BONE DISEASE FOR R2
By .. Rungnapa Laortanakul

Bone
Mineral Metabolism
•Hypercalcemia
•Hypocalcemia
•Vitamin D deficiency
Basic Bone Biology
•Osteoporosis
•Osteomalacia

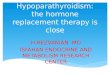
Vitamin D synthesis and metabolism
Skin Major source
UVB
circulation
Previtamin D3 �
vitaminD3 via
thermal
isomerization

Parathyroid hormone
Vitamin D

PTH action
• Hypocalcimia �stimulate PTH secretion
• Bone� bone resorption � Ca,PO4
• Kidney � Ca resorption
PO4 excretion
Calcitriol
• Net effect is Ca PO4
Calcitriol
1,25-dihydroxyvitamin D
• Small intestine � resorption of Ca,PO4
• Bone � bone resorption
• Kidney � excretion of Ca,PO4
• Net effect is Ca PO4

• Clinical depend on time onset and level
• Normal level is 8.5-10.5 mg/dl
• Calcium level 10.5-12 mg/dl asymptomatic
• Calcium level >12 usually symptomatic
Hypercalcemia

Clinical presentation
• Renal
• Nephrolithiasis/ Nephrocalcinosis
• Nephrogenic DI
• Polydipsia/ Polyuria
• Distal RTA
• Renal insufficiency
• Chronic hypercalcemic nephropathy
�nephrocalcinosis

• GI
Constipation, Anorexia, Abdominal pain, Pancreatitis, Increase gastrin secretion � PU
• CNS
Anxiety, Depression, Cognitive dysfunction, Confuse, Psychosis, Coma
• CVS
Calcify valve, HT, Shortened QT interval
• Skeleton
Gout, Pseudogout, Chondrocalcinosis, Osteoporosis, Osteopenia, Osteitis fibrosa cystica

Causes of hypercalcemia
Parathyroid-dependent hypercalcemia
• 1°hyperparathyroidism
• 3°hyperparathyroidism
• Familial hypocalciuric hypercalcemia
• Lithium-associated
• Antagonist autoantibodies to the calcium-sensing receptor
Williams texbook 11th ed.

Parathyroid-independent hypercalcemia
• Neoplasm-PTHrP dependent
-Other humoral syndromes-Local osteolytic dz(including metastasis)
• PTHrP excess
(non-neoplasia)• Excess vit D action
-Ingestion of excess vit D or
vit D analogues-Topical vit D analogues-Granulomatous dz-Williams’ syndrome
• Thyrotoxicosis• Adrenal insufficiency
• Renal failure
-ARF
-CRF with aplastic bone dz
• Immobilization
• Jansen’s dz• Drugs :
vit A intoxication
milk-alkali syndromethiazide diuretics theophylline
Williams texbook 11th ed.

Hyper Ca
Clinical evaluation
Hx,PE,
e’lyte,BUN,Cr,PO4,ALP
S.PTH
PTH dependent PTH independent
Hemoconcentration orSerum protein abnormality
Ionized Ca
S&S malignancy
Search for occult malignancyChest radiographSerum/urine IEP
MammogramAbdominal/chest CT
Evaluate forOther causes of
PTH-independent
Select appropriate tx,
consider bisphosphonate
High
Normal
Normal
or highLow

PTH dependent
24-hr urine calcium & Cr
Uca < 100 mg/day
or Clca/Clcr < 0.01YES NO
PTH
normal
PTH
high 1°hyperparathyroidismLi
therapy
Stop Li
Ca
High
Ca
normal
Li induce hyperPTH
BMD
Review criteria
For surgery
Age<40
or Family hx
YES NO
Presumptive FHH;Consider family screening

Work up• Ca, PO4 level
• Film find evidence of bone abnormality
• Find the solid organ tumor eg. CXR
• Alkaline phosphatase � bone lysis
• Hyperchloric metabolic acidosis suggest hyperPTH
• TFT � hyperthyroidism
• Cortisol � adrenal insufficiency
• Intact PTH level �hyperparathyroidism
• PTH-rP, vit D
• Urine calcium

Primary hyperparathyroidism
Present in one of four ways:
1. Asymptomatic hypercalcemia detected by
routine biochemical screening
2. Symptomatic hypercalcemia
3. During evaluation for manifestations of
hyperparathyroidism such as osteopenia,
osteoporosis, or nephrolithiasis
4. Rarely, hyperparathyroid bone disease (osteitis
fibrosa cystica) or parathyroid crisis

Primary hyperparathyroidism
• Adenoma
• Carcinoma
• Glandular hyperplasia
• MEN 1
• MEN 2A
• Familial hyperparathyroidism

