Global Conference
Adult Medicine PRN and Ambulatory Care PRN Focus Session—Transitions of Care Management: Best Practices Activity Number: 0217-0000-15-136-L01-P, 1.50 hours of CPE credit; Activity Type: An Application-Based Activity
Tuesday, October 20, 2015 1:30 p.m. to 3:00 p.m. Continental Ballroom 4
Moderator: Sarah L. Anderson, Pharm.D., BCPS Assistant Professor, University of Colorado Anschutz Medical Campus, Skaggs School of Pharmacy & Pharmaceutical Sciences, Aurora, Colorado
Agenda
1:30 p.m. Begin with the End in Mind: Best Practices for Transitions of Care Performed by Inpatient Pharmacists Zachary Lane Cox, Pharm.D., BCPS Associate Professor, Lipscomb University College of Pharmacy, Nashville, Tennessee; Heart Failure Clinical Pharmacist, Vanderbilt University Medical Center, Nashville, Tennessee
2:00 p.m. Hold On, We’re Going Home: Best Practices for Transitions of Care Performed by Ambulatory Care Pharmacists Julianna L. Burton, Pharm.D., BCPS, BCACP, FCSHP Assistant Chief of Pharmacy, Director of PGY2 Ambulatory Care, Pharmacy Department, UC Davis Medical Center, Sacramento, California
2:30 p.m. Lessons from the Trenches: Expanding Transition of Care Services Through Expansion of Student and Resident Roles Julianna L. Burton, Pharm.D., BCPS, BCACP, FCSHP Assistant Chief of Pharmacy, Director of PGY2 Ambulatory Care, Pharmacy Department, UC Davis Medical Center, Sacramento, California
Zachary Lane Cox, Pharm.D., BCPS Associate Professor, Lipscomb University College of Pharmacy, Nashville, Tennessee; Heart Failure Clinical Pharmacist, Vanderbilt University Medical Center, Nashville, Tennessee
Conflict of Interest Disclosures Sarah L. Anderson: no conflicts to disclose. Julianna L. Burton: no conflicts to disclose. Zachary Lane Cox: Received grant funding from Otsuka Pharmaceuticals and Cumberland Pharmaceuticals.
© American College of Clinical Pharmacy 1
Global Conference
Learning Objectives
1. Develop strategies to incorporate transitions of care medication reconciliation and patient education into inpatient pharmacist workflow.
2. Apply existing quality metrics endorsed by healthcare quality sponsoring organizations to track and measure the impact of care transitions in the inpatient care setting.
3. Evaluate established inpatient-focused care transition models. 4. Develop strategies to incorporate transitions of care medication reconciliation and patient education
into ambulatory care pharmacist workflow. 5. Apply existing quality metrics endorsed by healthcare quality sponsoring organizations to track and
measure the impact of care transitions in the ambulatory care setting. 6. Evaluate established ambulatory care-focused care transition models. 7. Identify successes and challenges encountered when integrating students and residents into transitions
of care services. 8. Describe a student-driven medication reconciliation process. 9. Given a case scenario, determine how to incorporate a learner into the transition of care process.
