
Application of Genetic Tools to Application of Genetic Tools to Clinical and Translational Clinical and Translational
ResearchResearch
Thomas A. Pearson, MD, PhDUniversity of Rochester
School of MedicineVisiting Scientist, NHGRI
TAProots VineyardTAProots Vineyard Keuka Lake, NY Keuka Lake, NY

Concord GrapesConcord Grapes
One year old French hybrid One year old French hybrid grapesgrapes
Vanessa Seedless GrapesVanessa Seedless Grapes

Lecture 8. Application of Genetic Tools Lecture 8. Application of Genetic Tools to Clinical and Translational Researchto Clinical and Translational Research
1. Examine the basis for inferring that gene variants are causal for a disease.
2. Consider the use of genetic tools in personalized medicine
a. Genetic Screening/susceptibility assessment
b. Pharmacogenomics3. Discuss the application of genetic tools to
future observational and experiential studies.
Contributions of GWAS to Contributions of GWAS to Basic ScienceBasic Science
Genome structure and function Exons, introns
Regulatory elements
Novel mechanisms of diseaseProteins as therapeuticsDrug targets
• Mass screening of small molecule inhibitors
U.S. Surgeon General’sU.S. Surgeon General’sCriteria for Causal AssociationCriteria for Causal Association
1. Temporal relationship2. Strength of the association3. Dose-response relationship4. Replication of findings5. Biologic plausibility6. Consideration of alternate explanations7. Cessation of exposure8. Consistency with other knowledge9. Specificity of the association
* Report of the Advisory Committee to the Surgeon General, 1964

