1
“I CAN’T BREATH”Respiratory Emergencies
Objectives
•Review of anatomical structures related to heart & lungs•Differentiate differences between adult and pediatric airways•Identify the need for airway assistance & management•Review of patient assessment skills & pearls•Identify interventions with case studies
AIRWAY & HEART ANOTOMY
Normal BreathingWe Must Have:
• Patent airway• Intact System
• Ventilatory • Musculoskeletal
• Pulmonary Blood Flow• Neurological Stimulation
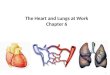
Anatomy of Lungs & Heart
Anatomy of the Upper Airway
• Nasal Cavity• Oral Cavity• Pharynx
– Nasopharynx– Oropharynx– Laryngopharynx
https://pocketdentistry.com/wp-content/uploads/285/f08-01-9781455745470.jpg

2
Anatomy of the Lower Airway
• Carina• Bronchi• Bronchioles• Alveoli
Anatomy of the Heart
http://the-cardiorespiratory-system.weebly.com/uploads/2/4/2/1/24210785/4254534_orig.png
Adult vs. Pediatric Airway
• Difference– Size– Cone Shaped Larynx
• Anterior Position• Epiglottis Rounder and Floppy• Cricoid Ring is the Narrowest Section
http://www.celebritydiagnosis.com/wp-content/uploads/2010/03/pediatric-airway.jpg
PATIENT ASSESSMENT
Decision Making
http://www.njms.in/articles/2014/5/2/images/NatlJMaxillofacSurg_2014_5_2_228_154844_f1.jpg

3
Assessment• General Impression• Mental Status
– AVPU– GCS
• Airway– Patent/Non Patent
• Breathing– Rate– Quality– SpO2 & ETCO2
Assessment• Circulation
– Pulses, Hemorrhage, Skin Color, Temperature & Condition
– Vascular Access– ECG & NIBP
• Disability
• Exposure– Remove clothing to visualize
Respiratory Assessment
Work of Breathing• What you Hear
• Stridor• Snoring• Gurgling• Grunting• Muffled/Hoarse Voice
• What you See• Tripoding• Sniffing Position• Accessory Muscle Use• Pursed Lip Breathing• Nasal Flaring• Head Bobbing• Seesaw Respirations• Prolonged Expiratory• Effortless Tachycardia
Physical Exam
• Inspection• Auscultation• Palpation• Percussion
Focused History
• OPQRST• Signs & Symptoms & Associated Symptoms• Allergies • Medications• Past Medical History• History of Present Illness
Non-Invasive Airway Monitoring• Pulse Oximetry Normal 95-100% <93-95% = Mild Hypoxia 85-90% = Moderate Hypoxia <85% = Severe Hypoxia Variation in Probe Locations
SpO2 reflects oxygenation, NOT ventilation

4
Non-Invasive Airway Monitoring
• Capnography (ETCO2)– Quantitative & Waveform– Qualitative
• Normal 35-45 mmHg
Measurement of Ventilation, NOT Oxygenation
http://4.bp.blogspot.com/-lsQAXTCM7uM/ViNUM3XbT4I/AAAAAAAAMfI/e3KfQYZvcGE/s640/normalcapnograph.jpg
AIRWAY MANAGEMENT
AIRWAYMANAGEMENT
“MOANS” “RODS”
“LEMONS” “SMART”
MOANS
• Difficult Bag-Valve-Mask Ventilations– Mask Seal– Obesity– Age– No Teeth– Stiff
http://livebearded.com/wp-content/uploads/2017/01/Steve.-K.jpg
Rules of 2’sTWO SKILL
Thumbs up technique 1 provider maintains seal1 provider ventilates
Airways NPA & OPA
Inches Raise patient (sniffing position)
Seconds Ventilation slow & gentle
PSI Minimum pressure

5
RODS• Difficult Extraglotic Device Placement
– Restricted Mouth Opening– Obstruction/Obesity– Distorted/Disrupted Airway– Stiff
http://3.bp.blogspot.com/_nhw37-0Cr1U/R8LikrnU2TI/AAAAAAAAAC8/phYylygZW5o/s320/005.JPG
http://www.jems.com/content/dam/jems/print-articles/2015/08/1508JEMS_BariatricAirway1.jpg
LEMONS & SMART• Difficult Intubation
– Look – Evaluate 3-3-2– Mallampati– Obstruction– Neck Mobility
• Difficult Cricothyrotomy– Surgery – Mallampati– Anatomy– Radiation– Tumor CARDIAC OR
RESPIRTORY
MI (Myocardial Infarction)
• Signs & Symptoms– Chest Discomfort– Dyspnea– Diaphoresis– EKG changes– Nausea & Vomiting– Anxiety– Radiated pain
• Treatment– 12 Lead– Oxygen– ASA– Pain Management
• Nitro• Fentanyl• Morphine
– Rapid Transport to PCI
CHF (Congestive Heart Failure)
• Signs & Symptoms– Non specific fatigue– Dyspnea
• With exertion• While flat (orthopnea)
– Edema– Anxiety– Coughing– Rales, Wheezing BS– S3 Gallop– JVD
• Treatment– Oxygen– NIPPV– Medications
• Nitro• Bronchodilator• Lasix

