Pratap Sagar Tiwari, Resident, Internal Medicine
BASAL GANGLIA & PARKINSON’S
DISEASE

THIS IS NOT PSART OF THE PPT BUT FOR THE
ONES WHO DOWNLOADED THIS.
• Note to those who downloaded this file :
• In many of the slides for eg regarding the basal ganglia
pathways…..only the illustration was shown in the slide and
most of the part was narrated and so this downloaded ppt may
not contain the portion of my narrations during the semiar but
still much info is hidden in the notes added in each slides.

TOPIC OUTLINES
• Basal Ganglia and its components
• Dopamine
• Basal Ganglia-thalamo-cortical motor circuit
• Parkinsonism and Parkinson’s disease
• Clinical features/workup/management
• Atypical Parkinsons/Secondary
• Recent Advances

NERVOUS SYSTEM DEVELOPMENT :
ANATOMICAL SUBDIVISIONS
Primary division of
neural tube
Sec. subdivision Final segments
Prosencephalon 1. Telencephalon
2. Diencephalon
1. The cortex,
Caudate, Putamen, Globus pallidus
2. Thalamus, hypothalamus, subthalamus,
subthalamic nuclei
Mesencephalon Mesencephalon
Mesencephalon (Midbrain),
Substantia nigra pars compacta (SNc),
Substantia nigra pars reticulata (SNr)
Rombencephalon 1. Metencephalon
2. Myelencephalon
1. Pons and cerebellum
2. Medulla

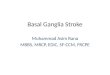
BASAL GANGLIA
Picture taken from : http://withfriendship.com/user/boss/basal-ganglia.php

Picture taken from : http://www.macalester.edu/academics/psychology/whathap/ubnrp/dopahypoweb04/josh%20page%202.html

BASAL GANGLIA: COMPONENTS
Corpus striatum = striatum (caudate + putamen ) ,Pallidum , Nucleus Accumbents
Substantia Nigra
Subthalamic Nucleus
Picture taken from :http://webspace.ship.edu/cgboer/basalganglia.html

BG COMPONENTS: CAUDATE Begins just behind the frontal lobe and curves
back towards the occipital lobe.
Involved in learning and memory .[1]
Overacticve : OCD
Underactive : ADD, depression, aspects of
schizophrenia
Also involved in PAP syndrome., Huntington
Disease
Reference:
1. Graybiel AM (2005) The basal ganglia: learning new tricks and loving it. Curr Opin
Neurobiol 15:638-644.

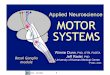
BG COMPONENTS: PUTAMEN lies just under & behind the front of the caudate.
It appears to be involved in coordinating automatic
behaviors and influence various type of learning.A/w
Tourette Syndrome.
The caudate nucleus is largely separated from the
lentiform complex by the anterior limb of the IC.

1. head of caudate nucelus
2. body of caudate nucelus
3. caudatolenticular
gray bridge
4. putamen
5. tail of caudate nucleus
6. external segment of
globus pallidus
7. internal segment of
globus pallidus
8. amygdaloid body
9. nucleus accumbens
Medial surface of basal ganglia

Picture Reference : http://thalamus.wustl.edu/course/cerebell.html

UNDERSTANDING THE PATHWAYS
Picture Reference: http://thalamus.wustl.edu/course/cerebell.html

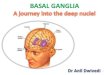
UNDERSTANDING THE PATHWAYS
D1 = direct pathway
D2 = Indirect pathway
Striatum
Gpi /SNr
Gpi / SNr
STN
Gpe and STN
Striatum & GPe
Inhibits
Excitatory influences

DOPAMINE: SYNTHESIS
Dopamine
L-DOPA Tyrosine
Tyrosine Hydroxylase
dopa decarboxylase

DOPAMINE : DEGRADATION

PARKINSONISM AND PARKINSON’S DISEASE
• Parkinsonism is a neurological syndrome characterized by
tremor, hypokinesia, rigidity, and postural instability.
• The underlying causes of parkinsonism are numerous.
• The neurodegenerative condition Parkinson's disease (PD) is
the most common cause of parkinsonism as it accounts for
~75% of all cases of parkinsonism