GWAS and the U.S. Surgeon General’s GWAS and the U.S. Surgeon General’s Criteria for Causal AssociationCriteria for Causal Association
Criteria GWAS Evidence
1. Temporal Relationship Genome precedes disease
?Expression of gene
2. Strength of association Multiple SNP’s and other gene variants
?Composite risk of all variants known or unknown
3. Dose-response relationship
Number of alleles
Recessive vs. Dominant
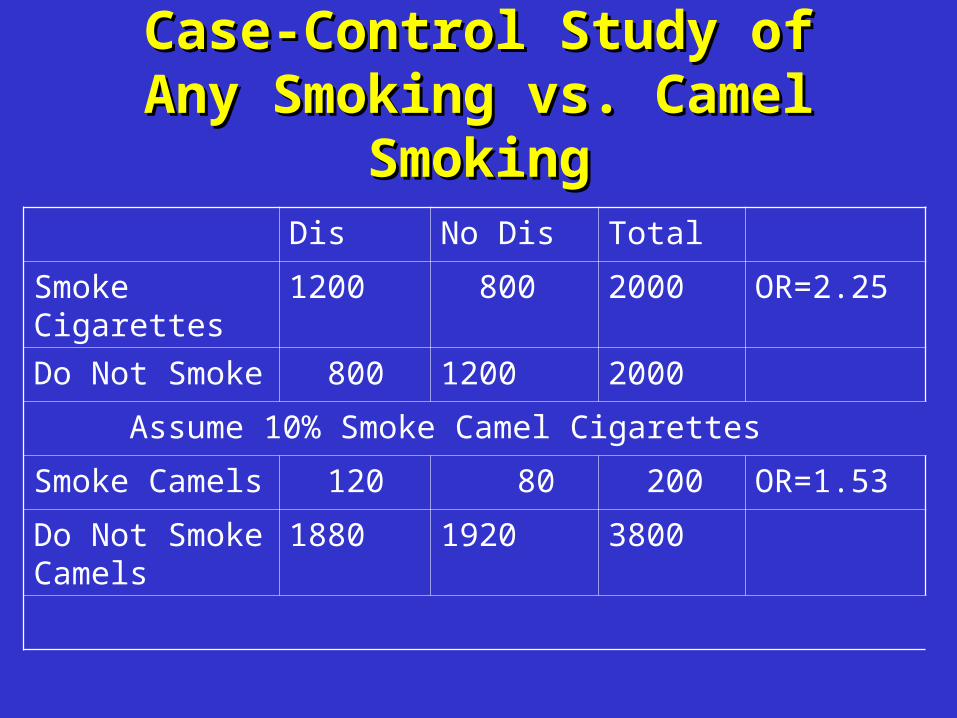
Case-Control Study of Any Case-Control Study of Any Smoking vs. Camel SmokingSmoking vs. Camel Smoking
Dis No Dis Total
Smoke Cigarettes
1200 800 2000 OR=2.25
Do Not Smoke 800 1200 2000
Assume 10% Smoke Camel Cigarettes
Smoke Camels 120 80 200 OR=1.53
Do Not Smoke Camels
1880 1920 3800
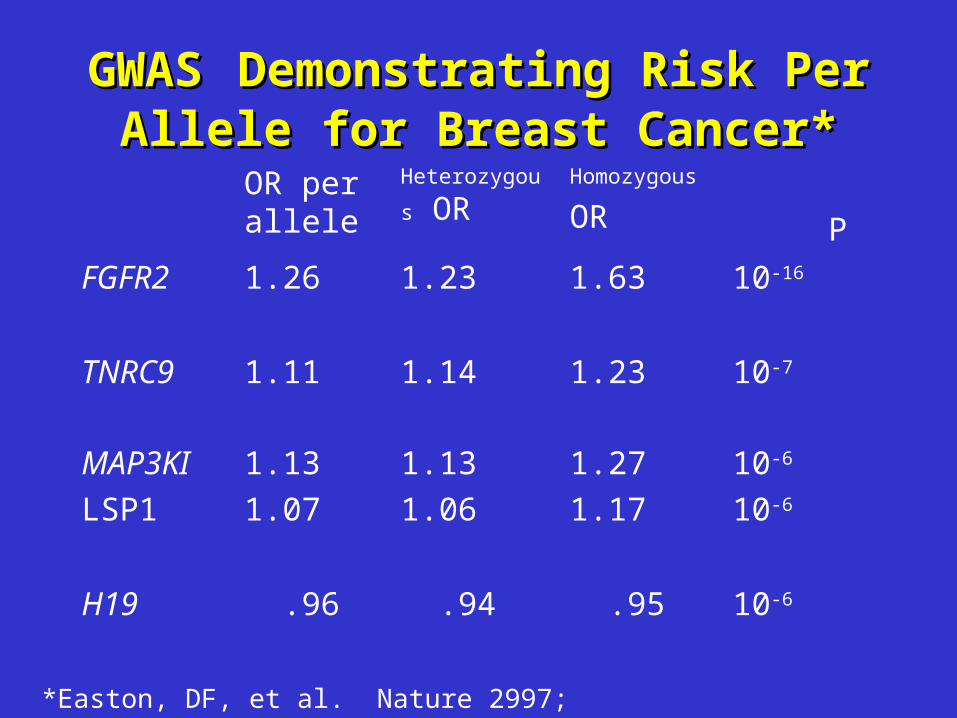
GWASGWAS Demonstrating Risk Per Demonstrating Risk Per Allele for Breast Cancer*Allele for Breast Cancer*
OR per allele
Heterozygous OR
Homozygous
OR P
FGFR2 1.26 1.23 1.63 10-16
TNRC9 1.11 1.14 1.23 10-7
MAP3KI
LSP1
1.13
1.07
1.13
1.06
1.27
1.17
10-6
10-6
H19 .96 .94 .95 10-6
*Easton, DF, et al. Nature 2997; 447: 1087-1093
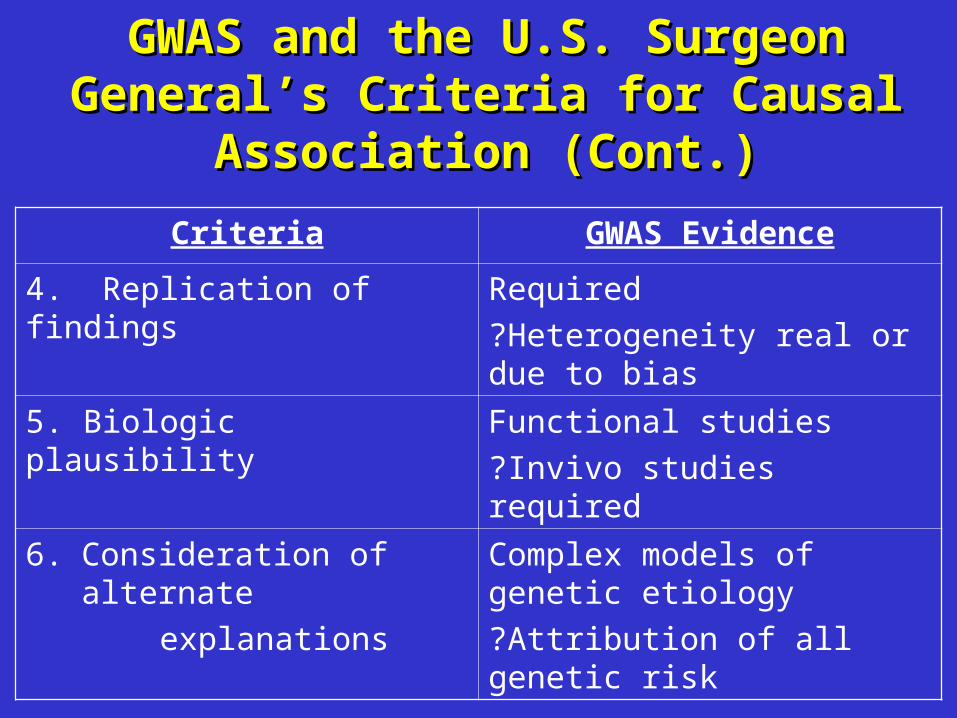
GWAS and the U.S. Surgeon General’s GWAS and the U.S. Surgeon General’s Criteria for Causal Association (Cont.)Criteria for Causal Association (Cont.)
Criteria GWAS Evidence
4. Replication of findings Required
?Heterogeneity real or due to bias
5. Biologic plausibility Functional studies
?Invivo studies required
6. Consideration of alternate
explanations
Complex models of genetic etiology
?Attribution of all genetic risk

Possible Explanations of Possible Explanations of Heterogeneity of Results in Genetic Heterogeneity of Results in Genetic
Association StudiesAssociation Studies• Biologic mechanisms
– Genetic heterogeneity– Gene-gene interactions– Gene-environment interactions
• Spurious mechanisms– Selection bias– Information bias– Publication bias
Confounding (population stratification)– Cohort, age, period (secular effects– Type I error

