© 2016 by the American Pharmacists Association. All rights reserved.
Billing Boot Camp I
Mary Ann Kliethermes, BS Pharm, PharmD
Sandra Leal, PharmD, MPH, FAPhA, CDE
Gloria Sachdev, BS Pharm, PharmD2
Billing Boot Camp I: Basic Training
3
Disclosures• Mary Ann Kliethermes is co-owner of Clinical pharmacy
Systems Inc.
• [INSERT FACULTY NAME(S)] [INSERT THE FOLLOWING TEXT IF NO CONFLICTS EXIST: “declare(s) no conflicts of interest, real or apparent, and no financial interests in any company, product, or service mentioned in this program, including grants, employment, gifts, stock holdings, and honoraria.” OR LIST THE CONFLICTS ]
The American Pharmacists Association is accredited by the Accreditation Council for Pharmacy Education as a provider of continuing pharmacy education.
4
• Target Audience: Pharmacists
• ACPE#: 0202-0000-16-012-L04-P
• Activity Type: Knowledge-based
5
Learning Objectives
• Explain basic billing terminology.
• Discuss the types of billing opportunities for pharmacists’ services.
• Explain general requirements for billing patient care services in the health care system, including Medicare.
• Identify the key billing decision makers and their influence on pharmacists billing services.
• Describe medication therapy management and billing codes for incident to physician services and how these codes are used to bill for pharmacists’ patient care services.
6
CPT Codes are:
A. Level 1 HCPC (Healthcare Common Procedure Coding System) codes
B. Codes that include the “incident to” Evaluation & Management codes which providers may use to support pharmacist services
C. Used by Medicare Part B for billing purposes
D. Adjusted by the Resource-based Relative Value Scale (RBRVS)
E. All of the above

© 2016 by the American Pharmacists Association. All rights reserved.
7
APC (Ambulatory Payment Classifications) Codes are used in which setting?
• Hospitals or health-systems for “facility fee” services in their ambulatory clinics
• Physician offices for diabetes education services
• Assisted living and group homes for clinical provider services
• For in-home services provided by Medicare Part B providers
8
Which one of the following statements is NOT a CMS criteria for billing incident to physician in a hospital-based outpatient clinic?
A. Must have an order/referral
B. Must have Direct Physician Supervision
C. Must have a continued physician relationship
D. Must be considered a recognized provider
9
Which of the following is a TRUE Statement?
A. MTM CPT codes can be billed under Medicare Part B
B. MTM CPT codes can be billed under Medicare Part D
C.MTM is required by Medicare to be provided by pharmacists
D.MTM is an “opt-in” requirement of Medicare prescription drug plans
10
What are key opportunities for pharmacists to comment on impending Medicare rules?
A. There is never an opportunity for pharmacists to comment on rules.
B. During the Notice of Proposed Rulemaking
C. During the Interim Final Rule
D. After the Final Rule is implement
11
“Je ne sais pa”Understanding
Billing Language
Mary Ann Kliethermes, BS Pharm, PharmD
Vice-Chair, Professor
Chicago College of Pharmacy
Midwestern University
12
Learning Objective
• Explain basic billing terminology
i.e. Words and acronyms you should know and have a basic understanding of what they mean

© 2016 by the American Pharmacists Association. All rights reserved.
13
Demystifying the language
Payer Site/type
Coding• Services• Disease
Forms Rules
14
Whose language do we need to understand?
Federal Medicare
Part A
Part B
Part C
Part D
State
Medicaid
Insurance exchanges
Commercial or Private
Employer based
Group
Individual
15
Commercial Health Insurance Language
Conventional indemnity plan • Allows the participant the choice of any provider without effect on
reimbursement. Reimburse as expenses are incurred.
PPO (Preferred provider organization)• Coverage is provided through a network of selected health care
providers. Enrollees may go outside network, but incur larger costs.
EPO (Exclusive provider organization)• A more restrictive type of preferred provider organization plan.
Employees must use providers from the specified network. There is no coverage for care received from a non-network provider except in an emergency situation.
16
Group Model HMO
• Contracts with a single multi-specialty medical group, the group may only see HMO patients or it may also provide services to non-HMO patients.
Staff Model HMO
• Closed-panel, members receive services only from providers who are HMO employees.
Network Model HMO
• Contracts with multiple physician groups to provide services to members.
IPA (Individual Practice Association) HMO
• A group of independent providers who maintain their own offices and band together to contract their services HMOs.
HMO (Health maintenance organization)
• Assumes financial risks associated with providing medical services & for health care delivery usually in return for a fixed, prepaid fee. Reimbursement only to HMO providers.
17
POS (Point-of-service) • A POS plan is an "HMO/PPO" hybrid• Resemble HMOs for in-network services. • Outside of the network are reimbursed like an indemnity plan
( reimbursement based on a fee schedule or usual, customary and reasonable charges).
PHO (Physician-hospital organization) • Alliances between providers & hospitals to help providers attain market
share, improve bargaining power & reduce administrative costs. • Sell their services to managed care organizations or directly to
employers.
Medigap Supplemental Plans• Pays the Medicare deductibles, copayments, and other expenses
18
Demystifying the language
Payer Site/type
Coding• Services• Disease
Forms Rules

© 2016 by the American Pharmacists Association. All rights reserved.
19
CMS: Center for Medicare and Medicaid Services(HCFA – Health Care Financing Administration – old name)
Medicare Part A
• Universal benefit
• Covers • Hospitals,
Health Systems
• Long term care
• Hospice and Home Health
Medicare Part B
• Must Opt out• Must have
contributed to Social Security
• Covers outpatient services
Medicare Part C
• May opt in • Medicare
Advantage• Administered
by commercial payers
Medicare Part D
• May opt in• Administered
by commercial payers (PDPs)
Hospital PDPsCommercial
PayersProvider
20
Medicare Part A Inpatient Services
Governed by IPPS (Inpatient Prospective Payment System)• MS-DRGs (Medical Severity Diagnosis Related
Groups)• Over 700 clinically cohesive groups that
demonstrate similar consumption of hospital resources and length of stay
• Example MS-DRG 007 – liver transplant• Revenue Codes (4 digits numeric)
• Example 0120 Room and Board/semi-private
www.cms.gov
21
Medicare Part B
Governance documents• PFS (Physician fee schedule)• EHR Incentive Programs “Meaningful use”• PQRS (Physician Quality Reporting
System)• HOPPS (Hospital Outpatient Prospective
Payment System) for hospitals
www.gpo.gov/fdsys/pkg/FR-2015-11-16/pdf/2015-2016.pdf 22
Medicare Part B and Outpatient Hospital ServicesGoverned by
• HOPPS (Hospital Outpatient Prospective Payment System)
• APC or “Facility Fee” Code– Pays the hospital the costs of using the facility to provide services
to the beneficiary
– Where hospital employees may bill for services
https://www.gpo.gov/fdsys/pkg/FR-2015-11-13/pdf/2015-27943.pdf
23
Medicare Part B Provider List
• Anesthesiology Assistants
• Audiologists
• Certified Nurse-Midwives
• Certified Registered Nurse Anesthetists
• Clinical Nurse Specialists
• Clinical Psychologists
• Clinical Social Workers
• Mass Immunization Roster Billers, individuals
• Nurse Practitioners
• Physical/Occupational Therapists in private practice
• Physicians (Doctors of Medicine or Osteopathy, Doctors of Dental Medicine; Dental Surgery; Podiatric Medicine; or Optometry)
• Physician Assistants
• Psychologists practicing independently
• Registered Dietitians or Nutrition Professionals
• Speech-Language Pathologists
https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/downloads/MedEnroll_PhysOther_FactSheet_ICN903768.pdf 24
Medicare Part C
Must provide enrollees with all Part A and Part B services
May also provide Part D
Rules on relationships with providers• Interfering with patient/provider relationship• Incentives to providers• Inclusion/exclusion of providers• Cost sharing
CMS Call Letter
www.cms.gov/Medicare/Health-Plans/HealthPlansGenInfo/