Multiple endocrine neoplasiaType 1
Primary hyperparathyroidism
(>90 percent)
Pituitary tumors (10 to 20 percent)
• Prolactinoma
• Growth hormone-secreting
• Corticotropin-secreting
• Non-hormone-secreting
Enteropancreatic tumors
(60 to 70 percent)
• Gastrinoma
(Zollinger-Ellison syndrome)
• Insulinoma
• Vasoactive-intestinal polypeptide-secreting
• Glucagonoma
• Pancreatic polypeptide-secreting
• Non-hormone-secreting
Other
Type 2A
• Medullary thyroid cancer
(>90 percent)
• Pheochromocytoma
(40 to 50 percent)
• Parathyroid hyperplasia
(10 to 20 percent)
• Cutaneous lichen amyloidosis
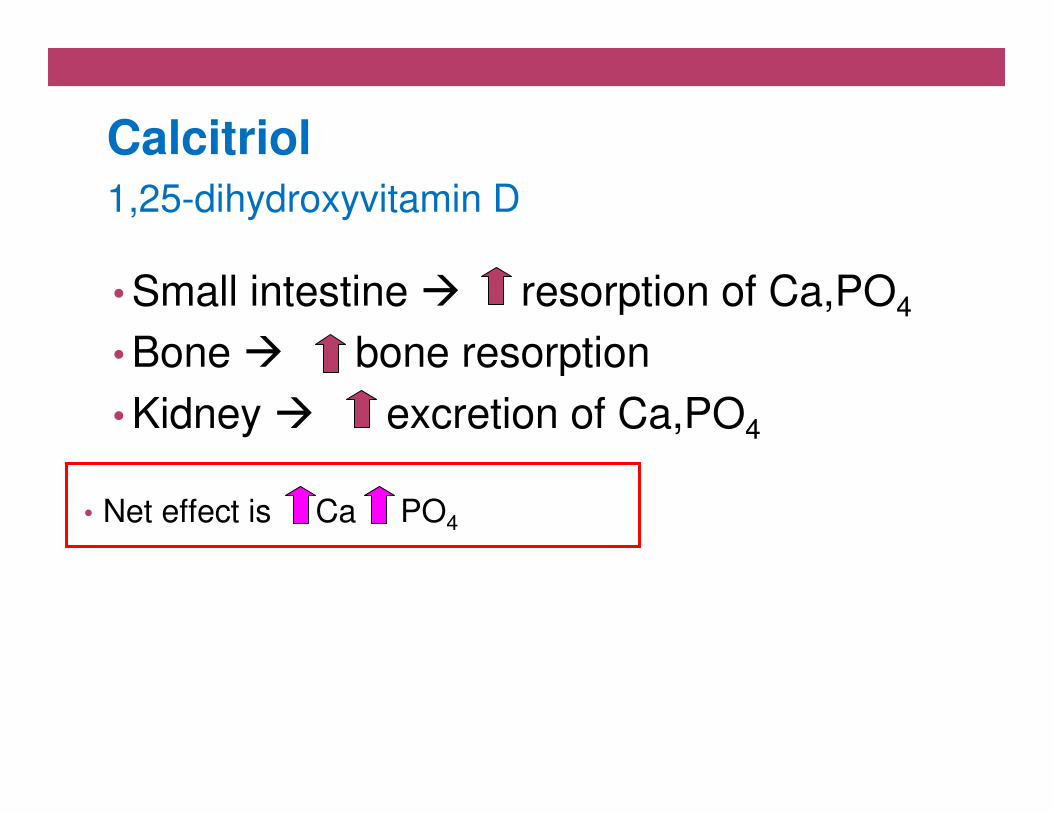
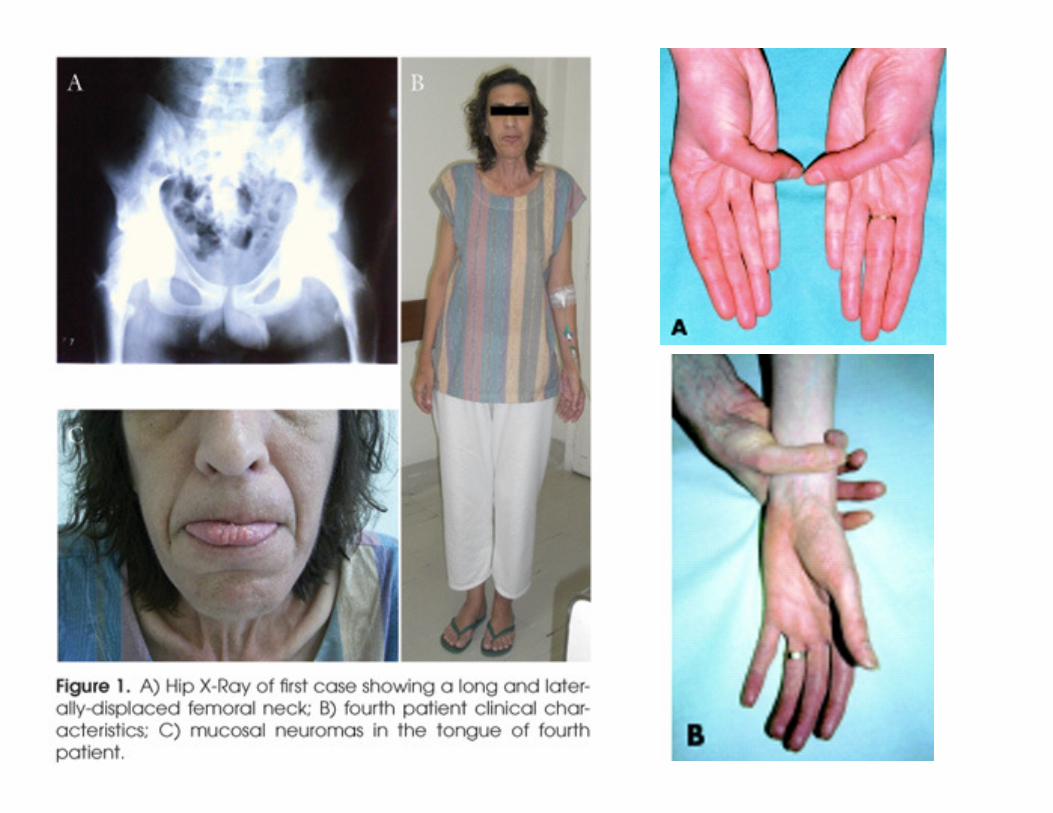
Type 2B
• Medullary thyroid cancer
• Pheochromocytoma
• Other
-Mucosal neuromas
-Intestingal ganglioneuromas
-Marfanoid habitus
Familial medullary thyroid cancer (variant of 2A)
• Medullary thyroid cancer