Self-Assessment Questions
Self-assessment questions are available online at www.accp.com/gc15.
© American College of Clinical Pharmacy 2
Begin with the end in mind: Best practices for transitions of care performed by inpatient pharmacists
Zachary Cox, PharmD, BCPSOctober 20, 2015
2015 ACCP Global Conference on Clinical Pharmacy
Conflict of Interests
Research funding from OtsukaPharmaceuticals
Learning Objectives
Evaluate established inpatient-focused caretransition models
Apply existing quality metrics endorsed byhealthcare quality sponsoring organizationsto track and measure the impact of caretransitions in the inpatient care setting
Develop strategies to incorporate transitionsof care medication reconciliation and patienteducation into inpatient pharmacist workflow
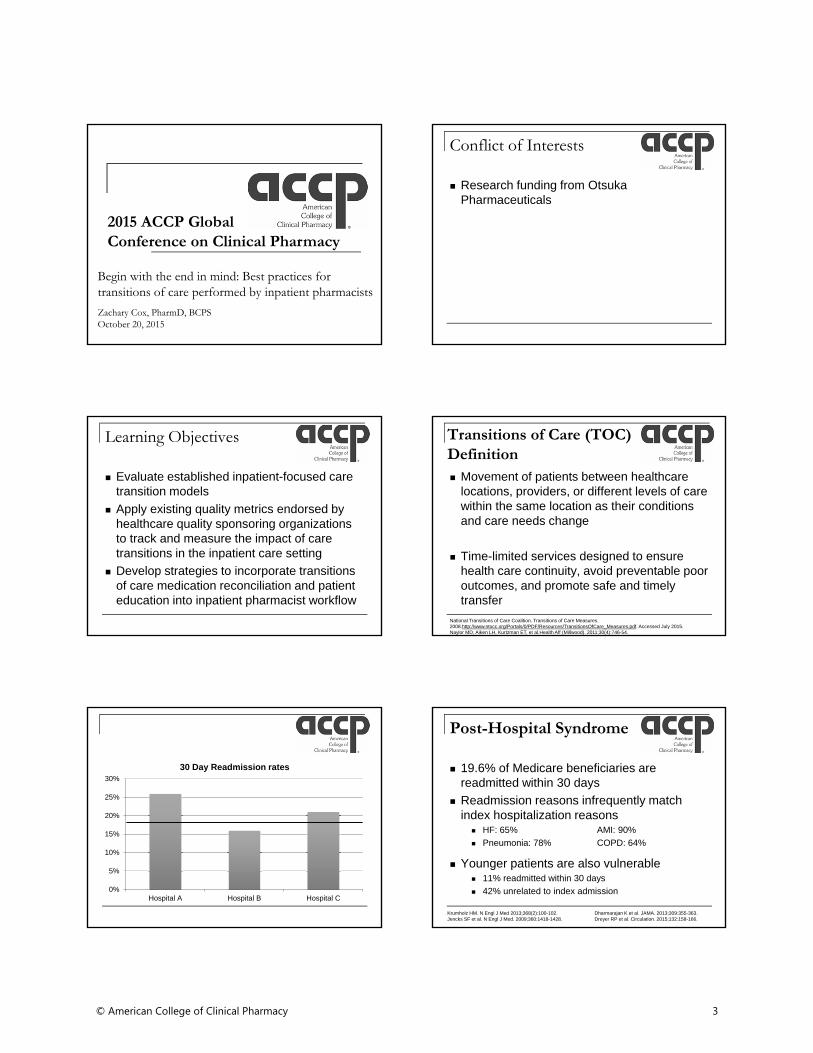
Transitions of Care (TOC) Definition Movement of patients between healthcare
locations, providers, or different levels of care within the same location as their conditions and care needs change
Time-limited services designed to ensurehealth care continuity, avoid preventable pooroutcomes, and promote safe and timelytransfer
National Transitions of Care Coalition. Transitions of Care Measures. 2008.http://www.ntocc.org/Portals/0/PDF/Resources/TransitionsOfCare_Measures.pdf. Accessed July 2015. Naylor MD, Aiken LH, Kurtzman ET, et al.Health Aff (Millwood). 2011;30(4):746-54.
0%
5%
10%
15%
20%
25%
30%
Hospital A Hospital B Hospital C
30 Day Readmission rates
Post-Hospital Syndrome
19.6% of Medicare beneficiaries arereadmitted within 30 days
Readmission reasons infrequently matchindex hospitalization reasons
HF: 65% AMI: 90%
Pneumonia: 78% COPD: 64%
Younger patients are also vulnerable 11% readmitted within 30 days
42% unrelated to index admission
Krumholz HM. N Engl J Med 2013;368(2):100-102. Dharmarajan K et al. JAMA. 2013;309:355-363.Jencks SF et al. N Engl J Med. 2009;360:1418-1428. Dreyer RP et al. Circulation. 2015;132:158-166.
© American College of Clinical Pharmacy 3
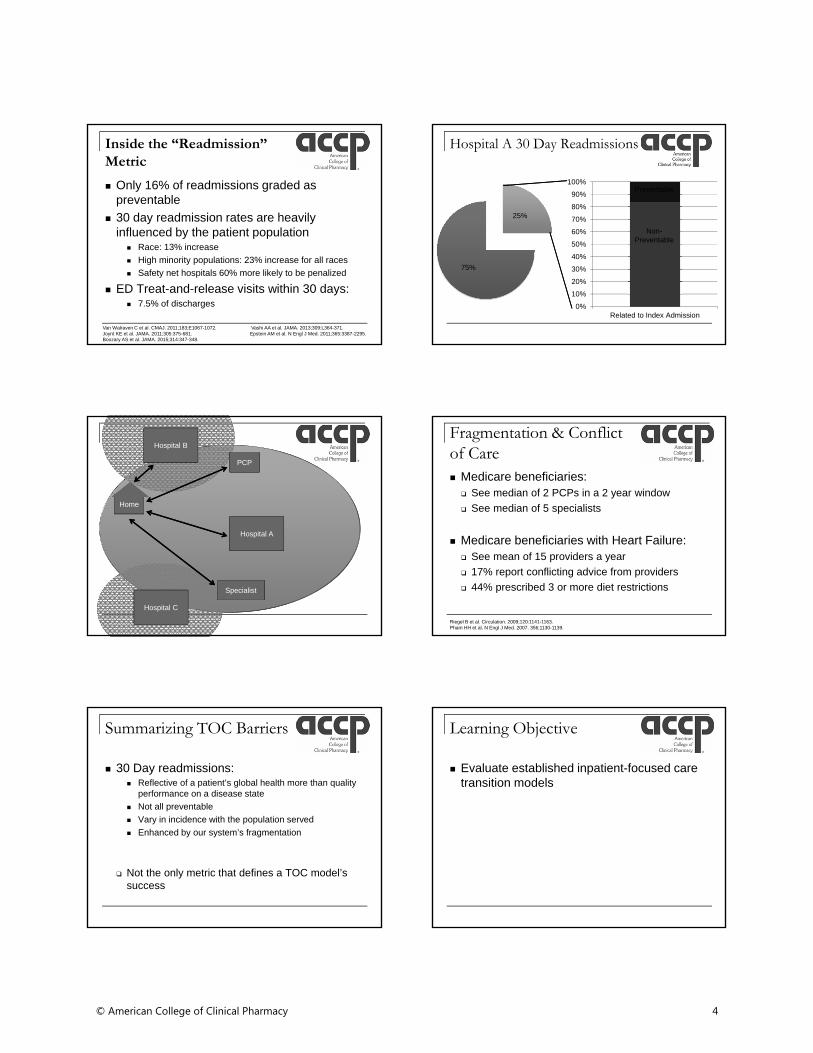
Inside the “Readmission” Metric
Only 16% of readmissions graded aspreventable
30 day readmission rates are heavilyinfluenced by the patient population
Race: 13% increase
High minority populations: 23% increase for all races
Safety net hospitals 60% more likely to be penalized
ED Treat-and-release visits within 30 days: 7.5% of discharges
Van Walraven C et al. CMAJ. 2011;183;E1067-1072. Vashi AA et al. JAMA. 2013;309:L364-371.Joynt KE et al. JAMA. 2011;305:375-681. Epstein AM et al. N Engl J Med. 2011;365:3387-2295.Boozary AS et al. JAMA. 2015;314:347-348.
Hospital A 30 Day Readmissions
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Related to Index Admission
25%
75%
Non-Preventable
Preventable
Hospital A
Home
Hospital B
Hospital C
PCP
Specialist
Fragmentation & Conflict of Care Medicare beneficiaries: See median of 2 PCPs in a 2 year window
See median of 5 specialists
Medicare beneficiaries with Heart Failure: See mean of 15 providers a year
