Reseamh in Developmental Disabilities, Vol. 14, pp. 299-312, 1993 0891-4222~93 $6.00 + .OO Printed in the USA. All rights reserved. Copyright Q 1993 Pergamon Press Ltd.
Assessment of Depression in Mentally Retarded Adults: Reliability and Validity of the Children’s Depression Inventory (CDI)
Wolfgang Meins
Psychiatric Clinic, University of Hamburg
The applicability of the Children’s Depression Inventory (CDI) in the infor- mant-rating version to mentally retarded adults (5 19 years of age) of all degrees of severity is researched here for the first time. The sample (N = 798) consisted of residents in community-based group homes (56.9%) and residents of a variety of institutions (43.1%). On average, 23 of the 24 CD1 items were to be assessed. Internal consistency, interrater reliability, and the item-total score correlations were adequate. The three factors derived from factor analysis were open to clear interpretation. The CDI score proved to be independent of age, sex, and degree of mental retardation. Persons with behavior problems, psy- chotropic drug treatment, non-Down syndrome status, as well as the residents of a psychiatric clinic, all returned a higher CDI score. Among those having a CDI score > 17 (n = 54). there were 57% with DSM-III-R depressive disorders. These results suggest that the CDI in an informant-rating version is suitable as a diagnostic and screening instrument for mentally retarded adults.
In their review of psychometric assessment of psychiatric disorders in peo- ple with mental retardation, Sturmey, Reed, and Corbett (1991) arrived at the estimate that the depressive disorders sector is currently still the best researched. Nevertheless, markers need to be put down with regard to the sometimes missing or inadequate details on the reliability and validity of individual procedures and the inadequate attention given to people with severe or profound mental retardation. With them, it may be assumed that
The author thanks Dirk Auwetter, Simone Bendig, S&rid Hedtfeld, Jorg Sussmann, and Yvonne Turnier for their invaluable assistance.
Requests for reprints should be sent to Wolfgang Meins, Universitits-Krankenhaus Eppendorf, Psychiatrische Klinik, Martinistrasse 52, W-2000 Hamburg 20, Germany.
299
300 w Meins
depressive disorders will to some extent manifest themselves clinically in other ways than they do with mildly mentally retarded persons (Love & Matson, 1990; Matson, 1983; Pawlarcyzk & Beckwith, 1987). In view of this deficit in research, existing instruments for diagnosing depressive dis- orders in profoundly or severely mentally retarded persons cannot be said to have established validity, which is also true of several instruments for assessing moderately mentally retarded people.
Most studies of depression in the mentally retarded employ self-report scales. Instruments designed for use among the general population (Beck, Carlson, Russell, & Brownfield, 1987; Kazdin, Matson, & Senatore, 1983; Laman & Reiss, 1987) or else specially developed measures, such as the Self-Report Depression Questionnaire (Reynolds & Baker, 1988) or the Psychopathology Instrument for Mentally Retarded Adults (PIMRA) (Matson, Kazdin, & Senatore, 1984; Senatore, Matson, & Kazdin, 1985) have been used. Even when the language has been adapted, the use of self- report scales calls for certain cognitive skills, and thus self-report scales are relevant for a part of the mentally retarded population. Beck, Carlson, Russell, and Brownfield (1987) regard an IQ of at least 55 as adequate. In addition, considerable validation problems exist for interviewing the mental- ly retarded person (Seltzer, 1991) and for self-rating scales of depression (Thompson, 1989). One alternative is rating scales, either completed direct- ly by an informant or conducted in the form of a standardized interview with an informant, irrespective of the degree of serve&y of mental retardation.
The PIMRA, which corresponds to DSM-III diagnostic categories, also offers the advantage of being available in an informant-report version. Apart from relatively high correlations between the informant-rating ver- sion of the PIMRA depression scale (PIMRA-D) and the Hamilton Rating Scale for Depression (Helsel & Matson, 1988; Kazdin, Matson, & Senatore, 1983), the other findings on PIMRA-D are unfortunately not very encour- aging: Factor analyses have failed to recover a depression factor (Linaker, 1991; Matson, Kazdin, & Senatore, 1984; Watson, Aman, & Singh, 1988). Whereas Watson et al. (1988) calculated relatively high but still lower alpha coefficients than those reported by previous studies (Matson et al., 1984; Senatore et al., 1985) Sturmey and Ley (1990) found an unacceptable alpha (0.09). Among no less than 168 institutionalized mentally retarded persons, Linaker and Nitter (1990) were unable to discover a single case of depres- sive disorder by using the PIMRA criteria - and this despite an unusually high prevalence of other diagnostic categories.
Similar diagnostic problems are partly found in children. Here again, one has to depend on statements by third parties. Of the various procedures, the Children’s Depression Inventory (CDI) (Kovacs, 1983, 1985) is regarded as the best researched depression scale in child and adolescent psychiatry and as an appropriate screening procedure for major depression in accor-
Assessment of Depression 301
dance with DSM III-R (Costello & Angold, 1988). Moreover, the CD1 is available in an informant-rating version and had been used in children with (Matson, Barrett, & Helsel, 1988) and without mental retardation (Helsel & Matson, 1984). Using a large sample of mentally retarded adults, the pre- sent research aims to investigate the informant-rating version of the CD1 more closely with respect to reliability and some aspects of validity.
