Aggression, Violence and Psychopathology:
A Developmental Approach
Hans Steiner, MDProfessor, Division of Child
Psychiatry Stanford University School of Medicine
Disclosure Information
• Consultant for: Abbott Laboratories, Janssen Pharmaceutica
• Receives research support from: Abbott Laboratories, Astra Zeneca, Janssen Pharmaceutica, Pfizer, Inc., Wyeth-Ayerst, Solvay Pharmaceuticals, GlaxoSmithKline
• Speaker for: Abbott Laboratories, Janssen Pharmaceutica, Pfizer, Inc., AstraZeneca
Disclaimer
All current psychopharmacologic treatments for aggression and its disorders in children and adolescents are off-label.
The Current Lecture
• The aggression system
• Update on the psychopharmacology of juvenile aggression
• Meta-analysis of stimulants and aggression
• Relationship of aggression to psychiatric trauma and psychopathology
• Reactive/Affective/Defensive/ (RAD) Aggression
• Antikindling treatment of aggression based on this model
• Early developmental manifestations of RAD aggression
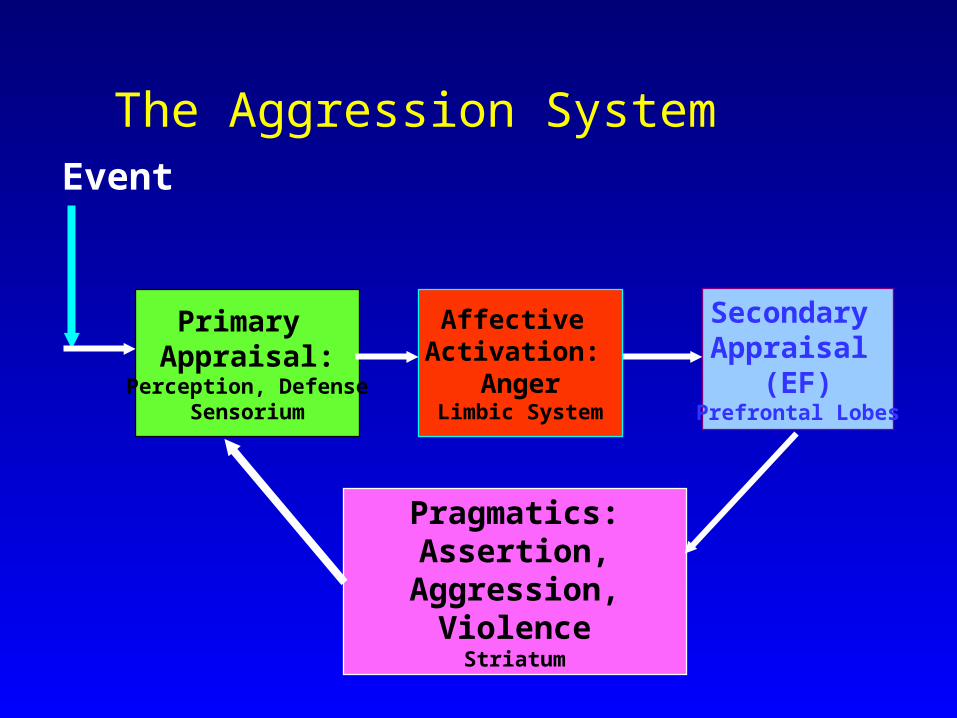
The Aggression System
Pragmatics:Assertion,
Aggression,Violence
Striatum
Event
Primary Appraisal:
Perception, DefenseSensorium
Secondary Appraisal
(EF)Prefrontal Lobes
Affective Activation:
AngerLimbic System
Randomized, Placebo-Controlled Clinical Trials of Medication for the Treatment of CD
• 13 studies, 559 subjects, 9 (8?) positive for medications, 4 (5?) equivocal
• Agents studied: Li, DVPX, Risperidone, Haloperidol, Molindone, Methylphenidate (MPH), CBZ, Vitamins
• Average Duration: 10 weeks, no long-term follow up, few comparative studies, small samples
• BUT antipsychotics are most commonly prescribed (60-80%) for aggression, regardless of diagnosis
Steiner, January 2002
Psychopharmacology of Aggression Effects of Stimulants in ADHD: A Meta-analysis• 28 studies
– Criteria: ADHD, peer reviewed, placebo-controlled, age <18,scaled aggression
• 2 with MR and CD as primary diagnoses each; rest were ADHD; 75% comorbid with ODD,CD
• Average N=24– 88% boys age: 9.7 (7.7-14.4)– MPH in 75% (dose 24 mg/day); duration = 13 days
Connor et al, 2002Connor et al, 2002
Psychopharmacology of Aggression Effects of Stimulants in ADHD• Overt aggression
– Clinician (d = .77)– Parent (d = .57)– Teacher ratings (d = .93) – All significant
• Presence of MR and CD/ODD reduces Effect Size
• AMPH and MPH equally effective (.8); PEM more (1.6)
Connor et al, 2002Connor et al, 2002
• Covert aggression– Clinician (d= .81) significant– Parent (d=.37)– Teacher ratings (d=.54) not significant
(but wide range, only seven studies)
• Drug type did not make a difference, duration and dose weakly contributed
• Overall sample age correlated positively with effect size; no gender effects
Connor et al, 2002Connor et al, 2002
Psychopharmacology of Aggression Effects of Stimulants in ADHD
• Conclusion: Stimulants have significant effects on aggression (especially overt, especially when ADHD is primary diagnosis and not comorbid with CD, MR); and maybe in older subjects
• Limitations– Not all double blind– Short duration– No long term follow-up– Other comorbidities? – PTSD, bipolar Connor et al, 2002Connor et al, 2002
Psychopharmacology of Aggression Effects of Stimulants in ADHD
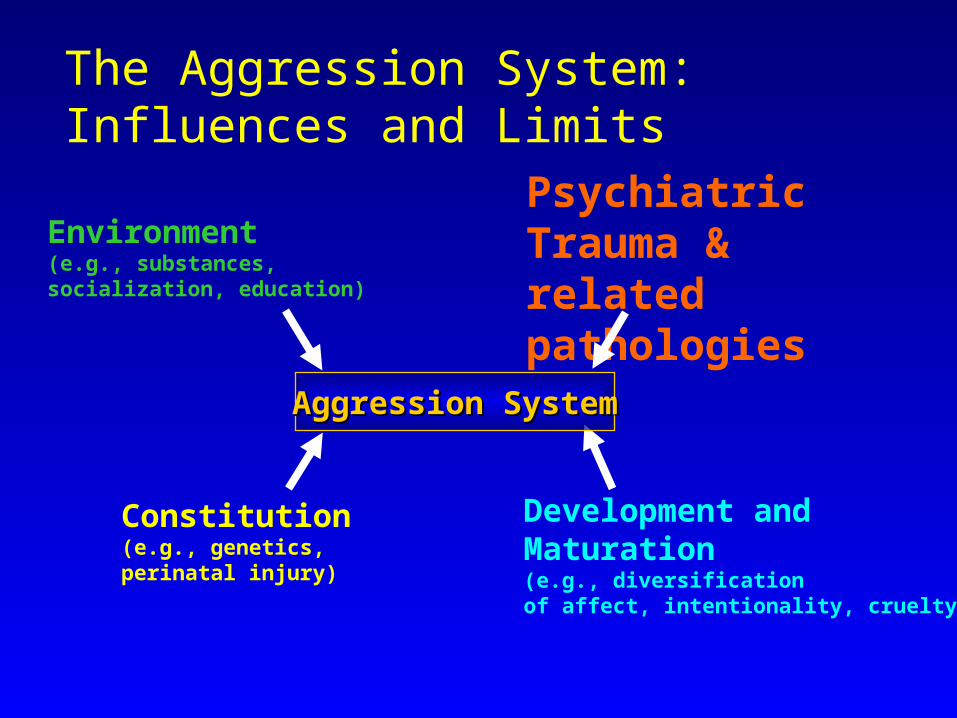
The Aggression System:Influences and Limits
Environment(e.g., substances,socialization, education)
Constitution(e.g., genetics, perinatal injury)
Psychiatric Trauma & related pathologies
Development and Maturation (e.g., diversification of affect, intentionality, cruelty)
Aggression SystemAggression System
Is there reason to think that trauma plays a role in disturbances of aggression?
