8/10/2019 Bening Prostatic Hyperplasia
http://slidepdf.com/reader/full/bening-prostatic-hyperplasia 1/8
8/10/2019 Bening Prostatic Hyperplasia
http://slidepdf.com/reader/full/bening-prostatic-hyperplasia 2/8
Methods
All patients gave written informed consent and were informed in detail
about our procedures for diagnostic fulfillment according to the proto-
col of this study, which was approved by the local hospital ethics
committee. One hundred and thirteen consecutive patients aged from
52 to 75 years (mean 63 years) with a clinical diagnosis of BPH in
whom transurethral resection of the prostate (TURP) was planned –
were examined by 3D XI modality.
Patients with other causes of infravesical obstructive uropathy were
excluded. Patients with proved prostatic neoplastic focal lesion after
pathology confirmations of specimens obtained by systematic trans-
rectal ultrasound guided biopsy were also excluded. Prostatic specific
antigen (PSA) levels were 3.1 up to 4.9 ng/mL (mean, 3.7 ng/mL).
Three-dimensional Trans-Rectal Ultrasound(3D-TRUS) procedures
The study was achieved by means of the 3D US machine (MEDISON-
Accuvix-XQ) provided with 3D XI software for extended thin sectional
panoramic appraisal of the prostate gland. Examinations were per-
formed with a 3D endocavitary motorized-sweep probe (5–8 MHz). We
routinely acquired the entire prostate for every patient in a single 3D
volume. XI Multi-Resolution (XI MR) computed maneuvers and inter-
pretations of volumes were fulfilled after the patient left the examina-
tion room.
Estimation of the prostate volume (PV) and PVR in all cases were
measured using 3D calculations – VOCAL-imaging program (Virtual
Organ Computer-aided AnaLysis). Volume = 1/2[åni = 2(Ai-1 + Ai) á
di-1].
3DUS display methods
The reconstructed 3D XI image data set was networked to the work-
station (Sonoview II). We used two formats. First, the Multi-Slice View(MSV), the milestone of 3D XI technology, which is a computed
tomography of the acquired volume, in which the set of a single volume
viewed as sequences of 2D US images in axial, coronal or transverse
planes. The thickness of images in a series can also be manipulated
from fractions of a millimeter to a few millimeters thick. Second, we
used the XI MR, which is a sophisticated form of interactive image
speckle removal with a scale of enhancement providing stronger, very
thin images. 3D XI Image quality was optimized by using algorithms to
vary opacity, transparency, part selection and depth.
Collection of tissue specimens
The complex zonal anatomy led us to believe that a single technique
could not be used to obtain specific tissue from the zones. For each
zone, the sampling techniques were standardized. Apart from the six
systematic biopsies prior to the patient’s selection, another two biopsies
were obtained guided by live 3D-TRUS, thus allowing direct sampling
of the transitional and central zone nodular lesions. Then, during the
TURP, several tissue samples were also collected from the same patient
with a resectoscope loop biopsy. All tissue specimens were fresh prior
to fixation in formalin, signifying where tissue samples were obtained.
Groups
Patients were grouped according to PVR into three groups, less and
more than 100 mL and urine retention according to the agreed limits 5–8
0
50
100
150
200
250
N
(mean)
PV
(mean)
PVR
Group I
Group II
Group III
R
PA
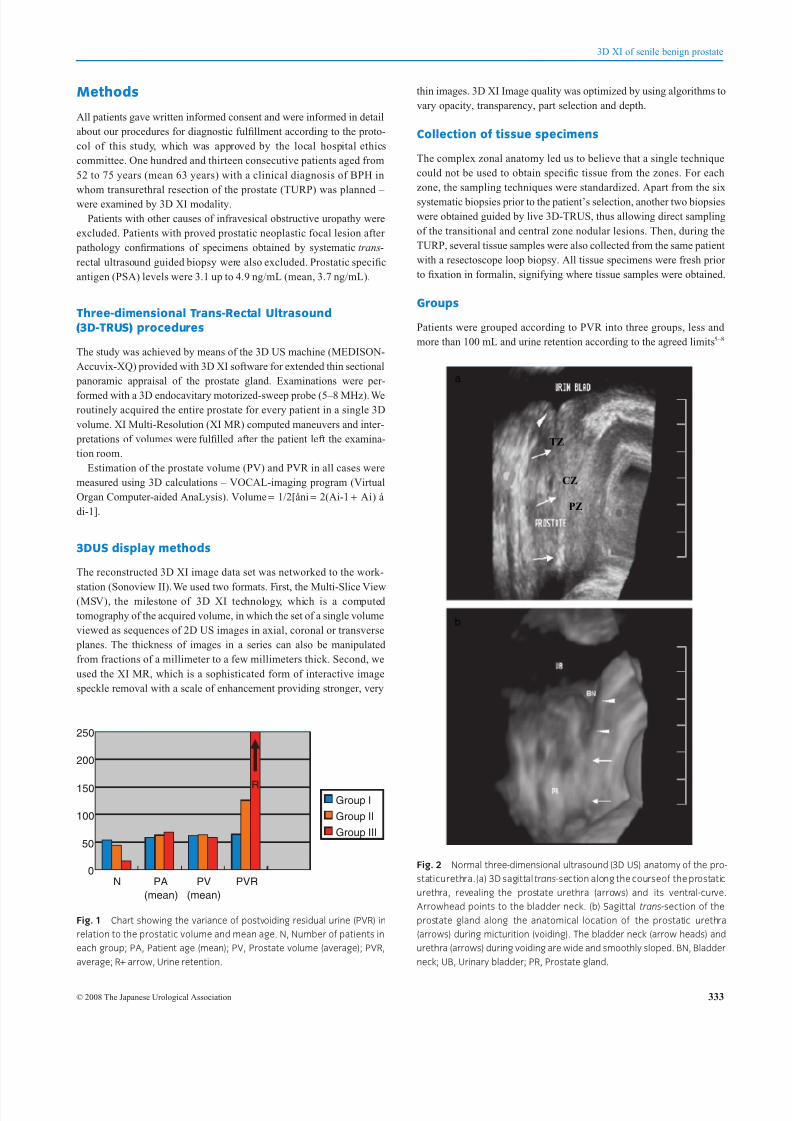
Fig. 1 Chart showing the variance of postvoiding residual urine (PVR) in
relation to the prostatic volume and mean age. N, Number of patients in
each group; PA, Patient age (mean); PV, Prostate volume (average); PVR,
average; R+ arrow, Urine retention.