METHOD
Setting
In total, 798 mentally retarded persons were surveyed. Of these, 56.9% (n = 454) were living in community-based group homes in the city of Hamburg, Germany. For them, an attempt was made to include all those residents older than 19 years of age of Hamburg group homes for the men- tally retarded (and supervised around the clock). Participation of more than 80% of this population was achieved. The persons surveyed were dis- tributed among 37 facilities, in which 4-48 people were living. In addi- tion, 43.1% (n = 344) of the total sample were living in different institu- tions located around Hamburg: (a) all (n = 67) the mentally retarded patients in a large psychiatric hospital, these being accomodated in a long term-care department for the mentally retarded; (b) all (n = 131) residents in a small institution for the mentally retarded; (c) all those residents (n = 18) of a nursing home (total beds, 240) classified as mentally retarded following scrutiny of the files; and (d) a representative sample (n = 128) taken on the basis of age, sex, and degree of mental retardation (pro- found/severe vs. moderate/mild) at an institution for the mentally retarded (total beds, 465).
Subjects
The mean age was 37.3 years (range, 20-85, SD = 12.7). The male to female ratio was about 1.0 : 0.9 (see also Table 3). The degree of mental retardation (n = 155, see later) was distributed as follows: profoundly men- tally retarded, 7.8%; severely mentally retarded, 19.4%; moderately men- tally retarded, 33.5%; and mildly mentally retarded, 39.4%.
Assessments
The degree of severity of mental retardation and the occurrence of behavior problems were not researched for the entire sample. For reasons of economy, these variables were derived from a representative subsample of n = 155 persons, stratified for type of residence and randomly selected.
302 W Meins
CDZ. The Children’s Depression Inventory (CDI; Kovacs 1983, 1985) served for the assessment of depression, this in a translation by the author. A modified informant-report was generated by rewording the self-report version in the third person. Of the 27 items in the original CD1 version, three (Nos. 15, 21, and 23) were deleted, because these items required a recent regular attendance at school. Each CD1 item consists of three choic- es, scored from 0 to 2 in the direction of increasing severity. For the 24- item version, the total score consequently can range from 0 (normal) to 48 (severe depression). The CD1 was conducted as a standardized interview with direct-care staff members, each of whom had known the subject for at least 12 months. The interviewers consisted of four medical students at an advanced stage of their studies supervised by the author, all of whom had practical experience with mentally retarded people. To determine some kind of interrater reliability, the CD1 was conducted again after an average of 2 days (range, l-3) for 27 subjects with the same staff member, but this time by the author, who was blind to the exact CD1 score but not blind as to whether the person was a high-scorer (see later) or not.
Psychiatric examination. On average, 4.6 days (range, 1-13) after the CD1 was conducted, the following groups were subject to a psychiatric exami- nation by the author: (a) those group home residents who had a CD1 score of 2 17, which corresponds to the cut-off score recommended by Costello and Angold (1988); (b) all those residents in institutions and clinics who had a score of 2 13; (c) 50% (n = 124) of a random selection of the low scorers (CD1 < 13) from the institutions. Finally, a psychiatric diagnosis was made according to DSM-III-R (American Psychiatric Association, 1987). The concept of major depression was liberalized by (a) a mild form - similar to ICD-10 (World Health Organization, 1991) - in which the subjects met four criteria (out of nine) and (b) a recurrent brief depression (Angst, 1990), though in contrast to Angst, the complete syndrome of major depression lasted at least a week and only one other comparable episode had occurred during the past 12 months.
DAS. The Disability Assessment Schedule (DAS) (Holmes, Shah, & Wing, 1982) was used in an abbreviated version to assess adaptive behavior and behavior problems. The scale was applied as a highly structured interview with direct-care staff members. On the basis of the adaptive behavior total score (range, 15-71), which is highly correlated (rho = 0.75) with the IQ, a classification was made into four degrees of mental retardation ranging from mild to profound (Meins & Sussmann, 1992). Behavior problems were assessed on 15 DAS items with a three-step scale ranging from (1) “considerable problems” through (2) “minor problems” to (3) “non-exis- tent.” The total score could vary accordingly between 15 and 45. Subgroups
Assessment of Depression 303
were formed in such way that those with a total score of less than 40 were categorized as behaviorally disturbed, and those with a total score of 40 to 45 were categorized as not behaviorally disturbed.
Medication and etiology. Along with information on whether Down syn- drome was present, details on regularly prescribed psychotropics (neu- roleptics, antidepressants, antimanics, anxiolytic and hypnotic drugs) were taken from the files. For anticonvulsives also having psychiatric indications (e.g., carbamazepine, valproate), where necessary, the purpose was estab- lished by consultation with the subject’s physician.
Data Analysis
Because the CD1 items were not distributed strictly normally, the item- total score correlations were also calculated as Spearman’s rho. Because not all CD1 items could be assessed for all the persons in the sample, the total score was prorated by multiplying by 24 (maximum item total) and dividing by the number of items that could be assessed. For the factor analysis of the 24 CD1 items, missing values were replaced by the mean. We used a principal component solution followed by (orthogonal) vari- max rotation.
RESULTS
Calculation of CD1 reliability for the entire sample (n = 798) produced a split-half correlation of r = 0.87 (Spearman Brown) and a Cronbach’s alpha of 0.86. Inter-rater reliability was calculated in terms of proportion of agree- ment between two different raters on a total of 648 CD1 items (533/648 = 0.82).
