Approaches to the Treatment of
Metastatic Bladder Cancer
Daniel P. Petrylak, MD
Professor of Medicine and Urology
Director, GU Translational Working Group
Co Director, Signal Transduction Program
Smilow Cancer Center, Yale University


M-VAC vs Cisplatin Phase IIILong term survival
Cisplatin M-VAC
Evaluable 122 133
3 years 4 17
6 years* 2 9
*6 patients died of TCC, 1 2nd Ca, 2 other, 1 lost to F/U
Saxman, JCO, 15:2564, 1997

M-VAC: EORTC Dose Intensification
HD M-VAC: Methotrexate 30 mg/m2 Day 1; Vinblastine 3 mg /m2 Day 2Adriamycin 30 mg / m2
Cisplatin 70 mg/m2
G-CSF
Classic M-VAC:
Methotrexate 30 mg/m2 Day 1, 14, 21
Vinblastine 3 mg /m2 Day 1, 14, 21Adriamycin 30 mg / m2 Day 2Cisplatin 70 mg/m2 Day 2
Accrual :263 patients
Sternberg, C. N. et al. J Clin Oncol;
19:2638-2646 2001

Stromal PD-L1
modulation of T cells
Immune cell
modulation of T cells
PD-L1/PD-1-mediated
inhibition of
tumor cell killing
IFNg-mediated
upregulation of
tumor PD-L1
Priming and
activation of T cells
PD-L2-mediated
inhibition of TH2 T cells
B7.1
Herbst RS et al. J Clin Oncol . 2013;31(suppl; abstr 3000)
Key Attributes of
the Immune System
• Specificity
• Memory
• Adaptive
• Cancer cells develop many
mutations that can make them
appear foreign to the immune
system
• T cells can recognize, attack
and kill these “foreign” cancer
cells
• Cancer cells can evade
immune attack by expressing
PD-L1
• Adaptive tumor expression of
PD-L1 turns the immune
system OFF
• Clinically, we want to block
PD-1 or PD-L1 to reactivate
the immune system
• PD-L1 plays an important role
in dampening the anti-tumor
immune response
Mechanism of Immune Checkpoint Inhibitors

Checkpoint Inhibitors Approved for Use in Urothelial
Carcinoma7 US FDA Approvals May 2016-May 2017
Setting Antibody Approval Status
First-line
(cisplatin-
ineligible)
Atezolizumab • Accelerated approval granted in April 2017.
Pembrolizumab • Accelerated approval granted in May 2017.
Platinum-
pretreated
Atezolizumab • Accelerated approval granted in May 2016.
• In May 2017, the subsequent phase 3
IMvigor211 trial did not meet primary endpoint of
overall survival.
Nivolumab • Accelerated approval granted in February 2017.
Durvalumab • Accelerated approval granted in May 2017.
Avelumab • Accelerated approval granted in May 2017.
Pembrolizumab • Full approval granted in May 2017.

Approvals: First-line, Cisplatin-
Ineligible
Atezolizumab Pembrolizumab
Apr 2017 May 2017
Above agents are indicated in patients with locally advanced or
metastatic urothelial carcinoma not eligible for cisplatin-containing
chemotherapy.

Definition of the Medically Unfit
Patient
• Concurrent renal insufficiency limits the
administration of drugs such as cisplatin
• Cardiac dysfunction and third space
accumulation of fluids limit hydration of
patients
• Performance status predisposes to
neutropenia and dose adminstration
• No consisteentstandard definition of “unfit”
based on objective criteria

Treatment of the Medically Unfit
Patient
• Treatment goals shift to palliation of
symptoms rather than response/survival
• Single agent vs non cisplatin containing
doublets
• Immune therapy for first line treatment

IMvigor210 (Cohort 1)
Balar et al. Lancet. 2017;389:67
Key primary endpoint :
• Confirmed ORR: RECIST v1.1
(per central IRF)
Key secondary endpoints :
• DOR, PFS, OS, safety
Cohort 1 (N = 119):
1L cisplatin-ineligible
IMvigor210:
• Inoperable locally advanced
or metastatic urothelial
carcinoma
• Predominantly UC histology
• Tumor tissue evaluable for
PD-L1 testinga
Cohort 2 (N = 310):
Platinum-treated mUC
Atezolizumab 1200 mg IV q3w
until RECIST v1.1 progression
Atezolizumab 1200 mg IV q3w
until loss of clinical benefit
Cohort 1–specific inclusion criteria
•No prior treatment for mUC (>12 mo since perioperative chemo)
•ECOG PS 0-2
•Cisplatin ineligibility1 based on ≥1 of the following:
− Renal impairment: GFR <60 and >30 mL/min
− Grade ≥2 hearing loss or peripheral neuropathy
− ECOG PS 2

IMvigor210 (Cohort 1)
Balar et al. Lancet. 2017;389:67
• N = 119
• ORR = 23% (9% CR) Overall Survival

Secondary Endpoints: DOR, PFS, OS, and ORR in all patients,
PD-L1‒positive and PD-L1–high-expressing patients; safety and
tolerability
Primary Endpoints:
• Planned interim analysis in first 100 patients
• Determine the PD-L1–high expression cutpoint
• ORR in all patients and PD-L1‒positive population
Pembrolizumab
200 mg Q3W
Primary Endpoints
• ORR in all patients
• ORR in patients with
PD-L1–positive
tumors
Patients (N = 350)
•Advanced urothelial cancer
•No prior chemotherapy for
metastatic disease
•ECOG PS 0-2
•Ineligible for cisplatin based
on ≥1 of the following:– CrCl <60 mL/min
– ECOG PS 2
– Grade ≥2 neuropathy or
hearing loss
– NYHA class III CHF
KEYNOTE-052: Pembrolizumab as 1st-Line
Therapy for Cisplatin-Ineligible Advanced
Urothelial Cancer
Balar et al. ESMO 2016; abstract LBA32_PR.