© 2016 by the American Pharmacists Association. All rights reserved.
25
Medicare Part D
• Governed by the CMS Call Letter– https://www.cms.gov/medicare/health-
plans/medicareadvtgspecratestats/downloads/announcement2016.pdf
• CY 2016 Medication Therapy Management Program Guidance and Submission Instructions Memo
– https://www.cms.gov/Medicare/Prescription-Drug-Coverage/PrescriptionDrugCovContra/Downloads/Memo-Contract-Year-2016-Medication-Therapy-Management-MTM-Program-Submission-v-040715.pdf
26
Demystifying the language
Payer Site/typeCoding• Services• Disease
Forms Rules
27
Language of Medicare Reimbursement代码
Medicare Coding System• HCPCS (Healthcare Common Procedure Coding
System)• Level 1 – CPT (Current Procedural Terminology codes)
• 5 numeric digits ex. 99605• Level 2 – Codes for product supplies and services not
covered under CPT (ambulance and durable medical equipment, prosthetics, orthotics, and supplies (DMEPOS) when used outside a physician's)• Single alphabetical letter followed by 4 numeric digits
28
Level 2 HCPC codes• A-codes: Transportation, Medical
Supplies, Misc.& Experimental
• B-codes: Enteral & Parenteral tx
• C-codes: Temporary Hospital Outpatient Prospective Payment System
• D-codes: Dental Procedures
• E-codes: Durable Medical Equip. (DME)
• G-codes: Temporary Procedures & Professional Services
• H-codes :Rehabilitative Services
• J-codes: Drugs Administered Other Than Oral Method, Chemotherapy Drugs
• K-codes: Temporary Codes for DME Regional Carriers
• L-codes: Orthotic/Prosthetic Procedures
• M-codes: Medical Services
• P-codes: Pathology and Laboratory
• Q-codes: Temporary Codes
• R-codes: Diagnostic Radiology Services
• S-codes: Private Payer Codes
• T-codes: State Medicaid Agency Codes
• V Codes: Vision/Hearing Services
29
APC (Ambulatory Payment Classifications) Codes
Pays for most clinic and emergency department visits
Outpatient payment groups based on HCPCS codes• Similar clinical services • Similar resource consumption
APC for Outpatient E/M service’• Describe use of space and supplies• Describe involvement of hospital employees• APC code 5012 (was 0634) with HCPCS code G0463
30
CPT: Current Procedural Terminology codes
Nomenclature to report medical services & procedures for payment
Maintained and owned by the AMA
Category 1 ( 3 categories)
• Evaluation and management (E&M): 99201–99499• Example 99211 incident to code
• Anesthesia: 00100–01999; 99100–99150• Surgery: 10000–69990• Radiology: 70000-79999• Pathology and laboratory: 80000–89398• Medicine: 90281–99099; 99151–99199; 99500–99607
• Example 99605–99607 medication therapy management services

© 2016 by the American Pharmacists Association. All rights reserved.
31
Resource-based Relative Value Scale (RBRVS)
• A system for describing, quantifying, and reimbursing physician services relative to one another.
• three components of physician services– physician work (time, technical skill & effort, judgment & stress)
– practice expense (rent, wages)
– professional liability insurance
• Relative value unit (RVU) is assigned to each
• RVU’s are determined by AMA Committee from physician survey and passed on to CMS to approve and adopt
• Must be budget neutral
• Based on Conversion factor that estimates the sustainable growth rate (SGR) and Geographic Practice Cost Index
32
Why are RVUs important
Work RVU x GPCI
Practice expense RVU x GPCI
Prof liability RVU X GCPI
Total RVU.
Total RVU conversion factor
$$ for a CPT code.
33
ICD-10 Codes: International Classification of Diseases, 10th Revision
• For classifying diagnoses and reason for visits in all health care settings.
• Codes may be 3, 4, 5, 6 or 7 alpha/numeric characters
• Code or codes from A00.0 through T88.9, Z00-Z99.8
• 69,000 codes
NPI number: National Provider Identifier• a unique 10-digit identification number issued to health
care providers
34
What you did: CPT
code
Why you did it:
ICD 10
Who did it: NPI
number
Coding for billing
RVUS
35
Demystifying the language
Payer SiteCoding• Services• Disease
Forms Rules
36
Language of Forms формы
• Health Care Financing Administration 1500 form (HCFA 1500)
– The official standard form used by individual health care providers (e.g., physicians, nurse practitioners) when submitting bills or claims for reimbursement to payers
– Primarily a federal government form, but used universally
• Uniform billing (UB 92- old) and the updated UB-04 also called the CMS-1450 (new)
– i. Form used by facilities or institutions (e.g., hospitals, long-term care facilities) when submitting bills
– Government payers use UB-04, but some private payers may still use UB-92.

© 2016 by the American Pharmacists Association. All rights reserved.
37
HCFA 1500
https://www.cms.gov/Medicare/CMS-Forms/CMS-Forms/downloads/cms1500.pdf
38
CMS-1450
http://www.amazon.com/1450-Medical-Billing-forms-Sheets/dp/B005TOD6YY
39
Demystifying the language
Payer SiteCoding• Services• Disease
Forms Rules
40
CMS General Rules
• “Medically necessary” as “services or supplies that are proper and needed for the diagnosis or treatment of a medical condition and are provided for the diagnosis, direct care, and treatment of the medical condition, meet the standards of good medical practice in the local area, and are not mainly for the convenience of the patient or the provider”
• “Usual /Customary/Reasonable” is the amount paid for a medical service in a geographic area based on what providers in the area usually charge for the same or similar medical service.
https://www.healthcare.gov/glossary//
41
Billing OpportunitiesMedicare Part A
• Governed by HOPPS regulations• Hospital bills• Billing codes: “facility fee” APC 5012, G0463• Chronic Care Management APC 5011, CPT 99490
Medicare Part B• Governed by PFS (Physician Fee Schedule) regulations• E&M codes
• “Incident to codes” 99211-99215 • TOC (Transition of Care) 99496, 99495• CCM (Chronic Care Management) 99490
• HCPC Level 2 codes• AWV (Annual Wellness Visits) G0438, G0439• Diabetes Education G0108, G0109
42
Billing Opportunities
Medicare Part C• Relationship/contracting with Commercial Payer
Medicare Part D• Relationship/contracting with PDP• MTM codes
Commercial or Private Payer• Like Medicare• Relationship/contracting

© 2016 by the American Pharmacists Association. All rights reserved.
43
Key Points
• Understanding the ontology of billing (language, definitions and their interrelationships) will greatly aid pharmacist providers of patient care services in understanding billing opportunities.
44
Identify the key billing decision makers and their influence on pharmacist
billing servicesSandra Leal, PharmD, MPH, CDE, FAPhA
Vice President for Innovation | SinfoniaRx
45
Disclosures• Sandra Leal declares no conflicts of interest, real or
apparent, and no financial interests in any company, product, or service mentioned in this program, including grants, employment, gifts, stock holdings, and honoraria.
The American Pharmacists Association is accredited by the Accreditation Council for Pharmacy Education as a provider of continuing pharmacy education.
46
Federal Policy Guidance
• Centers for Medicare and Medicaid Services (CMS)– Regulations: CMS periodically issues regulations
• Notice of Proposed Rulemaking (NPRM): Proposes policy and solicits public comment. All rules must be published in the Federal Register to notify the public and to give opportunity to comment.
• Interim Final Rule with Comment: Goes into effect when published but open for public comment for a specific period of time and then potentially revises and issues a Final Rule.
• Final Rule: Takes comments into consideration and formally codify policies that were proposed.
Source: Medicaid.gov; http://www.medicaid.gov/federal-policy-guidance/federal-policy-guidance.html
47
Medicare Parts
• Original Medicare– Part A: Hospital payment for inpatient, skilled nursing care, home
health care and hospice care– Part B: Medical insurance for doctors’ services, home health and
durable medical equipment
• Part D: Prescription drug coverage offered by private companies that have contracted with Medicare
• Medicare Supplement: Secondary health insurance policies offered by private companies to help pay for gaps
• Part C aka “Medicare Advantage”: A, B and sometimes D plus other benefits
Source: CMS; https://www.medicare.gov/sign-up-change-plans/decide-how-to-get-medicare/whats-medicare/what-is-medicare.html
48
Medicare Administrative Contractors (MACs)• CMS uses MACs
– To process Medicare claims
– Enroll health care providers in the Medicare program
– Educate providers on Medicare billing requirements
– Handle claims appeals
– Answer beneficiary and provider questions
– Section 1861 of the Social Security Act defines items and services for which Medicare “may” pay
Source, CMS; https://www.cms.gov/medicare/medicare-contracting/medicare-administrative-contractors/macjurisdictions.html

© 2016 by the American Pharmacists Association. All rights reserved.
49
Find Your MAC
Source: CMS; https://www.cms.gov/Research-Statistics-Data-and-Systems/Monitoring-Programs/Medicare-FFS-Compliance-Programs/Review-Contractor-Directory-Interactive-Map/#zpic
50
Resources
• Physician Fee Schedule (PFS)
– Physician Fee Schedule Look-Up Tool
– Link: https://www.cms.gov/apps/physician-fee-schedule/overview.aspx
• Medicare Learning Network– Education, information, and
resources for the health care professional community
• Articles• Web-Based Training• Calls and more
– Link: https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNGenInfo/index.html?redirect=/mlngeninfo
51
Source: CMS; https://www.cms.gov/Research-Statistics-Data-and-Systems/Monitoring-Programs/Medicare-FFS-Compliance-Programs/Review-Contractor-Directory-Interactive-Map/#zpic
52
Medicare versus Medicaid
• Medicare is a federal program that provides health coverage if you are 65 or older or have a severe disability, no matter your income.
• Medicaid is a state and federal program that provides health coverage if you have a very low income.
• If you are eligible for both Medicare and Medicaid (dual eligible), you can have both. Medicare and Medicaid will work together to provide you with very good health coverage.
53
Medicaid
• Medicaid: Jointly funded by the federal government and the state
• Federal government pays states for a specified percentage of program expenditures called the Federal Medical Assistance Percentage (FMAP)
• FMAPs adjusted every 3 years; range 50% to 75% with an average of 57%
• States can establish their own Medicaid provider payment rates within federal requirements
• States generally pay for services through fee-for-service or managed care arrangement
Source: Medicaid; http://www.medicaid.gov/medicaid-chip-program-information/by-topics/financing-and-reimbursement/financing-and-reimbursement.html
54
Medicaid Benefits
• States establish and administer their own Medicaid programs and determine the type, amount, duration and scope of services within the broad federal guidelines.
• Mandatory benefits are required
• Option benefits available like prescription drugs, physical therapy, podiatry services, dental services, etc.
Souce: Medicaid; http://www.medicaid.gov/medicaid-chip-program-information/by-topics/benefits/medicaid-benefits.html