• Developmental epidemiological studies (Widom, 1989)
• Community violence exposure studies (Osofsky, 1995; Schwab-Stone, 1999)
• Clinical self report studies (Burton et al, 1994)
• Structured interview studies (Steiner et al 1997; Cauffman et al 1998; Steiner et al 2002)
• Transcultural studies (Aichhorn, 1935; Rushkin et al, 2002)
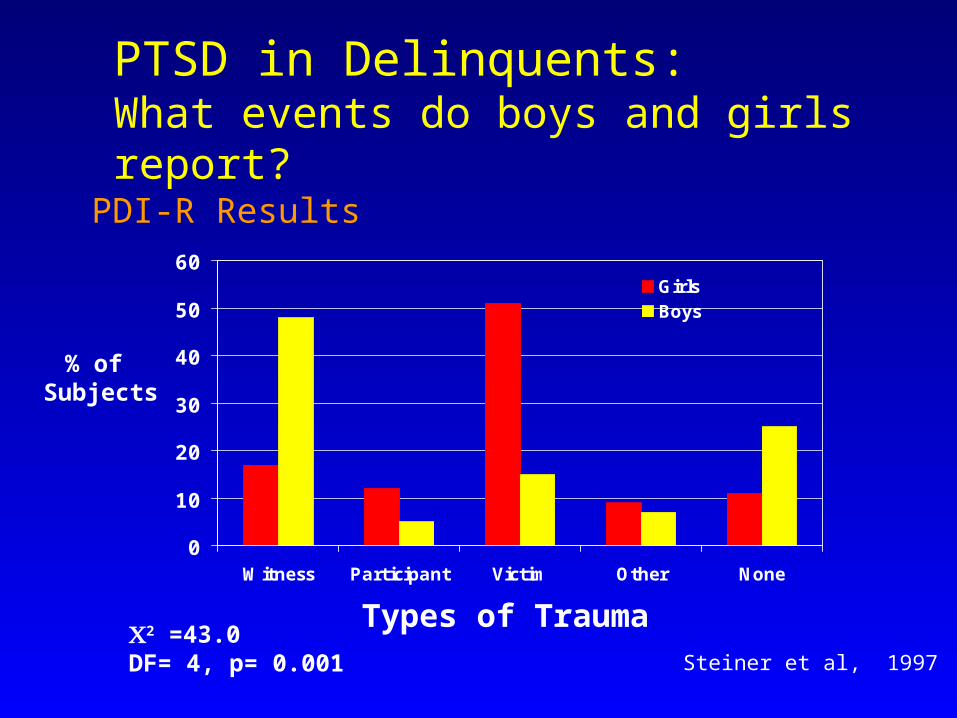
PTSD in Delinquents:What events do boys and girls report?