KEYNOTE-052 (ASCO17 Update)
O’Donnell et al. ASCO 2017; Abstract 4502.
N = 370
ORR: 29%
CR: 7%

Sequence of Therapy for Cisplatin-Eligible Patients
Cisplatin-based
chemotherapyPD-1 or PDL-1
Inhibitor
Single Agent
Chemotherapy

Sequence of Therapy for Cisplatin-Ineligible Patients
Carboplatin-
based
chemotherapy
Checkpoint
InhibitorSingle Agent
Chemotherapy
Carboplatin-
based
chemotherapy
Single Agent
Chemotherapy
Pembrolizumab/
atezolizumab
Comorbidity/patient
choice‒directed
(no validated
biomarkers)

Gem-Carbo (Ph III)1 Atezolizumab (Ph II)2 Pembrolizumab (Ph II)3
Number of patients 119 119 370
% with PS 2 44.5% 20% 42%
% CrCl <60 mL/min 55.5%a 70% 49%
% PS 2 + CrCl <60 mL/min 26.9%a 7% 9%
ORR 41.2% 23% 24%
Median PFS 5.8 mo 2.7 mo 2 mo; 3 mo on therapy
Median OS 9.3 mo 15.9 mo Not reported
Duration of response Not reported Not reached
(median f/u 17.2 mo)
Not reached
(78% ≥6 months)
aGFR 30-60 mL/min.
1. De Santis M, et al. J Clin Oncol. 2012;30(2):191-199; 2. Balar AV, et al. Lancet.
2017;389(10064):67-76; 3. Balar AV; et al. Lancet Oncol. 2017;18:1483-1492.
First-Line Therapy for Cisplatin-Ineligible Metastatic UC
PD-1/PD-L1 Inhibitor OR Gemcitabine-Carboplatin Based on Activity?

Use PD-L1 expression to select therapy for
cisplatin-ineligible patients?
5/18/2018
FDA Alert
•In two ongoing clinical trials (KEYNOTE-361 and
IMVIGOR-130), the Data Monitoring Committees’ (DMC)
found patients in the monotherapy arms of both trials
with PD-L1 low status had decreased survival
compared to patients who received cisplatin- or
carboplatin-based chemotherapy.
•Both trials have stopped enrolling patients whose
tumors have PD-L1 low status to the Keytruda or
Tecentriq monotherapy arms.
•The monotherapy arms remain open only to patients
whose tumors have PD-L1 high status.
Carboplatin-
based
chemotherapy
Pembrolizumab/
atezolizumab
PD-L1 (IHC)
Low High

First Line Chemotherapy +Checkpoint Therapy trials in
Metastatic Urothelial Cancer
CT ID Phase Target Experimental Arm(s) Standard Arm
NCT02807636
IMvigor130
III PD-L1 Atezo
OR
Atezo + Gem-Plat
Placebo + Gem-Plat
NCT02853305
KEYNOTE-361
III PD-1 Pembro
OR
Pembro + Gem-Plat
Gem-Plat
NCT02516241
DANUBE
III PD-L1 +/-
CTLA-4
Durvalumab
OR
Durva + Treme
Gem-Plat
NCT03036098
CM-901
III PD-1 + CTLA Nivo + Ipi* Gem-Plat
*This trial includes a substudy for cisplatin-eligible patients comparing
gemcitabine + cisplatin +/- nivolumab.

Approvals: Previously-treated
Disease
Atezolizumab Nivolumab Durvalumab Avelumab Pembrolizumab
May 2016 Feb 2017 May 2017
Above agents are indicated in patients with locally advanced or metastatic urothelial carcinoma who
have disease progression during or following platinum-containing chemotherapy or within 12 months of
neoadjuvant or adjuvant treatment with (platinum-containing) chemotherapy.

IMvigor210 (Cohort 2)
Rosenberg et al. Lancet. 2016; 387:1909.
IMvigor210:
• Inoperable locally advanced
or metastatic urothelial
carcinoma
• Predominantly UC histology
• Tumor tissue evaluable for
PD-L1 testinga
Cohort 1 (N = 119):
1L cisplatin-ineligible
Cohort 2 (N = 310):
Platinum-treated mUC
Atezolizumab 1200 mg IV q3w
until RECIST v1.1 progression
Atezolizumab 1200 mg IV q3w
until loss of clinical benefit
Cohort 2-Specific Inclusion Criteria
• Progression during/following platinum
(no restrictions on # prior lines of therapy)
• ECOG PS 0-1
• CrCl ≥ 30 mL/min
Key primary endpoint :
•Confirmed ORR: RECIST v1.1
(per central IRF)
Key secondary endpoints :
•DOR, PFS, OS, safety

IMvigor210 (Cohort 2)
Rosenberg et al. Lancet. 2016; 387:1909.
All patients:
• ORR = 15% (5% CR)
• mOS = 7.9 months

Phase Ia Trial of Atezolizumab in Pretreated Bladder Cancer
Petrylak et al. ASCO 2015; Abstract 4501.
• N = 92
• 72% with ≥2 prior
systemic therapies
• ORR 50% in PD-L1 high
(IC2/3)
• ORR 17% in PD-L1 low
(IC0/1)

OS by PD-L1 Status
Petrylak et al. ASCO 2015; Abstract 4501.

Median Survival by Baseline
Characteristics
Petrylak et al. ASCO 2015; Abstract 4501.

Patterns of AE Occurrence
Petrylak et al. ASCO 2015; Abstract 4501.

IMvigor211 Phase III Trial in
Previously-treated Urothelial Cancer
• Primary endpoint: OS in IHC 2/31/2/3ITT
• Secondary endpoints: PFS, ORR, DOR
• FPI: Q4 2014
Atezolizumab
1200 mg IV q3w
Patients with previously treated
relapsed UBC
(n = 767 [230 PD-L1+])
Vinflunine, paclitaxel, or docetaxel
IV q3w until progression
FPI=first patient in; ITT=intent-to-treat.
http://www.clinicaltrials.gov/ct2/show/NCT02108652.
.

