ATTITUDES OF PSYCHOLOGISTS TOWARD ALCOHOLISM WILMA J. KNOX
Ve&rana Adminislraliun, Bilozi, MiSaieSipp’
PROBLEM There are continuing efforts by the legal profession to prevent jailing and
punishment of alcoholics. (*, Legal definition of alcoholism as a disease could lead to the use of hospitals to the exclusion of jail for persons labeled “alcoholic”, in addition to their receiving other benefits now offered the sick such as pensions and retirement benefits. In this event, a large and generally demanding group of clients will be competing for services acknowledged to be in short supply throughout the field of psychology (”).
Psychologists have recognized the obligation to state their position on the most appropriate ways the profession can be used to meet human need“). Because the course of the law is extremely difficult to change once it has been codified@), the attitudes of a group of psychologists toward a shift from jail to hospital treatment are examined for consistency and to assess the manpower theoretically available for hospital treatment. Surveys of other professional groups have revealed some negative attitudes toward alcoholics or alcoholic treatment programs, but in- consistency of attitude has not been considered (7 , 9~ lo).
hf ETHOD
A survey of psychologists working in Veterans Administration hospitals was selected, since this group was available to the author and its members come in contact with a patient population containing many with an alcoholic diagnosis(6). A letter and questionnaire were sent to VA psychologists listed in the 1966 AMERICAN PSYCHOLOGICAL ASSOCIATION DIRECTORY, geographical and institutional section. The letter noted a recent court decision that an alcoholic should be immune from jail terms for public drunkenness and raised the question of whether alcoholism should be handled primarily within a treatment setting. Each respondent’s views were sought because of his special knowledge of hospital treatment of alcoholics. The accompanying questionnaire was mimeographed on two and one-half pages.
The survey material was mailed during the first six months of 1967. If no reply was received, a second letter and questionnaire were sent, identical to the first with the exception of the word “Please!” handwritten across the letter. Questionnaires were mailed to 699 psychologists. Of these, 60 letters were unclaimed and returned. Forty-eight replies were received from psychologists no longer employed by the VA; their answers were not used in this analysis. A sample of 591 remained. A total of 480 (81.2%) answers were received from these VA psychologists. Twenty-one (3.6%) returned their questionnaires and declined to answer; 90 psychologists (15.2%) did not reply. Answers were entered on 1BA.I cards and tabulated by a computer.’
The first section of the questionnaire was composed of six items to be completed by checking all of the answers with which the respondent agreed. After making checks, the respondent was asked to rank the answers checked in order of preference. The multiple choices offered to define alcoholism and its cause were derived from a survey(16) of theoretical considerations. The second section was composed of ten items to be completed by choosing one answer which best expressed the respondent’s opinion. Additional space was provided for comments or for descriptions of a treat- ment method that the respondent thought might be effective.*
‘Dr. Douglas Stevens, the VA Southern Research Support Center, and the Univervity of Georgia contributed consultation and computer facilities for the anal seu.
*Dr. Thomas Stritch, Dr. Ray Schrader, Dr. J(M h 6.‘ I)awson, Dr. Itichard Anderson, Dr. Larry Siege1 and other psychology consultants to the h o x i VA Center helped in developjrlg thk questionnaire. Some 236 psychologists oflered perswbal comments on their questioiinaires. ltecurrin sug estions were the use of behavior therapy, family therapy and a new type of institutiori devotJ to tie care of alcoholics.
