American Journal of Medical Genetics 22:791-809 (1985)
An Autosomal Dominant Syndrome of Short Stature With Mesomelic Shortness of Limbs, Abnormal Carpal and Tarsal Bones, Hypoplastic Middle Phalanges, and Bipartite Calcanei
William R. Osebold, David J. Remondini, Edward L. Lester, Jurgen W. Spranger, and John M. Opitz
Spokane Shriners Hospital for Crippled Children, Spokane, Washington (w. R. O., E. L. L.); Genetics Study Section, Division of Research Grants, National Institutes of Health, Bethesda, Maryland (D. J. R.); Universitats-Kinderklinik, Mainz, West Germany (J. W S.); and Department of Medical Genetics, Shodair Children’s Hospital, Helena, Montana (J. M. 0.)
This paper describes seven persons in a family affected with an autosomal domi- nant syndrome of short stature with mesomelic shortness of upper and lower limbs, abnormal carpal and tarsal bones, hypoplastic or absent middle phalanges of hands and feet, and delayed coalescence of bipartite calcanei. All affected relatives are of normal intelligence, are free of eye problems, and have a normal skull, spine, shoulders, and hips. The digits of the hands and feet are short, broad, and angulated. The hypoplastic or absent middle phalanges effectively result in one interphalangeal joint for each digit, with decreased mobility. The bones of the carpus and tarsus coalesce with increasing age. None of the previously described syndromes or brachydactylies encompasses the findings noted in this kindred.
Key words: autosomal dominant inheritance, shortness of stature, short limbs, brachydactyly, dysostosis condition, failure of phalangeal segmentation, hypoplastic, absent pha- langes, bipartite calcaneus ossification center
INTRODUCTION
Failure of segmentation of the capitate and hamate with short broad digits, cutaneous syndactylies, hypoplastic middle phalanges, and bipartite calcaneal ossifi-
Received for publication December 24, 1984; revision reccived February 19, 1985
Address reprint requests to Dr. William R. Osebold, Shriners Hospital for Crippled Children, N. 820 Summit Boulevard, Spokane, Washington 99201-1598.
0 1985 Alan R. Liss, Inc.
792 Osebold et a1
I
II
1 1 1
I V
1 , 2 3 - 5 6
1
1 . 2 3 4
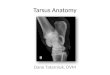
Fig. 1. Pedigree. S indicates syndactyly of toes 2 and 3
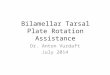
Fig. 2 . 12 yr.
(A) JB at 12 yr. Note rnesornelic shortness of limbs. (B) Feet of JB at 12 yr. (C) Hands of JB at
Mesomelic Shortness, Brachydactyly Syndrome 793
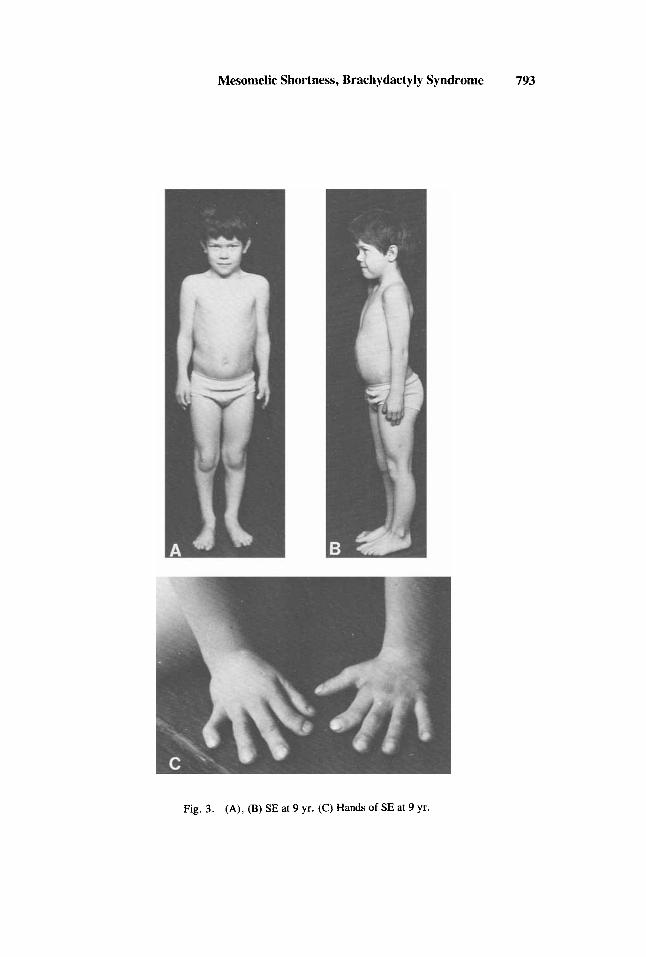
Fig. 3. (A), (B) SE at 9 yr. (C) Hands of SE at 9 yr.
794 Osebold et a1
Mesomelic Shortness, Brachydactyly Syndrome 795
cation center have been described in the oto-palato-digital (OPD) syndrome. How- ever, OPD syndrome patients have a characteristic facial appearance with palatal malformation, mental retardation, and vertebral involvement [Langer, 1967a; Gall et al, 1972; Spranger et al, 1974; Smith, 19761. Here, we describe seven relatives with a syndrome of normal intelligence and a characteristic constellation of skeletal anom- alies including “coalescence” of carpal and tarsal bones, absent or severely abnormal and hypoplastic middle phalanges of digits of hands and feet, delayed coalescence of calcaneal ossification centers, and short tibiae and radii with short stature and auto- soma1 dominant inheritance. None of the previously described brachydactylies encom- passes the findings noted in this kindred.
CLINICAL REPORTS
JE (11-7, Fig. l), the first affected person in this kindred, has 11 normal sibs. His parents were normal, and none of his sibs have had affected children. By his first wife he had five children, the second (LE) and the fourth (EE) being affected. The three unaffected sons have a total of five unaffected offspring. LE and her normal husband have one child, JB (IV-3) who is affected. EE and his normal wife have three children, one of whom is normal. JLE (IV-5) is affected. Recently EE and his wife had a stillborn daughter SB (IV-7), who was affected and whose cause of death is unknown despite an autopsy [Opitz and Gilbert, 19851. By his second wife, JE has had two children, one of whom, SE (111-7) is affected.
At age 65, JE denies pain due to his hand and foot changes. He was engaged in heavy labor in the lumber trade and suffered several disabling back and leg injuries. He feels that over the years he has lost much of the motion at his hand and wrist joints, and that this is progressive and related to “arthritis.” On examination, he has shortness of stature (height: 160 cm), mesomelic shortness of limbs with short, broad digits of hands and feet, and decreased range of motion at the distal joints of upper and lower limbs, with sparing of the proximal limb joints and trunk (Appendix I). The clinical and radiographic changes present in JE closely resemble those of his fourth child, EE and of his grandson, JB. The findings of LE, SE, and JLE are similar.
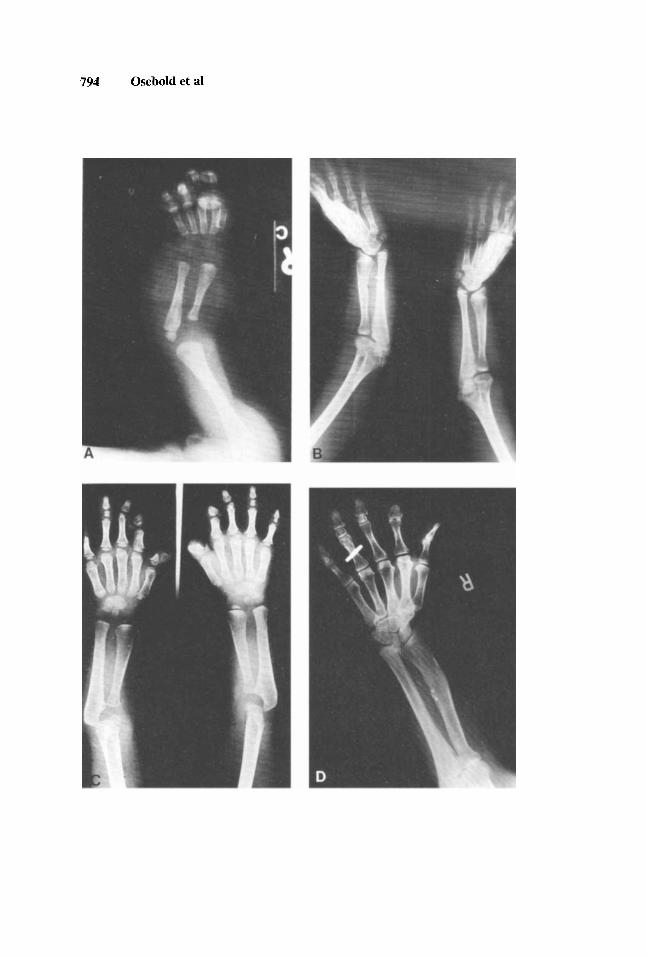
Fig. 4. (A) Radiographs of JLE at 8 wk show shortness of the forearm relative to the humerus. (B) JB at 12 yr. The forearms show short radii and longer ulnae with dyplastic distal epiphyses and radial deviation of the hands. There is a distal radial-ulnar diastasis. ( C ) LE at 5 yr shows symmetric hand changes. The proximal phalanx of the thumb is delta shaped due to lateral fusion of the epiphysis to the metaphysis. The proximal phalanges of the 2nd to 5th fingers and all the metacarpals have proximal and distal growth plates. The middle phalanges are hypoplastic, that of the index finger is an ulnar ossicle leading to radial deviation and that of the middle finger is fused to the shaft of the proximal phalanx. Hamate and capitate are conjoint with a separate h a t e and triquetrum. Radius and ulna are short. The distal end of the radius and the proximal end of the ulna are wide; both bones have a club-like appearance. (D) Radiograph of right arm of JE at 65 yr. The middle phalanx of both index fingers is absent, while that of the long, ring, and little fingers is hypoplastic and block shaped. The distal phalanges of the index fingers are short and broad. Each carpus shows a triangular configuration with the lunate at the apex. On the left is coalescence of the lunate, triquetrum, and hamate. On the right, the abnormally shaped capitate and hamate abut on each other, and the naviculars are oblong. The radii and ulnae are short and abnormally modeled.