Key Eligibility Criteriaa
• mUC with progression during or
following platinum-based chemotherapy
– ≤ 2 prior lines of therapy
• Measurable disease per RECIST v1.1
• ECOG PS 0-1
• Evaluable sample for PD-L1 testing
• TCC histology as primary component
(N = 931)
▪ Primary endpoint
– OS, tested hierarchically
in pre-specified populations
27 Powles T, et al. EAS 2017, IMvigor211.
DOR, duration of response; ECOG, Eastern Cooperative Oncology Group; EORTC, European Organisation for Research
and Treatment of Cancer; PRO, patient-reported outcome; q3w, every three weeks; RECIST, Response Evaluation
Criteria In Solid Tumors; TCC, transitional cell carcinoma. a ClinicalTrials.gov, NCT02302807. b Defined by time from prior
chemotherapy < 3 mo, ECOG performance status > 0 and hemoglobin < 10 g/dL. c Confirmed response was not required
for secondary efficacy endpoints. This analysis reports exploratory confirmed responses.
IMvigor211 Study Design
27
Atezolizumab 1200 mg q3w
R
1:1
No crossover permitted
per protocol
Survival
follow-up
Loss of
clinical benefit
RECIST v1.1
progression
Stratification Factors
• No. of risk factorsb (0 vs. 1/2/3)
• Liver metastases (yes vs. no)
• PD-L1 status (0/1 vs. 2/3)
• Chemotherapy (vinflunine vs. taxanes)
▪ Additional endpoints
– Efficacy: RECIST v1.1 ORR, PFS and DORc
– Safety
– PROs: EORTC QLQ-C30
Chemotherapy
(investigator’s choice)
• Vinflunine q3w
• Docetaxel q3w
• Paclitaxel q3w
Key secondary endpoints:
ORR, then PFS
Primary endpoint:
OS
OS: IC2/3
OS: IC1/2/3
OS: ITT
PFS: IC2/3
PFS: IC1/2/3
PFS: ITT
ORR: IC2/3
ORR: IC1/2/3
ORR: ITT
2-sided = 0.05

28 Powles T, et al. EAS 2017, IMvigor211.HR, hazard ratio.
OS Analysis: IC2/3 Population
HR = 0.87 (95% CI: 0.63, 1.21)
P = 0.41
Events/
PatientsMedian OS
(95% CI)
12-mo OS Rate(95% CI)
Atezolizumab 72/116 11.1 mo (8.6, 15.5) 46% (37, 56)
Chemotherapy 88/118 10.6 mo (8.4, 12.2) 41% (32, 50)
No. at Risk
Atezolizumab 116 100 85 77 71 58 51 39 27 19 11 6 0
Chemotherapy 118 100 91 82 71 61 47 32 24 15 9 5 1
80
60
0
10 12 14 16 18 202 4 6 80 2422
20
40
Overa
ll S
urv
ival
100
Months

29 Powles T, et al. EAS 2017, IMvigor211.
OS Analysis: IC1/2/3 Population
Events/
PatientsMedian OS
(95% CI)
12-mo OS Rate(95% CI)
Atezolizumab 220/316 8.9 mo (8.2, 10.9) 40% (35, 46)
Chemotherapy 232/309 8.2 mo (7.4, 9.5) 33% (28, 39)
HR = 0.87 (95% CI: 0.71, 1.05)
P = 0.14
No. at Risk
Atezolizumab 316 274 232 198 175 141 122 97 64 41 23 9 1
Chemotherapy 309 273 228 188 153 121 95 66 46 31 15 7 1
80
60
0
10 12 14 16 18 202 4 6 80 2422
20
40
Overa
ll S
urv
ival
100
Months

▪ Median follow-up duration in ITT population: 17.3 mo (range, 0 to 24.5 mo)
30 Powles T, et al. EAS 2017, IMvigor211.
OS Analysis: ITT Population
Events/
PatientsMedian OS
(95% CI)
12-mo OS Rate(95% CI)
Atezolizumab 324/467 8.6 mo (7.8, 9.6) 39% (35, 44)
Chemotherapy 350/464 8.0 mo (7.2, 8.6) 32% (28, 37)80
60
0
10 12 14 16 18 202 4 6 80 2422
20
40
Overa
ll S
urv
ival
100
Months
80
60
0
10 12 14 16 18 202 4 6 80 2422
20
40
Overa
ll S
urv
ival
100
Months
HR = 0.85 (95% CI: 0.73, 0.99)
P = 0.038
No. at Risk
Atezolizumab 467 405 327 280 245 201 177 138 90 59 34 13 1
Chemotherapy 464 397 330 268 219 175 140 99 60 42 17 7 1

▪ OS was also examined in
subgroups based on chemotherapy
type at randomization
– Improved OS was observed
with atezolizumab vs. taxanes
31 Powles T, et al. EAS 2017, IMvigor211.
OS by Chemotherapy Type
ITT With Taxane
No. at Risk
Atezolizumab 215 186 153 125 106 89 81 66 45 34 19 7 0
Taxane 214 179 147 122 94 74 58 35 20 16 4 3 1
80
60
0
10 12 14 16 18 202 4 6 80 2422
20
40
Ove
rall
Su
rviv
al
100
Months
HR = 0.73 (95% CI: 0.58, 0.92)
SubgroupMedian OS
(95% CI)
Atezolizumab 8.3 mo (6.6, 9.8)
Taxane 7.5 mo (6.7, 8.6)

Phase Ib JAVELIN Solid Tumor Trial of
Avelumab: Trial Schema
• Open-label, multicenter phase Ib study in pts with confirmed solid tumors
▪ Primary endpoint: ORR, safety
▪ Secondary endpoints: PFS, OS, and association of PD-L1 expression on tumor cells with clinical activity of avelumab
Advanced UC Cohort: Pts with
histology or cytology confirmed
metastatic UC after progression on
or ineligible for platinum-based
chemotherapy for metastatic
disease; ECOG PS 0-1
(N = 241)
Avelumab
10 mg/kg IV Q2W
Treated until PD, unacceptable
AE, or investigator decision
Patel M, et al. ASCO GU 2017. Abstract 330.