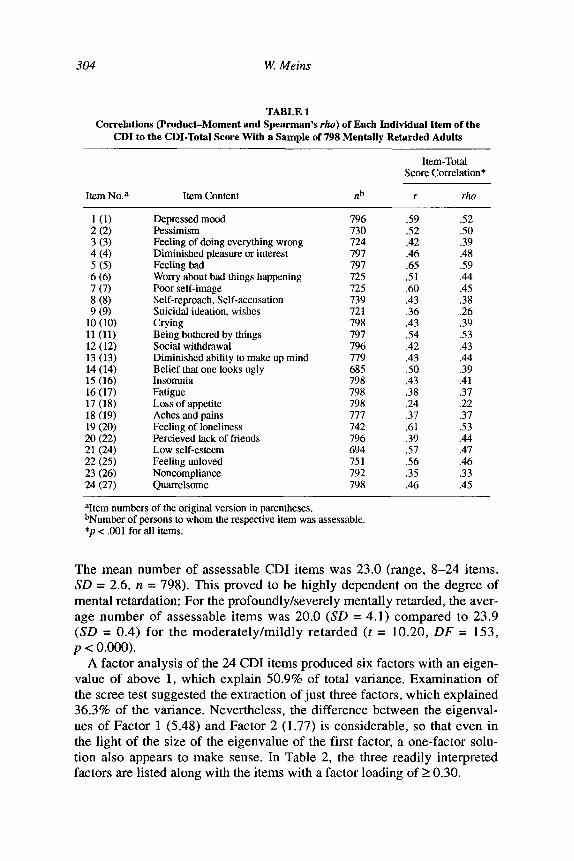
The item-total score correlations (r) listed in Table 1 lie between 0.24 and 0.65 with an average coefficient of 0.48 (on the basis of Fischer’s z transformation). The Spearman’s rho coefficients worked out somewhat lower for most items, indicating that the product-moment correlation may overestimate the strength of association. Two items (9 and 17) showed quite low coefficients, so they may be regarded as possible outliers. After elimination of these two items, the item-total score correlations improved minimally (by 5 0.01). The two items therefore remain in the total score. All in all, the assumption of a unitary concept of depression demonstrated by the CD1 seemed to be appropriate, hence the use of a total score appears to make sense.
It was possible to assess all 24 CD1 items in 81.2% of the subjects and at least 16 of these (67% of items) in 95.2% of subjects. Even item 14, proba- bly the most difficult item, was assessed in 85.8% of subjects (see Table 1).
304 W Meins
TABLE 1 Correlations (Product-Moment and Spearman’s rho) of Each Individual Item of the
CD1 to the CDI-Total Score With a Sample of 798 Mentally Retarded Adults
Item-Total Score Correlation*
Item No.~ Item Content .b r rho
1 (1) 2 (2) 3 (3) 4 (4) 5 (5) 6 (6) 7 (7) 8 (8) 9 (9)
10 (10) ll(11) 12 (12) 13 (13) 14 (14) 15 (16) 16 (17) 17 (18) 18 (19) 19 (20) 20 (22) 21 (24) 22 (25) 23 (26) 24 (27)
Depressed mood 796 .59 Pessimism 730 .52 Feeling of doing everything wrong 724 .42 Diminished pleasure or interest 797 .46 Feeling bad 797 .65 Worry about bad things happening 725 .51 Poor self-image 725 .60 Self-reproach, Self-accusation 739 .43 Suicidal ideation, wishes 721 .36 Crying 798 .43 Being bothered by things 797 .54 Social withdrawal 796 .42 Diminished ability to make up mind 779 .43 Belief that one looks ugly 685 .50 Insomnia 798 .43 Fatigue 798 .38 Loss of appetite 798 .24 Aches and pains 777 .37 Feeling of loneliness 742 .61 Percieved lack of friends 796 .39 Low self-esteem 694 .57 Feeling unloved 751 .56 Noncompliance 792 .35 Quarrelsome 198 .46
.52
.50
.39
.48
.59
.44
.45
.38
.26
.39
.53
.43
.44
.39
.41
.31
.22
.31
.53
.44
.47
.46
.33
.45
aItem numbers of tbe original version in parentheses. bNumber of persons to whom the respective item was assessable. *p < .OOl for all items.
The mean number of assessable CD1 items was 23.0 (range, 8-24 items, SD = 2.6, n = 798). This proved to be highly dependent on the degree of mental retardation: For the profoundly/severely mentally retarded, the aver- age number of assessable items was 20.0 (SD = 4.1) compared to 23.9 (SD = 0.4) for the moderately/mildly retarded (t = 10.20, DF = 153, p < 0.ooo).
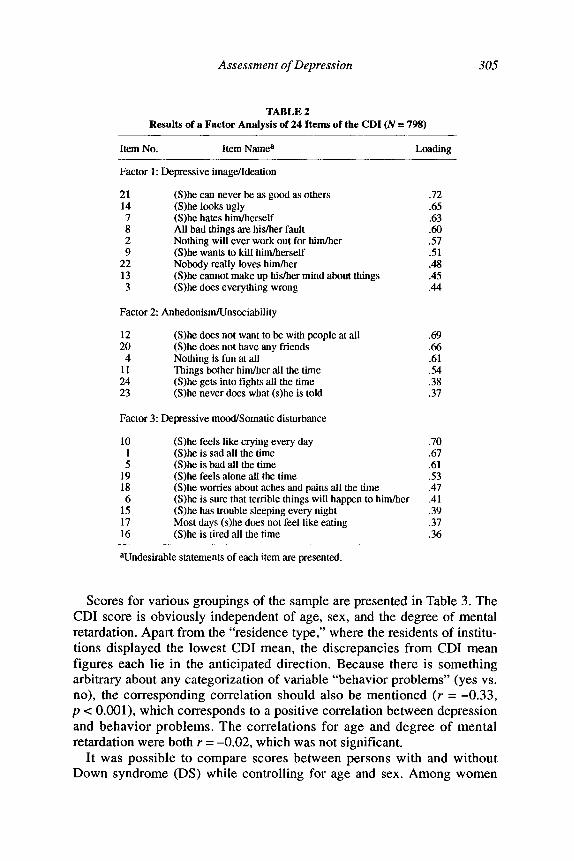
A factor analysis of the 24 CD1 items produced six factors with an eigen- value of above 1, which explain 50.9% of total variance. Examination of the scree test suggested the extraction of just three factors, which explained 36.3% of the variance. Nevertheless, the difference between the eigenval- ues of Factor 1 (5.48) and Factor 2 (1.77) is considerable, so that even in the light of the size of the eigenvalue of the first factor, a one-factor solu- tion also appears to make sense. In Table 2, the three readily interpreted factors are listed along with the items with a factor loading of 2 0.30.
