Abusive Head Trauma: An Overview and Review of the Literature
Bruce J. McIntosh, M.D. Co-Interim Statewide Medical Director Child Protection Team System
Abusive Head Trauma Objectives
Review the basic anatomy of the skull, brain and supporting membranes
Review the mechanisms of injury and clinical findings in Abusive Head Trauma
Discuss the reasons why the term “Abusive Head Trauma” is replacing the term “Shaken Baby Syndrome”
Discuss the scientific basis on which the diagnosis of Abusive Head Trauma can be made, issues of timing addresse, and exceptions to the rules
Review flawed literature and arguments often proffered by defense experts to explain away abusive head injuries
Abusive Head TraumaWhy Does It Happen?
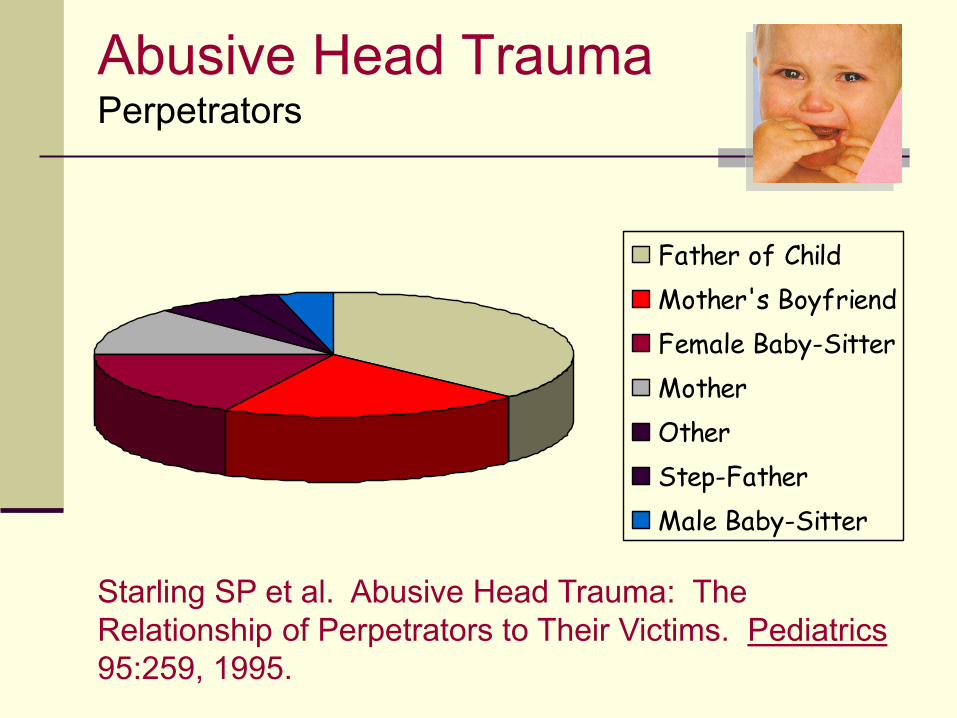
Father of Child
Mother's Boyfriend
Female Baby-Sitter
Mother
Other
Step-Father
Male Baby-Sitter
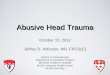
