
Wassam 1
Effects of Artificial Pacemakers on the Heart
Nick Wassam
BIO 496 DeHart

Wassam 2
Anatomy of the heart:
The mammalian heart has four
chambers, two atria and two ventricles. The
right side of the heart receives blood from the
body via the vena cava. Deoxygenated blood
from the body enters the right atrium and is
then pumped into the right ventricle. From
the right ventricle blood is pumped into the
pulmonary circuit through the pulmonary
artery. Blood is returned to the left side of the
heart from the pulmonary vein and enters the
left atrium. The left atrium pumps the
oxygenated blood into the left ventricle, which
then pumps blood into the systemic circuit in
the body. Figure 1 shows the blood flow
through the heart and systems in the body.
Natural pacemakers:
Normal hearts have an internal pacemaker that allow it to keep a resting heart rate of 60-
100 beats per minute. There are many specialized cells within the heart that help to accomplish
this. The heart beat is regulated by these cells and a feedback loop that connects to the medulla
oblongata, a portion of the brain located near the brain stem. The cells that make up the
Sinoatrial node are made up of slow response tissue that will spontaneously depolarize. This
spontaneous depolarization is what begins the contraction of the heart.
FIGURE 1 SHOWS THE CHAMBERS OF THE HEART AND THE TWO CIRCUITS WHICH THE HEART PUMPS BLOOD INTO, THE PULMONARY AND SYSTEMIC CIRCUITS. NUMBER 11 REPRESENTS THE RIGHT ATRIUM WHERE DEOXYGENATED BLOOD ENTERS FROM THE BODY. NUMBER 1 IS THE RIGHT VENTRICLE, 2 AND 3 REPRESENT THE PULMONARY CIRCUIT. NUMBER 4 IS THE LEFT ATRIUM AND 5 IS THE LEFT VENTRICLE. THE SYSTEMIC CIRCUIT IS REPRESENTED BY NUMBERS 6-10.

Wassam 3
A normal heart has five fully functioning areas to
help conduct the electrical impulse that is sent from the
depolarization of the Sinoatrial node. Figure 2 shows the
progression of that signal. The area labeled number 1
shows the Sinoatrial node (SA node) and is where the
electrical signal in the heart begins. This signal will
interact with the muscles in the atria. When the atria are
stimulated by the signal they will contract and force
blood into the ventricles. Number 2 is known as the
Atrioventricular node (AV node). The AV node will receive the signal from the SA node and
then pass it along to the area labeled number 3. The AV node, in conjunction with the lack of
slow response tissue between the SA and AV nodes, allows for a delay in the signal so the atria
can contract before the ventricles begin to contract. Number 3 is known as the Bundle of His.
This portion transmits the electrical impulse from the AV node to the areas labeled 4 and 5.
Number 4 corresponds to the point at which the cells split into left and right branches so they can
transmit the signal to the left and right ventricles of the heart, respectively. Number 5
corresponds to the bundle branches that innervate the left and right ventricles. These bundle
branches transmit the signal from the branch point and allow the ventricles to contract and pump
blood into the rest of the circulatory system (Strauss, 2013).
History of the artificial pacemaker:
An artificial pacemaker is a medical device for the heart that uses electrical impulses to
regulate and maintain a normal heartbeat. The heart has a natural internal pacemaker that helps it
to keep a resting rate of about 60 to 100 beats per minute. This internal pacemaker consists of
FIGURE 2. THE SPECIALIZED CELLS THAT MAKE UP A NORMAL PACEMAKER IN THE HEART

Wassam 4
special cells that can transmit an electrical impulse to the heart muscle cells and coordinate a
regular heartbeat. An artificial pacemaker does the same thing as the body’s normal pacemaker
but uses external electrical stimulation of the specialized heart cells and the heart’s muscle cells.
Artificial pacemakers have been around since the 1920’s and have become increasingly
more important in cardiology. A study conducted in 1889 showed that the heart could be
stimulated with an electrical impulse to beat at 60-70 beats per minute (McWilliam, 1889). The
first implantable pacemaker was used in 1950 and since then have been increasingly used to
solve many cardiac problems (Trimble, Heimbecker & Bigelow, 1964). There is an increasing
number of people who are in need of an artificial pacemaker, it has become ever more important
to know what a pacemaker is, how it works, who may need a pacemaker and how they are
implanted.
What a pacemaker does:
A pacemaker works by sending an electrical signal to the heart to cause the contraction of
the heart muscle. The pacemaker consists of sensors, electrodes and battery to keep the
pacemaker running. The sensors, depending on the complexity of the device, can sense if the
heart does not keep its normal rhythm, if the heart suddenly stops or skips a beat. If the heart
does not beat or is not beating at the correct pace, the sensor will signal the electrode to stimulate
the heart muscle via an electrical impulse. This impulse then acts as the signal to correct the
irregular beat or rhythm of the heart. The pacemaker can also be programmed to act as the SA
node and constantly stimulate the heart to beat at a normal rate.
Heart defects requiring a pacemaker:

