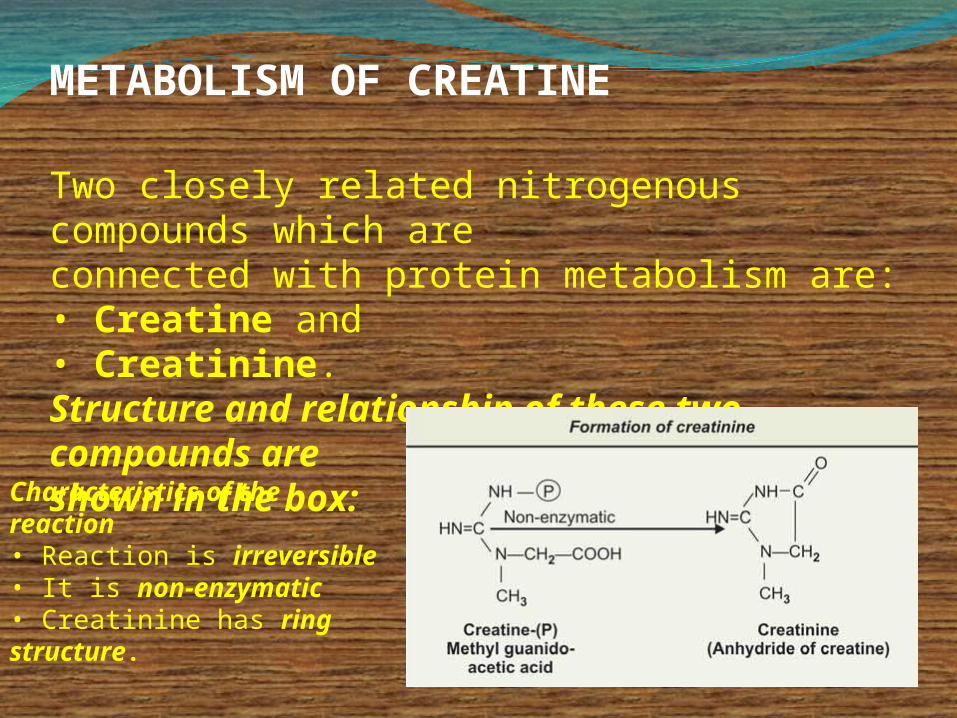
METABOLISM OF CREATINE
Two closely related nitrogenous compounds which areconnected with protein metabolism are:• Creatine and• Creatinine.Structure and relationship of these two compounds areshown in the box:
Characteristics of the reaction • Reaction is irreversible• It is non-enzymatic• Creatinine has ring structure.
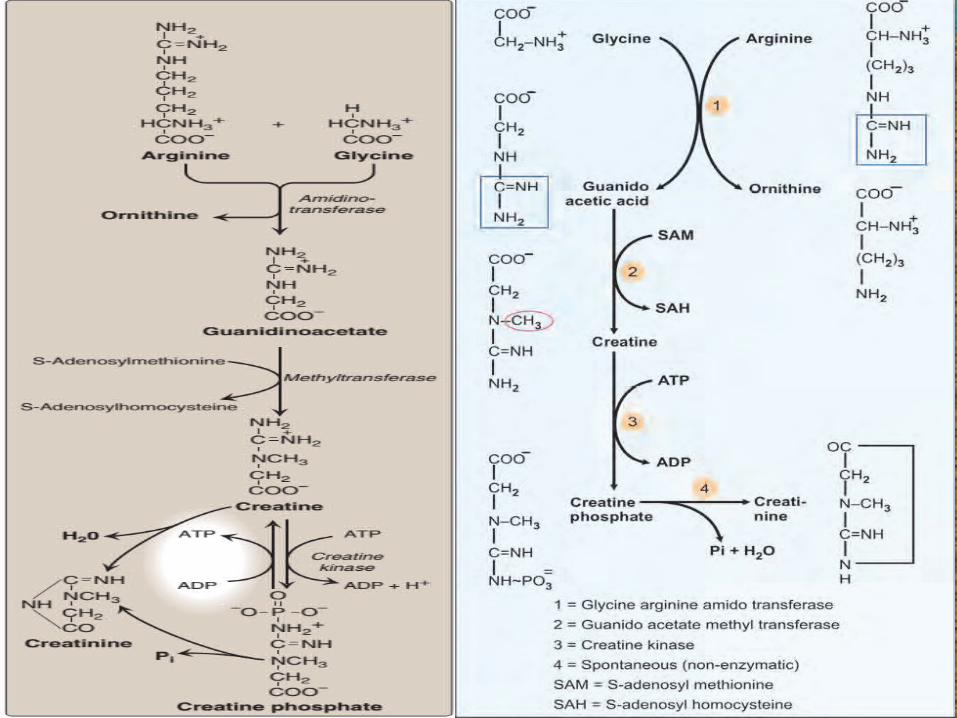
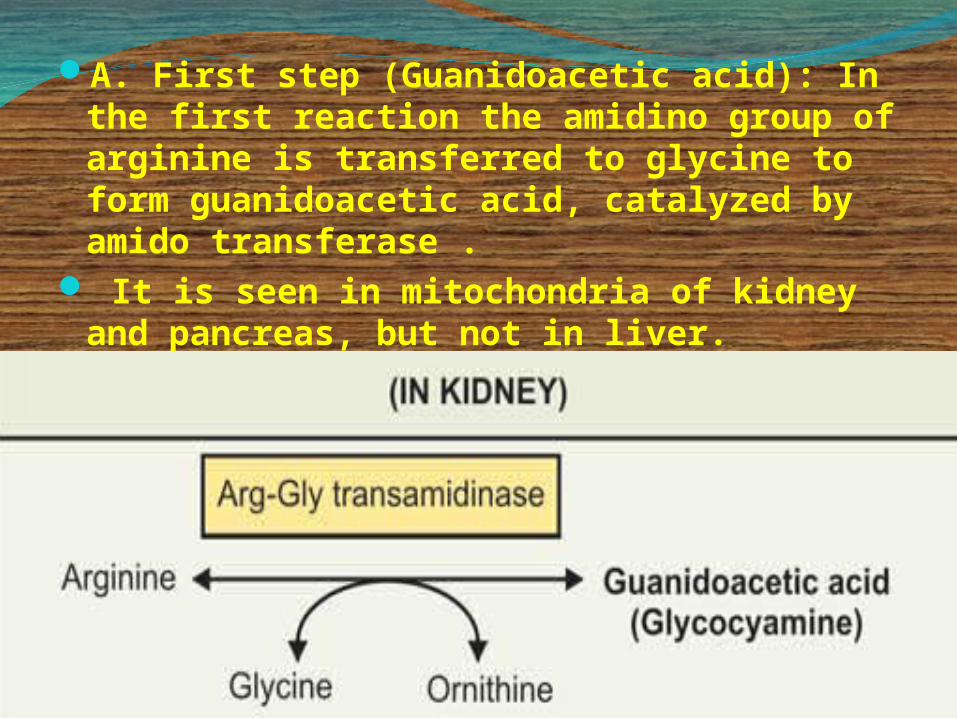
A. First step (Guanidoacetic acid): In the first reaction the amidino group of arginine is transferred to glycine to form guanidoacetic acid, catalyzed by amido transferase .
