LIVER TRAUMA
Dr. Niyaz Mohamed SInstitute of Digestive and Hepatobiliary
SciencesSAKRA WORLD HOSPITAL

CASE CAPSULE
• 40 year old male presented with alleged H/o fall from a height of 15 feet, sustaining multiple injuries.
• Had multiple rib fractures with right sided pneumothorax.
• Had multiple long bone fractures and pelvis fracture.

• H/o of pain abdomen following blunt injury abdomen.
• No Co morbidities.
• Hemodynamically stable.
• P/A- Tenderness in Right hypochondrium.
• Hemoglobin on presentation- 7.2g%.

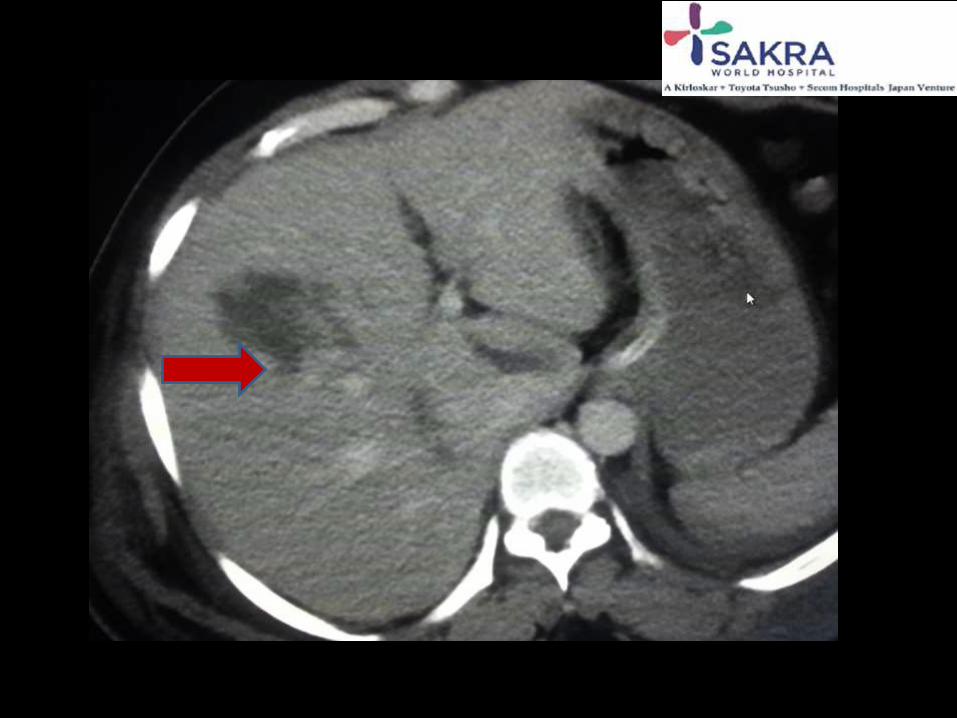
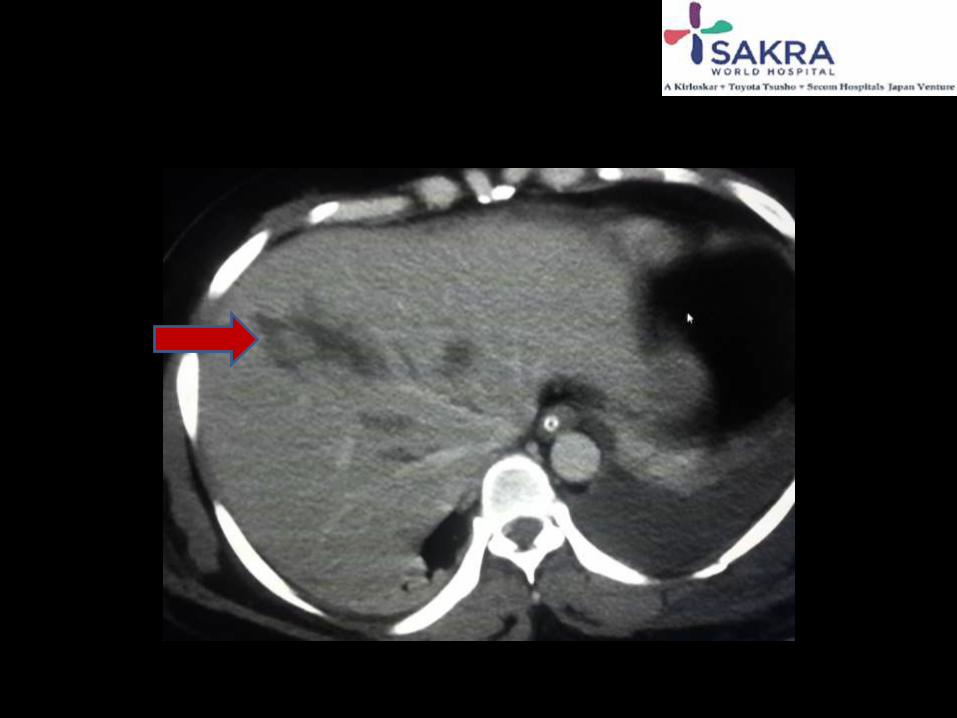
• CECT abdomen done-Grade 3-4 liver laceration with no arterial and venous extravasation
• Minimal sub-hepatic free fluid and pelvic extraperitoneal hematoma.


MANAGEMENT
• Patient hemodynamically stabilized and put on mechanical ventillatory support due to respiratory compromise as a result of lung injury and pneumothorax.
• Later underwent tracheostomy.
• Then evaluation and management of liver trauma done.
Management of Liver Trauma• Conservative management
– Monitoring of vital parameters in the ICU
– Serial hemoglobin monitoring
– Urine output
– Tranfused 2 PRBC
• Hospital Course– Patient remained hemodynamically stable,
– no fall in hemoglobin
– Abdominal distension decreased and oral feeds started
• Patient improved and was discharged in a stable state

Surgical treatment Non-operative treatment
World War II – 1965 Post 1965;1981
DPL CECT
Non-operative Management (NOM)
• 50-80% of liver injuries stop bleeding spontaneously
Patient selection criteria:Hemodynamically stable
Absence of peritoneal signs
Presence of neurologic integrity
No associated intra-abdominal injuries
Limited hemoperitoneum (125-250 ml)

Non-operative Management
Prerequisites for non-operative treatment:
– Good quality CT scan
– Experienced radiologist
– Ability to monitor patients in the ICU setting
– Feasibility of immediate surgery if warranted (experienced liver surgeons)

Results of NOM
Author N NOM% Success% Transfusions Mortality
Meredith 70 55 97 5.4 9
Croce 136 82 89 2.4 8
Brasel 82 61 96 6.1 -
Malhotra 661 85 92.5 4.4 7.9

THANK YOU
Recommended

