PARKINSON’S DISEASE; ETIOLOGY
• Genetic causes
• Environmental causes
• Oxidation Hypothesis
• Alpha-synuclein

GENETIC CAUSES OF PD
Table Ref: Powers A.C. Kasper DL, Fauci AS, Hauser SL, Longo DL, Jameson JL, Loscalzo J. Harrison's principles of internal medicine (18th ed.) .Parkinson's Disease and Other Movement Disorders . New York: McGraw-Hill .; 2011; 372

PARKINSON’S DISEASE : CLINICAL FEATURES.
Cardinal features Other motor features Nonmotor features
Bradykinesia
Rigidity
Resting Tremor
Gait disturbance/postural
instability
Micrographia
Masked facies
Reduced eye blink
Soft voice
Freezing
Anosmia
Mood disorders eg
depression
Sleep disturbances
Autonomic disturbances
Cognitive impairment/
dementia
Table Ref: Powers A.C. Kasper DL, Fauci AS, Hauser SL, Longo DL, Jameson JL, Loscalzo J. Harrison's principles of internal medicine (18th ed.) .Parkinson's Disease and Other Movement Disorders . New York: McGraw-Hill .; 2011; 372

PARKINSON’S DISEASE : CLINICAL FEATURES.
Cardinal features Other motor features Nonmotor features
Bradykinesia
Rigidity
Resting Tremor
Gait disturbance/postural
instability
Micrographia
Masked facies
Reduced eye blink
Soft voice
Freezing
Anosmia
Mood disorders eg
depression
Sleep disturbances
Autonomic disturbances
Cognitive impairment/
dementia
Table Ref: Powers A.C. Kasper DL, Fauci AS, Hauser SL, Longo DL, Jameson JL, Loscalzo J. Harrison's principles of internal medicine (18th ed.) .Parkinson's Disease and Other Movement Disorders . New York: McGraw-Hill .; 2011; 372

DEMENTIA IN PARKINSONS DISEASE
• The prevalence of dementia in Parkinson disease ranges from
20-40%. 1
• Hoops et al found that in dementia in Parkinson disease, the
Montreal Cognitive Assessment (MoCA) is superior to the
MMSE for screening for mild cognitive impairment or dementia.
As a screening instrument, MoCA was better than MMSE (64%
versus 54% correct diagnoses).2
References:
1. Weintraub D, Comella CL, Horn S. Parkinson's disease--Part 3: Neuropsychiatric symptoms. Am J Manag Care. Mar 2008;14(2 Suppl):S59-69
2. Hoops S, Nazem S, Siderowf AD, Duda JE, Xie SX, Stern MB. Validity of the MoCA and MMSE in the detection of MCI and dementia in Parkinson disease. Neurology.
Nov 24 2009;73(21):1738-45.

PARKINSON’S DISEASE: WORKUP • Positron emission tomography (PET) and single-photon emission CT (SPECT)
may show findings consistent with Parkinson disease but these are not easily
available. and olfactory testing may provide early evidence of Parkinson disease
but is not routinely needed.
• A sustained response to dopamine medications helps confirm the diagnosis.
• When an erroneous diagnosis of Parkinson disease is made, the most likely
correct diagnoses are essential tremor and the atypical parkinsonisms (MSA,
PSP, CBD).
• In patients with an unusual presentation, diagnostic testing may be indicated to
exclude other disorders in the differential diagnosis. Such tests may include
serum ceruloplasmin, or lumbar puncture.
Next: Diagnostic criterias

UKPDS BRAIN BANK CRITERIA1
• Step 1 – Diagnosis of a parkinsonian syndrome: bradykinesia +
• Rest tremor/ Rigidity/ Postural instability
• Step 2 – Exclusion criteria for PD
• Hx of strokes, HI, antipsychotic/DA depleting drugs, encephalitis, 1+ relatives, neg response to Ldopa, other neuro signs, tumour/hydroceph on imaging
• Step 3 – supportive criteria for PD: 3+ of:
• Unilat onset, rest tremor, progressive, persistent assymetry, excellent response to Ldopa, severe Ldopa induced chorea, Ldopa reponse over5 yrs, clinical course>10 yrs
Reference:
1. Hughes AJ, Daniel SE, Kilford L, Lees AJ. Accuracy of clinical diagnosis of idiopathic Parkinson’s disease. A clinico-pathological study of 100 cases.
JNNP 1992;55:181-184.