It is seen in mitochondria of kidney and pancreas, but not in liver.
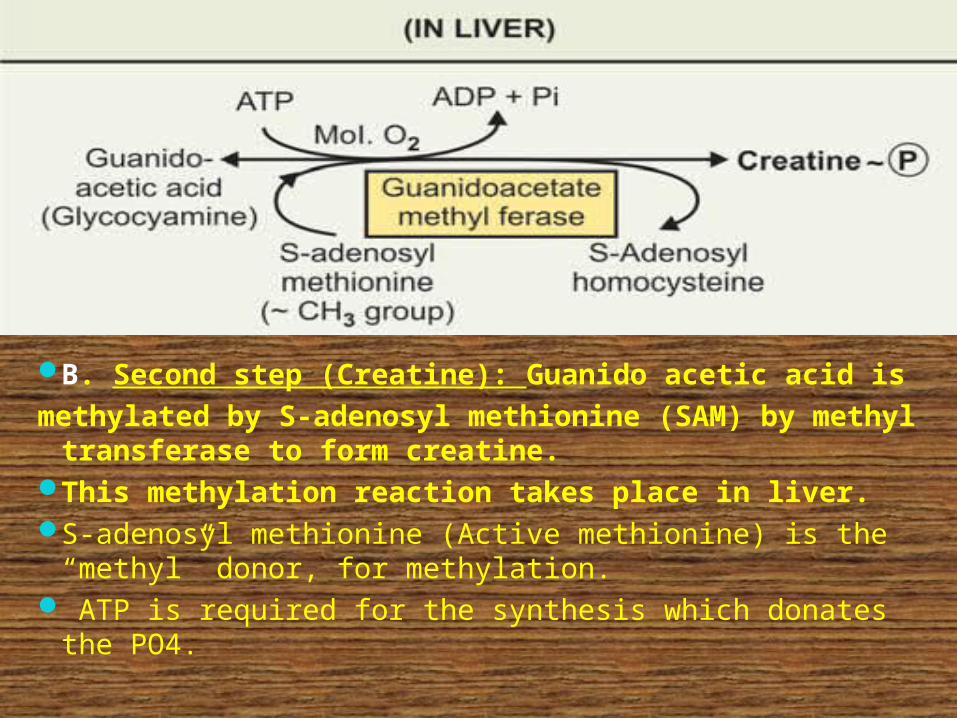
B. Second step (Creatine): Guanido acetic acid ismethylated by S-adenosyl methionine (SAM) by
methyl transferase to form creatine. This methylation reaction takes place in liver. S-adenosyl methionine (Active methionine) is the “methyl”
donor, for methylation. ATP is required for the synthesis which donates the PO4.
Also O2 is required for the reaction (aerobic). Reaction is irreversible, and also it occurs in liver.Once creatine-(P) is formed in liver, it goes to muscles,and stored. Creatinine is formed from creatine-(P) inmuscles by non-enzymatic and irreversible reaction.
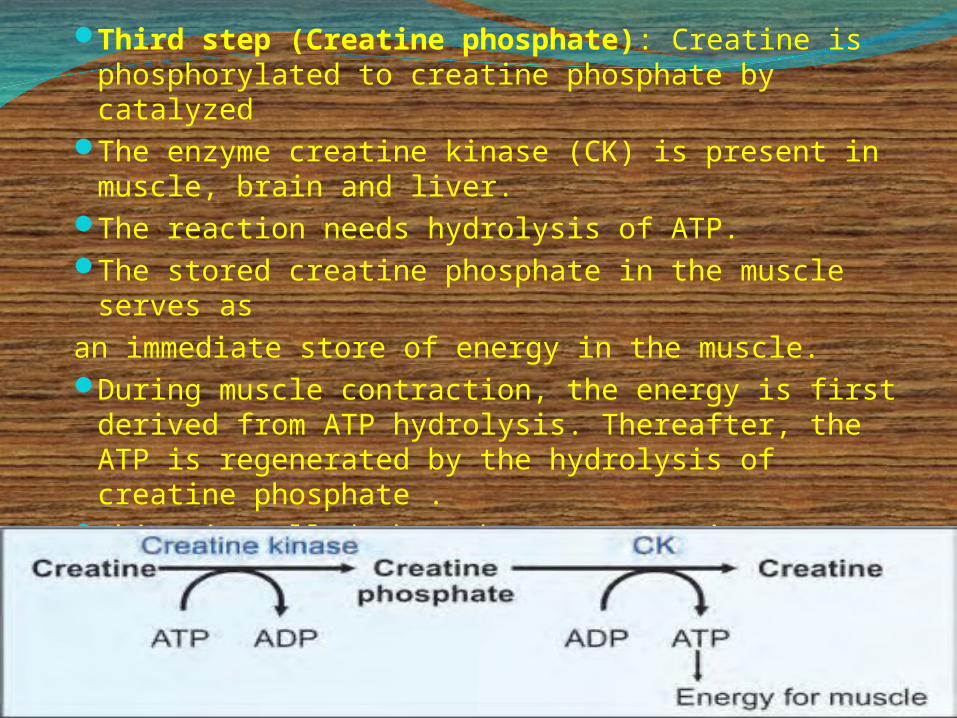
Third step (Creatine phosphate): Creatine is phosphorylated to creatine phosphate by catalyzed
The enzyme creatine kinase (CK) is present in muscle, brain and liver.
The reaction needs hydrolysis of ATP.The stored creatine phosphate in the muscle serves
asan immediate store of energy in the muscle. During muscle contraction, the energy is first
derived from ATP hydrolysis. Thereafter, the ATP is regenerated by the hydrolysis of creatine phosphate .