0
10
20
30
40
50
60
Witness Participant Victim Other None
Girls Boys
2 =43.0DF= 4, p= 0.001
% of Subjects
Types of Trauma
PDI-R Results
Steiner et al, 1997
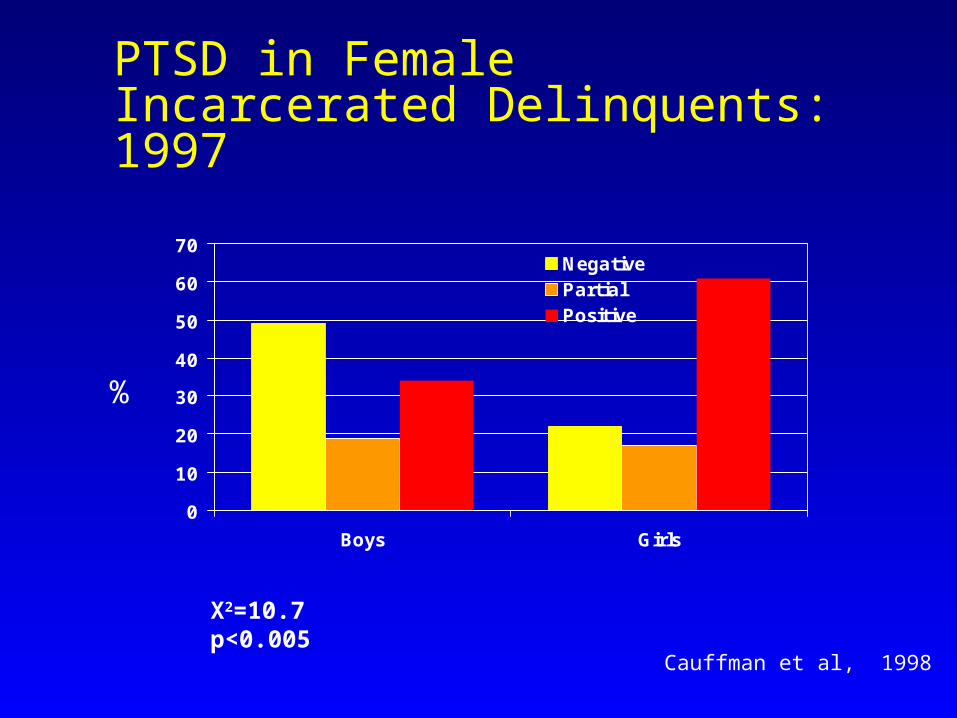
PTSD in Female Incarcerated Delinquents: 1997
0
10
20
30
40
50
60
70
Boys Girls
NegativePartialPositive
X2=10.7p<0.005
%
Cauffman et al, 1998
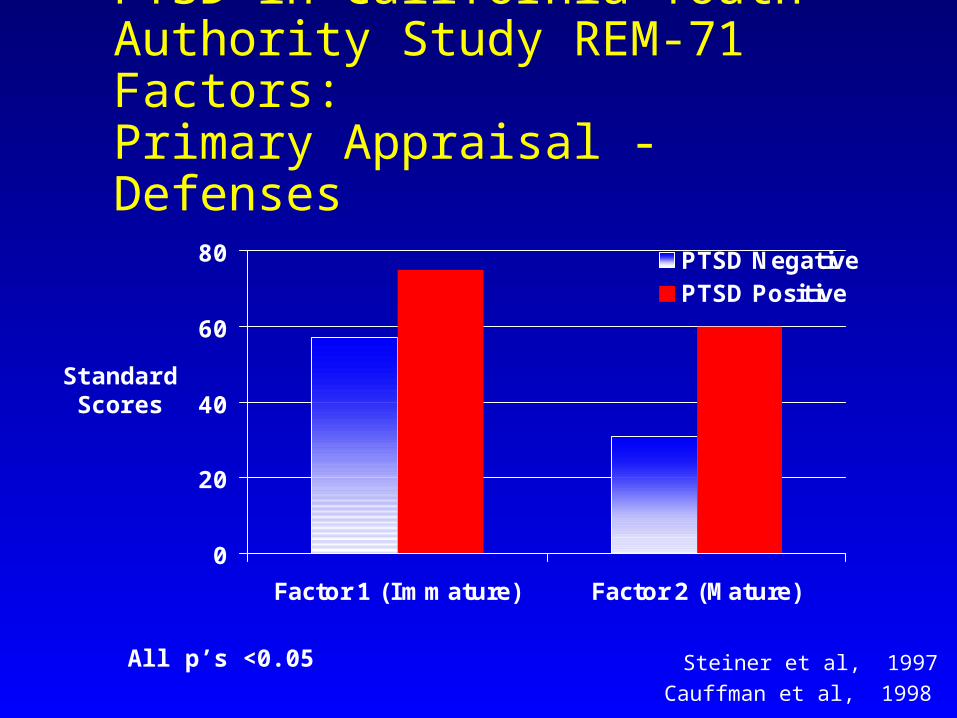
PTSD in California Youth Authority Study REM-71 Factors: Primary Appraisal - Defenses
0
20
40
60
80
Factor 1 (Immature) Factor 2 (Mature)
PTSD NegativePTSD Positive
All p’s <0.05
StandardScores
Steiner et al, 1997Cauffman et al, 1998
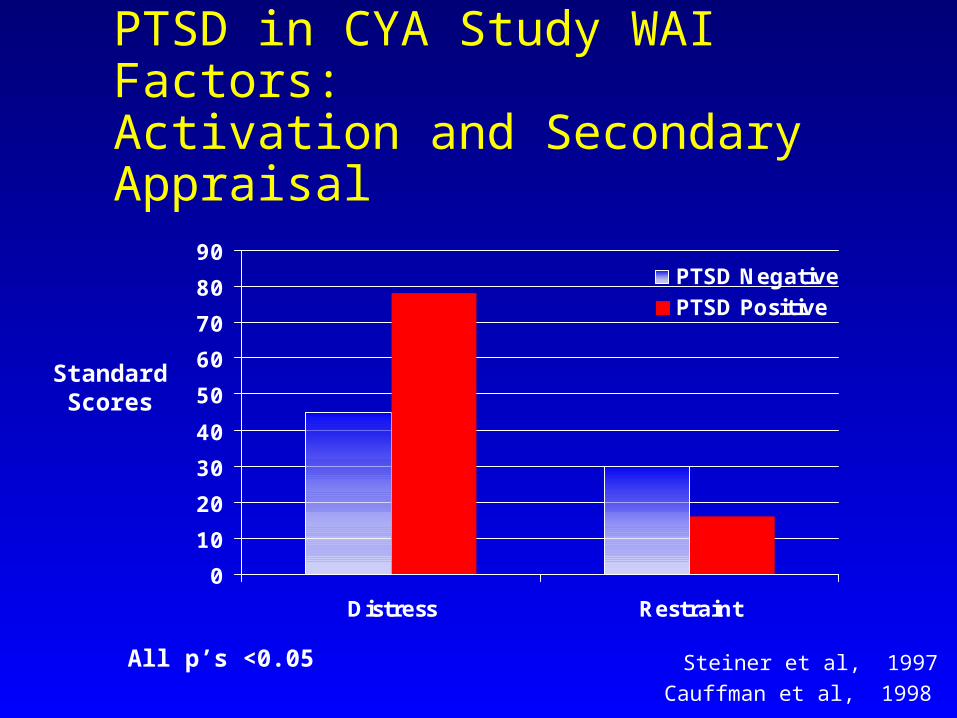
PTSD in CYA Study WAI Factors: Activation and Secondary
Appraisal
0
10
20
30
40
50
60
70
80
90
Distress Restraint
PTSD NegativePTSD Positive
StandardScores
Steiner et al, 1997All p’s <0.05Cauffman et al, 1998
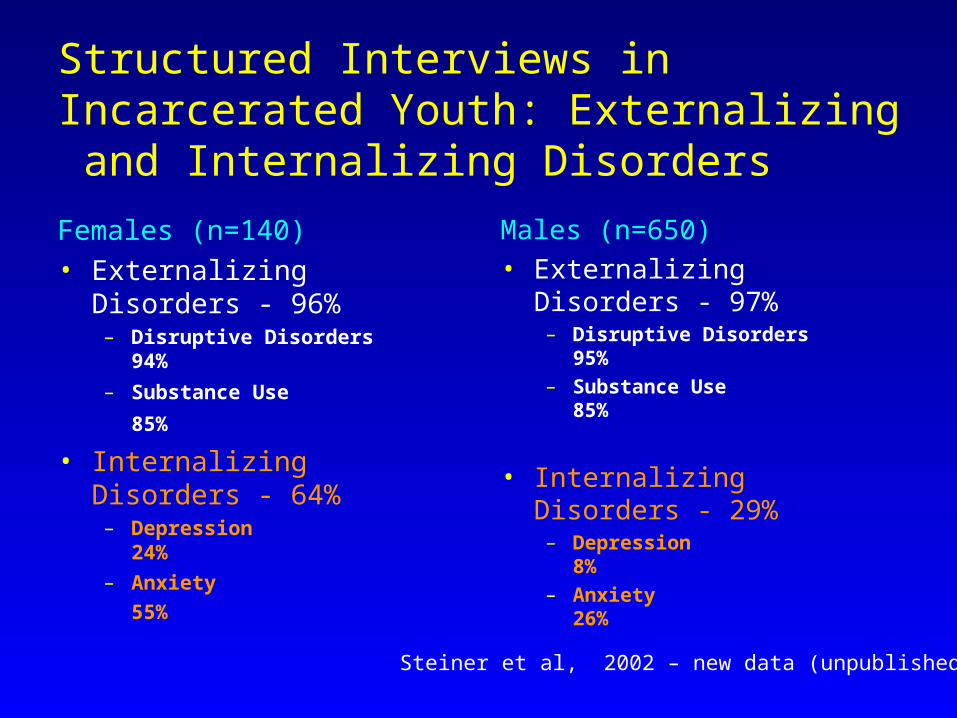
Structured Interviews in Incarcerated Youth: Externalizing and Internalizing Disorders
Females (n=140)• Externalizing
Disorders - 96%– Disruptive Disorders
94%
– Substance Use
85%
• Internalizing Disorders - 64%– Depression
24%– Anxiety
55%
Males (n=650) • Externalizing
Disorders - 97%– Disruptive Disorders
95%– Substance Use
85%
• Internalizing Disorders - 29%– Depression
8%– Anxiety
26%Steiner et al, 2002 – new data (unpublished)