Band keratopathy
Subepithelial Ca-PO4 deposits in the cornea

Sub-periosteal resorption

Cystic brown tumorsChondrocalcinosis

National Institutes of Health Consensus Conference
in 2008
Asymptomatic PHPT candidates for surgery
• Age < 50 yr
• Serum calcium level ≥ 1.0 mg/dl (0.25 mmol/liter)
above upper limits of normal
• Cr.Cl reduced to 60 ml/min by MDRD equation no.7
• Osteoporosis by T-score
• History of kidney stones or fractures
J Clin Endocrinol Metab 94: 366–372, 2009
Symptomatic PHPT
Cohort studies : after parathyroidectomy
• BMD & fracture rate : improve
• Cognitive function : improve
• Kidney stones : incidence declines after surgery.
• CVD & premature death : decrease

Sestamibi scan
• Noninvasive
• Most popular
• Localize abnormal
parathyroid glands
• Quality varies
• Nonlocalizing sestamibi
-Multigland disease
-Small parathyroid gl.
-Coexistent thyroid dz.

Secondary and tertiary hyperparathyroidism2°hyperparathyroidism
•Severe chronic kidney disease
•Usually have low or normal serum calcium concentrations
•Prolonged disease, may develop hypercalcemia
'Adynamic bone disease‘
3°hyperparathyroidism
•Advanced renal failure
•Due to progression from appropriate parathyroid
hyperplasia to autonomous overproduction of PTH
UTD18.1

Milk-alkali syndrome
• Triad of hypercalcemia, metabolic alkalosis, and
renal insufficiency
• Associated with the ingestion of large amounts of
calcium and absorbable alkali
• Typically occurs in the setting of excess calcium
carbonate supplementation to treat osteoporosis
or dyspepsia
UTD18.1
Milk-alkali syndrome
• Metabolic alkalosis can directly stimulating calcium reabsorption in the distal tubule, thereby diminishing
calcium excretion
• Calcium-induced decline in renal function, due to renal
vasoconstriction
• Chronic hypercalcemia, renal structural injury, can also contribute to the inability to excrete the excess calcium
• Renal function usually returns to baseline after cessation of milk or calcium carbonate intake, but irreversible injury
can occur in patients who have prolonged hypercalcemia
UTD18.1

Milk-alkali syndrome
• What remains unexplained is the apparent
difference in sensitivity of individuals to increased
intake of calcium and alkali
• Some individuals may not suppress
calcitriol levels in response to large doses of
calcium carbonate
UTD18.1