Assessment of Depression 305
TABLE 2 Results of a Factor Analysis of 24 Items of the CD1 (N = 798)
Item No. Item Namea Loading
Factor 1: Depressive image/Ideation
21 14
; 2 9
22 13 3
(S)he can never be as good as others .72 (S)he looks ugly .65 (S)he hates him/herself .63 AlI bad things are his/her fault x0 Nothing will ever work out for him/her 57 (S)he wants to kill him/herself .51 Nobody really loves him/her .48 (S)he cannot make up his/her mind about things .45 (S)he does everything wrong .44
Factor 2: AnhedonismKJnsociability
12 (S)he does not want to be- with people at all .69 20 (S)he does not have any friends 66 4 Nothing is fun at all .61
11 Things bother him/her all the time 54 24 (S)he gets into tights all the time .38 23 (S)he never does what (s)he is told .37
Factor 3: Depressive mood/Somatic disturbance
10 (S)be feels like crying every day 1 (S)he is sad all the time 5 (S)he is bad all the time
19 (S)he feels alone all the time 18 (S)he worries about aches and pains all the time 6 (S)he is sure that terrible things will happen to him/her
15 (S)he has trouble sleeping every night 17 Most days (s)he does not feel like eating 16 (S)he is tired all the time
Wndesirable statements of each item are presented.
.70
.67
.61
.53
.47
.41
.39
.37
.36
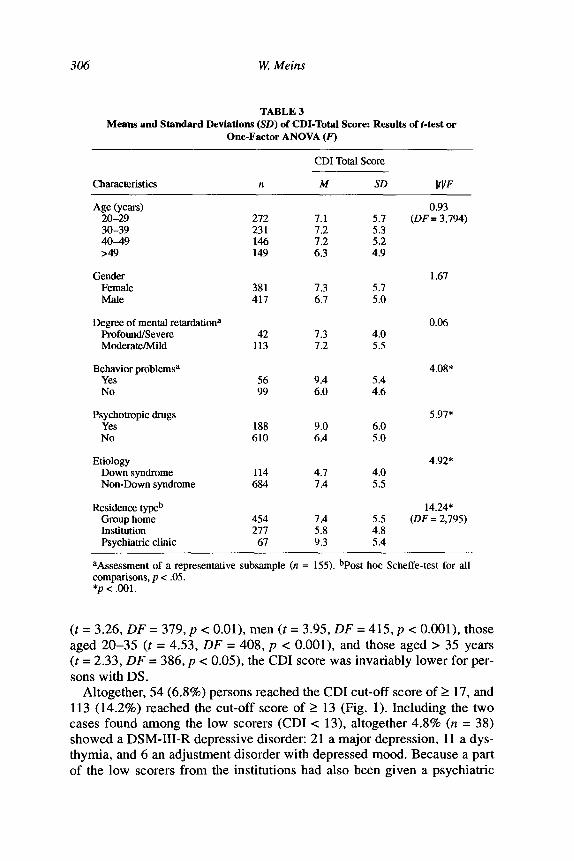
Scores for various groupings of the sample are presented in Table 3. The CD1 score is obviously independent of age, sex, and the degree of mental retardation. Apart from the “residence type,” where the residents of institu- tions displayed the lowest CD1 mean, the discrepancies from CD1 mean figures each lie in the anticipated direction. Because there is something arbitrary about any categorization of variable “behavior problems” (yes vs. no), the corresponding correlation should also be mentioned (r = -0.33, p c O.OOl), which corresponds to a positive correlation between depression and behavior problems. The correlations for age and degree of mental retardation were both r = -0.02, which was not significant.
It was possible to compare scores between persons with and without Down syndrome (DS) while controlling for age and sex. Among women
306 W Meins
TABLE 3 Means and Standard Deviations (SD) of CDI-Total Score: Results of f-test or
One-Factor ANOVA (8’)
CD1 Total Score
charactt_?ristics n M SD IWF
Age (years) 20-29 30-39 40-49 >49
Gender Female Male
Degree of mental retardationa Profound/Severe Moderate/Mild
Behavior problemsa Yes No
Psychotropic drugs Yes No
Etiology Down syndrome Non-Down syndrome
Residence typeb Croup home Institution Psychiatric clinic
0.93 (DF = 3,794) 272 7.1 5.7
231 7.2 5.3 146 7.2 5.2 149 6.3 4.9
1.67 381 7.3 5.7 417 6.7 5.0
0.06 42 7.3 4.0
113 7.2 5.5
4.08* 56 9.4 5.4 99 6.0 4.6
5.97* 188 9.0 6.0 610 6.4 5.0
4.92* 114 4.7 4.0 684 7.4 5.5
14.24* (DF=2,795) 454 7.4 5.5
277 5.8 4.8 67 9.3 5.4
aAssessment of a representative subsample (n = 155). hPost hoc Scheffe-test for all comparisons, p < .05. *p < ,001.