© 2016 by the American Pharmacists Association. All rights reserved.
55
Medicare versus Commercial
• Medicare is designed to absorb risk
• Commercial is required to protect its business interests– Risk depends on contractual obligations, state laws
56
Local
• Compliance Officer/Billing Department
• Board
• Academia
• Physicians
57
2014 Payer Mix in the United States
Employer50%
Non-Group6%
Medicaid19%
Medicare13%
Other Public2%
Uninsured10%
PERCENTAGE
Source: The Henry J. Kaiser Family Foundation: http://kff.org/other/state-indicator/total-population/
58
Issues to Consider
• Medicare’s path to risk-based payment– Value-based contacts by 2018
– Transition 90% of any remaining fee-for-service Medicare payment to pay-for-performance
– Value-Based Purchasing, Readmission Reduction Programs, Bundling Payments are leading to more risk
59
Population Health
• Accountable Care Organizations
• Employee groups
• Medicare Advantage plans
• Commercial markets
60
Consumer-driven Health Care
• More cost to the consumer
• Higher deducible plans
• Providers and systems must win consumer interest– Ease of scheduling
– Online care options, urgent care
– Affordability

© 2016 by the American Pharmacists Association. All rights reserved.
61
Differentiators
• Clinical Quality– Better outcomes than competitors
• Service Experience– Strong brand reputation
– High patient satisfaction
62
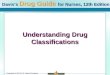
Source: eHealth, “Health Insurance Price Index Report for the 2015 Open Enrollment Period,” March 2015, available at: www.news.ehealthinsurance.com; HealthPocket.com, “2015 Obamacare Deductibles Remain High but Don’t Grow Beyond 2014 Levels,” November 20, 2014, available at: www.healthpocket.com; Advisory Board Company interviews and analysis.
Consumers Trade Low Premiums for High Deductibles
16% 16%
30%
39%
10%
23%
34% 34%
<$1,000 $1,000-$2,999 $3,000-$5,999 $6,000+
2014 2015
2015 Enrollees Favor Higher Deductibles
Annual Deductibles as Percentage of All Individual Plans Selected on eHealth Platform, 2014-2015
Average Public Exchange Deductibles by Tier, 2015
Bronze:
Silver:
Gold:
Platinum:
$5,181
$2,927
$1,198
$243
$5,081
$2,898
$1,277
$347
20142015
20142015
20142015
20142015
63
Billing CMS: Incident to Physician and Medication
Therapy Management
Gloria Sachdev, BS Pharm, PharmDPresident and CEO Employers’ Forum of Indiana
Clinical Assistant Professor, Purdue University College of Pharmacy
Adjunct Assistant Professor, Indiana University School of [email protected]
64
Disclosures• Gloria Sachdev declares no conflicts of interest, real or
apparent, and no financial interests in any company, product, or service mentioned in this program, including grants, employment, gifts, stock holdings, and honoraria.
The American Pharmacists Association is accredited by the Accreditation Council for Pharmacy Education as a provider of continuing pharmacy education.
65
Limited billing options as a
RECOGNIZED PROVIDER
Consider pharmacist billing options as an
Unrecognized Provider
66
Unrecognized Provider Billing Options Depend on 3 Factors
Service Provided
Payer Mix Practice Setting
Community-based
pharmacy clinic
Physician-based
outpatient clinic
Hospital -based outpatient clinic
Employer on-site
clinic for

© 2016 by the American Pharmacists Association. All rights reserved.
67
Learn Billing and Be Safe ll
Billing Options All of Michigan
except DetroitCPT billing codes Practice Setting
PB=physician based HB=hospital based
2016 Medicare Payment
Diabetes self-management training
G0108 (individual visit) G0109 (group visit)
all G0108 = $51.75G0109 = $13.91
CLIA-Waived Lab variable per POC test all fixed per CPT code
Medication Therapy Management (MTM)
99605, 99606, 99607 pharmacy, employer,health plan
variable per payer
Incident to physician: Office visit in a physician-based (aka, non-hospital) clinic
99211-99215 (PB) PB 99211 = $18.9999212 = $41.9799213 = $70.4499214 = $103.9799215 = $140.38
Incident to physician:Office visit in a hospital-based (aka, hospital outpatient clinic visit)
G0463 (HB) HB G0463 = $102.12
Incident to physician:Transitional Care Management (TCM) &RPh part of team
99496 (within 7d D/C)
99495 (within 14d D/C)PB & HB
99496 = $222.89 (PB) $157.30 (HB)_______99495 = $157.83 (PB) $108.72 (HB)
CMS Annual Wellness Visit (AWV)
G0438 (initial,once/lifetime)G0439 (subseq, annual)
PBHB
PB: G0438 = $166.02HB: G0439 = $111.88
Chronic Care Management (CCM)
99490 (20 minutes/month)
PBHB
PB: $39.37 monthlyHB: $30.80 monthly
69
How to look Up CMS Payment per CPT Codes Look up Professional Fee Payment Rates (determined annually, varies per region): • https://www.cms.gov/apps/physician-fee-schedule/license-agreement.aspx• Select first search option in web browser• Select “Accept”• Select PRICING INFORMATION; RANGE OF HCPCS CODES• Select SPECIFIC LOCALITY• Enter HCPC as “99211 - 99215” or any CPT code• Select modifier as “ALL MODIFIERS”; and select carrier/MAC locality (i.e.
Indiana • HIT SUBMIT
Look up Hospital Outpatient Prospective Payment (HOPPS) Facility Fee Payment Rates (determined annually, does not vary per region):
www.cms.gov/Medicare/Medicare‐Fee‐for‐Service‐Payment/HospitalOutpatientPPS/Addendum‐A‐and‐Addendum‐B‐Updates.html
• Select most recent date (i.e., January 2016)
• Under “related links,” select “Addendum B”
• Read and “Accept” the agreement to access the document
• Select Excel spreadsheet
• Search under “G0463 (the corresponding APC is 5012)
70
Hospital-Based Outpatient Clinic Incident to Physician
Setting: Physician outpatient clinic that is financially tied to a hospital (one tax ID number)
HospitalPhysician
Outpatient Clinic
71
Physician-Based Outpatient Clinic
Setting: Physician outpatient clinic that is NOT financially tied to a hospital (the physician group owns the practice under a separate business tax ID number)
Hospital Physician Outpatient Clinic
72
Key CMS Manual Regulations for Billing Incident to Physician
• Hospital Outpatient Services, Coverage of Outpatient Therapeutic Services Incident to a Physicians Services
– Medicare Benefit Policy Manual Chapter 6, Section 20.5.2
• https://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/bp102c06.pdf
• Services and Supplies Furnished Incident To a Physician’s/NPP’s Professional Service
– Medicare Benefit Policy Manual Chapter 15, Section 60.1
• https://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/bp102c15.pdf

© 2016 by the American Pharmacists Association. All rights reserved.
73
CMS Criteria-Billing Incident to Physician in a Hospital-Based Outpatient Clinic
1. Direct Supervision – physician or non-physician practitioner must :
• be present in the same building & immediately available• be prepared to step in and perform the service• “clinically appropriate” to supervise the service• NPP = nurse practitioner, physician assistant, clinical
nurse specialist, nurse midwife, clinical psychologist
2. Continued Physician-Patient Relationship• The patient must be an established patient• The physician must personally perform the initial service for each
new condition, make the initial diagnosis, and establish a plan of care which includes the subsequent incidental services
74
CMS Criteria-Billing Incident to Physician in a Hospital-Based Outpatient Clinic
3. Must be an integral though incidental part of a physician's or non-physician practitioner’s services
4. The services are of the type commonly rendered without charge or included in the physician’s bill
5. Of a type that are commonly furnished in physician’s offices or clinics
75
CMS Criteria-Billing Incident to Physician in a Hospital-Based Outpatient Clinic
6. Must be furnished on a physician’s or non-physician practitioner’s “order”
7. Must have employee relationship with hospital as an employee, leased employee, or independent contractor
8. Services provided are within the scope of practice for the pharmacist as dictated by the State pharmacy practice act
76
Facility Fee = Technical Fee
Every time a recognized provider sees a patient in a hospital-based outpatient
clinic
Bill a Professional Fee (PF) for cognitive services
by the physician group
Bill a separate Facility Fee (FF) from the hospital for use of the exam room, costs of lights, hospital
personnel resources, etc.
In a hospital-based outpatient clinic, incident to physician services provided by a pharmacist can be billed to Medicare via facility fee only. No professional fees
are billed to a payer unless a payer recognizes pharmacists as providers.
77
Hospital-Based Outpatient Clinic: How to Bill?
Using Facility Fee billing
• Fixed payment for outpatient services provided by a hospital• Single flat fee which is the same no matter
the region or length of visit• Similar concept to inpatient DRGs
• Facility Fees are overhead charges which are charged by a hospital for utilizing hospital resources to support practitioner services
78
2016 CMS Facility Fee-Only Billing
CPT G-0463 billing code goes on the CMS 1450 (aka UB-04) billing claim to Medicare
The payment from Medicare is received in the form of an APC code, APC 5012 = $102.12
Patient co-pay is $20.43
Effective January 1, 2016

