
Women and Birth xxx (2014) xxx–xxx
G Model
WOMBI-334; No. of Pages 5
Are midwifery clients in Ontario making informed choices aboutprenatal screening?
Vanessa Dixon *, Nadya Burton 1
Midwifery Education Program at Ryerson University in Toronto, Toronto, ON, Canada
A R T I C L E I N F O
Article history:
Received 16 September 2013
Received in revised form 30 January 2014
Accepted 16 February 2014
Keywords:
Midwifery
Prenatal screening
Informed choice
Counselling
Information provision
Ontario
A B S T R A C T
Background: Informed choice is often lacking in women’s decisions about prenatal screening.
Aim: The aim of this study is to evaluate how well midwives in Ontario, Canada are facilitating informed
choice in this area.
Methods: An Internet-based survey was used to investigate 171 midwifery clients’ knowledge, attitude
towards and experience of prenatal genetic screening tests, and to determine the proportion of study
participants who made an informed choice about prenatal screening.
Findings: All participants demonstrated adequate knowledge of prenatal screening. The vast majority
(93.0%) of participants made an informed choice. Participants who chose to screen had lower knowledge
scores than those who opted out of screening. Client satisfaction rates in regard to care received in this
area ranged from 97% to 100%.
Conclusions: Results of this study suggest that Ontario midwives are effective in conveying information
on prenatal genetic screening, contributing to high levels of client knowledge and satisfaction in
comparison to similar studies in other jurisdictions.
� 2014 Australian College of Midwives. Published by Elsevier Australia (a division of Reed International
Books Australia Pty Ltd). All rights reserved.
Contents lists available at ScienceDirect
Women and Birth
jo u rn al h om ep age: w ww.els evier .c o m/lo c ate /wo mb i
1. Introduction
Prenatal screening tests are blood tests, sometimes offered withan ultrasound, that are carried out prior to the 20th week ofpregnancy. Maternal serum screening was first introduced inOntario in 1991 and the standard tests, which are currentlycovered by provincial health insurance include screening for openneural tube defects, Down Syndrome, Trisomy 13, and Trisomy 18,beginning in the 11th week of pregnancy.1 Among the wellresourced countries in which prenatal screening has becomeincreasingly normative, there is variation in the types of testsavailable as well as their timing and insurance coverage.2,3
However, comparison of international screening guidelines revealsa common purpose of the tests: to inform pregnant women of theprobability that they are carrying a child affected by one of theseconditions.4 Echoing similar recommendations internationally, theSociety of Obstetricians and Gynecologists of Canada (SOGC)
* Corresponding author at: 650 Shaw Street, Toronto, ON M6G 3L7, Canada.
Tel.: +1 647 567 3348.1 Address: Midwifery Education Program, Faculty of Community Services,
Ryerson University, 350 Victoria Street, Toronto, ON M5B 2K3, Canada.
Tel.: +1 416 979 5000x7982.
Please cite this article in press as: Dixon V, Burton N. Are midwiscreening? Women Birth (2014), http://dx.doi.org/10.1016/j.wombi.2
http://dx.doi.org/10.1016/j.wombi.2014.02.003
1871-5192/� 2014 Australian College of Midwives. Published by Elsevier Australia
recommend that the screening tests be offered to all pregnantwomen in the country.1,4
In many ways, this is an accurate description of prenatalscreening. However, prenatal screening is also related to some oflife’s biggest questions: about what kinds of babies women wantand are able to bear and raise; about who should live and whoshould not; about the role of mothers, families, communities andsocieties in caring for and raising children born with disabilities.5
In this light, prenatal screening is more than a set of clinicalprocedures of blood tests and ultrasounds; it is a point of care thattouches on some of our most deeply held social, political andethical values and beliefs.