PARKINSON’S DISEASE: MANAGEMENT
• Dopaminomimetic therapy should be initiated as soon as the patient's
symptoms begin to interfere with quality of life.
• The aim of all dopaminomimetic strategies is to restore dopamine
transmission in the striatum.
This is accomplished by
I. stimulating postsynaptic receptors (directly with dopamine agonists),
II. increasing dopamine precursor availability (levodopa),
III. blocking the metabolism of levodopa in the periphery and in the brain, and
blocking the catabolism of dopamine at the synapse.

COMMON TREATMENT STRATEGY
Table Ref: Powers A.C. Kasper DL, Fauci AS, Hauser SL, Longo DL, Jameson JL, Loscalzo J. Harrison's principles of internal medicine (17h ed.) .Parkinson's Disease and Other Movement Disorders . New York: McGraw-Hill .; 2008; 372

PHARMACOLOGICAL THERAPY
Dopamine
L-DOPA Tyrosine
Tyrosine Hydroxylase
dopa decarboxylase
Levodopa
Carbidopa
Doesn’t
cross
BBB

• Levodopa-induced motor complications consist of fluctuations in motor
response and involuntary movements known as dyskinesias .
• With continued treatment, however, the duration of benefit becomes
progressively shorter . This loss of benefit is known as the wearing-off effect.
• At the same time, many patients develop dyskinesias. These tend to occur
at the time of maximal clinical benefit and peak plasma concentration (peak-
dose dyskinesia).
• In more advanced states, patients may cycle between "on" periods
complicated by disabling dyskinesias and "off" periods in which they suffer
severe parkinsonism.

COMMON TREATMENT STRATEGY
Table Ref: Powers A.C. Kasper DL, Fauci AS, Hauser SL, Longo DL, Jameson JL, Loscalzo J. Harrison's principles of internal medicine (17h ed.) .Parkinson's Disease and Other Movement Disorders . New York: McGraw-Hill .; 2008; 372

DOPAMINE AGONISTS: DOSING
Dopamine Agonists Initial Dosing Monotherapy As Adjuncts to LD
Pramipexole 0.125 mg tid 1.5–4.5 mg/d 0.375–3.0 mg/d
Ropinirole 0.25 mg tid 12–24 mg/d 6–16 mg/d
Rotigotine 2 mg/24 h 6 mg/d 2–6 mg/d
Bromocriptine
1.25 mg bid to tid 7.5–15 mg/d 3.75–7.5 mg/d
Apomorphine sc 2–8 mg
Drug Dosing Ref: Powers A.C. Kasper DL, Fauci AS, Hauser SL, Longo DL, Jameson JL, Loscalzo J. Harrison's principles of internal medicine (18th ed.) .Parkinson's Disease and Other Movement Disorders . New York: McGraw-Hill .; 2011; 372

COMMON TREATMENT STRATEGY
Table Ref: Powers A.C. Kasper DL, Fauci AS, Hauser SL, Longo DL, Jameson JL, Loscalzo J. Harrison's principles of internal medicine (17h ed.) .Parkinson's Disease and Other Movement Disorders . New York: McGraw-Hill .; 2008; 372

PHARMACOLOGICAL THERAPY Selegiline
Rasagiline
Entacapone
Tolcapone
Inhibitors of MAO-B block central dopamine metabolism and increase synaptic concentrations of the neurotransmitter.

MAO-B INHIBITORS /COMT INHIBITORS
DRUG DOSING
MAO-B Inhibitors Dosage
Selegiline 5 mg bid
Rasagiline 1.0 mg QAM
COMT Inhibitors
Entacapone 200 mg with each levodopa dose
Tolcapone 100–200 mg tid
Adverse effects of Tolcapone : Hepatotoxicity
Drug Dosing Ref: Powers A.C. Kasper DL, Fauci AS, Hauser SL, Longo DL, Jameson JL, Loscalzo J. Harrison's principles of internal medicine (18th ed.) .Parkinson's Disease and Other Movement Disorders . New York: McGraw-Hill .; 2011; 372