Malignancies associated with hypercalcemia
Osteolytic metastases:
•Breast cancer
•Multiple myeloma
•Lymphoma
•Leukemia
Humoral hypercalcemia (PTHrP):
•Squamous cell carcinomas
•Renal carcinomas
•Bladder carcinoma
•Breast cancer
•Ovarian carcinoma
•Non-Hodgkin lymphoma
•CML
•Leukemia
•Lymphoma
1,25- dihydroxyvitamin D:
•Lymphoma (Non-Hodgkin, Hodgkin,
lymphomatosis/granulomatosis)
•Ovarian dysgerminomas
Ectopic PTH sectretion:
•Ovarian carcinoma
•Lung carcinomas
•Neuroectodermal tumor
•Thyroid papillary carcinoma
•Rhabdomyosarcoma
•Pancreatic cancer
UTD18.1

Treatment of hypercalcemia
• Saline therapy
• Loop diuretic
• Initiated routinely once fluid repletion had been
achieved to further increase urinary calcium
excretion
• Calcitonin
• Bisphosphonate
• Dialysis
UTD18.1

Calcitonin
• Reduce serum calcium by increasing renal calcium excretion
• Decreasing bone reabsorption via interference with osteoclast maturation
• Salmon calcitonin (4 international units/kg) is usually
administered IM or SC every 12 hour
• Limited to first 48 hours, even with repeated doses,
indicating the development of tachyphylaxis, perhaps due to receptor downregulation
UTD18.1

Bisphosphonates
• Intravenous zoledronic acid or pamidronate
Side effects
• Flu-like symptoms
(fever, arthralgias, myalgia, fatigue, bone pain)
• Ocular inflammation (uveitis)
• Hypocalcemia
• Hypophosphatemia
• Impaired renal function/nephrotic syndrome
• Osteonecrosis of the jaw
UTD18.1

Glucocorticoid
Responsible for the hypercalcemia associated …
•Excess ingestion of vitamin D
•Endogenous overproduction of calcitriol
(1,25-dihydroxyvitamin D)
• Chronic granulomatous diseases
eg, sarcoidosis
• Lymphoma
UTD18.1

Hypocalcemia
• Clinical manifestations of hypocalcemia depend
upon the severity and chronicity of hypocalcemia
• Each 1 g/dL reduction in the serum albumin
concentration will lower the total calcium
concentration by approximately 0.8 mg/dL

Clinical manifestations of hypocalcemiaAcuteNeuromuscular irritability (Tetany) •Paresthesias (peri-oral, extremities) •Muscle twitching •Carpopedal spasm •Trousseau's sign •Chvostek's sign •Seizures •Laryngospasm •Bronchospasm
Chronic•Ectopic calcification (basal ganglia) •Extrapyramidal signs •Parkinsonism •Dementia
Cardiac •Prolonged QT interval •Hypotension •Heart failure •Arrhythmia •Papilledema
• Subcapsular cataracts • Abnormal dentition • Dry skin

Major causes of hypocalcemia
Low PTH (hypoparathyroidism) Genetic disorders •Abnormal parathyroid gland development
•Abnormal PTH synthesis •Activating mutations of calcium sensing receptor (autosomal dominant hypocalcemia or sporadic isolated hypoparathyroidism) Post-surgical :
thyroidectomy, parathyroidectomy, radical neck dissection Autoimmune•Autoimmune polyglandular syndrome (associated with chronic mucocutaneous candidiasis and primary adrenal insufficiency)
•Isolated hypoparathyroidism due to activating antibodies to calcium sensing receptor Infiltration of the parathyroid gland :granulomatous, iron overload, metastases
Radiation induced destruction parathyroid glands Hungry bone syndrome (post parathyroidectomy) HIV infection
UTD18.1

Major causes of hypocalcemia
Low PTH (hypoparathyroidism) Genetic disorders •Abnormal parathyroid gland development
•Abnormal PTH synthesis •Activating mutations of calcium sensing receptor (autosomal dominant hypocalcemia or sporadic isolated hypoparathyroidism)Post-surgical :
thyroidectomy, parathyroidectomy, radical neck dissection Autoimmune •Autoimmune polyglandular syndrome (associated with chronic mucocutaneous candidiasis and primary adrenal insufficiency)
•Isolated hypoparathyroidism due to activating antibodies to calcium sensing receptor Infiltration of the parathyroid gland :granulomatous, iron overload, metastases
Radiation induced destruction parathyroid glands Hungry bone syndrome (post parathyroidectomy) HIV infection

Major causes of hypocalcemia
High PTH (secondary hyperparathyroidism in response to hypocalcemia) •Vitamin D deficiency or resistance •Parathyroid hormone resistance
• Pseudohypoparathyroidism • Hypomagnesemia
•Renal disease •Loss of calcium from the circulation
• Hyperphosphatemia • Tumor lysis • Acute pancreatitis • Osteoblastic metastases • Acute respiratory alkalosis • Sepsis or acute severe illness
Drugs
•Inhibitors of bone resorption (bisphosphonates, calcitonin), especially in vitamin D deficiency
•Cinacalcet
•Calcium chelators (EDTA, citrate, phosphate)
•Foscarnet (due to intravascular complexing with calcium)
•Phenytoin (due to conversion of vitamin D to inactive metabolites)
•Fluoride poisoning
Disorders of magnesium metabolism
•Hypomagnesemia can reduce PTH secretion or cause PTH resistance and is therefore associated with normal, low, or high PTH levels
UTD18.1