Phase Ib JAVELIN Solid Tumor Trial of Avelumab (ASCO17 Update)
ORR in patients with ≥6 months follow-up (N = 161): 17% (6% CR)
Apolo, et al. ASCO17; Abstract 4528.
N = 242
mOS 7.4 mo
mPFS1.5 mo
(6.6 wk)

KEYNOTE-045: Phase III Study Design
CPS, combined positive score; PD, progressive disease.
Bellmunt et al. SITC 2016; Abstract 02.

Bajorin et al. ASCO 2017, Abstract 4501.
Pembrolizumab Chemotherapy
ORR
CR
21%
8%
11%
3%
Median OS HR P Value
Pembro 10.3 mo0.70 .0004
Chemo 7.4 mo
Data cutoff: Jan 18, 2017
Median follow-up: 18.5 mo
Median PFS HR P Value
Pembro 2.1 mo0.96 .32
Chemo 3.3 mo

Future Directions
Non Muscle Invasive Disease
Combinations
Adjuvant therapy
Biomarkers

Addition of Ipilimumab to Nivolumab at
Progression
• 10 patients who evidenced progression of
disease on nivolumab.
• 1 PR, 4 SD after addition of ipilimumab.
• Modest increase in grade 3/4 toxicities.
Callahan et al. ASCO GU 2017; Abstract 384.

Checkmate 032

Checkmate 032
Ipilimumab(Ipi) +Nivolumab(N)
ORR PFS OS
N 3 mg/kg 26% 2.8 9.9
N+ Ipi 3 mg/kg 27% 2.6 7.4
N+ Ipi 1 mg/kg 38% 4.9 15.3

PDL-1 Expression and ORR

Adjuvant PD-1/PD-L1 Inhibitor Phase
III Trials
PI Population Control
Arm
Experimental
Arm
Primary
Endpoint
Industry All-comers MIUC
Prior NAC- ≥pT2
No AC ≥pT3
No therapy Atezolizumab PFS
Industry All-comers MIUC
Prior NAC- ≥pT2
No AC ≥pT3
Placebo Nivolumab PFS
Intergroupa All-comers MIUC
Prior NAC- ≥pT2
No AC ≥pT3
No therapy Pembrolizumab PFS/OS
aPI: Apolo; SWOG PI: Sonpavde; ECOG PI: Srinivas.

Neoadjuvant Therapy With IO Agents
Selected Phase I-II Trials
Trial ID Phase Regimen Primary Endpoint
NCT03294304 II GC-Nivolumab pCR
NCT02690558 II GC-Pembrolizumab pCR
NCT02365766 I/II G/GC-Pembrolizumab Feasibility, pCR
NCT02451423 II Atezolizumab pCR, immune response
NCT02736266 II Pembrolizumab pCR
NCT02812420 II Durvalumab + Tremelimumab Feasibility
NCT02845323 II Nivolumab +/- Urelumab Immune response
Pending I Durvalumab +/- CD73i Feasibility, Immune response
Chemo-IO
IO
IO-IO

Planned Phase III Trial by NRG, SWOG
ChemoRT +/- Concurrent Adjuvant Atezolizumab
RT +
Chemotherapy
(5-FU-MMC,
Cisplatin +/- 5-FU)
ATEZOLIZUMAB x 1 year
OBSERVE
Survival
PFS

Standard MVAC
Gem/Ci
s
Accelerated
MVAC
Vinflunin
Atezolizuma
b
2009:
Vinflunine
EMA Approved
1978: Cisplatin
US FDA
Approved
2016:
Atezolizumab
US FDA
Approved
Targeted Therapy in Urothelial Cancer
Vinflunin
2009:
Vinflunine
EMA Approved
Vinflunin
2009:
Vinflunine
EMA Approved
1.Immunotherapy is active only in a small subset of patients
2.Resistance to immunotherapy is often seen.
3.Significant percentage of patients are not fit enough to receive
Cisplatin-combination chemotherapy.
4.In this era of precision medicine, there is no FDA approved,
biomarker-selected targeted therapy for mUC.

UC is molecularly heterogeneous
• While multiple pathways are altered, the frequency of mutation in any one gene/ pathway is modest, at best
• Unselected trials with targeted agents unlikely to yield positive results
TCGA Network, Nature
2014

Multiple alterations in kinase signaling pathways
TCGA Network, Nature
2014

TSC1 mutations in TCC
*
Sjödahl G et al. PLoS One. 2011
Knowles MA et al. Cancer Metastasis Rev
2009
Pymar LS et al. Hum Mol Genet 2008;
Frequency of TSC1 or TSC2 mutations: 8 to 15%.*

Personalized medicine in UC: mTOR/TSC1
• Whole genome sequencing revealed TSC1 and NF2 inactivating mutations
• In vitro evaluation shows TSC1 sensitizes urothelial cancer cells to mTOR inhibition
G Iyer et al. Science 2012;338:221

Personalized medicine in UC: mTOR/TSC1
• Patient treated on phase I study of everolimus/ pazopanib
• CR lasting 14 months
• WES showed activating mTOR mutations
Wagle, et al. Cancer Discovery
2014
Mutations are activating,
and can be inhibited by
rapamycin in vitro

MLN-0128 (aka. TAK228): NCI Protocol 9767
• Potent, highly selective ATP-competitive inhibitor of mTOR kinase that exhibits dual specificity against both TORC1 and TORC2 complexes.
• Dual TORC1/2 inhibition mitigates the feedback activation of AKT, known to cause resistance to TORC1 selective inhibitors.
• Displays cellular inhibition of TORC1 and TORC2 pathways with IC50 less than 10 nM.
• Potential of greater clinical activity than the currently available rapalogs.

Schema (NCI Protocol 9767)
TSC1 /
TSC2
mutation
sequencing
to be done
at
Yale
Profiling
Lab by Dr.
Jeff Sklar Primary
Endpoint: ORR
N=25

FGFR-3(Fibroblast Growth Factor
Receptor)• A membrane based tyrosine kinase receptor involved in cellular
proliferation, differentiation, and steroid biosynthesis.17

FGFR-3(Fibroblast Growth Factor
Receptor)
• In addition to activating mutations, FGFR over-expression has been implicated in bladder cancer with Turo et al. noting up-regulated FGFR expression via IHC in 53 and 56 of 106 matched pairs of primary tumors and metastases. 18
• FGFR inhibitors and anti-FGFR antibody-drug conjugates are in ongoing and upcoming trials in advanced urothelial carcinoma.