Components of the Aggression System Which Should Be Affected by Trauma
• Primary Appraisal: Defenses – YES – Feldman, Araujo & Steiner, 1996; Steiner, Garcia and Matthews, 1997
• Affective Activation: Anxiety and Aggression often go together – YES- Steiner, Garcia and Matthews, 1997; Cauffman et al, 1998; NEW DATA
• Secondary Appraisal: Restraint, Impulse control is impaired as a function of trauma– YES
This profile leads to reactive/affective/defensive (RAD) aggressionThis profile leads to reactive/affective/defensive (RAD) aggressionSteiner et al, 2002 – new data (unpublished)
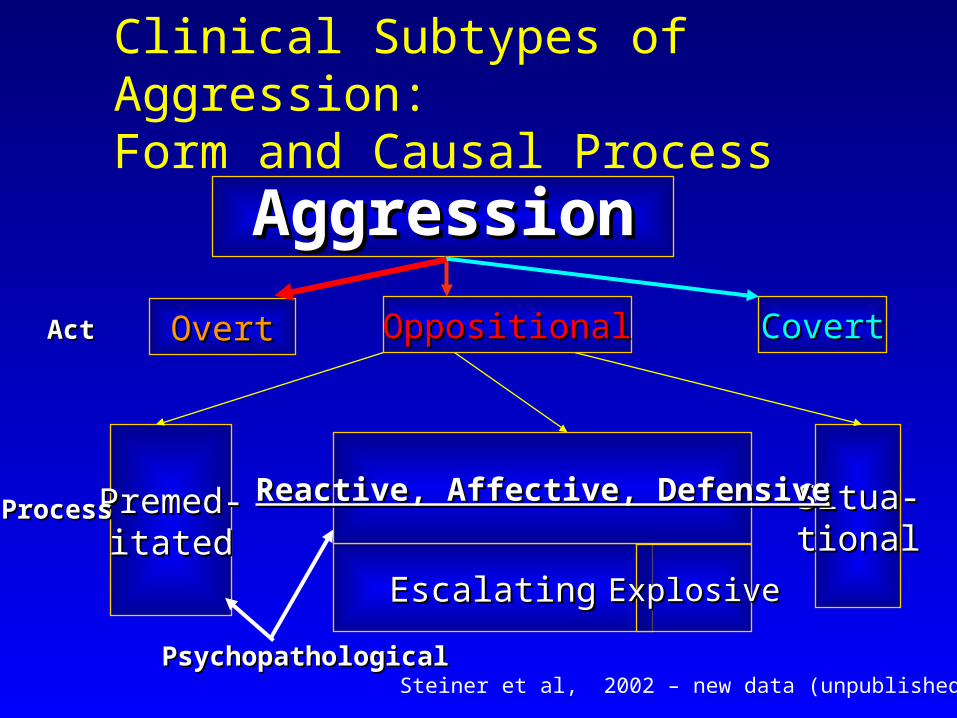
Clinical Subtypes of Aggression: Form and Causal Process
AggressionAggression
Premed-Premed-itateditated
EscalatingEscalating ExplosiveExplosive
Situa-Situa-tionaltional
OppositionalOppositional CovertCovert
Reactive, Affective, DefensiveReactive, Affective, Defensive
PsychopathologicalPsychopathological
OvertOvertActAct
ProcessProcess
Steiner et al, 2002 – new data (unpublished)
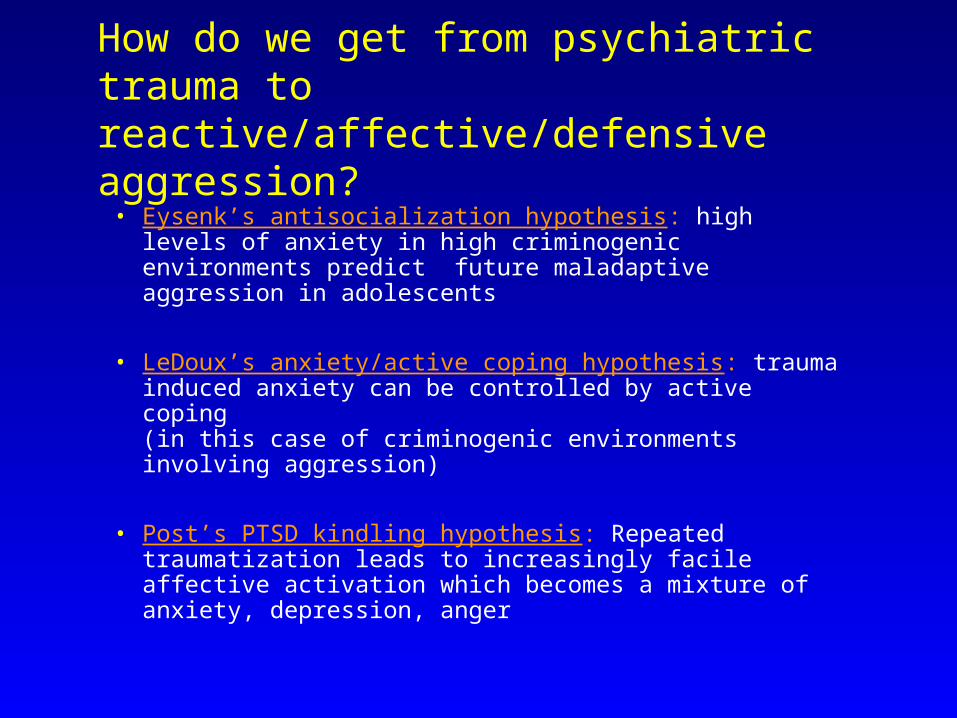
How do we get from psychiatric trauma to reactive/affective/defensive aggression?• Eysenk’s antisocialization hypothesis: high levels of
anxiety in high criminogenic environments predict future maladaptive aggression in adolescents
• LeDoux’s anxiety/active coping hypothesis: trauma induced anxiety can be controlled by active coping (in this case of criminogenic environments involving aggression)