COMMON TREATMENT STRATEGY
Table Ref: Powers A.C. Kasper DL, Fauci AS, Hauser SL, Longo DL, Jameson JL, Loscalzo J. Harrison's principles of internal medicine (18th ed.) .Parkinson's Disease and Other Movement Disorders . New York: McGraw-Hill .; 2011; 372

TREATING NONMOTOR SYMPTOMS IN PD1
• Sildenafil for erectile dysfunction.
• Polyethylene glycol for constipation.
• Modafinil for excessive daytime somnolence.
• Levidopa/carbidopa should be considered to treat periodic limb
movements of sleep in PD.
• Methylphenidate may be considered for fatigue.
References :
1. Zesiewicz TA, Sullivan KL, Arnulf I, et al. Practice Parameter: treatment of nonmotor symptoms of Parkinson disease: report of the Quality Standards
Subcommittee of the American Academy of Neurology. Neurology. Mar 16 2010;74(11):924-31

NEUROPROTECTIVE THERAPY
• Neuroprotective therapies are defined as those that slow
underlying loss of dopamine neurons.
• Currently, no proven neuroprotective therapies exist for
Parkinson disease.
• MAO-B inhibitors selegiline and rasagiline. coenzyme Q10.

DATATOP (DEPRENYL AND TOCOPHEROL ANTIOXIDATIVE
THERAPY OF PARKINSONISM) STUDY.[1]
• The Parkinson Study Group evaluated the ability of selegiline and tocopherol
to delay progression of clinical disability in early Parkinson disease by
randomizing 800 patients to receive selegiline (10 mg/d) or placebo and
tocopherol (2000 IU/d) or placebo.
• Patients who received placebo required levodopa at a projected median of
15 months from enrollment, while those who received selegiline required
levodopa at a projected median of 24 months after enrollment.
• Tocopherol had no effect on progression of disability.[18]
• Result= Selegiline was shown conclusively to delay the need for levodopa
therapy in early Parkinson disease.
Reference:
1. Effects of tocopherol and deprenyl on the progression of disability in early Parkinson's disease. The Parkinson Study
Group. N Engl J Med. Jan 21 1993;328(3):176-8

STUDY ON RASAGILINE :TEMPO[1]
• In the TEMPO study, treatment with rasagiline at either 1 or 2
mg daily doses over a 6-month period resulted in improved
Unified Parkinson's Disease Rating Scale (UPDRS) scores
relative to placebo.
• Note: TEMPO= TVP-1012 n Early Monotherapy for Parkinson's Disease
Outpatients
Reference :
1. A controlled trial of rasagiline in early Parkinson disease: the TEMPO Study. Arch Neurol. Dec 2002;59(12):1937-43

CO-ENZYME Q10
• In a preliminary study, coenzyme Q10, 1200 mg/d, slowed
progression of Parkinson disease disability. Coenzyme Q10 is a
scavenger of free radicals.[1]
Reference:
1. Shults CW, Oakes D, Kieburtz K, Beal MF, Haas R, Plumb S. Effects of coenzyme Q10 in early Parkinson disease: evidence of slowing
of the functional decline. Arch Neurol. Oct 2002;59(10):1541-50

SURGERY AND OTHERS
• Deep Brain Stimulation
• Neuroablative Lesion Surgeries
• Transplantation
• Gene Therapy

DEEP BRAIN STIMULATION
• A randomized controlled trial in 255 patients with advanced
Parkinson disease found that bilateral DBS was more effective
than best medical therapy in improving on time without
troublesome dyskinesias, motor function, and quality of life at 6
month.[1]
Reference :
1. Weaver FM, Follett K, Stern M, Hur K, Harris C, Marks WJ Jr. Bilateral deep brain stimulation vs best medical therapy
for patients with advanced Parkinson disease: a randomized controlled trial. JAMA. Jan 7 2009;301(1):63-73
Studies have shown that high-frequency electrostimulation in the ventral lateral nucleus (VL) of
the thalamus eliminates tremors in patients

NEUROABLATIVE LESION SURGERIES
• Lesion surgeries involve the destruction of targeted areas of the
brain to control the symptoms of Parkinson disease.
• Lesion surgeries for Parkinson disease have largely been
replaced by DBS.
• The 2 most commonly performed neuroablative procedures are
thalamotomy and pallidotomy.