2. Literature review
Despite the weight of these issues, the process of decidingwhether to undergo screening is one that is normalised to the pointof invisibility within regular obstetrical care.6,7 Indeed, theliterature suggests that many women undergo routine prenatalscreening with relatively little knowledge of the conditions theyare testing for or the efficacy of the test, and without muchdiscussion with their caregiver about the advantages anddisadvantages of testing.8–11
fery clients in Ontario making informed choices about prenatal014.02.003
(a division of Reed International Books Australia Pty Ltd). All rights reserved.

et al. / Women and Birth xxx (2014) xxx–xxx2
G Model
WOMBI-334; No. of Pages 5
Still, research suggests that women want to be offeredscreening through a comprehensive process in which they aregiven enough unbiased information to make a decision that reflectstheir personal values and ethics.12,13 Their desires echo the widelyused definition of informed choice as a decision based on relevantknowledge in which an individual’s decision to screen or not isconsistent with their attitude towards screening and their personalvalues.14
National and international screening guidelines reflect theintention of providing informed choice through ‘‘non-directive’’counselling and respect for a woman’s ‘‘right to accept ordecline’’.4,15,16 While the Association of Ontario Midwives hasnot published midwifery-specific guidelines in this area, theyfollow SOGC recommendations to universally offer prenatalscreening tests and the decision to undertake or decline prenatalscreening is made by each pregnant woman through a process ofinformed choice. The principle of informed choice is, in fact, one ofthe pillars of the model and philosophy of midwifery care inOntario. As such, the College of Midwives of Ontario’s (CMO)Informed Choice Standard applies to the process of informed choicein every facet of midwifery care. In this document, informed choiceis defined as that which:
[t]akes into account factual information, risks and benefits, theclinical experience of the midwife, and the experience, feelings,beliefs, values and preferences of the woman . . . [r]espects andencourages the individual autonomy of the woman as theprimary decision-maker . . . [and] . . . [r]esults in a decisionwhich is made by the woman, which is then supported by themidwife.17
The purpose of this study is to evaluate how midwives inOntario are applying this standard to prenatal screening among asample of their clients. The incidence of informed choice amongmidwifery clients is assumed to serve as an indicator of the qualityof care provision in this area.18 Similar studies have been employedin other jurisdictions such as the Netherlands,1,19 Australia20,21 andthe United Kingdom.22,23 This is the first study of this kind amongmidwifery clients in Canada and is part of a larger project thatexplores how information around prenatal screening is given andreceived by maternity care providers and pregnant women in theprovince of Ontario.24
3. Participants and methods
3.1. Survey
An Internet-based survey questionnaire was designed tomeasure the incidence of informed choice based on the Multi-dimensional Measure of Informed Choice (MMIC)14 as well as thedefinition of informed choice published by the College of Midwivesof Ontario.17 The questions assess clients’ knowledge of andattitudes towards screening. When knowledge scores are deemedadequate, and an individual’s decision to screen or not reflects theirattitudes towards screening, the decision can be deemed to be onebased on informed choice.14
Knowledge was assessed by a series of 14 true or falsestatements about the aims, process and significance of screening.The items in this section were derived from a review of surveyinstruments used in similar studies,18 the MMIC, and theinformation booklet, A Guide to Understanding Prenatal Screening
Tests for Women and their Families25 given to prospective parents byvarious health care providers in Ontario. Responses to thesestatements assess various knowledge domains, including knowl-edge of the conditions being screened for, reasons for screeningand capabilities of the tests. They reflect the knowledge domains
Please cite this article in press as: Dixon V, Burton N. Are midwiscreening? Women Birth (2014), http://dx.doi.org/10.1016/j.wombi.2
developed by Schoonen et al. through expert consensus, althoughwe have adapted them to suit the Ontario context.26
Attitude towards prenatal screening tests was assessed usingSchoonen’s adaptation of Marteau’s attitude assessment from theMMIC.14,18 The items utilise a 7-point Likert scale by whichparticipants rate prenatal screening as harmful versus beneficial,important versus unimportant, and so on.
