Antibiotic steward

Antibiotic Stewardship
& the Infection Preventionist
*Promoting Antimicrobial Stewardship in Human Medicine Infectious Disease Society of America http://www.idsociety.org/Stewardship_Policy/#sthash.7G8b9Xis.dpufhttp://www.idsociety.org/Stewardship_Policy/ (Accessed 7/7/2015)
Anthony F Ognjan, DO FACP
2015 MSIPC Annual Fall ConferenceCrowne Plaza Lansing MichiganOctober 8-9 2015

Anthony Ognjan,D.O., FACP
(Hungarian - French Canadian)
Past President, Macomb County Osteopathic Medical Association Chairman, M.O.A. Political Action Committee Member, Counsel of Governmental Affairs (MOA) Vice-Chair MOA House of Delegates (MOA) Associate Professor of Medicine MSU-COM
Diploma. Algonac High School B.S. Microbiology, MSU B.S. Pharmacy, Ferris State College MSU College of Osteopathic Medicine
Hospital Orderly (Orthopedics), Ingham Medical Center Pharmacist, Children's Hospital of Michigan Intern, Detroit Osteopathic Hospital / BCCH Resident, Internal Medicine, Henry Ford Hospital, Detroit Infectious Disease Fellowship, Henry Ford Hospital, Detroit

IDSA:Coordinated Interventions Designed to Improve and Measure the Appropriate use of Antimicrobials
By promoting the selection of the “Optimal” antimicrobial Drug Regimen, Dose, Duration of therapy, and Route of Administration.
Antibiotic Stewardship
*Promoting Antimicrobial Stewardship in Human Medicine Infectious Disease Society of America http://www.idsociety.org/Stewardship_Policy/#sthash.7G8b9Xis.dpufhttp://www.idsociety.org/Stewardship_Policy/ (Accessed 7/7/2015)

Antibiotic Stewardship
Needs Assessment
• RECOGNIZING: Antimicrobial resistance has emerged as a significant Healthcare Quality and patient Safety issue
• APPRECIATING: Dwindling Antimicrobial options. (critical threat to the public health of the United States.
• OPPORTUNITY: Antimicrobial stewardship Programs Optimize antimicrobial use to achieve the best clinical outcomes
- Minimizing Adverse Infection Events
- Limit Selective Pressures Driving the Emergence of Resistance
• COST EFFECTIVE: Reduce Excessive Costs Attributable to Suboptimal Antimicrobial use
Promoting Antimicrobial Stewardship in Human Medicine http://www.idsociety.org/Stewardship_Policy/

HOW DID WE GET HERE?

As Humans Evolve…..
…..So do Bacteria

Antibiotic Resistance
Historical perspective 1,2
“… A sample of the Culturable Microbiome* of Lechuguilla Cave, New Mexico: • A region of the cave that has been isolated for over 4 million years….• Sample of Surface microbes, were Highly resistant to Antibiotics…• Some strains were Resistant to 14 Different commercially available Antibiotics”
1 Antibiotic Drug-Resistant Cave Bacteria Found Posted by Pharmaceutical International's Global Correspondent on 12/04/2012 http://www.pharmaceutical-int.com/news/antibiotic-drug-resistant-cave-bacteria-found.html 2 Bhullar K, Waglechner N, Pawlowski A, Koteva K, Banks ED, et al. (2012) Antibiotic Resistance Is Prevalent in an Isolated Cave Microbiome. PLoS ONE 7(4): e34953. doi:10.1371/journal.pone.0034953
“Antibiotic resistance is hard-wired into bacteria”It could be billions of years old, but we have only been trying to understand it for the last 70 years" 1 - Dr. Gerry Wright, PhD
*A microbiome is the totality of microbes, their genetic elements (genomes), and environmental interactions in a particular environment -Joshua Lederberg

Antibiotic Resistance
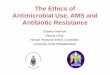
Implications Antibiotic Resistance Emergence of Antibiotic-Resistant Bacteria
Hospital- acquired S. aureus Gram Negative Rods Enterococcus sp. Community-acquired Shigella sp. N. gonorrhoeae H. influenza M.catarrhalis S. pneumonia
1950 1960 1970 1980 1990
Cohen; Science1992;257:1050

Drug Resistance:Antimicrobial Resistance: Global Report on
Surveillance 2014
http://www.who.int/drugresistance/documents/surveillancereport/en/(Accessed 5/5/2014)

AntibioticsDrug Resistance:Antimicrobial resistance: Global Report on Surveillance 2014
• All regions of the world are experiencing resistance to carbapenem antibiotics for treatment of Klebsiella pneumoniae, a major cause of hospital-acquired infections including pneumonia, bloodstream infections, and infections in newborns and intensive care unit patients. Carbapenem antibiotics are last-resort treatment for K pneumoniae and are ineffective in more than half of those treated for K pneumoniae infections in some countries.
• Resistance to Fluoroquinolones, one of the most commonly used antibiotics for the treatment of Escherichia coli–caused urinary tract infections, is very widespread. Fluoroquinolones are now ineffective in more than half of patients in some countries.
• Third-Generation Cephalosporins, the last-resort treatment for Gonorrhea, have been found to be ineffective in Austria, Australia, Canada, France, Japan, Norway, South Africa, Slovenia, Sweden, and the United Kingdom. At least 1 million people are infected with gonorrhea around the world every day.
• Antibiotic Resistance causes patients to be ill longer and increases the risk for death. It is estimated that patients with methicillin-resistant Staphylococcus aureus are 64% more likely to die than those with a nonresistant form of the infection. Healthcare costs are increased in patients with antimicrobial-resistant infections because of longer hospital stays and the need for more intensive care.