Abusive Head TraumaPerpetrators – Can Be “Nice People”
Starling SP et al. Abusive Head Trauma: The Relationship of Perpetrators to Their Victims. Pediatrics 95:259, 1995.
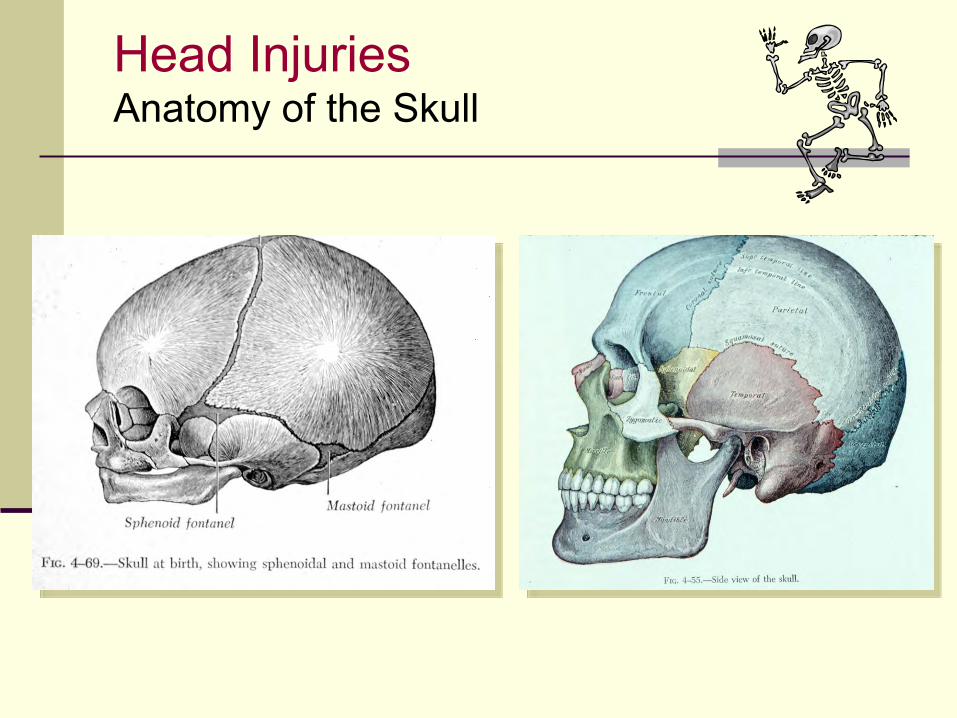
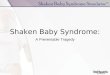
Head Injuries Anatomy of the Skull
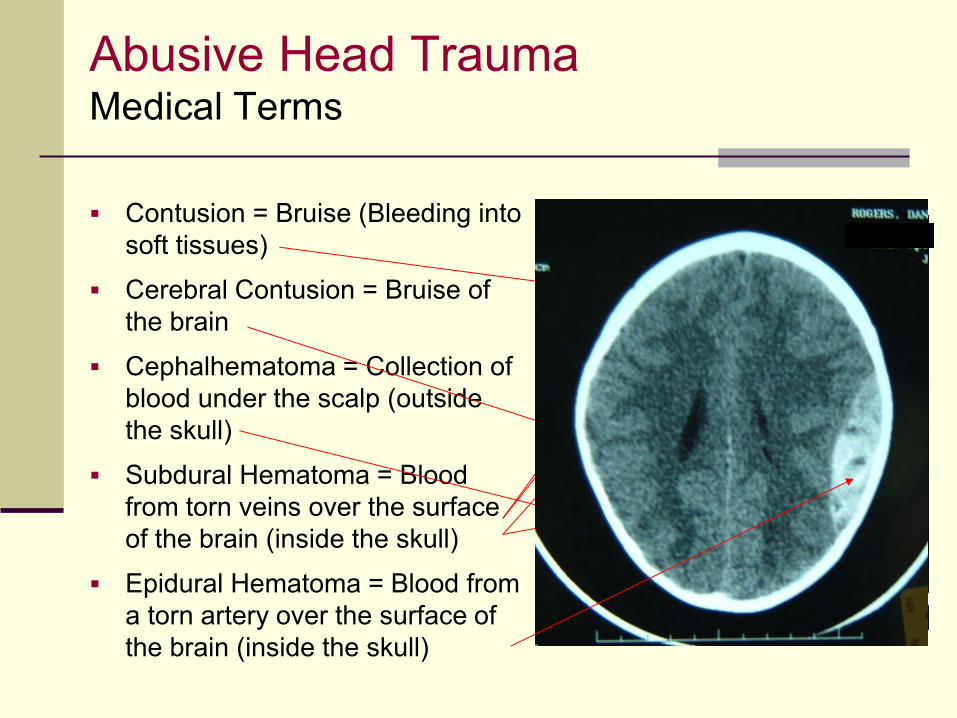
Abusive Head Trauma Medical Terms
Contusion = Bruise (Bleeding into soft tissues)
Cerebral Contusion = Bruise of the brain
Cephalhematoma = Collection of blood under the scalp (outside the skull)
Subdural Hematoma = Blood from torn veins over the surface of the brain (inside the skull)
Epidural Hematoma = Blood from a torn artery over the surface of the brain (inside the skull)
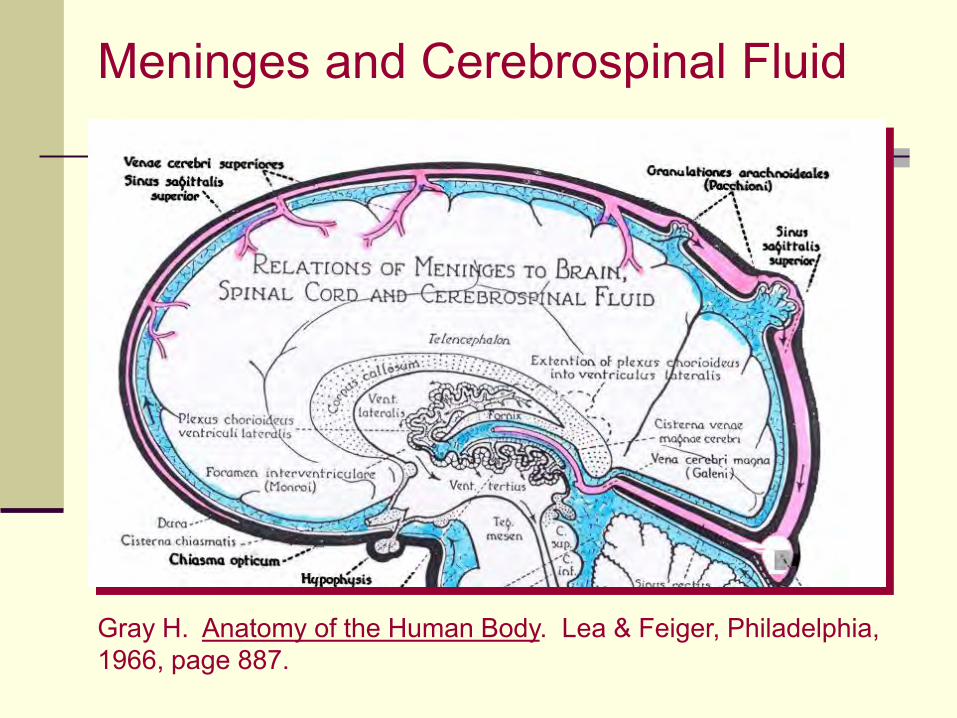
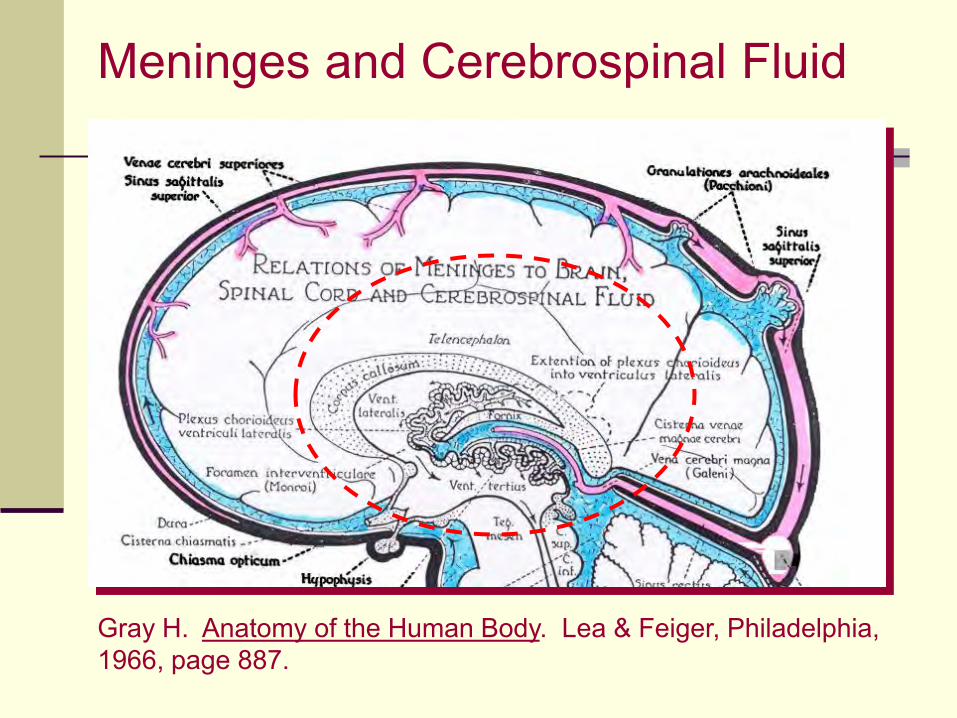
Meninges and Cerebrospinal Fluid
Gray H. Anatomy of the Human Body. Lea & Feiger, Philadelphia, 1966, page 887.