Action or decision in regard to opting in or out of screening wasassessed by asking whether the participant underwent or intendsto undergo prenatal genetic screening tests for their currentpregnancy, with response options ‘‘yes’’, ‘‘no’’ and ‘‘unsure’’.Additional questions using the same response categories exploredthe participant’s self-assessment about whether she made aninformed choice, whether she felt her values and beliefs aboutscreening were respected by her midwife, and whether she feltsupported in her choice to screen or not.
The questionnaire also contained several open-ended, shortanswer questions exploring whether any other resources wereused or desired, and other factors that may have affected thescreening decision. The findings based on this qualitative data willbe presented in a separate paper.
3.2. Recruitment and data collection
Ethics approval for this study was obtained from the ResearchEthics Board at Ryerson University. Invitations to act as recruit-ment sites were mailed to each of the 93 operating midwiferypractices in Ontario. Clinics in urban, suburban, and rural Ontariowere all represented among the 40 practices that agreed to act asrecruitment sites for this study. Current midwifery clients wereinvited to respond to an online survey via posters and fliers atparticipating midwifery clinics. The chance to win one of four $50grocery gift cards was offered as an incentive to participate.Consent was obtained by an Internet-based form that preceded theon-line survey. Those who had begun midwifery care after 20weeks gestation were excluded from participating in this study. Allthe data were gathered during the summer of 2012. A total of 171women responded to the survey.
3.3. Analysis
Correct responses to the knowledge questions were summed toform a knowledge score with a maximum of 14 points. Zero pointswere given for incorrect or unanswered knowledge questions. As insimilar studies, a participant with a knowledge score of 50% orhigher (in this case, seven or more correct answers out of 14) wasdeemed to have adequate knowledge.18–23
Responses to the attitude questions were summed to form ascore ranging between 4 (most negative) and 28 (most positive)and then divided by 2.8 to produce a final attitude score between 1and 10. As in the MMIC, the midpoint was used to distinguishpositive and negative attitudes.14 Thus, participants with anattitude score of 5.5 and below were classified as a having anegative attitude towards screening, while participants with ascore above 5.5 were deemed to have a positive attitude towardsscreening.
An informed choice to decline screening was defined as aknowledge score greater than 5 (out of 10), an attitude score of 5.5or less, and the decision not to undergo screening. An informedchoice to undertake screening was defined as a knowledge scoregreater than 5, an attitude score greater than 5.5, and the decisionto undergo screening. Cases with incomplete responses in theattitude or decision to screen categories were excluded fromanalysis.