17% report conflicting advice from providers
44% prescribed 3 or more diet restrictions
Riegel B et al. Circulation. 2009;120:1141-1163.Pham HH et al. N Engl J Med. 2007. 356;1130-1139.
Summarizing TOC Barriers
30 Day readmissions: Reflective of a patient’s global health more than quality
performance on a disease state
Not all preventable
Vary in incidence with the population served
Enhanced by our system’s fragmentation
Not the only metric that defines a TOC model’ssuccess
Learning Objective
Evaluate established inpatient-focused caretransition models
© American College of Clinical Pharmacy 4
Audience Response
Which TOC model is validated in multiplehospitals/populations in rigorous, outcome-based trials?
Coleman Care Transitions
Project RED
PROJECT BOOST
Rennke S, et al. Ann Intern Med. 2013;158:433-440.Herner SJ et al. PSAP Transitions of Care. 2014. Chronic Illness. Book 2:79-97.
Components of TOC Models
1. Secure institutional support
2. Define multidisciplinary team Engage key community stakeholders outside institution
3. Develop specific goals Define metrics of success for each goal
4. Collect baseline data of current performance Root cause analysis
5. Create intervention
Project BOOST Implementation Guide to Improve Care Transitions. First Edition. 2008. http://www.hospitalmedicine.org/Web/Quality_Innovation/Implementation_Toolkits/Project_BOOST/Web/Quality___Innovation/Implementation_Toolkit/Boost/First_Steps/Implementation_Guide.aspx. Accessed July 2015.
Readmission Root Cause Analysis
“It is clear that there are multiple factors along the care continuum that impact readmissions, and identifying the
key drivers of readmissions for a hospital and its downstream providers is the first step towards
implementing the appropriate interventions necessary for reducing readmissions.”
Interview all 30 day readmissions for 1 month
Quantify and characterize precipitationfactors in an institution’s population
CMS Community-Based Care Transition Program. http://innovation.cms.gov/initiatives/CCTP/. Accessed July 2015.CMS Community-Based Care Transition Program. http://innovation.cms.gov/resources/CCTP_HowtoApply.html. Accessed July 2015.
Components of TOC Models
1. Education on medication and self-care skills
2. Early post-discharge patient communication1. Schedule Follow up appointments and tests
2. Phone call
3. Identification of and action for “Red Flag”symptoms
4. Quick and complete written communicationwith outpatient providers
Paper ≠ Education
Written and Verbal discharge instructions ~50% of all instructions are able to be recalled or
understood 14-50% understood self care instructions
~1/3 could not name 1 symptom of an acute exacerbation
~1/3 take all medications as instructed
64% - 73% can identify a new medication after discharge
Moser DK et al. Am Heart J. 2005;150:984.e7-e13. Maniaci MJ et al. Mayo Clin Proc. 2008;83:554-558.J Gen Intern Med. 2014;29:1491-1498. Schillinger D et al. Arch Intern Med. 2003;163:83-90.