© 2016 by the American Pharmacists Association. All rights reserved.
79
Case Example Pro Forma: Hospital-Based Outpatient Clinic
Payer Mix
Medicare 70%
Medicaid 15%
Commercial 10%
Self-Pay 5%
Self-Insured Employer 0%
80
Case Example continued
• New pts are seen for 60 minutes• Follow-up pts are seen for 30
minutes
Clinic structure for pharmacist-
managed BMT clinic
• Schedule 1 new pt and 6 follow-up pts per ½ day clinic
Established clinic defined as 3
months from start date
• 1 week closed for holidays• 2 pharmacists each working 0.5
FTE
Clinic has pharmacist
coverage for 51 weeks
81
Case Continued: Financial Revenue Opportunity Billing Incident to Physician in a Hospital-Based Outpatient Clinic
Revenue projection for established pharmacist BMT in Michigan (except Detroit) clinic using FACILITY FEE‐ONLY BILLING. (This does not apply to physician‐based billing!)
•For ½ day clinic/wk (0.1 FTE) = 7 visits •For 5 days/wk (1.0 FTE) = 7 visits X 10 = 70 visits/wk X 51wks/yr = 3,570 visits/year max
•Assuming 10% of patient no‐show for visits = 3,213 visits
Payer Mix for 3,213 visits Facility Fee Sub‐Total
•Medicare 70% = 2,249 bill G0463 $102.12 $229,668
•Medicaid 15% = 482 bill 99212 facility fee avg $36.00 $17,352
Commercial 10% = 321 bill 99212 facility fee avg $75.00 $24,075
Self‐Pay 5% = 160 bill 99212 facility fee avg $0.00 $0.00___
TOTAL Revenue $271,095
82
Physician-Based Outpatient Clinic
Setting: Physician outpatient clinic that is NOT financially tied to a hospital (the physician group owns the practice under a separate business tax ID number)
HospitalPhysician Outpatient Clinic
83
CMS Physician-Based Outpatient Clinic Rules
• Pertains to Auxiliary Personnel who may be an employee, leased employee, or independent contractor of the physician….thus, must be a direct financial expenseto the physician or non-physician practitioner (NPP)
• Direct Supervision definition is different: physician or NPP must be in same “suite”
All prior Incident-to Physician
Rules apply, in addition
to:
84
CMS Physician-Based Outpatient Clinic Rules2016 Physician Fee Schedule – clarification noted in the background section regarding billing incident to physician by auxiliary personnel. It is clearly stated that the supervising provider should bill and get paid for incident to services provided by auxiliary personnel just as if the supervising provider were personally providing the service. Thus, pharmacists meeting all the incident to criteria and documentation criteria can have their services billed for using CPT 99211-99215 and paid at 100% the physician rate (or 85% of the NPP rate, if a NPP is supervising).
• Final Rule Posted in official Federal Registrar 11-16-15
– http://www.gpo.gov/fdsys/pkg/FR-2015-11-16/pdf/2015-28005.pdf
• Pages 71065-71068 and 71372

© 2016 by the American Pharmacists Association. All rights reserved.
85
Financial Revenue Opportunity billing Incident to Physician in a Physician-Based Outpatient Clinic
Revenue projection for established pharmacist clinician in a BMT clinic in Michigan (except Detroit). Bill using CPT 99211-99215 incident to physician for all payers. Can not bill 99211-99215 under pharmacist NPI unless recognized as a provider by a payer, for which payment would likely be 85% of MD rate.
• For ½ day clinic/wk (0.1 FTE) = 7 visits • For 5 days/wk (1.0 FTE) = 7 visits X 10 = 70 visits/wk X 51wks/yr =
3,570 visits/year max• Assuming 10% of patient no-show for visits = 3,213 visits
Payer Mix for 3,213 visits Reimbursement Sub-Total• Medicare 70% = 2,249 bill 99212 $41.97 $94,391• Medicaid 15% = 482 bill 99212 $15.00-guess $7,230• Commercial 10% = 321 bill 99212 $50.00-guess $16,050• Self-Pay 5% = 160 bill 99211 $0.00 $0.00___
TOTAL Revenue $117,671
86
Medicare Part D: Medication Therapy Management Program (MTMP)
As part of the 2003
Medicare Modernization Act (MMA),
Pharmacists as of Jan 1st 2006 are permitted for the first time to bill for
COGNITIVE SERVICES!
87
MTM Definition per CMS
A patient-centric and comprehensive approach to improve medication use, reduce the risk of adverse events, and improve medication adherence. Therefore, the programs include high-touch interventions to engage the beneficiary and their prescribers.
https://www.cms.gov/Medicare/Prescription-Drug-Coverage/PrescriptionDrugCovContra/Downloads/Memo-Contract-Year-2016-
Medication-Therapy-Management-MTM-Program-Submission-v-040715.pdf 88
Criteria Part D Sponsors Must Establish for their MTM Program
Effective Jan 1, 2016
Annualcomprehensive
medication review (CMR)
Quarterly targeted medication reviews (TMRs) with follow-
up interventions when necessary
Must auto-enroll (pt can opt-out)
MAY be furnished by a pharmacist or other
qualified provider
MAY distinguish between services in
ambulatory and institutional settings
MUST be developed in cooperation with
licensed & practicing pharmacists &
physicians
https://www.cms.gov/Medicare/Prescription-Drug-Coverage/PrescriptionDrugCovContra/Downloads/Memo-Contract-Year-2016-
Medication-Therapy-Management-MTM-Program-Submission-v-040715.pdf
89
Minimum Requirements that can be set by a Prescription Drug Plan
Minimum Threshold Criteria for MTM
2-3 chronic health conditions
If PDP opts to target by chronic disease, then must have 5 of 9 core
chronic conditions
2-8 Part D meds Likely to incur Part D drug costs > $3,507
90
Changes from 2015 to 2016 CMS MTMP
1. Under the Provider of MTM Services, sponsors will now be able to select Pharmacy Intern Under Direct Supervision of a Pharmacist or Pharmacy Technician, if applicable.
2. Under Qualified Provider of Interactive, Person-to-Person CMR with written summaries, sponsors will now be able to select Disease Management Pharmacist and Pharmacy Intern Under Direct Supervision of a Pharmacist, if applicable.
3. Annual cost threshold = $3,507 (2015 = $3,138)

© 2016 by the American Pharmacists Association. All rights reserved.
ll
Billing Options All of Michigan
except DetroitCPT billing codes Practice Setting
PB=physician based HB=hospital based
2016 Medicare Payment
Diabetes self-management training
G0108 (individual visit) G0109 (group visit)
all G0108 = $51.75G0109 = $13.91
CLIA-Waived Lab variable per POC test all fixed per CPT code
Medication Therapy Management (MTM)
99605, 99606, 99607 pharmacy, employer,health plan
variable per payer
Incident to physician: Office visit in a physician-based (aka, non-institutional) clinic
99211-99215 (PB) PB 99211 = $18.9999212 = $41.9799213 = $70.4499214 = $103.9799215 = $140.38
Incident to physician:Office visit in a hospital-based (aka, institutional) outpatient clinic
G0463 (HB) HB G0463 = $102.12
Incident to physician:Transitional Care Management (TCM) &RPh part of team
99496 (within 7d D/C)
99495 (within 14d D/C)PB & HB
99496 = $222.89 (PB) $157.30 (HB)_______99495 = $157.83 (PB) $108.72 (HB)
CMS Annual Wellness Visit (AWV)
G0438 (initial,once/lifetime)G0439 (subseq, annual)
PBHB
PB: G0438 = $166.02HB: G0439 = $111.88
Chronic Care Management (CCM)
99490 (20 minutes/month)
PBHB
PB: $39.37 monthlyHB: $30.80 monthly
92
Medication Therapy Management (MTM) CPT Codes
99605 (Prior 0115T): new patient, face-to-face• Initial 15 minutes
99606 (Prior 0116T): established patient, face-to-face• Initial 15 minutes
99607 (Prior 0117T): face-to-face• For each additional 15 minutes• Used only in addition to 99605 or 99606 • List separately
93
How To Use MTMP Codes?
Case 1: New Patient Visit = 45 min
Case 2: Follow-Up Patient Visit = 30 min
94
CMS Innovation Center testing new MTM Payment Model• Part D Enhanced Medication Therapy Management (MTM)
model will test whether providing Part D sponsors with additional payment incentives will lead to improving therapeutic outcomes, while reducing net Medicare costs.
• Begins January 1, 2017 with a 5 year performance period.
• Testing new payment model: per member per month (PMPM) base, plus performance-based incentive payment set at $2.00 PMPM
https://innovation.cms.gov/initiatives/enhancedmtm/
95
CMS Innovation Center testing new MTM Payment Model• Health Plans who apply must:
(a) be an individual market stand-alone basic plan
(b) have a minimum enrollment of 2,000
(c) have existed as a basic plan for at least 3 years
(d) not be under sanction by CMS or law enforcement
(e) rank at least 3-Star (case by case basis if < 3 Star)
96
CMMI Enhanced MTM model
11 States will participate: Virginia, Florida, Louisiana, Iowa, Minnesota, Montana, Nebraska, North Dakota, South Dakota, Wyoming, and Arizona