Structure of Human Genes:Structure of Human Genes:Potential Sites of Gene VariationPotential Sites of Gene Variation
• Exons• Introns• Regulatory Elements
– Promoters– PolyA Tail– Enhanceers– Silencers– Locus Control Regions
GWAS to Identify Novel Breast GWAS to Identify Novel Breast Cancer Susceptibility Loci*Cancer Susceptibility Loci*
• Known breast cancer loci explain <25% of familial risk.
• Two stage study of 4398 cases and 4316 controls with replication of 30 SNP’s in 21,860 cases and 22,578 controls.
• 227,876 SNP’s genotyped.• 5 novel loci related to breast cancer at P<I0-7
explain an additional 3.6% of familial risk.• 1792 additional SNP’s associated at P<.05
with 1343 expected, suggesting many additional susceptibility alleles exist.
Easton DF, et al. Nature 2007; 447: 1087-1093
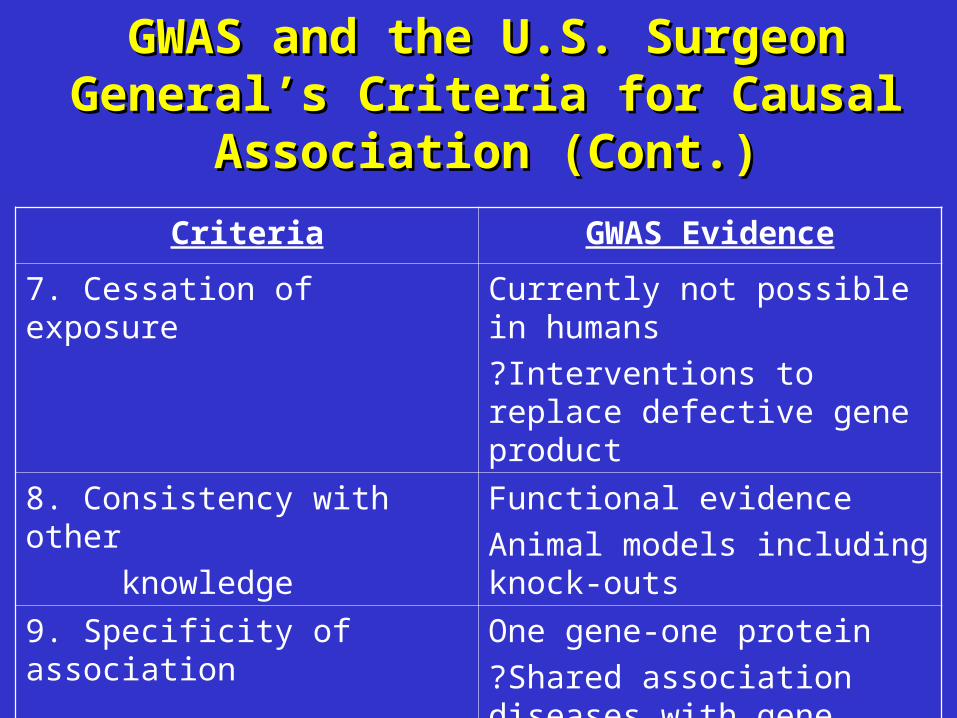
GWAS and the U.S. Surgeon General’s GWAS and the U.S. Surgeon General’s Criteria for Causal Association (Cont.)Criteria for Causal Association (Cont.)
Criteria GWAS Evidence
7. Cessation of exposure Currently not possible in humans
?Interventions to replace defective gene product
8. Consistency with other
knowledge
Functional evidence
Animal models including knock-outs
9. Specificity of association One gene-one protein
?Shared association diseases with gene variants
Intervention in Children with Hutchinson-Intervention in Children with Hutchinson-Gilford Progeria Syndrome*Gilford Progeria Syndrome*
• Rare disorder of accelerated aging with death from cardiovascular disease by age 13 years.
• Defect is a glycine GGC to glycine GGT in codon 608 of exon 11 of lamin A gene.• Activates a cryptic splice donor to produce an abnormal
protein, Lamin A.• Lamin A or progerin cannot release from farnesyl-cysteine
tether site on the nuclear membrane and alters transcription.• Farnesyl transferase inhibition prevents anchoring of progerin in
fibroblasts and in transgenic mouse models.• Open label clinical trial of inhibition of farnesyl transferase with
ABT 100 is underway.
*Merideth MA, et. al. NEJM 2008; 358: 592-604

GWAS Identifies Gene Variant rs4430796 GWAS Identifies Gene Variant rs4430796 Which Confers Risk for Prostate Cancer Which Confers Risk for Prostate Cancer
and Protection from Type 2 Diabetes*and Protection from Type 2 Diabetes*Iceland All Groups in
Replication Study
Prostate Cancer
Cases/Controls 1501/11289 3490/14345
OR 1.20 1.22
95% CI 1.11-1.31 1.15-1.30
P 1.4 x 10-5 1.4 x 10-11
Type 2 Diabetes
Cases/Controls 1380/9840 9936/23087
OR .86 .91
95% CI .78-.95 .87-.94
P .0021 2.7 x 10-7
*Gundmundsson J, et al. Nat Gen 7/1/07

Personalized MedicinePersonalized Medicine
“At its most basic, personalized medicine refers to using information about a person’s genetic make-up to tailor strategies for detection, treatment, and prevention of disease”
Francis Collins,Director, NHGRI7/17/05
Screening of Family Members of Screening of Family Members of Patients Admitted with Coronary Patients Admitted with Coronary
Heart DiseaseHeart Disease
• 5620 consecutive patients admitted to 53 randomly selected hospitals for MI, coronary bypass or angioplasty, or unstable angina.
• Medical record review of discharge plans.– 37/5620 (0.7%) identified plan to screen first
degree relatives.
• Follow-up 6 months after discharge– 16% of children screened for risk factors.– Little variance based on risk or risk factors of
proband.
Swanson JR, Pearson TA. Am J Prev Med 2001; 20:50-55
Larson, G. The Complete Far Side. 2003.