This is called the Lohmann’s reaction .
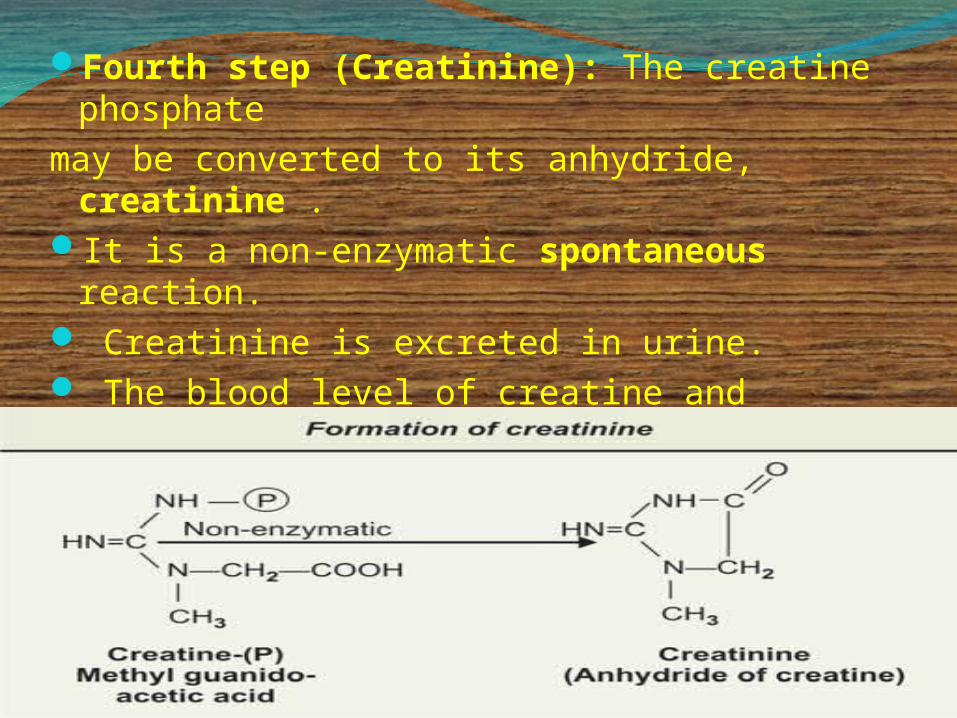
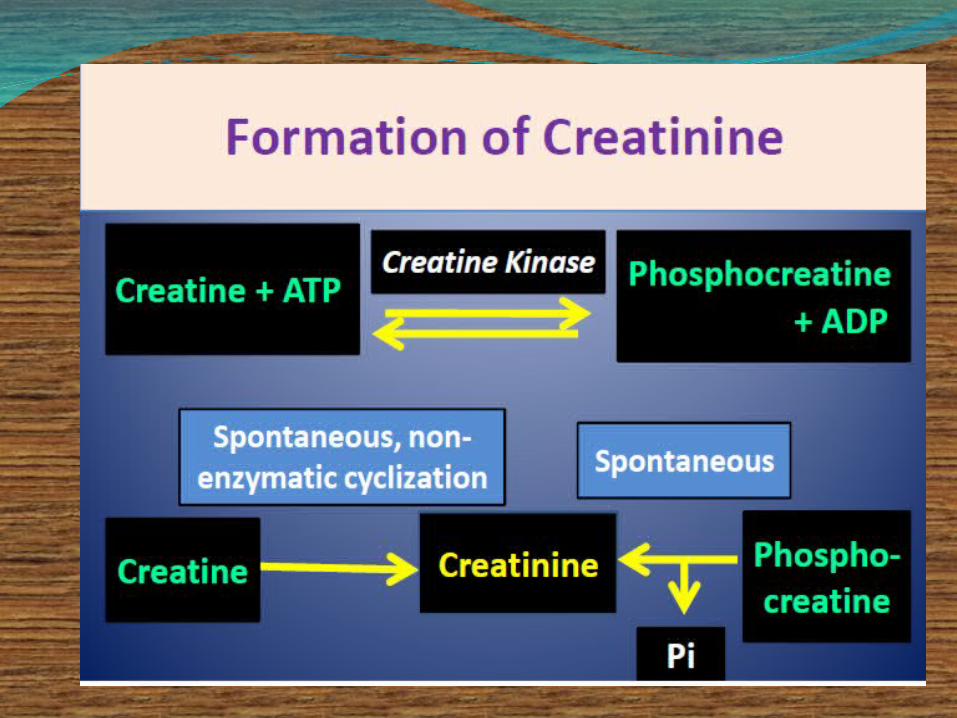
Fourth step (Creatinine): The creatine phosphate
may be converted to its anhydride, creatinine .
It is a non-enzymatic spontaneous reaction. Creatinine is excreted in urine. The blood level of creatine and creatinine,
and urinary excretion of creatinine are more or less constant, as long as the muscle mass is not affected.
Regulation of Creatine SynthesisDietary creatine has effect on creatine synthesis. Inrats, fed a complete diet containing 3 per cent creatine,transamidinase activity of the kidney was markedlylower as compared to control animals. But dietary creatine or a high blood creatine has noeffect on rate of synthesis of creatine in liver. It is also shown that hepatic synthesis of creatine isrelated to the blood glycocyamine levels and that thiscompound is produced in kidney, suggests that therate of creatine biosynthesis is actually dependenton kidney transamidinase activity
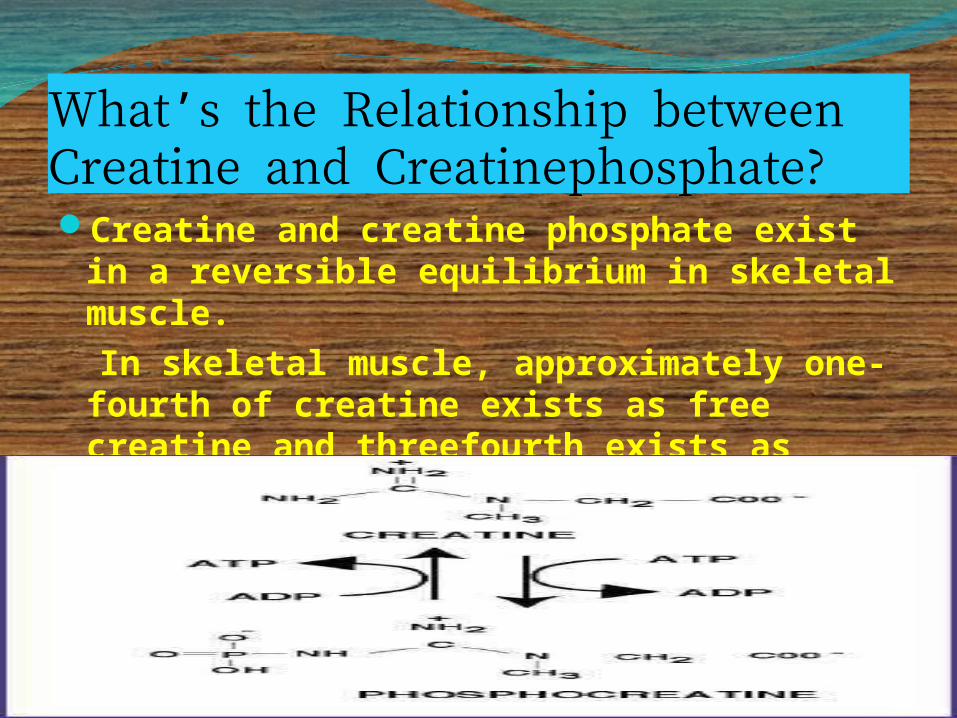
What’s the Relationship between Creatine and Creatinephosphate?Creatine and creatine phosphate exist in
a reversible equilibrium in skeletal muscle.