• Post’s PTSD kindling hypothesis: Repeated traumatization leads to increasingly facile affective activation which becomes a mixture of anxiety, depression, anger
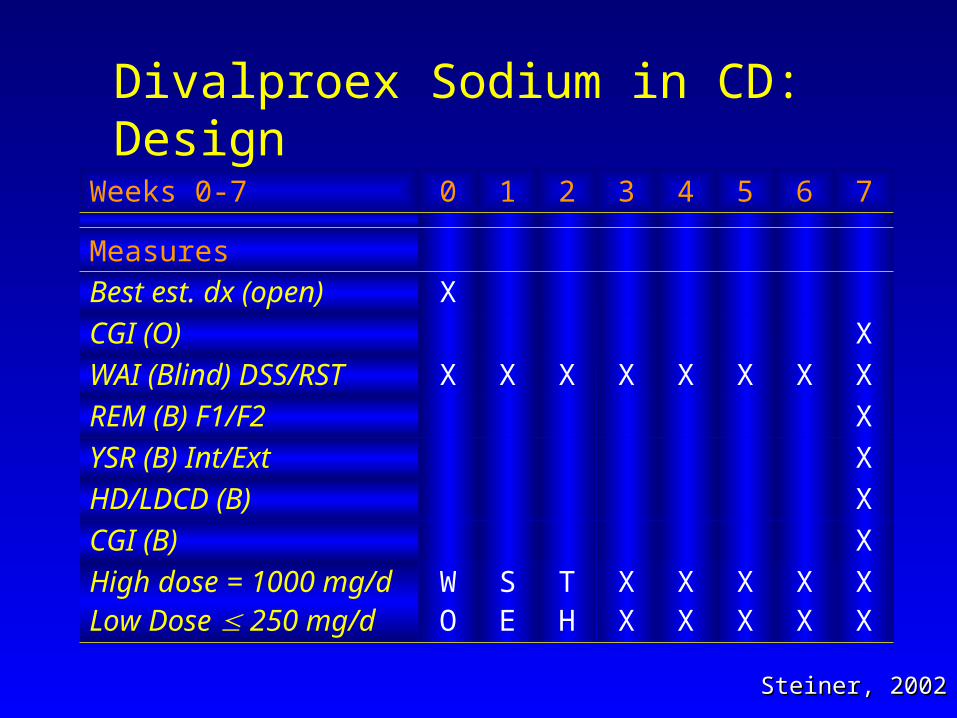
Divalproex Sodium in CD: Design
Weeks 0-7 0 1 2 3 4 5 6 7
MeasuresBest est. dx (open) X
CGI (O) X
WAI (Blind) DSS/RST X X X X X X X XREM (B) F1/F2 X
YSR (B) Int/Ext X
HD/LDCD (B) X
CGI (B) X
High dose = 1000 mg/dLow Dose 250 mg/d
WO
SE
TH
XX
XX
XX
XX
XX
Steiner, 2002Steiner, 2002
Divalproex Sodium for the Treatment of Severe CD in Boys
• Low ( 125 mg) and high dose (1000 mg) 7-week DBPC clinical trial
• Sample: 70 boys consented, 61 completed 3 month protocol (7 weeks on medication); 58 had all outcome measures
• Multi-method, Multi-trait measures
• CGI-I Intent-to-treat: 35% responded (53% in high dose vs. 8% in low dose condition)
• Significant differences in self rated slopes of weekly restraint
• No significant side effects (drowsiness, GI upset), easily tolerated
Steiner, 2002Steiner, 2002
Different Patterns of Aggression Respond to Divalproex Sodium• 61 adolescent males into predominantly High Distress
(HDCD) and Low Distress (LDCD) Conduct Disorders
• Low distress CD show predominantly premeditated aggression; High Distress CD are predominantly RAD aggressive.
