CVD Prevention and Control (2009) 4, 171–175
www.elsevier.com/locate/precon
Anti-hypertensive therapy for acute ischemicstroke survivors
Waleed M. Sweileh a,*, Ansam F. Sawalha b, Sa’ed H. Zyoud b,Samah W. Al-Jabi a
aCollege of Pharmacy, An-Najah National University, Nablus, Occupied Palestinian Territoryb Poison Control and Drug Information Center (PCDIC), An-Najah National University, Nablus,Occupied Palestinian Territory
Received 31 May 2009; revised 21 August 2009; accepted 5 October 2009Available online 31 October 2009
18do
KEYWORDSIschemic stroke;Anti-hypertensives;Hypertension
75-4570/$ - see front mattei:10.1016/j.cvdpc.2009.10.
* Corresponding author. Tel.E-mail address: waleedswe
r � 200001
: +972 5ileh@na
Summary
Background and objective: Anti-hypertensive medications are recommended for pre-vention of recurrent ischemic stroke in hypertensive and normotensive patients.The objective of this study was to analyze the use of anti-hypertensive therapy inacute ischemic stroke survivors.Methods: All ischemic stroke survivors discharged from Al-watani governmentalhospital in Palestine from August 2006 until September 2007 were investigated.Demographic data, clinical characteristics, and different classes of anti-hyperten-sive medications prescribed to stroke survivors were analyzed using SPSS 15.Results: One hundred and twenty four ischemic stroke survivors were identified, ofwhich 80 (64.5%) had a documented history of hypertension (HTN). Two thirds of thesurvivors (n = 82; 66.1%) were prescribed anti-hypertensive medications, mostly asmono-therapy, at discharge. Angiotensin-converting enzyme inhibitors (ACEI) 65(45.6%), followed by diuretics 41 (34.5%) were the most common drug classes pre-scribed. ACEI were used in combination with diuretics in 29 (23.4%) survivors. Amongsurvivors with a documented history of HTN, 70 (85.5%) were prescribed anti-hyper-tensive medications at discharge while 12 (8.5%) of survivors with no history of HTNwere prescribed anti-hypertensive medications at discharge.Conclusion: In this study, the use of anti-hypertensive medications as a mono-ther-apy was common among those with a history of hypertension but not among thosewithout a history of hypertension.� 2009 World Heart Federation. Published by Elsevier Ltd. All rights reserved.
9 World Heart Federation. Published by Elsevier Ltd. All rights reserved.
99225906/972 92940475.jah.edu (W.M. Sweileh).

172 W.M. Sweileh et al.
Introduction
Hypertension is one of the most important modi-fiable risk factors for stroke, and the use ofanti-hypertensive medications is known to reducethis risk substantially [1,2]. In one study, a mod-erate reduction in blood pressure during the firstweek after acute ischemic stroke was associatedwith improved short-term functional outcome[3]. However, a meta-analytic study assessingthe effect of altering blood pressure in peoplewith acute stroke, and the effect of differentvasoactive drugs on blood pressure in acute strokeconcluded that there was insufficient evidence toassociate altering blood pressure with outcomeduring the acute phase of a stroke [4]. Thismeta-analysis included 12 trials involving 1153participants (603 participants were assignedactive therapy and 550 participants receivedplacebo/control). The trials tested angiotensin-converting enzyme inhibitors, angiotensin recep-tor blockers, calcium channel blockers, clonidine,glyceryl trinitrate, thiazide diuretic and mixedanti-hypertensive therapy. One trial tested phen-ylephrine. Functional outcome and death werenot altered by any of the drugs [4]. Nevertheless,the new statement from the American Strokeassociation recommended the use of anti-hyper-tensive therapy for all hypertensive andnormotensive ischemic stroke survivors [5].Furthermore, the Joint National Committee onPrevention, Detection, Evaluation and Treatmentof high blood pressure (JNC-7) suggested the useof angiotensin-converting enzyme inhibitors plusthiazide diuretics for blood pressure reduction inpatients with recurrent stroke [6]. The LIFE study,a randomized, controlled trial showed that losar-tan was more effective than atenolol in reducingcardiovascular morbidity and mortality as well asmortality from all causes in patients with hyper-tension, diabetes, and LVH and that losartan ap-peared to have benefits beyond blood pressurereduction [7]. In the MOSES study group, eprosar-tan was compared with nitrendipine for secondaryprevention after stroke. The result was an earlycomparable normotensive blood pressure. How-ever, the combined primary end point of morbid-ity and mortality was significantly lower in theeprosartan group [8].