In skeletal muscle, approximately one-fourth of creatine exists as free creatine and threefourth exists as creatine phosphate.
Creatine PhosphateIs a high-energy phosphate compoundActs as a storage form of energy in the
muscleProvides a small but, ready source of
energy during first few minutes of intense muscular contraction
The amount of creatine phosphate in the body is proportional to the muscle mass
1. Creatine and creatine phosphate spontaneously form creatinine as an end product
2. Creatinine is excreted in the urine3. Serum creatinine is a sensitive indicator
of kidney disease (Kidney function test)4. Serum creatinine increases with the
impairment of kidney function
Creatine Degradation
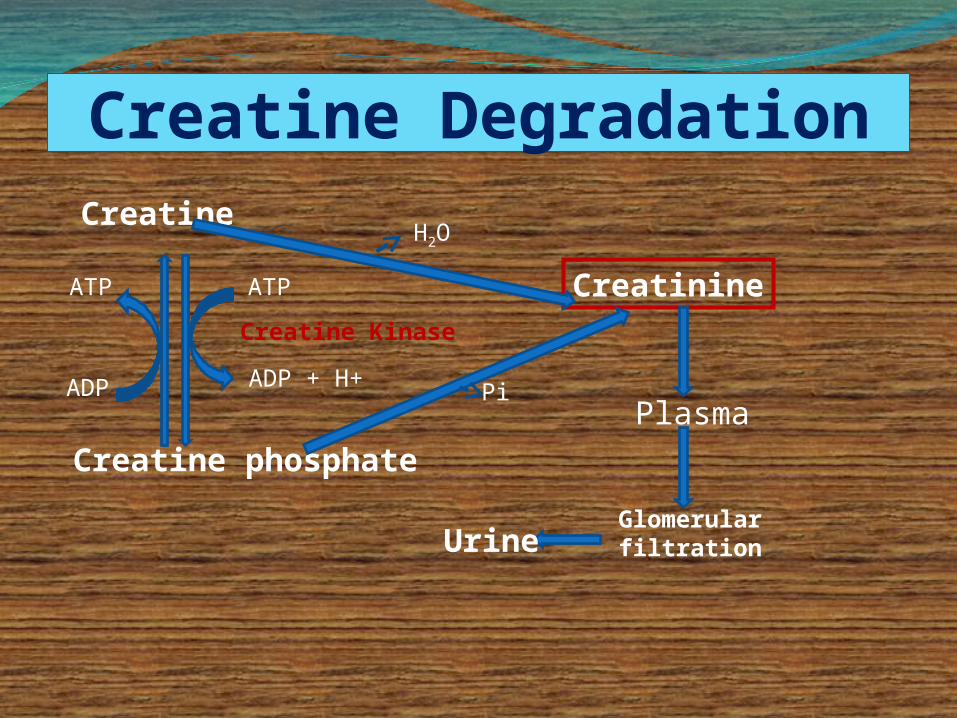
Creatine DegradationCreatine
Creatine phosphate
ATP
ADP + H+
ATP
ADP
Creatine Kinase
Creatinine
H2O
PiPlasma
Glomerular filtrationUrine
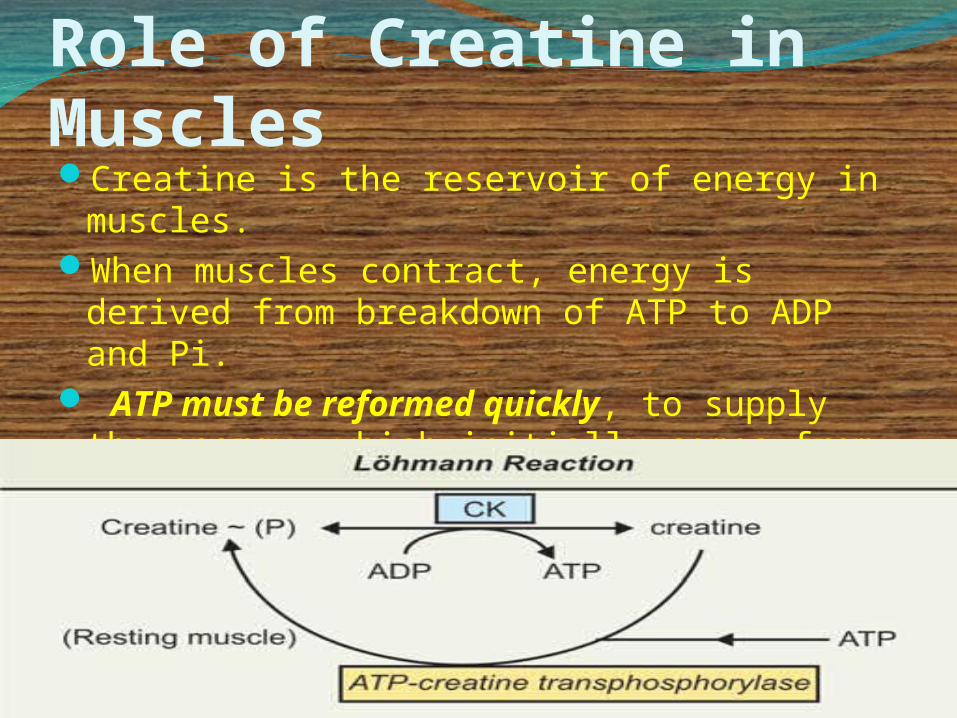
Role of Creatine in MusclesCreatine is the reservoir of energy in
muscles. When muscles contract, energy is derived
from breakdown of ATP to ADP and Pi. ATP must be reformed quickly, to supply
the energy, which initially comes from creatine ~ (P), subsequently from glycolysis (contracting muscle).