a
b
CZ
PZ
TZ
Fig. 2 Normal three-dimensional ultrasound (3D US) anatomy of the pro-
staticurethra.(a) 3D sagittal trans-section along the courseof the prostatic
urethra, revealing the prostate urethra (arrows) and its ventral-curve.
Arrowhead points to the bladder neck. (b) Sagittal trans-section of the
prostate gland along the anatomical location of the prostatic urethra
(arrows) during micturition (voiding). The bladder neck (arrow heads) and
urethra (arrows) during voiding are wide and smoothly sloped. BN, Bladder
neck; UB, Urinary bladder; PR, Prostate gland.
3D XI of senile benign prostate
© 2008 The Japanese Urological Association 333
8/10/2019 Bening Prostatic Hyperplasia
http://slidepdf.com/reader/full/bening-prostatic-hyperplasia 3/8
8/10/2019 Bening Prostatic Hyperplasia
http://slidepdf.com/reader/full/bening-prostatic-hyperplasia 4/8
Both XI MR and histopathological specimens were blindly inter-
preted. Imaging impressions finally compared to the histopathological
results of specimens obtained after TURP.
The recorded positive values included:
1 Assessment of image quality.
2 The relationship between the enlarged prostate gland to the volumeof PVR.
3 Nodular mapping and characterization according to histopathologi-
cal reports.
4 Demonstrating the effect of BPH nodules upon the prostatic
urethra.
Image analysis
Readability and diagnostic efficacy of images were undertaken using
computer software (HIT-Telepax). Analysis of the XI MR images was
carried out by comparing echo-intensity values for stromal vs glandular
tissue obtained by using computer software (Genstat 9).
Results
None of the suspected cancerous or other causes of lower bladder outlet
obstructive uropathy was included in this study.
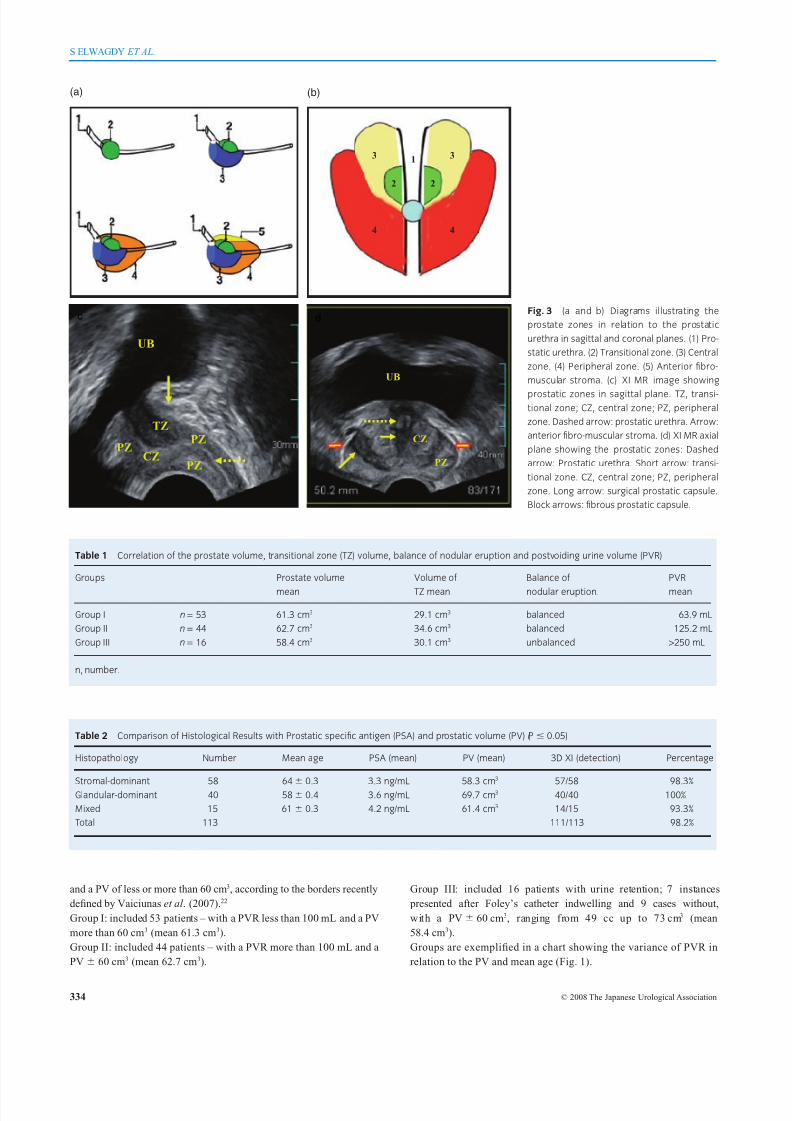
The normal 3D XI display of the prostatic urethra and the prostate
gland zones with diagrammatic illustrations designed by the working
group (Figs 2,3) was a preliminary essential.