The U.S. Surgeon General’s The U.S. Surgeon General’s Family History InitiativeFamily History Initiative
• My Family Health Portrait• Web-based tool to collect and organize family
history information
https://familyhistory.hhs.gov• Printout for sharing with healthcare providers
• National Family History Day (Thanksgiving)• Encourage Americans to talk about and write
down health problems running in their family
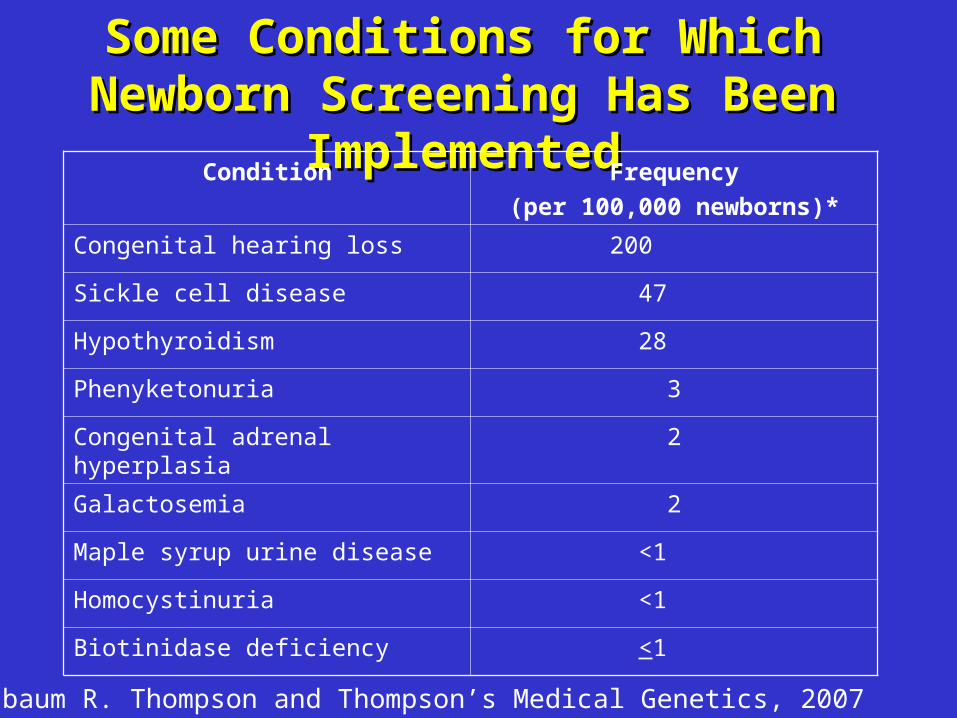
Some Conditions for Which Newborn Some Conditions for Which Newborn Screening Has Been ImplementedScreening Has Been Implemented
Condition Frequency
(per 100,000 newborns)*
Congenital hearing loss 200
Sickle cell disease 47
Hypothyroidism 28
Phenyketonuria 3
Congenital adrenal hyperplasia 2
Galactosemia 2
Maple syrup urine disease <1
Homocystinuria <1
Biotinidase deficiency <1
Nussbaum R. Thompson and Thompson’s Medical Genetics, 2007

