Adrenals and Adrenal carcinoma
Review
Dr Shankar Ram HSDepartment of Genito Urinary Surgery
TDMCH .




• Cortical vessel • Medullary vessel • Capsular vessel – Cortical- Medullary capillary
sinusoids – medullary vein• Medulla – Dual supply • Pericapsular adrenal arterial Plexus – emissary
vein – Central vein

Medulla - -- sympathetic ganglionChromaffin cells – post ganglionic symp neurons w/o axons & dentrites


Adrenal rests 1 %
• Path of gonadal descent and celiac axis • CAH- p/w palpable testes • Compensatory hypertrophy

GFR ACE



• 29% of adenomas have attenuation values higher than 10 HU (hyperattenuating) and remain indeterminate (5).
• Chemical shift MR imaging can be performed rapidly without contrast material injection
• strong correlation between the degree of signal intensity (SI) decrease on out-of-phase MR images and CT attenuation

• washout CT has excellent diagnostic performance for hyperattenuating adrenal adenoma
• lipid-poor adenomas with attenuation higher than 30 HU at unenhanced CT are not well diagnosed with chemical shift MR imaging





Cushigns syndrome
• Hypercortisolism secondary to excessive production of glucocorticoids by adrenal cortex
• Exogenous ACTH dependent and ACTH independent
• ACTH-independent hypercortisolism, on the other hand, results from unregulated overproduction of glucocorticoids by the adrenal(s) and is relatively rare.
• Up to 50% of• patients with Cushing syndrome exhibit urolithiasis;



Measurement of ACTH
• Serum levels • Inferior Petrosal sinus levels after CRH
stimulation
• Low serum levels –ACTH independent Etiology –Abd imaging



• LD DST -+ Only tells there is hypercortisolism • (Overnight and standard).• HD DST for cushings disease .- outdated


Dexamethasone Suppression Test
• http://emedicine.medscape.com/article/2114191-overview

Bilateral adrenalectomy
• AIMAH• PPNAD• Ectopic ACTH syndrome • Failure of Pit adenoma Rx

Primary Aldosteronism





PAC/PRA =ARR > 30 – screeningPAC > 20
• Conformatory - Autonomous aldoesterone cannot be supressed
• Fludorocortisone supression( test upright )PAC>6• Oral salt loading test (PAC>12)• IV saline test (PAC>5-10)• Captopril supression test (PAC>15)











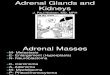
Adrenals Tumors



• Rare • Unilateral • Rarely bilateral • 5 the decade (60% functional) C+• Children – low stage functional (even small size) V+• local periadrenal tissue, lymph nodes, lungs,
liver, and bone• Syndromes – BW (IGF) , LF (p53)

Renal displacement Camoflague

ACC –C T
• Irregular borders,• irregular enhancement,• calcifications, and necrotic areas with cystic
degeneration. • Mean attenuation on non contrast CT scan in
ACC is significantly higher (39 HU) • The presence of contiguous adenopathy
serves as corroborating evidence• Thrombus


ACCs
• Larger than benign adrenal tumors,• Average size of 10 to 12 cm on presentation.• Indeed over 90% of ACCs are larger than 5 cm• numerous unnamed collateral vessels
associated with large adrenocortical carcinomas.
• tumoral capsule,• a stellate zone of central necrosis

MRI
• Venous thrombus• Iso-T1 (Liver spleen)• Hyper – T2• Marked uptake • Delayed washout

• NO Biopsy

Symptoms
• Size• Stage• Function


• Virtually all feminizing adrenal tumors in men are malignant.

Endocrine syndromes associated with AC include the following:
• Cushing syndrome (30%)• Virilization and precocious puberty (22%)• Feminization (10%)• Primary hyperaldosteronism (2.5%)• Combined hormone excess (35%)• Polycythemia (< 1%)• Hypercalcemia (< 1%)• Hypoglycemia (< 1%)• Adrenal insufficiency (particularly from primary adrenal lymphomas)• Non–glucocorticoid-mediated insulin resistance• Catecholamine excess due rarely coexisting pheochromocytoma• Cachexia (usually preterminal


Pre op
• Cortisol excess -inhibition with ketoconazole, mitotane, or metyrapone
• Treatment for appropriate coagulopathies • Serum potassium levels should be corrected in
hyperaldosteronism• hypertension control should be initiated.