Wassam 5
A heart defect is classified as a problem within the heart or surrounding vessels that do
not allow the heart to function or beat properly. They are caused by a number of reasons and
many require the use of an artificial pacemaker. A pacemaker can be used to treat different types
of heart blocks, syncope, congestive heart failure, and hypertrophic cardiomyopathy.
A heart block can be classified as a first, second or third degree heart block. A first
degree heart block can be seen by a prolonged P-R interval. It is usually caused by a delay in the
AV node. A first degree heart block normally does not require a pacemaker. A second degree
heart block can be classified as a Mobitz type 1 or a Mobitz type 2. Type 1 increases the P-R
interval and eventually causes the heart to skip a beat. Type 2 has repeated P-waves with some
not causing a full heartbeat. Both Type 1 and Type 2 can be treated with an artificial pacemaker
implant. A third degree heart block has a P-wave and QRS complex that have no relationship to
one another. This results in a slow ventricular rhythm and slow heartbeat (Strauss, 2013). This
can be fixed with a pacemaker implant which will act as the P-wave and stimulate normal heart
contraction.
Syncope is a medical term that means fainting or passing out. There are a number of
reasons why a patient may faint, but two causes can be cardiac arrhythmia and cardiac stenosis.
Cardiac arrhythmia can be tachycardia or bradycardia. Tachycardia is increased heart rate and
bradycardia is a slowed heart rate. Cardiac stenosis is the narrowing of the vessels leading in and
out of the heart, or the narrowing of the valves between chambers. Both of these conditions can
cause fainting in patients, and an artificial pacemaker can be implanted to help ensure the heart
beats at a normal rate and does not stop when the patient faints.
Congestive heart failure is the when the heart fails to pump blood through the body. It
can cause a buildup of fluid in different parts of the body. This is dangerous for a patient because

Wassam 6
it can lead to decreased kidney function, pulmonary edema and decreased liver function. By
implanting an artificial pacemaker the heart function will be increased to help meet the demands
of the body. This in combination with drug therapy, diet and exercise can help improve the heart
and overall health of the patient.
Hypertrophic cardiomyopathy is thickening of the heart muscles. This can cause
asynchronization between the chambers of the heart, and between the left and right ventricles. A
dual chamber pacemaker, which will act on each chamber separately, can be used to cause a
synchronized heartbeat. This treatment is not as effective as surgery, but has been shown to
increase heart function in 47% of patients (Ommen et al, 1999).
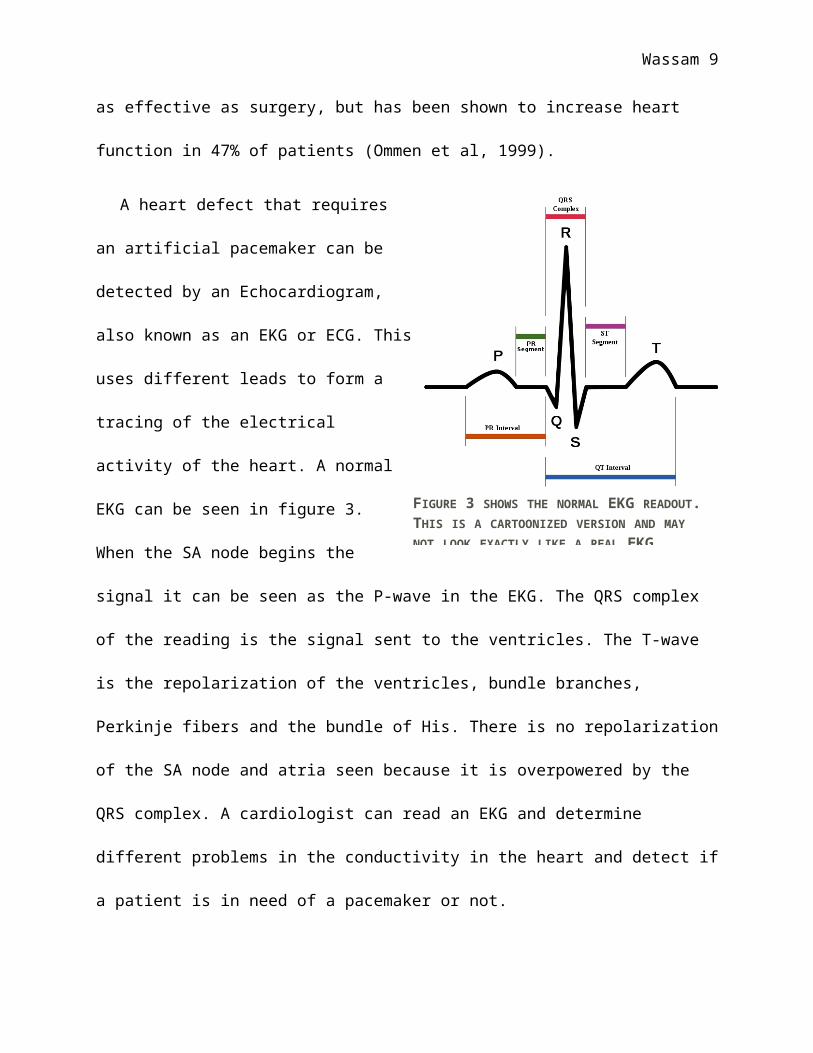
A heart defect that requires an artificial
pacemaker can be detected by an
Echocardiogram, also known as an EKG or
ECG. This uses different leads to form a tracing
of the electrical activity of the heart. A normal
EKG can be seen in figure 3. When the SA node
begins the signal it can be seen as the P-wave in
the EKG. The QRS complex of the reading is the
signal sent to the ventricles. The T-wave is the
repolarization of the ventricles, bundle
branches, Perkinje fibers and the bundle of His. There is no repolarization of the SA node and
atria seen because it is overpowered by the QRS complex. A cardiologist can read an EKG and
determine different problems in the conductivity in the heart and detect if a patient is in need of a
pacemaker or not.
FIGURE 3 SHOWS THE NORMAL EKG READOUT. THIS IS A CARTOONIZED VERSION AND MAY NOT LOOK EXACTLY LIKE A REAL EKG.