Antibiotic Stewardship
Clinical Stake HoldersBasic
Bacteria InfectionResistanceMorbidityMortality
Public Health
HumanMedicine
Veterinary Medicine

Antibiotic Stewardship
Clinical Stake holdersBasic
Bacteria InfectionResistanceMorbidityMortality
Health CareFacilities
Health Care
Providers
Health CarePayers
Physicians / RN Practitioners & PAs Respiratory Therapy Pharmacy RN / Health Aids etc.
Clinical Microbiology Infection Prevention Policies and Practice Environmental services
Private Governmental Agencies
OVERSITE AND REGULATION• Professional Organizations• Local State National: Public Health
Agencies• Local, State, Federal Government

Antibiotic Stewardship
Policy Statement on Antimicrobial Stewardship SHEA IDSA ICHE
Society for Healthcare Epidemiology of America
Infectious Diseases Society of America
Pediatric Infectious Diseases Society
Infection Control and Hospital Epidemiology
Policy Statement on Antimicrobial Stewardship by the Society for Healthcare Epidemiology of America (SHEA), the Infectious Diseases Society of America (IDSA), and the Pediatric Infectious Diseases Society (PIDS). Vol. 33, No. 4, Special Topic Issue: Antimicrobial Stewardship (April 2012), pp. 322-327 http://www.jstor.org/stable/10.1086/665010#full_text_tab_contents

PROGRAM DESIGN GOALS1. Antimicrobial Stewardship Programs Should Be Required through Regulatory Mechanisms. (Local / State/ National)
2. Antimicrobial Stewardship Should Be Monitored in Ambulatory Healthcare Settings
3. Education about Antimicrobial Resistance and Antimicrobial Stewardship Must Be Accomplished: Health care Providers / Patients / Public
4. Antimicrobial Use Data Should Be Collected and Readily Available: -Both Inpatient and Outpatient Antimicrobial Stewardship programs
COST EFFECTIVE PROGRAMS
Antibiotic Stewardship
RECOMMENDATIONSProfessional Societies

September 18, 2014
President Barack Obama (Executive Order 13676)
“The National Action Plan for Combating Antibiotic-Resistant Bacteria”
Developed by the interagency Task Force for Combating Antibiotic-Resistant Bacteria in response to Executive Order

“The National Action Plan for Combating Antibiotic-Resistant Bacteria”
Task Force
DEPARTMENT SECRETARIES:
Defense, Agriculture, and Health and Human Services
DEPARTMENTS
State, Justice, Veterans Affairs,
Homeland Security
Environmental Protection Agency
AGENCIES
United States Agency for International Development
Office of Management and Budget
Domestic Policy Council
National Security Council
Office of Science and Technology Policy
National Science Foundation
NATIONAL ACTION PLAN FOR COMBATING ANTIBIOTIC-RESISTANT BACTERIAIAhttps://www.whitehouse.gov/sites/default/files/docs/national_action_plan_for_combating_antibotic-resistant_bacteria.pdf (Accessed: 8/27/2015)

Polity Plans and Objects
“The National Action Plan for Combating Antibiotic-Resistant Bacteria”
Policy Plans Object
Outlines Federal activities over the next Five years:
Enhance Domestic and International Capacity to prevent and contain outbreaks of Antibiotic-Resistant Infections
Maintain the efficacy of Current and New Antibiotics :
Develop and deploy next-generation:• Diagnostics• Antibiotics • Vaccines• Other therapeutics
Roadmap to guide the Nation in rising to the challenge of antibiotic resistance
“Doubling” the amount of Federal funding for combating and preventing antibiotic resistance to more than $1.2 billion
NATIONAL ACTION PLAN FOR COMBATING ANTIBIOTIC-RESISTANT BACTERIAIAhttps://www.whitehouse.gov/sites/default/files/docs/national_action_plan_for_combating_antibotic-resistant_bacteria.pdf (Accessed: 8/27/2015)

Objects & Goals
“The National Action Plan for Combating Antibiotic-Resistant Bacteria”
Slow the Emergence of Resistant Bacteria and Prevent the Spread of Resistant Infections
Strengthen National One-Health Surveillance Efforts to Combat Resistance
Advance Development and Use of Rapid and Innovative Diagnostic Tests for identification and Characterization of Resistant Bacteria
Accelerate Basic and Applied Research and Development for New Antibiotics, Other Therapeutics, and Vaccines
Improve International Collaboration and Capacities for Antibiotic-resistance Prevention, Surveillance, Control, and Antibiotic Research and Development
-FACT SHEET: Obama Administration Releases National Action Plan to Combat Antibiotic-Resistant Bacteria https://www.google.com/search?site=&source=hp&q=obama+antibiotic+stewardship&oq=obama+antibiotic&gs_l=hp.1.1.0l3.20488.31442.0.33938.25.17.3.5.6.0.147.1806.4j13.17.0....0...1c.1.64.hp..2.23.1700.0.IStFTSPFCuo-NATIONAL ACTION PLAN FOR COMBATING ANTIBIOTIC-RESISTANT BACTERIAIAhttps://www.whitehouse.gov/sites/default/files/docs/national_action_plan_for_combating_antibotic-resistant_bacteria.pdf (Accessed: 8/27/2015)
The Goals of the National Action Plan Include:

ANTIBIOTICS“Against Life”*
*1889 by Louis Pasteur's pupil Paul Vuillemin
Bacteria Fungus
Single “Scoop” of soil, Bacteria and Fungi number in the Millions. With Thousands of Varieties, and survive by “fighting” each other. Past century, several newly discovered Antibiotics have been found by isolating them from the Bacteria and Fungi that produce them to defend their own lives.
(1861–1932
*History of Antibiotics http://inventors.about.com/od/pstartinventions/a/Penicillin_2.htm

Antibiotics :Naturally Occur in the environmentMost available today are “Man made” from previous Antibiotics…
AND therefore, to the Medicinal purists…are considered Chemotherapeutic agents…
Over 60 years the world has been searched and scoured…virtually Hundreds of compounds from all over the world have been discovered and evaluated….
Some Great….Some NOT so Good….

