BETA BLOCKERS IN
ACUTE MYOCARDIAL INFARCTION
Dr. Satyam RajvanshiSR Cardiology
OVERVIEW
Overview Introduction Mechanism of benefit in AMI Indications and Recommendation Evidence behind the Recommendations
With and without Reperfusion therapy IV vs Oral initiation Early vs Late
Contraindications Choice of Drug
INTRODUCTION
IntroductionMyocardial infarction (MI) - clinical (or
pathologic) event caused by myocardial ischemia with evidence of myocardial injury or necrosis
Criteria - rise and/or fall of cardiac biomarkers, along with supportive evidence in the form of typical symptoms, suggestive electrocardiographic (ECG) changes, or imaging evidence of new loss of viable myocardium or new regional wall motion abnormality
Early management of the patient involves the simultaneous achievement of several goals:
Relief of ischemic pain Assessment of the hemodynamic state and
correction of abnormalities if present Initiation of reperfusion therapy with primary
percutaneous coronary intervention (PCI) or fibrinolysis
Antithrombotic therapy to prevent rethrombosis or acute stent thrombosis
Beta blocker therapy to prevent recurrent ischemia and life-threatening ventricular arrhythmias
In-hospital initiation of drugs – improve long-term prognosis:
Antiplatelet therapy to reduce the risk of recurrent coronary artery thrombosis
Angiotensin converting enzyme inhibitor therapy to prevent remodeling of the left ventricle
Statin therapy Anticoagulation in the presence of left
ventricular thrombus or chronic atrial fibrillation to prevent embolization
Beta blocker therapy reduces infarct size and early mortality when started early and lowers the risk of death when continued long term
Evidence supporting the benefit of beta blockers has been obtained primarily from randomized trials that included predominantly patients with ST-elevation MI (STEMI).
No randomized trials specifically addressing the efficacy of these drugs in non-ST elevation MI (NSTEMI); however, no observational evidence to suggest different outcomes in patients with NSTEMI.

MECHANISM OF BENEFIT

Beneficial Pharmacodynamics
Decreased oxygen demand - reductions in heart rate, blood pressure, and contractility, and the consequent relief of ischemic chest pain
Decreased risk of ventricular fibrillationexperimental studies demonstrating an increase in the ventricular fibrillation thresholdclinical trials showing a relative risk reduction in sudden cardiac death (30 to 47 percent)
Decreased automaticity, increased electrophysiologic threshold for activation, and slowing of conduction.

Bradycardia prolongs diastole and therefore improves coronary diastolic perfusion and reduces after-depolarizations and triggered activity.
Reduction in remodeling and improvement in left ventricular hemodynamic function (depending upon infarct size and the timing of treatment)
Improved left ventricular diastolic function with a less restrictive filling pattern
Slowing progression of coronary atherosclerosis Inhibition of platelet aggregation and thromboxane
synthesis Reduction in reperfusion injury.
INDICATIONS/RECOMMENDATIONS
INDICATIONS Unless contraindicated, all patients with
acute myocardial infarction (MI) should receive beta blocker therapy.

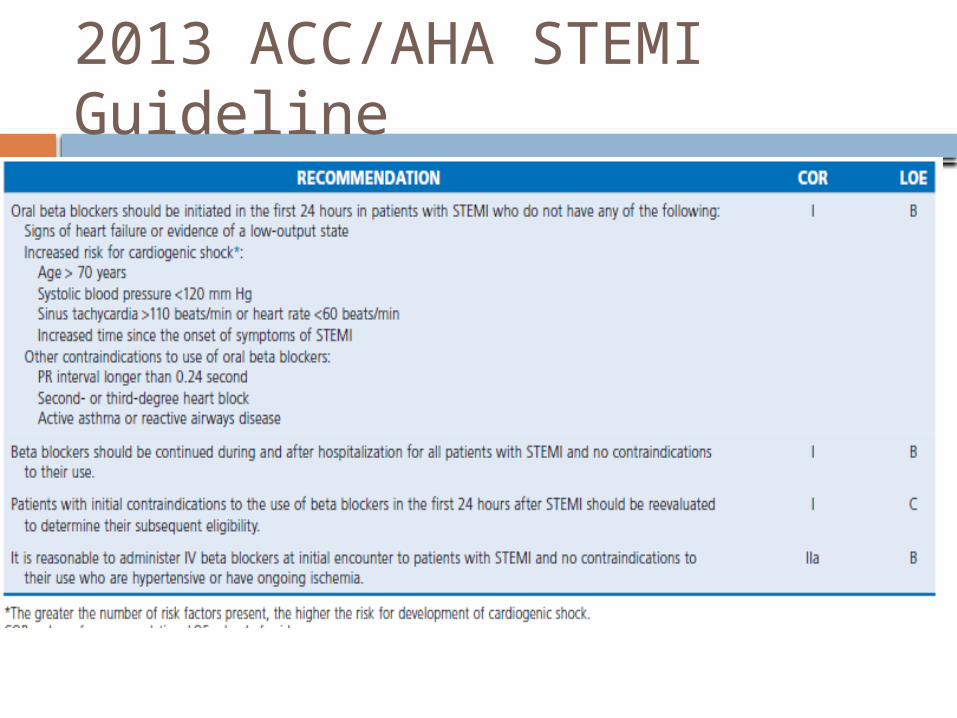
2013 ACC/AHA STEMI Guideline
EVIDENCE

While the evidence is robust for patients with ST-elevation MI (STEMI) treated without fibrinolysis or percutaneous coronary intervention (PCI), this recommendation also applies to STEMI patients who are treated with reperfusion as well as those with non-ST elevation MI (NSTEMI).