In the present study, we evaluated the fre-quency and pattern of anti-hypertensive therapyfor acute ischemic stroke survivors at dischargein relation to recent recommendations and guide-lines.
Methodology
Study population
This hospital-based study was conducted at Al-watani Governmental Hospital in Nablus, Palestine.Data were collected retrospectively from Septem-ber 01, 2006 until August 31, 2007. All patientsadmitted to Al-watani hospital with an ischemicstroke and discharged alive were included in thestudy. The diagnosis of ischemic stroke was basedon the World Health Organization definition ofstroke and the computerized tomography (CT) scanresults [9]. Patients with no definitive CT scan re-sults or those suspected to have transient ischemicattacks were excluded.
Data collection
Data collection was authorized by the hospitaladministration. For each patient, demographicdata, risk factors, and different classes of anti-hypertensive medications prescribed at dischargewere obtained from patients’ medical files. Demo-graphic variables included age and sex. Risk factorsconsisted of a documented diagnosis of hyperten-sion (HTN), ischemic heart disease (IHD), renal dys-function, congestive heart failure (CHF), atrialfibrillation (AF), recurrent stroke, obesity, andage >65 years. Obesity was defined as a body massindex (BMI) > 30 for both males and females. Renaldysfunction was defined as a creatinine clear-ance <60 ml/min. Creatinine clearance (CrCl) wascalculated for all patients using the Cockcroft–Gault formula with values for women obtained bymultiplying the result by 0.85. A history of hyper-tension was based on a documented diagnosis ofthe disease in a patient’s medical file.
We identified the prescribing rates of differentanti-hypertensive drug classes, including angioten-sin-converting enzyme inhibitors (ACE-I), angioten-sin receptor blockers (ARB), b-adrenergic blockingagents (BB), calcium channel blockers (CCB), anddiuretics. We then examined and analyzed theuse of different classes of anti-hypertensive medi-cations among patients with and without a docu-mented diagnosis of hypertension. The number ofprescriptions was documented for each class ofanti-hypertensive drugs.
Statistical analysis
Analysis of data was carried out using the "Statisti-cal Program for Social Sciences" (SPSS) for Windows
Anti-hypertensive therapy for acute ischemic stroke survivors 173
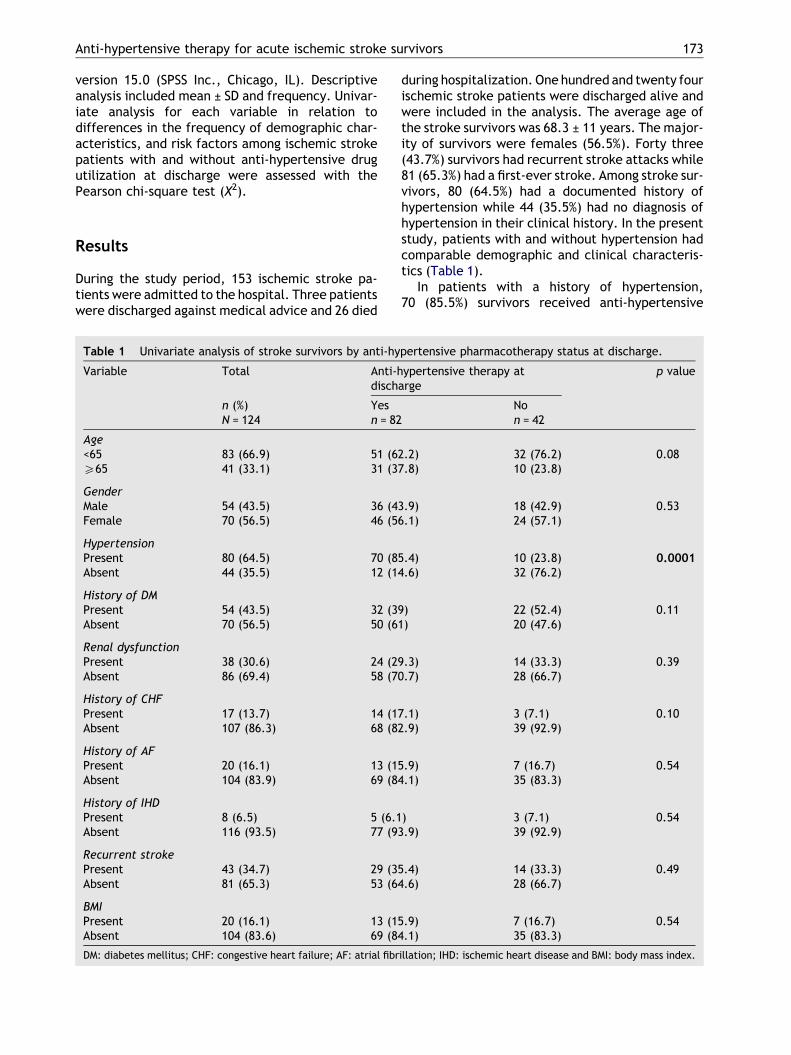