Antibiotic StewardshipGOALS
Regarding Antibiotics• Achieve Optimal Clinical Outcomes • Minimize Toxicity and other Adverse Events• Reduce Infections in Health Care • Limit the Selection for Antimicrobial Resistant Strains.
Promoting Antimicrobial Stewardship in Human Medicine http://www.idsociety.org/Stewardship_Policy/

Antibiotics DO NOT CURE an Infection: You must have a “Reasonably”
Functioning Immune system

Immunity:
Is the “balanced state” of having Adequate Biological Defenses to Fight Infection, disease…
-Or-
Other unwanted Biological Invasion,while having adequate tolerance to avoid Allergy, and Autoimmune Diseases.
https://en.wikipedia.org/wiki/Immunity_%28medical%29

Antibiotic Goals:
Control / “Eliminate” Infecting OrganismBoth antibiotic types are effective:
• BACTERICIDEL Antibiotic • BACTERIOSTATIC Antibiotic
Bact
eria
l Mas
s
Bact
eria
l Mas
sTime Time
ImmuneResponse
ImmuneResponse
Antibiotic Antibiotic

Bacteria: Race for Life
Bacteria Vs. Immune System

Repair Cell Aging Damage:
• Replace Enzymes Consumed• Repair DNA Damage• Repair Cell Wall Damage• Repair (Replace) Organelle Damage
Metabolic Organism Maintenance: Bacteria “Age” and prepare to replicateRepair Cell Damage: DNA, Cell Wall, Internal Organelles etc.Replace used Enzymes: Structural, Metabolic proteins etc.

Replication (Optimum environment):“Healthy” Bacteria Cell Divide every 20 minutes:
Must produce Enough Cell wall, Structural and Metabolic proteins for
TWO cells Structural (Cell Wall); Metabolic Proteins, Lipids and Enzymes Enzymes: Energy…. Proteins Lipids… Carbohydrates Enough DNA for TWO Cells

Bacterial Anatomy And
Physiology
Structural components: Organelles Cell WallCarbohydrates, Lipids, Proteins, Lipoproteins
Metabolic Proteins “Life”:Enzymes: Protein, Lipid, Carbohydrate synthesis
Energy Production

Bacteria Anatomy
Potential Antibiotic targets
Cell wallExoskeleton
DNACell replicationCell function
PlasmidMetabolic DNA
1940 - 2009

Antibiotic targetsBacteria
Ribosome: Structural proteins, Metabolic proteins• Cell Repair• Daughter cells
PlasmidAnti-metabolites:
Sulfonamides
1940 - 2014
DNA: QUINOLONE METRONIDAZOLE RIFAMPIN
Ribosome 50s: CLINDAMYCIN TETRACYCLINES MACROLIDES BIAXIN /ZITHROMAX
LINEOZOLID (23s)
AMINOGLYCOSIDES30S
Cell Wall: BETA LACTAMASES GLYCOPEPTIDES
Membrane Detergents Daptomycin

Plasmids (1940 - 2015) Are (typically) Circular Double - Stranded
DNA molecules. Separate from the Chromosomal DNA. Size varies from 1 to over 400 kilo-base (kbp).
EACH BACTERIA CELL: • Anywhere from one copy, (For large plasmids)
to hundreds of copies of the same plasmid
• A variety of resistance factors are found: β-lactamase Extended Spectrum β lactamase (ESBL) All Ribosomal active agents
Antibiotic Resistance
Mechanisms : Acquisition of Resistance“Mobile Genetic Elements”
1940 Westergard Mercury
2015 Ferrari 458

In 1918….H1N1 Influenza circled to globe 3 times in 18 months
using 1918 Transportation Systems…..

Let the GAMES begin….

1880
Before the Germ Theory…. “EVIL TUMORS and VAPORS”
Puerperal fever, also known as “Child-bed fever“:• Physicians did not scrub before surgery or wash their hands
between patients • Doctors and Medical students routinely moved from Dissecting
Corpses to examining New Mothers without first Washing their hands…
Puerperal Fever: • Common in hospitals and often fatal, with mortality at 10%–35%. • Autopsies showed a confusing multitude of physical signs, which
emphasized the belief that puerperal fever was not one, but many different, yet unidentified, diseases.
• Conventional wisdom that diseases spread in the form of “Bad Air", also known as miasmas or vaguely as "un-favorable atmospheric-cosmic-terrestrial influences"
• “And, with due respect for the cleanliness of the Viennese Students, it seems improbable that enough infective matter or vapor could be secluded around the fingernails to kill a patient."
Vienna General Hospital

1880
Before the Germ Theory….Puerperal fever, also known as "childbed fever"
In 1840’s (1847) while the Director of the maternity clinic at the Vienna General Hospital in Ignaz Philliop Semmelweis (a Hungarian physician) demonstrated that hand-washing with a chlorinated lime solutions could drastically reduce the number of women dying after childbirth. (35% Mortality to <1%)
However his observations conflicted with the established Scientific and Medical opinions of the time: • His ideas were rejected by the medical community.• Some doctors were offended at the suggestion that they should wash
their hands • Semmelweis could offer no acceptable scientific explanation for his
findingsWe all now know how important it is to wash our hands:• In hospitals, bacteria are wiped out by the simple act of hand-washing.• Wards are supplied with Antiseptic Hand Gel, medical staff and visitors use before they
see patients • Routine of ‘scrubbing up’ by surgeons before an operation is, a well-established practice.
Beginning in 1861, Semmelweis suffered from various nervous complaints, severe depression, and became absentminded.. On July 30, 1865 he was lured to a Viennese insane asylum. He tried to leave, was severely beaten by several guards; secured in a straitjacket, and confined to a darkened cell. (Mental institution therapy included dousing cold water, castor oil, and enemas). He died after two weeks, (August 13, 1865, aged 47), from a gangrenous wound- possibly caused by the beating. The autopsy gave the cause of death as “pyemia”—blood poisoning
Ignaz Phillip Semmelweis 1818-65