Teach-back Assessment
Patient teaches concept back
Re-education of
misconceptions
Re-assessment of Understanding
Education of new concept
Schillinger D et al. Arch Intern Med. 2003;163:83-90.
© American College of Clinical Pharmacy 5
Customization of TOC Models
Root Cause Analysis Disease state prevalence
Population served Resources
Socioeconomic limitations
Education barriers
Institutional system
Learning Objective
Apply existing quality metrics endorsed byhealthcare quality sponsoring organizationsto track and measure the impact of caretransitions in the inpatient care setting
How do you measure TOC success?
Developing Institutional Metrics Outcome
Are you accomplishing your goal?
Process Measure how well the new process is functioning
Structure Measures staff/materials required for process
Balancing Measures new process’ impact on other processes
Donabedian A. Evaluating the quality of medical care. Milbank Mem Fund Q. 1966;44:Suppl:166-206.
National Standards
JC National Patient Safety Goal 03.06.01 D/C medication reconciliation, education, &
communication
CTM-3 My preferences were considered in my post-D/C health
care needs
I understood my responsibilities post-D/C in my care
I understood the purpose of each medication post-D/C
http://www.jointcommission.org/assets/1/6/2015_NPSG_HAP.pdf. Accessed July 2015.http://www.hcahpsonline.org/files/HCAHPS%20V10.0%20Appendix%20A%20-%20HCAHPS%20Mail%20Survey%20Materials%20(English)%20March%202015.pdf. Accessed July 2015.
National Standards
Physician Consortium for PerformanceImprovement
1. Medication List at Discharge New, Continued, Discontinued, & Allergies/Adverse Reactions
2. Transition Record for the Patient
3. Transmission of Transition Record within 24 hours
National Transitions of Care Coalition Framework for Measuring TOC
http://www.ntocc.org/Portals/0/PDF/Resources/TransitionsOfCare_Measures.pdf. Accessed July 2015.http://www.ama-assn.org/ama/pub/physician-resources/physician-consortium-performance-improvement/pcpi-measures.page. Accessed July 2015.
Developing TOC Goals
Define baseline performance Process mapping
Patient discharge knowledge assessment tool
SMART Goals
Establish Data Collection Methods
SpecificMeasurableAchievableRealisticTime defined
Project BOOST. First http://www.hospitalmedicine.org/Web/Quality___Innovation/Implementation_Toolkit/Boost/Home/Project_Team.aspx.
Accessed July 2015.
© American College of Clinical Pharmacy 6
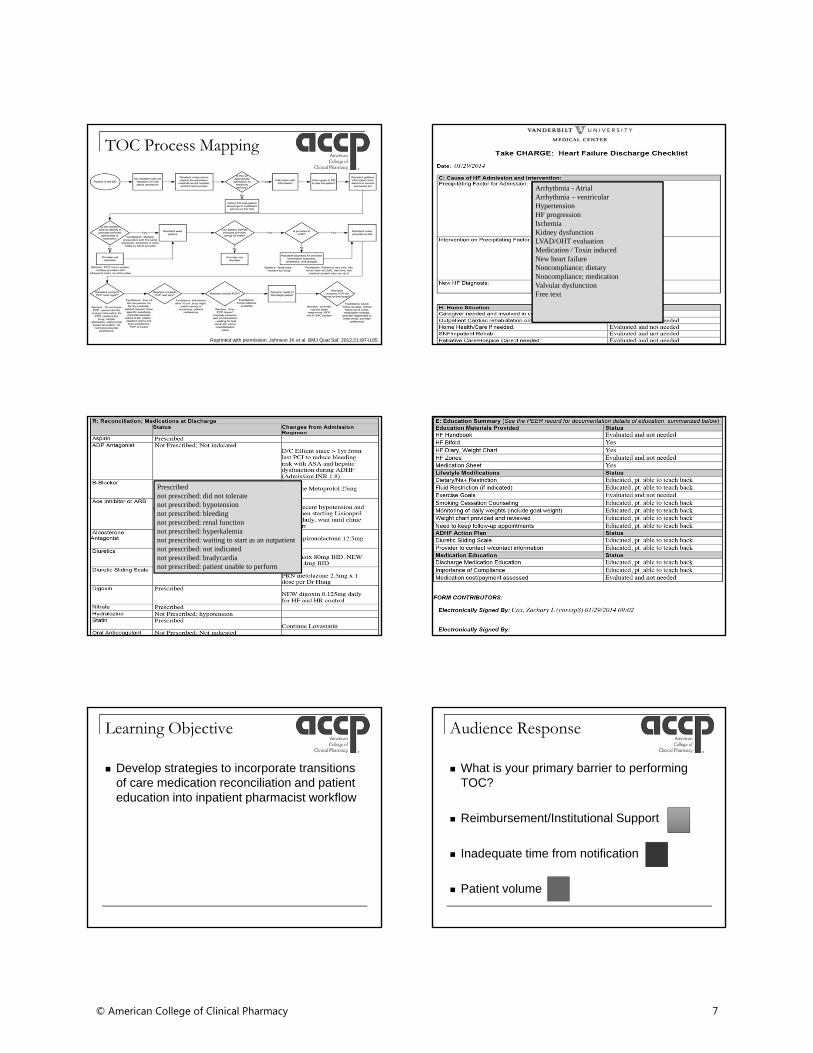
TOC Process Mapping
Reprinted with permission. Johnson JK et al. BMJ Qual Saf. 2012;21:i97-i105.
