NASHP Annual Conference
Blazing New Trails:Shifting the Focus on Alcohol
and Drugs
Barbara CimaglioSally Fogerty, BSN, M.Ed.
John C. Higgins-Biddle, Ph.D.October 15, 2007

© 2002-07 John C. Higgins-Biddle 2
Main Topics
What’s the Problem?
What is Screening, Brief Intervention, and Referral to Treatment?
What is the Federal Government Doing?
What States Can Do?

© 2002-07 John C. Higgins-Biddle 3
Alcohol and Drugs . . .
Kill over 85,000 Americans per year; third leading cause of death
Cost over $250 billion in lost productivity, health costs, legal and justice issues
Are perceived to be moral problems, legal problems, social problems, a failure of individual responsibility

© 2002-07 John C. Higgins-Biddle 4
Alcohol and Drugs . . .
Cause/exacerbate many medical, mental, social and family problems
Their use is often unidentified by doctors Diagnose & treatment of many diseases &
disorders often neglect their use This applies to many levels of use besides
alcoholism and drug dependence Understanding requires new perspective

© 2002-07 John C. Higgins-Biddle 5
How we address other issues
Are you a better driver than a typical 16 year-old male?
Have you had an auto crash? Does your state require seatbelt use? Who has more heart attacks: People diagnosed
with heart disease; those without heart disease? So what?

© 2002-07 John C. Higgins-Biddle 6
The Preventive Paradox
Large group (LG) with small problems vs. small group (SG) with big problems
Good drivers (LG) have more accidents than high-risk drivers (SG)—hence seatbelts for all
Patients without a diagnosis of heart disease (LG) have more heart attacks than those with a diagnosis (SG) —hence screen all for cholesterol

© 2002-07 John C. Higgins-Biddle 7
Types of Alcohol/Drug Risk
Dependence—a cluster of behavioral, cognitive, and physiological phenomena that may develop after repeated use
Harmful Use—consumption causing physical, mental, or social harm
Hazardous Use—consumption causing elevated risk without presence of physical or mental harm (yet)

© 2002-07 John C. Higgins-Biddle 8
Who Causes the Harm?
Small group with Dependence experience & cause the most harm
But there are far more Hazardous and Harmful users
So Hazardous & Harmful drinkers cause at least half of alcohol/drug harm
Two ways—high-level regular use and occasions of intoxication lead to work, health, social, legal problems

© 2002-07 John C. Higgins-Biddle 9
What we don’t see can hurt!

© 2002-07 John C. Higgins-Biddle 10
Biggest Drug Issue: Alcohol
Despite publicity, illicit drugs are a small part of America’s problems
Alcohol misuse dwarfs the problems of illicit drugs
Misuse occurs in all age, racial, and social groups, and in both genders
But the biggest problem is not alcoholism

© 2002-07 John C. Higgins-Biddle 11
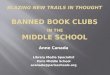
The Drinkers’ Pyramid
Dependent Drinkers
Harmful/Hazardous Drinkers
Responsible Drinkers
Abstainers

© 2002-07 John C. Higgins-Biddle 12
Treatment alone won’t work
For 50 years USA has had the world’s best treatment system but always 5% dependent
87% of people who need TX don’t want it We typically wait 20 years—until dependence-
to help people who drink too much For every dependent patient who quits or dies,
a harmful user becomes dependent Meanwhile harmful users produce ½ our harm
while we could help many in 5 minutes

© 2002-07 John C. Higgins-Biddle 13
Summary of the Problem
25% use too much at least once/year 5% are dependent; 20% are not Reducing problems requires finding and
helping both groups So how can we find them and help the
hazardous, harmful, and dependent—each of whom needs somewhat different kinds of help?

© 2002-07 John C. Higgins-Biddle 14
We need a new focus
Alcohol & drug treatment are not provided where most people regularly go
To find a health problem among all Americans we must go to general medical settings
So to find people who misuse alcohol & drugs we must enlist medical services
This is requiring a new focus & approach

© 2002-07 John C. Higgins-Biddle 15
SBIRT Provides a Way
Screening identifies degree of risk and likelihood of a condition
Brief Intervention helps patients reduce hazardous and harmful use
Referral sends dependent patients to specialized Treatment

© 2002-07 John C. Higgins-Biddle 16
Screening for Drugs/Alcohol
25 years of research in medical sites Where people go with health issues and
expect to be asked questions Self-report screening is quick, accurate, and
inexpensive Can be done via paper, oral, computer Good screens distinguish risk levels But do patients get upset?