ATTITUDES OF PSYCHOLOOI8T8 TOWARD ALCOHOLISM 447
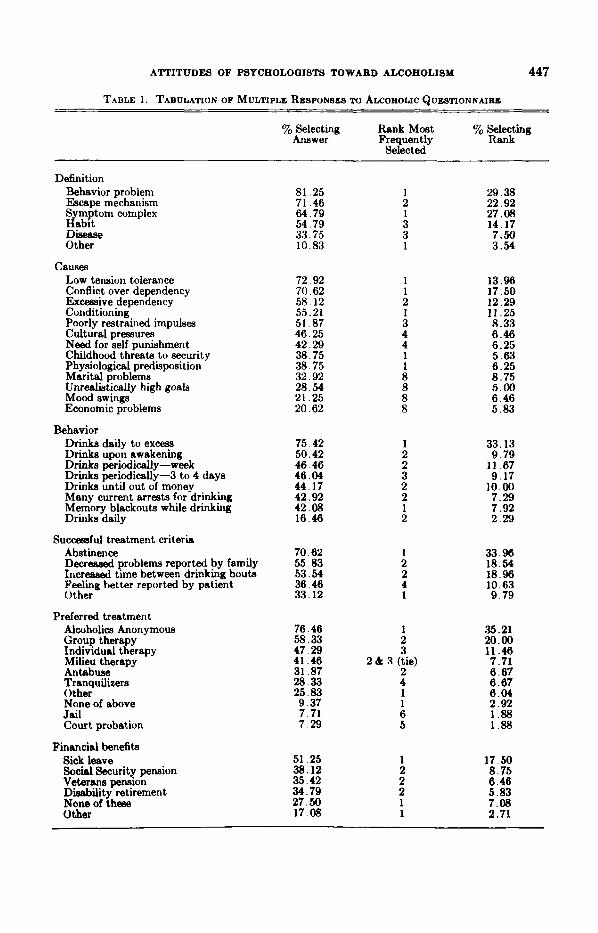
TABLE 1. TABULATION OF MULTIPLE RESPONSES TO ALCOHOLIC QUESTIONNAIRE
yo Selecting Rank Most % Selecting Answer Frequently Rsnk
Selected
Definition Behavior problem Escape mechanism Symptom complex Habit Disease Other
Causes Low tension tolerance Conflict over dependency Exceasive dependency Conditioning Poorly restrained impulses Cultural pressures Need for self punishment Childhood threats to security Physiological predisposition Marital problems Unrealistically high goals
Economic problems
Drinks daily to excess Drinks upon awakening Drinke periodically-week Drink5 periodically-3 to 4 days D r i n h until out of money Many current arrests for drinking Memory blackouts while drinking Drinks daily
Mood 5 W U l g S
Behavior
Successful treatment criteria Abstinence Decregsed problems reported by family Increased time between drinking bouts Feeling better reported by patient Other
Preferred treatment Alcoholics Anonymous Group thera y Individual tRerapy Milieu therapy Antabuse Tranquilizers Other None of above Jail Court probation
Financial benefits Sick leave Social Security pension Veterans pension Disability retirement None of these Other
81.25 71.46 64.79 54.79 33.75 10.83
72.92 70.62 58.12 55.21 51.87 46.25 42.29 38.75 38.75 32.92 28.54 21.25 20.62
75.42 50.42 46.46 46.04 44.17 42.92 42.08 16.46
70.62 55.83 53.54 36.46 33.12
76.46
47.29 41.46 31.87 28.33 25.83 9.37 7.71 7.29
58.33
51.25 38.12 35.42 34.79 27.50 17.08
1 2 1 3 3 1
1 1 2 1 3 4 4 1 1 8 8 8 8
1 2 2 3 2 2 1 2
1 2 2 4 1
1 2 3
2 2 & R (tie)
4 1 1 6 5
1 2 2 2 1 1
29.38 22.92 27.08 14.17 7.50 3.54
13.96 17.50 12.28 11.25 8.33 6.46 6.25 5.63 6.25 8.75 5.00 6.46 5.83
33.13 9.79
11.07 9.17
10.00 7.29 7.92 2.29
33.96 18.54 18.96 10.63 9.79
.%.21 20.00 11.46 7.71 6.67 6.67 6.04 2.92 1.88 1.88
17.50 8.75 6.40 5.83 7.08 2.71
448 WILMA J. KNOX
RESULTS Table 1 shows the tabulation of answers to questions permitting multiple re-
sponses and a ranking of those responses. Psychologists sampled think of alcoholism as (1) a behavior problem, (2) a symptom complex, (3) an escape mechanism, or (4) a habit. The causes of alcoholism are judged to be (1) conflict over dependency needs, (2) low tension tolerance, (3) conditioning, or (4) excessive dependency. Less agreement is found on behavior that characterizes an alcoholic, but drinking daily to excess is considered typical of an alcoholic. Abstinence is the primary index of successful treatment. Increased time between periods of drinking and reports of decreased problems by the family are accepted less frequently. Alcoholics Anony- mous and group therapy are clearly the preferred treatments. About half of the respondents (51.3%) feel the alcoholic is entitled to sick leave. Interestingly, 30 to 35% of the respondents feel alcoholics are also entitled to Social Security benefits, veterans pension, and disability retirement when unable to work because of the effects of drinking.