Arrhythmia - AtrialArrhythmia – ventricularHypertensionHF progressionIschemiaKidney dysfunctionLVAD/OHT evaluationMedication / Toxin inducedNew heart failureNoncompliance; dietaryNoncompliance; medicationValvular dysfunctionFree text
Prescribednot prescribed: did not toleratenot prescribed: hypotensionnot prescribed: bleedingnot prescribed: renal functionnot prescribed: hyperkalemianot prescribed: waiting to start as an outpatient not prescribed: not indicatednot prescribed: bradycardianot prescribed: patient unable to perform
Learning Objective
Develop strategies to incorporate transitionsof care medication reconciliation and patienteducation into inpatient pharmacist workflow
Audience Response
What is your primary barrier to performingTOC?
Reimbursement/Institutional Support
Inadequate time from notification
Patient volume
© American College of Clinical Pharmacy 7
Reimbursement
By 2018, CMS to reimburse with: 50% of payments as alternative payment models
Bundled Payments for Care Improvement
Hospitals bear financial risk
Incentivizes institutional shared-risk partnerships
90% of payments as quality-linked Hospital Value-Based Purchasing Program
Meds to Beds Program
http://www.cms.gov/Newsroom/MediaReleaseDatabase/Fact-sheets/2015-Fact-sheets-items/2015-01-26-3.html. Accessed July 2015.
Too many patients
Risk-based triage of patients Retrospective administrative data models
C statistic range 0.55-0.65
Inpatient data models C statistic range 0.56-0.83
Risk models perform poorly outside ofisolated settings and improvements areneeded for widespread application
Post-acute care inpatient facilities risk
Kanasagara D et al. JAMA. 2011;306:1688-1698.
BOOST Risk Assessment
Problem medications
Psychological/depression
Principle diagnosis
Polypharmacy (> 5 meds)
Poor health literacy
Patient support
Prior hospitalization in 6 months
Palliative careProject BOOST Implementation Guide to Improve Care Transitions. First Edition. 2008. http://www.hospitalmedicine.org/Web/Quality_Innovation/Implementation_Toolkits/Project_BOOST/Web/Quality___Innovation/Implementation_Toolkit/Boost/First_Steps/Implementation_Guide.aspx. Accessed July 2015.
Who is discharging? When?
Multi-disciplinary “huddles”
Case managers
Electronic discharge indicators
Create a discharge culture where pharmacyis integral
More than Meds
MedsMeds
Self Care SkillsSelf Care Skills
Red Flag Symptom
Recognition
Red Flag Symptom
Recognition
Outpatient Follow-upOutpatient Follow-up
Discharge Planning
Discharge Planning
Acknowledgements
Erin Neal, PharmD, BCPS
© American College of Clinical Pharmacy 8
Hold on, we’re going home: Best Practices for Transitions of Care performed by ambulatory care pharmacistsJulianna Burton, Pharm.D., BCPS, BCACP, FCSHP –Assistant Chief of Pharmacy, UC Davis, Sacramento, CAOctober 20th, 2015
2015 ACCP Global Conference on Clinical Pharmacy
Conflict of Interests
I have no conflicts to disclose
UC Davis Medical Center
Multispecialty, university-affiliated medical center 619 bed tertiary care hospital located in Sacramento, CA
Serves approximately six million residents in the region
3Facts and Figures. http://www.ucdmc.ucdavis.edu/newsroom/facts_figures/index.html. Accessed: April 23, 2014
Learning Objectives
Develop strategies to incorporate transitionsof care medication reconciliation and patienteducation into ambulatory care pharmacistworkflow
Apply existing quality metrics endorsed byhealthcare quality sponsoring organizationsto track and measure the impact of caretransitions in the ambulatory care setting
Evaluate established ambulatory care-focused care transition models
Acronyms
BOOST – Better Outcomes by OptimizingSafe Transitions
Project RED (Re-Engineered Discharge)
NTOCC – National Transitions of CareCoalition
Patient Centered Primary Care Collaborative(PCPCC)
Patient Centered Medical Home (PCMH)
Question 1
Which of the following models could bestincorporate an amcare pharmacists? A. Project Red
B. AHRQ
C. PCPCC
D. BOOST
© American College of Clinical Pharmacy 9
Question 2
There are several great resources availableonline to start a new TOC service. Which of thefollowing resources would be the best to utilizeto get an in-depth, detailed understanding of theimplementation of TOC services at your site? A. Project RED
B. BOOST
C. AHRQ
D. National Quality Forum
BOOST
Hospitalmedicine.org
1st edition free, 2nd only $65
Proven to decrease readmits
Features: Speaks of accountability
Best Possible Medication History (BPMH)
8P’s including pharmacy component
Has TOC from hospital to SNF
8P’s
Problems with meds
Psych issues
Principal diagnosis
Physical limitations+
Poor health literacy*
Poor social support
Prior hospitalization
Palliative care
Further BOOST features
Provides checklists that can be used by all teammembers
Review to see what the discharge status is for pt
Provides for a medication action plan
Bring to amcare/primary care visit
Pharmacist in primary care can use as a first step
Suggests MARQUIS (Multi-Centered MedicationReconciliation Quality Improvement Study)
Has videos, manual, BPMH pocket cards, andpresentations about med rec
Project RED
Proven to decrease readmits
Free to implement, but not easy
Has several toolkits, including how to implementprogram
Very in depth information
Includes measures to review
MUST have staff and hospital administration onboard to implement
Virtual dc educator Louise
12 components
Language barriers
Make appts for pt
Pending results?