Many of the relevant studies were performed before the routine use of long-term antiplatelet and statin therapy.
It is possible that the absolute magnitude of the mortality benefit from beta blocker described below may be smaller due to the beneficial impact of these preventative medications as well as the use of reperfusion therapies.
Evidence with no reperfusion Randomized trials performed before the
use of reperfusion therapy with either fibrinolysis or PCI consistently showed a reduction in cardiovascular mortality of 10 to 25 percent in patients treated with metoprolol, propranolol, or atenolol
Meta-analysis of these studies found a 25 percent reduction in mortality at one year
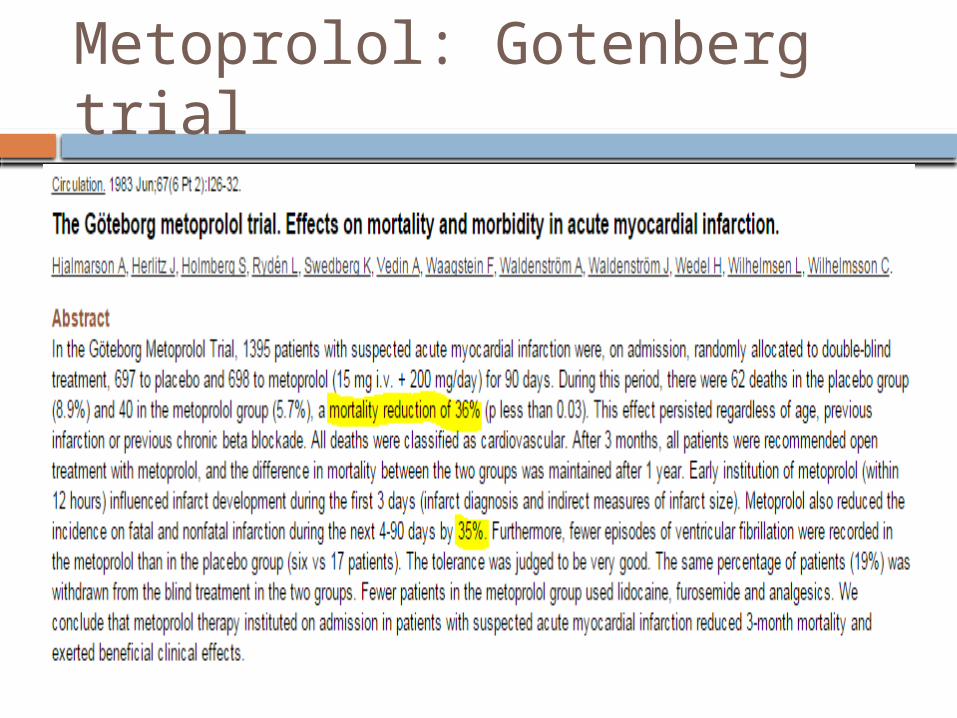
Metoprolol: Gotenberg trial

IV Metoprolol: MIAMI trial
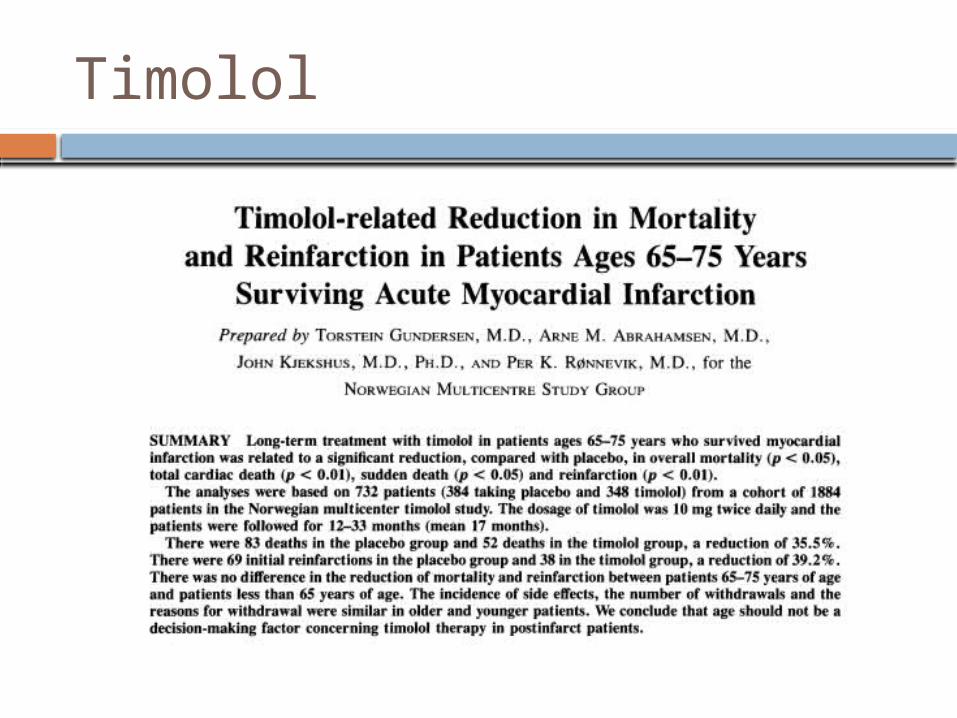
Timolol
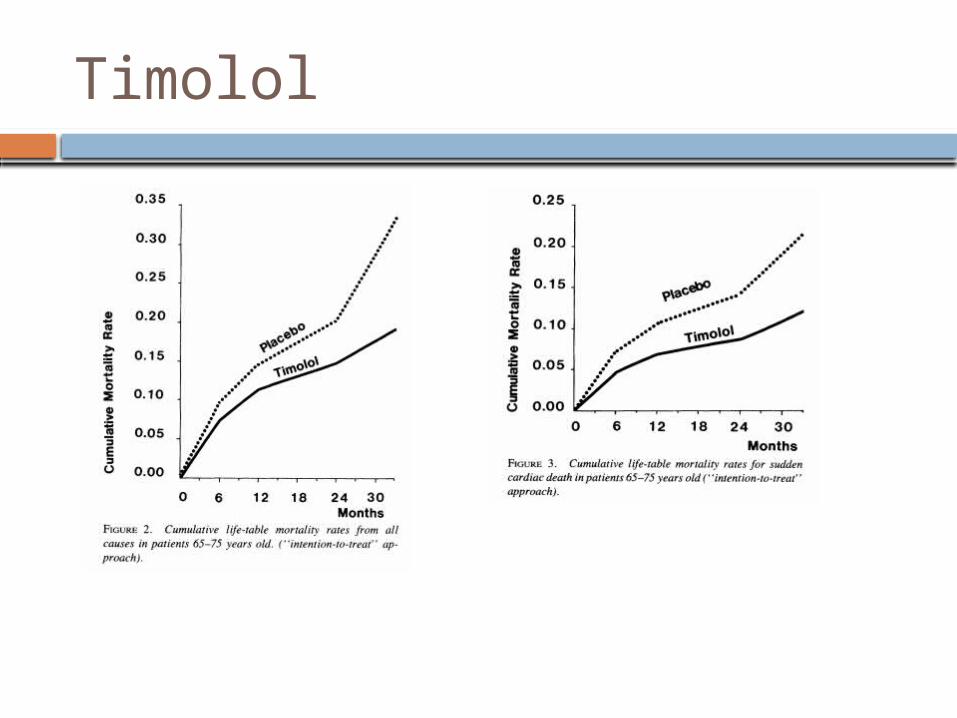
Timolol
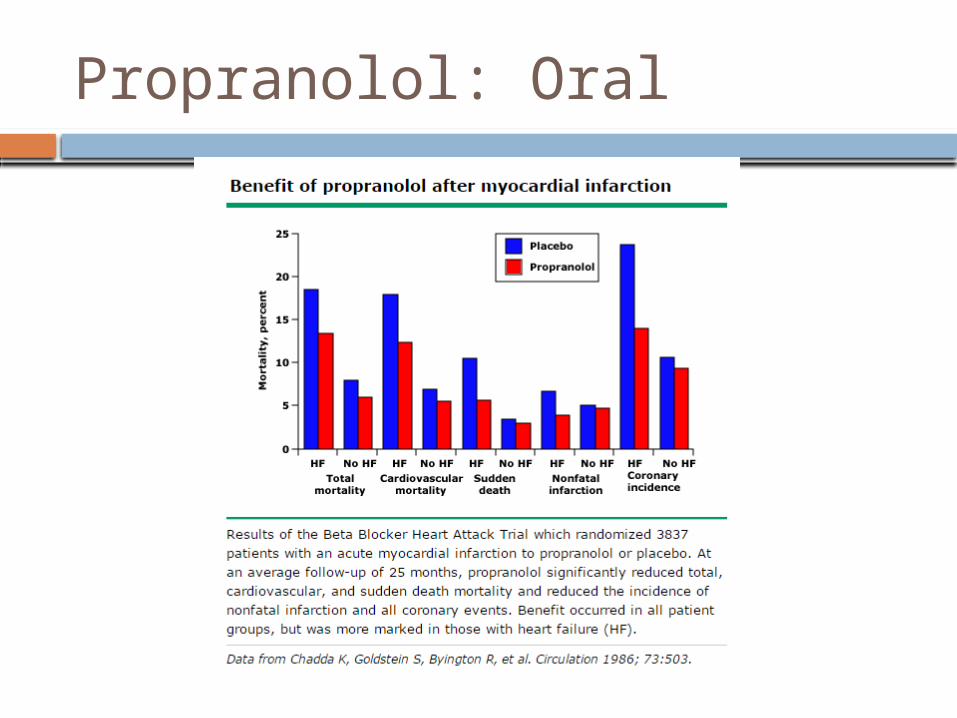
Propranolol: Oral