© 2016 by the American Pharmacists Association. All rights reserved.
97
References
NACDS White Paper
Oct 2015
http://avalere-health-production.s3.amazonaws.com/uploads/pdfs/1446827136_102915_Avalere_NACDS_WhitePaper_LP_04.pdf
www.pharmacist.com/sites/default/files/files/mtm_billing_tips.pdf
APhA MTM Tips for Pharmacists
98
Additional References
G-Code 2014: Hospital-Based Outpatient Clinic Facility Fee PaymentAvailable at the American Society of Health-System Pharmacist bookstore
Kliethermes MA, Brown TR, eds. Building a successful ambulatory care practice: a complete guide for pharmacists. Bethesda, MD: American Society of Health-System Pharmacists; 2012
99
CPT Codes are:
A. Level 1 HCPC (Healthcare Common Procedure Coding System) codes
B. Codes that include the “incident to” Evaluation & Management codes which providers may use to support pharmacist services
C. Used by Medicare Part B for billing purposes
D. Adjusted by the Resource-based Relative Value Scale (RBRVS)
E. All of the above
100
APC (Ambulatory Payment Classifications) Codes are used in which setting?
• Hospitals or health-systems for “facility fee” services in their ambulatory clinics
• Physician offices for diabetes education services
• Assisted living and group homes for clinical provider services
• For in-home services provided by Medicare Part B providers
101
Which one of the following statements is NOT a CMS criteria for billing incident to physician in a hospital-based outpatient clinic?
A. Must have an order/referral
B. Must have Direct Physician Supervision
C. Must have a continued physician relationship
D. Must be considered a recognized provider
102
Which of the following is a TRUE Statement?
A. MTM CPT codes can be billed under Medicare Part B
B. MTM CPT codes can be billed under Medicare Part D
C.MTM is required by Medicare to be provided by pharmacists
D.MTM is an “opt-in” requirement of Medicare prescription drug plans

© 2016 by the American Pharmacists Association. All rights reserved.
103
What are key opportunities for pharmacists to comment on impending Medicare rules?
A. There is never an opportunity for pharmacists to comment on rules.
B. During the Notice of Proposed Rulemaking
C. During the Interim Final Rule
D. After the Final Rule is implement
Billing Boot Camp II
Mary Ann Kliethermes, BS Pharm, PharmD
Sandra Leal, PharmD, MPH, FAPhA, CDE
Gloria Sachdev, BS Pharm, PharmD106
Billing Boot Camp II: Advanced Training
107
Disclosures• Mary Ann Kliethermes is co-owner of Clinical pharmacy
Systems Inc.
• [INSERT FACULTY NAME(S)] [INSERT THE FOLLOWING TEXT IF NO CONFLICTS EXIST: “declare(s) no conflicts of interest, real or apparent, and no financial interests in any company, product, or service mentioned in this program, including grants, employment, gifts, stock holdings, and honoraria.” OR LIST THE CONFLICTS ]
The American Pharmacists Association is accredited by the Accreditation Council for Pharmacy Education as a provider of continuing pharmacy education.
108
• Target Audience: Pharmacists
• ACPE#: 0202-0000-16-013-L04-P
• Activity Type: Knowledge-based

© 2016 by the American Pharmacists Association. All rights reserved.
109
Learning Objectives• Describe the opportunities and billing requirements for
Diabetes Self-Management Training services.
• Describe the opportunities and billing requirements for pharmacists to participate in Medicare Annual Wellness Visits, Transitional Care Management, and Chronic Care Management services.
• Identify quality and outcome measures tied to performance payment in both fee-for-service and new care model payment strategies that can be impacted by pharmacists’ services.
• Discuss how to leverage pharmacist skills and services to design practice models that provide value in new payment models.
110
Diabetes Self-Management can be billed:
A. Any site that provides the services
B. A site accredited by AADE or ADA
C. Any providers as long as they have are a Certified Diabetes Educator (CDE)
D. On the same day they see another provider at a Federally Qualified Health Center
111
You are providing pharmacy patient care services in a primary care practice whose patient population payment source is 70% Medicare Advantage. Which of the following value based performance measures should you focus on to prove the value of your patient care services?
A. ACO 33 measures
B. HEDIS measures
C. STAR Measures
D. Hospital readmission rates
E. Universal Data Set
112
Medication Adherence measures are used in which Medicare Programs
A. Medicare Advantage and Medicare Part D prescription plans
B. Federally Qualified Health Centers and Accountable Care Organizations
C. Medicare Part D prescription plans only
D. Medicare Advantage, Medicare Part D and Health Insurance Marketplace
113
What is the FIRST step in developing a sustainable business plan,?
A. Provide a service that you like to provide.
B. Meet referring physicians and see what services they suggest.
C. Conduct a needs assessment
D. Ascertain billing options
114
Describe the opportunities and billing requirements for Diabetes Self-Management Training (DSMT) services
Sandra Leal, PharmD, MPH, CDE, FAPhA
Vice President for Innovation | SinfoniaRx

© 2016 by the American Pharmacists Association. All rights reserved.
115
Disclosures• Sandra Leal declares no conflicts of interest, real or
apparent, and no financial interests in any company, product, or service mentioned in this program, including grants, employment, gifts, stock holdings, and honoraria.
The American Pharmacists Association is accredited by the Accreditation Council for Pharmacy Education as a provider of continuing pharmacy education.
116
To bill the Medicare Part B program for DSMT, a number of key elements must be in place.
The DSMT Program must have:– Accreditation from AADE or ADA
– A partnership with a provider that can bill Medicare
The beneficiary must have: – A diabetes diagnosis
– A written referral for DSMT
Source: The CMS Health Disparities Pulse Resource Center; http://www.cmspulse.org/resource-center/health-topics/diabetes/documents/DSME-Toolkit.pdf
117
Accreditation Considerations
American Diabetes Association (ADA)
American Association of Diabetes Educators (AADE)
First site: $1,100 1 to 10 sites: $800
Additional sites: $100 each 11 to 20 sites: $1200
Same fee for renewal 20 sites: Contact AADE
Valid for 4 years Same fee for renewal
Annual status report required Valid for 4 years
Status update and annual reports
5% of recognized sites audited 10% of recognized sites audited
118
DSMT First Year
Codes Description Allowable Units
G0108 • Individual DSMT• Medicare allows for 1 hour• Billable in 30 minute
increments (1 unit)
2 units = 1 hour
G0109 • Group DSMT• 2 or more participants• Medicare allows 9 hours• Billable in 30 minutes
increments (1 units)
18 units = 2 hours
*CPT Codes that may be accepted by private insurers: 98960, 98961, 98962
Source: AADE, https://www.diabeteseducator.org/docs/default-source/legacy-docs/_resources/pdf/general/Diabetes_Services_Order_Form_Backgrounder__Final.pdf
119
DSMT Subsequent Years After Initial Year
Codes Description Allowable Units
G0108/G0109 • Medicare allows for any combination of 2 hours
• Billable in 30 minute increments (1 unit)
4 units = 4 hour
Source: AADE, https://www.diabeteseducator.org/docs/default-source/legacy-docs/_resources/pdf/general/Diabetes_Services_Order_Form_Backgrounder__Final.pdf
120
Codes 2015 Medicare Fee Schedule
G0108 (individual) 1 unit (30 minutes): $46.46 - $71.06
G0109 (group) 1 unit (30 minutes): $12.57 - $19.20
Source: HSAG: https://www.hsag.com/contentassets/051dd35e6100416db6b5bef77987e663/dsme_dsmt_crosswalk_20150303.pdf
Billing Codes

© 2016 by the American Pharmacists Association. All rights reserved.
121
Reimbursement Example
G0108: Individual visit
$48.46 X 2 units X 8 patients = $775.36/ (8 hour day)
G0109: Group visit
$12.05 X 4 units X 8 patients = $385.60 (2 hour class)
*FQHCs can only bill G0108; not on the same day as a provider visit
122
Source: AADE, https://www.diabeteseducator.org/docs/default-source/legacy-docs/_resources/pdf/general/Diabetes_Services_Order_Form_v4.pdf
123
Describe the opportunities and billing requirements for pharmacists to participate in Medicare Annual
Wellness Visits, Transitional Care Management Services, and Chronic
Care Management
Sandra Leal, PharmD, MPH, CDE, FAPhA
Vice President for Innovation | SinfoniaRx
124
Initial Preventative Physical Exam (IPPE) and Annual Wellness Visits (AWV)
• CMS added IPPE and AWV codes to the physician fee schedule in 2011
125
Initial Preventative Physical Exam (IPPE) and Annual Wellness Visits (AWV)
Visit Type Frequency Billing Elements
Welcome to Medicare (IPPE)
Within first 12 months of initial Medicare Part B coverage
• Only primary care provider can bill
•No copay/coinsurance
• History: Medical and social,screening for depression/mood disorders, functional ability and safety evaluations
• Examination: Assessment and end-of-life planning
• Counseling and Education: Including written plan
126
Visit Type Frequency Billing Elements
Initial Annual Wellness Visit
Not within first 12 months of initial Medicare Part B coverage
• Pharmacist“incident to” a provider request*
• No copay/coinsurance
• History: Same asIPPE
• Examination: Same as IPPE but no mention of end-of-life planning, list of current healthcare providers and suppliers
• Counseling and Education: Written screening schedule, interventions and health advise, referral to health education and preventive counseling services
*FQHCs do not utilize “incident to” for this service as they reimburse with the Prospective Payment System (PPS) therefore pharmacists can not initiate an AWV as they are not recognized providers in an FQHC.