796 Osebold et a1
Mesomelic Shortness, Brachydactyly Syndrome 797
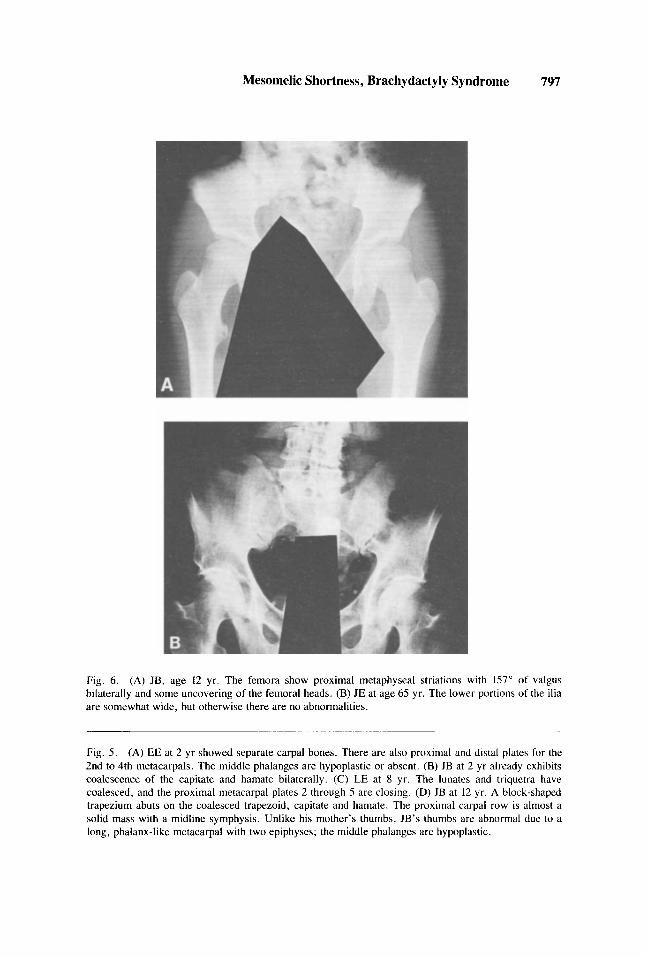
Fig. 6. (A) JB, age 12 yr. The femora show proximal metaphyseal striations with 157" of valgus bilaterally and some uncovering of the femoral heads. (B) JE at age 65 yr. The lower portions of the ilia are somewhat wide, but otherwise there are no abnormalities.
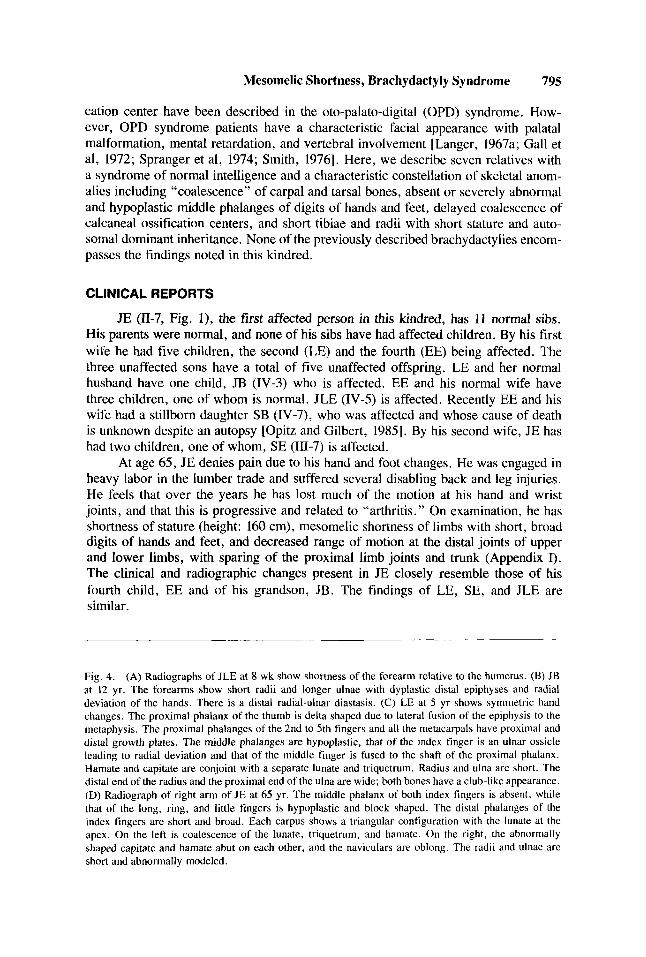
Fig. 5 . (A) EE at 2 yr showed separate carpal bones. There are also proximal and distal plates for the 2nd to 4th metacarpals. The middle phalanges are hypoplastic or absent. (B) JB at 2 yr already exhibits coalescencc of the capitate and hamate bilaterally. (C) LE at 8 yr. The lunates and triquetra have coalesced, and the proximal metacarpal plates 2 through 5 are closing. (D) JB at 12 yr. A block-shaped trapezium abuts on the coalesced trapezoid, capitate and hamate. The proximal carpal row is almost a solid mass with a midline symphysis. Unlike his mother's thumbs, JB's thumbs are abnormal due to a long, phalanx-like metacarpal with two epiphyses; the middle phalanges are hypoplastic.
798 Osebold et a1
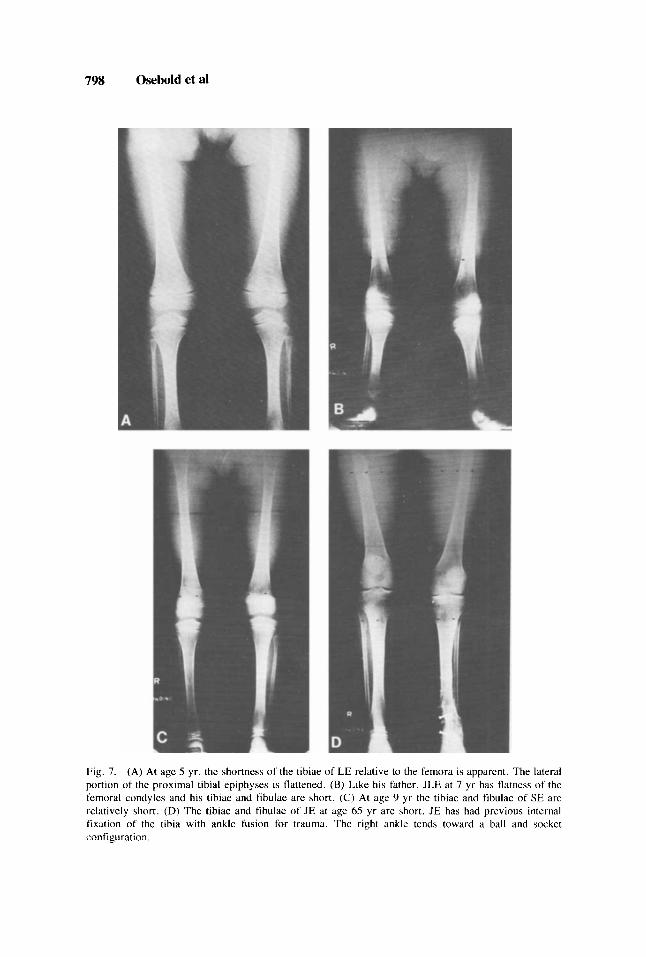
Fig. 7. (A) At age 5 yr, the shortness of the tibiae of LE relative to the femora is apparent. The lateral portion of the proximal tibia1 epiphyses is flattened. (B) Like his father, JLE at 7 yr has flatness of the femoral condyles and his tibiae and fibulae are short. (C) At age 9 yr the tibiae and fibulae of SE are relatively short. (D) The tibiae and fibulae of JE at age 65 yr are short. JE has had previous internal fixation of the tibia with ankle fusion for trauma. The right ankle tends toward a ball and socket configuration.