(t = 3.26, DF = 379, p c O.Ol>, men (t = 3.95, DF = 415, p c O.OOl), those aged 20-35 (f = 4.53, DF = 408, p c O.OOl), and those aged > 35 years (t = 2.33, DF = 386, p < 0.05), the CD1 score was invariably lower for per- sons with DS.
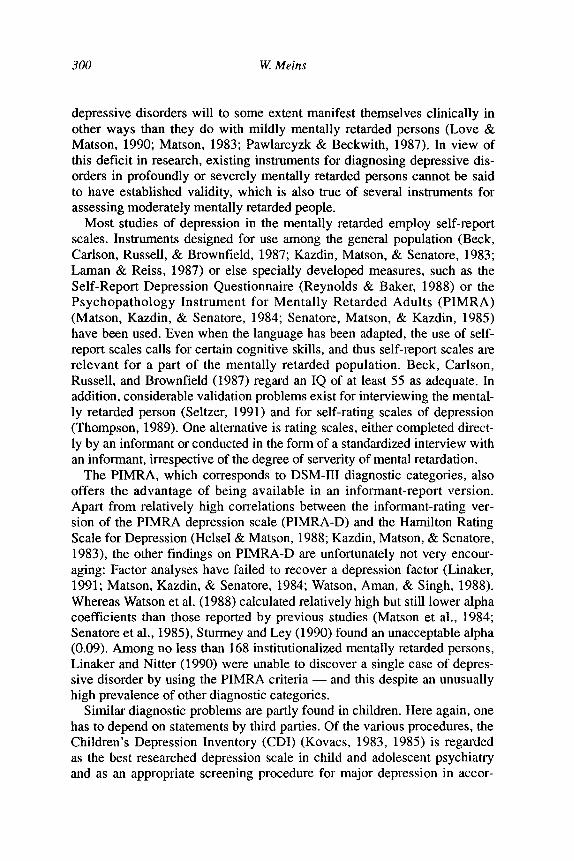
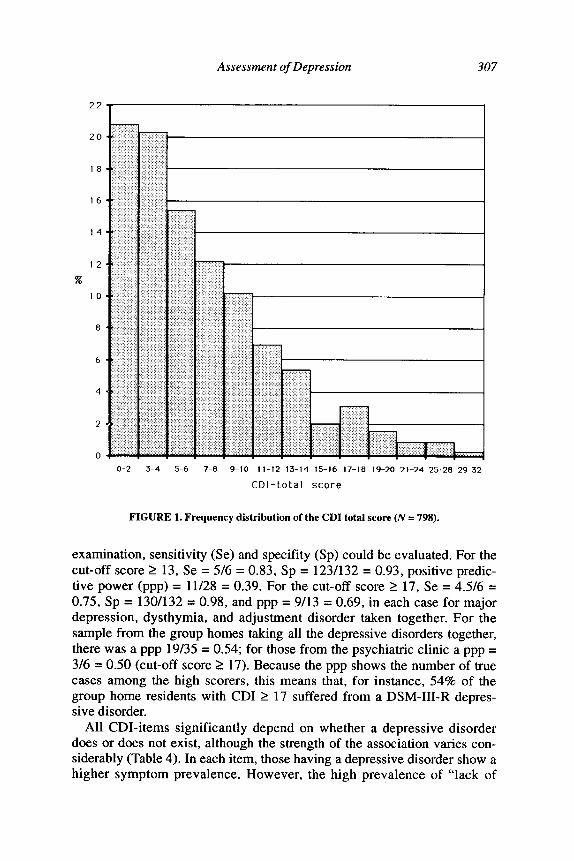
Altogether, 54 (6.8%) persons reached the CD1 cut-off score of 2 17, and 113 (14.2%) reached the cut-off score of 2 13 (Fig. 1). Including the two cases found among the low scorers (CD1 < 13), altogether 4.8% (n = 38) showed a DSM-III-R depressive disorder: 21 a major depression, 11 a dys- tbymia, and 6 an adjustment disorder with depressed mood. Because a part of the low scorers from the institutions had also been given a psychiatric
Assessment of Depression 307
16
14
12
x
IO
a
6
4
2
0
o-2 3-4 5-6 7-8 9-10 11-12 13-14 15-16 17-18 19-20 21-24 25-28 29-32
CDI-total score
FIGURE 1. Frequency distribution of the CD1 total score (N = 798).
examination, sensitivity (Se) and specifity (Sp) could be evaluated. For the cut-off score 2 13, Se = 516 = 0.83, Sp = 123/132 = 0.93, positive predic- tive power (ppp) = 11/28 = 0.39. For the cut-off score 2 17, Se = 4.5/6 = 0.75, Sp = 130/132 = 0.98, and ppp = 9/13 = 0.69, in each case for major depression, dysthymia, and adjustment disorder taken together. For the sample from the group homes taking all the depressive disorders together, there was a ppp 19/35 = 0.54; for those from the psychiatric clinic a ppp = 3/6 = 0.50 (cut-off score 2 17). Because the ppp shows the number of true cases among the high scorers, this means that, for instance, 54% of the group home residents with CD1 2 17 suffered from a DSM-III-R depres- sive disorder.