IV Atenolol: ISIS-1
Evidence with Fibrinolytic therapy
No high quality evidence demonstrating a beneficial impact of long-term beta blocker use in patients treated with fibrinolytic therapy.
Much of the evidence is indirect - from the benefit shown in patients not receiving reperfusion.
Individual studies that evaluated the long-term impact of beta blockade in patients treated with fibrinolysis were limited by small size, early termination, observational design, or relatively short duration follow-up.
Evidence with PCI The same evidence supporting long-term
beta blocker use in patients treated with or without fibrinolysis - basis for a similar recommendation in patients who undergo primary PCI.
Some experts suggest - the benefit of beta blockers in this subpopulation may be reduced by the improvement in outcome afforded by revascularization - no randomized trials and few observational studies of long-term beta blocker therapy patients treated with primary PCI.

“EARLY” Initiation For patients without contraindications -
treat ALL patients with an oral beta blocker within the first 24 hours after diagnosis

Some earlier trials tested IV beta blockade
Intravenous beta blocker - potential for development of hemodynamic instability.
Some authors recommend - reserve the intravenous route principally for patients with refractory angina who have ongoing ischemia prior to percutaneous coronary intervention (PCI) in whom there is no hemodynamic instability including heart failure.
Early vs Late in fibrinolytic t/t Available evidence does not support
routine, early initiation of intravenous beta blockade in patients treated with fibrinolytic therapy - oral therapy is recommended
This recommendation for these patients is based on the overall benefit of beta blockers
Three randomized trials (1989, 1991, and 1993) of ST-elevation myocardial infarction (STEMI) patients treated with fibrinolytic therapy compared early and deferred beta blocker therapy and found no clear evidence of a mortality benefit with early beta blocker.
In these studies, deferred therapy occurred within 24 hours to up to six days.
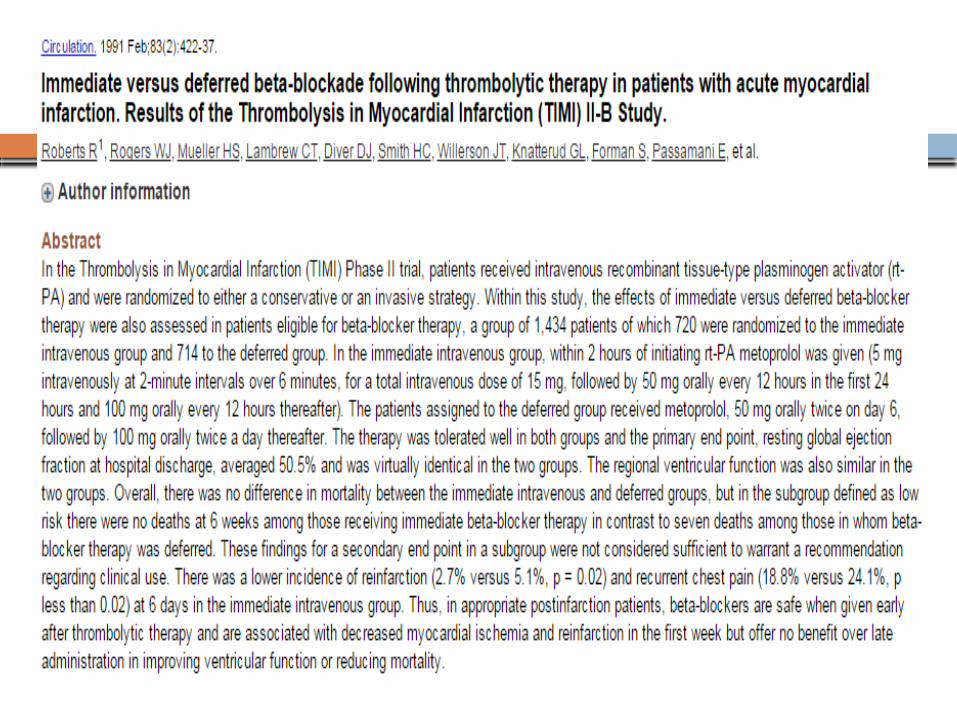
The optimal timing of beta blocker therapy was evaluated in a study of patients enrolled in the TIMI II trial [30]. (See "Trials of conservative versus early invasive therapy in unstable angina and non-ST elevation myocardial infarction", section on 'TIMI IIIB trial'.) A subset of 1390 patients who were eligible for intravenous beta blockade were randomly assigned to 15 mg of IV metoprolol tartrate (followed by oral metoprolol) or oral metoprolol begun on day six. There was no significant difference between the two groups in the in-hospital left ventricular ejection fraction or in mortality at 6 and 42 days. However, by day six, the early therapy group had significant reductions in nonfatal reinfarction (16 versus 31 patients) and recurrent ischemic episodes (107 versus 147 patients).
In an observational study of 2537 patients enrolled in primary angioplasty trials, those who received beta blocker therapy before primary angioplasty, compared to those who did not, had lower adjusted in-hospital mortality (odds ratio [OR] 0.41, 95% CI 0.20-0.84) and nonsignificantly lower one-year mortality (OR 0.72, 95% CI 0.47-1.08). The dose and route of administration of beta blocker was not reported.
Patients who do not receive a beta blocker during the first 24 hours because of early contraindications should be re-evaluated for beta blocker candidacy for subsequent therapy.
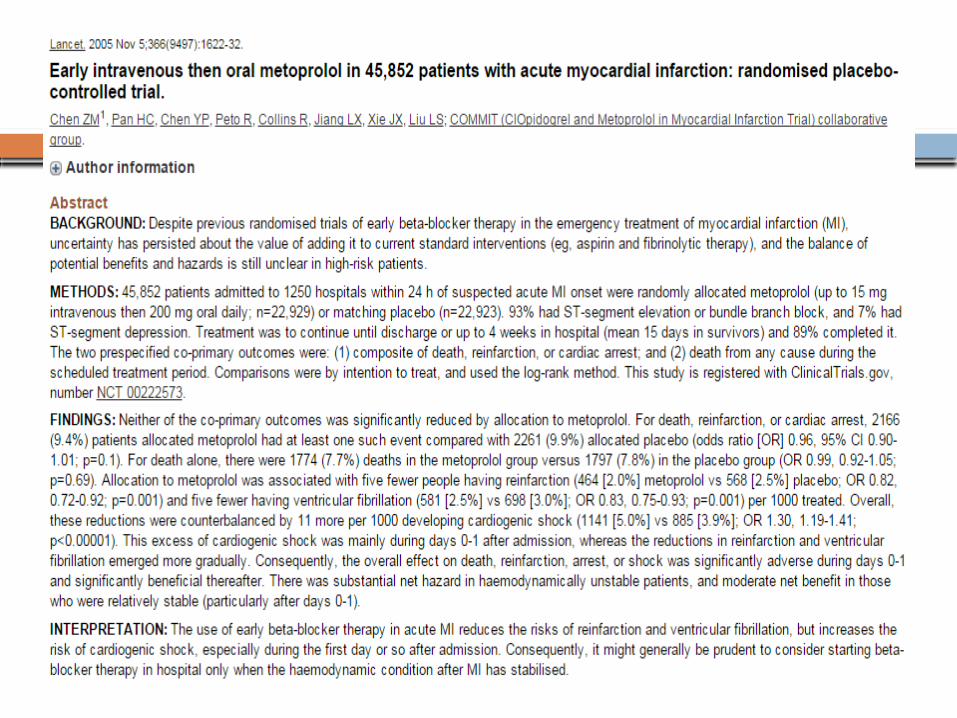
COMMIT/CCS2 trial - 46,000 MI patients, 50% fibrinolytic therapy - Placebo or to three 5 mg intravenous boluses of metoprolol followed by oral metoprolol extended release (succinate)200 mg/day for 30 days.
No overall mortality benefit from early intravenous beta blocker therapy.

Immediate beta blocker therapy may reduce the incidence of intracerebral hemorrhage.
This effect was suggested in a review of data from 60,329 patients treated with Alteplase in the National Registry of Myocardial Infarction.
Immediate beta blocker use was associated with a lower incidence of intracerebral hemorrhage (0.67 versus 1 percent for no immediate beta blocker; odds ratio 0.69, 95% CI 0.57-0.84). This apparent benefit was seen in all age groups and in both men and women.
Hemodynamic stability appeared to be an important determinant of the response to beta blockers. There was a significant increase in mortality in patients who presented with hemodynamic compromise that was balanced by a trend toward reduced mortality in patients who were hemodynamically stable.

