Session 11BREAST AND NIPPLE CONDITIONS
Session Objectives:
1. List the points to look for when examining a mother’s breasts and nipples.
2. Describe causes, prevention and management of engorgement and mastitis.
3. Describe causes, prevention and management of sore nipples.
4. Demonstrate through role-play assisting a mother with breast or nipple conditions.
Flat & Inverted Nipples
Mothers can breastfeed with flat and inverted nipples.
Nipple exercises and breast shells have not been shown to be effective in correcting nipples during pregnancy. During the third trimester, nipple exercises may stimulate contractions and are therefore discouraged.
Strategies for Inverted Nipples
Pumping on low setting with soft flange kit will evert many nipples.
Check to be sure any devices sold specifically to evert nipples have evidence-based safety and efficacy studies to include with your protocol.
Frequent post-discharge weight checks are strongly recommended.
Nipple shields reduce milk supply and are rarely indicated for any nipple problems.
Sore and Cracked Nipples
Correct positioning and latch-on is critical to nipple comfort.
Nipple sucking is associated with sore, cracked nipples. This is an example of incorrect latch-on.
An infant with a tight labial or lingual frenulum may cause nipple pain or soreness.
Nipple irritants may include creams and ointments, plastic-backed breast pads, nipple shields, etc.
Stabbing pain in nipple and breast may be due to a bacterial or other infection, and may be multifactoral.
Strategies for Nipple PainFirst, identify and correct the cause(s) of sore
and cracked nipplesIndividual assessment leads to an appropriate
treatment plan, which includes correcting latch-on and Changing the latch or nursing positionhealing plannursing on the unaffected breast first
Consider pain relief medications if necessary (aspirin or acetaminophen). Use short-acting preparations taken just before nursing.
Nipple Ointments
Creams or ointments that should NOT be used include any preparation that the manufacture states is not for ingestion these usually include:any substance that must be removed before feedingsVitamin ETopical antibiotic creamAstringentsSteroidspreparations containing bismuth subnitrate,
petrolatum or benzalkonium chloride
Engorgement
Fullness in the breasts in the early postpartum period is due to increased vascularity as well as increased milk production.
Drainage is important for optimal milk production.
Frequent breastfeeding is the most effective way to assure drainage.
Engorgement, cont.
If mother and baby are separated for medical reasons, hand express or pump to promote drainage.
Comfort measures such as warm or cold packs should be determined in consultation with the mother. There is no research to support superiority of either warm or cold applications.
Engorgement has been associated with nipple discomfort.
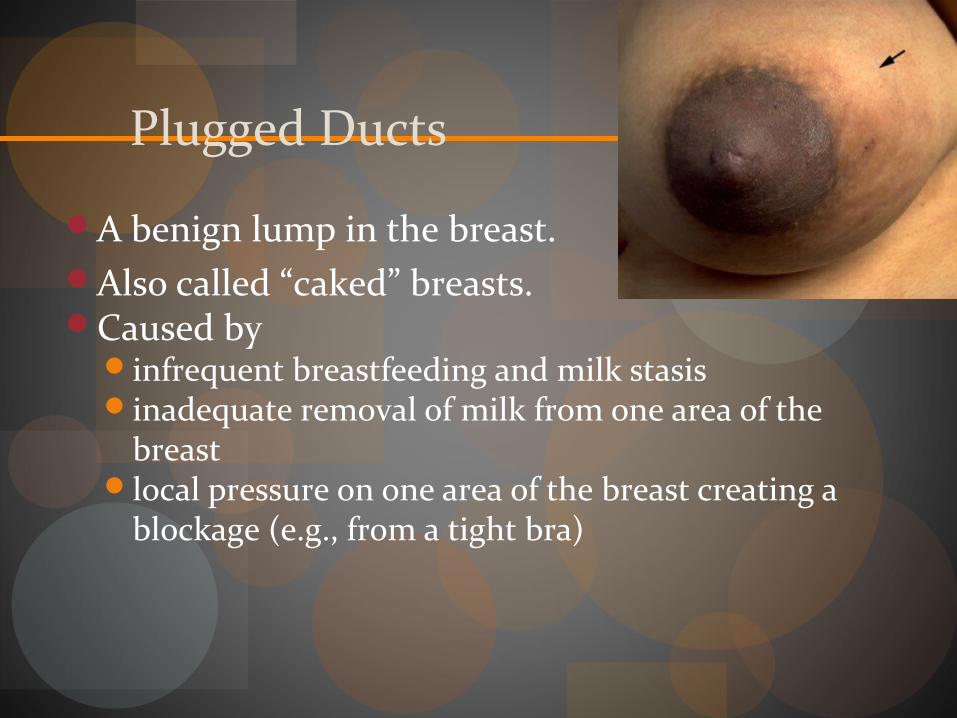
Plugged Ducts
A benign lump in the breast. Also called “caked” breasts.Caused by
infrequent breastfeeding and milk stasisinadequate removal of milk from one area of the
breastlocal pressure on one area of the breast creating a
blockage (e.g., from a tight bra)
Managing Plugged Ducts
Continue nursing. Feed frequently on affected side.Gently massage affected area, trying to move lump
toward nipple to assure drainage. This can be done before and during feedings.
Try warm moist compresses as a comfort measureTry nursing infant in different positions to ensure
drainage of affected area.Is clothing restricting milk flow?