Chi-square tests were performed to explore the relationshipbetween nominal or categorical variables such as the decision to
fery clients in Ontario making informed choices about prenatal014.02.003
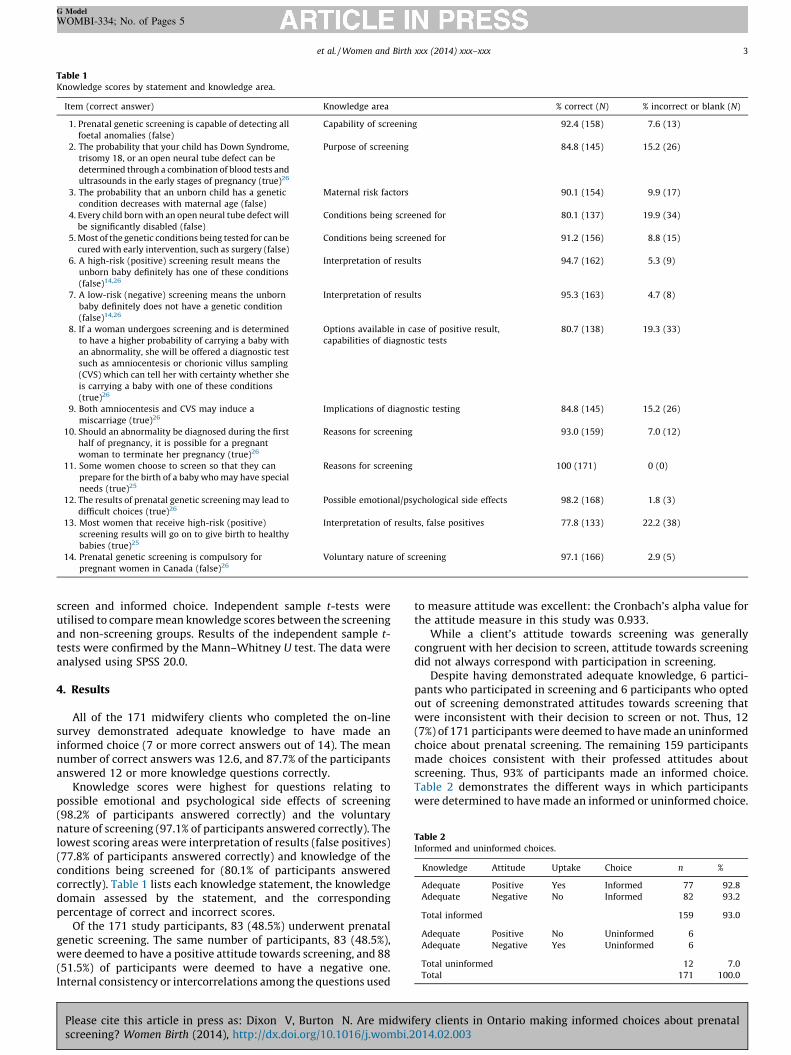
Table 1Knowledge scores by statement and knowledge area.
Item (correct answer) Knowledge area % correct (N) % incorrect or blank (N)
1. Prenatal genetic screening is capable of detecting all
foetal anomalies (false)
Capability of screening 92.4 (158) 7.6 (13)
2. The probability that your child has Down Syndrome,
trisomy 18, or an open neural tube defect can be
determined through a combination of blood tests and
ultrasounds in the early stages of pregnancy (true)26
Purpose of screening 84.8 (145) 15.2 (26)
3. The probability that an unborn child has a genetic
condition decreases with maternal age (false)
Maternal risk factors 90.1 (154) 9.9 (17)
4. Every child born with an open neural tube defect will
be significantly disabled (false)
Conditions being screened for 80.1 (137) 19.9 (34)
5. Most of the genetic conditions being tested for can be
cured with early intervention, such as surgery (false)
Conditions being screened for 91.2 (156) 8.8 (15)
6. A high-risk (positive) screening result means the
unborn baby definitely has one of these conditions
(false)14,26
Interpretation of results 94.7 (162) 5.3 (9)
7. A low-risk (negative) screening means the unborn
baby definitely does not have a genetic condition
(false)14,26
Interpretation of results 95.3 (163) 4.7 (8)
8. If a woman undergoes screening and is determined
to have a higher probability of carrying a baby with
an abnormality, she will be offered a diagnostic test
such as amniocentesis or chorionic villus sampling
(CVS) which can tell her with certainty whether she
is carrying a baby with one of these conditions
(true)26
Options available in case of positive result,
capabilities of diagnostic tests
80.7 (138) 19.3 (33)
9. Both amniocentesis and CVS may induce a
miscarriage (true)26
Implications of diagnostic testing 84.8 (145) 15.2 (26)
10. Should an abnormality be diagnosed during the first
half of pregnancy, it is possible for a pregnant
woman to terminate her pregnancy (true)26
Reasons for screening 93.0 (159) 7.0 (12)
11. Some women choose to screen so that they can
prepare for the birth of a baby who may have special
needs (true)25
Reasons for screening 100 (171) 0 (0)
12. The results of prenatal genetic screening may lead to
difficult choices (true)26
Possible emotional/psychological side effects 98.2 (168) 1.8 (3)
13. Most women that receive high-risk (positive)
screening results will go on to give birth to healthy
babies (true)25
Interpretation of results, false positives 77.8 (133) 22.2 (38)
14. Prenatal genetic screening is compulsory for
pregnant women in Canada (false)26
Voluntary nature of screening 97.1 (166) 2.9 (5)
Table 2Informed and uninformed choices.
