Tweedie J1, Roberts MJ1, Herron B1, Sheppard M2, McClements B3.
1 Royal Victoria Hospital, Grosvenor Road, Belfast. 2. National Heart and Lung Institute, Imperial College London.
3. Mater Infirmary Hospital, Crumlin Road Belfast
An usual cardiac manifestation of a very common systemic inflammatory condition

Presenting complaintA 69 year old lady presents to the primary
percutaneous intervention service (PPCI) with central crushing chest pain. ECG demonstrates right bundle branch block
Angiographically normal coronary arteries and mild left ventricular impairment.
Represents seven months later with generalised fatigue, chest pain and muscle ache
PMHPolymyalgia RheumaticaHypertensionHyperlipidaemia

Hospital CourseClincial examination unremarkableECG – junctional bradycardia and right bundle
branch blockNT Pro-BNP significantly elevated at 2051Echocardiography – moderate left ventricular
impairmentCardiomyopathy bloods negative
Beta-blocker discontinuedClass III NYHA

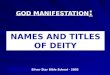
CMRLeft ventricular function moderately
impaired secondary to a non-ischaemic cardiomyopathy

Within the mid ventricular region the contrast enhancement was mid wall and in places transmural

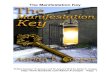
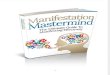
Figure 5 and Figure 6Endomyocardial biopsy, cardiac myocytes replaced with fibrosis (stained green in lower picture).
Figure 5
Figure 6

Conclusion
Diagnosis of left ventricular systolic impairment secondary to PMR was made.
The patient was commenced on high dose oral glucocorticosteroid and remains under review.
A previous case report describes resolution of CMR findings and left ventricular dysfunction six months after commencing oral corticosteroid therapy3, follow-up CMR is awaited.
This case highlights the importance of considering systemic causes of LV dysfunction even when an association is not well recognised.
Recommended