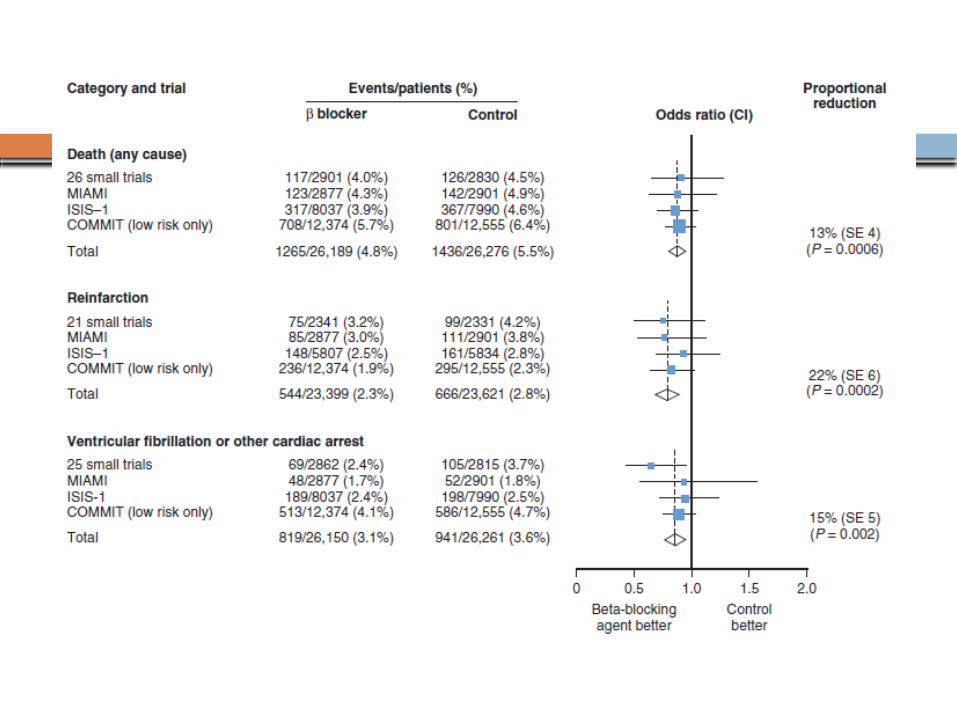
Combining the results of the low-risk patients from COMMIT with the data from earlier trials13% reduction in all-cause mortality (7 lives saved/1000 patients treated)22% reduction in reinfarction (5 fewer events/1000 patients treated)15% reduction in ventricular fibrillation or cardiac arrest (5 fewer events/1000 patients treated)
To achieve these benefits safely, it is important to avoid the early administration of beta blockers to patients with relative contraindications
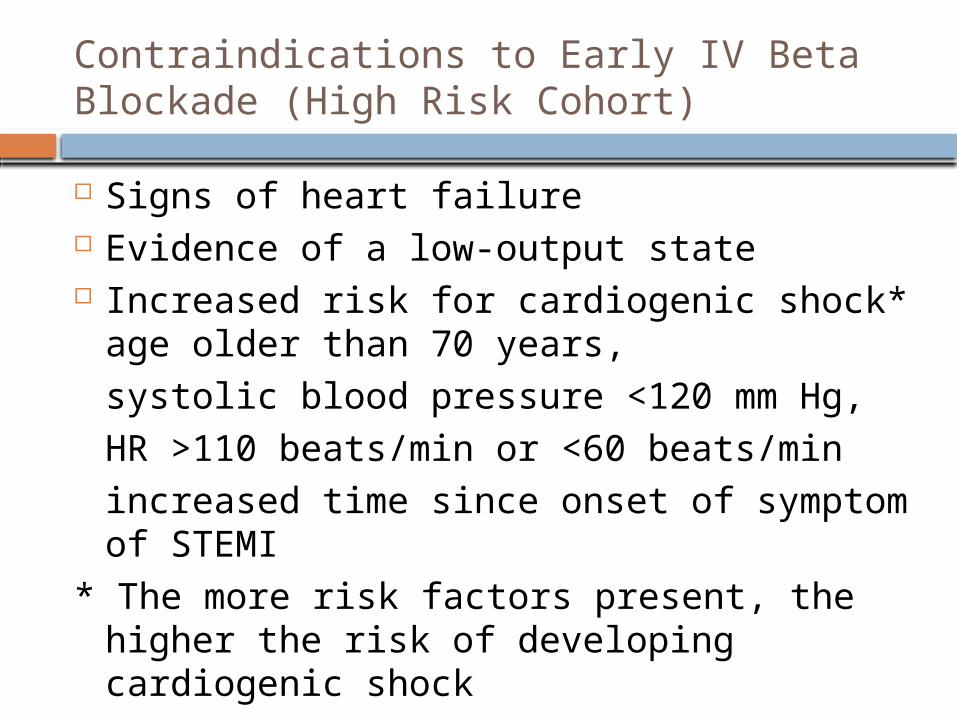
Contraindications to Early IV Beta Blockade (High Risk Cohort)
Signs of heart failure Evidence of a low-output state Increased risk for cardiogenic shock*
age older than 70 years, systolic blood pressure <120 mm Hg, HR >110 beats/min or <60 beats/minincreased time since onset of symptom of STEMI
* The more risk factors present, the higher the risk of developing cardiogenic shock
Early beta blockade in PCIEvidence for early beta blockade initiation in
patients treated with current recommended therapies - METOCARD-CNIC trial (2013)270 patients with Killip class II or less anterior STEMI were randomly assigned to receive intravenous metoprolol (up to three 5 mg boluses of metoprolol tartrate given two minutes apart) or not before reperfusion and all patients received oral metoprolol within 24 hours.
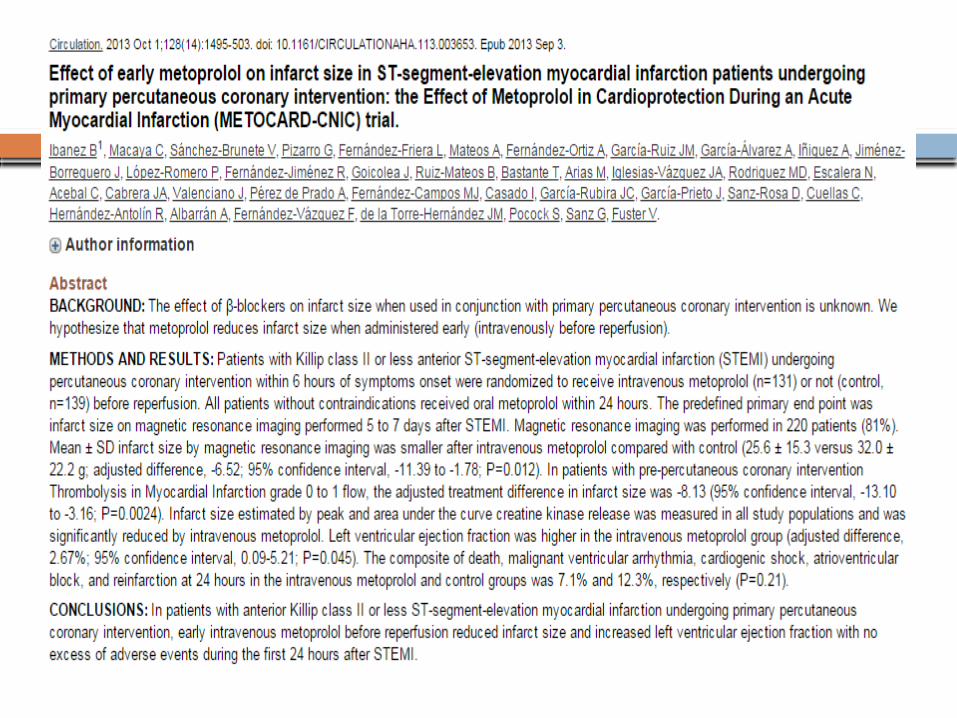
The primary end point of infarct size on magnetic resonance imaging performed five to seven days was significantly smaller in the group that was treated early (25.6 versus 32.0 grams; p = 0.012). In addition, left ventricular ejection fraction was higher in the treated group at five to seven days and at six months (adjusted treatment difference 2.67 percent; p = 0.045 and 3.49 percent; p = 0.025)
There was no difference in the safety end point. Limitations of the study include lack of a placebo
control and exclusion of patients with inferior MI.
Retrospective analysis from the CADILLAC trial of 2082 patients. At 30 days, patients who had received a preprocedural beta blocker had a significantly lower mortality than those who had not (1.5 versus 2.8 percent);
The lower mortality was limited to patients who had not been receiving an oral beta blocker before admission