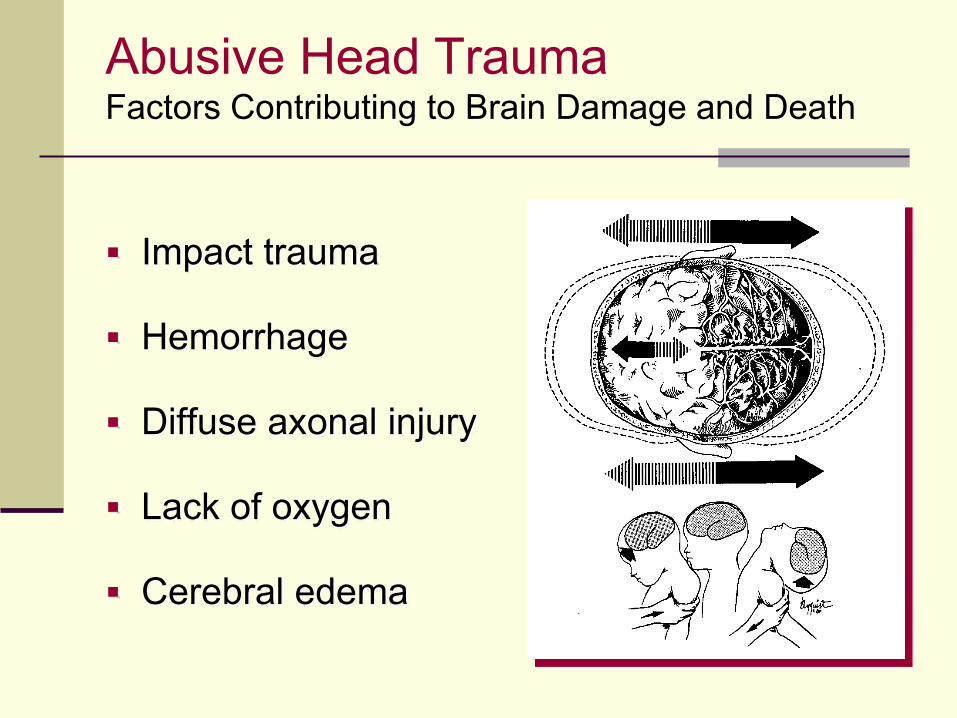
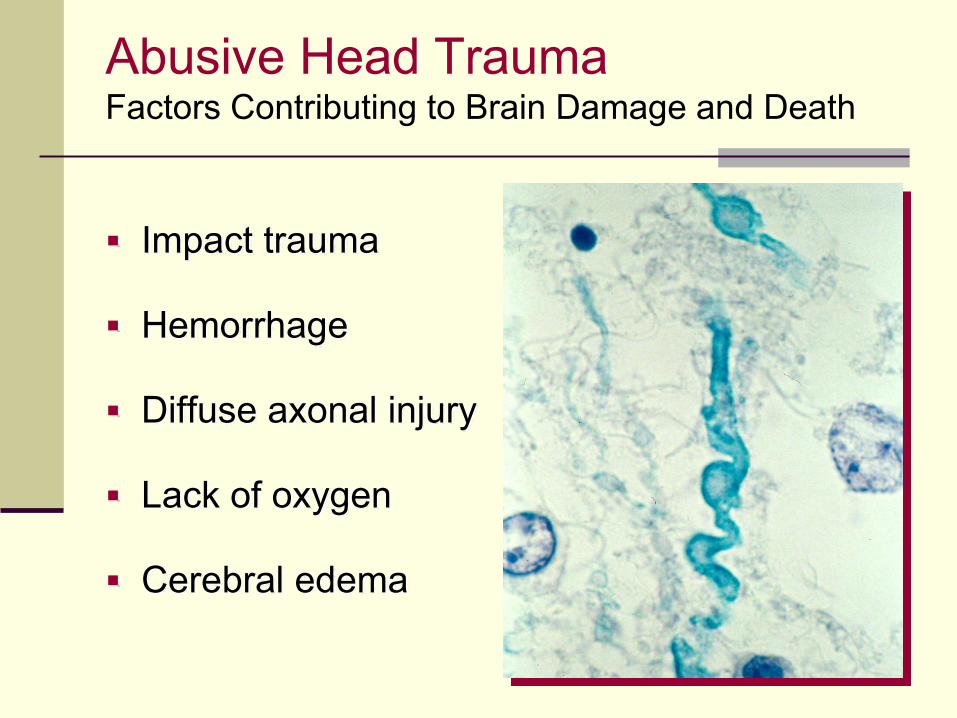
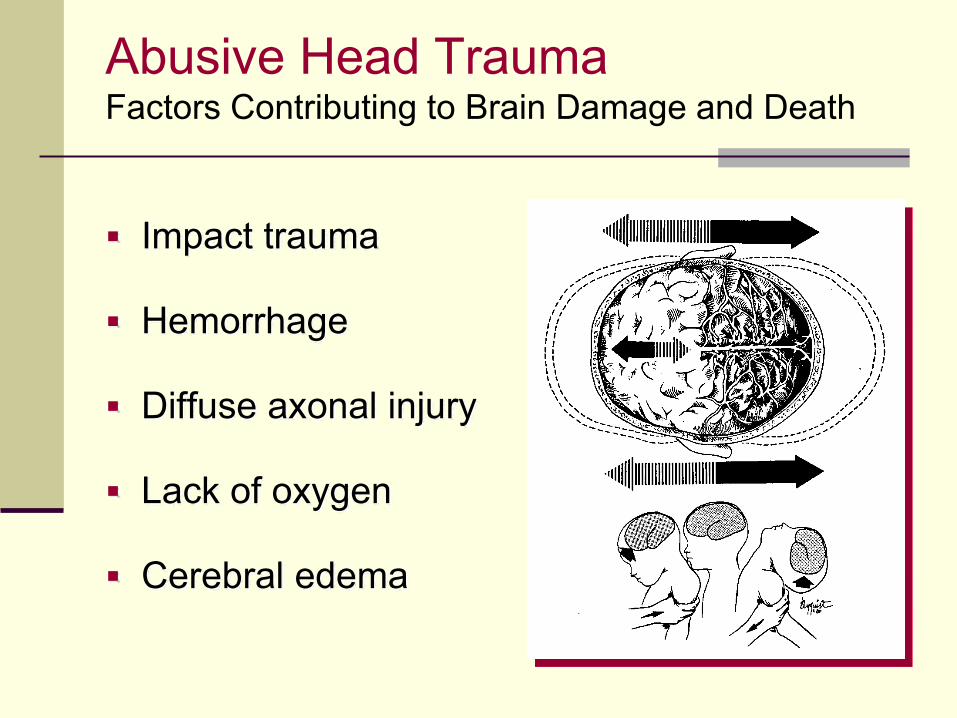
Abusive Head Trauma Factors Contributing to Brain Damage and Death
Impact trauma
Hemorrhage
Diffuse axonal injury
Lack of oxygen
Cerebral edema
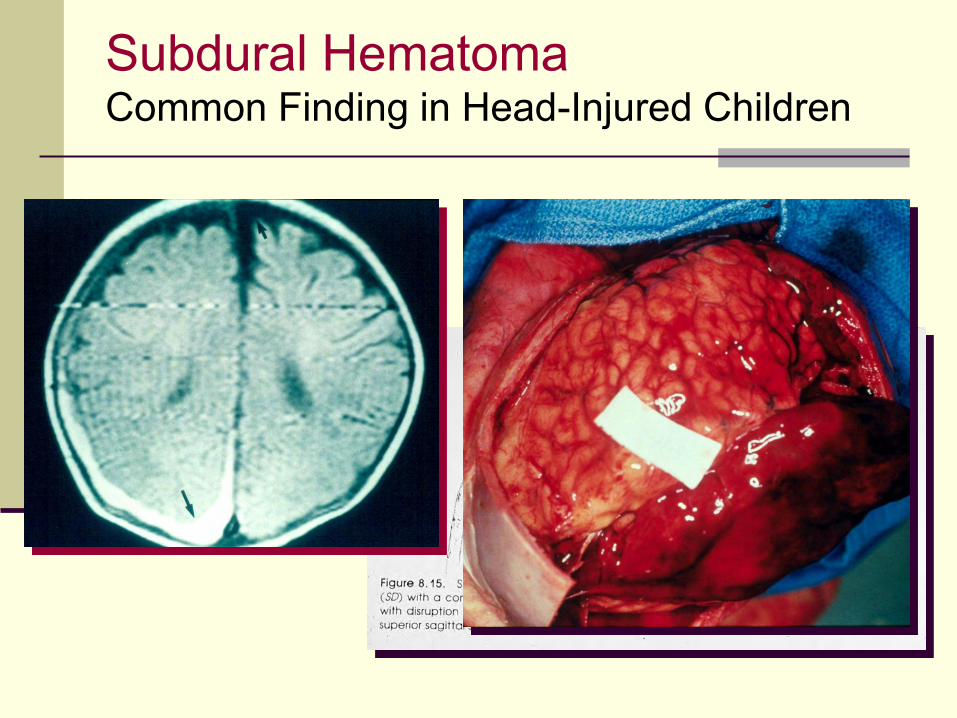
Subdural Hematoma Common Finding in Head-Injured Children
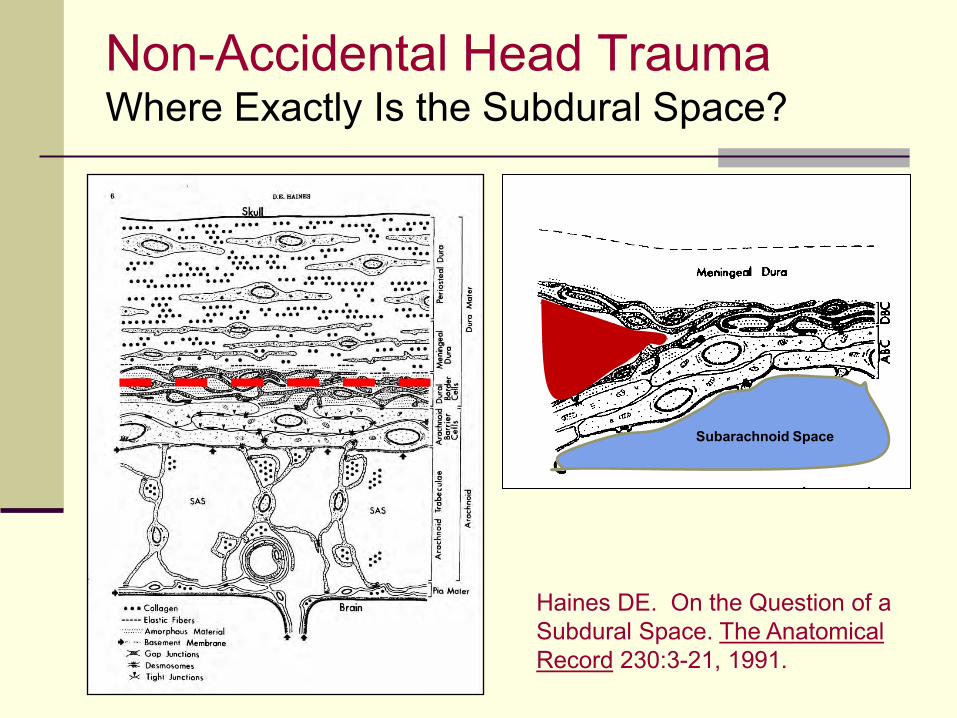
Non-Accidental Head Trauma Where Exactly Is the Subdural Space?
Haines DE. On the Question of a Subdural Space. The Anatomical Record 230:3-21, 1991.