Semmelweis, Ignaz
Bibilography
• Semmelweis, Ignaz; Carter, K. Codell (translator, extensive foreword) (September 15, 1983) [1861], Etiology, Concept and Prophylaxis of Childbed Fever, University of Wisconsin Press, ISBN 0-299-09364-6 (references to Carter's foreword and notes indicated "*")
• Carter, K. Codell; Carter, Barbara R. (February 1, 2005), Childbed fever. A scientific biography of Ignaz Semmelweis, Transaction Publishers, ISBN 978-1-4128-0467-7
• Ignaz Semmelweis From Wikipedia, the free encyclopedia https://en.wikipedia.org/wiki/Ignaz_Semmelweis#cite_note-Carter1-13
• Dr. Semmelweis’ Biography Semmelweis Society International http://semmelweis.org/about/dr-semmelweis-biography
• M Best, D Neuhauser, Heroes and martyrs of quality and safety Ignaz Semmelweis and the birth of infection control Qual Saf Health Care 2004;13:233-234 doi:10.1136/qshc.2004.010918
• Howard Markel. In 1850, Ignaz Semmelweis saved lives with three words: wash your hands PBS News hour. http://www.pbs.org/newshour/author/hmarkel/
• John H. Lienhard No. 622: IGNAZ PHILIPP SEMMELWEIS.Engines of our ingenuity http://www.uh.edu/engines/epi622.htm

1935: THE AGE OF ANTIBIOTICS
BEGINS:

Age of Sulfonamides
Time Line IYear Historical Factoid
1909 Paul Gelmo, a chemistry student working at the University of Vienna in his 1909 thesis, first synthesized. although he had not realized its medical potential [Prontosil® (Sulfonamidochrysoidine)]
1931 Josef Klarer and Fritz Mietzsch: synthesized Prontosil® (Part of a research program designed to find dyes that might act as systemic antibacterial drugs). Theory : Coal-tar dyes which are able to bind preferentially to bacteria and parasites might be used to attack harmful organisms in the body.
1932 *IG Farben filed a German patent application concerning Prontosil® medical utility
1932 Prontosil® was found effective against some important bacterial infections in mice by Gerhard Domagk
1932-1934
Prontosil Solubile®, clinically investigated between 1932 and 1934, at Wuppertal-Elberfeld Hospital and Düsseldorf university hospital (Philipp Klee)
1935Feb
The study results published in a series of articles (February 15, 1935) Deutsche Medizinische Wochenschrift, [5] • Initially received with some skepticism by a medical community bent on vaccination and crude
immunotherapy.
Prontosil®

Age of Sulfonamides
Time Line IIYear Historical Factoid
1935 Leonard Colebrook showed Prontosil was effective against Haemolytic Streptococcus in childbirth : cure for puerperal fever.
Impressive clinical successes with Prontosil started to be reported from all over Europe, and especially after the widely published treatment of Franklin Delano Roosevelt, Jr…..Acceptance was quick and dozens of medicinal chemistry teams set out to improve Prontosil.
1937 Elixir Sulfanilamide (diethylene glycol) caused mass poisoning (United States) Deaths >100 people. The public outcry caused by this incident (and other similar disasters) led to the passing of the 1938 Federal Food, Drug, and Cosmetic
*IG Farben (Interessen-Gemeinschaft Farbenindustrie AG) German chemical industry conglomerate, notorious for its role in the Holocaust. Formed in 1925; During its heyday, largest chemical company in the world and the fourth largest overall industrial concern, after General Motors, U.S. Steel, and Standard Oil of New Jersey.
Following the Nazi takeover of Germany, IG Farben became involved in war crimes during World War II. The firm's pro-Nazi leadership openly collaborated the Nazi government to produce the large quantities of Zyklon B. Post war, the firm ceased operating (1945), assets were liquidated 1952; 13 executives were imprisoned for terms ranging from 1 to 8 years at the Nuremberg Trials.

Age Of Sulfonamides
Bibliography
1. The 1937 Elixir Sulfanilamide Incident“ Medicine: Post-Mortem". Time (magazine). December 20, 1937.2. Defunct Companies Of Germany: IG Farben. Snip view.http://www.snipview.com/q/IG_Farben3. Dunn PM. Perinatal lessons from the past Dr Leonard Colebrook, FRS (1883–1967) and the chemotherapeutic conquest of puerperal infection.
Arch Dis Child Fetal Neonatal Ed 2008;93:F246-F248 doi:10.1136/adc.2006.1044484. Medicine: Prontosil, TIME Magazine, December 28, 1936 (Franklin Delano Roosevelt, Jr)5. G. Domagk, "Ein Beitrag zur Chemotherapie der bakteriellen Infektionen", Deutsch. Med. Wschr., 61, 15 February 1935, p. 2506. The makings of a miracle Drug. Smells like science. http://smellslikescience.com/the-making-of-a-miracle-drug/

Katherine Woglon10-year-old daughter of a Brooklyn physician; the target was the bacterium that caused her meningitis. (H. influenza)
After an apparent cure, Katherine suffered a relapse a few months later and died.
The First recorded use of a Sulfa antibiotic drug in the United States took place at Babies Hospital, Brooklyn New York, July 1935.….. Dr. Alexander Ashley Weech MD
- Eric Oatman The drug that changed the changed the world. P&S The College of Physicians and Surgeons of Columbia University, http://www.cumc.columbia.edu/psjournal/archive/winter-2005/drug.html (Accessed 3/15/2014)- Schwentker FF, Gelman S, Perrin HL . The Treatment of Miningococcic Meinigitis with Sulfanillamide: Preliminary JAMA. 1937;108(17):1407-1408

AntibioticsClinical Beginning (1-6)
The first test case treatment of Infections with Penicillin 1940
Albert Alexander (1873-1941)
1 Markel H. The Real Story Behind Penicillin. The rundown : PBS News hour. http://www.pbs.org/newshour/rundown/the-real-story-behind-the-worlds-first-antibiotic/ 2 David Greenwood. Antimicrobial Drugs Chronicle of the twentieth Century Medical Triumph. Oxford University press 2008 pg 1013 Albert Alexander. From Wikipedia, the free encyclopedia http://en.wikipedia.org/wiki/Albert_Alexander4 "Making Penicillin Possible: Norman Heatley Remembers". Science Watch. Thomson Scientific. 20075 Abraham, E.P., Gardner, A.D., Chain E et al. Further Observations of Penicillin. Lancet 1941, August 16; pp 6155-666 The Almost -Cure All Urine of Albert Alexander. http://bmackie.blogspot.com/2012/08/the-almost-cure-all-urine-of-albert.html (Accessed 3/15/2014)
• September 1940, an Oxford county England police constable, Albert Alexander, 48, working in his rose garden, “nicked” the corner of his mouth on a rose thorn. • By the end of the month, the scratch was badly infected, with both Staphylococcus
and Streptococcus. • The infection, un-responsive to Sulfonamides antibiotics, spread to his eyes, scalp,
lungs, and shoulder.• Alexander admitted to the Radcliffe Infirmary. The infection worsened despite efforts
with various treatments including Sulfa antibiotics. • Alexander's head and scalp became covered with infection, he was persistently
bacteremic, his face was matted with weeping red abscesses, and • Progressing, one of his eyes had to be removed.