© 2016 by the American Pharmacists Association. All rights reserved.
127
Key Points
• Prevention visits, not an annual physical
• Separate evaluation and management (E/M) and medically necessary services can be billed at the same time as an IPPE or AWV with a modifier - 25
128
Billing Codes
Codes Billing Code Descriptors Non-Facility Price
G0438 AWV; includes a personalized prevention plan of service (PPPS), initial visit
~$174.28
G0439 AWV, includes a personalized prevention plan of service (PPPS), initial visit, subsequent visit
~$117.86
Source: CMS, https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/downloads/AWV_chart_ICN905706.pdf
129
Implementation considerations…
• Time burden
• Recruitment of patients
• FQHC issues
130
Transitional Care Management (TCM) Services• CMS added TCM codes to the physician fee schedule in
2013– 99495 and 99496
• Complex requirements
131
Who Qualifies
Inpatient Setting Community Setting
Acute Care Hospital Home
Psychiatric Hospital Domiciliary
Long Term Care Hospital Rest Home
Skilled Nursing Facility Assisted Living
Rehabilitation Facility
Hospital Outpatient Observation or Partial Hospitalization
Partial Hospitalization at a Community Mental Health Center
Source: Medicare Learning Network. Transitional Care Management Services. 2013; ICN908628
132
Requirements
• Within 2 business days of discharge, contact with patient or caregiver.
• If unsuccessful, document 2 attempts.
• General supervision “incident to” applies; same location requirement at same time not necessary

© 2016 by the American Pharmacists Association. All rights reserved.
133
Things to know…
• Physician
• Non-physician practitioners (NPP): certified midwives, clinical nurse specialists, nurse practitioners, physician assistants
• Claim submission must be 30 days from discharge date
• Not paid if patient is readmitted before the 30 days
134
Things to consider…
• Can be performed ”incident to” with general supervision
135
Where do you fit in?
• Can provide the non face-to-face components
• Mandatory medication reconciliation requirement
• Other elements in team-based care
136
Face-to-face codes
• 99495
• Moderate medical decision making
• Within 14 days of discharge
• 99496
• High medical decision making
• Within 7 days of discharge
137
Billing Codes
Codes Non-Facility Price
99495 $166.37
99496 $233.57
Source: CMS, https://www.cms.gov/apps/physician-fee-schedule/
138
Implementation considerations…
• Identification of patients being discharged from hospitals
• Difference in claim submission dates

© 2016 by the American Pharmacists Association. All rights reserved.
139
Chronic Care Management (CCM)
• Introduced January 2015 Physician Fee Schedule• As of 11/15 only 26% of eligible providers had launched
CCM programs• 23% intended to do so in the next 12 months• 11% had no plans to participate in the next 12 months• Early struggles:
– Physician engagement– Patient education– Efficient processes– Regulatory compliance
Source: The National Chronic Care Management Survey, http://www.pyapc.com/chronic-care-management-survey-released/
140
Who Qualifies?
Source, CMS: https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/Downloads/ChronicCareManagement.pdf
Chronic Care Management Service
Multiple (2 or more) chronic conditions expected to last 12 months, or until the death of a patient
Chronic condition that places the patient at significant risk of death, acute exacerbation/decompensation or functional decline,
Comprehensive care plan established, implemented, revised or monitored.
141
Practitioners Eligible
• Physicians• Non-physician practitioners (NPP)
– Certified Nurse Midwives– Clinical Nurse Specialists– Nurse Practitioners– Physician Assistants
142
Requirements
• Patient Agreement– Patient Consent
• Inform the patient of the availability of the CCM service and obtain written agreement to have the services provided, including authorization for the electronic communication of medical information with other treating practitioners and providers
• Explain and offer the CCM service to the patient. In the patient’s medical record, document this discussion and note the patient’s decision to accept or decline the service
• Explain how to revoke the service.
• Inform the patient that only one practitioner can furnish and be paid for the service during a calendar month
• Cost-sharing
143
Requirements
• Scope of Services Elements– Structured Data Recording using a certified EHR
– Comprehensive Care Plan
– Access to Care: Ensure 24/7 access
144
Things to consider…
• Can be performed ”incident to” with general supervision

© 2016 by the American Pharmacists Association. All rights reserved.
145
Key Points
• A sustainable practice will likely require the use of several of these codes
• Know your payer mix
• Consider front end and back end payments based on a blend of different contracts
• Negotiation is constant with internal and external players
• Stay informed
146
Who are you beholding to?
Choosing Quality Measures
Mary Ann Kliethermes, BS Pharm, PharmD
Vice-Chair, Professor
Chicago College of Pharmacy
Midwestern University
147
Learning Objective
• Identify quality and outcome measures tied to performance payment in both fee-for-service and new care model payment strategies that can be impacted by pharmacists’
148
Triple AimReducing per-capita costs
Better health for populations
Better care for individuals
Health Care
Reform
149
CMS Quality Strategy 2016
• Goal 1: Make care safer by reducing harm caused in the delivery of care.
• Goal 2: Strengthen person and family engagement as partners in their care.
• Goal 3: Promote effective communication and coordination of care.
• Goal 4: Promote effective prevention and treatment of chronic disease.
• Goal 5: Work with communities to promote best practices of healthy living.
• Goal 6: Make care affordable.
http://www.ahrq.gov/workingforquality/agencyplans/2016-cms-agency-specific-plan.pdf
150
IOM Vital Signs Core MeasuresMeasuring what matters to patients
Am I healthier? Do I feel better to the level where I can
function as I desire?
Did your care make me sicker?
Can I reach you when I need you?
Can I afford this
care?

© 2016 by the American Pharmacists Association. All rights reserved.
151
Whose measures should we care about?
Federal Medicare
Part A
Part B
Part C
Part D
State
Medicaid
Insurance exchanges
Commercial or Private
Employer based
Group
Individual
152
Medicare Part AHospital Readmissions Reduction Program’’ (ACA)
• ‘‘Base operating DRG payments’’ are reduced by a hospital-specific adjustment factor that accounts for the hospital’s excess readmissions
• ‘‘Excess readmissions ratio’’ - risk-adjusted readmissions based on actual readmissions
• Look up: http://cdn.kaiserhealthnews.org/attachments/MedicareReadmissionPenaltiesByHospital,Year4.pdf
153
Hospital Readmission Program (ACA)
Conditions that apply• AMI• HF • Pneumonia• Chronic obstructive pulmonary disease (COPD)• Elective primary total hip and/or total knee arthroplasty (THA/TKA)• Coronary Artery Bypass Graft (CABG) - in 2017
Penalties• 0 to 3%• In 2016 - 2,592 hospitals will receive lower payments for every Medicare patient
that stays in the hospital • Rural, non-teaching, less than 100 beds fair the worst
154
Medicare Part B: Fee for Service
• Physician Quality Reporting System (PQRS)– https://www.cms.gov/medicare/quality-initiatives-patient-
assessment-instruments/pqrs/measurescodes.html
• Meaningful Use– https://www.cms.gov/Regulations-and-
Guidance/Legislation/EHRIncentivePrograms/2016ProgramRequirements.html
155https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/PQRS/index.html 156

© 2016 by the American Pharmacists Association. All rights reserved.
157
Stage 2 Meaningful Use (2015-2017)
Protect Patient Health Information
Clinical Decision Support
CPOE
Electronic Prescribing (eRx)
Health Information Exchange
Patient Specific Education
Medication Reconciliation
Patient Electronic Access (VDT)
Secure Messaging (EPs only)
Public Health and Clinical Data Registry Reporting
Medication Reconciliation:medication reconciliation for more than 50 percent of transitions of care in which the patient is transitioned into the care
Public Health and Clinical Data Registry Reporting:
(immunization and others)
158
Stage 3 Meaningful Use (2018)
Protect Electronic Health Information
Electronic Prescribing (eRx)
Clinical Decision Support
Computerized Provider Order Entry (CPOE)
Patient Electronic Access to Health Information
Coordination of Care through Patient Engagement
Health Information Exchange
Public Health Reporting .
https://www.cms.gov/eHealth/downloads/Webinar_eHealth_May11_ONCStage3.pdf
159
Medicare Shared Savings ACO
434 ACOs in 49 states as of 2016
• 100 new for 2016
Showed improvement in 27 of the 33 measures
18 of the 22 measures that are similar are in the PQRS, the Shared Savings ACO had better results
28% held spending below targets
• 37% if an ACO since 2012
John Pilotte, Dir. Performance-Based Payment Policy Group, CMSAPM Framework Webinar, HCPLAN Payment Network 1/12/16
160
ACO–33 Quality MeasuresPatient Experience - 7 measures CAHPS
• Education
Care Coordination and Patient Safety - 6 measures• Hospital readmissions• Admissions for COPD and Heart Failure • Med reconciliation
Preventive Health – 8 measures• Pneumococcal and Influenza vaccination• Obesity, Smoking• Depression, BP
At Risk Populations – 12 measures• DM: HgA1c, LDL, BP, ASA, smoking• HTN: BP• Ischemic Vascular Dx (IVD): LDL, ASA or anti-thrombotic• HF: beta-blocker• CAD: LDL lowering, ACE/ARB
https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/sharedsavingsprogram/Downloads/ACO_Quality_Factsheet_ICN907407.pdf
161
Federally Qualified Health Centers
FQHCs are “safety net” providers such as community health centers, public housing centers, outpatient health programs funded by the Indian Health Service, and programs serving migrants and the homeless
162
Universal Data Set – HRSA
Adult weight screening (BMI) and follow up
Tobacco use and cessation
Appropriate Asthma therapy
Lipid lowering therapy for CAD
ASA for AMI, CABG, PTCA or IVD
http://www.bphc.hrsa.gov/datareporting/reporting/2015udsmanual.pdf