Mastitis
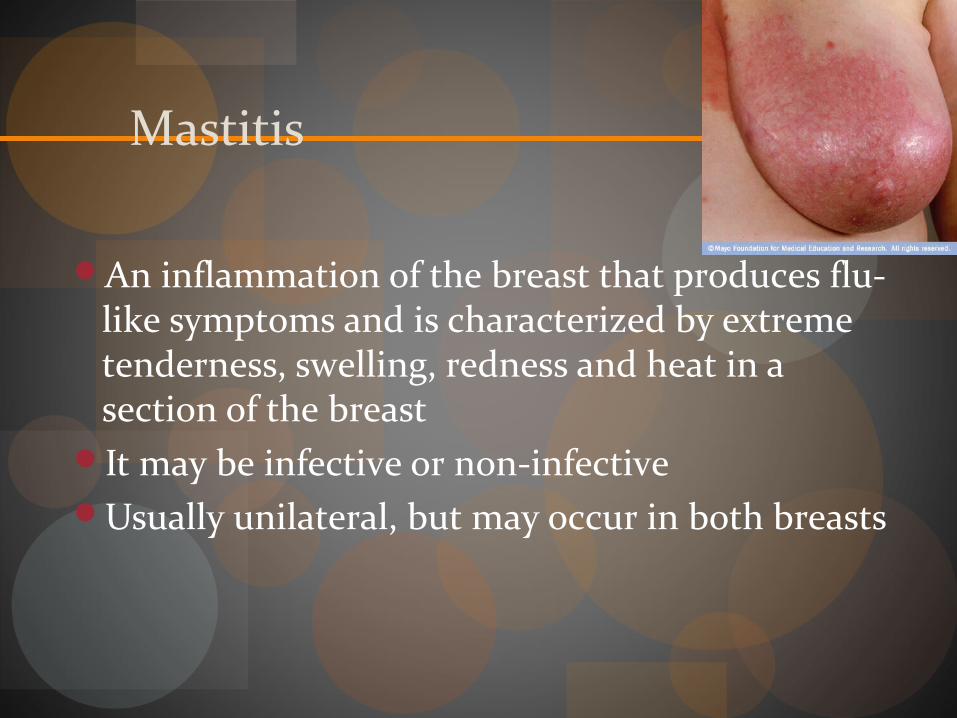
An inflammation of the breast that produces flu-like symptoms and is characterized by extreme tenderness, swelling, redness and heat in a section of the breast
It may be infective or non-infectiveUsually unilateral, but may occur in both breasts
Mastitis II
May be caused by bacterial infiltration through cracked or fissured nipple. Usually Staphylococcus aureus or Escherichia coli; occasionally Streptococcus.
Untreated plugged ducts or unresolved engorgement may lead to milk stasis and inflammation or infection.
Contributors to Mastitis
Contributing factors include:lowered resistance to infection (stress, exhaustion,
anemia)insufficient drainage of the area or obstruction of
ducts missed feedingssudden changes to feeding schedule (e.g., infant
begins to sleep through the night)
Management of Mastitis
Antibiotic treatment is usually prescribed in the United States
Treat with an antibiotic that is appropriate to the causal organism, and which is tolerated well by the infant
Management of Mastitis II
Antibiotics, if prescribed, should continue for at least 10-14 days. Tell mother to complete entire course of medication.
Continue to breastfeed on both sides, starting infant on unaffected side. Additional expression or feeding may be necessary to adequately drain the affected breast.
Management of Mastitis III
Mother should consider bed rest, keeping the baby in close proximity to assure frequent nursing.
Apply ice packs or warm packs to the breast, depending on mother’s comfort.
Drink plenty of fluidsConsider a mild analgesic especially one with
anti-inflammatory propertiesAssure that the bra or other clothing does not
restrict flow or apply painful pressure
Preventing Mastitis
Practice early, frequent feedingAvoid supplementationAlternate feeding positions for optimal drainageIdentify and treat sore nipples and plugged ducts
proactively
Mastitis for Woman is HIV-positiveIf a woman is HIV-positive, mastitis or nipple
fissure may increase the risk of HIV transmissionIf an HIV-positive woman develops mastitis, an
abscess or a nipple fissure, she should avoid breastfeeding from the affected breast while the condition persists. She must express milk from the affected breast, by hand or pump, to ensure adequate removal of milk.
If only one breast is affected, the infant can feed from the unaffected side, feeding more often and for longer to increase milk production.
Breast AbscessA deep-seated localized infection Mother feels illCauses include inadequate or delayed
treatment of mastitisManagement:
Drainage is usually required. Older techniques such as surgical lancing and drain insertion are being replaced by ultrasound visualization and needle drainage.
Bacterial cultures of purulent matter help the prescriber to select appropriate antibiotic.

Management of Abscess
Nurse or express breast every few hours If location of surgery/drain would not interfere
with infant attachment to the breast, baby may continue to breastfeed on the infected side.
Management of Abscess II
Milk will remain clean unless the abscess ruptures into the ductal system. Abscesses usually rupture to the outside.
If the location of the surgery/drain is incompatible with breastfeeding, mother should hand express or pump to promote drainage.
Candida Infections
Candida albicans is a fungal organism that may affect the surface of the nipple and areola. Candida has not been found to penetrate the breast.
The appearance of shiny or flaky on the nipple/areola was predictive of Candidiasis when combined with burning pain (Francis-Morrill, 2004).
Candida Infections II
Predisposing factors:lowered immune responsebacterial and viral infection, anemia, diabetestrauma to nippledamp breast pads, damp bras or occlusive clothingprevious use of antibioticspoor hygiene (especially of hand washing)repeated exposure through intimate contact with
infected family members
Management of Candida Infection
Both mother and baby need to be treated simultaneously. Other members of family should be treated in recurrent infections.
Infant Rx: nystatin mouthwash for 14 daysMother Rx:
vaginal infection: miconazole for 10-14 daysnipple infection: mycolog for 14 days or nystatin
cream after every feedingRecalcitrant cases: ketoconazole, fluconazole
Recommended