Adjuvant treatments for melanoma: how can we best expand oncology services to cope with the demand?
… with the involvement of pharmacists and CNSs?
Dr. Paul Nathan
Consultant Medical Oncologist
Mount Vernon Cancer Centre

Dermatologist involvement in melanoma oncology management is essential

Dermatologist involvement in melanoma oncology management is essential
• Lightening dark humour
• Improving dress sense in oncology clinic

Dermatologist involvement in melanoma oncology management is essential
• Lightening dark humour
• Improving dress sense in oncology clinic
• Management of systemic therapy side effects
• Skin lesion diagnosis and management• Early diagnosis and treatment
• Reduces multiple clinic visits for already burdened patients

Total cycles of treatment delivered
0
100
200
300
400
500
600
700
800
Aug 16 –Jan 17
May 18 –Oct 18
Nov 18 –Apr 19
May 19 –Oct 19

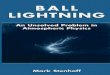
Metastatic patients receiving systemic treatment
Metastatic patients on treatment:• 10-20% increase in numbers every 6 months for the last 3 years
• Number of new metastatic patients currently stable at 65 per year
0
20
40
60
80
100
120
140
Total number of metastatic patients on treatment
Apr 16 –Jan 17
May 18 – Oct 18
Nov 18 –Apr 19

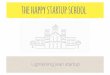
Use of Adjuvant Therapy in Patients With Stage IIIB/IIIC Melanomaa
UK, United Kingdom.
a Diagnosis made between 1 January 2009 and 31 December 2011; b Unknown therapy given in a blinded clinical trial investigating therapies licensed for stage IIIA/B melanoma; c Includes carboplatin/paclitaxel, bacillus Calmette-Guérin, radiotherapy and radiochemotherapy. In France, “other” also included 5 patients treated with interferon regimens at unspecified doses; dData missing for 1 patient. Percentage equals the number of patients with further progression of locoregional recurrence divided by all patients with locoregional recurrence.
Harries M, et al. Int J Clin Pract. 2017;71:e12946.
Considerable variation in use of adjuvant therapy (mostly interferon) between patients with stage IIIB/IIIC melanoma in Germany (≈ 33% use) and France/UK (3-7% use)
Adjuvant Systemic Therapy Received, n
(%)
France
(n = 199)
Germany
(n = 164)
UK
(n = 195)
Overall
(n = 558)None 185 (93.0) 109 (66.5) 190 (97.4) 484 (86.7)
Interferon
High dose
Intermediate dose
Low dose
Pegylated
Unknownb
Otherc
3 (1.5)
1 (0.5)
0
0
1 (0.5)
9 (4.5)
18 (11.0)
8 (4.9)
25 (15.2)
3 (1.8)
0
1 (0.6)
0
0
0
0
0
5 (2.6)
21 (3.8)
9 (1.6)
25 (4.5)
3 (0.5)
1 (0.2)
15 (2.7)
Disease progression, n (%)
Deceased
Any recurrence
Type of first occurrence
Locoregional
Further progression to distant metastases
Distant metastasis
66 (33.2)
131 (65.8)
57 (43.5)
32 (57.1)d
74 (56.5)
59 (36.0)
100 (61.0)
39 (39.0)
17 (43.6)
61 (61.0)
71 (36.4)
120 (61.5)
48 (40.0)
26 (54.2)
72 (60.0)
196 (35.1)
351 (62.9)
144 (41.0)
75 (52.4)
207 (59.0)
Real-World Data From the 2016 MELABIS Observational Study (France, Germany, UK)

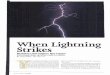
Patients receiving adjuvant treatment
0
10
20
30
40
50
60
70
80
90
Aug 16 –Jan 17
May 18 –Oct 18
Nov 18 –Apr 19
May 19 –Oct 19

Number of cycles of adjuvant treatment delivered
0
20
40
60
80
100
120
Adjuvant targeted (total cycles) Adjuvant IO (total cycles)
Aug 16 –Jan 17
May 18 – Oct 18
Nov 18 – Apr 19
May 19 – Oct 19

Clinic visits for an adjuvant patient
• First clinic post-surgery Doctor• Risk of relapse
• Absolute risk reduction of adjuvant treatment
• Side effect profile of adjuvant treatment
• Patient information sheets
• Surveillance protocols & contact numbers
• Clinical trial options

Subsequent visits – Dab+Tram & Nivo
1 Consent, scan result and initiation of treatment D/N/(P)
2 Treatment review and prescription N/P
3 Treatment review and prescription N/P
4 Scan result, treatment review and prescription N/P/(D)
5 Treatment review and prescription N/P
6 Treatment review and prescription N/P
7 Scan result, treatment review and prescription N/P/(D)
8 Treatment review and prescription N/P
9 Treatment review and prescription N/P
10 Scan result, treatment review and prescription N/P/(D)
11 Treatment review and prescription N/P
12 Treatment review and prescription N/P
13 Scan result, treatment review and prescription D/N/P

Subsequent visits – IO therapy (6/52 pembro)1 Consent, scan result and initiation of treatment D/N/(P)2 Review & bloods N/P3 Treatment review and prescription N/P4 Review & bloods N/P5 Treatment review, scan result and prescription N/P/(D)6 Review & bloods N/P7 Treatment review and prescription N/P8 Review & bloods N/P9 Scan result, treatment review and prescription N/P/(D)10 Review & bloods N/P11 Treatment review and prescription N/P12 Review & bloods N/P13 Scan result, treatment review and prescription N/P/(D)14 Review & bloods N/P15 Treatment review and prescription N/P16 Review & bloods N/P17 Scan result, treatment review and prescription D/N/P

Impact upon capacity
• A prescribing clinical nurse specialist or pharmacist could see almost all visits (as could a dermatologist)
• All would need to discuss abnormal scan findings with oncologist
• All would currently need to discuss abnormal bloods with oncologist

Cost of service improvement
• 188 cycles adjuvant therapy in last 6/12 (approx. 8 on-treat adjuvant patients per week)
• Most institutions do not have spare capacity• New role needs to be supported by business case and activity back-filled


DERM NURSE / PHARM

DERM NURSE / PHARM
1 DERM = 2.53 NURSE / PHARM

The near future
• Patients with microscopic stage III disease – as currently
• Patients with macroscopic stage III disease • Neoadjuvant combination immunotherapy
• Adjuvant depending on response
• Increasing oncology input required

Dermato-oncology and/or oncology?
• Melanoma oncology care delivered by dermato-oncologists in France, Germany, Japan and others to a greater or lesser extent
• In UK systemic anti-cancer treatment is only delivered by specialist trained oncologists
• We could change this and have dual training for derm-onc or
• Train more oncologists

The solution
• Reducing attendance at clinics• Telephone / video consultations for on treat patients
• CNS / Pharmacist led clinics.
• Do not require a doctor
• Trials of improved schedules
• A prescribing nurse / pharmacist in clinic allows• The oncologist to focus on oncological problems
• The dermatologist to focus on dermatological problems
Recommended