Knowledge Attitude Uptake Choice n %
Adequate Positive Yes Informed 77 92.8
Adequate Negative No Informed 82 93.2
Total informed 159 93.0
Adequate Positive No Uninformed 6
Adequate Negative Yes Uninformed 6
Total uninformed 12 7.0
Total 171 100.0
et al. / Women and Birth xxx (2014) xxx–xxx 3
G Model
WOMBI-334; No. of Pages 5
screen and informed choice. Independent sample t-tests wereutilised to compare mean knowledge scores between the screeningand non-screening groups. Results of the independent sample t-tests were confirmed by the Mann–Whitney U test. The data wereanalysed using SPSS 20.0.
4. Results
All of the 171 midwifery clients who completed the on-linesurvey demonstrated adequate knowledge to have made aninformed choice (7 or more correct answers out of 14). The meannumber of correct answers was 12.6, and 87.7% of the participantsanswered 12 or more knowledge questions correctly.
Knowledge scores were highest for questions relating topossible emotional and psychological side effects of screening(98.2% of participants answered correctly) and the voluntarynature of screening (97.1% of participants answered correctly). Thelowest scoring areas were interpretation of results (false positives)(77.8% of participants answered correctly) and knowledge of theconditions being screened for (80.1% of participants answeredcorrectly). Table 1 lists each knowledge statement, the knowledgedomain assessed by the statement, and the correspondingpercentage of correct and incorrect scores.
Of the 171 study participants, 83 (48.5%) underwent prenatalgenetic screening. The same number of participants, 83 (48.5%),were deemed to have a positive attitude towards screening, and 88(51.5%) of participants were deemed to have a negative one.Internal consistency or intercorrelations among the questions used
Please cite this article in press as: Dixon V, Burton N. Are midwiscreening? Women Birth (2014), http://dx.doi.org/10.1016/j.wombi.2
to measure attitude was excellent: the Cronbach’s alpha value forthe attitude measure in this study was 0.933.
While a client’s attitude towards screening was generallycongruent with her decision to screen, attitude towards screeningdid not always correspond with participation in screening.
Despite having demonstrated adequate knowledge, 6 partici-pants who participated in screening and 6 participants who optedout of screening demonstrated attitudes towards screening thatwere inconsistent with their decision to screen or not. Thus, 12(7%) of 171 participants were deemed to have made an uninformedchoice about prenatal screening. The remaining 159 participantsmade choices consistent with their professed attitudes aboutscreening. Thus, 93% of participants made an informed choice.Table 2 demonstrates the different ways in which participantswere determined to have made an informed or uninformed choice.
fery clients in Ontario making informed choices about prenatal014.02.003

et al. / Women and Birth xxx (2014) xxx–xxx4
G Model
WOMBI-334; No. of Pages 5
The incidence of informed choice was very high among both thescreening and non-screening groups, 92.8% and 93.2%, respective-ly. Those who choose to screen, however, had higher knowledgescores than those who opted out (p-value = 0.046, t = 2.01, 95% CI;confirmed by Mann–Whitney U test: p-value = 0.007). Gestationalage at initiation of midwifery care was not related to making aninformed choice and there was no significant difference inknowledge scores among women who had or had not beenexposed to the issue of prenatal screening in a previous pregnancy.
The majority of participants, 98.8%, felt they had adequateinformation to make an informed choice (n = 86). All of theseparticipants (n = 87) also felt their values and beliefs wereacknowledged and respected by their midwife during the process.Finally, 98.9% felt that their decision to screen or not wassupported by their midwife (n = 88).