BISCAY – Umbrella StudyA biomarker-directed study in patients with muscle-invasive bladder cancer
Module A: Durvalumab* +AZD4547 OR
AZD4547
Module D: Durvalumab*
Module B: Durvalumab* + Lynparza
Module C: Durvalumab* + AZD1775
Dx sample
analysed
FGFR
inhibitor
PD-L1
only
PARP
inhibitor
WEE1
inhibitor
Treatment option MOA
*PD-L1
FGFR3 mutations/
fusions
None
ATM, BRCA1/2,
HRR gene trunc or
missense mut/del
CDKN2A loss
RB1 loss
CCNE1 ampl
MYC ampl
Biomarkers
Assignment to module dependent on presence of biomarker
Module B2: Durvalumab + Treme + Lynparza
Module C2: Durvalumab + Treme + AZD1775
54
~11%
~22%
~46%
~19%
Adjusted
Prev

Binding of Ramucirumab to VEGFR-2 and
Icrucumab to
VEGFR-1 Inhibits Subsequent Signaling

Rationale for VEGF Blockade in Bladder
Cancer• Antiangiogenic agents, particularly anti-VEGFR-2 monoclonal
antibodies (MAbs), may be capable of acting as chemosensitizing
agents when given in combination with docetaxel, since this effect was
demonstrated in mice when an anti-VEGFR-2 MAb, DC101, was
combined with paclitaxel.
• Anti-VEGFR-1 MAbs may inhibit metastasis, based on the observed
impact of the anti-VEGFR-1 MAb, MF1, on VEGFR-1-positive circulating
hematopoietic progenitor cells in mice.

Enfortumab Vedotin: Proposed Mechanism of Action
Presented by: Daniel P.
Petrylak
Enfortumab Vedotin is being co-developed by Seattle Genetics, Inc. and Astellas Pharma Inc.

Study Design
• This phase 1, 3-part study (NCT02091999) enrolled patients with
metastatic malignant solid tumors treated with ≥1 prior chemotherapy
regimen
• IV administration over 30 minutes on Days 1, 8, and 15 every 28 days
• Study enrollment in Parts B and C ongoing
Presented by: Daniel P.
Petrylak
Part A (closed) Dose escalation/expansion, adaptive trial
design utilizing a Continual Reassessment
Method, to determine RP2D
• Cohort 1: 0.5 mg/kg
• Cohort 2: 0.75 mg/kg
• Cohort 3: 1 mg/kg
• Cohort 4: 1.25 mg/kg
Nectin-4 expressing tumors, including mUC
RP2D1.25
mg/kg
Part B (enrolling)Dose expansion: 3 cohorts (n=15/cohort)• Cohort 1: Urothelial Cancer-Cis-ineligible
(1 mg/kg escalating to 1.25 mg/kg)
• Cohort 2: NSCLC (1.25 mg/kg)
• Cohort 3: Ovarian Cancer (1.25 mg/kg)
Part C (enrolling) Dose expansion: 1 cohort (n=60)
• CPI-treated mUC patients (1.25 mg/kg)
https://www.clinicaltrials.gov. Accessed 12 May 2017.

Screening of Nectin-4 Expression in mUC
• At screening, patients with mUC had
samples that were centrally assessed
by immunohistochemistry (IHC) for
Nectin-4
– Almost all patient (97%) samples
showed Nectin-4 expression
– Expression of Nectin-4 was high
(median H-score 280 out of a 300
maximum score)
• Due to the above findings, pre-
screening for Nectin-4 is no longer an
eligibility requirement for subjects with
mUC
Presented by: Daniel P.
Petrylak
0
50
100
150
200
250
300
H-s
core
PatientsGray bars indicate patients with Nectin-4 H-score <150
Blue bars indicate patients with H-scores of ≥150Note: data cutoff November 2016, N=186

EV-101: Disposition of Patients With Metastatic Urothelial Cancer
Patients With mUC
All Doses
(N=155)
Patients with mUC
1.25 mg/kg EV
(N=112 )
Subjects continuing treatment, n (%) 29 (19) 27 (24)
Treatment discontinuations, n (%) 126 (81) 85 (76)
Disease progression (radiographic) 83 (53.5) 56 (50)
Disease progression (clinical symptoms) 11 (7) 7 (6)
Adverse event 18 (12) 12 (11)
Subject withdrew consent 5 (3) 3 (3)
Investigator’s decision 7 (4.5) 5 (4)
Other 2 (1) 2 (2)
Median time on treatment, weeks (range)22.6
(1.1, 89)
23.7
(1.1, 78)
Data presented as n (%).
mUC, metastatic urothelial cancer. Data cut-off date is April 9, 2018.
6
0
Jonathan E. Rosenberg

Patients With mUC
1.25 mg/kg
(N=112)
Primary tumor site bladder, n (%) 86 (77)
Site of metastases at baseline, n (%)
Liver 33 (29)
Lung 54 (48)
Lymph node only 21 (19)
≥2 prior therapies in the metastatic
setting, n (%)71 (63)
Prior platinum-based therapy, n (%) 105 (94)
Prior taxane treatment, n (%) 32 (29)
Prior CPI treatment, n (%) 89 (79)
CPI was most recent therapy 65 (73*)
Data cut-off date is April 9, 2018.
*Percentage based on number of patients with prior CPI.
CPI, checkpoint inhibitors; mUC, metastatic urothelial cancer.
Patients With mUC
1.25 mg/kg
(N=112)
Median age, years (range) 67 (24–86)
Male, n (%) 82 (73)
Race, n (%)
Caucasian 103 (92)
Asian 5 (5)
Other 3 (3)
ECOG Score
0 36 (32)
1 76 (68)
Hemoglobin levels <10 g/dL, n (%) 23 (21)
GFR <60 mL/min 56 (50)
Data cut-off date is April 9, 2018.
ECOG, Eastern Cooperative Oncology Group; GFR, Glomerular filtration rate;
mUC, metastatic urothelial cancer.
EV–101: Demographics and Disease Characteristics
6
1
Jonathan E. Rosenberg