From the above reaction, ATP is formed from creatine~ (P).
The high energy phosphate is transferred to ADP and ATP is formed.
This reaction is called Löhmann reaction and it takes place during activity of the muscles.
In the resting condition, creatine ~ (P) is reformed, the
enzyme that catalyses the reaction is ATP-creatine transphosphorylase
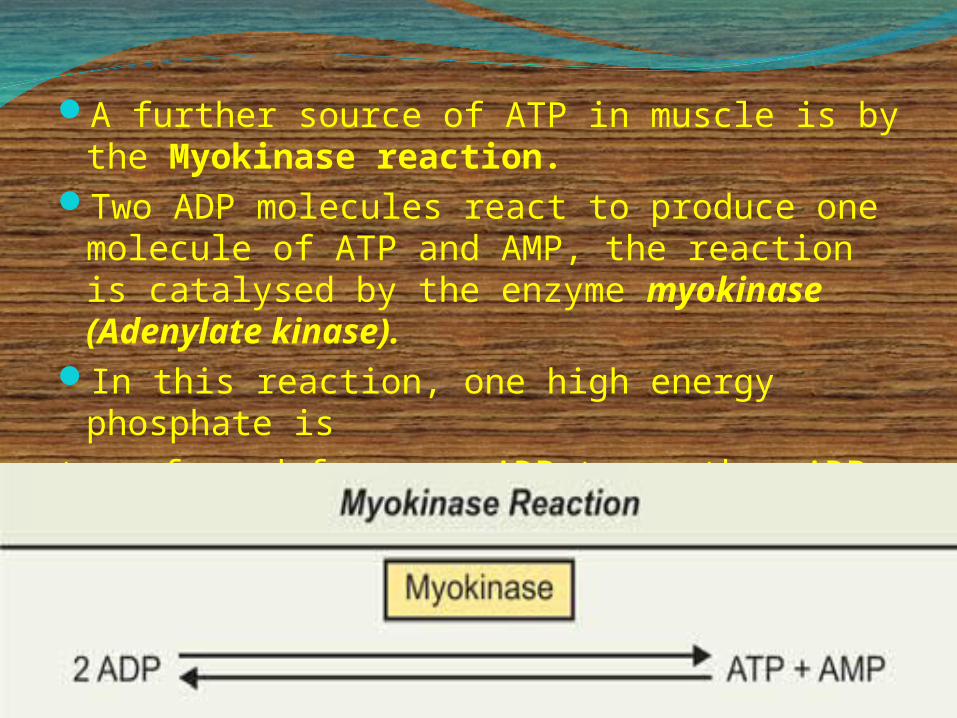
A further source of ATP in muscle is by the Myokinase reaction.
Two ADP molecules react to produce one molecule of ATP and AMP, the reaction is catalysed by the enzyme myokinase (Adenylate kinase).
In this reaction, one high energy phosphate istransferred from one ADP to another ADP
molecule to form one ATP.
Creatine: It is a normal constituent of the body. It is present in muscle, brain, liver, and in blood.Can occur in free form and also as phosphorylated form. The phosphorylated form is called as creatine-PO4 or
phosphocreatine or Phosphagen.Total amount in adult human body is approximately 120gm. 98 per cent of total amount is present in muscles, 80 per cent occurs in phosphorylated form, 1.3 per cent in nervous system (brain) and 0.5 to 0.7 per cent in tissues
Urinary excretion: Urinary excretion in normal health is in the form of creatinine and it is only 2 per cent of the total.
In males, it is 1.5 to 2.0 gm in 24 hrs urine, and in
females, varies from 0.8 to 1.5 gm. Only vertebrate muscles contain creatine. Creatine concentration is higher in striated muscle
as compared to smooth muscle and also in rapidlycontracting muscle as compared to pale muscles.Total is 300 to 500 mg/100 gm.
In invertebrates: Arginine replaces creatine in muscles.
Blood and plasma level In whole blood: Creatine level varies from
2 to 7 mg%. In plasma: It is less than 1 mg%.In male: It varies from 0.2 to 0.6 mg%.In females: 0.35 to 0.9 mg%.
Creatinine: Creatinine is the anhydride of creatine,
and it is in this form that creatine is excreted in
normal health. Removal of one molecule of H2O isnon-enzymatic and irreversible.Total creatinine in muscle is only 0.01 per
cent (10 mg).
Whole blood Muscles• Creatine 2.0 to 7.0 mg% 300 to 500 mg• Creatinine 1.0 to 2.0mg% 0.01% (10 mg)
Urinary excretion Creatinine males: 1.5 to 2.0 gm in 24 hr females: 0.8 to 1.5 gm in 24 hr
CreatinuriaExcretion of creatine in urine is called
Creatinuria. Creatine excretion occurs: In children: Reason probably lack of ability to
convertcreatine to creatinine. In adult females in pregnancy and maximum
after parturition (2 to 3 weeks).In febrile conditions•In thyrotoxicosis, probably due to
associated myopathies
In muscular dystrophies, myositis, myasthenia gravis. Lack of carbohydrate in diets and in diabetes mellitus. In wasting diseases, e.g. in malignancies. In starvation
Forms of Creatine SupplementsCreatine Monohydrate – Most CommonCreatine PhosphateCreatine CitrateCreatine blended w/CHO, Proteins, AA,
CaffeinePowdersTabletsGelLiquid
Documented Side EffectsPotential side effects are minorGastrointestinal (GI) distressNo renal or liver dysfunctionNo cramping in controlled studiesIncreased Body Mass (water retention in
muscle cell due to osmotic changes)Urinary Volume decrease during loading
Function of CreatineThe body only has limited stores of ATP &
ADPWhen a Cr supplement is ingested, & enters
the intestines, a majority of Cr is absorbed into the bloodstream.