Approach to hypocalcemia
• Measure serum albumin
• Family history of hypocalcemia genetic cause
• Chronic hypocalcemia • Activating mutation of calcium sensing receptor
• Pseudohypoparathyroidism
• Acquired hypoparathyroidism • Postsurgical or autoimmune damage
• Autoimmune hypoparathyroidism • Isolated abnormality/polyglandular autoimmune syndrome type I
• Lab : iPTH, Cr, Mg, PO4, 25(OH) vitD
UTD18.1

N Engl J Med 2004;350:2068-79

PTH Correct
Ca
PO4 Mg 25(OH)D 1,25(OH)D Cr
Hypoparathyroid
Activating
mutation calcium
sensing receptor
Hypo Mg
PTH resistance
(pseudohypo-
parathyroid)
Vitamin D
deficiency
Chronic kidney
disease
UTD18.1

PTH Correct
Ca
PO4 Mg 25(OH)D 1,25(OH)D Cr
Hypoparathyroid
Activating
mutation calcium
sensing receptor
Hypo Mg
PTH resistance
(pseudohypo-
parathyroid)
Vitamin D
deficiency
Chronic kidney
disease
UTD18.1

Osteoporosis
• Decrease bone strength and increase fracture
• Imbalance of bone resorption and bone formation
• Bone strength
• Structural properties : Size, Shape,
Microarchitecture
• Material properties : Mineral, Collagen

WHO definition of Osteoporosis
Diagnostic Category T-score
Normal > -1
Osteopenia -1 to -2.5
Osteoporosis ≤ -2.5
Severe Osteoporosis ≤ -2.5 and
≥ 1 fragility fracture

ข้อบ่งชี ในการส่งตรวจ BMD
Thai osteoporosis guideline
Thai osteoporosis guideline

BMD (DEXA)
Central
•Lumbar spine (L1-L4)
•Femoral area
Peripheral
•Radius
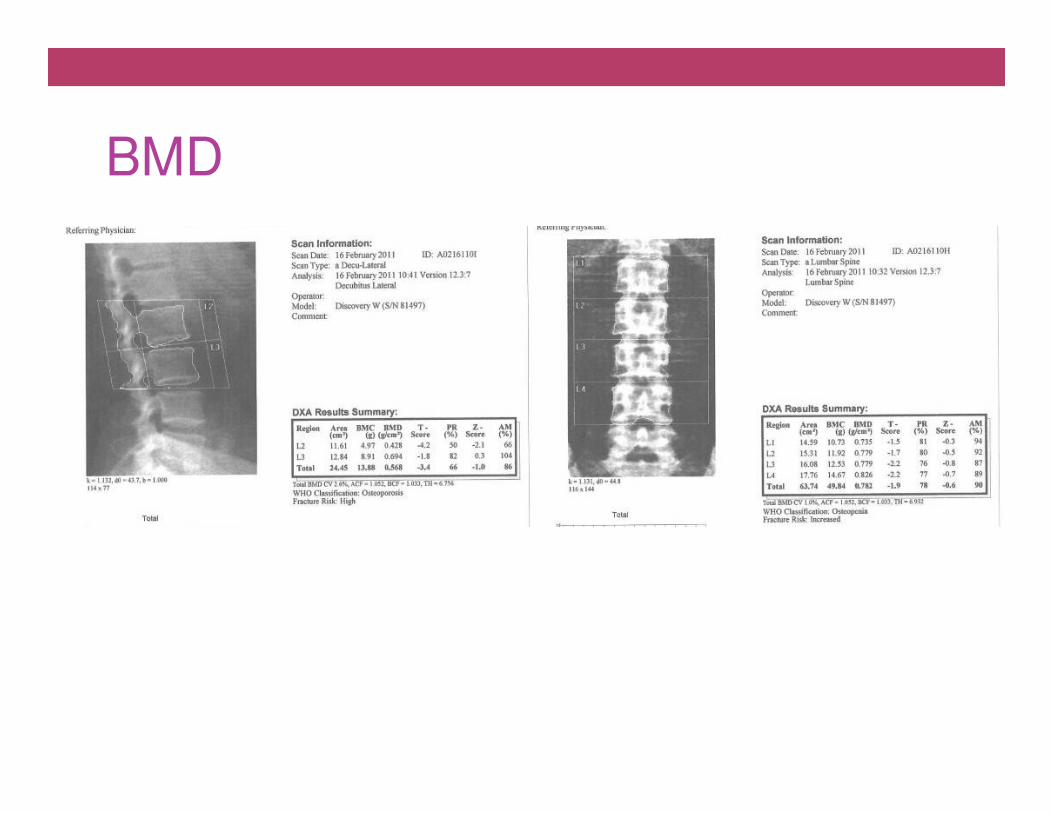
BMD