Open Adrenalectomy
• Masses that are greater than 6 cm have a rate of adrenocortical carcinoma of 25% and should be managed surgically.
• gold standard for masses suspected of benign adrenal carcinoma
• Cytoreductive

Pathiological evaluation


IHC
• Insulinlike growth factor–2 (IGF-2) and Ki-67 overexpression identified ACs with 96% sensitivity and 100% specificity
• adrenocortical cells stain positive for D11, SF-1
• Adrenomedullary tumors positive for neuroendocrine markers eg, synaptophysin, NSE,Chromogranin A),

ACCs
• weight of more than 500 g, • presence of areas of calcification or necrosis, • grossly lobulated appearance.• numerous mitoses, • scant cytoplasm, and • none of the rosettes observed in
neuroblastoma.


Prognostics
• Disease stage at diagnosis• Completeness of resection at surgery• metastasis at the time of diagnosis• Estrogen receptor (ER)–negative –Poor Prognosis• overall five-year survival 20-35%

Recognition of primary adrenal lymphoma
• Recognised as distinct from adrenocortical carcinoma
• associated with a better prognosis than AC, • Very rare .• potential roles for standard lymphoma
treatment using multiagent chemotherapy and radiotherapy.

Follow up
• For low-grade tumors, imaging every 3-6 months and biomarkers (if Active)
• For high-grade tumors, -adjuvant therapy• Mets- Low grade - adrenalectomy if 90% of tumor
can be removed surgically; • follow-up should be oriented to the residual
disease (Thoracotomy /Lobectomy in selected pts).• Survival reported > 10 years

Mitotane
• Relatively specific adrenocortical cytotoxin• It is used as primary therapy, as adjuvant therapy, and as
therapy in recurrent or relapsing disease..• adrenal inhibition without cellular destruction. • controls endocrine hypersecretion in 70-75% pts. • Tumor response correlate with serum levels .• Months of continuous therapy.• efficacy at least 15 mcg/mL.• The potential benefit of postoperative adjuvant therapy
with mitotane is still controversial.

(FIRM-ACT) The First International Randomized Trial in Locally Advanced and Metastatic Adrenocortical
Carcinoma Treatment study
• mitotane and etoposide * Vs• mitotane and streptozocin
First line therapy had higher response rates and longer median progression-free survival than patients treated with (5 mo vs 2.1 mo, respectively)
*

• Sumarin • Gossypol • Cisplatin• Doxorubicin • Long acting alpla and beta blockers • Antiandrogens • Antiestrogens • New molecules

Radiotherapy
• If Local recurrence is expected • Adjuvant RRx to tumor bed • 40 gray (Gy), # 1.8-2 Gy • (including a boost volume to reach from 50-60
Gy in individual patients)

Thoracoabdominal Approach

















Video • https://www.youtube.com/watch?v=smgB0nO7KTs (open )
• https://www.youtube.com/watch?v=XJoiYDpcf4c lap
• https://www.youtube.com/watch?v=5s3JHZF2uTY L Thoraco abdominal nephrectomy
• https://www.youtube.com/watch?v=wZFC8kShzFE
• https://www.youtube.com/watch?v=xC50mVH2RSE

https://www.youtube.com/watch?v=UNGRer0v7o0



R0






Open Adrenalectomy
• First Resection is the best Resection • Lnymphadenectomy is absolute • Nothing Short of R0 Resection for best results






References
• Campbell and Walsh 11 e• SAGES symposium - youtube • NCCN• E medicine • Guidelines for the management of the incidentally discovered adrenal mass- Anil Kapoor .Canadian Urology association
https://www.cua.org/themes/web/assets/files/guidelines/en/guidelines_for_the_management_of_the_incidentally_discovered.pdf
AACE/AAES Guidelineshttps://www.aace.com/files/adrenal-guidelines.pdf
Recommended