version 15.0 (SPSS Inc., Chicago, IL). Descriptiveanalysis included mean ± SD and frequency. Univar-iate analysis for each variable in relation todifferences in the frequency of demographic char-acteristics, and risk factors among ischemic strokepatients with and without anti-hypertensive drugutilization at discharge were assessed with thePearson chi-square test (X2).
Results
During the study period, 153 ischemic stroke pa-tients were admitted to the hospital. Three patientswere discharged against medical advice and 26 died
Table 1 Univariate analysis of stroke survivors by anti-hy
Variable Total Anti-hdisch
n (%) YesN = 124 n = 82
Age<65 83 (66.9) 51 (6P65 41 (33.1) 31 (3
GenderMale 54 (43.5) 36 (4Female 70 (56.5) 46 (5
HypertensionPresent 80 (64.5) 70 (8Absent 44 (35.5) 12 (1
History of DMPresent 54 (43.5) 32 (3Absent 70 (56.5) 50 (6
Renal dysfunctionPresent 38 (30.6) 24 (2Absent 86 (69.4) 58 (7
History of CHFPresent 17 (13.7) 14 (1Absent 107 (86.3) 68 (8
History of AFPresent 20 (16.1) 13 (1Absent 104 (83.9) 69 (84
History of IHDPresent 8 (6.5) 5 (6.1Absent 116 (93.5) 77 (93
Recurrent strokePresent 43 (34.7) 29 (35Absent 81 (65.3) 53 (64
BMIPresent 20 (16.1) 13 (15Absent 104 (83.6) 69 (84
DM: diabetes mellitus; CHF: congestive heart failure; AF: atrial fibr
during hospitalization. One hundred and twenty fourischemic stroke patients were discharged alive andwere included in the analysis. The average age ofthe stroke survivors was 68.3 ± 11 years. The major-ity of survivors were females (56.5%). Forty three(43.7%) survivors had recurrent stroke attacks while81 (65.3%) had a first-ever stroke. Among stroke sur-vivors, 80 (64.5%) had a documented history ofhypertension while 44 (35.5%) had no diagnosis ofhypertension in their clinical history. In the presentstudy, patients with and without hypertension hadcomparable demographic and clinical characteris-tics (Table 1).
In patients with a history of hypertension,70 (85.5%) survivors received anti-hypertensive
pertensive pharmacotherapy status at discharge.
ypertensive therapy atarge
p value
Non = 42
2.2) 32 (76.2) 0.087.8) 10 (23.8)
3.9) 18 (42.9) 0.536.1) 24 (57.1)
5.4) 10 (23.8) 0.00014.6) 32 (76.2)
9) 22 (52.4) 0.111) 20 (47.6)
9.3) 14 (33.3) 0.390.7) 28 (66.7)
7.1) 3 (7.1) 0.102.9) 39 (92.9)
5.9) 7 (16.7) 0.54.1) 35 (83.3)
) 3 (7.1) 0.54.9) 39 (92.9)
.4) 14 (33.3) 0.49
.6) 28 (66.7)
.9) 7 (16.7) 0.54
.1) 35 (83.3)
illation; IHD: ischemic heart disease and BMI: body mass index.