5. Discussion
The results of this study suggest that Ontario midwives aredelivering adequate information and promoting informed choiceon prenatal genetic screening, with extremely high levels of clientknowledge and satisfaction. The high levels of knowledge andinformed choice reported here contrast with the findings of bothnational and international studies measuring informed choiceamong women receiving maternity care which, utilising similarsurvey instruments, have reported informed choice levels rangingfrom 37% to 75%.18–23 Such findings should be viewed in thecontext of the Ontario midwifery model of care in which theprinciple of informed choice is a central tenet and appointmenttimes are typically longer than with family doctors and obste-tricians, allowing more time for in-depth discussions.27
The rate of informed choice among women receiving care hasbeen accepted as a proxy measure for how well midwives areproviding care in this area.18 However, qualitative data from thesurvey suggested that although midwives served as the mainsource of information for the vast majority of participants, womenalso reported seeking information from other sources including theInternet, books, friends and family. Thus, the authors acknowledgethat midwifery clients gather information from a range of sourcesand the high levels of knowledge reported here cannot beattributed solely to the efforts of midwives.
In Ontario, where only 10% of pregnant women utilisemidwifery care, midwifery clients represent a small subset ofwomen receiving prenatal care. Thus, it is also possible that theresults reflect as much on midwifery clients as they do midwivessince women who choose midwifery care may be more invested inexercising informed choice, personal control, and minimal medicalintervention. Indeed, the relatively high proportion of women whoreported opting out of prenatal screening (51.5% in this studycompared to 33% of all pregnant women in Ontario), likely reflectsboth midwives’ refusal to treat the screening as a routine aspect ofprenatal care as well as the inclination of some of their clients toexercise informed choice and minimise medical intervention.28
Other possible sources of error include a volunteer bias since itis possible that midwifery clients with more of an interest inprenatal screening may have been more likely to complete oursurvey. However, we hope that offering a chance to win a grocerygift card as an incentive to participate encouraged a wide range ofwomen to complete our survey.
In addition, those without sufficient English language skills tocomplete the survey were excluded from participating in thisstudy. This exclusion may have skewed our results towards ahigher incidence of informed choice since the incidence ofinformed choice in prenatal screening has been demonstrated tobe lower among ethnic minority groups and women for whom
Please cite this article in press as: Dixon V, Burton N. Are midwiscreening? Women Birth (2014), http://dx.doi.org/10.1016/j.wombi.2
English is a second language.29–31 Clients without Internet accesswere also excluded from participating.
Finally, since midwifery clients at all stages of care (from 6weeks gestation to 6 weeks post partum) were eligible toparticipate, some respondents had already made the choicewhether to participate in prenatal screening, while others recordedtheir intention to participate in screening or not. While intention toparticipate has been found to be predictive of screeningbehaviour,32 participants who completed the survey retrospec-tively may have been subject to bias due to the outcome of theirdecision to screen or not affecting their assessment of the choicethey had made.18 This was reflected in the qualitative data whenparticipants described a change in attitude towards screening frompositive to negative after receiving a false positive result. Whilerecall bias would not likely affect knowledge scores, it may haveskewed individual attitude scores in either the positive or negativedirection.
This study points to several areas in which midwives canimprove their clients’ knowledge levels, such as knowledge of theconditions being tested for and interpretation of test results.Further research might expand on this study to compare rates ofinformed choice between clients of various types of maternity careproviders in Ontario (that is, midwives, family doctors andobstetricians) while adjusting for factors such as clients’ educationlevel, attitude toward medical intervention, and personal commit-ment to informed choice.
6. Conclusion
This study found very high rates of knowledge, informed choice,and satisfaction among Ontario midwifery clients in regard toprenatal genetic screening choices.