BMD

BMD

BMD

Common causes for secondary osteoporosisEndocrine diseases GI disorders
• Diabetes mellitus
• GH deficiency (rare)
• Acromegaly (rare)
• Hypercortisolism
• Hyperparathyroidism
• Hyperthyroidism
• Premature menopause
• Male hypogonadism
• Gastrectomy
• Celiac disease
• Inflammatory bowel
disease
• Liver cirrhosis
• Chronic biliary tract obstruction
• Chronic therapy with proton pump inhibitors
European Journal of Endocrinology (2010) 162 1009–1020

Hematologic diseases Rheumatological
• Myeloma
• Monoclonal gammopathy of undetermined significance
• Lymphoma/leukemia
• Systemic mastocytosis (rare)
• Disseminated carcinoma
• Chemotherapy
• Rheumatoid arthritis
• Ankylosing spondylitis
• Systemic lupus
erythematosus
European Journal of Endocrinology (2010) 162 1009–1020
Other
Common causes for secondary osteoporosisCommon causes for secondary osteoporosis
• Osteogenesis imperfecta
• Anorexia nervosa

Glucocorticoid excess
• Glucocorticoids impairs skeletal health
• Inhibition of bone formation due to induction of
osteoblast and osteocyte apoptosis
European Journal of Endocrinology (2010) 162 1009–1020

Glucocorticoid excess
• Predominant spinal bone loss and vertebral
fractures
• Increased risk of falls due to muscular atrophy
and altered neuromuscular function
• Low doses of glucocorticoids (prednisolone 2.5–
7.5 mg/day) associated with a 2.6-fold higher risk
of vertebral fractures
European Journal of Endocrinology (2010) 162 1009–1020

Glucocorticoid-induce Osteoporosis
N Engl J Med 2011;365:62-70

Glucocorticoid-induce Osteoporosis
N Engl J Med 2011;365:62-70
• National osteoporosis foundation
• Prednisolone ≥ 5 mg/day for at least 3 months
• Yearly BMD testing
• Threshold for treatment : T-score ≤ 2.5
• Calcium 1200 mg/day, vitamin D 2000 units/day
• Bisphosphonate
• Teriparatide : only for patients at high risk

Hyperthyroidism
• Thyroid hormone excess
(suppressed TSH)
• Activation of thyroid
hormone receptor a on
osteoblasts and osteoclasts
results in enhanced bone
resorption and bone loss
European Journal of Endocrinology (2010) 162 1009–1020

Hyperthyroidism
Large study of 686 postmenopausal women
•serum TSH level < 0.1 mIU/l
•4x – 5x risk of hip and vertebral fractures
Meta-analysis of 21 studies indicated that
•thyroid hormone therapy for TSH suppression in
differentiated thyroid cancer
•subclinical hyperthyroidism is associated with
osteoporosis in postmenopausal women
European Journal of Endocrinology (2010) 162 1009–1020

Drug-induced osteoporosis
• Numerous drugs affect bone metabolism
interfere
• Absorption of vitamin D, Ca, and PO4
• Vitamin D metabolism and action
• Direct cellular effects on
osteoblasts, osteoclasts, and osteocytes
• Interference amount or quality of bone matrix
proteins
European Journal of Endocrinology (2010) 162 1009–1020

Drug-induced osteoporosis
• TZDs (rosiglitazone and pioglitazone)
• Insulin sensitizers
• Act as agonists of the peroxisome proliferator-
activated receptor-gamma
• 3-5 fold higher risk of fractures of the humerus,
femur, and hip in postmenopausal women
European Journal of Endocrinology (2010) 162 1009–1020

Drug-induced osteoporosis
• TZD
• Shunting pluripotent mesenchymal stem cells
Osteoblastic lineage Adipocyte
European Journal of Endocrinology (2010) 162 1009–1020

Drug-induced osteoporosis
European Journal of Endocrinology (2010) 162 1009–1020
Drug class Examples Indications
Glucocorticoids Prednisolone Autoimmune diseases
Chemotherapeutic drugs Methotrexate, ifosfamide
Tyrosine kinase inhibitors Imatinib Chronic myelogenous
leukemia
Thiazolidinediones Rosiglitazone, pioglitazone Type 2 diabetes mellitus
Proton pump inhibitor Omeprazole and
pantoprazole
Peptic ulcer and reflux
diseases
Thyroid hormone L-thyroxine Replacement therapy for
hypothyroidism, thyroid
cancer
Anticonvulsants Valproic acid Chronic seizure disorders
Antidepressants Selective serotonin re-
uptake inhibitors
Chronic depression
Anti-retroviral drugs Tenofovir HIV disease