© 2016 by the American Pharmacists Association. All rights reserved.
163
Medicare Part C “Medicare Advantage”Medicare Part D “Prescription Drug Plan
• Rules based on CMS Call letter (every spring)
• Quality determined by Star Measures
164
Star Ratings CMS: Plan Evaluation
Part C Domains1. Staying healthy –
prevention
2. Managing Chronic Conditions
3. Member experience
4. Member complaints and changes in performance
5. Customer Service
Part D Domains1. Drug plan customer
service
2. Complaints, access problems and improvement
3. Member Experience
4. Drug Pricing and Patient Safety
http://www.cms.gov/Medicare/Prescription-Drug-Coverage/PrescriptionDrugCovGenIn/index.html?redirect=/PrescriptionDrugCovGenIn/06_PerformanceData.asp
Ratings displayed as 1-5 stars1.★ = poor performance
2.★★ = below average performance3.★★★ = average performance
4.★★★★ = above average performance5.★★★★★ = excellent performance
165
Star ratings – cut points/bonus
http://www.cms.gov/Medicare/Prescription-Drug-overage/PrescriptionDrugCovContra/Downloads/Announcement2012final.pdfhttp://www.cms.gov/Medicare/Health-Plans/MedicareAdvtgSpecRateStats/Downloads/Advance2015.pdf
Star Rating QBP Percentage for 2012/2013
QBP Percentagefor 2014
QBP Percentage for 2015
QBPPercentage For 2015
Less than 3 stars
0% 0% 0% 0%
3 stars 3% 3% 0% 0%
3.5 stars 3.5% 3.5% 0% 0%
4 stars 4% 4% 5% 5%
4.5 stars 4% 5% 5% 5%
5 stars 5% 5% 5% 5%
166
Measures to Care About – Medicare C
Staying Healthy: Screenings, Tests and Vaccines
• C01 - Breast Cancer Screening • C02 - Colorectal Cancer Screening • C03 - Annual Flu Vaccine • C04 - Improving or Maintaining Physical Health• C05 - Improving or Maintaining Mental Health• C06 - Monitoring Physical Activity• C07 - Adult BMI Assessment
https://www.cms.gov/Medicare/Prescription-Drug-Coverage/PrescriptionDrugCovGenIn/Downloads/2017-Star-Ratings-Request-for-Comments.pdf
167
Measures to Care About – Medicare C
Managing Chronic (Long Term) Conditions
• C01 - SNP Care Management• C09 - Care for Older Adults – Medication Review• C10 - Care for Older Adults – Functional Status Assessment• C11 - Care for Older Adults – Pain Screening• C12 - Osteoporosis Management in Women with a Fracture• C13 - Diabetes Care – Eye Exam• C14 - Diabetes Care – Kidney Disease Monitoring• C15 - Diabetes Care – Blood Sugar Controlled• C16 - Controlling Blood Pressure• C17 - Rheumatoid Arthritis Management• C18 - Reducing the Risk of Falling• C19 - Plan All-Cause Readmissions
168
Measures to Care About – Medicare C
Member Experience with Health Plan
• C20 - Getting Needed Care• C21 - Getting Appointments & Care
Quickly• C22 - Customer Service• C23 - Rating of Health Care Quality• C24 - Rating of Health Plan• C25 - Care Coordination.

© 2016 by the American Pharmacists Association. All rights reserved.
169
Measures to Care About – Medicare DDrug Safety and Accuracy of Drug Pricing
•
• D10 - MPF Price Accuracy• D11 - High Risk Medication• D12 - Medication Adherence for Diabetes
Medications• D13 - Medication Adherence for Hypertension
(RAS Antagonists)• D14 - Medication Adherence for Cholesterol
(Statins)• D15 - MTM Program Completion Rate for CMR
170
State: Health Insurance Marketplace or State ExchangesState’s subsidized health insurance for those without
Assistance for small businesses “the SHOP” (Small Business Health Options Program
Cost assistance for those at 400% FPL
https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/QualityInitiativesGenInfo/Downloads/2016-QRS-Measure-Technical-Specifications.pdfhttp://obamacarefacts.com/state-health-insurance-exchange/
171
States Status in the Marketplace
http://www.commonwealthfund.org/interactives-and-data/maps-and-data/state-exchange-map172
NCQA (HEDIS) Measures• Adult BMI Assessment
• Annual Monitoring for Patients on Persistent Medications
• Antidepressant Medication Management
• Avoidance of Antibiotic Treatment in Adults with Acute Bronchitis
• Comprehensive Diabetes Care: Eye Exam (Retinal)
• Comprehensive Diabetes Care: Hemoglobin A1c (HbA1c) Control (<8.0%)
• Comprehensive Diabetes Care: Hemoglobin A1c (HbA1c) Testing
• Comprehensive Diabetes Care: Medical Attention for Nephropathy
173
NCQA (HEDIS) Measures• Controlling High Blood Pressure
• Follow-Up After Hospitalization for Mental Illness (7-Day Follow-Up)
• Follow-Up Care for Children Prescribed ADHD Medication
• Human Papillomavirus Vaccination for Female Adolescents
• Immunizations for Adolescents (Combination 1)
• Initiation and Engagement of Alcohol and Other Drug Dependence Treatment
• Medication Management for People With Asthma (75% of Treatment Period)
• Plan All-Cause Readmissions
174
Pharmacy Quality Alliance Measures
Medication Adherence for Diabetes Medications
Medication Adherence for Hypertension (RAS Antagonists)
Medication Adherence for Cholesterol
PDC = Proportion of Days Covered

© 2016 by the American Pharmacists Association. All rights reserved.
175
State and Commercial Payers
Variable
May be contractual
Commercial primarily HEDIS Measures• NCQA National Committee for Quality Assurance
• Accreditor for Health Insurance Companies and Physicians• HEDIS Healthcare Effectiveness Data and Information Set
• 81 measures• 5 domains
176
Example of a Commercial Payer• Upper Eastern NY Health Plan
• Use a risk adjusted global payment at 40% above the typical FFS payment
• 20% bonus based on triple aim– 4 categories of HEDIS measures
– CHAPS survey
– Utilization measures
• Hospitalization, ER visits
• Medication use
• Lab and imaging use
• Specialists
– Netted $17 PMPM for 2014
Eileen Wood from Capital District Physicians' Health Plan APM Framework Webinar, HCPLAN Payment Network 1/12/16
177
Key Points
• Choose measures that matter to PATIENTS!
• Keep in mind national quality goals
• What quality measures you should focus on DEPENDS!
• Who are you doing business with?
• Who is paying the bill for the patients you are seeing?
178
Value Proposition Considerations
Gloria Sachdev, BS Pharm, PharmDPresident and CEO Employers’ Forum of Indiana
Clinical Assistant Professor, Purdue University College of Pharmacy
Adjunct Assistant Professor, Indiana University School of [email protected]
179
Disclosures
Gloria Sachdev declares no conflicts of interest, real or apparent, and no financial interests in any company, product, or service mentioned in this program, including grants, employment, gifts, stock holdings, and honoraria.
The American Pharmacists Association is accredited by the Accreditation Council for Pharmacy Education as a provider of continuing pharmacy education.
180
Objective
Discuss how to leverage pharmacist skills and
services to DESIGN practice models that provide VALUE
in new payment models