Acknowledgments
The authors wish to thank the women who took the time toparticipate in this study as well as the many midwifery practicesthat made this research possible. We are also grateful to theMidwifery Education Program at Ryerson University for theirfinancial support of this project and to Steve Kanters and Dr.Marcos Escobar for their advice on all things statistical.
References
1. Chitayat D, Langlois S, Wilson RD. Prenatal screening for fetal aneuploidy insingleton pregnancies. Joint SOGC-CCMG Clinical Practice Guideline. J ObstetGynaecol Can 2011;261:736–60.
2. Tapon D. Prenatal testing for Down syndrome: comparison of screening prac-tices in the UK and USA. J Genet Couns 2010;19(2):112–30.
3. Boyd PA, DeVigan C, Khoshnood B, Loane M, Garne E, Dolk H. Survey of prenatalscreening policies in Europe for structural malformations and chromosomeanomalies, and their impact on detection and termination rates for neural tubedefects and Down’s syndrome. BJOG 2008;115(6):689–96.
4. Bombard Y, Miller FA, Hayeems RZ, Avard D, Knoppers BM. Reconsideringreproductive benefit through newborn screening: a systematic review of guide-lines on preconception, prenatal and newborn screening. Eur J Hum Genet2010;18(7):751–60.
5. Katz Rothman B. Spoiling the pregnancy: prenatal diagnosis in the Netherlands.In: De Vries R, Benoit C, van Teijlingen E, Wrede S, editors. Birth by design:pregnancy, maternity care, and midwifery in North America and Europe. NewYork: Routledge; 2001. p. 180–98.
6. Press N, Browner C. Why women say yes to prenatal screening. Soc Sci Med1997;45(7):979–89.
7. Seavilleklein V. Challenging the rhetoric of choice in prenatal screening. Bio-ethics 2009;23(1):68–77.
8. Green JM, Hewison J, Bekker HL, Bryant LD, Cuckle HS. Psychosocial aspects ofgenetic screening of pregnant women and newborns: a systematic review.Health Technol Assess 2004;8(33):1–109.
9. Kelly S. Choosing not to choose: reproductive responses of parents of childrenwith genetic conditions or impairments. Sociol Health Illn 2009;31(1):91–7.
fery clients in Ontario making informed choices about prenatal014.02.003
et al. / Women and Birth xxx (2014) xxx–xxx 5
G Model
WOMBI-334; No. of Pages 5
10. Park A, Mathews M. Women’s decisions about maternal serum screeningtesting: a qualitative study exploring what they learn and the role prenatalcare providers play. Women Birth 2009;22:73–8.
11. Gagnon S, Labrecque M, Njoya M, Rousseau F, St-Jacques S, Legare F. How muchdo family physicians involve pregnant women in decisions about prenatalscreening for Down syndrome? Prenat Diagn 2010;30(2):115–21.
12. Carroll JC, Brown JB, Reid AJ, Pugh P. Women’s experience of maternal serumscreening. Can Fam Physician 2000;46:614–20.
13. Potter BK, O’Reilly N, Etchegary H, Howley H, Graham ID, Walker M. Exploringinformed choice in the context of prenatal testing: findings from a qualitativestudy. Health Expect 2008;11(4):355–65.
14. Marteau TM, Dormandy E, Michie S. A measure of informed choice. HealthExpect 2001;4:99–108.
15. Benn P, Borrell A, Crossley J, Cuckle H, Dugoff L, Gross S, et al. Aneuploidyscreening: a position statement from a committee on behalf of the Board of theInternational Society for Prenatal Diagnosis, January 2011. Prenat Diagn2011;31(6):519–22.
16. Cartier L, Murphy-Kaulbeck L. Counselling considerations for prenatal geneticscreening, SOGC committee opinion. J Obstet Gynaecol Can 2012;34(5):489–93.
17. College of Midwives of Ontario. Informed choice standard. 2005. Available from:http://www.cmo.on.ca/downloads/communications/standards/G14-Infor-med%20Choice%20Standard%20Sept%2005.pdf [accessed 17.02.13].