Wassam 7
Who may need a pacemaker:
There a number of different reasons for the implantation of an artificial pacemaker. Anyone
who may be suffering from the aforementioned problems may need an artificial pacemaker. The
implantation of an artificial pacemaker will regulate the heartbeat and prevent the heart from
stopping abruptly due to traumatic events. A certified cardiologist will determine when an
implant is necessary. The most common groups that may need a pacemaker are:
The elderly who have a weak heart
Young athletes who suffer from thickening of the heart muscles
Those born with a heart defect
A patient who has suffered traumatic injury
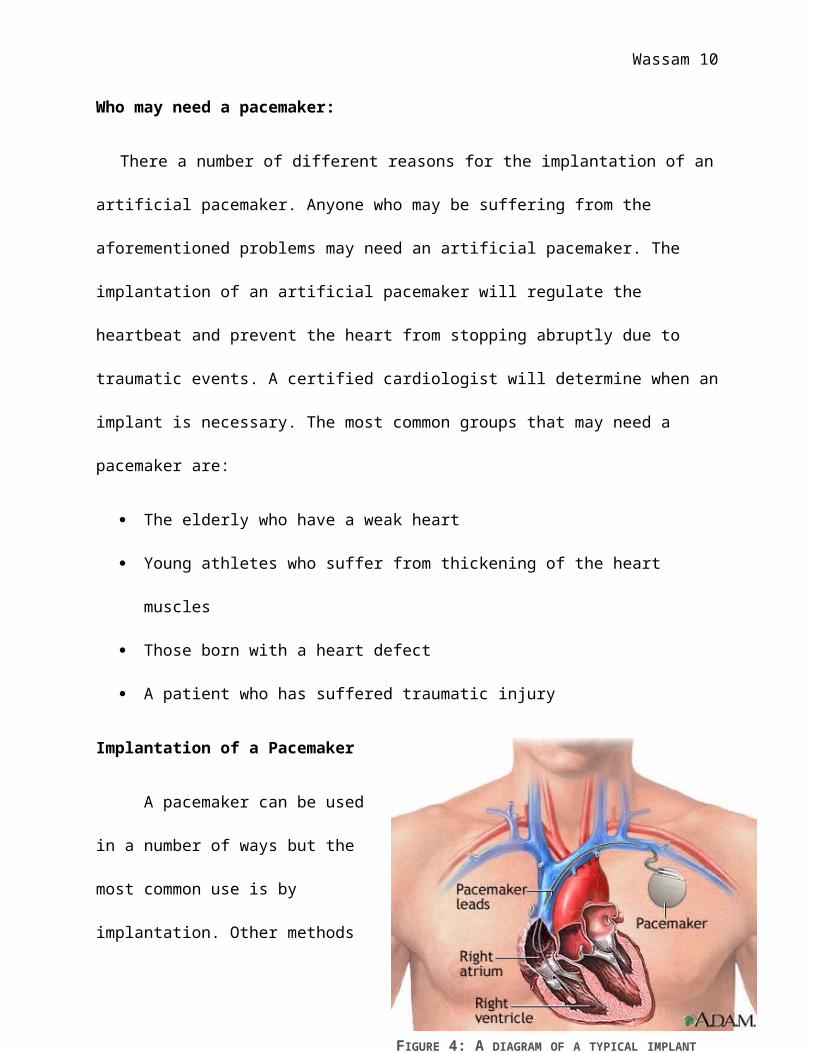
Implantation of a Pacemaker
A pacemaker can be used in a
number of ways but the most common use
is by implantation. Other methods that are
less popular include, transcutaneous and
wearable pacemakers. Implantation is the
preferred method and is much more
common than wearable or other types of
pacemakers. Implantation is an invasive
procedure and may cause some complications but is normally safe and doesn’t cause much harm
to patients. The pacemaker can be inserted transvenously and the electrodes will fun from the
pacemaker into the chambers of the heart. Figure 4 shows a typical transvenous implant. Another
FIGURE 4: A DIAGRAM OF A TYPICAL IMPLANT