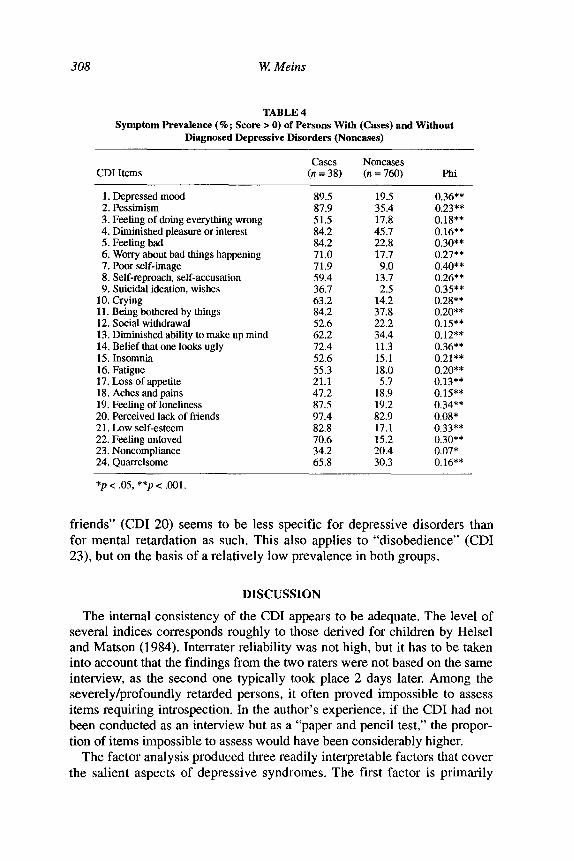
All CDI-items significantly depend on whether a depressive disorder does or does not exist, although the strength of the association varies con- siderably (Table 4). In each item, those having a depressive disorder show a higher symptom prevalence. However, the high prevalence of “lack of
308 W! Meins
TABLE 4 Symptom Prevalence (%; Score > 0) of Persons With (Cases) and Without
Diagnosed Depressive Disorders (Noncases)
CD1 Items Cases Noncases
(II = 38) (n = 760) Phi
1. Depressed mood 89.5 2. Pessimism 87.9 3. Feeling of doing everything wrong 51.5 4. Diminished pleasure or interest 84.2 5. Feeling bad 84.2 6. Worry about bad things happening 71.0 7. Poor self-image 71.9 8. Self-reproach, self-accusation 59.4 9. Suicidal ideation, wishes 36.7
10. Crying 63.2 11. Being bothered by things 84.2 12. Social withdrawal 52.6 13. Diminished ability to make up mind 62.2 14. Belief that one looks ugly 72.4 15. Insomnia 52.6 16. Fatigue 55.3 17. Loss of appetite 21.1 18. Aches and pains 47.2 19. Feeling of loneliness 87.5 20. Perceived lack of friends 97.4 2 1. Low self-esteem 82.8 22. Feeling unloved 70.6 23. Noncompliance 34.2 24. Quarrelsome 65.8
19.5 35.4 17.8 45.7 22.8 17.7 9.0
13.7 2.5
14.2 37.8 22.2 34.4 11.3 15.1 18.0 5.7
18.9 19.2 82.9 17.1 15.2 20.4 30.3
0.36** 0.23** 0.18** 0.16** 0.30** 0.27** 0.40** 0.26** 0.35** 0.28** 0.20** 0.15** 0.12** 0.36** 0.21** 0.20** 0.13** 0.15** 0.34** 0.08* 0.33** 0.30** 0.07* 0.16**
*p < .05, **p < ,001.
friends” (CD1 20) seems to be less specific for depressive disorders than for mental retardation as such. This also applies to “disobedience” (CD1 23), but on the basis of a relatively low prevalence in both groups.
DISCUSSION
The internal consistency of the CD1 appears to be adequate. The level of several indices corresponds roughly to those derived for children by Helsel and Matson (1984). Inter-rater reliability was not high, but it has to be taken into account that the findings from the two raters were not based on the same interview, as the second one typically took place 2 days later. Among the severely/profoundly retarded persons, it often proved impossible to assess items requiring introspection. In the author’s experience, if the CD1 had not been conducted as an interview but as a “paper and pencil test,” the propor- tion of items impossible to assess would have been considerably higher.
The factor analysis produced three readily interpretable factors that cover the salient aspects of depressive syndromes. The first factor is primarily
Assessment of Depression 309
based on items ranging from a view of self distorted by depression, to crazy notions of blame, to ideas of suicide. The second factor was based on items indicating loss of pleasure in life and unsociableness. In addition, the factor seemed to have something to do with noncompliance and irritability. The loadings for these items are rather low, however. The third factor was typified by depressive mood and, to a lesser extent, by somatic and vegeta- tive disturbances. There were few similarities with the factor structure found by Helsel and Matson (1984) in children who were not mentally retarded, except for overlaps between their Factor 3 (interpersonal relation) and Factor 2.
The results concerning sensitivity and specifity apply to a relatively small sample and should be regarded as tentative. If, however, one takes the often highly favourable positive predictive values into account, it does seem likely that the CD1 can be a satisfactory screening instrument for depressive disorders in mentally retarded adults. The different prevalence rates found in this extensive study fit in with the rates of major depression and dysthymia in the general population (Meins, 1992). In view of the lack of valid surveys of the prevalence of depressive disorders in mentally retarded people (Fleisher & Weiler, 1990; Meins, in press), this may be regarded as a validation for the screening properties of the CDI.