• Howard Florey and Boris Chain heard about the horrible case and asked the Radcliffe physicians if they could try their “purified” penicillin.
• On February 12, 1941 Mr. Alexander began receiving Penicillin: the Initial dose was 200 Units (160mg), then 100 mg every 3 hours.
• After five days of injections, Alexander began to recover. But Chain and Florey did not have enough penicillin to eradicate the infection; the Penicillin ran out on February 17, 1941 (Despite recycling Penicillin from the Alexander’s urine (6)).
• Mr. Alexander ultimately died of an overwhelming Staphylococcal sepsis on
March 15, 1941.
1 Markel H. The Real Story Behind Penicillin. The rundown : PBS News hour http://www.pbs.org/newshour/rundown/the-real-story-behind-the-worlds-first-antibiotic/ 2 David Greenwood. Antimicrobial Drugs Chronicle of the twentieth Century Medical Triumph. Oxford University press 2008 pg 1013 Albert Alexander From Wikipedia, the free encyclopedia http://en.wikipedia.org/wiki/Albert_Alexander4 "Making Penicillin Possible: Norman Heatley Remembers". Science Watch. Thomson Scientific. 20075 Abraham, E.P., Gardner, A.D., Chain E et al. Further Observations of Penicillin. Lancet 1941, August 16; pp 6155-666 The Almost -Cure All Urine of Albert Alexander http://bmackie.blogspot.com/2012/08/the-almost-cure-all-urine-of-albert.html (accessed 3/15/2014)
AntibioticsClinical Beginning (1-6)
The first test case treatment of infections with Penicillin Albert Alexander (1873-1941)

Antibiotics
History: Penicillin in America 1,2,3,4
Anne Sheafe Miller (1909 -1999)
In March 194233-year-old Anne Sheafe Miller • Wife of the Yale Athletic Director, Ogden D. Miller• 1931 Graduate of Columbia Presbyterian School of Nursing, (Now part of Columbia
University).
Hospitalized for almost one month, lay dying of β-Hemolytic Streptococcus “Puerperal sepsis”, (S pyogenes) following a miscarriage, in a New Haven, Connecticut hospital.
Despite the best efforts of contemporary medical science:Sulfa antibiotics, Blood Transfusions, and several Surgeries, She remained Delirious, Febrile (103-1060 F) and Bacteremic. Her physician John Bumstead, M.D. could not eradicate her bloodstream infection………
1 Curtis J. Fulton, Penicillin and chance. Yale Medicine. http://yalemedicine.yale.edu/autumn1999/features/capsule/55396 (Accessed 3/15/2014)2 David Greenwood. Antimicrobial Drugs Chronicle of the twentieth Century Medical Triumph. Oxford University press 2008 pg 1014)3 Tager M. John F. Fulton, coccidioidomycosis, and penicillin. Yale J Biol Med. 1976 Sep;49(4):391-8.4 Grossmen CM. The First Use of Penicillin in the United States Ann Intern Med. 2008;149:135-136.

Penicillin: The Miracle Drug Clinical Research at Yale, Yale School of Medicine http://www.yalestudies.org/clinicalTrials/page.asp?p=penicillin
Serendipitously: Mrs. Miller’s physician, Dr. Bumstead was treating a colleague Dr. John Fulton, who was hospitalized at the same time - with Pulmonary Coccidioidomycosis .
Dr. Bumstead approached his patient (Dr. Fulton) with a plea: He was ware of Fulton’s friendship with Dr. Howard Florey, (Clinically developing Penicillin) and asked Fulton if he could talk to Florey, and obtain for a sample of Penicillin for treatment of the infection. Several phone calls later (Merck & Co) the antibiotic was procured. (3)
Dr. Norman Heatley, (Biochemist developing Penicillin) a colleague of Dr. Florey from Oxford University UK, brought the vial of Penicillin (5.5 grams) to New Haven (From Merck & Co in Rahway, New Jersey.)
Intern, Herbert Tabor, M.D., was responsible for injecting the drug, and recycling Miller’s urine (Sent Merck & Co), where up to 70% of the scarce and costly drug could be recovered and reused.

History: Penicillin in AmericaAnne Sheafe Miller
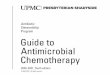
Miller began receiving her first dose via intravenous drip at 3:30 p.m. on a Saturday. (10-40,000 Units/Day) A The next morning her temperature, which had hovered between 103 and 106.5 degrees, dropped to normal for the first time in four weeks. B Her Blood bacteria count dropped (Quantative) By Monday her appetite had returned and she had eaten four full meals.
A
B
Anne Sheafe Miller (1909-1999)
with Alexander Fleming,
- Curtis J. Fulton, Penicillin and Chance. Yale Medicine. http://yalemedicine.yale.edu/autumn1999/features/capsule/55396 (Accessed 3/15/2014)- Grossmen CM. The First Use of Penicillin in the United States Ann Intern Med. 2008;149:135-136.
.
Hemolytic Streptococcal Septicemia
Rectal Temperature
O F
Blood CultureColonies/ml
Penicillin
Units/Day x 1000
Sulfadiazine Grams/Day
Hospital Week
10810
610
4102
10098
4030
2010
Firs
tO
pera
tion
Seco
ndO
pera
tion
1 2 3 4 5 6 7 8
63