The prevalence of histopathological benign prostate hyperplasia and symptoms enrolled in our study was usually found in patients older
than 50 years.
Our records of the three groups concluded that the prostate gland in
a significant proportion of cases is distinctly enlarged (>60 cm3) with
an estimated PVR of less than 100 mL. On the other hand, prostate
enlargement (<60 cm3) may come in the company of big volumes of
PVR up to urine retention.
XI MR proved capable of localization of the prostate urethral course
and the morphology of the BPH nodules. XI MR could explain the
changes of the transitional zone (TZ) and the central zone (CZ) of the
prostate gland according to the balance of nodular eruption alongside
of the prostatic urethra; scheduled in Table 1.
a
N
b
N
BN
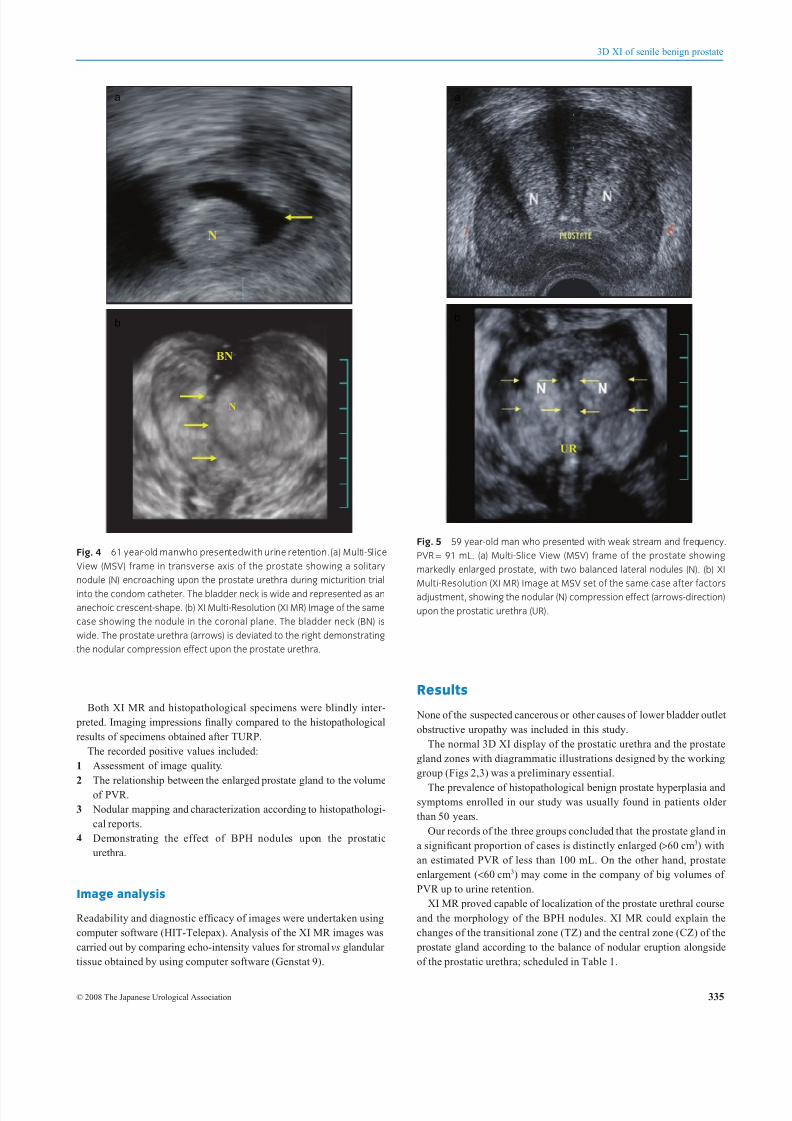
Fig. 4 61 year-old manwho presentedwith urine retention.(a) Multi-Slice
View (MSV) frame in transverse axis of the prostate showing a solitary
nodule (N) encroaching upon the prostate urethra during micturition trial
into the condom catheter. The bladder neck is wide and represented as an
anechoic crescent-shape. (b) XI Multi-Resolution (XI MR) Image of the same
case showing the nodule in the coronal plane. The bladder neck (BN) is
wide. The prostate urethra (arrows) is deviated to the right demonstrating
the nodular compression effect upon the prostate urethra.
UR
a
b
Fig. 5 59 year-old man who presented with weak stream and frequency.
PVR = 91 mL. (a) Multi-Slice View (MSV) frame of the prostate showing
markedly enlarged prostate, with two balanced lateral nodules (N). (b) XI
Multi-Resolution (XI MR) Image at MSV set of the same case after factors
adjustment, showing the nodular (N) compression effect (arrows-direction)
upon the prostatic urethra (UR).
3D XI of senile benign prostate
© 2008 The Japanese Urological Association 335
8/10/2019 Bening Prostatic Hyperplasia
http://slidepdf.com/reader/full/bening-prostatic-hyperplasia 5/8
Accuracy of XI MR in nodular detection and characterization real-
ized about 98.2% referenced to histopathological reports. Diagnostic
accuracy of 3D XI in nodular detection compared to the histopatho-
logical type intended in Table 2.