CD1 scores proved to be unrelated to age. Whether this finding would also apply to samples containing a higher proportion of older persons, especially those with DS, is questionable, because a higher prevalence of dementia may be reckoned with in such samples (Lai & Williams, 1989; Lund, 1985). The partial overlapping of symptoms of depression and dementia (Harper & Wadsworth, 1990) could indicate higher CD1 scores. Somewhat unexpected was the lack of any CD1 difference between men and women, because a higher rate of depressive disorders, for example, major depression, among women is well documented (Weissman, 1987). On the other hand, Angst and Dobler-Mikola (1984) reported that the sex ratio for depressive disorders is significantly influenced by the fact that women report more symptoms. With an informant-rating procedure, how- ever, this effect may be felt considerably less, if at all. Another possibility that remains open is that this sex ratio does not extend to persons suffering from mental retardation.
CD1 scores were also unrelated to the degree of mental retardation. It therefore seems improbable that mental retardation represents a direct risk factor for depressive disorders..Instead, we may assume an interaction between the degree of mental retardation and known risk factors, such as, for example, social support (Billings, Cronkite, & Moos, 1983; Brown, Andrews, Harris, Adler, & Bridge, 1986; Reiss & Benson, 1985) or differ- ent effects on different types of depressive disorders, for example, major depression versus dysthymia.
310 W Meins
The higher CD1 score in the group with behavior problems and in the one being treated with psychotropic drugs can be basically explained by two - nonalternative - factors: (a) In mentally retarded people depres- sive disorders may present with nonspecific behavior problems (Sovner, 1986). (b) A higher CD1 score partly is an expression of nondepressive psychopathology, because the CD1 does not cover only phenomena that are characteristic of depressive disorders.
The differences in the CD1 score for persons with and without DS, respectively, were especially marked. This could be regarded as supporting the notion that psychiatric normality and DS are associated (Gillberg, Persson, Grufman, & Themner, 1986; Meins & Hedtfeld, 1992) also applies specifically for depression.
The high CD1 score for patients in the psychiatric clinic may be attributable to the particularly high rate there of nonspecific psychopatholo- gy. The higher CD1 scores among residents of community-based group homes as compared with those in institutions may be taken as an indication of a higher risk of depression. Even though valid empirical findings on this have so far been lacking, theoretical suppositions (Menolascino, 1990) cer- tainly suggest that for some mentally retarded persons, daily contact and comparison with people of normal intelligence is not beneficial in psy- chohygienic terms.
All in all, the findings presented here suggest that, when applied in cer- tain conditions, the informant-rating version of the CD1 can be usefully employed with people suffering from all degrees of mental retardation. Along with economy in application, it also offers the opportunity for arriv- ing at a uniform or comparable case definition for depressive disorders in people with mental retardation of different degrees. That represents an essential preliminary step for being able to investigate the influence exerted on depressive symptoms by the degree of cognitive impairment, for exam- ple. Whether a standard CD1 cut-off score of 2 17 is the best criterion in this context needs further investigation.
REFERENCES
American Psychiatric Association. (1987). Diagnostic and statistical manual of mental disorders (3rd ed., rev.). Washington, DC: Author.
Angst, J. (1990). Recurrent brief depression: A new concept of depression. Pharmacopsychiatry, 23,63-66.
Angst, J., & Dobler-Mikola, A. (1984). Do the diagnostic criteria determine the sex ratio in depression? Journal of Afictive Disorders, 1, 189-198.
Beck, D. C., Carlson, G. A., Russell, A. T., & Browntield, F. E. (1987). Use of depression rating instruments in developmentally and educationally delayed adolescents. Journal of the American Academy of Child and Adolescent Psychiatry, 26,97-100.
Billings, A. G., Cronkite, R. C., & Moos, R. H. (1983). Social-environmental factors in unipolar depression: Comparison of deptes.sed patients and nondepressed controls. Journal of Abnormal Psychology, 92,119-133.
Assessment of Depression 311
Brown, G. W., Andrews, B., Harris, T. O., Adler, Z., & Bridge, L. (1986). Social support, self- esteem and depression. Psychological Medicine, 16.813-831.
Costello, E. J., 8~ Angold, A. (1988). Scales to assess child and adolescent depression: Checklists, screens, and nets. Journal of the American Academy of Child and Adolescent Psychiatry, 27, 726-737.
Fleisher, M. H., & Weiler, M. A. (1990). The prevalence and specific aspects of depression in mentally retarded adults. In A. Dosen & F. J. Menolascino (Eds.), Depression in mentally retarded children and adults (pp. 51-61). Leiden: Logon Publications.
Gillberg, C., Persson, E., Grufman, M., & Themner, U. (1986). Psychiatric disorders in mentally retarded urban children and adolescents: Epidemiological aspects. British Journal of Psychiatry, 149.68-74.
Harper, D. C., & Wadsworth, J. S. (1990). Dementia and depression in elders with mental retarda- tion: A pilot study. Research in Developmental Disabilities, 11, 177-198.
Helsel, W. J., & Matson, J. L. (1984). The assessment of depression in children: The internal structure of the Child Depression Inventory (CDI). Behaviour Research and Therapy, 22, 289-298.
Helsel, W. J., & Matson, J. L. (1988). The relationship of depression to social skills and intellectu- al functioning in mentally retarded adults. Journal of Mental Deficiency Research, 32, 411-418.
Holmes, N., Shah, A., & Wing, L. (1982). The Disability Assessment Schedule: A brief screening device for use with the mentally retarded. Psychological Medicine, 12,879-890.