Cr from bloodstream is taken up by skeletal and cardiac muscle through insulin-mediated active transport
After absorption, a portion of Cr combines with phosphate to form PCr
This storage of Cr and PCr allows rapid resynthesis of ATP to meet energy demands via the creatine kinase (CK) reaction
Theoretically, Cr supplementation will increase Cr and PCr stores, providing more PCr to be utilized in CK reactions
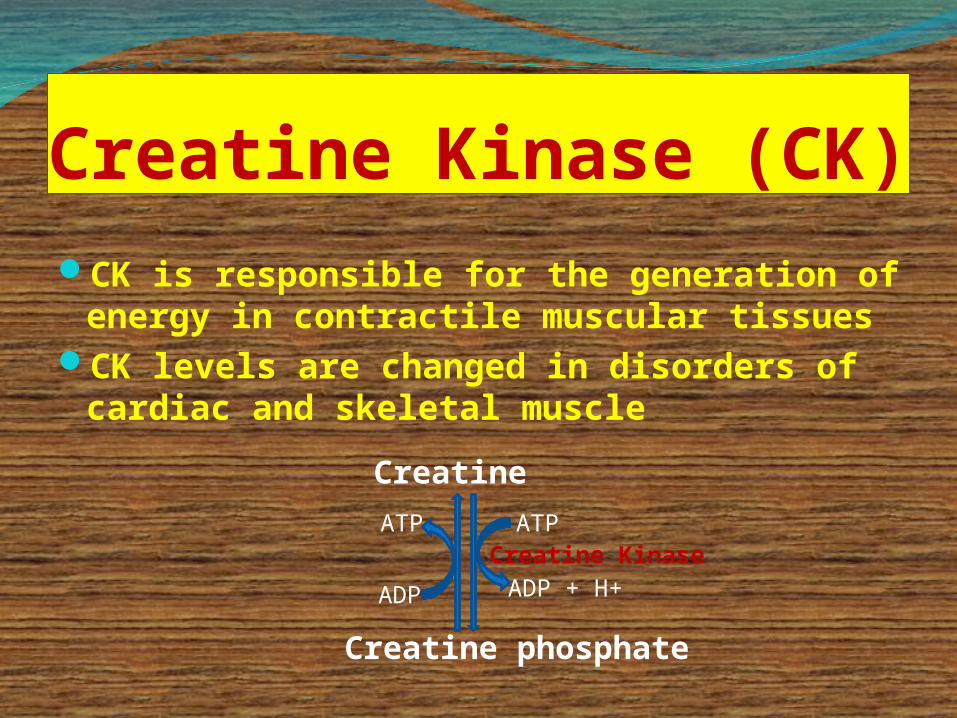
Creatine Kinase (CK)CK is responsible for the generation of
energy in contractile muscular tissuesCK levels are changed in disorders of
cardiac and skeletal muscleCreatine
Creatine phosphate
ATP
ADP + H+
ATP
ADP
Creatine Kinase
1. CK is required for conversion of creatine into creatine phosphate
2. CK has 3 isoenzymes:CK-MM mainly in skeletal muscleCK-MB mainly in heart muscleCK-BB mainly in brain
3. Serum total CK is increased in: Crush injuries (Damage of skeletal
muscles)Myocardial infarction (Damage of
heart muscle)
Creatine Kinase (CK)
What is the purpose of assaying for CK over a period of time?
Isozymes creatine kinase are tissue specific CK is a dimer of MM, MB, BB isozymes, and only MB is present in the myocardium (15% TOTAL CK)
MB-CK: myocardial specific injury- 100% increase in MB-CK within 4 hr- Peaks at 8-24 hr then decreases, with aminotranserase change much slower peak ~ 60 hrs , LDH is the best indicator to follow the MI from third day(To maximize treatment, prompt recognition essential)- Usually [CK] cardium & % MB/total CK are constant, [MB-CK] is proportional to degree injury to myo cardium
What is the relation of CK activity in the blood to tissue damage?
. Diagnostic Value: CK is present in all tissues but only SELECTIVE RELEASE (brain, muscle, but not liver) therefore different from liver damage caused by:Myocardial infarction muscle trauma, muscle dystrophy, severe exertion, IM injections, hypothyroidism, chronic alcoholism (with myopathy
IS Creatine as an Antioxidant?The mitochondrial isoform of creatine kinasedecreases superoxide production by limiting themagnitude of the mitochondrial membrane potential.Meyer et al. J Biol Chem 281: 37361-71, 2006
This is also evident in livers from transgenic mice in
which the mitochondrial creatine kinase has beenintroduced. Hatano et al. Hepatology 24: 663-9,
1996.
ConclusionsDietary creatine is found in muscle meats and
dairy products; however de novo synthesis is responsible for the provision of the greater part of our creatine.
The importance of creatine synthesis has recently been underscored by the discovery of the creatine deficiency syndromes.
Creatine synthesis makes quite large metabolic demands on amino acid metabolism, particularly
that of glycine, arginine and methionine
ReferencesText book of biochemistry – M N Chatterjia
8th editnText book of biochemistry - LehningerText book of biochemistry - D M Vasudevan
8th editnText book of biochemistry- A R Aroora 2nd
edition Text book of biochemistry – Pankaja Naik 4th
edition

What is the Fate of Creatinine that was Produced from Break Down of Creatine Phosphate during Anaerobic Exercise..?CREATININE EXCRETION The creatinine is a waste product of creatine
phosphate and it will be excreted by the kidney in the urine at a rate of 1 to 2 g/day.
When creatinine is ingested, most of it is rapidly eliminated in urine.
It can be quantitatively recovered. But when creatine is taken, some is retained in the body. It has been seen by giving labelled creatine that 20 to 30 per cent is excreted as creatinine and some is retained in the body whose fate is not known.
Urine of normal healthy adult male contains creatinine but no creatine.
Amount of creatinine excreted as discussed above is approximately 1.0 to 1.5 gm/day and this is:
Independant of amount of proteins taken in the diet.Excretion is greater in muscular persons and appears
to be related to muscular development and muscular activity. After severe exercise, it may increase,
but total amount remains constant from day-to-day.
Estimation of CreatinineJaffe’s reaction: Serum is treated with alkaline picratesolution when a red colour develops (Jaffe’s reaction).The colour is read against a ‘standard’ similarly treatedin a colorimeter.Estimation of CreatineWhen heated with acid solution, creatine is converted to
creatinine, which can be measured in a similar way as stated above.