• In a 7 week RDBPC trial of DVPX we found that the HDCD had a more robust response to therapeutic doses of DVPX Sodium
• Responsive targets were: observer rated CGI, weekly slopes of self reported Distress (decreased) and Restraint (increased)
New Poster APA, 2002New Poster APA, 2002
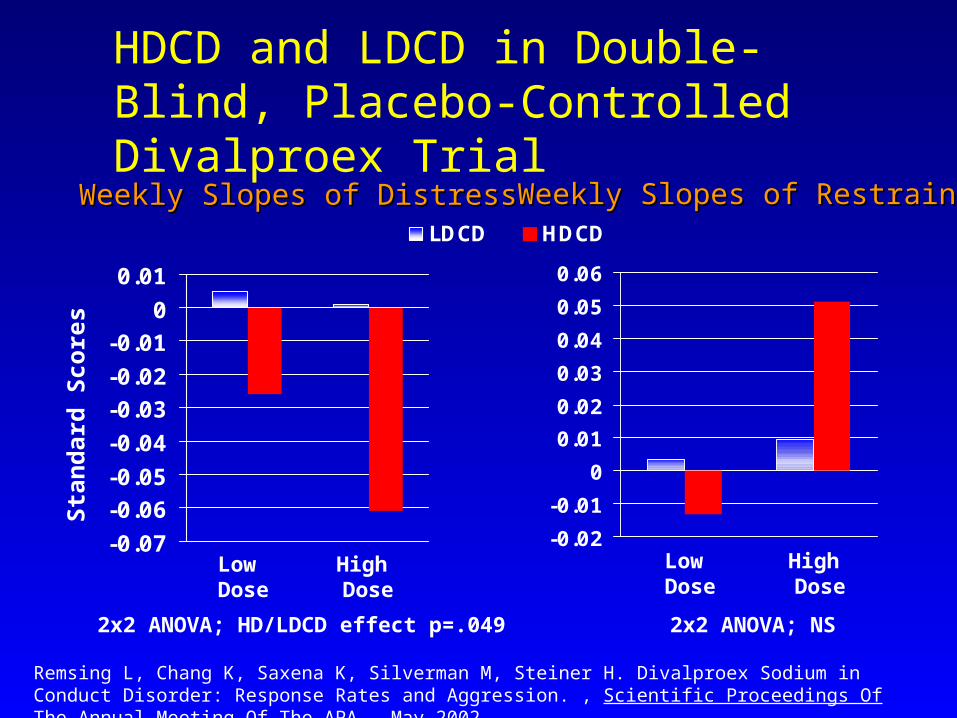
HDCD and LDCD in Double-Blind, Placebo-Controlled Divalproex Trial
-0.07
-0.06-0.05
-0.04
-0.03-0.02
-0.010
0.01
LDCD HDCD
2x2 ANOVA; HD/LDCD effect p=.049
Sta
nd
ard
Score
s
Low Dose
High Dose
Weekly Slopes of DistressWeekly Slopes of Distress Weekly Slopes of RestraintWeekly Slopes of Restraint
2x2 ANOVA; NS
-0.02
-0.01
0
0.01
0.02
0.03
0.04
0.05
0.06
Low Dose
High Dose
Remsing L, Chang K, Saxena K, Silverman M, Steiner H. Divalproex Sodium in Conduct Disorder: Response Rates and Aggression. , Scientific Proceedings Of The Annual Meeting Of The APA, May 2002
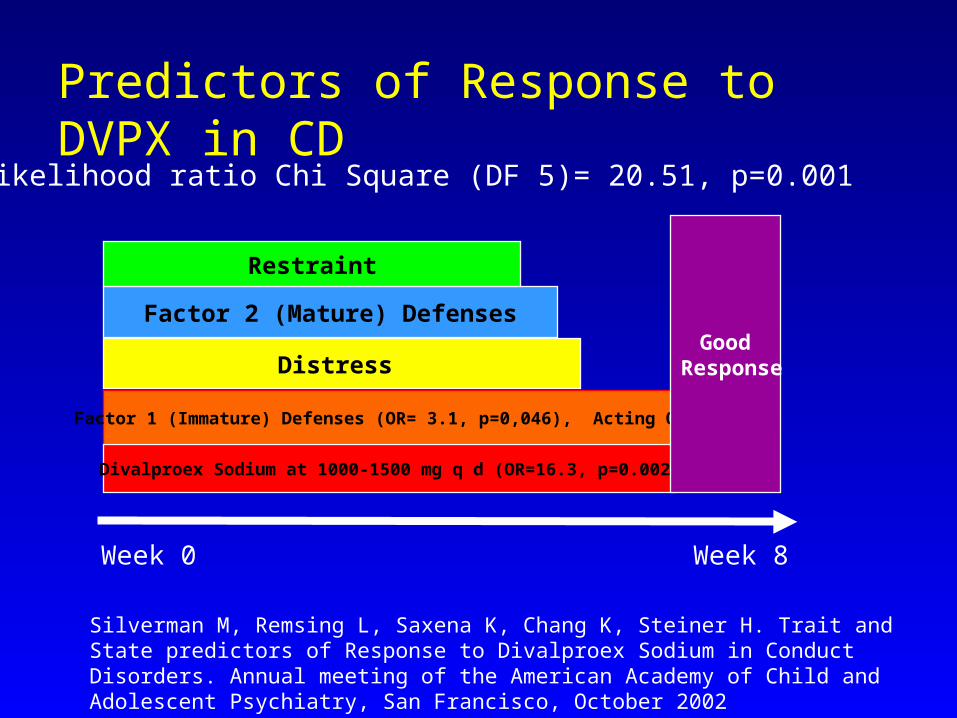
Predictors of Response to DVPX in CD
Week 0 Week 8
Distress
Factor 2 (Mature) Defenses
Restraint
Likelihood ratio Chi Square (DF 5)= 20.51, p=0.001
Factor 1 (Immature) Defenses (OR= 3.1, p=0,046), Acting Out!