In 1950 Eli Lilly Instituted a Program Aimed at Discovering New Antibiotics
In 1952 a Missionary in Borneo sent a sample of Dirt to his friend Dr. EC Kornfield (An organic chemist) A Fungal organism was isolated from that sample (Streptomyces orientalis) Which produced a substance: “Compound 05865”
The compound was dubbed “Mississippi Mud” Because of its Brown Color
Resulting Drug was called “Vancomycin” (From the word Vanquish)
Levine DP, Vancomycin: A History. CID 2006:42 (Suppl 1), S5-S12

VANCOMYCIN November 21, 1961, Michael C. Rockefeller, 23-year old
Edmund Carl Kornfeld 1919 –2012

Beta-lactams
Monobactam(Azetreonam)
penicillinCephalosporins
Carbapenems
β-lactam

“Pus”:• A protein-rich fluid called “Liquor puris” usually
Whitish-Yellow, Yellow, or Yellow Brown in color. • Pus consists of a buildup of Dead leukocytes
(White Blood Cells) from the body's immune system in response to infection.
• It accumulates at the site of inflammation.
http://www.medicalnewstoday.com/articles/249182.php

MRSA
One “Loop-full” (“Drop”) of Suspended S. aureus colony contains 250,000 organisms…
Loop = 1 drop 20 drops in 1 cc (cm³). 1cc ~ 5.0 million Bacteria

MRSAGenome
• 1 : 250,000 contain the
• mecA 2a Genetic Mutation
• The Bacterial Cell and Daughter Bacteria Cells • will be Resistant to…….
• ALL BETA LACTAM Antibiotics *
*Remains Sensitive to Vancomycin:ANY De-novo MUTATIONAL attempt for S. aureus to become resistant to Vancomycin is a Lethal event to the Bacteria….(VANCOMYCIN : “Ace in the Hole”).

PLASMA MEMBRAMEPBP
I
II2a
III
CELL WALLPeptidoglyca
n
Peri-plasma space
IV
V
VI
Bacterial Cell wallChromosome
Methicillin Resistant“MRSA”
mecA
β-lactamases

MRSA
1964 Likely “Original” MRSA infections developed in Immunocompromized; Hospitalized patients with Methicillin Sensitive (MSSA) infections.
Antibiotics eliminated the Penicillin “Sensitive Bacteria”….
….In their “Weaken” Immune state the patients could not clear the residual Methicillin Resistant (“MRSA”) Bacteria leading to “Super” Infections…
1970’s the MRSA organisms “escaped” the hospital and began infecting and colonization the General Population……

S. Aureus
Epidemiology: Human Carriers
30 - 40% Healthy Human Carriers (Any given time)
1% Humans are MRSA Carriers
S aureus: “Uniquely” a Human Bacteria
Transmission: Close personal contact Infected secretions (“Pus”) / Objects Skin Contact (Athletic competition, Draining lesions) Shared Personal items (Towels, Razors, Medical Equipment
etc.)
300 Million Americans:100 Million MSSA carriers
1 million MRSA Carrier

2002It must be a “Spider bite”….…..What else could it be?

U.S. Geographic Distribution of Verified Widespread Populations of Six Native
Loxosceles Species.
Loxosceles spiders purportedly are transported beyond the areas where they are endemic in household goods and warehouse cargo…but uncorroborated… actual epidemiology essentially does not occur beyond the spiders' usual habitat.

Where Did all this Community AcquiredCA-MRSA Come from?
Community MRSA
(USA 300)2000
MRSA Hospital “Community Staph” 1960-1970s MSSA
“Staff-ala-roar-e-us”“Staff-full-of-oreos”
Increased Virulence Panton-Valentine leukocidin genes Expression of core genome-encoded
toxins

Creatures Walk Among Us

Creatures Walk Among Us
Multidrug-Resistant “MDR” : Pneumococci, Gonococci, and Salmonella spp
Extremely Drug-Resistant Tuberculosis (MDRTD, XDRTB)
Vancomycin-Resistant Enterococci “VRE” (and Vancomycin-Resistant S. aureus “VRSA”
Extended-Spectrum Beta-Lactamase “ESBL”- Enterobacteriaceae, Pseudomonas aeruginosa
Carbapenemase-Producing Klebsiella pneumonia
Pan-Resistant: Acinetobacter baumanii

Gram Positive BacteriaSkin Mucus Membrane
Gram Negative BacteriaEnvironmental
AndContagious bacteria
(Pulmonary, STD’s etc)
Gram Negative BacteriaEnterobacteriaceae(Human GI Flora)

Hans Christian GramWikipedia, the free encyclopedia
Hans Christian Joachim Gram Danish bacteriologist Gram studied Botany at the University of Copenhagen and
assisted Japetus Steenstrup. His interest in plants introduced him to the basis of pharmacology and the use of the microscope.
• He entered medical school in 1878 and graduated in 1883. He traveled throughout Europe between 1878 and 1885. In Berlin in 1884, he developed a method for distinguishing between two major classes of bacteria. This technique, the Gram Stain, continues to be a standard procedure in medical microbiology.
• In 1891, Gram became a lecturer in pharmacology, and later that year was appointed professor at the University of Copenhagen. In 1900 he resigned his Chair in Pharmacology to become Professor of Medicine
The Gram Stain• The work that gained him international reputation was his
development of a method of staining bacteria. The stain later played a major role in classifying bacteria
• Gram was a modest man, and in his initial publication he remarked
"I have therefore published the method, although I am aware that as yet it is very defective and imperfect; but it is hoped that also in the hands of other investigators it will turn out to be useful".
Hans Christian Joachim GramSeptember 13, 1853 - November 14, 1938