Mesomelic Shortness, Brachydactyly Syndrome 799
LE, the 38-year-old daughter of JE, finds that her finger abnormalities require use of both hands for most tasks, such as opening car doors and unscrewing jar lids. For many years her knees, right ankle, and low back hurt with activities such as running. She notes numbness and a dysesthesia resembling electrical shocks in the radial aspects of her distal forearms. She has a chronic, partial, uncharacterized hearing loss affecting only the right ear. Slit lamp examination of LE and JB showed no corneal or lens opacities, and their vision is 20/20. LE has bilateral partial syndactyly of toes 2 and 3 and a mild cavus deformity of both feet.
JB, the 12-year-old son of LE (Fig. 2A-C), also has broad, short hands and fingers but does not have radial deviation of the distal thumb phalanx. Instead, he has radial deviation of the distal phalanx of digits 2 and 3 (2.5" both index fingers, 15" at the middle fingers). He complains of a diffuse ache in his right hand (but not in the wrist) when he writes. He had a bilateral club foot deformity treated with a series of casts, followed by nighttime splinting. His feet ache with prolonged weight bearing,
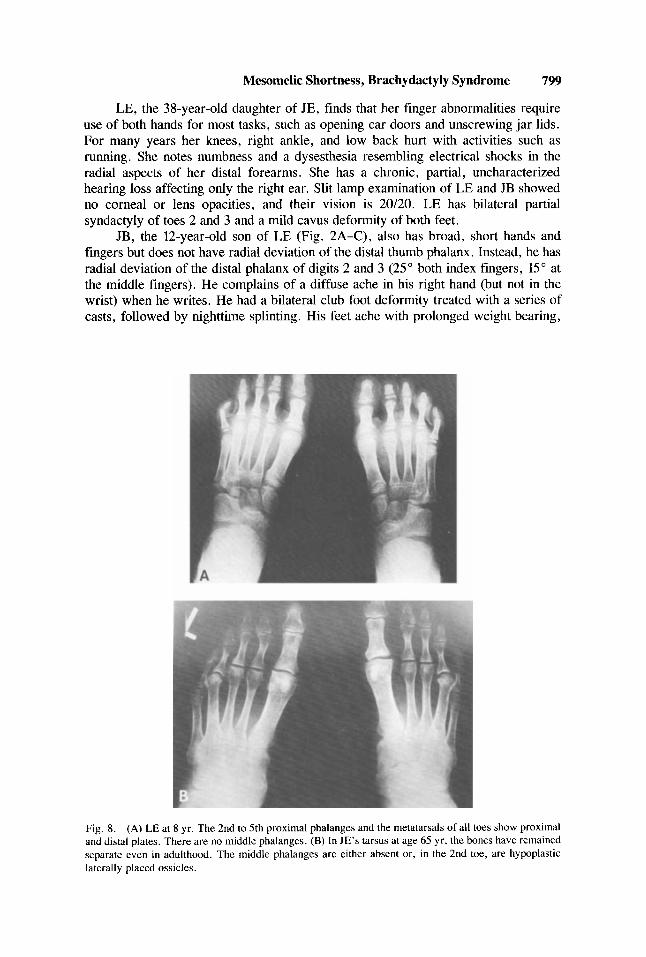
Fig. 8. (A) LE at 8 yr. The 2nd to 5th proximal phalanges and the metatarsals of all toes show proximal and distal plates. There are no middle phalanges. (B) In JE's tarsus at age 65 yr, the bones have remained separate even in adulthood. The middle phalanges are either absent or, in the 2nd toe, are hypoplastic laterally placed ossicles.
800 Osebold et a1
and he has a prominent right hallux varus. Unlike his affected mother, he has no syndactyly .
EE, the 32-year-old son of JE, has bilateral partial cutaneous syndactyly of toes 2 and 3, as does his sister LE. This syndactyly extends to the level of the nails of the right foot, but the nails remain separate. On the left, the syndactyly extends to the PIP joints. Aside from some awkwardness in use due to short, broad digits with essentially one interphalangeal joint apiece, neither EE nor JLE have significant functional impairment.