Criteria for an Effective Criteria for an Effective Screening ProgramScreening Program
Analytic Validity Clinical Validity Clinical Utility 1. Condition is frequent to justify cost
2. Detection would otherwise not occur at early enough stage
3. Early treatment prevents morbidity 4. Treatment is available
5. Families and personnel available to perform screening, inform about results, and
institute treatment.
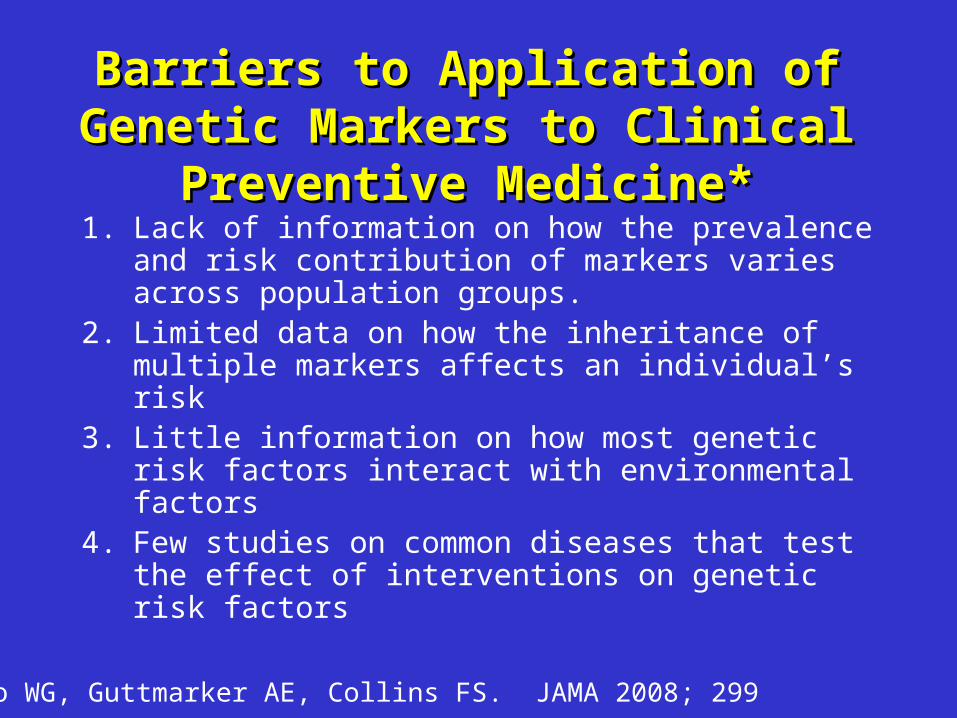
Barriers to Application of Genetic Barriers to Application of Genetic Markers to Clinical Preventive Markers to Clinical Preventive
Medicine*Medicine*1. Lack of information on how the prevalence
and risk contribution of markers varies across population groups.
2. Limited data on how the inheritance of multiple markers affects an individual’s risk
3. Little information on how most genetic risk factors interact with environmental factors
4. Few studies on common diseases that test the effect of interventions on genetic risk factors
Faero WG, Guttmarker AE, Collins FS. JAMA 2008; 299
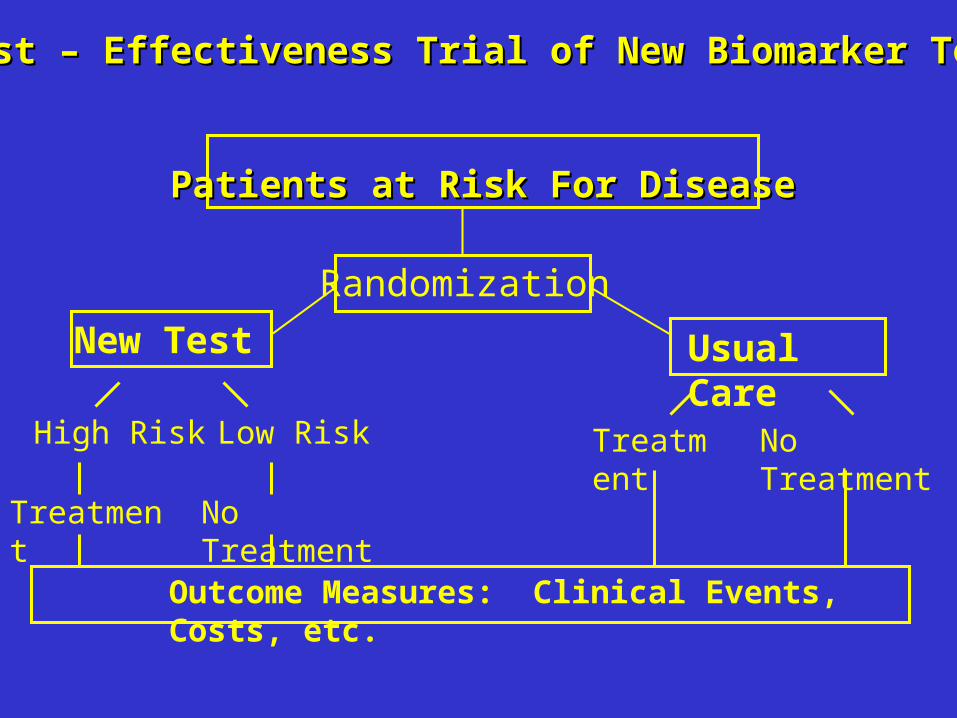
Cost – Effectiveness Trial of New Biomarker Test Cost – Effectiveness Trial of New Biomarker Test
Patients at Risk For DiseasePatients at Risk For Disease
Usual Care
No TreatmentTreatment
Treatment No Treatment
High Risk Low Risk
Outcome Measures: Clinical Events, Costs, etc.
Randomization
New Test