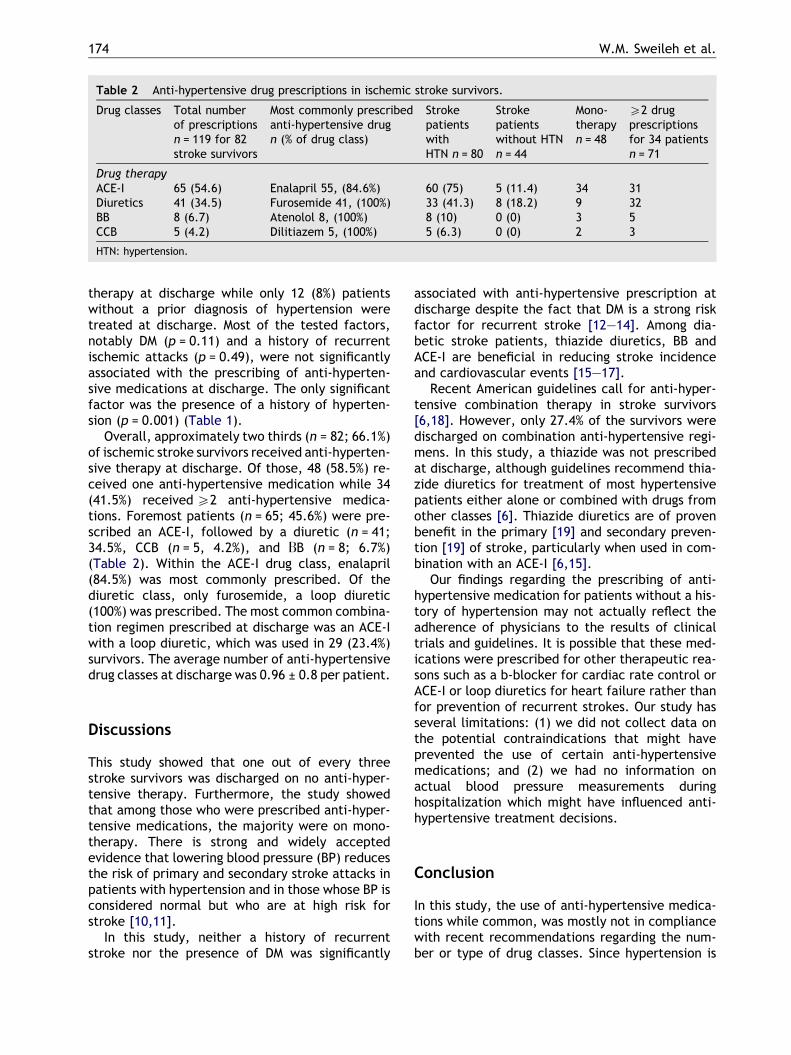
Table 2 Anti-hypertensive drug prescriptions in ischemic stroke survivors.
Drug classes Total numberof prescriptionsn = 119 for 82stroke survivors
Most commonly prescribedanti-hypertensive drugn (% of drug class)
StrokepatientswithHTN n = 80
Strokepatientswithout HTNn = 44
Mono-therapyn = 48
P2 drugprescriptionsfor 34 patientsn = 71
Drug therapyACE-I 65 (54.6) Enalapril 55, (84.6%) 60 (75) 5 (11.4) 34 31Diuretics 41 (34.5) Furosemide 41, (100%) 33 (41.3) 8 (18.2) 9 32BB 8 (6.7) Atenolol 8, (100%) 8 (10) 0 (0) 3 5CCB 5 (4.2) Dilitiazem 5, (100%) 5 (6.3) 0 (0) 2 3
HTN: hypertension.
174 W.M. Sweileh et al.
therapy at discharge while only 12 (8%) patientswithout a prior diagnosis of hypertension weretreated at discharge. Most of the tested factors,notably DM (p = 0.11) and a history of recurrentischemic attacks (p = 0.49), were not significantlyassociated with the prescribing of anti-hyperten-sive medications at discharge. The only significantfactor was the presence of a history of hyperten-sion (p = 0.001) (Table 1).