Psychologists rarely rank disease as a preferred definition of alcoholism and leave i t blank 66.3y0 of the time. In over half of the instances, psychologists do not select as causes of alcoholism: Cultural pressures, need for self-punishment, child- hood threats to security, physiological predisposition, marital problems, unrealistic- ally high goals, mood swings and economic problems. Simply drinking daily is not considered typical of alcoholic behavior. Jail and court probation are rejected as offering treatment potential for the alcoholic.
In responding to questions limited to one answer, the group of psychologists feel the known alcoholic, drunk and staggering on the street, should be taken to a hospital (47.10/,) or taken home (29.4%). Some 5% recommend leaving him alone, 4.6y0 select jail and 10.4y0 select jail only if he starts to drive or commit a crime. The agency selected as the one equipped to handle most of the problems related to alcoholism is primarily AA (40.4%). A neuropsychiatric hospital was selected by 36.7% and a general medical hospital by lo%, a combined selection of hospital care by 46.7%. The courts were rarely selected (1.9%).
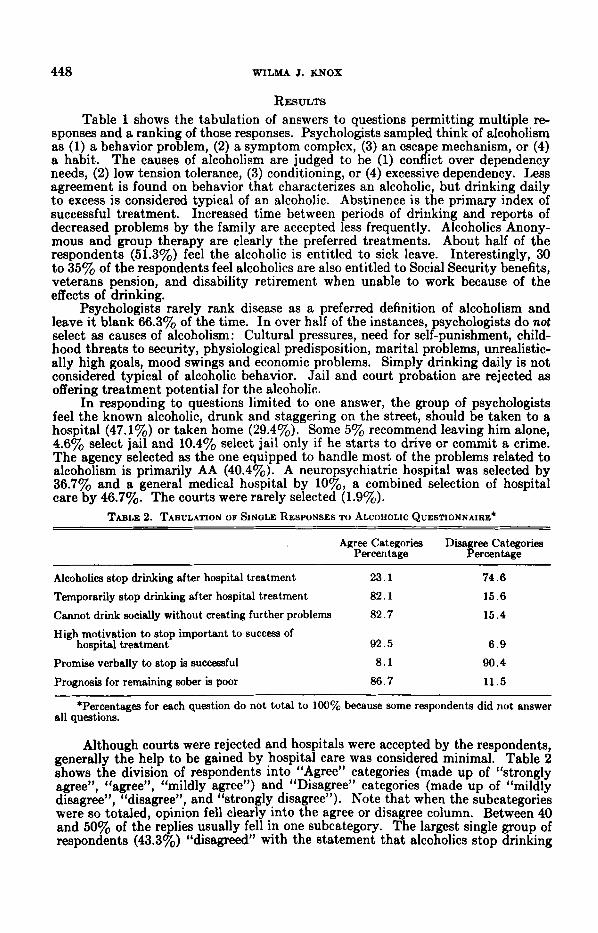
TABLE 2. TABULATION OF SINGLE RESPONSES TO ALCOHOLIC QUESTIONNAIRE*
Agree Categories Disagree Categories Percentage Percentage
Alcoholics stop drinking after hospital treatment 23.1 74.6
Temporarily stop drinking after hospital treatment 82.1 15.6 Cannot drink socially without creating further problems 82.7 15.4
High motivation to stop important to success of hospital treatment 92.5 6 . 9
Promise verbally to stop is successful 8 . 1 90.4
Prognosis for remaining sober is poor 86.7 11.5
all questions.