SE, the 9-year-old son of JE (Fig. 3A-C), required a two-stage surgical correc- tion of his right congenital vertical talus. He requires a plastic splint to support the right foot, otherwise he has no functional limitations, and has no pain. Unlike EE, he has no cutaneous syndactyly of toes.
JLE, the 7-year-old son of EE, notes only that his short, broad digits make some manipulations difficult. Otherwise, he has no complaints.
All affected relatives are normocephalic, of normal intelligence, and with appropriate, normal speech. Except for the chronic partial unilateral hearing loss of LE, there are no ear, nose, or throat symptoms or findings. There are no visual disturbances, and no cardiac, pulmonary, abdominal or genitourinary symptoms or findings. All have broad, short hands, feet, fingers, and toes, with consequent loss of motion and strength distally, with resulting partial functional impairments. The me- somelic segments are less severely affected but are shorter than usual with decreased range of motion. The arms, shoulders, spine and pelvis, and hips and thighs are relatively uninvolved and have full range of motion. Gestation and delivery of the affected relatives were normal.
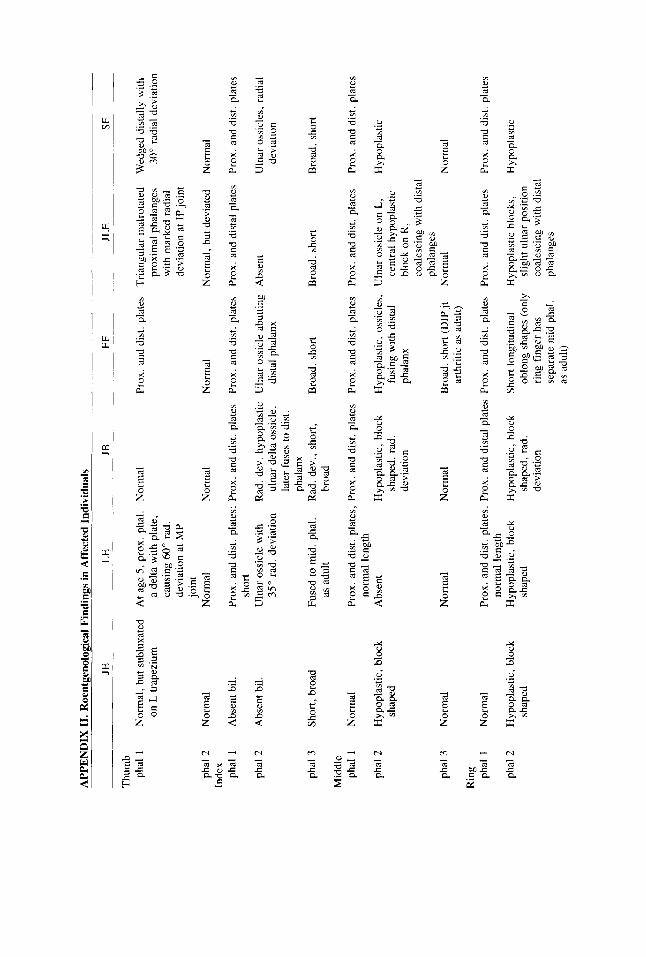
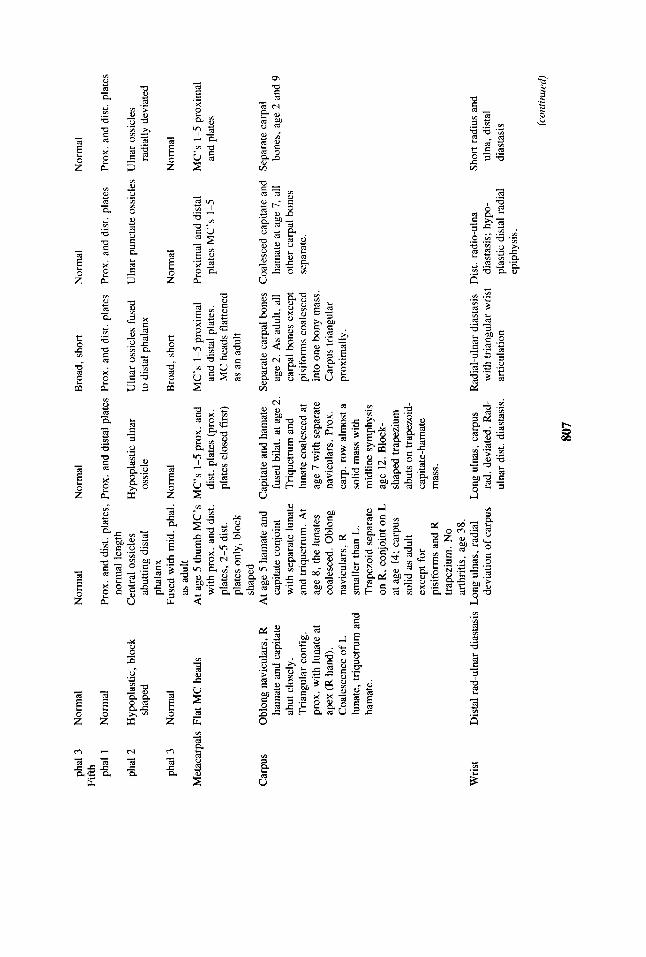
RADIOGRAPHIC FINDINGS
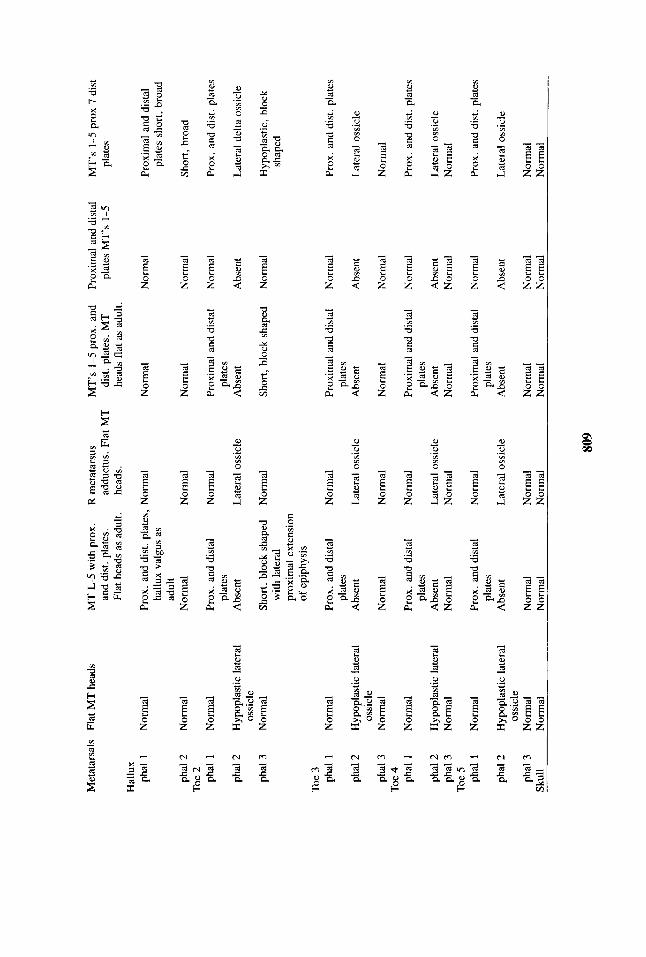
Radiographically (Figs. 4-10 and Appendix II), the middle phalanges of the fingers and toes are either absent or hypoplastic. The carpal bones show various degrees of coalescence. The humeri, shoulders, skull, cervical spine, and thoraco-
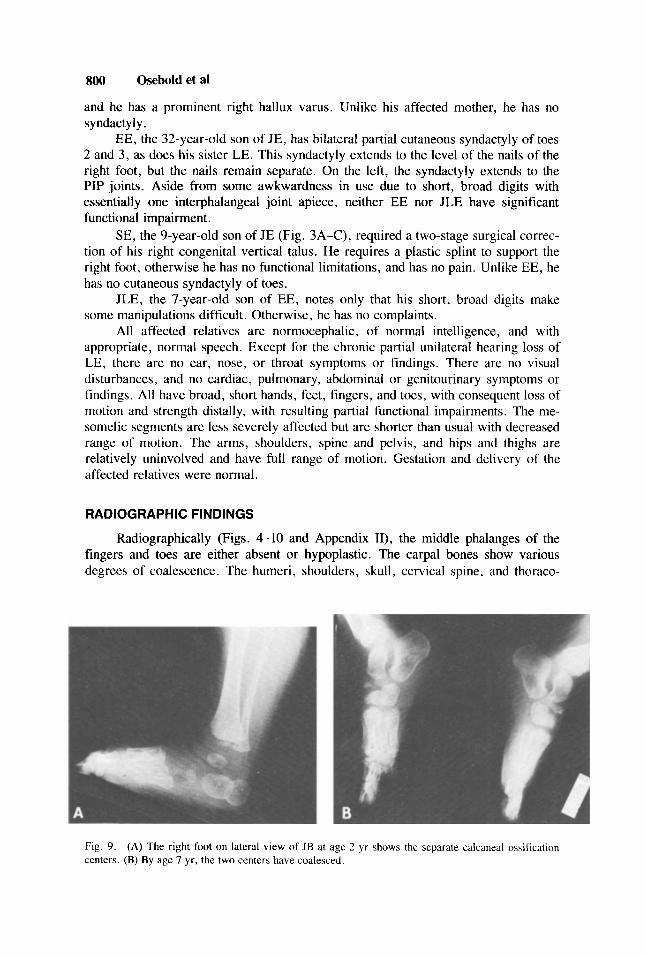
Fig. 9. (A) The right foot on lateral view of JB at age 2 yr shows the separate calcaneal ossification centers. (B) By age 7 yr, the two centers have coalesced.
Mesomelic Shortness, Brachydactyly Syndrome 801
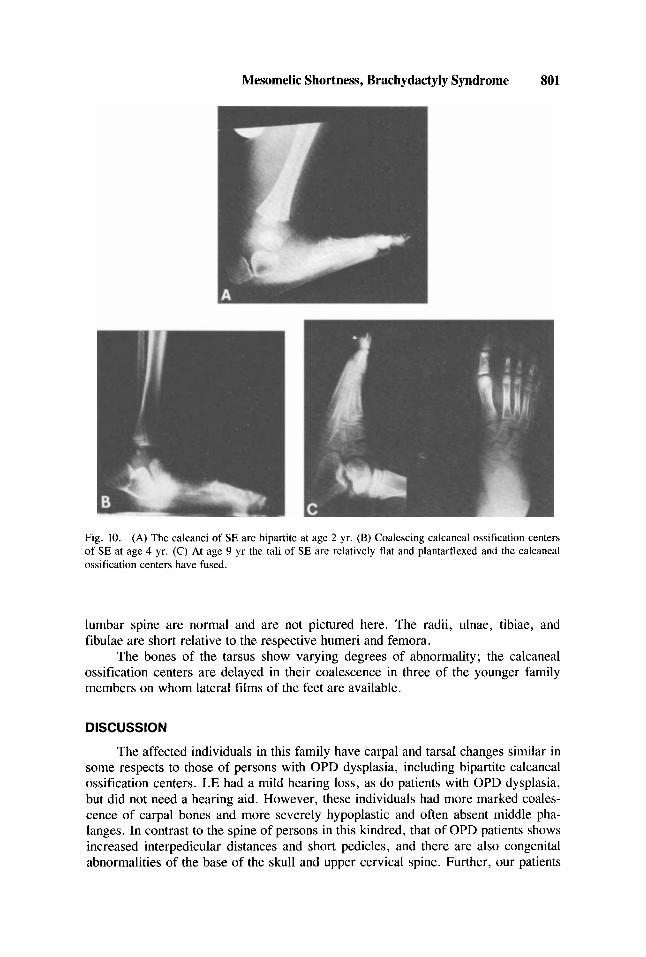
Fig. 10. (A) The calcanei of SE are bipartite at age 2 yr. (B) Coalescing calcaneal ossification centers of SE at age 4 yr. (C) At age 9 yr the tali of SE are relatively flat and plantarflexed and the calcaneal ossification centers have fused.