© 2002-07 John C. Higgins-Biddle 17
Patient Comfort
0102030405060708090
100
Very
Comfortable
Very
Uncomfortable
Diet/Exercise
Smoking
Drinking

© 2002-07 John C. Higgins-Biddle 18
Patient Sense of Importance
0102030405060708090
100
Very
Important
Very
Unimportant
Diet/Exercise
Smoking
Drinking

© 2002-07 John C. Higgins-Biddle 19
Goals of Screening
• Identify both hazardous/harmful use and those likely to be dependent
• Create a professional, helping atmosphere• Gain the patient information needed for an
appropriate intervention• Use as little patient/staff time as possible

© 2002-07 John C. Higgins-Biddle 20
Who and When to Screen?
Not knowing who drinks or uses drugs, we must screen everyone who is able yearly
Rough estimates of excessive use by setting: Primary Care—10-25% Ob-Gyn—10-20% Emergency—20-40% Trauma—40-60%
Should become as common as blood pressure Can be done by existing or special personnel

© 2002-07 John C. Higgins-Biddle 21
Brief Intervention
Structured brief advice/counseling Builds upon screening info Non-judgmental, interactive, empathic Aims: to reduce or stop use; or to refer patient
to specialized treatment Cognitive info and motivation to change Differing protocols, similar results

© 2002-07 John C. Higgins-Biddle 22
Elements of an Intervention
1. Feedback from screening on risks
2. Advice to reduce use & risk
3. Negotiation of patient acceptance of responsibility & choice of a goal
4. Information on limits and “how to”
5. Encouragement/Motivation

© 2002-07 John C. Higgins-Biddle 23
Referral To Treatment
• Screening can supply a likelihood of dependence
• Those who are dependent may benefit from a brief intervention but probably need motivation for traditional treatment
Early identification may get more patients to treatment earlier; thus increasing effectiveness of therapy, decreasing costs

© 2002-07 John C. Higgins-Biddle 24
Research Findings
Since 1980, 50+ different clinical trials—One 3-5 min. to multiple 15-30 min. sessions
Most studies show positive results of decreasing use among many (not all) patients
Effective with all ages, races, genders, ethnics Some benefit from follow-up session; least
effective with most severe cases Low cost: One study--<$1 screen; <$4 doc BI Supports a preventive public health service

© 2002-07 John C. Higgins-Biddle 25
Policy Actions to Date
USPSTF rates evidence for alcohol SBI with Cholesterol Screening and Flu Shots for Elderly
Most physician societies have endorsed it Am. College of Surgeons Com. on Trauma
requires it in Level I centers; other levels to follow
Federal govt. agencies now acting

© 2002-07 John C. Higgins-Biddle 26
How to pay for SBIRT
CMS issued new Medicaid codes for SBIRT H0049 for Screening H0050 for Brief Intervention
Must be adopted within state plans AMA will announce in November two CPT codes
for SBIRT to be used for private insurance and Medicare beginning Jan. 08

© 2002-07 John C. Higgins-Biddle 27
Federal Agency Actions
NIAAA supported research; NIDA beginning VA initiated program; IHS starting in trauma NHTSA supporting dissemination; CDC supports
emergency/trauma dissemination White House ONDCP supporting budgets and
implementation SAMHSA providing large state & university
grants; more on the way

© 2002-07 John C. Higgins-Biddle 28
SAMHSA SBIRT Initiative
Largest Federal program 11 state/tribal coop. agreements ave. >$2 mil.
per year for 5 years; 12 campus grants ave. $1.3 mil. over 3 years Over 500,000 patients screened since 2004 Programs in large urban hospitals to small rural
clinics More grants to come; plus residency training Stay informed at:
http://sbirt.samhsa.gov/index.htm

Massachusetts Implementation of SBIRT into Primary Care
Sally Fogerty, BSN, M.Ed.Director, Bureau of Family and Community Health

30
Four Models
MASBIRT – Implementation in one large Boston medical center. Implementation on medical inpatient floors, in one ED and several outpatient clinics.
3 Mass colleges are completing the final year of their SAMHSA college SBIRT grants
Twelve Emergency Departments around the state Community Health Centers – adolescents and women of
child-bearing age integration into regular care

31
4 Key Components All Models Screening Brief Intervention Referral to Assessment and/or Treatment

32
MASBIRT Massachusetts is one of 10 states and one tribal
council awarded this SAMHSA funded 5 year grant
Clinical service that utilizes specially trained Health Promotion Advocates to universally screen and help patients with risky or unhealthy tobacco, drug and alcohol use through brief intervention counseling and facilitated referrals to assessments and specialty addiction treatment.
Screening in hospital inpatient, emergency department, and rolling out to 4-5 outpatient clinics

33
MASBIRT
3 CHCs will be added in FY08 Staffing resources –
Health Promotion Advocates work with hospital social workers, some clinical staff in clinics – medical assistants, nurses and physicians.
Standardized questionnaire. Automated patient screening using TLC (telephonic linked care) and a web-based link from EMR to questionnaire and back being developed
New level of treatment – brief treatment

34
Massachusetts Colleges Purpose was to screen students and link with
services Wrapping up and evaluation just being
completed Three colleges involved:
Northeastern University, Boston University of Massachusetts, Amherst Bristol Community College, Fall River
Issue was campus vs. community services – how do you link and get students to utilize community services.