Although courts were rejected and hospitals were accepted by the respondents, generally the help to be gained by hospital care was considered minimal. Table 2 shows the division of respondents into “Agree” categories (made up of “strongly agree”, “agree”, “mildly agree”) and “Disagree” categories (made up of “mildly disagree”, “disagree”, and “strongly disagree”). Note that when the subcategories were so totaled, opinion fell clearly into the agree or disagree column. Between 40 and 50% of the replies usually fell in one subcategory. The largest single group of respondents (43.3%) “disagreed” with the statement that alcoholics stop drinking
*Percentages for each question do not total to 100% because some respondents did not answer
ATTITUDES OF PSYCHOLOGISTS TOWARD ALCOHOLISM 449
after hospital treatment. “Mildly agree” (42.3y0) was checked most frequently when the statement read alcoholics temporarily decrease drinking following hos- pital treatment. About half of the respondents (46.5%) checked “agree” to a poor prognosis for alcoholics remaining sober, and 52.1y0 “strongly agreed” that high motivation by the alcoholic for hospital treatment is important for treatment suc- cess. Many (42.5y0) “disagreed” with the statement that the alcoholic who promises verbally to stop drinking is likely to be successful. In addition, 36.7% “strongly agreed” that an alcoholic cannot return to social drinking without creating further drinking problems.
Hospital treatment is recommended despite the poor prognosis for alcoholics, but clinical psychologists are largely unwilling to devote much of their own time and efforts to the treatment of alcoholics. When given a choice of selecting one of six figures ranging from 100~o to 0% as the maximum amount of professional time the respondent was willing to devote to the treatment of alcoholism, the largest group (32.7%) chose 10%. Categories representing 25% or less time were selected by 74.8%. Further, reaction to this hypothetical situation was assessed: If you received definitive notification that your present position were to be primarily de- voted to the treatment of alcoholism, you would leave (20.2%), grudgingly comply (21.7%), neutral reaction (36.5%), be somewhat pleased (14.2%), be enthusiastic (4.6%). Thus, 41.9% rate themselves as unwilling to undertake full time work with alcoholics, and 113.8y0 welcome it.
A group of 15 research psychologists waa included in the sample. They were encouraged to reply to the questionnaire even though they felt they did not have special knowledge of hospital treatment of alcoholics. This small sub-group differed from the general sample by selecting conditioning most frequently as the cause of alcoholism and by selecting drinking until out of money and daily drinking as behaviors characteristic of alcoholics. They selected increased time between drink- ing bouts, closely followed by abstinence and decreased problems reported by the family, as criteria for successful treatment. Individual therapy was second to AA as preferred treatment; whereas, the overall sample placed group therapy in second place. Hospitals were selected with greater frequency to handle problems related to alcoholism, including that posed by the known alcoholic drunk and staggering on the street. As might be expected, most of the group were unwilling to devote any time to the treatment of alcoholism and would leave if notified their present position were to be devoted primarily to the treatment of alcoholism.
DISCUSSION One may argue that VA psychologists are atypical clinicians, yet other surveys
of personnel associated with alcoholic treatment show commitment to the im- portance of motivation(O9 la). Other experts note also the poor prognosis for treatr ment, while AA, a group of laymen, popularizes the disease concept‘’, 8 , ‘2). The “typical psychologist” in this study is not committed to the disease concept. Yet he is in favor of removing the alcoholic from jail and placing treatment responsibility in hospitals, although he considers treatment benefits limited at best and d m not wish to be associated with it personally to any degree. If a ychologist is to make
the individual psychologist should examme any inconsistencies in his own attitudes in relation to the gross disparity between the magnitude of the problem, the results of therapy and the facilities for treatment ( 6 e 16).
Perhaps two separate dimensions, pathological drinking behavior and patbolo- gical physical condition due to drinking, become confused, and the possibility of the latter leads to an overcautious call for standardieed hospital admissions. This sur- vey does suggest agreement that hospital treatment is not the panacea for patholo- gical drinking behavior and that psychologists have only limited interest in treating hospitalized alcoholics. In reacting to the current societal concern with alcoholism,
cogent comments to courts or 1egislato.rs on the problem, t F is study suggests that
450 WILMA J. KNOX
an appropriate position might be to favor that (1) the present overload of general medical and surgical hospital facilities be spared the addition of alcoholics, and (2) additional experimental clinical work on the problem take place within mental hospitals as current bed capacities permit. Psychologists might consider making their contribution as consultants to the jail system, trying to effect therapeutic changes and treatment within that system. Just as “snake pits” have largely been remade into mental hospitals, so jail could conceivably become protective custody.