6
PUEMOTHORAX
• Signs & Symptoms– Altered LOC– Severe Dyspnea– Diminished or Absent BS
One Side– Low BP– Tachycardia
• Treatment– Oxygen– Needle Decompression– Chest Tube
BRONCHITIS (acute or chronic)
• Signs & Symptoms– Chest Discomfort– Dyspnea– Productive Cough– Rhinorrhea– BS-Rhonchi; Wheezing– Anxiety– BS reduced
• Treatment– Oxygen– Nebulized Medication
• Duo Neb• Albuterol• Racemic Epi
– Intubation?– Antibiotic– Anti-inflammatory– Corticosteroid
EMPHYSEMA
• Signs & Symptoms– Chest Discomfort– Progressive Dyspnea– SOB worse in AM– Anxiety– Cough worse in AM– Tachypnea– Accessory muscle use– Hyperinflation– Decreased BS
• Treatment– Oxygen– Nebulized Medication
• Duo Neb• Albuterol• Racemic Epi
– Intubation?– Antibiotic– Anti- inflammatory– Corticosteroid
PULMONARY EMBOLISM
• Signs & Symptoms– Shortness of Breath– Anxiety– Agitation– Mild to Sudden
Dyspnea– Chest pain– Hypoxemia– Hyperventilation
• Treatment– Oxygen– Nebulized Medication
• Duo Neb• Albuterol• Racemic Epi
– Epi – Intubation?– Anti-inflammatory– Corticosteroid
PNEUMONIA
• Signs & Symptoms– Shortness of Breath– Dry cough– Increased Temperature– Productive cough
• Green/brown/rust colored
– Tachycardia– Tachypnea
• Treatment– Oxygen– Nebulizer Medication
• Duo Neb• Albuterol• Racemic Epi
– Antibiotics– Intubation?
ASTHMA
• Signs & Symptoms– Shortness of Breath– Wheezing – Cough– Anxiety– Agitation– Speech Dyspnea– Chest Tightness– Pulsus Paradoxus– Tachycardia
• Treatment– Oxygen– Nebulized Medication
• Duo Neb• Albuterol• Racemic Epi
– Epi – Intubation?– Anti-inflammatory

7
ANAPHYLAXIS• Signs & Symptoms
– Shortness of Breath/tightness in Throat
– Anxiety– Agitation– Mild to Sudden
Dyspnea– Urtiicaria– Angioedema– Hypoxemia– Hyperventilation
• Treatment– Oxygen– Epi
• More epi
– Nebulizer Medication• Duo Neb• Albuterol• Racemic Epi
– Corticosteroid– Benadryl
Case #1
62 year old MaleProgressive SOB over 18 monthsIncreased over 4-5 daysProductive CoughAccessory Muscle UseHyperinflated
VitalsA- patent,B- 30 bpm; minor wheezing 85% RAC- 120 bpmD- speaks in full sentences; GCS-15E- No Trauma notedSkin- warm and dry but pale
http://4.bp.blogspot.com/_7zQULPNQ7FQ/Sfh8F5-qOQI/AAAAAAAAAB4/f5niTU0epGU/s320/bluebloater.jpg.jpeg
Treatment ?

8
Case #222 year old FemaleFour Wheeler AccidentEjected Off WheelerHit Face & Head on Roof of RazorPatient is seated on ground leaning forward
AirwayVitals
A- As seenB- 30 bpm; minor wheezing 85% RAC- 140 bpmD- can answer yes & no GCS-13E- Only facial traumaSkin- pink and dry
Treatment ? Case #3

9
85 year old MaleIncreased SOB over 3 hoursNebulizer did not helpAccessory Muscle UseHyperinflated
VitalsA- PatentB- 40 bpm; minor wheezing 80% RAC- 140 bpmD- Speaks in 1-2 word sentence GCS-12E- Barrel chest, ribs visibleSkin- dry and pale
Treatment ?
https://www.google.com/url?sa=i&rct=j&q=&esrc=s&source=images&cd=&cad=rja&uact=8&ved=0ahUKEwiYtenH29TUAhUQz2MKHUqCDCUQjRwIBw&url=https%3A%2F%2Fwww.youtube.com%2Fwatch%3Fv%3Dy82dL8QAUF8&psig=AFQjCNFULFv5Kl1XLSSHliXxKRRkCzkGww&ust=1498333009494688
Case #4
35 year old FemaleSudden onset of SOB for last 3 daysProductive cough for 7 daysLeft side chest pain
VitalsA- Green sputumB- 22 bpm; BS-left side cracklesbilateral dullness SpO2 90%C- 120 bpm BP 155/72D- GCS-15E- no noted traumaSkin- hot, flushed

10
Treatment ?
Recommended