35
Emergency Room Specially trained Health Promotion Advocates
are funded in emergency departments to screen for tobacco, drug and alcohol use, brief intervention counseling and facilitating referrals
12 emergency departments – at least one in each region of the state
800 people screened in August

36
CHC Integration Model
Goal: integration into existing primary care services of on-going screening for Violence Tobacco use Substance use Behavioral health issues
Utilized a new procurement for services for women of reproductive age and adolescents which were previously funded as prenatal and adolescent health programs under MCH.

37
Integration into CHC Primary Care Joint effort of two program areas: Bureau of
Substance Abuse Services and Bureau of Family and Community Health
Paradigm shift from how care currently delivered for women of reproductive age with focus on pre and intra conception and prenatal period.
Train existing providers to do screening and brief intervention
32 programs funded – 17 both adolescents and Women of Reproductive Age; 5 adolescents only and 10 women only.

38
Process – CHC Integration Model Screening of all individuals at annual
visit/prenatal care visit Adult screening tools utilized CRAFFT for adolescents
Early identification of individuals at risk for problems or addiction Brief intervention if high-risk
If positive screen further assessment by professional, may or may not be on site, with additional training
Referral for treatment

© 2002-07 John C. Higgins-Biddle 39
Process – CHC Integration Model Primary care site will follow-up to ascertain
individual goes for first appointment Collaboration between Primary Care and
Treatment providers.

40
Implementation CHC Integration Model Identifying an SBIRT champion Regional trainings by substance abuse vendor
Basic Overview Interview skills Referrals
One-on-one at each site to develop plan to integrate into existing care

41
Where are we – 1 year later CHC Integration Model 100% integrated tobacco 90+ integrated violence Substance abuse/behavior health
1/3 have integrated utilizing questionnaire 1/3 in process majority “tweaking” electronic
medical record to incorporate questions 1/3 still at early stage of implementation

42
CHC Integration Implementation Challenges Takes time – long learning curve Need to change “pattern” of how care delivered
– asking to do something new according to prescribed questions difficult
RFR spelled out expectations and requirements but needed to reinforce and reinforce.
If just setting up electronic medical record easier

43
What have we learned?
Basic acceptance of Concept Development of HCSPCS codes for CMS billing
and CPT codes may promotes screening and brief intervention
Implementation in all sites requires change in process and is a challenge
Need to have a champion If provide “trained advocate” easier to begin
implementation and collect data but sustainability is questionable

© 2002-07 John C. Higgins-Biddle 44
What Have We Learned
Need to have treatment/referral resources available and easy to access.
Need to have relationships between health care and substance abuse/behavioral health treatment providers.

© 2002-07 John C. Higgins-Biddle 45
What States Can Do
Executive Organization Substance abuse agencies often do not relate to
general medicine. Coordinate across many agencies & budgets to reposition the focus & linkages
A public health issue affecting economic development, health, safety, & more (see below)
Establish relations with Level I trauma centers now developing programs & link treatment programs
Work with state medical society to develop programs, provide training, and TA

© 2002-07 John C. Higgins-Biddle 46
What States Can Do
Economic Development/Labor Educate employers that hazardous/harmful users
cause lower productivity and higher health costs Encourage SBIRT coverage in all health plans
Health/Insurance Assure insurance reimburses cost for intoxicated
patients so health services can screen & get paid Include new HCPCS codes in state Medicaid plan Encourage state insurers/HMOs to cover new
CPT codes Get state-supported medical systems to include
SBIRT

© 2002-07 John C. Higgins-Biddle 47
What States Can Do
Administrative Services—Include SBIRT services in health plans for state employees
Higher Education—Implement SBIRT in campus health services
Veterans Affairs—Implement SBIRT Legislature—Require SBIRT inclusion in state
plans & set measurable goals and timelines Everywhere: Educate all in state leaders &
legislators about the real problem & SBIRT Stay informed at:
http://sbirt.samhsa.gov/index.htm
Recommended