SUMMARY Current legal struggles to determine whether alcoholics can be constitutionally
punished for public drunkenness led to this survey of VA clinical psychologists’ attitudes toward alcoholism. A sample of 591 based on the 1966 AMERICAN PSYCHO- LOQICAL ASSOCIATION DIRECTORY yielded an 81.2% return. Opinions regarding definitions of alcoholism, causes, typical behaviors, indices of successful treatment and preferred treatments are reported. Recommended monetary benefits, re- actions to public drunkenness, and treatment or incarceration agencies were also surveyed. Prognoses for sobriety and social drinking after treatment were assessed, as well as the time the respondent was personally willing to devote to the treatment of alcoholism.
The disease concept of alcoholism was not widely accepted by the respondents. High agreement was found in rejecting the court as the agency to handle most of the problems related to alcoholism. Some type of hospitalization or AA was preferred. High agreement was also found in a generally poor prognosis for sobriety following hospital treatment, and few psychologists were willing to devote a major proportion of their time to treatment of alcoholism. The inconsistencies involved in these opinions were discussed, and more consistent alternatives were offered.
REFERENCES 1. Alcoholice Anon-8. (2nd ed.) New York: Alcoholics Anonymous World Services, Inc., 1955. 2. AMERICAN HOSPITAL ASSOCIATION. Supreme Court to decide if chronic alcoholica may be con- victed. Hospilale, 1967,4l, (21), 21. 3. BELLAK L. The concept of acting out: Theoretical considerations. In L. E. Abt and S. L. Weisman (hs.). Acling W. New York: Grune & Stratton, 1965, pp. 3-19. 4. BLAU, T. H. Legislation and professional roles. The CIinical Psycho1 ist, 1967, ZO, 102-103. 5. BLUM, R. H. and FUNKHOUSER, MARY Lou. Legislators’ views on alcxolism: Some dimensions relevant to making new laws. Quart. J . Stud. Ale., 1965, Z6, 666669. 6. HARRINOTON, L. G. and PRICE, A. C. Alcoholism in a geriatric setting. I. Disciplinary problems, marital status and income level. J. Amer. Geridrics So!., 1962, 19, 197-200. 7. JOHNSON, MARILYN W. Nurses speak out on alcoholism. Nursmng Forum, 1965, 4, 16-22. 8. JONES, R. 0. Appraising the total network of services. Hospilal & Community Psychiatry, 1967,
18, 9-10. 9. MOORE, R. A. and BUCHANAN, T. K. State hos itals and alcoholism: A nationwide survey of
treatment techniques and results. Quart. J. Stud. Ape., 1966,67,459-468. 10. ROBINSON, LILLIAN and PODNOS, B. Resistance of psychiatrists in treatment of alcoholism.
J . Nm. M d . Dis., 1966, 143, 22CL.225. 11. Ross, S. Man ower and psychology. Amer. PSydrObgiSt, 1968, 93, 307. 12. SCHULBERO, 6: C. Private practice and community mental health. Hospital & Community
13. ~ T E R N E , MURIEL ’w. & PITIWAN, D. J. The concept of motivation: A source of institutional and professional blockage in the treatment of.alcohol.ics. Quart. J. Stud. Ak . , l(365, 96, 41-57.
14. TIME, INC. Public druiikennevs is a crime. Time, 1‘968, 91, (26), 344-3?. 15.. YOLLES, S. F. and MENDELSON, J. H.. qlcohol and alcoholism. Public Health Semi@ Publica-
lum No. 1640,1967, U. S. Government Prntuig Office, Washwgton, D. C. 16. ZWERLINQ, I. and ROSENBAUM, M. Alcoholic addiction and personality (non-psychotic condi-
tions). In Arieti, S. (Ed.) Amcricon Handbook of PSychdfy. New York: Basic Books, 1959, pp. 623-644.
PS c h d t y , 1968, 17 363-366.
Recommended