Edwin Kleb*
German physician and Bacteriologist noted for his work on the Bacterial Theory of infection:
• Assistant to Rudolf Virchow (Pathological Institute, Berlin 1861–66). • Rush Medical College (1896). • Preceded Robert Koch in studying the bacteriology of traumatic
infections,• 1876: Succeeded in producing endocarditis by mechanical means
combined with general infection• Tuberculosis : Was able to produce bovine infection by means of milk. • 1878: Successfully transmitted syphilis to monkeys
Studied: • Malaria, Hemorrhagic pancreatitis, and Gigantism.
Published:Monographs and Articles; Handbook of pathological anatomy (1869–76)
Teatise on general pathology (1887–89).
(Died from Tuberculosis)
* Encyclopedia Britannica http://www.britannica.com/EBchecked/topic/319924/Edwin-Klebs
(2/6/1834 – 10/23/1913)

Antibiotic Resistance
Human/Bacterial Ecology
Important Human pathogens Gram Positive (Skin, Mucus Membranes)
S. aureus (MSSA,MRSA,VRSA,CA-MRSA)
S. epidermidis
STREPTOC0CCI S. pyogenes (β Streptococci)
S. agalactiae (β Streptococci)
Pneumococcus Enterococcus (GDE,VRE) Viridian streptococcus Group
Anerobic Bacteria:Cocci, Rods, Spiral
Gram Negative (Enterobacteriaceae GI Tract)
Five tribes:
I. E. coliII. Salmonella, ShigellaIII. Proteus, MorganellaIV. Klebsiella, Serratia, Enterobacter sp. (KES)V. Yersinia
H. influenza
Anaerobic Gram Negative:Bacteroides sp.
Gram Negative
(Environmental)
P. aeruginosaAeromonas sp.
Acinetobacter sp.

Question 121
A 52-year-old woman called her physician and reported Urinary Frequency and Urgency, Mild fever, Nausea accompanied by Supra pubic pain.
UA Results
Protein Positive
Glucose Negative
Ketones Negative
Leukocyte Esterase Positive
Nitrates Positive
WBC Too Numerous To Count

QuestionShe completed a three-day course of ciprofloxacin, but her symptoms did not improve. Bacterial Urine Culture were positive for K. pneumonia.
Which of the following details of the patient's history may have put her at risk for this infection?
(A) She received levofloxacin for urinary tract infections at two separate times during the past year.
(B) She received breast implants in Brazil three months ago.(C) She accompanied her husband to India, where he underwent knee surgery six months ago.(D) She is of Korean origin, and she traveled to Korea to visit family and friends six months ago.
Antibiotic Susceptible
Resistant
Imipenem - X
Meropenem - X
Piperacillin/Tazobactam
- X
Cefotaxime - X
Ceftazidime - X
Cefpirome - X
Aztreonam - X
Ciprofloxin - X
Gentamicin - X
Tobramycin - X
Amikacin - X
Minocycline - X
Tigecycline X -
Colistin X -
K. pneumonia
New Delhi metallo-lactamase-1

Question 121
• The carbapenem resistance, broad cross-class resistance, and susceptibility only to Tigecycline and Colistin of this member of the Enterobacteriaceae are characteristic of the New Delhi metallo-beta-lactamase 1 (NDM-1).
• Among the confirmed cases of NDM-1, the majority of those who have sought care have traveled to India or Pakistan and been hospitalized within those countries.
• The encapsulated Klebsiella bacteria known to cause serious deep and metastatic infection in persons of East Asian (including Korean) descent have generally not been highly resistant organisms.
• There have been outbreaks due to Mycobacterium fortuitum and other rapid-growth mycobacteria in association with breast implants in Brazil as well as in the United States and other countries.
• Brazil, moreover, has a high prevalence of resistant gram-negative organisms; therefore, exposure to Brazilian healthcare is a potential but as yet unreported risk for cases of resistant infection in the United States.
• There are also documented cases of patients who have undergone plastic surgery in India and returned with NDM-1 infection.
For further information, see the following:1. Kumarasamy KK, Toleman MA, Walsh TR, Bagaria J, et al . Emergence of a new antibiotic resistance mechanism in India, Pakistan, and the UK: a molecular, biological, and epidemiological study. Lancet Infect Dis Sep 2010;10(9):597-602. 2. Rossi F. The challenges of antimicrobial resistance in Brazil. Clin Infect Dis May 2011;52(9):1138-1143

New Delhi metallo-lactamase-1
“Gram-negative Enterobacteriaceae with resistance to carbapenem conferred by New Delhi metallo-β-lactamase 1 (NDM-1) are potentially a
major global health problem.
Highly resistant to many antibiotic classes, potentially herald the end of treatment with β-lactams, fluoroquinolones, and aminoglycosides—the main antibiotic classes for the treatment of Gram-negative infections” *
* Kumarasamy, KK, Toleman MA, Walsh TR et al. Emergence of a new antibiotic resistance mechanism in India, Pakistan, and the UK: a molecular, biological, and epidemiological study Lancet Infect Dis. 2010 September; 10(9): 597–602.

New Delhi metallo-lactamase-1
Emergence/Recognition
Year Factoid19961 metallo-β- lactamase-producing Klebsiella pneumoniae Singapore
2008 NDM-1 detected in a K. pneumoniae isolate from a Swedish patient of Indian origin in 2008.
2008 NDM-1 Detected in bacteria in India, Pakistan, the United Kingdom 2008
2010 - United States (September ) - Canada (August) - Japan (September) - Brazil (October)
2010December
Australia, Belgium, Canada, Germany, Hong Kong, Japan, Kenya, the Netherlands, Norway, Oman, Singapore, Sweden, Taiwan, and the USA, Denmark.*
1 Koh TH, Babini GS, Woodford N, Sng LH, Hall LM, Livermore DM. Carbapenem hydrolysing IMP-1 beta-lactamase in Klebsiella pneumoniae from Singapore. Lancet 1999; 353: 2162. 2 Hammerum AM, Toleman MA, Hansen F, etal. Global spread of New Delhi metallo-β-lactamase 1 .The Lancet Infectious Diseases, Volume 10, Issue 12, Pages 829 - 830, December 2010
*Most of these patients also had direct links to Asia 2