Subarachnoid Space
Abusive Head Trauma Factors Contributing to Brain Damage and Death
Impact trauma
Hemorrhage
Diffuse axonal injury
Lack of oxygen
Cerebral edema
Meninges and Cerebrospinal Fluid
Gray H. Anatomy of the Human Body. Lea & Feiger, Philadelphia, 1966, page 887.
Abusive Head Trauma Factors Contributing to Brain Damage and Death
Impact trauma
Hemorrhage
Diffuse axonal injury
Lack of oxygen
Cerebral edema
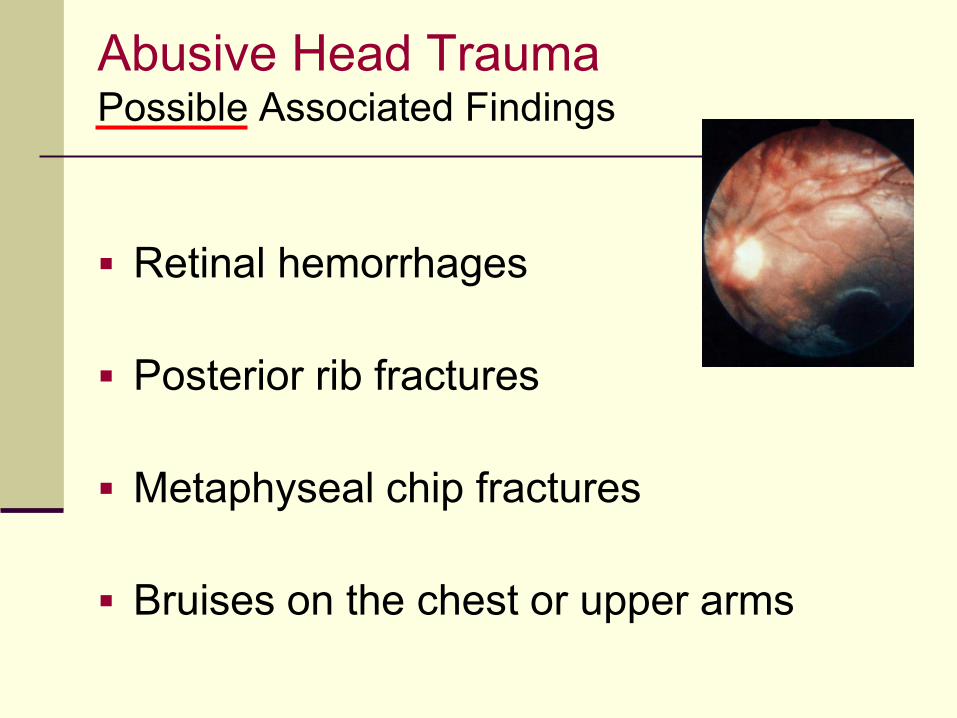
Abusive Head Trauma Possible Associated Findings
Retinal hemorrhages
Posterior rib fractures