PARKINSONISM :DIFFERENTIALS Atypical Parkinsonisms
Parkinson's Disease
Genetic
Sporadic
Dementia with Lewy bodies
Multiple-system atrophy
Progressive supranuclear palsy
Corticobasal ganglionic degeneration
Frontotemporal dementia
Secondary Parkinsonism Other Neurodegenerative Disorders
Drug-induced
Tumor
Infection
Vascular
Normal-pressure hydrocephalus
Trauma
Liver failure
Toxins (e.g., CO, Mn, MPTP, cyanide,
methanol, carbon disulfide)
Wilson's disease
Huntington's disease
Neurodegeneration with brain iron
accumulation
SCA 3 (spinocerebellar ataxia)
Fragile X–associated ataxia-tremor-
parkinsonism
Prion disease
Dystonia-parkinsonism (DYT3)
Alzheimer's disease with parkinsonism

ATYPICAL PARKINSONISMS
Conditions Features
Multiple-system atrophy
MSA is suspected when a patient presents with
atypical parkinsonism in conjunction with
cerebellar signs ,cst signs and/or early and
prominent autonomic dysfunction, usually
orthostatic hypotension and poor response to
levodopa/carbidopa
Progressive supranuclear palsy
Progressive supranuclear palsy (PSP) is the most
common Parkinson-plus syndrome.
Early onset of postural instability, supranuclear
gaze palsy, and cognitive dysfunction.
Parkinsonism-dementia-amyotrophic
lateral sclerosis complex

ATYPICAL PARKINSONISMS
Conditions Features
Diffuse Lewy body disease
Progressive dementia is often the first and predominant
symptom. In Parkinson disease, they are mainly observed in
the substantia nigra. In contrast, in DLBD they are scattered
throughout the cerebral cortex and also are seen in the nigra
and other subcortical regions. Its like Alziehmers with
extrapyramidal .
Corticobasal ganglionic
degeneration
Corticobasal ganglionic degeneration (CBGD) is characterized
by frontoparietal cortical atrophy in addition to
degeneration within basal ganglia. Alien limb’ phenomenon.
5 initial presentations, including a
"useless" arm (55%),
gait disorder (27%),
prominent sensory symptoms,
isolated speech disturbance,
behavioral disturbance.[1]
Reference: 1. Rinne JO, Lee MS, Thompson PD, Marsden CD. Corticobasal degeneration. A clinical study of 36 cases.Brain. Oct 1994;117 ( Pt 5):1183-96

HISTORY AND C/F SUGGESTING DX OTHER
THAN PARKINSON'S DISEASE
MSA-p (previously striato-nigral degeneration
MSA-c (previously olivopontocerebellar atrophy

THANKYOU
References:
• Table Ref: Powers A.C. Kasper DL, Fauci AS, Hauser SL, Longo DL, Jameson JL, Loscalzo J. Harrison's
principles of internal medicine (18th ed.) .Parkinson's Disease and Other Movement Disorders . New York: McGraw-Hill .; 2011; 372
• www.emedicine.com
• http://en.wikipedia.org/

PARKINSON OR PARKINSON PLUS ?
• An inadequate response to treatment
Other clinical clues suggestive of Parkinson-plus syndromes include the following:
• Early onset of dementia ,postural instability
• Early onset of hallucinations or psychosis with low doses of levodopa/carbidopa or dopamine agonists
• Ocular signs, such as impaired vertical gaze, blinking on saccade, square-wave jerks, nystagmus, blepharospasm, and apraxia of eyelid opening or closure
• Pyramidal tract signs not explained by previous stroke or spinal cord lesions
• Autonomic symptoms such as postural hypotension and incontinence early in the course of the disease
• Alien-limb phenomenon
• Marked symmetry of signs in early stages of the disease

ESSENTIAL TREMOR
• The most common early sign of PD – in about three-quarters of cases – is a 4–6 Hz, unilateral resting tremor.
• The cardinal difference between essential tremor and the tremor of PD is that the former is associated with voluntary movements or postures and is absent at rest, whilst the tremor of PD is present at rest.
Other characteristics that may help to distinguish essential tremor from that of PD include:
• onset early in adult life when PD is rare
• bilateral onset
• head and voice tremor
• family history
• other features of PD are absent
• unresponsive to levodopa
• alcohol responsiveness
• beta-blocker or primidone/gabapentin responsive
• positional and kinetic tremor.