Wassam 8
option for implantation is epicardial implantation. This is more common in children and the
pacemaker will rest in the abdomen as opposed to the chest.
The type of heart defect determines what type of pacing the implantation will do and
where the electrodes will be placed. A single chamber pacemaker will be inserted into one
chamber of the heart and will stimulate the heart for a normal coordinated heartbeat. A dual
chamber pacemaker will have electrodes in two chambers of the heart and work to synchronize
the heartbeat and heart function. Another less common type of pacemaker is a dual ventricular
pacemaker. This is inserted into 3 chambers of the heart, the right atria, right ventricle and left
ventricle (Cleveland Clinic, 2010).
Conclusion
There are a broad range of reasons why one would need a pacemaker to help correct a
defect in the heart. The need for a pacemaker is also not limited to one group of people and is
becoming more widespread with the growing population. Pacemakers have been prominent in
cardiology for almost a century. They can be used to correct a number of heart defects and are
becoming increasingly more common and enhances the need to know what they are and when
they are needed.
References:
Websites:
American Heart Association. (n.d.). Retrieved from
http://www.heart.org/HEARTORG/Conditions/CongenitalHeartDefects/AboutCongenital
HeartDefects/About-Congenital-Heart-Defects_UCM_001217_Article.jsp
Wassam 9
Cleveland Clinic. Pacemaker Implant. (2010, April 1). Retrieved , from
http://my.clevelandclinic.org/heart/services/procedures/pacemaker.aspx
National Heart, Lung and Blood Institute. What is a pacemaker? Department of Health and
Human Services. Retrieved from
http://www.nhlbi.nih.gov/health/health-topics/topics/pace/
Stanford Hospitals and Clinics. (2014). Permanent pacemakers. Retrieved from
http://stanfordhospital.org/cardiovascularhealth/arrhythmia/treatments/permanent-
pacemaker/
Text:
Casteel. (2012, March 26). Pacemaker prevents fainting among select patient population.
Retrieved from http://www.cardiosource.org/News-Media/Media-Center/News-
Releases/2012/03/ISSUE_3.aspx?
w_nav=Search&WT.oss=pacemakers&WT.oss_r=2468&
Liptak, G. (2006, April). Heart defects. Retrieved from
http://www.merckmanuals.com/home/childrens_health_issues/birth_defects/
heart_defects.html?qt=&sc=&alt=
McWilliam, J. (1889). Electrical stimulation of the heart in man.British Medical
Journal, 1(1468), 348-350.
Strauss, J. (2013). Biology 472 lecture note packet and study guide. (16 ed.). State College:
ProCopy CourseWorks.
Wassam 10
Trimble, A., Heimbecker, R., & Bigelow, W. (1964). The implantable cardiac
pacemaker. Canadian Medical Association Journal, 90(1), 106-110.
Images:
Figure 1 borrowed from: http://cikgurozaini.blogspot.com/2011/01/circulation.html
Figure 2 borrowed from: http://www.healthyheart.nhs.uk/images/heart03.jpg
Figure 3 borrowed from: http://www.todayifoundout.com/index.php/2011/10/how-to-read-an-
ekg-electrocardiograph/
Figure 4 borrowed from:
http://stanfordhospital.org/cardiovascularhealth/arrhythmia/treatments/permanent-
pacemaker/
Recommended

