The severity of the patients’ symptoms reported in our series was in
association with prominent big peri-urethral nodules in two patients
(Fig. 4), bilateral symmetrical prominent nodules in three patients
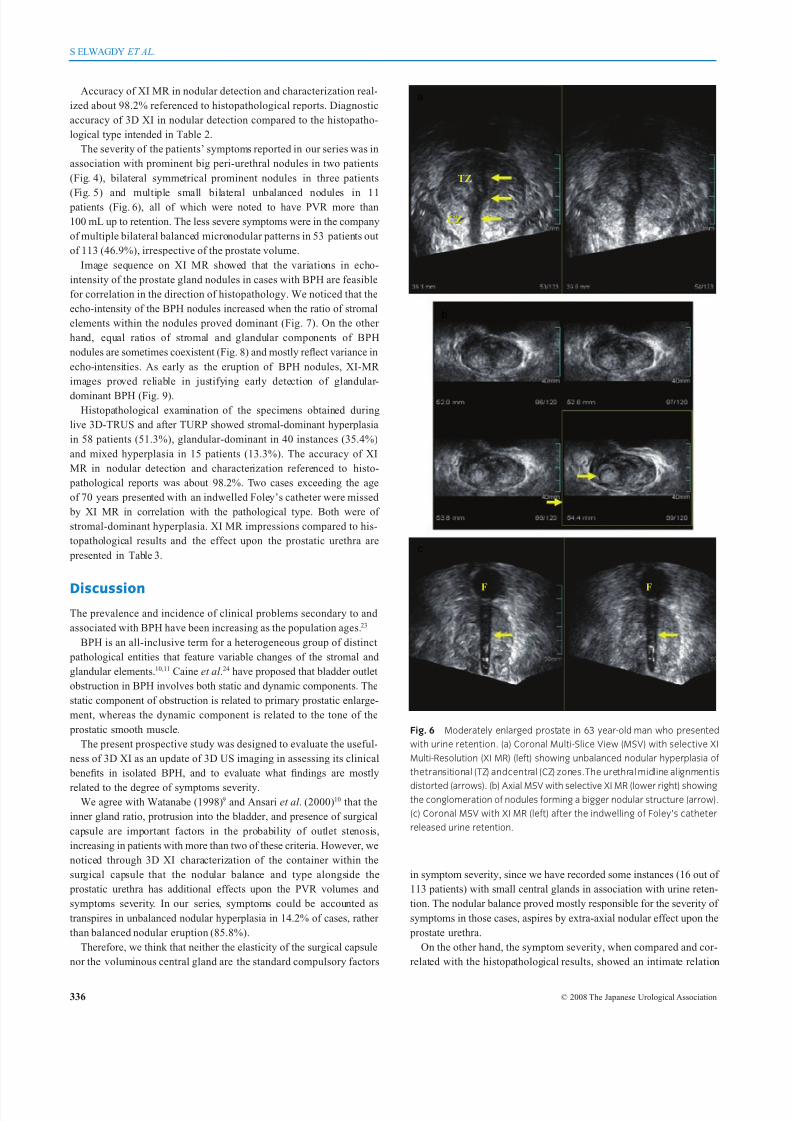
(Fig. 5) and multiple small bilateral unbalanced nodules in 11 patients (Fig. 6), all of which were noted to have PVR more than
100 mL up to retention. The less severe symptoms were in the company
of multiple bilateral balanced micronodular patterns in 53 patients out
of 113 (46.9%), irrespective of the prostate volume.
Image sequence on XI MR showed that the variations in echo-