Metaphyseal chip fractures
Bruises on the chest or upper arms
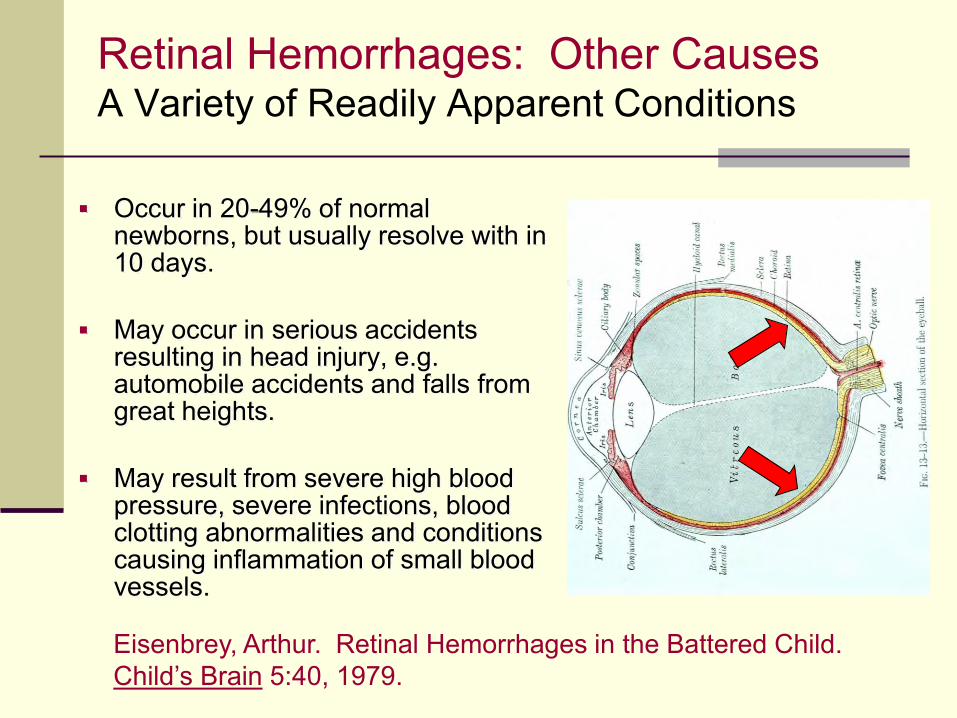
Retinal Hemorrhages: Other Causes A Variety of Readily Apparent Conditions
Occur in 20-49% of normal newborns, but usually resolve with in 10 days.
May occur in serious accidents resulting in head injury, e.g. automobile accidents and falls from great heights.
May result from severe high blood pressure, severe infections, blood clotting abnormalities and conditions causing inflammation of small blood vessels.