Kazdin, A. E., Matson, J. L., & Senatore, V. (1983). Assessment of depression in mentally retard- ed adults. American Journal of Psychiatry, 140, 1040-1043.
Kovacs, M. (1983). The Children’s Depression Inventory: A self rated depression scale for school- aged youngsters. University of Pittsburgh, School of Medicine. Unpublished manuscript.
Kovacs, M. (1985). The Children’s Depression Inventory (CDI). Psychopharmacology Bulletin, 21,995-998.
Lai, F., & Williams, R. S. (1989). A prospective study of Alzheimer disease in Down syndrome. Archives of Neurology, 46,849-853.
Laman, D. S., & Reiss, S. (1987). Social skill deficiencies associated with depressed mood of mentally retarded adults. American Journal of Mental DeJiciency, 92,2U-229.
Linaker, 0. (1991). DSM-III diagnoses compared with factor structure of the Psychopathology Instrument for Mentally Retarded Adults (PIMRA), in an institutionalized, mostly severely retarded population. Research in Developmental Disabilities, 12, 143-153.
Linaker, 0. M., & Nitter, R. (1990). Psychopathology in institutionalized mentally retarded adults. British Journal of Psychiatry, 156,522-525.
Love, S. R., & Matson, J. L. (1990). Diagnostic instruments for depression in the mentally retard- ed. In A. Dosen & F. J. Menolascino (Eds.), Depression in mentally retarded children and adults (pp. 199-218). Leiden: Logon Publications.
Lund, J. (1985). The prevalence of psychiatric morbidity in mentally retarded adults. Acta Psychiatrica Scandinavica, 72,563-570.
Matson, J. L. (1983). Depression in the mentally retarded: Toward a conceptual analysis of diag- nosis. In M. Hersen, R. M. Eisler & l? M. Miller (Eds.), Progress in behavior modification (pp. 57-79). New York: Academic Press.
Matson, J. L., Barrett, R. P., & Helsel, W. J. (1988). Depression in mentally retarded children. Research in Developmental Disabilities, 9, 39-46.
Matson, J. L., Kazdin, A. E., & Senatore, V. (1984). Psychometric properties of the Psychopathology Instrument for Mentally Retarded Adults. Applied Research in Mental Retardation, 5,81-89.
Meins, W. (1992, August). Prevalence and risk factors of depressive disorders in mentally retard- ed adults. Paper presented at the 9th World Congress of IASSMD. Gold Coast, Australia.
Meins, W. (in press). Affektive Storungen. In U. Koch, W. Lotz, & B. Stahl (Eds.), Psychotherapeutische behandlung bei menschen mit geistiger behinderung. Weinheim: Edition Medizin.
312 W Meins
Meins, W., & Hedtfeld, S. (1992). Prevalence of epilepsy, behavior problems and depression in Down syndrome. In J. J. Roosendaal (Ed.), Mental retardation and medical care (pp. 234-239). Z&t, the Netherlands: Uitgeverij Kerckebosch.
Meins, W., & Sussmann, D. (1992, August). Evaluafion of an aakptive behavior classification. Poster presented at the 9th World Congress of IASSMD. Gold Coast, Australia.
Menolascino, F. J. (1990). Mental retardation and the risk, nature and types of mental illness. In A. Dosen & F. J. Menolascino (Ed%), Depression in menially retarded children and adults (pp. 11-34). Leiden: Logon Publications.
Pawlarcyzk, D., & Beckwith, B. E. (1987). Depressive symptoms displayed by persons with men- tal retardation: A review. Mental Retardation, 25, 325-330.
Reiss, S., & Benson, B. A. (1985). Psychosocial correlates of depression in mentally retarded adults: I. Minimal social support and stigmatization. American Journal of Mental Deficiency, 89,331-337.
Reynolds, W. M., & Baker, J. A. (1988). Assessment of depression in persons with mental retar- dation. American Journal of Mental Retardation, 93,93-103.
Seltzer, M. M. (1991). Nonexperimental and quasi-experimental field research methods. In J. L. Matson & J. A. Mulick (Eds.), Handbook of mental retardation (2nd ed., pp. 603-619). Tarrytown, NY Pergamon Press.
Senators, V., Matson, J. L., & Kazdin, A. E. (1985). An inventory to assess psychopathology of mentally retarded adults. American Journal of Mental Deficiency, 89,459-466.
Sovner, R. (1986). Limiting factors in the use of DSM-III criteria with mentally ill/mentally retarded persons. Psychopharmacology Bulletin, 22, 1055-1059.
Sturmey, P., & Ley, T. (1990). The psychopathology instrument for mentally retarded adults. British Journal of Psychiatry, 156.428-430.
Sturmey, P., Reed, J., & Corbett, J. (1991). Psychometric assessment of psychiatric disorders in people with learning difficulties (mental handicap): A review of measures. Psychological Medicine, 21, 143-155.
Thompson, C. (1989). Affective diorders. In C. Thompson (Ed.), The instruments of psychiatric research (pp. 87-126). New York: Wiley.
Watson, J. E., Aman, M.G., & Singh, N. N. (1988). The psychopathology instrument for mentally retarded adults: Psychometric characteristics, factor structure, and relationship to subject char- acteristics. Research in Developmental Disabilities, 9.277-290.
Weissman, M. M. (1987). Advances in psychiatric epidemiology: Rates and risks for major depression. American Journal of Public Health, 17,445-451.
World Health Organization. (1991). Tenth revision of the International Cla.sstfication of Diseases, Chapter V (F). Geneva: Author.
Recommended