Diagnostic tests in the work-up of secondary osteoporosis
European Journal of Endocrinology (2010) 162 1009–1020
Diagnostic tests Purpose
CBC Anemia as in myeloma or celiac
disease, Leukocytosis as in leukemia
Renal and Liver function test Renal or liver failure, alcohol abuse
Ca and PO4 Primary hyperparathyroid, myeloma
Serum bone specific or ALP Paget’ disease, osteomalacia
Serum 25-hydroxyvitamin D Vitamin D deficiency, osteomalacia
Serum TSH Hyperthyroidism
FBS Diabetic mellitus
Intact PTH Primary hyperparathyroidism
Serum protein electrophoresis,
immunofixation
MGUS, myeloma

European Journal of Endocrinology (2010) 162 1009–1020
Diagnostic tests Purpose
Serum free testosterone Male hypogonadism
Serum CRP Chronic infection/inflammation
24 hour urine calcium excretion Hypercalciuria
Anti-tissue transglutaminase
antibodies
Celiac disease
Anti-HIV antibodies HIV disease, AIDS
Morning fasting serum cortisol after
dexamethasone suppression
Cushing’s syndrome
Serum tryptase levels, urinary
histamine excretion
Systemic mastocytosis
COL1A genetic testing Osteogenesis imperfecta
Iliac crest bone biopsy Systemic mastocytosis,
MGUS/myeloma,
osteomalacia, lymphoma/leukemia
Diagnostic tests in the work-up of secondary osteoporosis

Laboratory Evaluation
• CBC
• Renal function
• Chemistry : Ca, PO4, ALP, LFT
• ESR, CRP
• Thyroid function test
• 25- hydroxyvitamin D
• Gonadal function

Treatment of Osteoporosis
• Pharmacotherapy
• Secondary cause
• Lifestyle Modification

Factor Influencing Fractures
Hormone
Nutrition
Exercise &
Life style
Bone massBone
strength
Falls
Postural
reflexes
Soft tissue
padding
Fracture
Shape &
architecture
Material
properties

Lifestyle Modification
• Weight-bearing exercise : jogging, aerobic
dancing, jumping rope
• Physical activity : 30 min / most day of week
• Fall prevention

Treatment (NOF 2008)
• Postmenopausal women and men older than 50 yr
• A hip or vertebral fracture fracture
• T –score < -2.5 at femoral neck, total hip or spine
• Low bone mass (T –score -1 to -2.5 at femoral neck, total
hip or spine) with other prior fracture
• Low bone mass (T –score -1 to -2.5 at femoral neck, total
hip or spine) with secondary causes associated with high
risk fracture
• Low bone mass (T –score -1 to -2.5 at femoral neck, total hip or spine) and 10- yr probability of hip fracture ≥ 3% or
a 10-yr probability of any major osteoporosis related fracture ≥ 20%

การรักษาภาวะโรคกระดกูพรุน
Thai osteoporosis guideline

Thai osteoporosis guideline

Thai osteoporosis guideline

Pharmacotherapy
Adequate Calcium and vitamin D intake
•NOF 2008 : -Ca 1200 mg per day,
-Vitamin D 800-1000 IU per day
•Thai :
-Ca ; 19-50 yr : 1000 mg per day, >50 yr : 800 mg per day
-Vitamin D : 400-800 IU per day

Which drugs should be used?
• Antiresorptive agents
• Bisphosphonate
• Calcitonin
• Hormone replacement therapy
• Selective estrogen receptor modulators
• Bone formative (anabolic) agents
• Teriparatide (1-34 PTH)
• Double action
• Strontium ranelate

• Targeting of bisphosphonates to bone, localized
release during osteoclastic bone resorption
• Intestinal absorption is low
• Taken with a glass of tap water and ≥ 30 min
before food or other fluids
• 40-60% absorbed bisphosphonate not bound to bone & not metabolized
• Eliminated unchanged by renal excretion
Bisphosphonate

Flu-like symptoms
• Bisphosphonates IV can block FPP production in
monocytes
• Accumulation of isopentenyl diphosphate (IPP)
• Because IPP is also a bacterial antigen,
peripheral blood T cells recognize this as
bacterial infection
• Releasing TNF-α and IFN-γ, increasing IL-6 and
CRP, and causing flu-like symptoms
• Associated with 1st bisphosphonate doses

Esophagitis and ulceration
• Before absorption, bisphosphonates taken orally
can bind to gastric cells
• Inhibition of FPP synthase rapidly leads to cell death.
• This may explain the ability of orally administered
N-BPs to cause esophagitis and ulceration