18. Schoonen MH, Wildschut HIJ, Essink-Bot ML, Peters IA, Steegers EAP, de KoningHJ. The provision of information and informed decision-making on prenatalscreening for Down syndrome: a questionnaire- and register-based survey in anon-selected population. Patient Educ Couns 2012;87(3):351–9.
19. van den Berg M, Timmermans D, ten Kate L, van Vugt J, van der Wal G. Arepregnant women making informed choices about prenatal screening? GenetMed 2005;7:332–8.
20. Jaques AM, Sheffield LJ, Halliday JL. Informed choice in women attendingprivate clinics to undergo first-trimester screening for Down syndrome. PrenatDiag 2005;25(8):656–64.
21. Rowe J, Fisher JRW, Quinlivan JA. Are pregnant Australian women well in-formed about prenatal genetic screening? A systematic investigation using theMultidimensional Measure of Informed Choice. Aust NZ Obstet Gynaecol2006;46:433–9.
Please cite this article in press as: Dixon V, Burton N. Are midwiscreening? Women Birth (2014), http://dx.doi.org/10.1016/j.wombi.2
22. Michie S, Dormandy E, Marteau TM. The multi-dimensional measure of in-formed choice: a validation study. Patient Educ Couns 2002;48(1):87–91.
23. Dormandy E, Hooper R, Michie S, Marteau TM. Informed choice to undergoprenatal screening: a comparison of two hospitals conducting testing either aspart of a routine visit or requiring a separate visit. J Med Screen 2002;9(3):109–14.
24. Burton N. Limited and limiting knowledges: talking to clients about prenatalscreening. Int J Commun Health 2014:11–8. [in press].
25. Genetics Education Project. A guide to understanding prenatal screening tests forwomen and their families. 2007. Available from: http://mountsinai.on.ca/care/family-medicine-genetics-program/prenatal [accessed 05.01.13].
26. Schoonen MH, van Agt HME, Essink-Bot ML, Wildschut HI, Steegers EAP,de Koning HJ. Informed decision-making in prenatal screening for Down’ssyndrome: what knowledge is relevant? Patient Educ Couns 2011;84(2):265–70.
27. MacDonald ME, Bourgeault IL. The Ontario midwifery model of care. In: Davis-Floydd R, Barclay L, Tritten J, editors. Birth models that work. Berkeley, CA:University of California Press; 2009. p. 89–117.
28. Better Outcomes Registry and Network. Highlights from the BORN Ontario LHINregion reports for 2009–2010. August 2011. Available from: http://www.bor-nontario.ca/_documents/LHIN%202009-2010%20Reports/Perinatal%20Heal-th%20Report%202009-2010_Provincial%20Overview%20 Presentation.pdf[accessed 15.06.12].
29. Browner CH, Preloran HM, Casado MC, Bass HN, Walker AP. Genetic counselinggone awry: miscommunication between prenatal genetic service providers andMexican-origin clients. Soc Sci Med 2003;56(9):1933–46.
30. Dormandy E, Michie S, Hooper R, Marteau TM. Low uptake of prenatal screeningfor Down syndrome in minority ethnic groups and socially deprived groups: areflection of women’s attitudes or a failure to facilitate informed choices? Int JEpidemiol 2005;34(2):346–52.
31. Fransen MP, Schoonen MH, Mackenbach JP, Steegers EA, de Koning HJ, Laudy J,et al. Ethnic differences in participation in prenatal screening for Downsyndrome: a register-based study. Prenat Diag 2010;30(10):988–94.
32. Bryant LD, Green JM, Hewison J. The role of attitudes towards the targets ofbehaviour in predicting and informing prenatal testing choices. Psychol Health2010;25(10):1175–94.
fery clients in Ontario making informed choices about prenatal014.02.003
Recommended

