Commercial Direct-to-Commercial Direct-to-Consumer Genomic Testing*Consumer Genomic Testing*
Type of Testing Tests Offered
Whole genome Complex trait risk screening based on SNPs discovered through ongoing research
Single or Multiple Trait Testing for conditions or specific diseases by using proprietary SNP panels or ongoing research
Ancestry Paternity and family relations testing using mitochondrial or y chromosomal genotyping or SNP panels
Other Products or recommendations (e.g. diet) based on SNP panels
*Offit K. JAMA 2008, 299; 1353-4
Larson, G. The Complete Far Side. 2003.
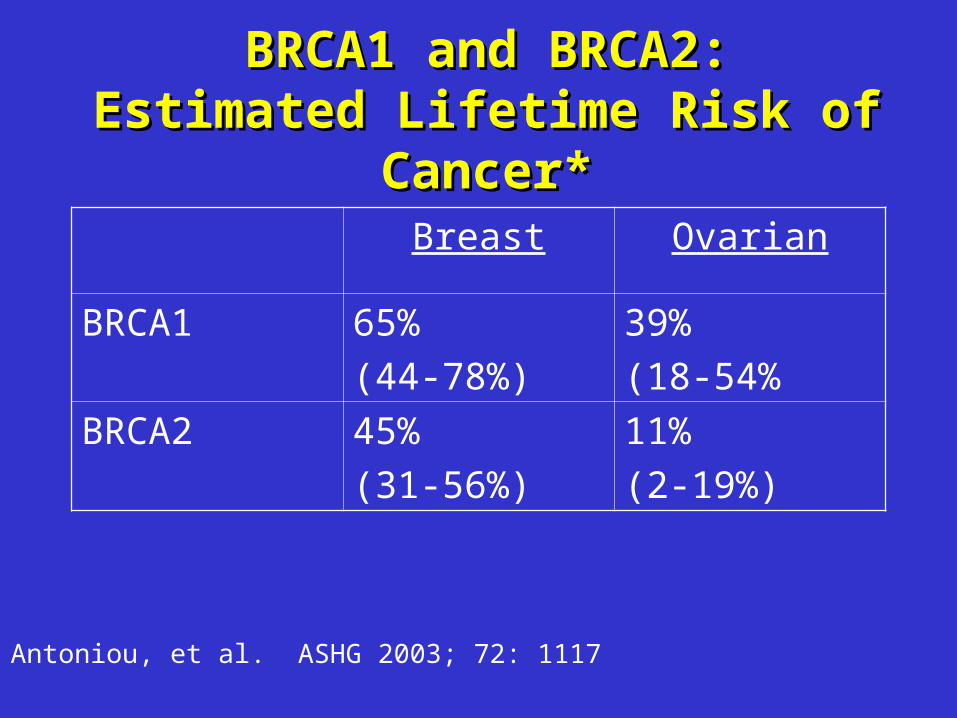
BRCA1 and BRCA2:BRCA1 and BRCA2:Estimated Lifetime Risk of Cancer*Estimated Lifetime Risk of Cancer*
Breast Ovarian
BRCA1 65%
(44-78%)
39%
(18-54%
BRCA2 45%
(31-56%)
11%
(2-19%)
Antoniou, et al. ASHG 2003; 72: 1117
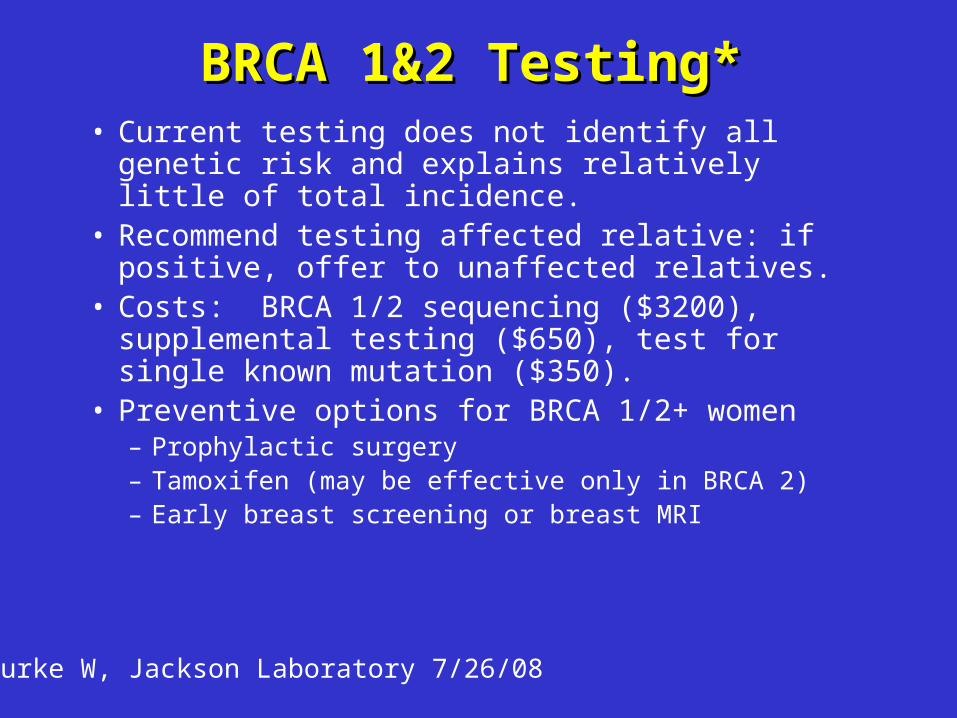
BRCA 1&2 Testing*BRCA 1&2 Testing*• Current testing does not identify all genetic risk and
explains relatively little of total incidence.• Recommend testing affected relative: if positive,
offer to unaffected relatives.• Costs: BRCA 1/2 sequencing ($3200),
supplemental testing ($650), test for single known mutation ($350).
• Preventive options for BRCA 1/2+ women– Prophylactic surgery– Tamoxifen (may be effective only in BRCA 2)– Early breast screening or breast MRI
Burke W, Jackson Laboratory 7/26/08