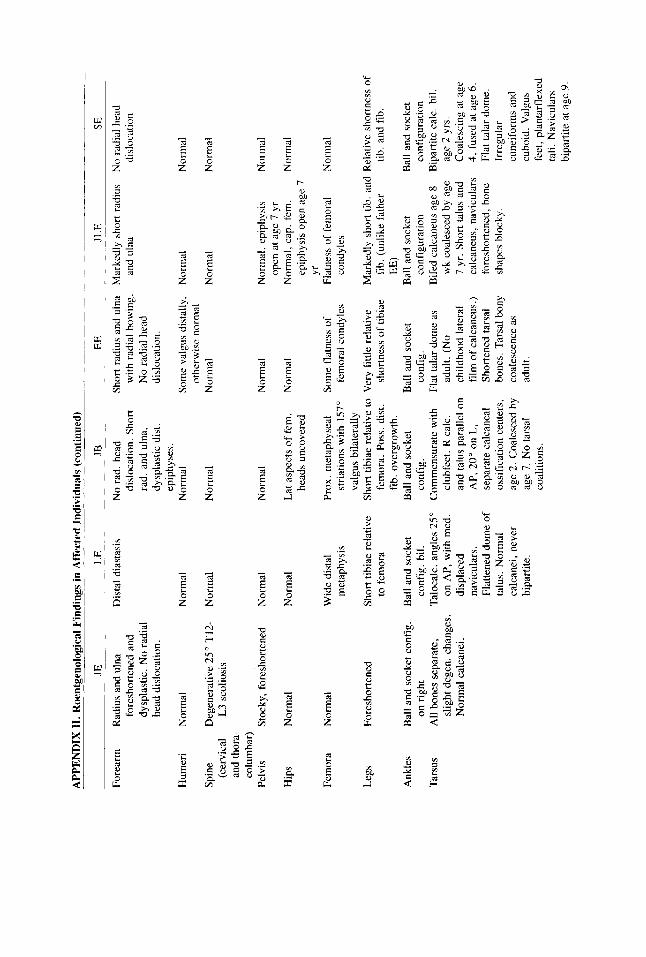
lumbar spine are normal and are not pictured here. The radii, ulnae, tibiae, and fibulae are short relative to the respective humeri and femora.
The bones of the tarsus show varying degrees of abnormality; the calcaneal ossification centers are delayed in their coalescence in three of the younger family members on whom lateral films of the feet are available.
DISCUSSION
The affected individuals in this family have carpal and tarsal changes similar in some respects to those of persons with OPD dysplasia, including bipartite calcaneal ossification centers. LE had a mild hearing loss, as do patients with OPD dysplasia, but did not need a hearing aid. However, these individuals had more marked coales- cence of carpal bones and more severely hypoplastic and often absent middle pha- langes. In contrast to the spine of persons in this kindred, that of OPD patients shows increased interpedicular distances and short pedicles, and there are also congenital abnormalities of the base of the skull and upper cervical spine. Further, our patients
802 Osebold et a1
are of normal intelligence and all three affected adults were married. None of the patients had the cleft palate, mild mental retardation, or the facial appearance typical of OPD dysplasia (with antimongoloid slant, small mouth, broad nasal root, and hypertelorism). Unlike in OPD dysplasia, there is no sex difference in expression in this kindred with the one woman as severely affected as the five males [Langer, 1967a; Gall et al, 1972; Spranger et al, 1974; Smith, 19761.
Patients with Larsen syndrome may have accessory calcaneal ossification ten- ters similar to the “bipartite calcanei” seen in the affected persons of this kindred, as well as abnormal middle phalanges of hands and feet, but they have extra, rather than fewer, carpal bones, and the digits are not short. None in this kindred had hip, knee, or elbow dislocations, the characteristic facial appearance, finger changes, big head, or the spinal anomalies that may be present in Larsen syndrome individuals. One person in the kindred did have a club foot [Larsen et al, 1950; Latta et al, 1971; McKusick, 1972; Steel and Kohl, 1972; Spranger et al, 1974; Smith, 19761.
Individuals with the trichorhinophalangeal (TRP) syndrome(s) lack the severe changes of the middle phalanges, but instead have hair, nail, nasal, and capital femoral epiphy seal changes, cone-shaped epiphyses, exostoses , and mental retardation that are absent in this kindred [Spranger et al, 1974; Smith, 1976).
Although the tibiae and radii of individuals in this kindred are proportionately shorter than their femora and humeri, they are not as short as in individuals with the Langer type of mesomelic dwarfism who also have mandibular hypoplasia [Langer, 3967b; Spranger et al, 1974; Smith 19761.
Unlike the mesomelic short stature of individuals with dyschondrosteosis, the ulnae in our patients are not prominent or subluxated. Also, the males in this lundred are as affected as the female, unlike the condition pertaining in dyschondrosteosis [McKusick, 1972; Spranger et al, 19741.
Broad phalanges of hands and feet, hypoplastic or absent middle phalanges with radial deviation of thumbs, and partial syndactyly with normal intelligence are also found in the Apert and Pfeiffer type of acrocephalosyndactyly. However, these individuals did not have the acro-oxy-brachycephaly with early closure of sagittal and coronal sutures, hypertelorism, hypoplastic maxillae, and resulting facial changes or Kleeblattschadel, trapezoidal proximal phalanges of the thumb and hallux, or radio- humeral synostosis that may be found in the Apert and Pfeiffer syndrome [Pfeiffer, 1964; Martsolf et al, 1971; Spranger et al, 1974; Smith, 19761.
Brachydactyly A, C, and E, as described by Bell, are autosomal dominant traits but do not affect all five digits of each hand and foot [Bell, 19511. The type-A variants involve digital anomalies usually confined to the middle phalanges of fingers and toes. In type Al , the middle phalanges of all digits are hypoplastic. However, in our patients, the middle phalanges of the long fingers were often in the form of ulnarly placed ossicles with consequent radial deviation of the distal phalanges, unlike the ulnar deviation of the distal phalanges of the middle fingers illustrated in radiographs of patients with type Al . In type Al , the index and little fingers are more severely affected than the middle and ring fingers, and no A1 case was found to show the middle phalanx as a separate bone. However, in our patients the middle phalanges of the index and little fingers were often separate, hypoplastic block shaped or centrally or ulnarly placed ossicles. Roentgenograms of patients with type Al do not show the coalescence of the carpal bones, especially of the proximal carpal row, nor the mesomelic dysplasia demonstrated in our patients. In type A2, only the second digits
Mesomelic Shortness, Brachydactyly Syndrome 803
are involved, and in type A3, only the middle phalanx of the little fingers is involved with consequent clinodactyly. Types A3 and usually C do not involve the feet. In type B, the terminal phalanges are severely affected, and thumbs and great toes are normal. There is no carpal coalition. In type C, the ring and little fingers are normal. In type D, the thumbs are short, but the hands are otherwise normal. In type E, the metacarpals and metatarsals are most severely affected with relative sparing of the middle phalanges [Bell, 1951; Riccardi and Holmes, 19741. Patients with the preaxial brachydactyly described by Christian et a1 [ 19721 have nearly normal carpal bones and middle phalanges. Patients with the Weill-Marchesani syndrome of brachydactyly and spherophakia also have short stature and broad digits, but rather characteristic skull changes, lens and visual disturbances, relatively normal middle phalanges, and their trait are due to autosomal recessive inheritance [McKusick, 1972; Smith, 19761.
Short hands, feet, shanks, and forearms are present in acromesomelic dysplasia [Maroteaux et al, 19711. It differs from the present condition by the systemic involvement of all tubular bones of the hands and feet, spinal changes, and the autosomal recessive mode of inhertance.
Patients with the multiple synostosis disease of Maroteaux, Bouvet, and Briard exhibit autosomal dominant symphalangism and fusion of carpal and tarsal bones, but unlike our patients they also have elbow joint ankylosis, deafness, amputation of distal phalanges, and a characteristic face [Maroteaux et al, 1972; Herrmann, 1974; Higashi and Inoue, 19831.
“Bipartite” calcaneus (or, more accurately, delayed coalescence of separate calcaneal centers of ossification) has also been described in OPD dysplasia, Down syndrome, and mucopolysaccharidosis type I [Caffey, 19721. The first ossification center appears at about 4 to 5 fetal mo laterally in the area of the trochlear process; the second appears at about 7 mo; they normally coalesce by about age 1 yr [Kohler and Zimmer, 19681. The calcanei of JE, LE, and EE were normal in appearance by adulthood. Foot films of LE and EE at 8 yr showed normal calcanei. The calcanei of JB were bipartite at 2 yr and coalesced by 7 yr. The calcanei of JLE were bipartite at 8 wk, but coalesced by 7 yr. Those of SE were bipartite at 2 yr, coalescing at 4 yr, and fused by 9 yr.
In summary, the presence in our patients of carpal and tarsal coalescence, hypoplastic or absent middle phalanges, delayed coalescence of bipartite calcanei , normal eyes, normal intelligence, shortness of stature and mesomelic shortness of limbs with autosomal dominant inheritance seems to represent a previously unde- scribed syndrome.
ACKNOWLEDGMENTS
The authors thank the family whose affected members are described here. It is their desire to know more about their syndrome and to share this knowledge with the medical community, which made this paper possible.
REFERENCES
Bell J (1951): On brachydactyly and symphalangism. In “Treasury of Human Inheritance.” Vol V.
Caffey J (1972): “Pediatric X-Ray Diagnosis.” 2nd Ed. Chicago: Year Book Medical Publishers, Inc., London: Cambridge University Press, Vol V, pp 1-3 1.