Eisenbrey, Arthur. Retinal Hemorrhages in the Battered Child. Child’s Brain 5:40, 1979.
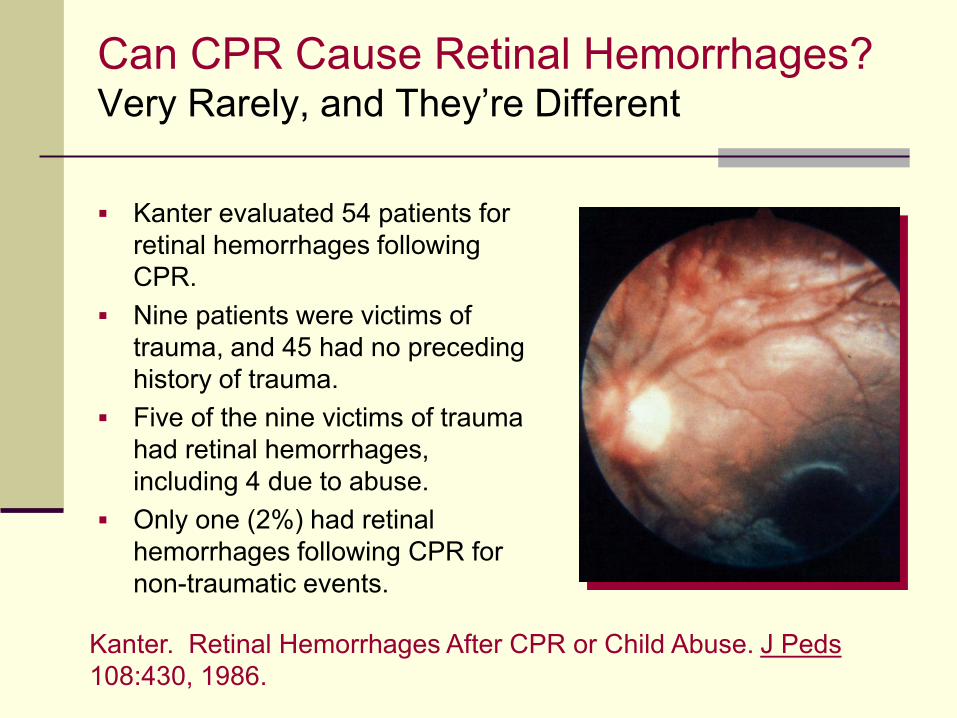
Can CPR Cause Retinal Hemorrhages? Very Rarely, and They’re Different
Kanter evaluated 54 patients for retinal hemorrhages following CPR.
Nine patients were victims of trauma, and 45 had no preceding history of trauma.
Five of the nine victims of trauma had retinal hemorrhages, including 4 due to abuse.
Only one (2%) had retinal hemorrhages following CPR for non-traumatic events.
Kanter. Retinal Hemorrhages After CPR or Child Abuse. J Peds 108:430, 1986.