DME/Social
Medications*
Compare to NationalGuidelines
Discharge plan for pt
Educate patient
Assess understanding
Problems arise? Whatto do?
D/C summary to MDw/in 24 hrs
Follow up call -PharmD
© American College of Clinical Pharmacy 10
Follow up call - PharmD
Three days after discharge
Reviews most of the 12 components again
Script provided on website
Asks open ended questions
Use teach-back method
PCPCC
Patient-Centered Primary Care Collaborative
Website provides broad overview of PatientCentered Medical Home (PCMH) model
For patients, HCP, employers, purchasers,and policy makers
Takes a different approach to readmits –keep patients from being admitted in the firstplace!
PCPCC
Best Amcare Care Coordination/TOCresource
Reviews multiple practice “expert” sites
Asks applicable questions of sites using thePCPCC TOC model
Information provided in Q/A format
Many have a pharmacist embedded into thePCMH for medication management andadherence issues
NTOCC
Wealth of information
TOC checklist – similar to BOOST, moretheory than practice
Supports webinars, conferences and taskforces on TOC with policy groups around thenation
More measures than BOOST or Project Red
Provides sections of the site for patients,HCP, and policy makers
NTOCC
Has section on TOC in primary care Suggests MD, but could be performed by a
PharmD
Uses the Modified Morisky Scale
Has a 3 page medication reconciliationelements document Shows extensive definition of proper way to
perform med rec
Review Metrics - Amcare
NTOCC - Measures Work Group
NQF – HCAHPS CTM-3 questions
Care Coordination Measures Atlas –Measure 18, MUPM
© American College of Clinical Pharmacy 11
Question 3
Which of the following metrics might be bestincorporated into and amcare TOC program? A. HCAHPS Care Transitions questions
B. Efficiency measures such as reducingduplicative lab tests
C. Pharmacist/Physician contribution metrics
D. Decreasing Length of Stay
NTOCC - Measures
Structural – adequate systems
Process – timeliness/completeness,adequacy of providers
Outcomes - Adverse events
Efficiency – inappropriate resource utilization
Experience – Pt/providers
National Quality Forum
HCAHPS Care Transitions Questions: The hospital staff took my preferences and those of
my family or caregiver into account in deciding whatmy health care needs would be when I left thehospital.
When I left the hospital, I had a good understanding ofthe things I was responsible for in managing my health
When I left the hospital, I clearly understood thepurpose for taking each of my medications.