© 2016 by the American Pharmacists Association. All rights reserved.
Strategic Plan for SustainabilityConduct an Environmental Scan - focusing on a Needs Assessment
Conduct a SWOT Analysis
Conduct a Gap Analysis and Feasibility Analysis
Consider Financial Opportunities
Consider Interest of Stakeholders - Send Out The Feelers
Develop a Business Plan
Implement the Service • Billing• Legal• Operations• Policy & Procedures
Measure Outcomes! 182
CMS Provides Financial Incentives to achieve the Triple Aim: Improve Care, Improve Quality, and Reduce Costs
ACOAccountable Care Org
HRRP Hospital
Readmission Reduction
Program
VBPValue Based
Purchasing
HAC Hospital Acquired Conditio
n Reductio
n Program
MU Meaningful Use of the
Electronic
Medical Record
PQRS Physician
Quality Reporting System
PCMH Patient
Centered Medical Home
5 Star Ratings
Health Plans
Needs Assessment
Hospitals ACO HRRP VBP MU HAC
Physician practices
ACO PQRS PCMH MUPhysician compare
Health Plan 5‐star ratingsTotal health care
costs
Self‐Insured Employer
Employee wellness
Employee disease mgmt
Total health care costs
Nursing Homes
Nursing home compare
Community Pharmacies
Community pharmacy practice accreditation
CMS data publically available184
Sustainable Pro Forma Considerations
Cost-Savings &
Cost Avoidance
• HRRP - 3% penalty• VBP - 1.5% • HAC (FY 2015) – 1%• MU (CY 2015) – 1%• PQRS (FY 2015) – 1.5%
P4P: Pay-for-
Performance
• ACO • PCMH• 5-Star Ratings• VBP• Local payer P4P
Revenue • Billing for services
BUSINESS PLAN
Integrated or Con
tractual
CMS Programs Web Site
Hospital Readmission Reduction Program
www.checkmypenalty.com
https://www.medicare.gov/hospitalcompare/readmission‐reduction‐program.html
Health Plan Compare (using 5‐star ratings)
www.medicare.gov/find‐a‐plan/questions/home.aspx
Accountable Care Organizations https://www.cms.gov/Medicare/Medicare‐Fee‐for‐Service‐Payment/sharedsavingsprogram/ACOs‐in‐Your‐State.html
https://www.medicare.gov/physiciancompare/aco/search.html
Physician Compare
https://data.medicare.gov/Hospital CompareNursing Home CompareDialysis Facility CompareHome Health Compare
Hospital Value‐Based Purchasing
https://www.cms.gov/Medicare/Quality‐Initiatives‐Patient‐Assessment‐Instruments/hospital‐value‐based‐purchasing/index.html?redirect=/Hospital‐Value‐Based‐Purchasing/
https://www.medicare.gov/HospitalCompare/Data/payment‐adjustments.html
Hospital‐Acquired Condition Reduction Program
https://www.medicare.gov/hospitalcompare/HAC‐reduction‐program.html
Needs Assessment
CMS HRRP: Hospital Readmission Reduction Program
GOAL = lower 30‐day hospital readmissions
FY 2013 penalty max 1% per Medicare claim Heart Failure, Pneumonia, AMI
FY 2014 penalty max 2%
FY 2015 penalty max 3%
*Added 2 more measures: COPD, TKA/THA
http://cms.gov/Medicare/Medicare-Fee-for-Service-Payment/AcuteInpatientPPS/Readmissions-Reduction-Program.html/
Sachdev, G. Sustainable business models: systematic approach toward successful ambulatory care pharmacy practice. Am J Health-Syst Pharm, 71, Aug 15, 2014:1266-1374. Figure 2

© 2016 by the American Pharmacists Association. All rights reserved.
Which Hospitals are in the Red from Hospital Readmission Reduction Program?
• http://cdn.kaiserhealthnews.org/attachments/MedicareReadmissionPenaltiesByHospital,Year4.pdf
188
CMS Hospital Readmission Reduction Program
http://www.healthrecoverysolutions.com/penalty.php
189
Hospital Medicare Readmission PenaltyArkansas Methodist Medical Center
www.checkmypenalty.com accessed 11-5-15
CHF 254 patientsAMI 166 patientsPNM 391 patientsHIP/KNEE 76 patientsCOPD 317 patients
190
Hospital Medicare Readmission PenaltyArkansas Valley Regional Medical Center
CHF 254 patientsAMI 166 patientsPNM 391 patients
HIP/KNEE 76 patientCOPD 317 patients
191
ACO’s in Arkansas
Accessed 11-5-15, www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/sharedsavingsprogram/ACOs-in-Your-State.html
# 6-14
192
Articulate Value Proposition
Increase # of Patients achieving therapeutic goals
Increase Revenue potential for physicians
Increase Revenue potential for clinic • Ordering more labs• Ordering more Rx and DME
Increase Access to patient care
Increase Revenue/Cost Savings per pharmacist service• Direct Billing• Cost Savings• Pay-for-Performance

© 2016 by the American Pharmacists Association. All rights reserved.
193
Pro Forma (financial projection) Determinants
What are the GAPS in care (needs assessment results)
WHAT types of services are available to close gaps identified
WHERE is the service located • Place of Service (POS) 22 - hospital based outpatient clinic• POS 11 - physician based outpatient clinic• POS 1 - retail pharmacy
194
Pro Forma (financial projection) Determinants continued
WHO will provide supervision
• Billing incident to physician services (direct supervision)
• Billing TCM and CCM (general supervision)
HOW many patients can be seen per day
WHAT is projected no-show rate
ll
Billing Options All of Michigan
except DetroitCPT billing codes Practice Setting
PB=physician based HB=hospital based
2016 Medicare Payment
Diabetes self-management training
G0108 (individual visit) G0109 (group visit)
all G0108 = $51.75G0109 = $13.91
CLIA-Waived Lab variable per POC test all fixed per CPT code
Medication Therapy Management (MTM)
99605, 99606, 99607 pharmacy, employer,health plan
variable per payer
Incident to physician: Office visit in a physician-based (aka, non-hospital) clinic
99211-99215 (PB) PB 99211 = $18.9999212 = $41.9799213 = $70.4499214 = $103.9799215 = $140.38
Incident to physician:Office visit in a hospital-based (aka, hospital outpatient clinic visit)
G0463 (HB) HB G0463 = $102.12
Incident to physician:Transitional Care Management (TCM) &RPh part of team
99496 (within 7d D/C)
99495 (within 14d D/C)PB & HB
99496 = $222.89 (PB) $157.30 (HB)_______99495 = $157.83 (PB) $108.72 (HB)
CMS Annual Wellness Visit (AWV)
G0438 (initial,once/lifetime)G0439 (subseq, annual)
PBHB
PB: G0438 = $166.02HB: G0439 = $111.88
Chronic Care Management (CCM)
99490 (20 minutes/month)
PBHB
PB: $39.37 monthlyHB: $30.80 monthly
196
Case Example Pro Forma: Physician-Based Outpatient Clinic
Payer Mix
Medicare 70%
Medicaid 15%
Commercial 10%
Self-Pay 5%
Self-Insured Employer 0%
197
Case Example continued
• New pts are seen for 60 minutes• Follow-up pts are seen for 30
minutes
Clinic structure for pharmacist-
managed BMT clinic
• Schedule 1 new pt and 6 follow-up pts per ½ day clinic
Established clinic defined as 3
months from start date
• 1 week closed for holidays• 2 pharmacists each working 0.5
FTE
Clinic has pharmacist
coverage for 51 weeks
198
Financial Revenue Opportunity billing Incident to Physician in a Physician-Based Outpatient Clinic
Revenue projection for established pharmacist clinician in a HF clinic in Michigan (except Detroit). Bill using CPT 99211-99215 incident to physician for all payers. Can not bill 99211-99215 under pharmacist NPI unless recognized as a provider by a payer, for which payment would likely be 85% of MD rate.
• For ½ day clinic/wk (0.1 FTE) = 7 visits • For 5 days/wk (1.0 FTE) = 7 visits X 10 = 70 visits/wk X 51wks/yr =
3,570 visits/year max• Assuming 10% of patient no-show for visits = 3,213 visits
Payer Mix for 3,213 visits Reimbursement Sub-Total• Medicare 70% = 2,249 bill 99212 $41.97 $94,391• Medicaid 15% = 482 bill 99212 $15.00-guess $7,230• Commercial 10% = 321 bill 99212 $50.00-guess $16,050• Self-Pay 5% = 160 bill 99211 $0.00 $0.00___
TOTAL Revenue $117,671

© 2016 by the American Pharmacists Association. All rights reserved.
199
Final Thoughts…
The growth of ambulatory care pharmacist services depends on practice leaders being able
to clearly articulate the value proposition for these services in the context of the prevailing
health care payment and delivery systems
200
Thank You
201
Diabetes Self-Management can be billed:
A. Any site that provides the services
B. A site accredited by AADE or ADA
C. Any providers as long as they have are a Certified Diabetes Educator (CDE)
D. On the same day they see another provider at a Federally Qualified Health Center
202
You are providing pharmacy patient care services in a primary care practice whose patient population payment source is 70% Medicare Advantage. Which of the following value based performance measures should you focus on to prove the value of your patient care services?
A. ACO 33 measures
B. HEDIS measures
C. STAR Measures
D. Hospital readmission rates
E. Universal Data Set
203
Medication Adherence measures are used in which Medicare Programs
A. Medicare Advantage and Medicare Part D prescription plans
B. Federally Qualified Health Centers and Accountable Care Organizations
C. Medicare Part D prescription plans only
D. Medicare Advantage, Medicare Part D and Health Insurance Marketplace
204
What is the FIRST step in developing a sustainable business plan,?
A. Provide a service that you like to provide.
B. Meet referring physicians and see what services they suggest.
C. Conduct a needs assessment.
D. Ascertain billing options.

© 2016 by the American Pharmacists Association. All rights reserved.
Recommended