Enfortumab Vedotin Toxicity Profile
Patients With mUC
1.25 mg/kg
(N=112)
Treatment-Related Adverse Events in ≥25% of Patients With
mUC
All Grade Grade ≥3
Fatigue 60 (54) 1 (1)
Alopecia 50 (45) 0
Decreased appetite 45 (40) 1 (1)
Dysgeusia 43 (38) 0
Nausea 40 (36) 1 (1)
Pruritus 39 (35) 1 (1)
Peripheral neuropathy 39 (35) 0
Diarrhea 36 (32) 1 (1)
Maculo-papular rash 28 (25) 3 (3)
Data cut-off date is April 9, 2018.
Data presented as n (%). Adverse events listed are individual preferred terms.
mUC, metastatic urothelial cancer.
• Consistent with previous reports, EV
was generally well tolerated1
6
2
1Petrylak DP et al. J Clin Oncol. 2017;35:106–106.
• The majority of adverse events considered at least possibly related to EV were mild-to-moderate in severity
Jonathan E. Rosenberg

Grade ≥3 Adverse Events Regardless of Treatment Attribution
6
3
Patients With mUC
1.25 mg/kg
(N=112)
Grade ≥3 Adverse Events in ≥5% Patients with mUC Regardless of Treatment Attribution
Anemia 9 (8)
Hyponatremia 8 (7)
Urinary tract infection 8 (7)
Hyperglycemia 7 (6)
Grade 5 Adverse Events Regardless of Treatment Attribution
Diabetic ketoacidosis* 1 (0.9)
Dyspnea 1 (0.9)
Multiple organ dysfunction syndrome* 1 (0.9)
Progressive disease 1 (0.9)
Sepsis 1 (0.9)
Small intestinal perforation 1 (0.9)
Respiratory failure* 1 (0.9)
Urinary tract obstruction* 1 (0.9)
Data cut-off date is April 9, 2018. Data presented as n (%). Adverse events listed are individual preferred terms.
*Fatal AEs that were considered at least possibly related to enfortumab vedotin. mUC, metastatic urothelial cancer.
Jonathan E. Rosenberg

Investigator-Assessed Response in Patients With mUC on Enfortumab Vedotin
1
0
1.25 mg/kg
(N=112)a
Confirmed CR 4%
Confirmed PR 37%
Confirmed ORRb (95% CI) 41% (31.9, 50.8)
SD 30%
DCRb (95% CI) 71% (62.1, 79.6)
Data cut-off date is April 9, 2018. CR, complete response; DCR, disease control rate
(DCR=CR+PR+SD); overall response rate (ORR=CR+PR); PR, partial response; SD, stable
disease. aPatients must have at least one post-baseline assessment; responses assessed per
RECIST 1.1. b95% CI based on the Clopper-Pearson method.
Jonathan E. Rosenberg

Duration of Response in Patients With Metastatic Urothelial Carcinoma
6
5
Median duration of confirmed
response, months (range)
5.75
(1.8, 12.9)
Jonathan E. Rosenberg

Prior CPI Treatmenta CPI-Naïvea Liver Metastasesa
1.25 mg/kg
(n=89)
1.25 mg/kg
(n=23)
1.25 mg/kg
(n=33)
Confirmed CR 3.4% 9% 0
Confirmed PR 37% 35% 39%
Confirmed ORRb (95% CI)40%
(30.2, 51.4)
44%
(23.2, 65.5)
39%
(22.9, 57.9)
SD 34% 17% 21%
DCRb (95% CI)74%
(63.8, 82.9)
61%
(38.5, 80.3)
60%
(42.1, 77.1)
Data cut-off date is April 9, 2018.
Data presented as n (%), unless otherwise indicated.
CR, complete response; CPI, checkpoint inhibitor, DCR, disease control rate (DCR=CR+PR+SD); PR, partial response; ORR, overall response rate (ORR=CR+PR);
SD, stable disease. aEvaluable patients must have at least one post-baseline assessment; responses assessed per RECIST 1.1.bData presented as % (95% CI); 95% CI based on the Clopper-Pearson method.
Clinical Response With Enfortumab Vedotin in mUC Patients With or Without Prior CPI or Liver Metastases
6
6
Jonathan E. Rosenberg

Clinical Response With Enfortumab Vedotin in mUC Patients With or Without Prior CPI or Liver Metastases
6
7
Prior CPI Treatmenta CPI-Naïvea Liver Metastasesa
1.25 mg/kg
(n=89)
1.25 mg/kg
(n=23)
1.25 mg/kg
(n=33)
Confirmed CR 3.4% 9% 0
Confirmed PR 37% 35% 39%
Confirmed ORRb (95% CI)40%
(30.2, 51.4)
44%
(23.2, 65.5)
39%
(22.9, 57.9)
SD 34% 17% 21%
DCRb (95% CI)74%
(63.8, 82.9)
61%
(38.5, 80.3)
60%
(42.1, 77.1)
Data cut-off date is April 9, 2018.
Data presented as n (%), unless otherwise indicated.
CR, complete response; CPI, checkpoint inhibitor, DCR, disease control rate (DCR=CR+PR+SD); PR, partial response; ORR, overall response rate (ORR=CR+PR);
SD, stable disease. aEvaluable patients must have at least one post-baseline assessment; responses assessed per RECIST 1.1.bData presented as % (95% CI); 95% CI based on the Clopper-Pearson method.
Jonathan E. Rosenberg

Progression-Free Survival in Patients With mUC Treated With Enfortumab Vedotin 1.25 mg/kg
6
8
Jonathan E. Rosenberg
Median PFS, Months (95% CI)
All patients with mUC 5.4 (5.1, 6.2)
Patients with prior
CPI5.4 (5.1, 6.2)

Preliminary Overall Survival in Patients With mUC Treated With Enfortumab Vedotin 1.25 mg/kg
6
9
Jonathan E. Rosenberg
Overall Survival
OS at 6 Months, %
All patients with mUC 74.4
Patients with prior
CPI75.6
OS at 12 Months, %
All patients with mUC 56.3
Patients with prior
CPI54.2
Data cut-off date is April 9, 2018.