804 Osebold et al
pp 920--92 1. Christian JC, Cho KS, Franken EA, Thompson BH (1972): Dominant preaxial brachydactyly with hallux
varus and thumb abduction. Am J Hum Genet 24:694-701. Gall JC, Stern AM, Poznanski AK, Garn SM, Weinstein ED, Hayward JR (1972): Oto-palato-digital
syndrome: Comparison of clinical and radiographic manifestations in males and females. Am J Hum Genet 24:24-36.
Herrmann J (1974): Symphalangism and brachydactyly syndromes: Report of the WL symphalangism- brachydactyly syndrome: Review of literature and classification. In Bergsma D (ed): “Limb Malformations.” Miami: Symposia Specialists for the National Foundation-March of Dimes,
Higashi K, Inoue S (1983): Conductive deafness, symphalangism, and facial abnormalitics: The WL
Kohler A, Zimmer EA (1968): “Borderlands of the Normal and Early Pathologic in Skeletal Roentgen-
Langer LO, Jr. (1967a): The Roentgenographic Features of the Oto-palato-digital (OPD) Syndrome. Am
Langer LO, Jr. (1967b): Mesomelic dwarfism of the hypoplastic ulna, fibula, mandible type. Radiology
Larsen JL, Schottstaedt ER, Bost RC (1950): Multiple congenital dislocations associated with character-
Latta RJ, Graham B, Aase J, Scham SM, Smith DW (1971): Larsen’s Syndrome. J Pediatr 78:291-298. McKusick VA (1972): “Heritable Disorders of Connective Tissue.” Saint Louis: The CV Mosby
Company, pp 282-29 1. Maroteaux P, Martinelli B, Campailla E (1971): Le nanisme acromtsomClique. Presse Med 79: 1839-
1842. Maroteaux P, Bouvet JP, Briard ML (1972): La maladie des synostoses multiples. Nouv Presse Med
I :304-3047. Martsolf JT, Cracco JB, Carpenter GG, O’Hara AE (1971): Pfeiffer Syndrome. Am J Dis Child 121 :257-
262. Opitz JM, Gilbert EF (1985): Brief clinical report: Autopsy findings in a still-born female infant with
the Osebold-Remondini Syndrome. Am J Med Genet 22:811-819. Pfeiffer RA (1964): Dominant erbliche Akrocephalosyndactylie. Z Kinderheilkd 90:301-320. Riccardi VM, Holmes LB (1974): Brachydactyly, type E. J Pediatr 84:251-254. Smith D (1976): “Recognizable Patterns of Human Malformation.” Philadelphia: WB Saunders Company. Spranger JW, Langer LO, Wiedemann HR (1974): “Bone Dysplasias. ” Philadelphia: WB Saunders
Steel HH, Kohl J (1972): Multiple congenital dislocations associations with other skeletal anomalies
BD: OAS X (5): 23-53.
syndrome in a Japanese family. Am J Med Genet 16:105-109.
ology.” 3rd American Ed. New York: Grune and Stratton, pp 479-481.
J Roentgen 100:63-70.
891654-660.
istic facial abnormality. J Pediatr 37:574-581.
Company.
(Larsen’s syndrome). J Bone Joint Surg 54A:75-82.
Edited by James F. Reynolds
APP
EN
DIX
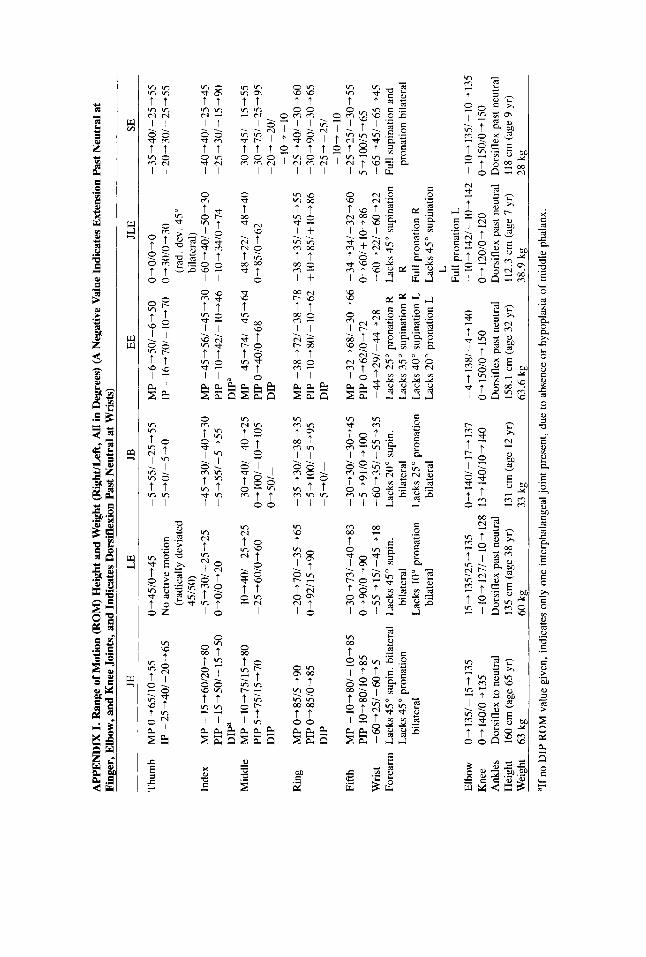
I. R
ange
of M
otio
n (R
OM
) Hei
ght a
nd W
eigh
t (R
ight
lLef
t, AU
in
Deg
rees
) (A
Neg
ativ
e Val
ue In
dica
tes E
xten
sion
Pas
t Neu
tral
at
Fing
er, E
lbow
, and
Knee
Join
ts, a
nd In
dica
tes D
orsi
flexi
on P
ast N
eutr
al a
t Wri
sts)
JE
LE
JB
E
E
JLE
SE
Thum
b M
P 0+
65/1
0-55
0-
45/0
+45
-5+5
5/-2
5+55
M
P -6
+50/
-6-5
0 O-
O/O+
O -3
5-40
1 -2
5 -5
5 IP
-25
+40/
-2O
j6.5
N
o ac
tive
mot
ion
-5-0
/-5+
0 IP
-16
+701
-10+
70
0+30
/0+3
0 -2
0+30
/ -2
5-55
(r
adic
ally
dev
iate
d (r
ad. d
ev. 4
5"
4515
0)
bila
tera
l) In
dex
MP
-15-
60/2
0-80
-5
+30/
-25+
25
-45+
30/-
40-3
0 M
P -4
5+56
/-45
-30
-60+
401-
50+3
0 -4
0+40
1-25
+45
PIP - 15
+50
/ - 15
+ 50
0+
0/0-
20
-5+
55/-
5+55
PI
P - 1
0-42
1-
10-4
6 - 1
0+34
/0+7
4 -2
5 +3
0/ - 15
-90
DIP
D
IPa
Mid
dle
MP
-10+
75/1
5+80
-1
0-40
/-25
-25
-30+
40/-
40-2
5 M
P -4
5-74
1-45
+64
-48+
22/-
48+4
0 -3
0-45
1-
15-5
5 PI
P 5+
75/1
5-70
- 25
+ 60
/0 +
60
0-
10
0-
10-
105
PIP
0+40
/0+6
8 0 +
85/0
- 62 - 30
- 75
1 -2s
+95
D
IP
0-50
/-
DIP
-2
0-
-201
- 1
0- - 10
R
ing
MP
0-85
/5-9
0 -2
0+70
/ -3
5 -6
5 - 35
+ 30
/ - 38
+ 35
M
P -3
8 +
72/ -
38-
78
-38
+ 3.5
1 -4
5 -5
5 -2
5 -4
01 -
30-
60
PIP
0-85
/0-8
5 0-
92/1
5+90
-5
+100
/-5+
95
PIP
-10+
801-
10+6
2 +1
0+85
/+10
+86
-30+
90/-
30+6
5 D
IP
-5+
0/-
DIP
-2
5-
-2.5
1 - 1
0- - 10
PIP
10+8
0/10
-85
0490
/0-
90
-5+
91/0
-t10
0 PI
P 0-
+62/
0+72
0-
60/+
10
-86
5+10
0/5-
65
Fifth
M
P -1
0-80
/-
10-8
5 -3
0-73
/-40
-83
-30-
301-
30-4
5 M
P -3
2-68
1-30
-66
-34-
341-
32-6
0 -2
5+25
/-30
-55
Wris
t - 60
+25
/ - 60
+ 5
-55-
15
/ -45
- 18
-6
0-39
-5
5-35
-U
+2
9/
-44-
28
-60-
221-
60-2
2 -6
5 -4
.5-6
5-45
Fo
rear
m
Lack
s 45
" su
pin.
bila
tera
l La
cks
45"
supi
n.
Lack
s 20
" su
pin.