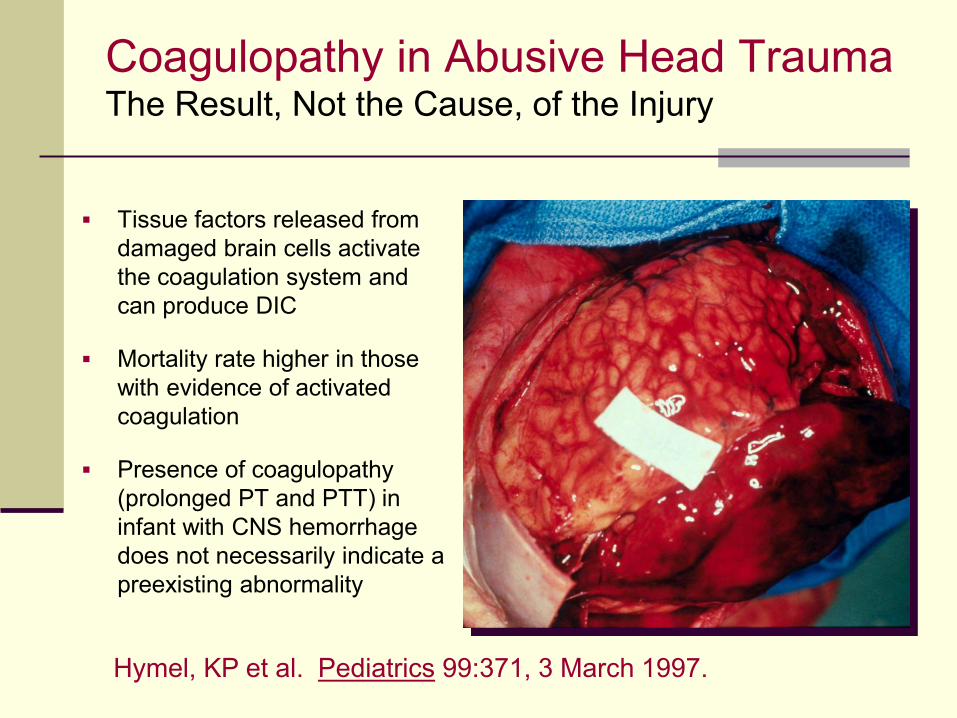
Coagulopathy in Abusive Head Trauma The Result, Not the Cause, of the Injury
Tissue factors released from damaged brain cells activate the coagulation system and can produce DIC
Mortality rate higher in those with evidence of activated coagulation
Presence of coagulopathy (prolonged PT and PTT) in infant with CNS hemorrhage does not necessarily indicate a preexisting abnormality
Hymel, KP et al. Pediatrics 99:371, 3 March 1997.
Bleeding Studies for ICH
• May not be needed if:
• Independently witnessed trauma, abusive or otherwise
• Other medical findings consistent with abuse
• If needed, initial recommended testing panel:
• CBC with differential and platelet count
• PT and PTT
• Factor VIII level
• Factor IX level
• DIC panel (d-dimer and fibrinogen)
Different from Those to Evaluate Bruising
AAP Section on Hematology/Oncology and Committee on Child Abuse and Neglect. Evaluation for Bleeding Disorders in Suspected Child Abuse. Pediatrics 2013: 131; e1314, March 25, 2013.
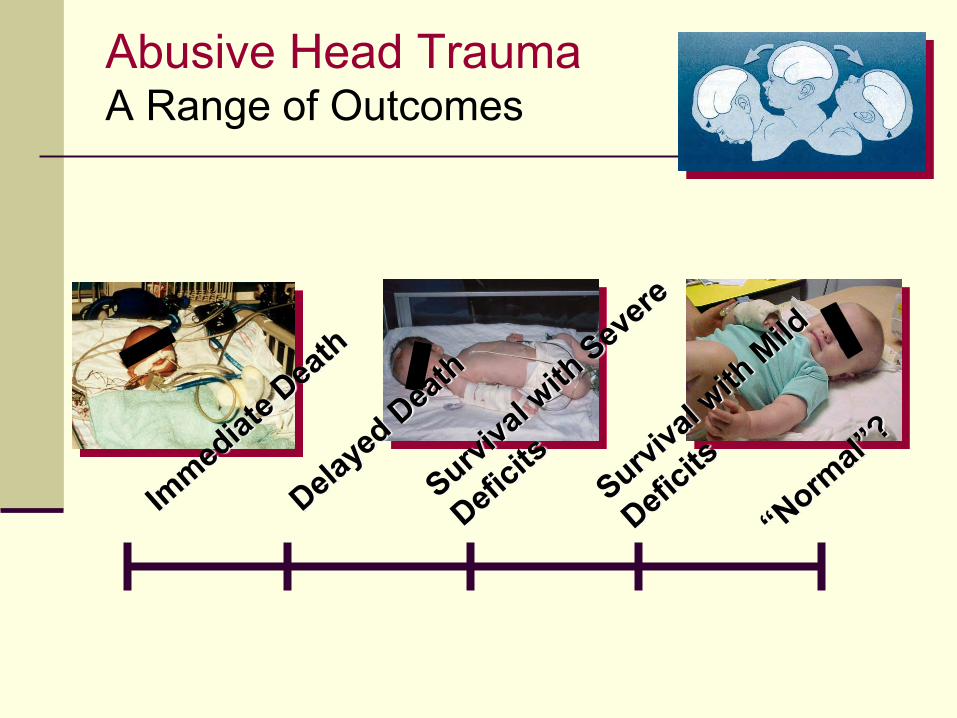
Abusive Head Trauma A Range of Outcomes
Abusive Head Trauma Late Consequences
Partial or total blindness
Developmental delays
Mental retardation
Seizures
Paralysis
Cerebral palsy
Hearing loss
Florida Hospital Association. Children’s Network Special Report, January 1998.