intensity of the prostate gland nodules in cases with BPH are feasible
for correlation in the direction of histopathology. We noticed that the
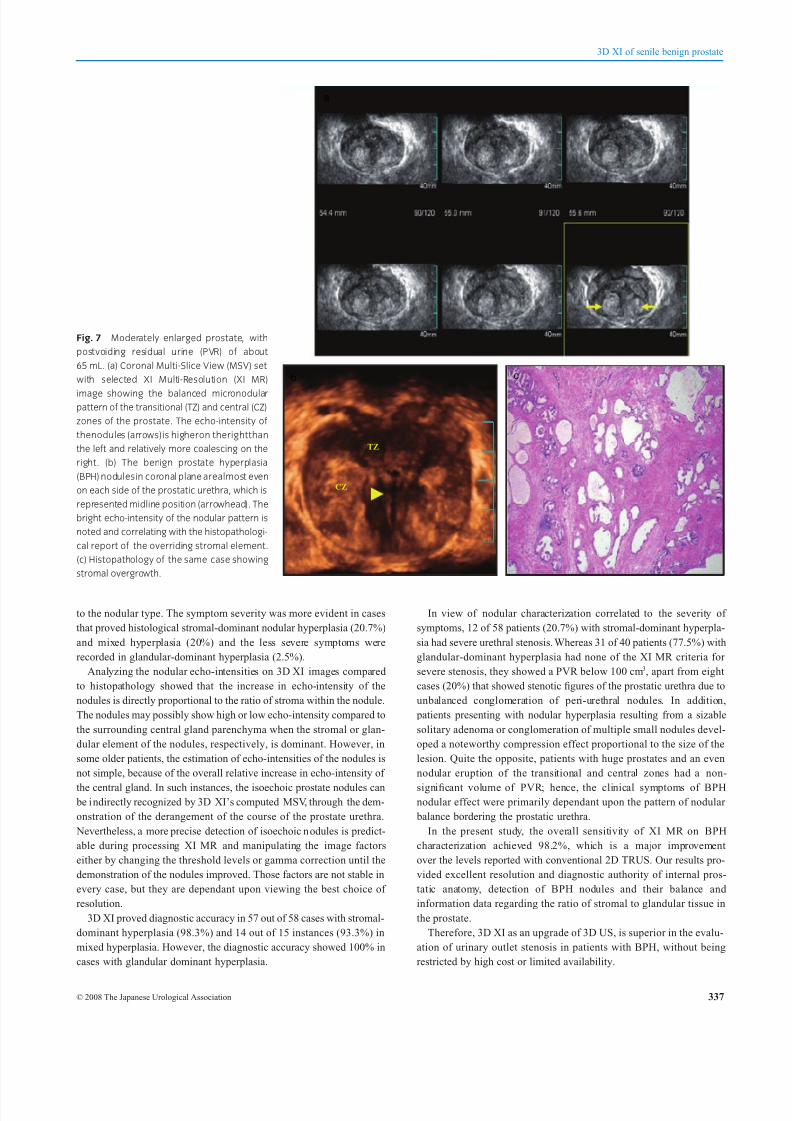
echo-intensity of the BPH nodules increased when the ratio of stromal
elements within the nodules proved dominant (Fig. 7). On the other
hand, equal ratios of stromal and glandular components of BPH
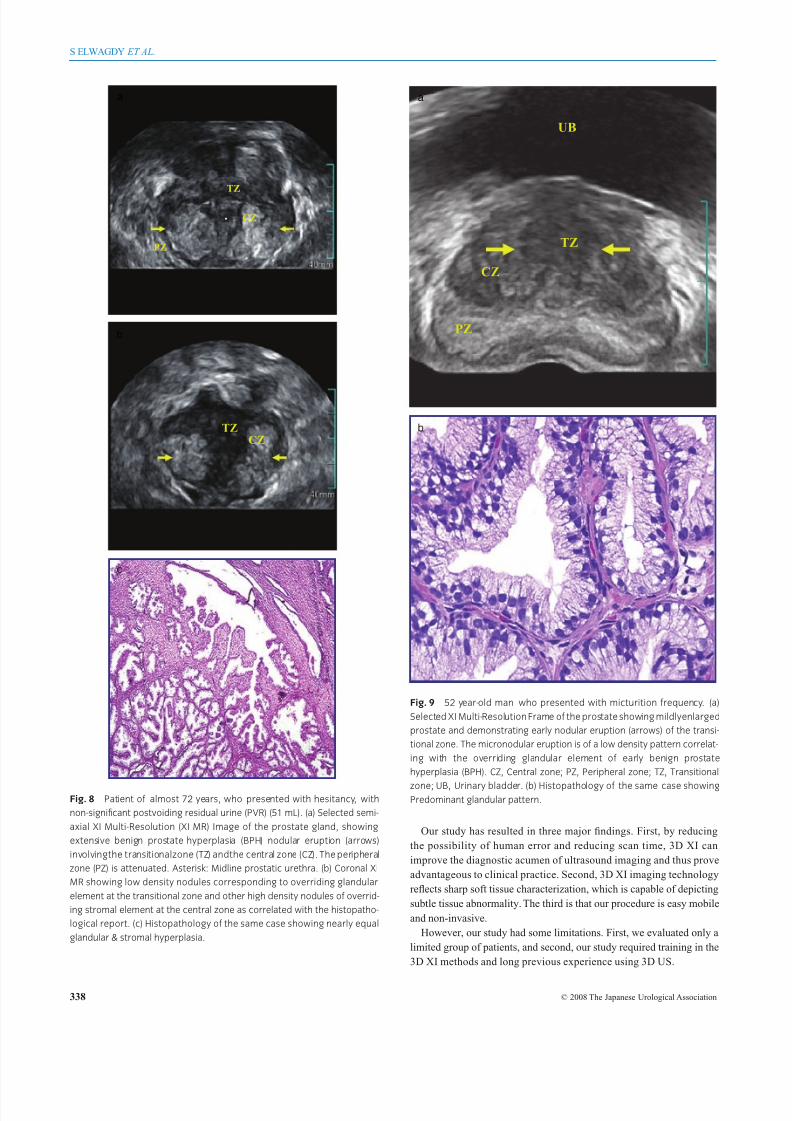
nodules are sometimes coexistent (Fig. 8) and mostly reflect variance in
echo-intensities. As early as the eruption of BPH nodules, XI-MR
images proved reliable in justifying early detection of glandular-
dominant BPH (Fig. 9).