Delivery of Genomic Medicine for Delivery of Genomic Medicine for Common Chronic Diseases: A Common Chronic Diseases: A
Systematic ReviewSystematic ReviewAreas Assessed Key Findings
Outcomes of genetic services
(13 studies, 3 systematic reviews)
Consumer information needs
(1 systematic review, 1 RCT, 14 studies)
Barriers to integrations (1 systematic review, 19 studies)
•Modest positive effects on anxiety•Mixed results on behavior change•Few studies on clinical outcomes•Low levels of genetics knowledge•Positive attitudes•Inadequacy of primary care workforce•Lack of oversight of testing•Privacy and discrimination
Scheuner MT, et al. JAMA 2008; 299: 1320-1334
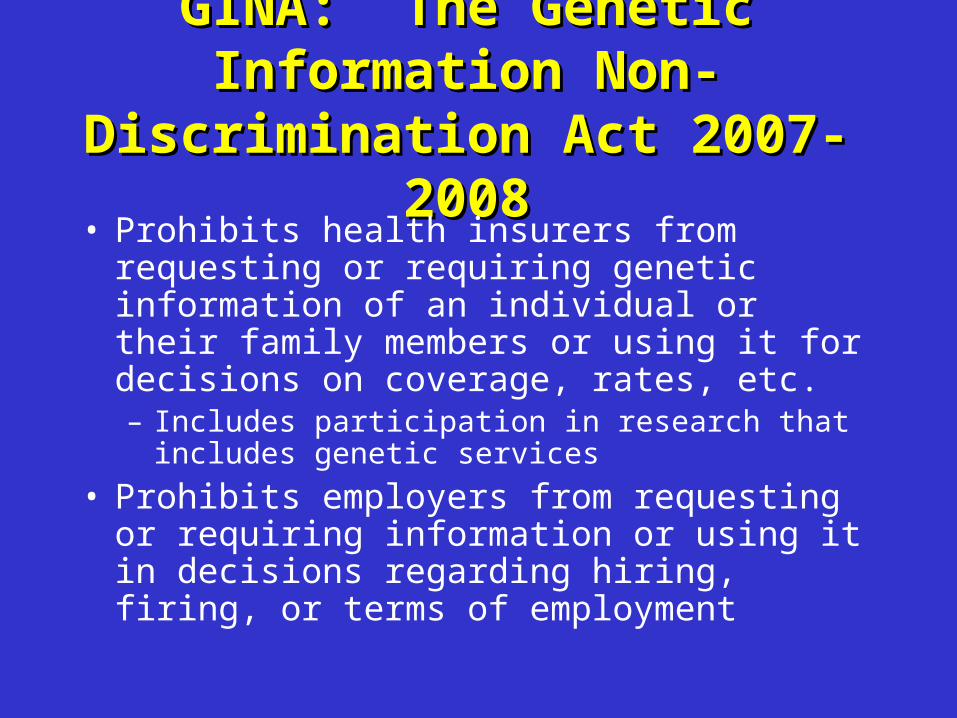
GINA: The Genetic Information GINA: The Genetic Information Non-Discrimination Act 2007-2008Non-Discrimination Act 2007-2008
• Prohibits health insurers from requesting or requiring genetic information of an individual or their family members or using it for decisions on coverage, rates, etc.– Includes participation in research that includes
genetic services
• Prohibits employers from requesting or requiring information or using it in decisions regarding hiring, firing, or terms of employment