AHRQ Measures
AHRQ has measures related to pharmacy Measure 18 – MD-PharmD Collaboration
Instrument Measures pharmacist/MD collaboration
Family Medicine Medication Use ProcessesMatrix (MUPM) Measures MD’s perspectives of pharmacist contributions
Incorporation
Barriers of cost, time and culture
Need to develop new role for pharmacist
May need to obtain more credentials, certifications,advanced practice licenses, or even privileging
Studies abound in this area and metrics can help todevelop a sound pilot
Residents/students can help start small initiatives, buteventually a culture shift (and resources) will benecessary for a fully successful program
Question 4
Patient Case: MC is a 78 yo female with hx of AMI, DMand HTN. She is taking Atorvastatin 20mg, ASA 81 mgand insulin. Her MD just saw her for the first time in 4years after she was dc’d from the hospital. Medicationnon-adherence is a probable cause for her admit. Whatwould be the best first step in the PCMH pharmacistvisit? A. Take the patient’s blood pressure
B. Contact the patient’s pharmacy to get prior auths approved
C. Perform a BPMH and medication reconciliation
D. Create a patient specific medication calendar
© American College of Clinical Pharmacy 12
2012 UC Davis Pilot- CHF
2012 Added 0.5 FTE pharmacist and 0.5 FTE nursein an amcare role (grant funded)486 total Patient encounters 77 Face to face visits (total patients 77) 402 Telephonic education and assessments Seven Email communications (MyChart)
77 Total Patients Medication Adherence Interventions: 81
Patient was either not taking the medication at all or was taking an incorrect dose or frequency 49% of Patients had at least one lack of adherence event(range 1‐14 events)
Most patients had 2‐3 adherence events
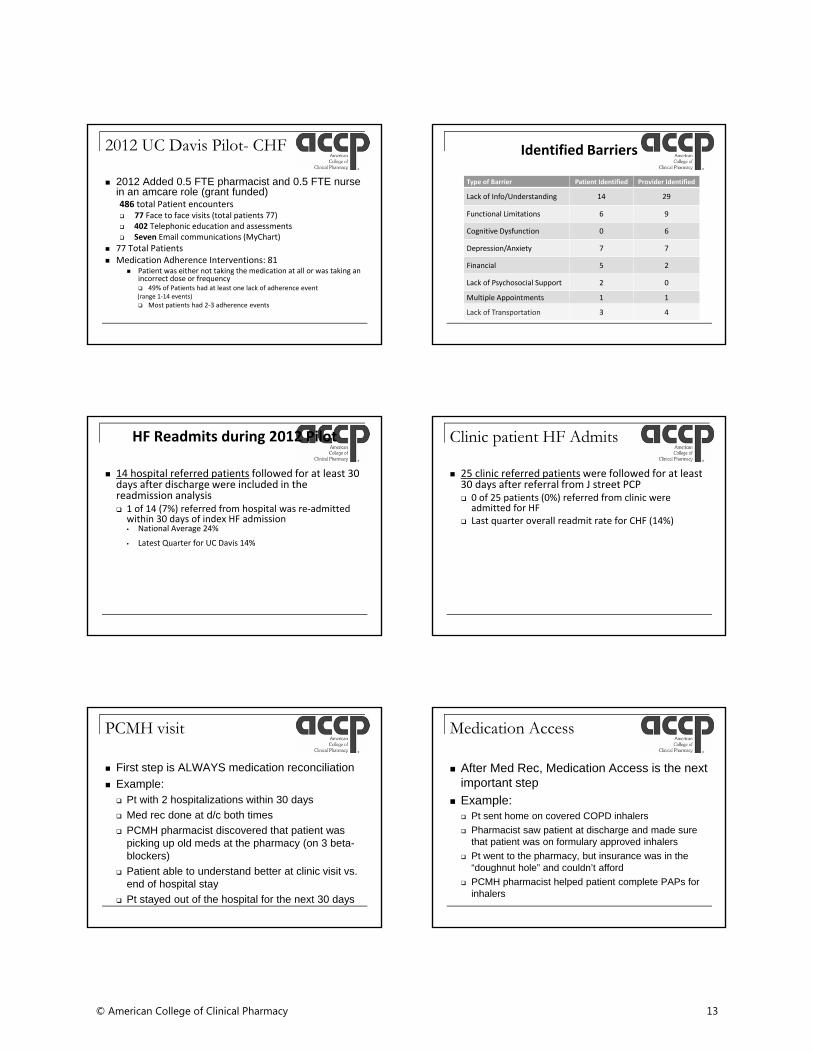
Identified Barriers
Type of Barrier Patient Identified Provider Identified
Lack of Info/Understanding 14 29
Functional Limitations 6 9
Cognitive Dysfunction 0 6
Depression/Anxiety 7 7
Financial 5 2
Lack of Psychosocial Support 2 0
Multiple Appointments 1 1
Lack of Transportation 3 4
HF Readmits during 2012 Pilot
14 hospital referred patients followed for at least 30 days after discharge were included in the readmission analysis 1 of 14 (7%) referred from hospital was re‐admittedwithin 30 days of index HF admission• National Average 24%
• Latest Quarter for UC Davis 14%
Clinic patient HF Admits
25 clinic referred patients were followed for at least 30 days after referral from J street PCP 0 of 25 patients (0%) referred from clinic were admitted for HF
Last quarter overall readmit rate for CHF (14%)
PCMH visit
First step is ALWAYS medication reconciliation
Example: Pt with 2 hospitalizations within 30 days
Med rec done at d/c both times
PCMH pharmacist discovered that patient waspicking up old meds at the pharmacy (on 3 beta-blockers)
Patient able to understand better at clinic visit vs.end of hospital stay
Pt stayed out of the hospital for the next 30 days
Medication Access
After Med Rec, Medication Access is the nextimportant step
Example: Pt sent home on covered COPD inhalers
Pharmacist saw patient at discharge and made surethat patient was on formulary approved inhalers
Pt went to the pharmacy, but insurance was in the“doughnut hole” and couldn’t afford
PCMH pharmacist helped patient complete PAPs forinhalers
© American College of Clinical Pharmacy 13
Health Literacy
Third most important is Health Literacy or LanguageBarriers
Example: Pt was discharged on NOAC for PE
PharmD at d/c got PAP approved for pt
PharmD at retail pharmacy told patient not to take dueto renal dysfunction
Pt went without any anticoagulant x 1 week
Saw PCMH pharmacist and reviewed list, pt wasSpanish speaking and didn’t understand importance ofmed
Question 5
Which of the following was identified as thenumber one barrier to medication non-adherence by both patients and providers atUC Davis, during the CHF pilot study? A. Lack of Transportation
B. Financial Barriers