Histopathological examination of the specimens obtained during
live 3D-TRUS and after TURP showed stromal-dominant hyperplasia
in 58 patients (51.3%), glandular-dominant in 40 instances (35.4%)
and mixed hyperplasia in 15 patients (13.3%). The accuracy of XI
MR in nodular detection and characterization referenced to histo-
pathological reports was about 98.2%. Two cases exceeding the age
of 70 years presented with an indwelled Foley’s catheter were missed
by XI MR in correlation with the pathological type. Both were of
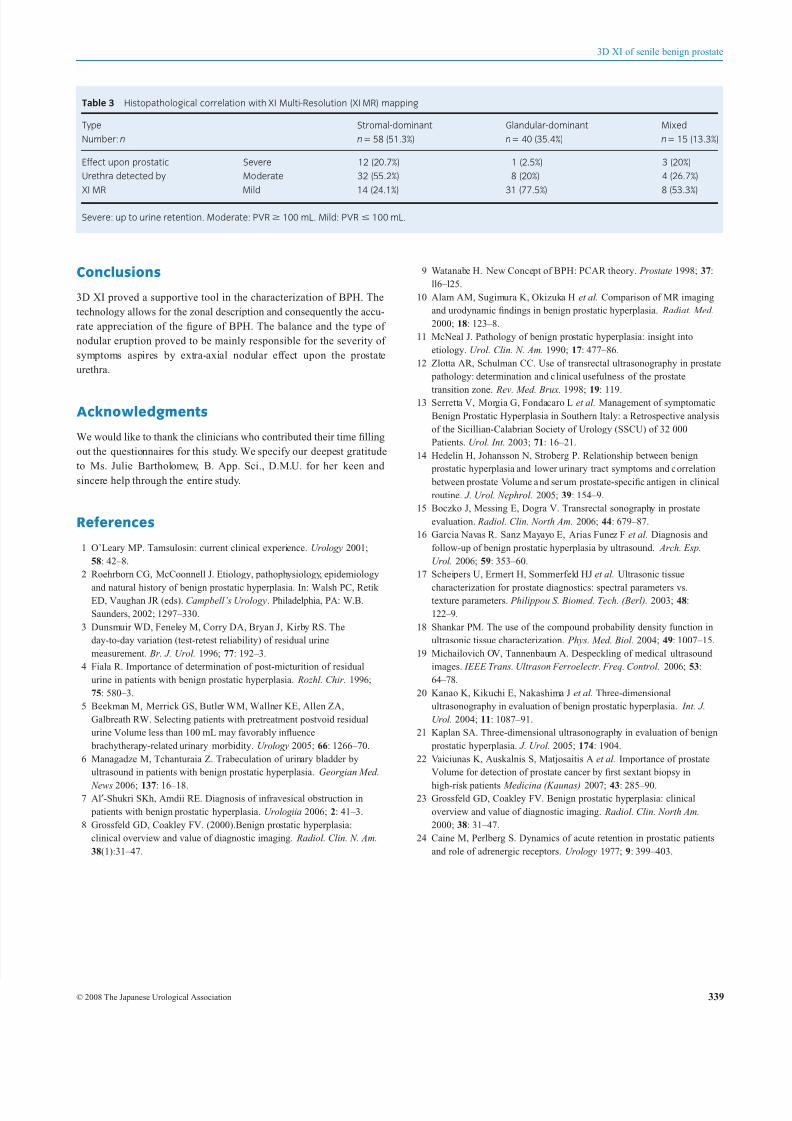
stromal-dominant hyperplasia. XI MR impressions compared to his-
topathological results and the effect upon the prostatic urethra are
presented in Table 3.
DiscussionThe prevalence and incidence of clinical problems secondary to and
associated with BPH have been increasing as the population ages. 23
BPH is an all-inclusive term for a heterogeneous group of distinct
pathological entities that feature variable changes of the stromal and
glandular elements.10,11 Caine et al .24 have proposed that bladder outlet
obstruction in BPH involves both static and dynamic components. The
static component of obstruction is related to primary prostatic enlarge-
ment, whereas the dynamic component is related to the tone of the
prostatic smooth muscle.
The present prospective study was designed to evaluate the useful-
ness of 3D XI as an update of 3D US imaging in assessing its clinical
benefits in isolated BPH, and to evaluate what findings are mostly
related to the degree of symptoms severity.We agree with Watanabe (1998)9 and Ansari et al . (2000)10 that the
inner gland ratio, protrusion into the bladder, and presence of surgical
capsule are important factors in the probability of outlet stenosis,
increasing in patients with more than two of these criteria. However, we
noticed through 3D XI characterization of the container within the
surgical capsule that the nodular balance and type alongside the
prostatic urethra has additional effects upon the PVR volumes and
symptoms severity. In our series, symptoms could be accounted as
transpires in unbalanced nodular hyperplasia in 14.2% of cases, rather
than balanced nodular eruption (85.8%).
Therefore, we think that neither the elasticity of the surgical capsule
nor the voluminous central gland are the standard compulsory factors
in symptom severity, since we have recorded some instances (16 out of
113 patients) with small central glands in association with urine reten-
tion. The nodular balance proved mostly responsible for the severity of
symptoms in those cases, aspires by extra-axial nodular effect upon the
prostate urethra.
On the other hand, the symptom severity, when compared and cor-
related with the histopathological results, showed an intimate relation
FF
TZ
CZ
a
b
c
Fig. 6 Moderately enlarged prostate in 63 year-old man who presented
with urine retention. (a) Coronal Multi-Slice View (MSV) with selective XI
Multi-Resolution (XI MR) (left) showing unbalanced nodular hyperplasia of
thetransitional (TZ) andcentral (CZ) zones.The urethral midline alignmentis
distorted (arrows). (b) Axial MSV with selective XI MR (lower right) showingthe conglomeration of nodules forming a bigger nodular structure (arrow).
(c) Coronal MSV with XI MR (left) after the indwelling of Foley’s catheter
released urine retention.
S ELWAGDY ET AL.
336 © 2008 The Japanese Urological Association
8/10/2019 Bening Prostatic Hyperplasia
http://slidepdf.com/reader/full/bening-prostatic-hyperplasia 6/8
to the nodular type. The symptom severity was more evident in cases
that proved histological stromal-dominant nodular hyperplasia (20.7%)
and mixed hyperplasia (20%) and the less severe symptoms were
recorded in glandular-dominant hyperplasia (2.5%).
Analyzing the nodular echo-intensities on 3D XI images compared
to histopathology showed that the increase in echo-intensity of the
nodules is directly proportional to the ratio of stroma within the nodule.
The nodules may possibly show high or low echo-intensity compared to
the surrounding central gland parenchyma when the stromal or glan-
dular element of the nodules, respectively, is dominant. However, in
some older patients, the estimation of echo-intensities of the nodules is
not simple, because of the overall relative increase in echo-intensity of
the central gland. In such instances, the isoechoic prostate nodules can be indirectly recognized by 3D XI’s computed MSV, through the dem-
onstration of the derangement of the course of the prostate urethra.