Trials in Progress
• Phase II trial of Enfortumab Vedotin
– Platinum treated cohort: 100 patients closed to accrual
– Cisplatin ineligible, carboplatin naïve: Accruing, targeting 100 patients
• Phase I trial of Enfortumab Vedotin +pembrolizumab
• Phase III trial of Enfortumab Vedotin vs chemotherapy
(paclitaxel, docetaxel, vinflunine)in checkpoint failures

Sacituzumab Govitecan (IMMU- 132)
in Patients With Previously Treated Metastatic
Urothelial Cancer (mUC):
Results From a Phase I/II Study
Scott T. Tagawa1, Bishoy Faltas1, Elaine T. Lam2, Philip Saylor3, Aditya Bardia3, Julio J. Hajdenberg4, Alicia K.
Morgans5, Emerson Lim6, Kevin Kalinsky6, Pamela Simpson7, Matthew D. Galsky8, Robert M. Sharkey9,
David M. Goldenberg9†, Trishna Goswami9, William A. Wegener9, Daniel Petrylak10
1Weill Cornell Medicine, New York, NY; 2University of Colorado Cancer Center, Aurora, CO; 3Massachusetts General Hospital Cancer
Center, Harvard Medical School, Boston, MA; 4University of Florida Health Cancer Center, Orlando, FL; 5Vanderbilt Ingram Cancer Center,
Nashville, TN; 6Columbia University Irving Medical Center-Herbert Irving Comprehensive Cancer Center, New York, NY; 7Helen F. Graham
Cancer Center, Christiana Care Health System, Newark, DE; 8Icahn School of Medicine Mount Sinai, Tisch Cancer Institute, New York, NY; 9Immunomedics, Inc., Morris Plains, NJ; 10Yale School of Medicine, Yale Cancer Center, New Haven, CT.
*Work done while Chairman and Chief Scientific Officer of Immunomedics, Inc.
View Poster Board #B5; Feb 15th 5:15 PM

mUC results in IMMU-132-01 Study
Trop-2: trophoblast cell surface antigen 2; 1. Avellini et al. Oncotarget 2017;8:58642.. 2. Starodub et al. Clin Cancer Res 2015;21:3870. 3. Cardillo et al. Clin Cancer Res. 2011;17:3157-3169. 4. Sharkey et al. Clin Cancer Res. 2015;21:5131-
5138. 5. Cardillo et al. Bioconjugate Chem. 2015;26:919-931. 6.Govindan et al. Mol Cancer Ther. 2013;12:968-978. 7. Faltas et al. Nat Genet. 2016;48:1490-1499. 8. Bardia et al. J Clin Oncol. 2017;35:2141-2148
• Trop-2 is an epithelial cell surface antigen
highly expressed in UC1.
• Sacituzumab govitecan is distinct from
other ADCs:2-6
− High drug-to-antibody ratio5
− Hydrolysis of the linker releases the
SN-38 cytotoxic intracellularly and in
the tumor microenvironment. Thus,
Sacituzumab govitecan-bound tumor
cells are killed by intracellular uptake
of SN-38, and adjacent tumor cells are
killed by SN-38 released
extracellularly6
• Sacituzumab govitecan has shown
preclinical and clinical activity.3,7,8
Humanized anti-Trop-2
antibody
• Directed towards Trop-
2, an epithelial antigen
expressed on many
solid cancers
Linker for SN-38
• Hydrolysable linker for
payload release
• High drug-to-antibody
ratio (7.5:1)5
SN-38 payload
• SN-38 more potent than
parent compound,
irinotecan
• In xenograft models,
ADC delivers up to 136-
fold more SN-38 than
irinotecan
Sacituzumab Govitecan is a Trop-2-Directed
Antibody-Drug Conjugate (ADC)
72

mUC results in IMMU-132-01 Study
Demographic and Baseline Characteristics
Characteristic N=45
Age (y), median (range) 67 (49, 90)
Male, n (%) 41 (91)
Race, n (%)
White 39 (87)
Black 2 (4)
Asian 1 (2)
Other 2 (4)
Not reported 1 (2)
ECOG PS, n (%)
0 14 (31)
1 31 (69)
Visceral metastatic sites, n (%) 33 (73)
Lung 27 (60)
Liver 15 (33)
Other 5 (11)
Nonvisceral metastatic sites, n (%) 12 (27) *Placeholder for Bellmunt risk groups description.
Characteristic N=45
Median prior anticancer regimens, range 2 (1-6)
Median prior anticancer regimens in CPI-treated
pts (n=17), range
3 (1-6)
Lines of prior therapies, n, (%)
≤2 prior lines 28 (62)
≥3 prior lines 17 (38)
Bellmunt risk groups*, n, (%)
Low 25 (56)
Intermediate 16 (36)
High 4 (9)
73
*Risk factors are ECOG PS >0, presence of liver metastases, and hemoglobin <10 g/dL

mUC results in IMMU-132-01 Study
Adverse Events (Worst Grade CTCAE) ≥20% or 5% grade
≥3 (Regardless of Causality; N=45)
• Most frequent SAEs included:
– Febrile neutropenia, diarrhea and
neutrophil count decreased in 2 pts each
– 24% of pts used GCSF
• No treatment-related deaths
• 6/45 pts discontinued due to AE not related to
progressive disease
– No patient discontinued due to
neutropenia
– And one patient discontinued due to
diarrhea
GCSF, granulocyte colony-stimulating factor; SAE, serious adverse event.
74
Event All Grades (%) Grades 3 (%) Grade 4 (%)
Diarrhea 69 9 0
Nausea 67 2 0
Fatigue 58 9 0
Neutropenia* 51 22 16
Constipation 44 0 0
Alopecia 40 0 0
Decreased appetite 38 0 0
Anemia 33 13 0
Cough 31 0 0
Vomiting 31 2 0
Pyrexia 24 0 0
Back pain 22 0 0
Dizziness 22 0 0
Rash 22 0 0
Hypophosphatemia 20 11 0
Febrile neutropenia 7 7 0
*Combined terms of Neutropenia' or 'Neutrophil count decrease'.