C. Depression/Anxiety
D. Lack of info/understanding
Medication Calendar
Generic (Brand)/ Name
Dose When to take:
Breakfast Lunch Dinner Bedtime
This medication is for your:
Side Effects
Incorporation
Need to have an amcare place to “catch”d/c’d patients
Utilize learners to help extend reach
Need to work with other disciplines/aspects: Care Coordination – schedule patients/refer
MA’s to room patients
Analysts to review outcomes
Go to MD huddles/meetings to develop trust/getreferrals
Conclusion
Pharmacists can play in important role in catchingpatients after hospitalization
They are uniquely suited for a role with medicationreconciliation and medication access
Since 2003, outpatient visits are up by 12% and inpatientvisits are down by 20% (PWC)
ACO’s make pharmacist costs less important
Now is the time to move pharmacists into the clinics toprovide better patient care, including TOC
References
1. Moore C, Wisnivesky J, Williams S, et al. Medical Errors Related to Discontinuity of Care from an Inpatient to an Outpatient Setting. J Gen Intern Med. 2003; 18:646-651.
2. Kripalani S, Roumie CL, et al. Effect of a Pharmacist Intervention on Clinically Important Medication Errors after Hospital Discharge: A RandomizedControlled Trial. Ann Intern Med. 2012; 157(1):1-10.
3. Walker PC, Bernstein SJ, et al. Impact of a Pharmacist-Facilitated Hospital Discharge Program: A Quasi-Experimental Study. Arch Intern Med. 2009; 169(21):2003-2010.
4. Schnipper JL, Kirwin JL, et al. Role of Pharmacist Counseling in Preventing Adverse Drug Events After Hospitalization. Arch Intern Med. 2006; 166:565-571.
5. Sarangarm P, London MS, et al. Impact of Pharmacist Discharge Medication Therapy Counseling and Disease State Education Pharmacist Assisting atRoutine Medical Discharge (Project PhARMD). American Journal of Medical Quality. 2013; 28: 292-299.
6. Schnipper JL, Kirwin JL, Cotugno MC, et al. Role of pharmacist counseling in preventing adverse drug events after hospitalization. Arch Intern Med 2006; 565-71. DOI 10.1001/archinte.166.5.565.
7. Centers for Medicare and Medicaid Services. http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/AcuteInpatientPPS/Readmissions-Reduction-Program.html. Accessed: September 25, 2013.
8. University Health System Consortium. University of California, Davis Medical Center Quality Management Dashboard. July 2012.9. UHC Benchmarking Project on Reducing Readmissions 2009. Oakbrook, IL.10. Unpublished data presented at UHC Pharmacy Council, December 2009 and personal communications.
11. ACCP BCPS PSAP module, 2014, TOC chapter.
12. Project Red. Accessed 8/1/15. Internet Citation: https://www.bu.edu/fammed/projectred/
13. NTOCC website. Accessed 8/1/15 Internet Citation: http://www.ntocc.org/
14. AHRQ Care Coordination Atlas. Accessed 8/1/15. Internet Citation: Chapter 1: Background: Care Coordination Measures Atlas Update. June 2014. Agency for Healthcare Research and Quality, Rockville, MD. http://www.ahrq.gov/professionals/prevention-chronic-care/improve/coordination/atlas2014/chapter1.html
15. BOOST Toolkit. Accessed 8/1/15. Internet Citation: http://www.hospitalmedicine.org/Web/Quality_Innovation/Implementation_Toolkits/Project_BOOST/Web/Quality___Innovation/Implementation_Toolkit/Boost/BOOST_Intervention/Tools/Medication_Reconciliation.aspx
16. PCPCC Patient Centered Primary Care Collaborative. Accessed 8/1/15. Internet Citation: http://www.aafp.org/dam/AAFP/documents/practice_management/pcmh/initiatives/PCMHJoint.pdf
17. PWC Health. Accessed 8/1/15. Internet Citation: http://pwchealth.com/cgi-local/hregister.cgi/reg/pwc-hri-medical-cost-trend-2016.pdf
© American College of Clinical Pharmacy 14

Special Thanks!
Stephanie Roberts, Pharm.D.,BCPS
Stephanie Marin, Pharm.D., BCPS
Pamela Mendoza, Pharm.D.
Jennifer Nguyen, Pharm.D.
Patricia Poole, Pharm.D., BCPS, AAHIVE
Contact info: [email protected]
© American College of Clinical Pharmacy 15
Recommended

