PharmacogeneticsPharmacogenetics: The study of : The study of differences in drug response due to differences in drug response due to
allelic variation in genes affecting drug allelic variation in genes affecting drug metabolism, efficacy, and toxicity.metabolism, efficacy, and toxicity.
• Drug metabolism under genetic control– Hydroxylation– Conjugation
• Glucuronidation• Acetylation• Methylation
• Phenotypes of drug metabolismNormal metabolizersPoor metabolizersUltrafast metabolizers
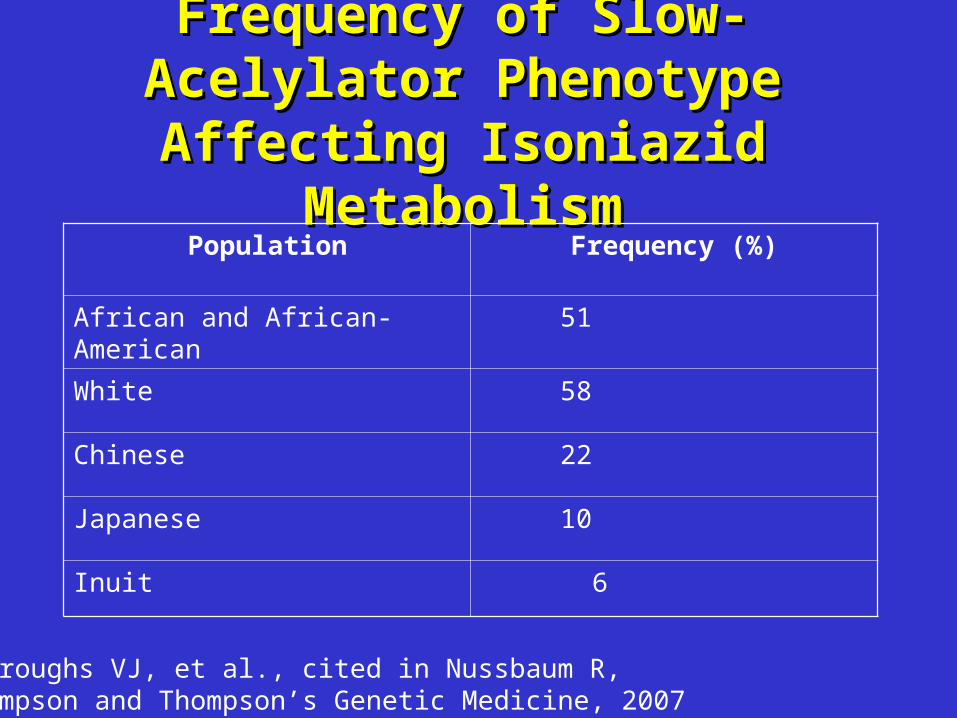
Frequency of Slow-Acelylator Frequency of Slow-Acelylator Phenotype Affecting Isoniazid Phenotype Affecting Isoniazid
MetabolismMetabolismPopulation Frequency (%)
African and African-American 51
White 58
Chinese 22
Japanese 10
Inuit 6
Burroughs VJ, et al., cited in Nussbaum R, Thompson and Thompson’s Genetic Medicine, 2007
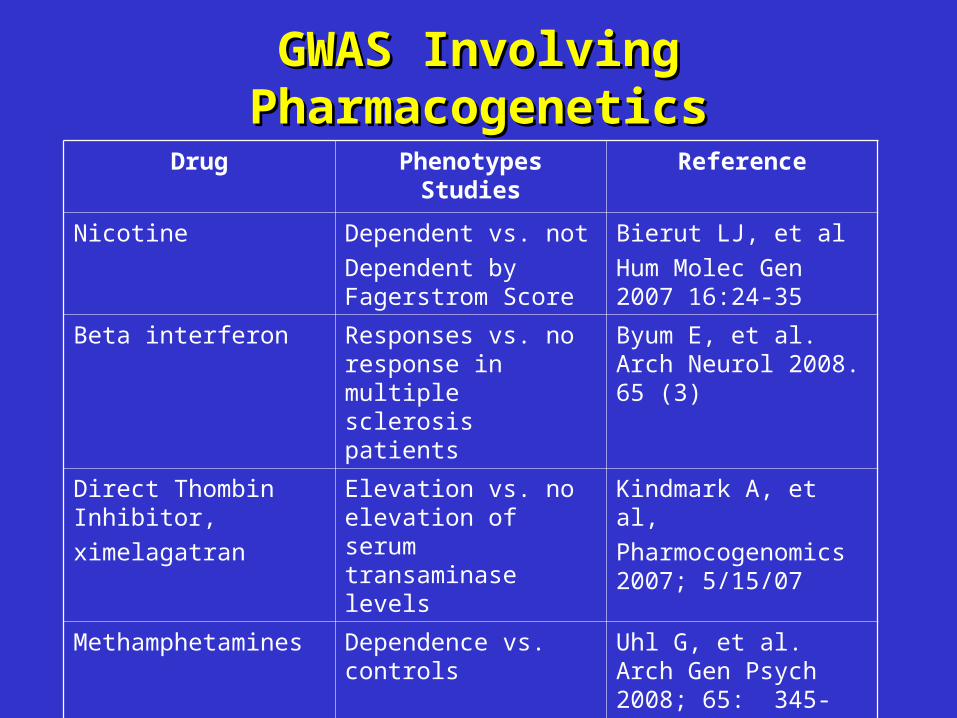
GWAS Involving GWAS Involving PharmacogeneticsPharmacogenetics
Drug Phenotypes Studies Reference
Nicotine Dependent vs. not
Dependent by Fagerstrom Score
Bierut LJ, et al
Hum Molec Gen 2007 16:24-35
Beta interferon Responses vs. no response in multiple sclerosis patients
Byum E, et al. Arch Neurol 2008. 65 (3)
Direct Thombin Inhibitor,
ximelagatran
Elevation vs. no elevation of serum transaminase levels
Kindmark A, et al,
Pharmocogenomics 2007; 5/15/07
Methamphetamines Dependence vs. controls
Uhl G, et al. Arch Gen Psych 2008; 65: 345-355
Nicotine Inability to quit vs. able to quit smoking
Uhl G, et al. BMC Genetics 2007; 8:10
Policy for Sharing of Data Obtained Policy for Sharing of Data Obtained in NIH Supported and Conducted in NIH Supported and Conducted
GWAS (NOT-OD-07-088)GWAS (NOT-OD-07-088) Goal:
To make available the genotype and phenotype datasets as rapidly as possible to a wide range of scientific investigators.
Components:Data repository (NCBI, dbGAP)Data submission and protectionData accessPublicationIntellectual property

Investigators Requesting and Investigators Requesting and Receiving GWAS DataReceiving GWAS Data
• Submit a description of proposed research project
• Submit a data access request, co-signed by Institutional Official
• Protect data confidentiality• Ensure data security measures are in place • Notify appropriate Data Access Committee of
policy violations, if any• Submit annual reports on research findings

ConclusionsConclusions1. Evidence for the causal association of gene
polymorphisms in common chronic diseases is still in formative stages
2. Application of products of genomics research such as susceptibility assessment and pharmacogenomics holds promise but barriers persist
• Technologies are currently being marketed to consumers• Survey evidence suggesting low level of genetic knowledge in
consumers and low levels of skills in providers
3. Genome research has been a boom for basic scientists; clinical investigators should ready themselves to participate in this developing field

Sample Collection Sample Collection andand Processing Processing
• Obtaining samples for DNA preparation– Blood– Buccal cells– Serum– Pathology specimens– Other?
• Purifyign and quantifying DNA• Whole genome amplification (WGA)• Trace individual DNAs (QC)
Courtesy S. Chanock, NCi
Recommended

