Value after boiling with acid solution –value beforeboiling = creatine content.1.0 gm of creatinine is formed from 1.16 gm of creatine.Hence, substract the pre-formed creatinine from the totalcreatinine × multiply by 1.16.
“True” CreatinineSerum creatinine estimation by Jaffe’s reaction
does not give “true” creatinine. It measures also certain noncreatinine chromogens, upto 20 per cent in blood and up to 5 per cent in urine.
For excluding the chromogens and to get ‘true’ creatinine, after precipitating the proteins,creatinine is adsorbed on to Lloyd’s reagent (Fuller’s earth), a hydrated aluminium silicate, and then colour developed with alkaline picrate.
Urinary CreatinineA typical male excretes about 15 mmol of
creatinine per dayA decrease in muscle mass due to
muscular dystrophy or paralysis leads to decreased level of creatinine in urine
The amount of creatinine in urine is used as an indicator for the proper collection of 24 hours urine sample
Creatinine Co-efficientIt is the ratio of mg of creatinine in urine in
24hours Body wt. in kgThe value is 20 to 26 for males 14 to 22 in females.
Significance It depends on muscular development and remains
fairly constant. As the rate is so constant in a given individual thecreatinine co-efficient may serve as a reliable index
ofthe adequacy of a 24-hr urine collection.
Creatinine Clearance
Endogenous creatinine clearance is used as renal function test. At normal levels of creatinine in the blood, this metabolite is filtered at the glomerulus but neither secreted nor re-absorbed by the tubules. Hence its clearance measures the glomerular filtrate rate (GFR)
(Refer Chapter on Renal Function Tests)
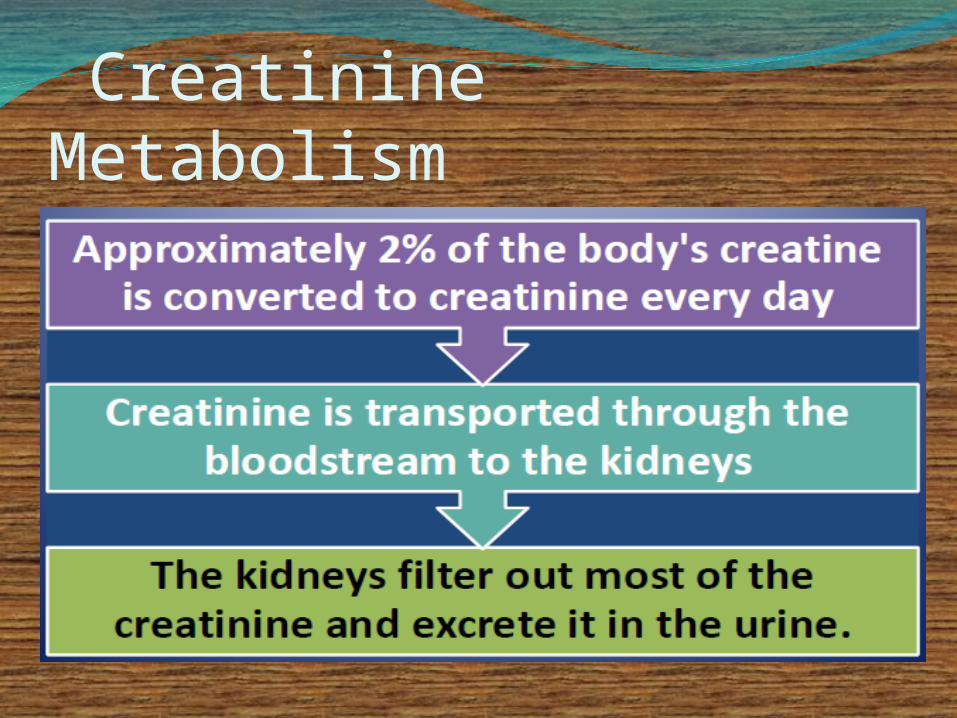
Creatinine Metabolism
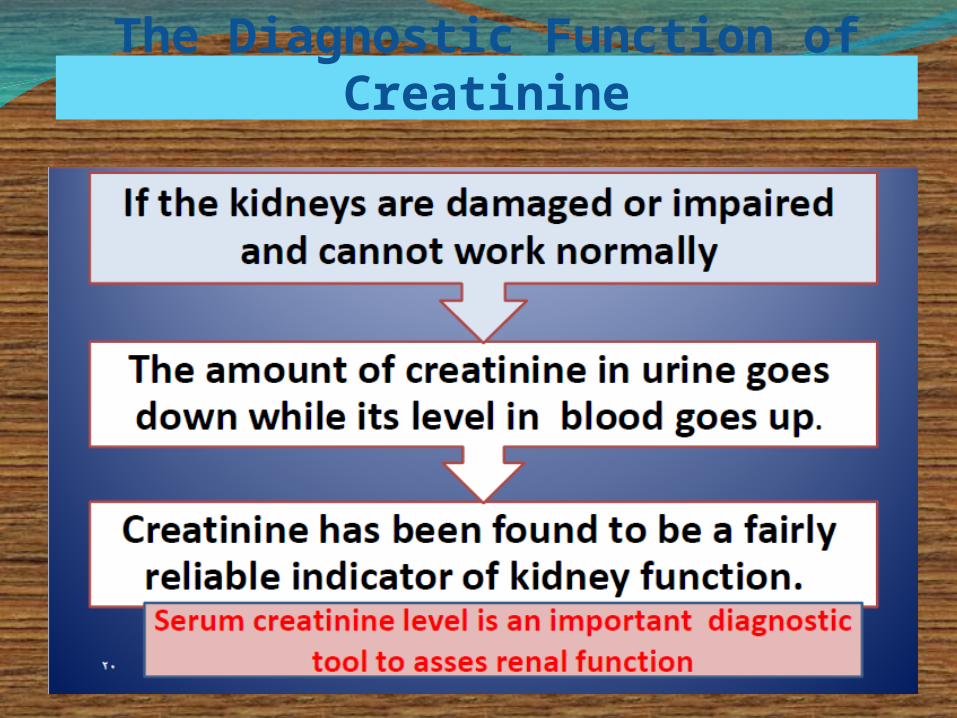
The Diagnostic Function of Creatinine
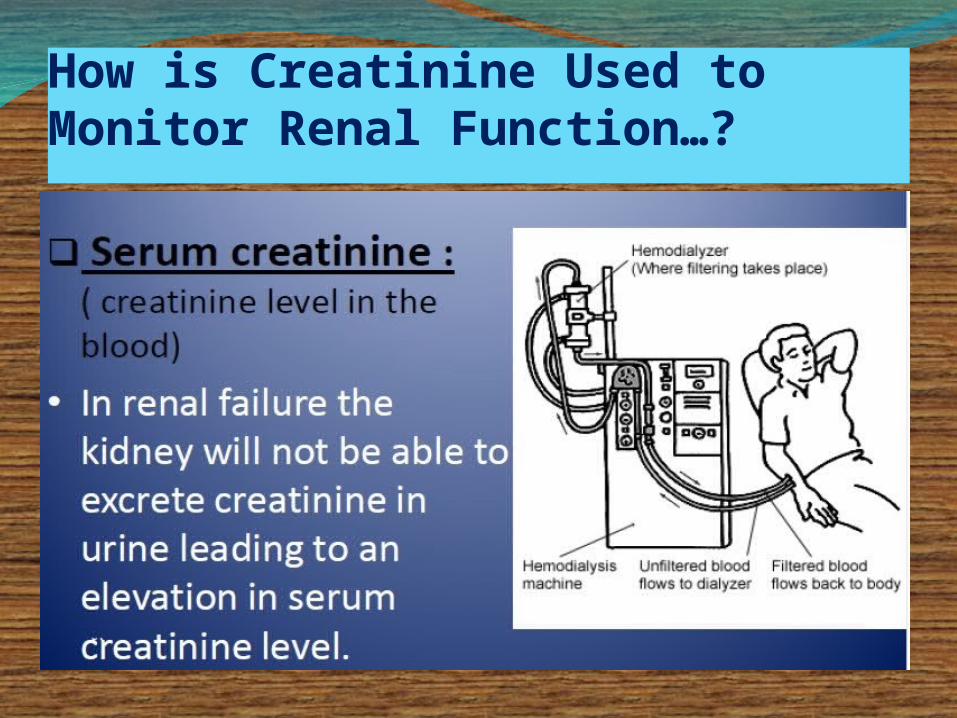
How is Creatinine Used to Monitor Renal Function…?
Levels of Creatinine in the Blood Depends Mainly on Renal Function….but…Is there other factors may affect creatinine level in the blood…?