Overall, approximately two thirds (n = 82; 66.1%)of ischemic stroke survivors received anti-hyperten-sive therapy at discharge. Of those, 48 (58.5%) re-ceived one anti-hypertensive medication while 34(41.5%) received P2 anti-hypertensive medica-tions. Foremost patients (n = 65; 45.6%) were pre-scribed an ACE-I, followed by a diuretic (n = 41;34.5%, CCB (n = 5, 4.2%), and DB (n = 8; 6.7%)(Table 2). Within the ACE-I drug class, enalapril(84.5%) was most commonly prescribed. Of thediuretic class, only furosemide, a loop diuretic(100%) was prescribed. The most common combina-tion regimen prescribed at discharge was an ACE-Iwith a loop diuretic, which was used in 29 (23.4%)survivors. The average number of anti-hypertensivedrug classes at discharge was 0.96 ± 0.8 per patient.
Discussions
This study showed that one out of every threestroke survivors was discharged on no anti-hyper-tensive therapy. Furthermore, the study showedthat among those who were prescribed anti-hyper-tensive medications, the majority were on mono-therapy. There is strong and widely acceptedevidence that lowering blood pressure (BP) reducesthe risk of primary and secondary stroke attacks inpatients with hypertension and in those whose BP isconsidered normal but who are at high risk forstroke [10,11].
In this study, neither a history of recurrentstroke nor the presence of DM was significantly
associated with anti-hypertensive prescription atdischarge despite the fact that DM is a strong riskfactor for recurrent stroke [12–14]. Among dia-betic stroke patients, thiazide diuretics, BB andACE-I are beneficial in reducing stroke incidenceand cardiovascular events [15–17].
Recent American guidelines call for anti-hyper-tensive combination therapy in stroke survivors[6,18]. However, only 27.4% of the survivors weredischarged on combination anti-hypertensive regi-mens. In this study, a thiazide was not prescribedat discharge, although guidelines recommend thia-zide diuretics for treatment of most hypertensivepatients either alone or combined with drugs fromother classes [6]. Thiazide diuretics are of provenbenefit in the primary [19] and secondary preven-tion [19] of stroke, particularly when used in com-bination with an ACE-I [6,15].
Our findings regarding the prescribing of anti-hypertensive medication for patients without a his-tory of hypertension may not actually reflect theadherence of physicians to the results of clinicaltrials and guidelines. It is possible that these med-ications were prescribed for other therapeutic rea-sons such as a b-blocker for cardiac rate control orACE-I or loop diuretics for heart failure rather thanfor prevention of recurrent strokes. Our study hasseveral limitations: (1) we did not collect data onthe potential contraindications that might haveprevented the use of certain anti-hypertensivemedications; and (2) we had no information onactual blood pressure measurements duringhospitalization which might have influenced anti-hypertensive treatment decisions.
Conclusion
In this study, the use of anti-hypertensive medica-tions while common, was mostly not in compliancewith recent recommendations regarding the num-ber or type of drug classes. Since hypertension is

Anti-hypertensive therapy for acute ischemic stroke survivors 175
one of the important risk factors for stroke, bettercontrol of blood pressure is needed to minimize therisk of stroke. Furthermore, screening stroke survi-vors for blood pressure control and initiating appro-priate anti-hypertensive medications should helpreduce the risk of recurrent strokes and increasesurvival. Finally, continuing medication educationand increased awareness among health practitio-ners regarding the latest guidelines, including rec-ommended therapeutic choices for the control ofhigh blood pressure among stroke patients, isrequired.
Conflict of interest
None declared.
References
[1] MacMahon S, Peto R, Cutler J, Collins R, Sorlie P, Neaton J,Abbott R, Godwin J, Dyer A, Stamler J. Blood pressure,stroke, and coronary heart disease, part 1: prolongeddifferences in blood pressure: prospective observationalstudies corrected for the regression dilution bias. Lancet1990;335(8692):765–74.
[2] Collins R, MacMahon S. Blood pressure, antihypertensivedrug treatment and the risks of stroke and of coronaryheart disease. Br Med Bull 1994;50(2):272–98.
[3] Rodriguez-Garcia J, Botia E, de La Sierra A, Villanueva MA,Gonzalez-Spinola J. Significance of elevated blood pressureand its management on the short-term outcome of patientswith acute ischemic stroke. Am J Hypertens 2005;18(3):379–84.