CHOICE OF DRUG

Which Beta blocker? Cardioselective oral beta blocker, such
as Metoprolol or Atenolol preferred Use oral metoprolol tartrate 25 to 50 mg
every 6 to 12 hours or atenolol 25 to 50 mg twice daily, initially, titrating upward as needed.
Short-acting beta blockers are preferred early to allow for more rapid adjustment of dose based on the patient’s blood pressure and heart rate response.
Near the time of discharge - switch to longer-acting beta blockers.
Intravenous Beta blockade?For the uncommon patient in whom
intravenous therapy may be chosen, such as those with ongoing ischemia prior to PCI in whom there is no hemodynamic instability including heart failure – following regimes:

Intravenous Metoprolol tartrate - 5 mg increments by slow intravenous administration (5 mg over one to two minutes), repeated every five minutes for a total initial dose of 15 mg (three doses). Patients who tolerate this regimen should then receive maintenance oral therapy with metoprolol succinate 50 mg daily beginning 15 min after the last intravenous dose.
Intravenous Atenolol - 5 mg dose followed by another 5 mg five minutes later. Patients who tolerate this regimen should then receive maintenance oral therapy with atenolol 50 mg twice daily beginning one to two hours after the last intravenous dose.
Intravenous Esmolol (50 mcg/kg per min increasing to a maximum of 200 to 300 mcg/kg per min), an ultra-short-acting beta blocker, can be given to assess tolerance to beta blockade in patients with borderline or questionable left ventricular function.
Bradycardia and hypotension are the most common limitations to achieving the full dose. In this setting, the rate of administration should be slowed or oral therapy initiated.
A rigid "cookbook" regimen should not be used since there is a variable sympathetic response to acute MI.
Patients with hypertension — Some experts recommend the use of intravenous beta blocker therapy for patients with acute MI and hypertension
At some centers – intravenous NTG, starting at a low dose, is preferred for such patients
2013 ACC/AHA STEMI Guideline

LONG TERM THERAPY

Optimal duration of beta blocker therapy after myocardial infarction (MI) is not known
Evidence supports the use of beta blockers in patients with MI for as long as 3 years
Evidence supporting a longer duration, or indefinite therapy, is limited - preferred in patients with high-risk features at presentation such as cardiogenic shock, heart failure, or chronic kidney disease
For patients without these high-risk features - the potential benefits and risks of continued therapy maybe discussed with patients
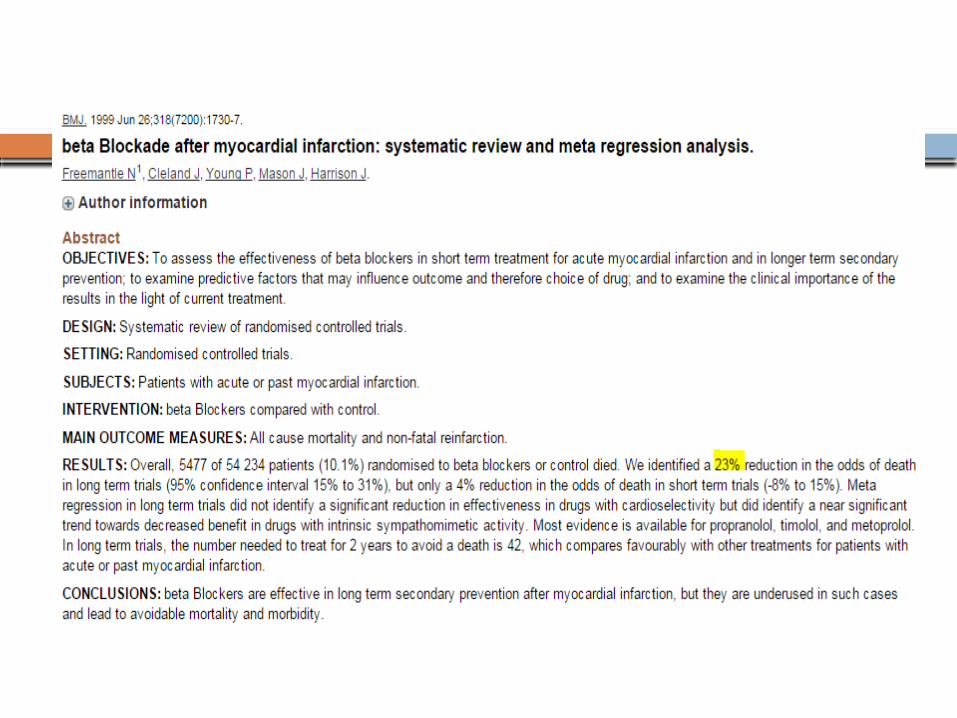
Many patients have been continued on this therapy indefinitely based on a 1999 meta-analysis of over 50,000 patients that showed a 23 percent reduction in death at a mean follow-up of 1.4 years.
Limitations - relatively short duration of follow-up, Reperfusion and Current GDMT were underutilized