Nevertheless, a more precise detection of isoechoic n odules is predict-
able during processing XI MR and manipulating the image factors
either by changing the threshold levels or gamma correction until the
demonstration of the nodules improved. Those factors are not stable in
every case, but they are dependant upon viewing the best choice of
resolution.
3D XI proved diagnostic accuracy in 57 out of 58 cases with stromal-
dominant hyperplasia (98.3%) and 14 out of 15 instances (93.3%) in
mixed hyperplasia. However, the diagnostic accuracy showed 100% in
cases with glandular dominant hyperplasia.
In view of nodular characterization correlated to the severity of
symptoms, 12 of 58 patients (20.7%) with stromal-dominant hyperpla-
sia had severe urethral stenosis. Whereas 31 of 40 patients (77.5%) with
glandular-dominant hyperplasia had none of the XI MR criteria for
severe stenosis, they showed a PVR below 100 cm3, apart from eight
cases (20%) that showed stenotic figures of the prostatic urethra due to
unbalanced conglomeration of peri-urethral nodules. In addition,
patients presenting with nodular hyperplasia resulting from a sizable
solitary adenoma or conglomeration of multiple small nodules devel-
oped a noteworthy compression effect proportional to the size of the
lesion. Quite the opposite, patients with huge prostates and an even
nodular eruption of the transitional and central zones had a non-
significant volume of PVR; hence, the clinical symptoms of BPHnodular effect were primarily dependant upon the pattern of nodular
balance bordering the prostatic urethra.
In the present study, the overall sensitivity of XI MR on BPH
characterization achieved 98.2%, which is a major improvement
over the levels reported with conventional 2D TRUS. Our results pro-
vided excellent resolution and diagnostic authority of internal pros-
tatic anatomy, detection of BPH nodules and their balance and
information data regarding the ratio of stromal to glandular tissue in
the prostate.
Therefore, 3D XI as an upgrade of 3D US, is superior in the evalu-
ation of urinary outlet stenosis in patients with BPH, without being
restricted by high cost or limited availability.
Fig. 7 Moderately enlarged prostate, with
postvoiding residual urine (PVR) of about
65 mL. (a) Coronal Multi-Slice View (MSV) set
with selected XI Multi-Resolution (XI MR)
image showing the balanced micronodularpattern of the transitional (TZ) and central (CZ)
zones of the prostate. The echo-intensity of
thenodules (arrows)is higheron therightthan
the left and relatively more coalescing on the
right. (b) The benign prostate hyperplasia
(BPH) nodulesin coronal plane arealmost even
on each side of the prostatic urethra, which is
represented midline position (arrowhead). The
bright echo-intensity of the nodular pattern is
noted and correlating with the histopathologi-
cal report of the overriding stromal element.
(c) Histopathology of the same case showing
stromal overgrowth.
TZ
CZ
a
b c
3D XI of senile benign prostate
© 2008 The Japanese Urological Association 337
8/10/2019 Bening Prostatic Hyperplasia
http://slidepdf.com/reader/full/bening-prostatic-hyperplasia 7/8
Our study has resulted in three major findings. First, by reducing
the possibility of human error and reducing scan time, 3D XI can
improve the diagnostic acumen of ultrasound imaging and thus prove
advantageous to clinical practice. Second, 3D XI imaging technology
reflects sharp soft tissue characterization, which is capable of depicting
subtle tissue abnormality. The third is that our procedure is easy mobile
and non-invasive.
However, our study had some limitations. First, we evaluated only a
limited group of patients, and second, our study required training in the
3D XI methods and long previous experience using 3D US.
TZCZ
TZ
CZ
PZ
a
b
c
Fig. 8 Patient of almost 72 years, who presented with hesitancy, with
non-significant postvoiding residual urine (PVR) (51 mL). (a) Selected semi-
axial XI Multi-Resolution (XI MR) Image of the prostate gland, showing
extensive benign prostate hyperplasia (BPH) nodular eruption (arrows)
involvingthe transitionalzone (TZ) andthe central zone (CZ). The peripheral
zone (PZ) is attenuated. Asterisk: Midline prostatic urethra. (b) Coronal XI
MR showing low density nodules corresponding to overriding glandular
element at the transitional zone and other high density nodules of overrid-
ing stromal element at the central zone as correlated with the histopatho-
logical report. (c) Histopathology of the same case showing nearly equal
glandular & stromal hyperplasia.
TZ
CZ
PZ
UB
a
b
Fig. 9 52 year-old man who presented with micturition frequency. (a)
Selected XI Multi-Resolution Frame of the prostate showing mildlyenlarged
prostate and demonstrating early nodular eruption (arrows) of the transi-
tional zone. The micronodular eruption is of a low density pattern correlat-
ing with the overriding glandular element of early benign prostate
hyperplasia (BPH). CZ, Central zone; PZ, Peripheral zone; TZ, Transitional
zone; UB, Urinary bladder. (b) Histopathology of the same case showingPredominant glandular pattern.
S ELWAGDY ET AL.
338 © 2008 The Japanese Urological Association
8/10/2019 Bening Prostatic Hyperplasia
http://slidepdf.com/reader/full/bening-prostatic-hyperplasia 8/8
Conclusions
3D XI proved a supportive tool in the characterization of BPH. The
technology allows for the zonal description and consequently the accu-
rate appreciation of the figure of BPH. The balance and the type of
nodular eruption proved to be mainly responsible for the severity of
symptoms aspires by extra-axial nodular effect upon the prostate
urethra.
Acknowledgments
We would like to thank the clinicians who contributed their time filling
out the questionnaires for this study. We specify our deepest gratitude
to Ms. Julie Bartholomew, B. App. Sci., D.M.U. for her keen and
sincere help through the entire study.