[4] Geeganage C, Bath PM. Interventions for deliberatelyaltering blood pressure in acute stroke. Cochrane DatabaseSyst Rev 2008;4:CD000039 [October 8].
[5] Sacco RL, Adams R, Albers G, Alberts MJ, Benavente O,Furie K, et al. Guidelines for prevention of stroke inpatients with ischemic stroke or transient ischemic attack:a statement for healthcare professionals from the Americanheart association/American stroke association council onstroke: co-sponsored by the council on cardiovascularradiology and intervention: the American academy ofneurology affirms the value of this guideline. Stroke2006;37(2):577–617.
[6] Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA,Izzo Jr JL, et al. Joint national committee on prevention,detection, evaluation, and treatment of high blood pres-sure. National heart, lung, and blood institute. National highblood pressure education program coordinating committee.Seventh report of the joint national committee on preven-
tion, detection, evaluation, and treatment of high bloodpressure. Hypertension 2003;42(6):1206–52.
[7] Dahlof B, Devereux RB, Kjeldsen SE, Julius S, Beevers G, deFaire U, et alLIFE study group. Cardiovascular morbidityand mortality in the losartan intervention for endpointreduction in hypertension study (LIFE): a randomised trialagainst atenolol. Lancet 2002;359(9311):995–1003.
[8] Schrader J, Luders S, Kulschewski A, Hammersen F, Plate K,Berger J, et alMOSES study group. Morbidity and mortalityafter stroke, eprosartan compared with nitrendipine forsecondary prevention: principal results of a prospectiverandomized controlled study (MOSES). Stroke 2005;36(6):1218–26.
[9] WHO task force on stroke and other cerebrovasculardisorders. Recommendations on stroke prevention, diagno-sis, and therapy. Stroke 1989;20(10):1407–31.
[10] Straus SE, Majumdar SR, McAlister FA. New evidence forstroke prevention: scientific review. JAMA 2002;288(11):1388–95.
[11] Chalmers J, Todd A, Chapman N, Beilin L, Davis S, DonnanG, et alInternational society of hypertension writing group.International society of hypertension (ISH): statement onblood pressure lowering and stroke prevention. J Hypertens2003;21(4):651–63.
[12] Petty GW, Brown Jr RD, Whisnant JP, Sicks JD, O’Fallon WM,Wiebers DO. Survival and recurrence after first cerebralinfarction: a population-based study in Rochester, Minne-sota, 1975 through 1989. Neurology 1998;50(1):208–16.
[13] Hillen T, Coshall C, Tilling K, Rudd AG, McGovern R, WolfeCD, for the South London stroke register. Cause of strokerecurrence is multifactorial: patterns, risk factors, andoutcomes of stroke recurrence in the South London strokeregister. Stroke 2003;34(6):1457–63.
[14] Hier DB, Foulkes MA, Swiontoniowski M, Sacco RL, GorelickPB, Mohr JP, Price TR, Wolf PA. Stroke recurrence within 2years after ischemic infarction. Stroke 1991;22(2):155–61.
[15] PROGRESS collaborative group. Randomised trial of aperindopril-based blood-pressure-lowering regimen among6105 individuals with previous stroke or transient ischaemicattack. Lancet 2001;358(9287):1033–41.
[16] Effects of ramipril on cardiovascular and microvascularoutcomes in people with diabetes mellitus: results of theHOPE study and MICRO-HOPE substudy: heart outcomesprevention evaluation study investigators. Lancet2000;355(9200):253–9.
[17] Shindler DM, Kostis JB, Yusuf S, Quinones MA, Pitt B,Stewart D, Pinkett T, Ghali JK, Wilson AC. Diabetesmellitus, a predictor of morbidity and mortality in thestudies of left ventricular dysfunction (SOLVD) trials andregistry. Am J Cardiol 1996;77(11):1017–20.
[18] Law M, Wald NJ, Morris JK, Jordan RE. Value of low-dosecombination treatment with blood pressure lowering drugs:analysis of 354 randomised trials. BMJ 2003;326(7404):1427.
[19] MacMahon S, Rodgers A. Blood pressure, antihypertensivetreatment and stroke risk. J Hypertens 1994;12(Suppl. 10):S5–S14.
Recommended