Serum Creatinine may be Affected Partly by….
The amount of muscle tissue you have. Men tend to have higher levels of blood creatinine because they have more skeletal muscle tissues than women.
Protein in diet . Vegetarians have been shown to have lower creatinine levels in blood.
CLINICAL SIGNIFICANCE OF CREATININEThe amount of creatinine excreted from The amount of creatinine excreted from
the body is proportional to the total the body is proportional to the total creatine phosphate content of the body, creatine phosphate content of the body, and thus and thus can be used to estimate muscle can be used to estimate muscle mass.mass.
Serum creatinine is a sensitive indicator Serum creatinine is a sensitive indicator of kidney disease (Renal function test)of kidney disease (Renal function test)
Serum creatinine increases with the Serum creatinine increases with the impairment of kidney functionimpairment of kidney function
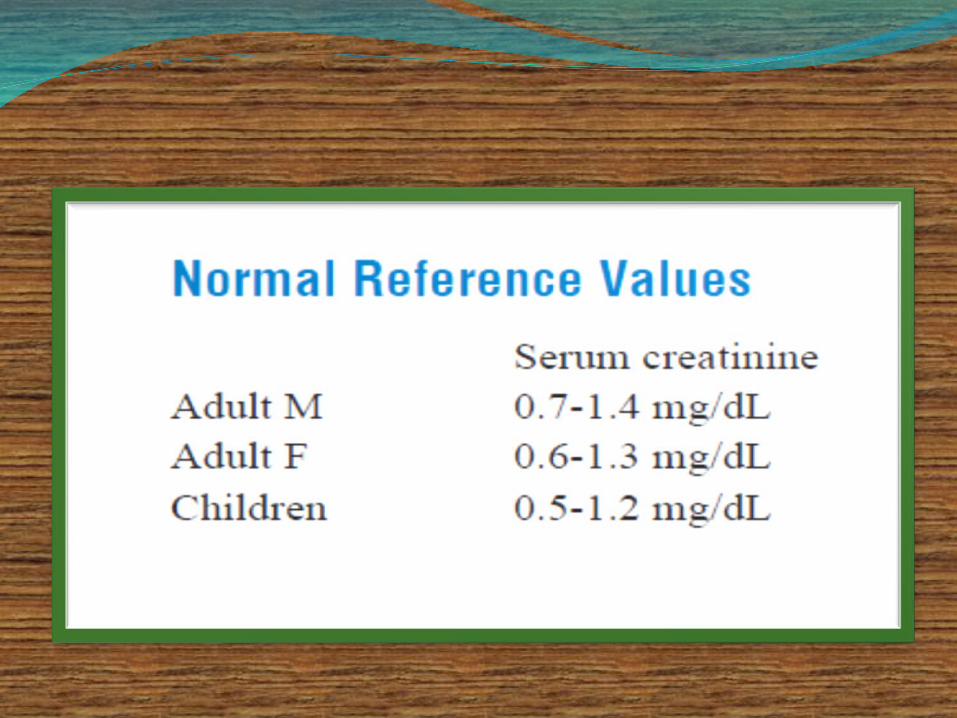
Factors reducing serum creatinine:Low muscle mass Malnutrition Factors increasing serum creatinine :Old age Renal diseases Glomerulonephritis Pyelonephritis Renal failure Urinary obstruction Congestive cardiac failure
URINE CREATININEThe normal daily excretion of creatinine
ranges from 1-2 gm. A decrease in muscle mass due to
muscular dystrophy or paralysis leads to decreased level of creatinine in urine
Creatinine clearance test is widely used as a measure of the glomerular filtration rate and is decreased in renal failure
Let’s all sing from the same hymn bookCreatine….cellular molecule, obtained in the
diet orproduced endogenously. Creatine-phosphate (phosphocreatine)
”High energy”cellular molecule. Creatine Kinase…an enzyme that reversibly
phosphorylates creatine to creatine phosphate. Creatinine…formed as a result of the
spontaneous breakdown of creatine and creatine-phosphate. Excreted in the urine. Urinary excretion of creatinine often used to normalize the excretion of other substances. Plasma levels related to renal function

Recommended