mUC results in IMMU-132-01 Study
Objective Response Rate by Subgroup
75
Objective Response Rate, % (n/N) [95% CI]
Overall cohort 31.1 (14/45) [18.2, 46.6]
Lines of prior therapies
≤2 prior lines 39.3 (11/28) [21.50, 59.42]
≥3 prior lines 17.6 (3/17) [3.80, 43.43]
Prior checkpoint inhibitors
(median of 3 prior lines of therapy)23.5 (4/17) [6.81, 49.90]
Prior platinum and checkpoint
inhibitors26.7 (4/15) [7.79, 55.10]
Visceral involvement at study entry
Yes 27.3 (9/33) [13.30, 45.52]
Liver 33.3 (5/15) [11.82, 61.62]
No 41.7 (5/12) [15.17, 72.33]

mUC results in IMMU-132-01 Study
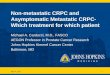
Best Percent Change From Baseline in Tumor Size*
76
CR, complete response; PD, progressive disease; PR, partial response; SD, stable disease. *Based on the sum of the diameters of the target lesions (longest for non-nodal, short axis for nodal
lesions); †pt had % change of 0 with best overall response of PD; ‡qualified for CR based on lymph node target lesion shrinkage to <10 mm. **One subject had 100% reduction of target lesions, but
limited response in non-target lesions, hence classified as PR.
†
‡
Be
st P
erc
en
t C
ha
nge
Fro
m B
ase
line
Ta
rge
t L
esio
ns
• Excludes 5 pts with no post-baseline scans
**

mUC results in IMMU-132-01 Study
Patients With Objective Responses (n=14/45)
77
EndpointOverall
(N=45)
ORR (CR or PR), n (%) [95% CI]14 (31)
[18.2, 46.6]
CR, n (%) 2 (4)
PR, n (%) 12 (27)
Time to onset of response (mo),
Median
(Range)
1.9
(1.7, 7.4)
Duration of response (mo),
Median
(Range)
12.9
(1.3, 29.4+)
Censored: subjects whose duration of responses are censored due to missing 2 tumor assessments or
discontinuation
Three patients have ongoing response with durations of 16.9+, 18.7+, and 29.4+ months and all three of
them are still on treatment
and all three of them are still on treatment
• 50% of responders demonstrated
a DoR of ≥ 12 mo

mUC results in IMMU-132-01 Study
Progression-Free and Overall Survival*
78
At risk:P
rob
ab
ility
of O
S
Pro
ba
bili
ty o
f P
FS
Progression-Free Survival Overall Survival
45 29 19 13 8 6 5 3 2 2 1 0 45 40 32 30 25 23 17 12 9 7 6 3 2 1 0
Median PFS
7.3 months
(95% CI: 5.0, 10.7)
39 42 450 3 6 9 12 15 18 21 24 27 30 33 36
Time (months) Time (months)
Median PFS
7.3 months
(95% CI: 5.0, 10.7)
0 3 6 9 12 15 18 21 24 27 30 33 36
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0
Median OS
16.3 months
(95% CI: 9.0,
31.0)
*Data as of Sept 1, 2018; PFS: 3 progression-free pts have an ongoing response and on treatment; OS: 5 live pts still on treatment. OS, overall survival; PFS,
progression-free survival.

mUC results in IMMU-132-01 Study
Summary
• Sacituzumab govitecan, a novel Trop-2-directed ADC, demonstrated clinically significant activity in pts with heavily pre-treated relapsed/refractory mUC
– ORR: 31% (2 CR, 12 PR) overall with an ORR of 39% in those with ≤2 prior lines of treatment• 26.7% in CPI- and platinum-treated pts
• 33.3% in pts with liver metastases
– Median duration of response: 12.9 months
– Median PFS: 7.3 months
– Median OS: 16.3 months
• Sacituzumab govitecan was well tolerated, with a predictable safety profile
– Most common treatment-emergent AEs were neutropenia and diarrhea, which were manageable
– Low rate of patient discontinuation due to AEs• No patients discontinued due to neutropenia and 1 patient discontinued due to diarrhea
– No treatment-related deaths
• In conclusion, sacituzumab govitecan demonstrated significant clinical activity in pts with relapsed/refractory mUC, including pts with prior CPI + platinum treatment and visceral disease
79

mUC results in IMMU-132-01 Study
TROPHY-U-01 (IMMU-132-06) StudyA Phase II Open Label, Study of IMMU-132 in Metastatic Urothelial Cancer After Failure of
Platinum-based Regimen or Anti-PD-1/ PD-L1 Based Immunotherapy
• Results from the Study-01 basket trial warranted further investigation in a dedicated phase 2 trial.
• TROPHY-U-01 (NCT03547973) is an international, single-arm, open-label, phase 2 trial evaluating
the antitumor activity and safety of sacituzumab govitecan in 140 pts with advanced UC.
80
View TROPHY-U-01 Poster on Feb 15th TPS #495; Poster Board #N5
NCT Trial Number: 03547973
PD-1, programmed cell death-1; PD-L1, programmed death ligand-1.
Continue
treatment in the
absence of
unacceptable
toxicity or PD
Sacituzumab Govitecan 10 mg/kg
Days 1 and 8, every 21 days
Objectives:
• Overall response rate
(ORR) will be centrally
reviewed
• Duration of response
(DOR)
• Progression-free survival
(PFS)
• Overall survival (OS)
Cohort 1 (100 patients): pts who
progressed after prior platinum-
based and anti PD-1/anti PD-L1
based therapies.
Cohort 2 (40 patients): pts ineligible
for platinum-based therapy and who
progressed after prior anti PD-1/anti
PD-L1 based therapies.
Recommended