UK BRAIN BANK DIAGNOSTIC CRITERIA
STEP ONE: DIAGNOSIS OF PARKINSONISM
BRADYKINESIA AND AT LEAST ONE OF THE FOLLOWING:
• Muscular Rigidity
• 4-6 Hz Resting Tremor
• Postural Instability not caused by primary visual, vestibular, cerebellar or Proprioceptive
dysfunction
Hughes AJ, Daniel SE, Kilford L, Lees AJ. Accuracy of clinical diagnosis of idiopathic
Parkinson’s disease. A clinico-pathological study of 100 cases. JNNP 1992;55:181-184.

UK BRAIN BANK DIAGNOSTIC CRITERIA
STEP TWO: FEATURES TENDING TO EXCLUDE PARKINSON’S DISEASE AS THE CAUSE OF PARKINSONISM
• History of repeated strokes/repeated head injury /encephalitis
• More than one affected relative
• Sustained remission
• Strictly unilateral features after 3 years
• Supranuclear gaze palsy
• Cerebellar signs
• Early severe autonomic involvement
• Early severe dementia with disturbances of memory, language, and praxis
• Babinski’s sign
• Presence of cerebral tumor or communicating hydrocephalus on CT scan
• MPTP exposure
a positive predictive value of 98.6% for the clinical diagnosis of PD

UK BRAIN BANK DIAGNOSTIC CRITERIA
STEP THREE: FEATURES THAT SUPPORT A DIAGNOSIS OF PARKINSON’S DISEASE, 3
OR MORE REQUIRED
• Unilateral onset
• Rest tremor present
• Progressive disorder
• Persistent asymmetry affecting the side of onset most
• Excellent (70 – 100%) response to levodopa
• Severe levodopa-induced chorea
• Levodopa response for equal to or greater than 5 years
• Clinical course of equal to or greater than 10 years
Three or more required for diagnosis of definite Parkinson’s disease in combination with step 1

DOPAMINERGIC PATHWAYS
mesolimbic transmits D from the ventral tegmental area to the
nucleus accumbens. The VTA is located in the
midbrain, and the nucleus accumbens is in the
limbic system.
schizophrenia
mesocortical transmits D from the VTA to the frontal cortex. schizophrenia
nigrostriatal The nigrostriatal pathway transmits dopamine
from the substantia nigra to the striatum. This
pathway is associated with motor control.
Parkinson disease
Tubero
infundibular
transmits D from the hypothalamus to the
pituitary gland. This pathway influences the
secretion of certain hormones, including prolactin.
"Infundibular" in the word "tuberoinfundibular"
refers to the infundibulum out of which the
pituitary gland develops.
hyperprolactinaemia

PATHOLOGY
Pathologically, the hallmark features of PD are
• degeneration of dopaminergic neurons in the substantia nigra pars compacta (SNc),
• reduced striatal dopamine,
• intracytoplasmic proteinaceous inclusions known as Lewy bodies
Neuronal degeneration with inclusion body formation can also affect
• cholinergic neurons of the nucleus basalis of Meynert (NBM),
• norepinephrine neurons of the locus coeruleus (LC),
• serotonin neurons in the raphe nuclei of the brainstem, and
• neurons of the olfactory system, cerebral hemispheres, spinal cord, and peripheral autonomic nervous system.

DIETERY CONSIDERATIONS
• Protein-restricted diets may be useful in patients who are experiencing motor fluctuations
with long-term levodopa treatment.
• Levodopa is transported into the brain by a carrier protein that also transports large
neutral amino acids found in dietary protein.
• Consequently, high-protein meals can compete for the transport of levodopa and reduce
or eliminate its effects.
• A protein-restricted diet can therefore improve the response to levodopa and can be
useful in patients with otherwise refractory motor fluctuations.
Recommended