La
cks
25"
pron
atio
n R
Lack
s 45
" su
pina
tion
Full
supi
natio
n an
d La
cks 4
5 pr
onat
ion
bila
tera
l bi
late
ral
Lack
s 35
" su
pina
tion
R
R
pron
atio
n bi
late
ral
bila
tera
l La
cks
10"
pron
atio
n La
cks
25"
pron
atio
n La
cks 4
0" s
upin
atio
n L
Full
pron
atio
n R
bi
late
ral
bila
tera
l La
cks
20"
pron
atio
n L
Lack
s 45"
sup
inat
ion
L Fu
ll pr
onat
ion
L El
bow
0- 1
35/ - 15
+ 13
5 15
+135
/25+
135
0+14
0/-1
7+13
7 -4
+138
/-4+
140
-10+
142/
-10+
142
-10+
135/
-10-
135
Kne
e 0-
14
0/0+
135
- 10
- 12
71-
10-
128
13-
140/
10+
140
0-
150/
0+ 1
50
0-
1201
0-
120
0-
150/
0-
150
Ank
les
Dor
sifle
x to
neu
tral
Dor
sifle
x pa
st n
eutra
l D
orsi
flex
past
neu
tral
Dor
sifle
x pa
st n
eutra
l D
orsi
flex
past
neu
tral
Hei
ght
Wei
ght
63 k
g 60
kg
33 k
g 63
.6 k
g 38
.9 k
g 28
kg
aIf n
o D
IP R
OM
val
ue g
iven
, in
dica
tes
only
one
inte
rpha
lang
eal j
oint
pre
sent
, du
e to
abs
ence
or
hypo
plas
ia o
f m
iddl
e ph
alan
x.
160
cm (
age
65 y
r)
135
cm (a
ge 3
8 yr
) 13
1 cm
(ag
e 12
yr)
15
8.1
cm [
age
32 y
r)
112.
3 cm
[age
7 y
r)
118
cm (
age
9 yr
)
APP
EN
DIX
11.
Roe
ntge
nolo
gica
l Fi
ndin
gs in
Aff
ecte
d In
divi
dual
s
LE
JB
JL
E
SE
EE
~~
~_
__
~~
Thu
mb
phal
1
phal
2
phal
1
phal
2
Inde
x
phal
3
Mid
dle
phal
1
phal
2
phal
3
Rin
g phal
1
phal
2
Nor
mal
, but
sub
luxa
ted
on L
trap
eziu
m
Nor
mal
Abs
ent b
il.
Abs
ent b
il.
Shor
t, br
oad
Nor
mal
Hyp
opla
stic
, bl
ock
shap
ed
Nor
mal
Nor
mal
Hyp
opla
stic
, bl
ock
shap
ed
At
age
5, p
rox.
pha
l. N
orm
al
a de
lta w
ith p
late
, ca
usin
g 60
" ra
d.
devi
atio
n at
MP
join
t N
orm
al
Nor
mal
Prox
. and
dis
t. pl
ates
T
rian
gula
r m
alro
tate
d pr
oxim
al p
hala
nges
w
ith m
arke
d ra
dial
de
viat
ion
at I
P jo
int
Nor
mal
N
orm
al, b
ut d
evia
ted
Prox
. and
dis
t. pl
ates
; Pr
ox.
and
dist
. pla
tes
Prox
. an
d di
st. p
late
s Pr
ox. a
nd d
ista
l pla
tes
Uln
ar o
ssic
le w
ith
Rad
. dev
. hy
popl
astic
U
lnar
oss
icle
abu
tting
A
bsen
t sh
ort
35"
rad.
dev
iatio
n ul
nar
delta
oss
icle
, di
stal
pha
lanx
la
ter
fuse
s to
dis
t. ph
alan
x Fu
sed
to m
id. p
hal.
Rad
. dev
., sh
ort,
Bro
ad,
shor
t B
road
, sh
ort
as a
dult
broa
d
Prox
. an
d di
st.
plat
es,
Prox
. and
dis
t. pl
ates
Pr
ox.
and
dist
. pla
tes
Prox
. an
d di
st. p
late
s
Abs
ent
Hyp
opla
stic
, bl
ock
Hyp
opla
stic
, os
sicl
es,
Uln
ar o
ssic
le o
n L
, no
rmal
len
gth
shap
ed,
rad.
fu
sing
with
dis
tal
cent
ral
hypo
plas
tic
devi
atio
n ph
alan
x bl
ock
on R
, co
ales
cing
with
dis
tal
Wed
ged
dist
ally
with
30
" ra
dial
dev
iatio
n
Nor
mal
Prox
. and
dis
t. pl
ates
Uln
ar o
ssic
les,
rad
ial
devi
atio
n
Bro
ad,
shor
t
Prox
. and
dis
t. pl
ates
Hyp
opla
stic
phal
ange
s N
orm
al
Nor
mal
B
road
, sh
ort (
DIP
jt
Nor
mal
N
orm
al
arth
ritic
as
adul
t)
Prox
. an
d di
st.
plat
es,
Prox
. an
d di
stal
pla
tes
Prox
. and
dis
t. pl
ates
Pr
ox. a
nd d
ist.
plat
es
Hyp
opla
stic
, bl
ock
Hyp
opla
stic
, bl
ock
Shor
t lon
gitu
dina
l H
ypop
last
ic b
lock
s,
Hyp
opla
stic
Prox
. an
d di
st. p
late
s no
rmal
len
gth
shap
ed
shap
ed, r
ad.
oblo
ng s
hape
s (o
nly
slig
ht u
lnar
pos
ition
de
viat
ion
ring
fin
ger
has
coal
esci
ng w
ith d
ista
l se
para
te m
id p
hal.
phal
ange
s as
adu
lt)
phal
3
Nor
mal
phal
1
Nor
mal
phal
2
Hyp
opla
stic
, blo
ck
Fifth
shap
ed
phal
3
Nor
mal
Met
acar
pals
Fla
t MC
hea
ds
Car
pus
Obl
ong
navi
cula
rs, R
ha
mat
e an
d ca
pita
te
abut
clo
sely
. Tr
iang
ular
con
fig.
prox
. with
ha
te at
ap
ex (
R h
and)
. C
oale
scen
ce o
f L
Nor
mal
N
orm
al
Bro
ad, s
hort
Nor
mal
N
orm
al
Prox
. an
d di
st.
plat
es,
Prox
. an
d di
stal
pla
tes
Cen
tral o
ssic
les
Hyp
opla
stic
uln
ar
norm
al le
ngth
abut
ting
dist
al
ossi
cle
p h a 1
an x
as a
dult
with
pro
x. a
nd d
ist.
plat
es, 2
-5 d
ist.
plat
es o
nly,
blo
ck
shap
ed
At a
ge 5
ham
ate
and
Fuse
d w
ith m
id. p
hal.
Nor
mal
At a
ge 5
thum
b M
C’s
MC
’s 1
-5 p
rox.
and
di
st. p
late
s (p
rox.
pl
ates
clo
sed
first
)
Cap
itate
and
ham
ate
capi
tate
con
join
t w
ith s
epar
ate
luna
te
and
triqu
etru
m.
At
age
8, th
e lu
nate
s co
ales
ced.
Obl
ong
navi
cula
rs, R
lu
nate
, tri
quet
rum
and
sm
alle
r th
an L
. ha
mat
e.
Trap
ezoi
d se
para
te
on R
, con
join
t on
L at
age
14;
car
pus
solid
as
adul
t ex
cept
for
pi
sifo
rms
and
R
trape
zium
. N
o ar
thrit
is.
age
38.
Prox
. an
d di
st. p
late
s Pr
ox.
and
dist
. pla
tes
Uln
ar o
ssic
les
fuse
d U
lnar
pun
ctat
e os
sicl
es
Uln
ar o
ssic
les
to d
ista
l pha
lanx
ra
dial
ly d
evia
ted
Prox
. an
d di
st. p
late
s
Bro
ad, s
hort
Nor
mal
N
orm
al
MC
’s 1
-5 p
roxi
mal
Pr
oxim
al a
nd d
ista
l M
C’s
1-5
pro
xim
al
and
dist
al p
late
s.
plat
es M
C’s
1-5
an
d pl
ates
M
C h
eads
flat
tene
d as
an
adul
t
Sepa
rate
car
pal b
ones
C
oale
sced
cap
itate
and
Se
para
te c
arpa
l fu
sed
bila
t. at
age
2
age
2. A
s adu
lt, a
ll Tr
ique
trum
and
ca
rpal
bon
es e
xcep
t ot
her
carp
al b
ones
h
ate
coal
esce
d at
pi
sifo
rms
coal
esce
d se
para
te.
age
7 w
ith s
epar
ate
into
one
bon
y m
ass.
na
vicu
lars
. Pr
ox.