Osteonecrosis of the Jaw (ONJ)
• Rarely with oral bisphosphonates
• Most cases of Pt cancer with IV bisphosphonates
• Risk factors
-Cancer
-Concomitant therapies
(chemotherapy, radiotherapy and corticosteroids)
-Poor oral hygiene
-Comorbid eg. anemia, coagulopathy, infection
-Duration of exposure, and older age CKD

www.wondershare.com
Osteonecrosis
of Jaw
Prevention (recommend)
• Before use bisphosphonates :removal of all foci of
dental infection.
• Routine dental care
• Regular oral examinations

Osteomalacia
• Osteomalacia : disorder of mineralization of newly formed matrix in adults
• Rickets : disorder of defective mineralization of cartilage
in the epiphyseal growth plates of children, leading to widening of the ends of long bones, growth retardation,
and skeletal deformities.

Normal bone
Osteoporosis
Osteomalacia
Osteoporosis + osteomalacia
Suggest osteomalacia• Bone pain, tenderness
• Myopathy
• Pseudofracture• Increased alkaline P
Decreased bone mineralization and matrix
Decreased bone mineralization
with normal or increased matrix
Causes of osteomalaciaAbnormal vitamin D metabolism : 2° hyperparathyroidism & hypophosphatemia
Deficient intake or absorption•Dietary •Inadequate sunlight exposure •Malabsorption •Gastrectomy •Small bowel disease •Pancreatic insufficiency Defective 25-hydroxylation •Biliary cirrhosis •Alcoholic cirrhosis •Anticonvulsants Loss of vitamin D binding protein•Nephrotic syndrome Defective 1-alpha 25-hydroxylation •Hypoparathyroidism •Renal failure •Vitamin D-dependent rickets type 1 Defective target organ response to calcitriol •Vitamin D-dependent rickets, type II (Hereditary vitamin D resistant rickets, HVDRR)
Vitamin D

Causes of osteomalacia
Mineralization defects
Abnormal matrix
•Chronic renal failure
•Osteogenesis imperfecta
•Fibrogenesis imperfecta
•Axial osteomalacia
Enzyme deficiency
•Hypophosphatasia
Inhibitors of mineralization
•Fluoride
•Aluminium
•Bisphosphonates
Phosphate deficiency Decreased intake •Antacids Impaired renal reabsorption -Primary defects •X-linked hypophosphatemic rickets
(vitamin D resistant rickets, VDRR) •Hereditary hypophosphatemic rickets with hypercalciuria •Sporadic acquired hypophosphatemic rickets •Fanconi Syndrome-Wilson disease, cystinosis, multiple myeloma -Secondary defects •Primary hyperparathyroidism •Secondary hyperparathyroidism (renal tubular acidosis, type 1 and disorders of vitamin D metabolism) •Oncogenic osteomalacia

CLINICAL PRESENTATION
• Asymptomatic and present radiologically as osteopenia
• Proximal muscle weakness • Muscle wasting, hypotonia, and discomfort with movement
• Waddling gait
• Bone pain • lower spine, pelvis, lower extremities
• may be associated with tenderness to palpation
• dull & aching, aggravated by activity & weight bearing
• Fractures • may occur with little or no trauma
• ribs, vertebrae, long bones
• Skeletal deformities are infrequent in adults.
• Abnormal spinal curvature or deformity of the thorax or pelvis appears only in severe osteomalacia of long duration


• Looser zones : pseudofractures or narrow radiolucent lines
Two theories have been proposed:1. Stress fractures that have been repaired by the laying down of inadequately mineralized osteoid2. Result of erosion by arterial pulsations.

Disorder Phosphate Calcium ALP
Vit D deficiency with 2° hyper PTH
Low Low to low normal
Elevated
Metabolic acidosis Normal Normal Normal
Proximal RTA Low Normal Normal
Hypophosphatasia Normal Normal Low
Osteogenesis imperfecta and
axial osteomalacia
Normal Normal Normal
Osteoporosis Normal Normal Normal

Vitamin D deficiency
• 25-Hydroxyvitamin D levels are inversely associated with parathyroid hormone levels until the former reach 30 to 40
ng per milliliter, at which point PTH begin to level off (at
their nadir)
Vitamin D insufficiency ..
25-hydroxyvitamin D < 30 ng per milliliter
Vitamin D intoxication ..
25-hydroxyvitamin D > 150 ng per milliliter

Treatment
Preventive and Maintenance to Avoid Deficiency
•800–1000 IU of vitamin D3/day
•50,000 IU of vitamin D2 every 2 wk or every
month
Treatment of Deficiency
•50,000 IU of vitamin D2 every wk for 8 weeks
•Then repeat treatment for another 8 wk if 25-
hydroxyvitamin D <30 ng/ml
Recommended