References
1 O’Leary MP. Tamsulosin: current clinical experience. Urology 2001;
58: 42–8.
2 Roehrborn CG, McCoonnell J. Etiology, pathophysiology, epidemiology
and natural history of benign prostatic hyperplasia. In: Walsh PC, Retik ED, Vaughan JR (eds). Campbell’s Urology. Philadelphia, PA: W.B.
Saunders, 2002; 1297–330.
3 Dunsmuir WD, Feneley M, Corry DA, Bryan J, Kirby RS. The
day-to-day variation (test-retest reliability) of residual urine
measurement. Br. J. Urol. 1996; 77: 192–3.
4 Fiala R. Importance of determination of post-micturition of residual
urine in patients with benign prostatic hyperplasia. Rozhl. Chir. 1996;
75: 580–3.
5 Beekman M, Merrick GS, Butler WM, Wallner KE, Allen ZA,
Galbreath RW. Selecting patients with pretreatment postvoid residual
urine Volume less than 100 mL may favorably influence
brachytherapy-related urinary morbidity. Urology 2005; 66: 1266–70.
6 Managadze M, Tchanturaia Z. Trabeculation of urinary bladder by
ultrasound in patients with benign prostatic hyperplasia. Georgian Med.
News 2006; 137: 16–18.7 Al′-Shukri SKh, Amdii RE. Diagnosis of infravesical obstruction in
patients with benign prostatic hyperplasia. Urologiia 2006; 2: 41–3.
8 Grossfeld GD, Coakley FV. (2000).Benign prostatic hyperplasia:
clinical overview and value of diagnostic imaging. Radiol. Clin. N. Am.
38(1):31–47.
9 Watanabe H. New Concept of BPH: PCAR theory. Prostate 1998; 37:
ll6–l25.
10 Alam AM, Sugimura K, Okizuka H et al. Comparison of MR imaging
and urodynamic findings in benign prostatic hyperplasia. Radiat. Med.
2000; 18: 123–8.
11 McNeal J. Pathology of benign prostatic hyperplasia: insight into
etiology. Urol. Clin. N. Am. 1990; 17: 477–86.
12 Zlotta AR, Schulman CC. Use of transrectal ultrasonography in prostate
pathology: determination and c linical usefulness of the prostate
transition zone. Rev. Med. Brux. 1998; 19: 119.13 Serretta V, Morgia G, Fondacaro L et al. Management of symptomatic
Benign Prostatic Hyperplasia in Southern Italy: a Retrospective analysis
of the Sicillian-Calabrian Society of Urology (SSCU) of 32 000
Patients. Urol. Int. 2003; 71: 16–21.
14 Hedelin H, Johansson N, Stroberg P. Relationship between benign
prostatic hyperplasia and lower urinary tract symptoms and c orrelation
between prostate Volume a nd ser um prostate-specific antigen in clinical
routine. J. Urol. Nephrol. 2005; 39: 154–9.
15 Boczko J, Messing E, Dogra V. Transrectal sonography in prostate
evaluation. Radiol. Clin. North Am. 2006; 44: 679–87.
16 Garcia Navas R. Sanz Mayayo E, Arias Funez F et al. Diagnosis and
follow-up of benign prostatic hyperplasia by ultrasound. Arch. Esp.
Urol. 2006; 59: 353–60.
17 Scheipers U, Ermert H, Sommerfeld HJ et al. Ultrasonic tissue
characterization for prostate diagnostics: spectral parameters vs.texture parameters. Philippou S. Biomed. Tech. (Berl). 2003; 48:
122–9.
18 Shankar PM. The use of the compound probability density function in
ultrasonic tissue characterization. Phys. Med. Biol. 2004; 49: 1007–15.
19 Michailovich OV, Tannenbaum A. Despeckling of medical ultrasound
images. IEEE Trans. Ultrason Ferroelectr. Freq. Control. 2006; 53:
64–78.
20 Kanao K, Kikuchi E, Nakashima J et al. Three-dimensional
ultrasonography in evaluation of benign prostatic hyperplasia. Int. J.
Urol. 2004; 11: 1087–91.
21 Kaplan SA. Three-dimensional ultrasonography in evaluation of benign
prostatic hyperplasia. J. Urol. 2005; 174: 1904.
22 Vaiciunas K, Auskalnis S, Matjosaitis A et al. Importance of prostate
Volume for detection of prostate cancer by first sextant biopsy in
high-risk patients Medicina (Kaunas) 2007; 43: 285–90.23 Grossfeld GD, Coakley FV. Benign prostatic hyperplasia: clinical
overview and value of diagnostic imaging. Radiol. Clin. North Am.
2000; 38: 31–47.
24 Caine M, Perlberg S. Dynamics of acute retention in prostatic patients
and role of adrenergic receptors. Urology 1977; 9: 399–403.
Table 3 Histopathological correlation with XI Multi-Resolution (XI MR) mapping
Type
Number: n
Stromal-dominant
n = 58 (51.3%)
Glandular-dominant
n = 40 (35.4%)
Mixed
n = 15 (13.3%)
Effect upon prostatic Severe 12 (20.7%) 1 (2.5%) 3 (20%)
Urethra detected by Moderate 32 (55.2%) 8 (20%) 4 (26.7%)
XI MR Mild 14 (24.1%) 31 (77.5%) 8 (53.3%)
Severe: up to urine retention. Moderate: PVR 100 mL. Mild: PVR 100 mL.
3D XI of senile benign prostate
© 2008 The Japanese Urological Association 339
Recommended