Divalproex Sodium at 1000-1500 mg q d (OR=16.3, p=0.002)
Good Response
Silverman M, Remsing L, Saxena K, Chang K, Steiner H. Trait and State predictors of Response to Divalproex Sodium in Conduct Disorders. Annual meeting of the American Academy of Child and Adolescent Psychiatry, San Francisco, October 2002
Divalproex in PTSD: The Sample• 12 boys • Ages 14-17, mean 15.9 (SD=0.9)• Highly comorbid:
– Conduct disorder (12)– Mood Disorder (8)– ADHD (6)
• Average number of diagnoses: 4.8 (SD=1.2)
Silverman M, Carrion V, Chang K, Matthews Z, Peterson M, Steiner H : Divalproex Sodium and PTSD Treatment: A Randomized Controlled Clinical Trial, Scientific Proceedings Of The Annual Meeting Of The American Academy Of Child And Adolescent Psychiatry, 17: 115, 2001
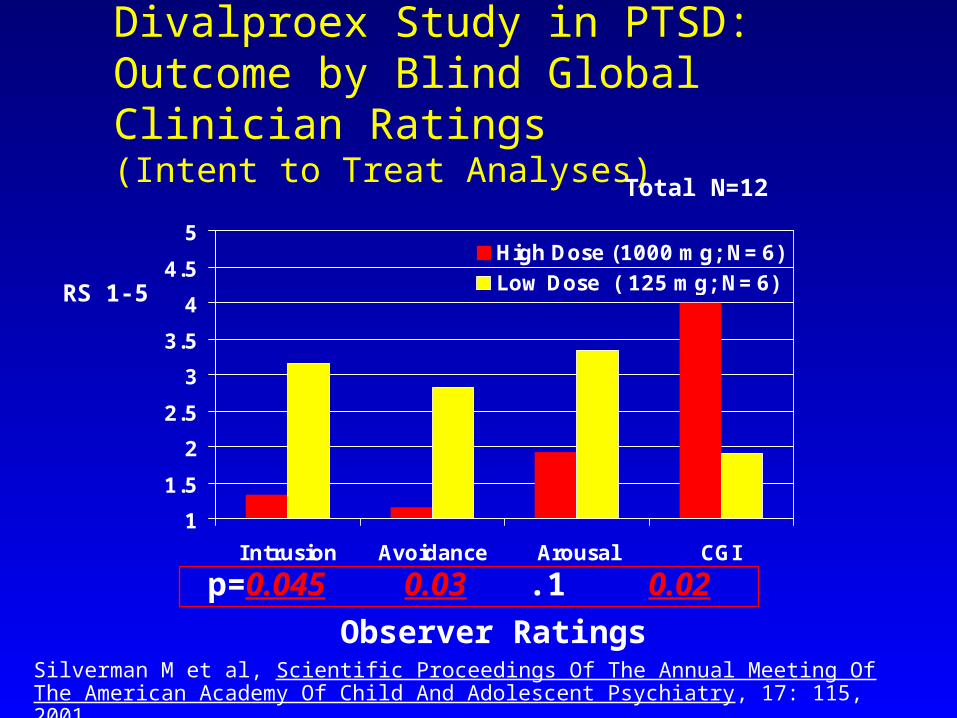
Divalproex Study in PTSD: Outcome by Blind Global Clinician Ratings (Intent to Treat Analyses)
1
1.5
2
2.5
3
3.5
4
4.5
5
Intrusion Avoidance Arousal CGI
High Dose (1000 mg; N=6)Low Dose ( 125 mg; N=6)RS 1-5
p= 0.045 0.03 .1 0.02
Total N=12
Observer RatingsSilverman M et al, Scientific Proceedings Of The Annual Meeting Of The American Academy Of Child And Adolescent Psychiatry, 17: 115, 2001
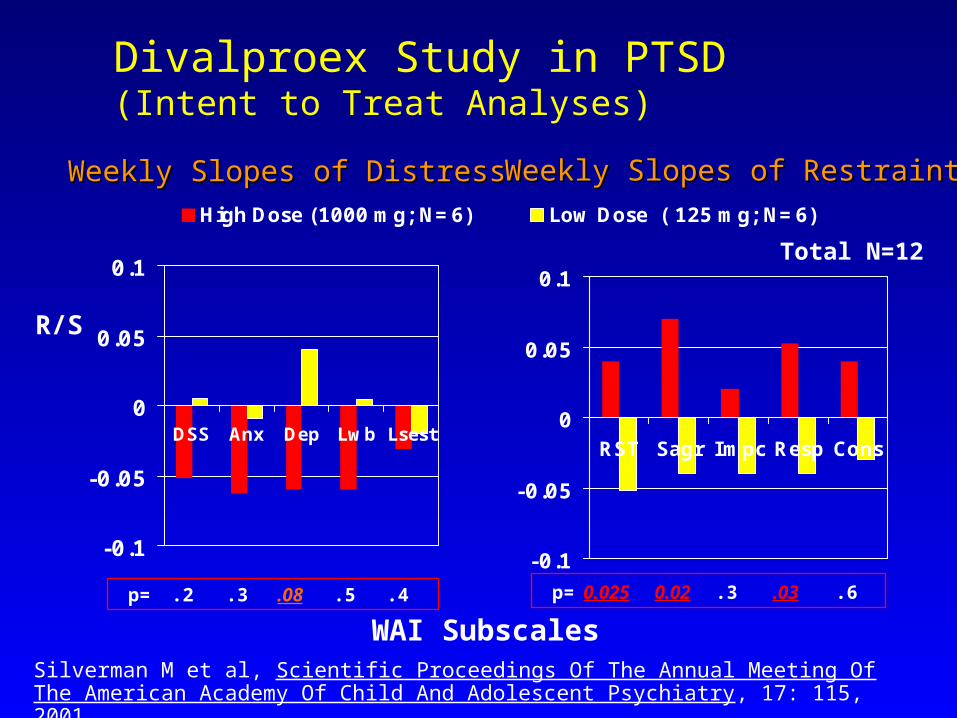
Divalproex Study in PTSD(Intent to Treat Analyses)
-0.1
-0.05
0
0.05
0.1
DSS Anx Dep Lwb Lsest
High Dose (1000 mg; N=6) Low Dose ( 125 mg; N=6)
p= .2 .3 .08 .5 .4
WAI Subscales
R/S
Total N=12
Weekly Slopes of DistressWeekly Slopes of Distress Weekly Slopes of RestraintWeekly Slopes of Restraint
-0.1
-0.05
0
0.05
0.1
RST Sagr Impc Resp Cons
p=0.025 0.02 .3 .03 .6
Silverman M et al, Scientific Proceedings Of The Annual Meeting Of The American Academy Of Child And Adolescent Psychiatry, 17: 115, 2001
Implications of DBPC trials in CD 2002Emerging Pathways
• Lithium may be most applicable in prepubertal aggression with a reactive/affective/defensive profile
• Divalproex may be most useful in pubertal CD with a high affective component either to mood disorder or trauma – especially chronic trauma
• Antipsychotics (risperidone; haloperidol; may be most helpful when executive cognitive functions are impaired (MR, PDD, psychosis)
• Stimulants should be considered when there is a comorbid attention deficit (caveat – juvenile bipolar)
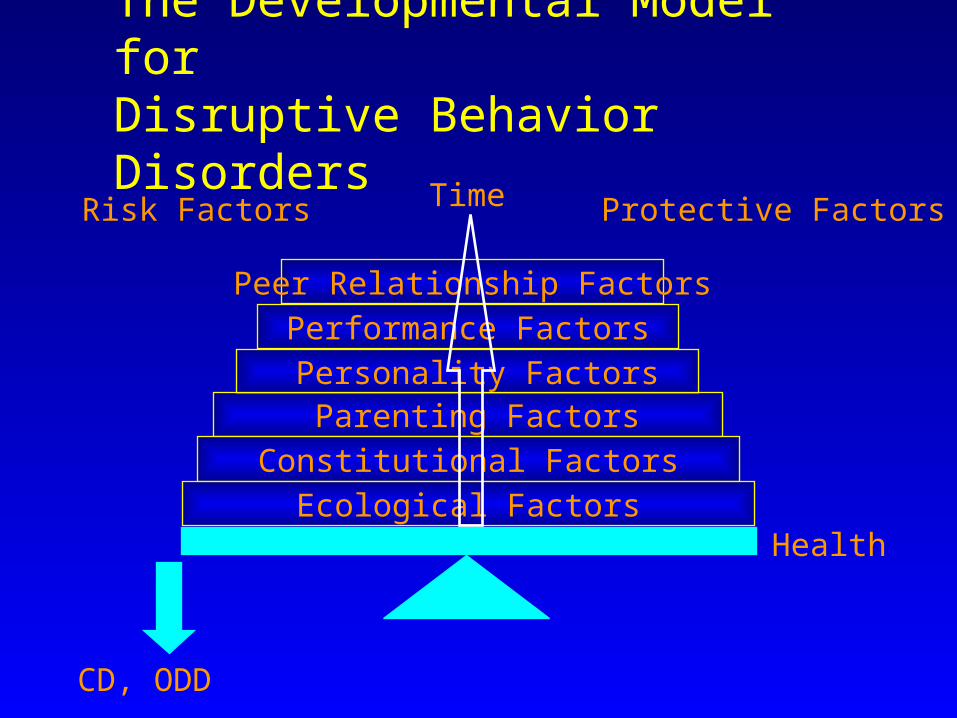
The Developmental Model for
Disruptive Behavior Disorders
Peer Relationship FactorsPerformance Factors Personality Factors Parenting Factors