More recent evaluation of the potential benefit from long-term beta blocker use - 2012 observational study of over 14,000 patients with known prior MI enrolled in the international REACH registry.
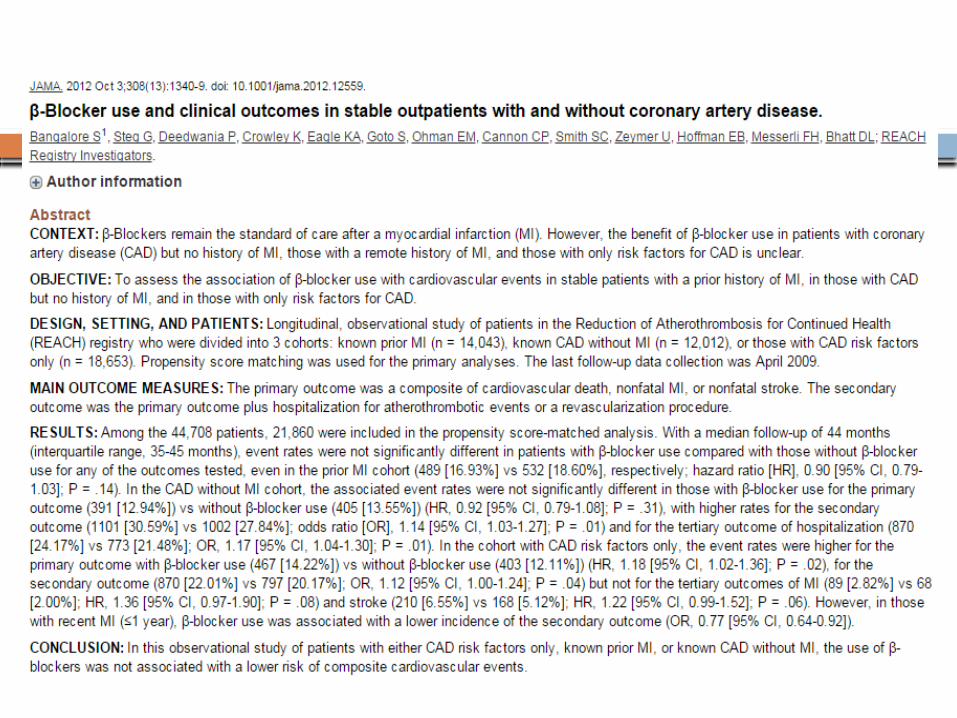
Patients were enrolled in 2003 and 2004 and followed prospectively for up to four years.
The primary outcome was a composite of cardiovascular death, nonfatal MI, or nonfatal stroke - 3599 pairs of patients with and without beta blocker use.
After a median follow-up of 44 months, there was a trend toward a lower incidence of the primary outcome with beta blocker therapy (16.9 versus 18.6 percent, respectively; hazard ratio 0.90, 95% CI 0.79-1.03). However, little difference was seen in the event rates in the beta blocker and no beta blocker groups as early as two years.
A 2013 observational study evaluated outcomes in 5628 patients with ST-elevation MI (STEMI) treated with primary percutaneous coronary intervention
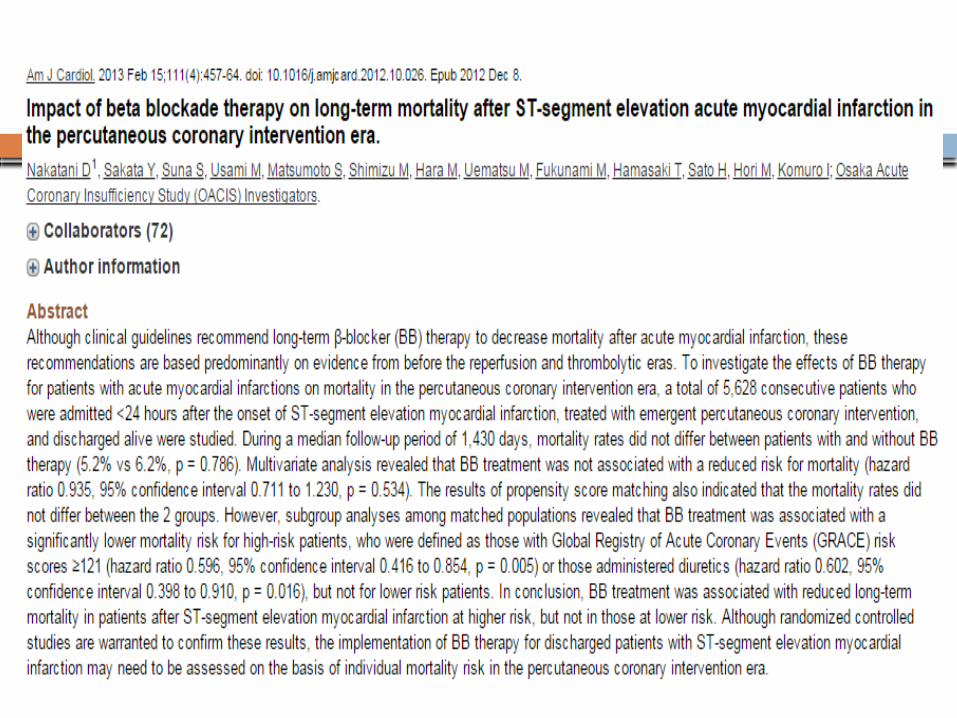