First death
• August 2010, the first reported death due to bacteria expressing the NDM-1 enzyme was recorded.
• Belgian man, become infected while being treated in a hospital in Pakistan, died despite being administered Colistin.
• Doctor involved in his treatment said: "He was involved in a car accident during a trip to Pakistan.
• He was hospitalized with a major leg injury and then repatriated to Belgium, but he was already infected".
Belgian man dies of South Asian superbug (AFP) – Aug 13, 2010http://www.google.com/hostednews/afp/article/ALeqM5g2UVNIO5tUQAqbWeE7l2PjSW34cg
(AFP) – Aug 13, 2010
New Delhi metallo-lactamase-1
Emergence/Recognition

THE PARADOX

Scientists, (Microbial genetics, Mathematicians, Bio-chemists,
Pharmacologists, Pharmaceutical Chemists, Microbial geneticists:
Will tell you….
It is IMPOSSIBLE for ANY bacterial organism especially Staphylococcus
to develop resistance to
VANCOMYCIN……
Vancomycin Resistant Enterococcus
“VRE”Europe 1980s……..
* Uttley AH, Collins CH, Naidoo J, George RC (1988). "Vancomycin-resistant enterococci". Lancet 1 (8575-6): 57–8**Leclercq R, Derlot E, Duval J, Courvalin P (July 1988). "Plasmid-mediated resistance to Vancomycin and teicoplanin in Enterococcus faecium". N. Engl. J. Med. 319 (3): 157–61.

ALL S. aureus are Sensitive to Vancomycin…
ANY “Intrinsic” organism attempt to develop
Mutational resistance IS a Lethal Mutational event……
S. Aureus:Vancomycin is the
Therapeutic
“Ace in the Hole”
* Noble WC, Virani Z, Cree RG (June 1992). "Co-transfer of vancomycin and other resistance genes from Enterococcus faecalis” NCTC 12201 to Staphylococcus aureus". FEMS Microbiol. Lett. 72 (2): 195–8
“VRE” “Van A”
gene“MRSA”
“VRSA”Vancomycin Resistant
S. aureus1992*
Vancomycin

Can you Imagine a world…. Where there are NO antibiotics
available to treat S. aureus Infections?....
Thank goodness we have Vancomycin!........
VRSAWilliam Beaumont
HospitalRoyal Oak, Michigan
2002*…
* Chang S, Sievert DM, Hageman JC, et al. (April 2003). "Infection with vancomycin-resistant Staphylococcus aureus containing the vanA resistance gene". N. Engl. J. Med. 348 (14): 1342–7.

Vancomycin Resistant S. aureus (“VRSA”)Historical U.S. VRSA 2010 Case count and geographical information
Case
State Year Age
Source Diagnosis Underlying Conditions
1 MI 2002 40 Plantar ulcers &Catheter tip
Plantar soft tissue infection Diabetes, dialysis
2 PA 2002 70 Plantar Ulcer Osteomyelitis Obesity
3 NY 2002 63 Urine from anephrostomy tube
No Infection Multiple Sclerosis,Diabetes, Kidney stones
4 MI 2005 78 Toe Wound Gangrene Diabetes, Vascular disease
5 MI 2005 58 Surgical site woundafter Panniculectomy
Surgical Site Infection Obesity
6 MI 2005 48 Plantar Ulceration Osteomyelitis MVA, Chronic Ulcers
7 MI 2006 43 Triceps Wound Necrotizing Fasciitis Diabetes, Dialysis, Chronic ulcers
8 MI 2007 48 Toe Wound Osteomyelitis Diabetes, Obesity, Chronic ulcers
9 MI 2007 54 Surgical site woundafter foot amputation
Osteomyelitis Diabetes, Hepatic Encephalopathy
10 MI 2009 54 Plantar foot wound Plantar soft tissueinfection
Diabetes, Obesity, Lupus,Rheumatoid Arthritis
11 DE 2010 64 Wound Drainage Prosthetic joint infection Diabetes, Dialysis
* Centers for Disease Control http://www.shea-online.org/Assets/files/newsletter/VRSA_Lab_Update.pdf
Country # isolates
Iran 2005 1 513 case 2014J Clin Microbiol. 2014 Mar; 52(3): 998–1002. doi: 10.1128/JCM.02187-13

WHAT IS NEXT

INSIDE
OUTSIDE

Physician/Patient and Clinical
• Education & Campaigns• Surveillance Systems• Laboratory Testing & Training• References & Resources availability• Antibiotic Stewart programs
Centers for Disease Control http://www.cdc.gov/drugresistance/index.html

Are we running out of antibiotics?
Maybe / Yes
Research continues to Develop New Antibiotic Classes….…. And to Extend the life of Present AntibioticsCombinations of Antibiotics (Beta lactam / Clindamycin)Restricting Antibiotic Policies (Hospital, 3rd Party payers)Culturing Infections for Antibiotic DirectionEmpiric Choices……

2015 A NEW DAWN? Dirt from a Grassy Field in Maine…
PARADOX1% of the Microbes in the Soil (Or Sea water) can be Reliably Grown Under Lab Conditions. Remaining 99% Likely produce “Unknown” / Un-discovered Antibiotics
iChip technology: Eleftheria terraeTeixobactin Inhibits Cell Wall Synthesis by Binding to a Highly Conserved Motif of Lipid II (Precursor of Peptidoglycan) and lipid III (Precursor of Cell Wall Teichoic Acid)If Teixobactin makes it to the market, it could be the First New Class of Antibiotic in Decades*
-Ling LL, Schneider T, Peoples AJ, et al. A New antibiotic kills pathogens without detectable resistance. Nature 517, 455–459 (22 January 2015) doi:10.1038/nature14098-*New class of antibiotic found in dirt could prove resistant to resistance. https://www.washingtonpost.com/news/speaking-of-science/wp/2015/01/07/new-class-of-antibiotic-found-in-dirt-could-prove-resistant-to-resistance/
Gram-Positive Pathogens including S. aureus, E. faecium / faecalis, various streptococci, M. tuberculosis, C. difficile. Teixobactin had equivalent activity to Oxacillin (Methicillin) in vitro, and “Superior activity “ to Vancomycin both in Vitro and Animal model.

Questions?
Recommended