Car
pus
trian
gula
r ca
rp. r
ow a
lmos
t a
prox
imal
ly.
solid
mas
s w
ith
mid
line
sym
phys
is
age
12. B
lock
- sh
aped
trap
eziu
m
abut
s on
trap
ezoi
d-
capi
tate
-ham
ate
mas
s.
ham
ate
at a
ge 7
, all
bone
s, a
ge 2
and
9
,-
Wris
t D
ista
l fad
-uln
ar d
iast
asis
Lon
g ul
nas,
rad
ial
Long
uln
as,
carp
us
Rad
ial-u
lnar
dia
stas
is
Dis
t. ra
dio-
ulna
Sh
ort r
adiu
s an
d de
viat
ion
of c
arpu
s ra
d. d
evia
ted.
Rad
- w
ith tr
iang
ular
wris
t di
asta
sis;
hy
p-
ulna
, dis
tal
ulna
r di
st. d
iast
asis
. ar
ticul
atio
n pl
astic
dis
tal r
adia
l di
asta
sis
epip
hysi
s.
(con
tinue
d)
807
APP
END
IX 1
1. R
oent
geno
logi
cal F
indi
ngs
in A
ffec
ted
Indi
vidu
als
(con
tinue
d)
JE
Fore
arm
R
adiu
s an
d ul
na
fore
shor
tene
d an
d dy
spla
stic
. N
o ra
dial
he
ad d
islo
catio
n.
Hum
eri
Nor
mal
Spin
e D
egen
erat
ive
25"
T12-
(c
ervi
cal
L3
scol
iosi
s an
d th
ora-
co
lurn
bar)
Pe
lvis
St
ocky
, for
esho
rten
ed
Hip
s N
orm
al
Fem
ora
Nor
mal
Legs
Fo
resh
orte
ned
Ank
les
Bal
l and
soc
ket c
onfig
. on
righ
t Ta
rsus
A
ll bo
nes
sepa
rate
, sl
ight
deg
en.
chan
ges
Nor
mal
cal
cane
i.
JB
____
LE
Dis
tal d
iast
asis
N
o ra
d. h
ead
disl
ocat
ion.
Sho
rt ra
d. a
nd u
lna,
dy
spla
stic
dis
t. ep
iphy
ses.
N
orm
al
Nor
mal
Nor
mal
N
orm
al
Nor
mal
N
orm
al
Nor
mal
La
t asp
ects
of
fem
. he
ads
unco
vere
d
Wid
e di
stal
Pr
ox.
met
aphy
seal
m
etap
hysi
s
Shor
t tib
iae
rela
tive
to fe
mor
a
Bal
l and
soc
ket
conf
ig.
bil.
Talo
calc
. an
gles
25"
on
AP,
with
med
. di
spla
ced
navi
cula
rs.
Flat
tene
d do
me
of
talu
s. N
orm
al
calc
anei
, nev
er
bipa
rtite
.
EE
JLE
SE
Shor
t rad
ius
and
ulna
M
arke
dly
shor
t rad
ius
No
radi
al h
ead
with
rad
ial b
owin
g.
and
ulna
di
sloc
atio
n N
o ra
dial
hea
d di
sloc
atio
n.
Som
e va
lgus
dis
tally
, N
orm
al
Nor
mal
N
orm
al
othe
rwis
e no
rmal
N
orm
al
Nor
mal
Nor
mal
N
orm
al,
epip
hysi
s N
orm
al
Nor
mal
N
orm
al, c
ap. f
em.
Nor
mal
op
en a
t age
7 y
r
epip
hysi
s op
en a
ge 7
Yr
So
me
flatn
ess
of
Flat
ness
of
fem
oral
N
orm
al
._
st
riatio
ns w
ith 1
57"
fem
oral
con
dyle
s va
lgus
bila
tera
lly
fem
ora.
Pos
s. d
ist.
fib.
ove
rgro
wth
.
conf
ig.
conf
ig.
club
feet
. R c
alc.
ad
ult.
(No
and
talu
s pa
ralle
l on
child
hood
late
ral
AP,
20"
on
L,
film
of
calc
aneu
s.)
sepa
rate
cal
cane
al
Shor
tene
d ta
rsal
os
sific
atio
n ce
nter
s,
bone
s. T
arsa
l bon
y ag
e 2.
Coa
lesc
ed b
y ag
e 7.
No
tars
al
adul
t. co
aliti
ons.
Shor
t tib
iae
rela
tive
to V
ery
little
rel
ativ
e sh
ortn
ess
of ti
biae
Bal
l and
soc
ket
Com
men
sura
te w
ith
Bal
l and
soc
ket
Flat
tala
r dom
e as
coal
esce
nce
as
cond
yles
Mar
kedl
y sh
ort t
ib. a
nd R
elat
ive
shor
tnes
s of
fi
b. (
unlik
e fa
ther
tib
. an
d fi
b.
EE
) B
all a
nd s
ocke
t co
nfig
urat
ion
conf
igur
atio
n B
ipar
tite
calc
. bil.
w
k co
ales
ced
by a
ge
7 yr
. Sho
rt ta
lus
and
calc
aneu
s, n
avic
ular
s fo
resh
orte
ned,
bon
e Fl
at ta
lar
dom
e.
shap
es b
lock
y.
Irre
gula
r cu
neifo
rms
and
cubo
id.
Val
gus
feet
, pla
ntar
flexe
d ta
li. N
avic
ular
s bi
parti
te a
t age
9.
Bal
l and
soc
ket
Bife
d ca
lcan
eus
age
8 ag
e 2
yrs.
C
oale
scin
g at
age
4
, fus
ed a
t age
6.
Met
atar
sals
Fl
at M
T h
eads
Hal
lux
phal
1
phal
2
phal
1
phal
2
phal
3
Toe
2
Toe
3 ph
al 1
phal
2
phal
3
phal
1
phal
2 ph
al3
phal
1
phal
2
phal
3
Toe
4
Toe
5
Nor
mal
Nor
mal
Nor
mal
Hyp
opla
stic
late
ral
Nor
mal
os
sicl
e
Nor
mal
Hyp
opla
stic
late
ral
Nor
mal
os
sicl
e
Nor
mal
Hyp
opla
stic
late
ral
Nor
mal
Nor
mal
Hyp
opla
stic
late
ral
Nor
mal
N
orm
al
ossi
cle
MT
L-5
with
pro
x.
R m
etat
arsu
s M
T’s
1-5
prox
. an
d an
d di
st. p
late
s.
addu
ctus
. Fl
at M
T
dist
. pla
tes.
MT
Fl
at h
eads
as
adul
t.
Prox
. an
d di
st. p
late
s,
hallu
x va
lgus
as
adul
t N
orm
al
Prox
. an
d di
stal
Abs
ent
plat
es
Shor
t, bl
ock
shap
ed
with
late
ral
prox
imal
ext
ensi
on
of e
piph
ysis
Prox
. an
d di
stal
Abs
ent
plat
es
Nor
mal
Prox
. an
d di
stal
pl
ates
A
bsen
t N
orm
al
Prox
. and
dis
tal
Abs
ent
plat
es
Nor
mal
N
orm
al
head
s.
Nor
mal
Nor
mal
Nor
mal
Late
ral
ossi
cle
Nor
mal
Nor
mal
Late
ral o
ssic
le
Nor
mal
Nor
mal
Late
ral
ossi
cle
Nor
mal
Nor
mal
Late
ral o
ssic
le
Nor
mal
N
orm
al
head
s fla
t as
adul
t.
Nor
mal
Nor
mal
Prox
imal
and
dis
tal
Abs
ent
Shor
t, bl
ock
shap
ed
plat
es
Prox
imal
and
dis
tal
Abs
ent
plat
es
Nor
mal
Prox
imal
and
dis
tal
plat
es
Abs
ent
Nor
mal
Prox
imal
and
dis
tal
Abs
ent
plat
es
Nor
mal
N
orm
al
Prox
imal
and
dis
tal
plat
es M
T’s
1-5
Nor
mal
Nor
mal
Nor
mal
Abs
ent
Nor
mal
Nor
mal
Abs
ent
Nor
mal
Nor
mal
Abs
ent
Nor
mal
Nor
mal
Abs
ent
Nor
mal
N
orm
al
MT’
s 1-
5 pr
ox 7
dis
t pl
ates
Prox
imal
and
dis
tal
plat
es s
hort,
bro
ad
Shor
t, br
oad
Prox
. and
dis
t. pl
ates
Late
ral d
elta
oss
icle
Hyp
opla
stic
, bl
ock
shap
ed
Prox
. an
d di
st. p
late
s
Late
ral o
ssic
le
Nor
mal
Prox
. and
dis
t. pl
ates
Late
ral o
ssic
le
Nor
mal
Prox
. an
d di
st. p
late
s
Late
ral o
ssic
le
Nor
mal
N
orm
al
809
Recommended