Median follow-up of nearly four years, mortality rates did not differ between patients with and without beta blocker therapy (5.2 versus 6.2 percent).
Subgroup analyses revealed that beta blocker treatment was associated with a significantly lower mortality for only high-risk patients, such as those with heart failure.
Is it Reasonable to discontinue Beta-blockade? In patients with unacceptable side effects Financial burden is unacceptable use of multiple medications is problematic
(polypharmacy) In absence of compelling indications –
Systolic HF (LVEF < 40%); Ventricular arrhythmias
May use a tapering protocol over a few weeks
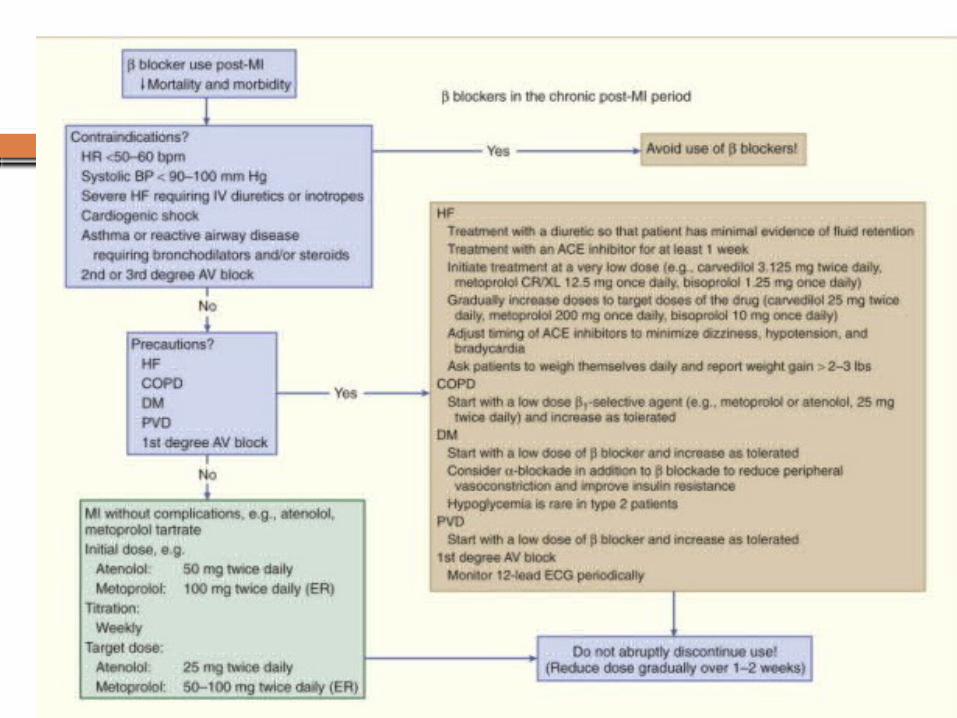
Which Blocker in long term? Choice of drug — For long-term administration, we believe that the
benefit from beta blockers (table 2) is a class effect and that agents without intrinsic sympathomimetic activity (ISA), such as pindolol, are preferred [39-41]. In a 1999 meta-analysis of randomized controlled trials, there was no significant difference in benefit with cardioselective compared to nonselective drugs, but there was an almost significant trend toward less benefit with drugs that have ISA [24].
We start with a beta-1-selective agent in most patients. Usual initial doses are metoprolol tartrate (immediate release preparation) 50 to 100 mg twice daily or metoprolol succinate (extended release preparation) 50 or 100 mg daily or atenolol 50 to 100 mg divided twice daily. When possible, we use the longer-acting preparation. For patients in whom there is a concern for intolerance to these doses, lower initial doses should be used; in this setting, up-titration should occur as promptly as possible.
Patients with heart failure and systolic left ventricular dysfunction should be treated long-term with carvedilol, extended-release preparation metoprolol, orbisoprolol.
Post MI with Systolic LV dysfunctionPreferred agents
CarvedilolMetoprolol Extended-release
preparation Bisoprolol
Post MI without Systolic LV dysfunctionBenefit from beta blockers likely a class effectAgents without intrinsic sympathomimetic activity (ISA), such as pindolol are preferred
A 1999 meta-analysis of RCTs - no significant difference between
cardio - selective compared to nonselective drugs
- an almost significant trend toward less benefit with drugs that have ISA
Heart rate goal of below 70 beats per minute while maintaining a systolic pressure above 90 mmHg
An inverse relationship between short-term and long-term mortality and the degree of heart rate reduction with beta blockade after MI is evident
CONTRAINDICATIONS
Absolute ContraindicationsPotential absolute contraindications to the
immediate use of beta blocker therapy include the following groups:
Hemodynamically compromised individuals, including those with hypotension with or without shock
Patients with active bronchospasm, severe bradycardia, or heart block greater than first degree (unless the patient has a permanent pacemaker).
Patients with myocardial infarction (MI) precipitated by cocaine use; there is a risk of precipitating coronary artery spasm
Patients with overt heart failure, including pulmonary edema. However, there is a strong indication for carefully initiated oral beta blocker therapy (beginning at very low doses) in such patients whose heart failure has been brought under control prior to discharge
Relative or Potential Contraindications
Comorbidities Uncontrolled COPD/asthma, Uncontrolled DMSymptomatic Peripheral artery disease

Occasionally, the clinician may wish to proceed with beta blocker therapy even in the presence of relative contraindications - a history of mild asthma, mild bradycardia, mild heart failure, or first-degree heart block.
In this situation, a trial of Esmolol may help determine whether the patient can tolerate beta-blockade - half-life of 9 minutes, hemodynamic effects disappear in less than 30 minutes
CONCLUSIONSIn the broad range of patients with ST
elevation and non-ST elevation myocardial infarction (MI), including those who have or have not received revascularization, judicious beta blocker use reduce short-term complications and improve long-term survival.
CONCLUSIONSFor all patients who have sustained an
acute MI, beta blockade is recommendedFor all patients with acute MI, initiation of
oral beta blockers within the first 24 hours is recommend, as long as no contraindications are present
Patients who do not receive a beta blocker during the first 24 hours because of early contraindications should be reevaluated for beta blocker candidacy

Recommended
![Differential Metabolic Effects of Beta-Blockers: an Updated … · 2018-09-25 · beta-blockers [33]. By impairing beta2-mediated insulin re-lease, beta-blockers decrease the first](https://img.pdfslide.us/doc/110x75/5f41a562c5d9b012e330e205/differential-metabolic-effects-of-beta-blockers-an-updated-2018-09-25-beta-blockers.jpg)