Constitutional FactorsEcological Factors
TimeRisk Factors Protective Factors
CD, ODD
Health
Observing Infants’ Aggression at 1 Year: Teen Mothers’ and Researchers’ Reports
• Sample of 60 teen mothers at high risk , predominantly Hispanic, 33 boys and 28 girls followed from pre-birth, assessment at 13 months
• Variables: maternal psychopathology, CAPI, PSI; Reported infant aggression, negative emotional reactivity and emotion regulation; Same infant variables observed
• Experimental tasks: strange situation, Bailey testing
Gschwendt, Zelenko & Steiner, 2002Gschwendt, Zelenko & Steiner, 2002
Observing Infants’ Aggression at 1 year: Results
• In infants, negative affective reactivity, emotion regulation and aggression were significantly correlated by mother’s and observer’s reports, separately (Spearman’s 0.47 to - .81, p’s < 0.05)
• Maternal depression, anxiety, CAPI and PSI correlated with mother’s reports of infant aggression, negative affective reactivity (Spearman’s 0.22 to 0.47, p’s <0.05) in infants
• Mother’s reports correlated with observer ratings only if their own functioning was taken into account
Gschwendt, Zelenko & Steiner, 2002Gschwendt, Zelenko & Steiner, 2002
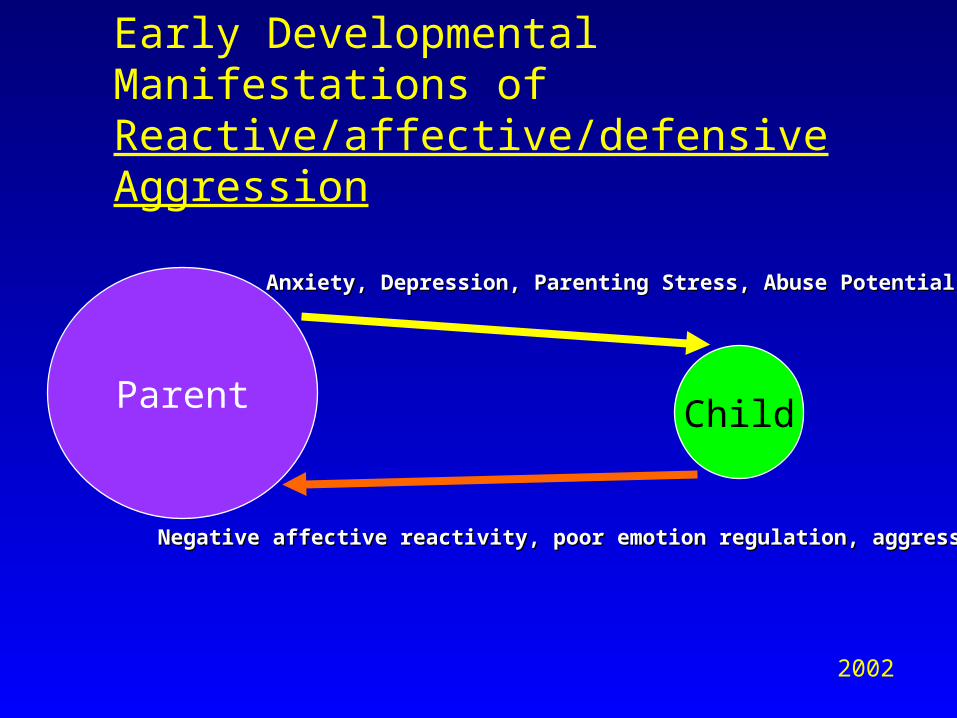
Early Developmental Manifestations of Reactive/affective/defensive Aggression
Parent Child
Anxiety, Depression, Parenting Stress, Abuse PotentialAnxiety, Depression, Parenting Stress, Abuse Potential
Negative affective reactivity, poor emotion regulation, aggressionNegative affective reactivity, poor emotion regulation, aggression
2002
Trauma and Reactive/Affective/Defensive (RAD) Aggression – Summary APA 2002• Traumatic Events are extremely common in the lives of maladaptively
aggressive (MAA) youth
• PTSD is extremely common in MAA youth
• PTSD leads to faulty primary appraisal, anxious/angry activation and loss of self restraint – reactive/affective/defensive aggression – kindling
• Treatment with DVPX is effective in CD, even more effective in CD and PTSD
• Antikindling treatment seems to treat reactive/affective/defensive aggression; good response is predicted by variables related to PTSD at baseline
• Early antecedents of reactive/affective/defensive aggression involve negative affect/ poor emotion regulation and aggression in the infant (by both observer and mothers’ reports and increased attribution of negative characteristics by the mother as a function of her anxiety and depression
Recommended