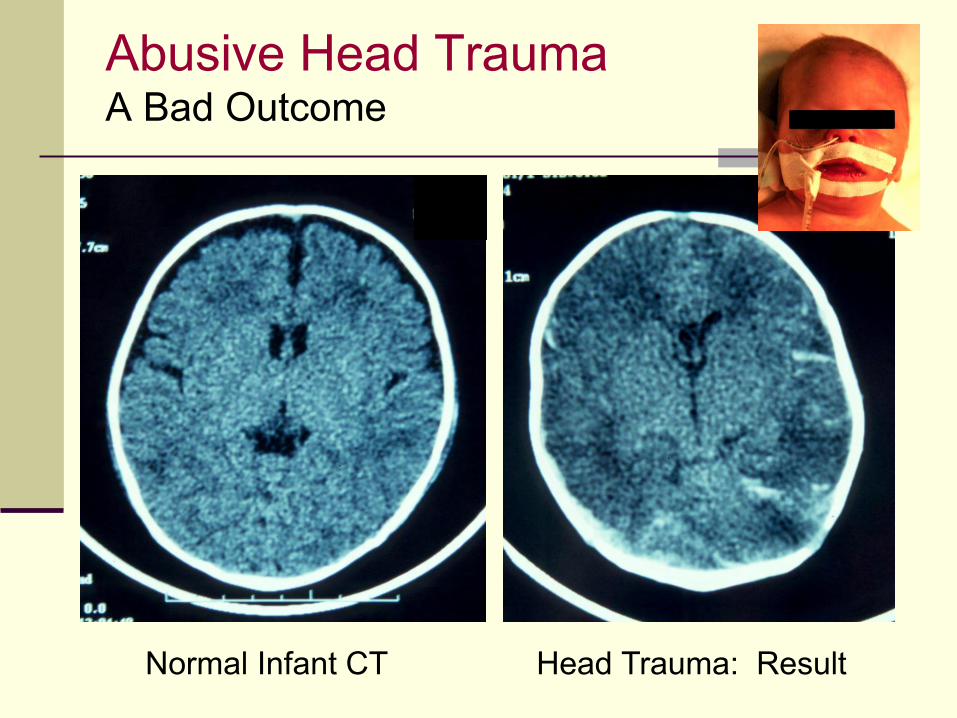
Abusive Head Trauma A Bad Outcome
Normal Infant CT Head Trauma: Result
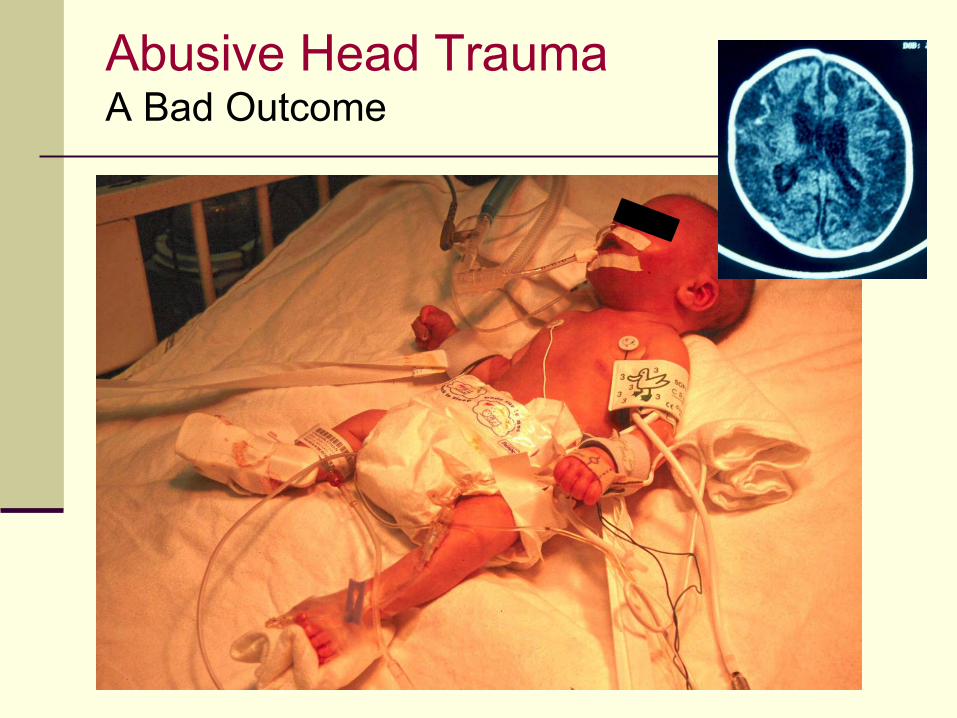
Abusive Head Trauma A Bad Outcome
Caffey, John. The Whiplash Shaken Infant Syndrome: Manual Shaking by the Extremities with Whiplash-Induced Intracranial and Intraocular Bleedings, Linked with Residual Permanent Brain Damage and Mental Retardation. Pediatrics 54:396, 1974.
The Whiplash Shaken Infant Syndrome The Original Description
Some Claim It’s Impossible to Shake a Baby to Death
Duhaime found evidence of blunt impact trauma at autopsy in all of 13 fatal cases of supposed shaken baby syndrome
In a study in which adults shook and/or slammed life-like dolls to measure the forces that could be generated, results suggested that shaking alone could not produce forces necessary to produce damage
Author proposes that the injuries attributed to shaking are in fact due to impact, hence the term “Shaken Impact Syndrome”
Duhaime AC, et al. The Shaken Baby Syndrome. Journal of Neurosurgery 66:409-415, March 1987.
Duhaime’s Biomechanics Study Questionable Assumptions
That mature and immature primate brains have identical biomechanical properties
That repetitive shakes will produce injuries at the same thresholds as single shakes
That the model used is sufficiently true-to-life that it accurately reflects what happens when a real infant is shaken
That shaking is performed in a uniform and predictable manner and that potential variations in technique are not important
Spivak B. “Biomechanics” p. 40 in Frasier L, Rauth-Farley K, Alexander R and Parrish R. Abusive Head Trauma in Infants and Children. G.W. Medical Publishing, St. Lewis, 2006.
Biomechanical Studies Attempts to Measure the Forces Involved
Use dolls and models in an attempt to reproduce and measure the effects of accidental and non-accidental trauma
Purport to prove that it is not possible to shake a baby to death
Purport to prove that it should be common for children to be killed falling out of bed
All present models too seriously flawed to be considered scientifically valid
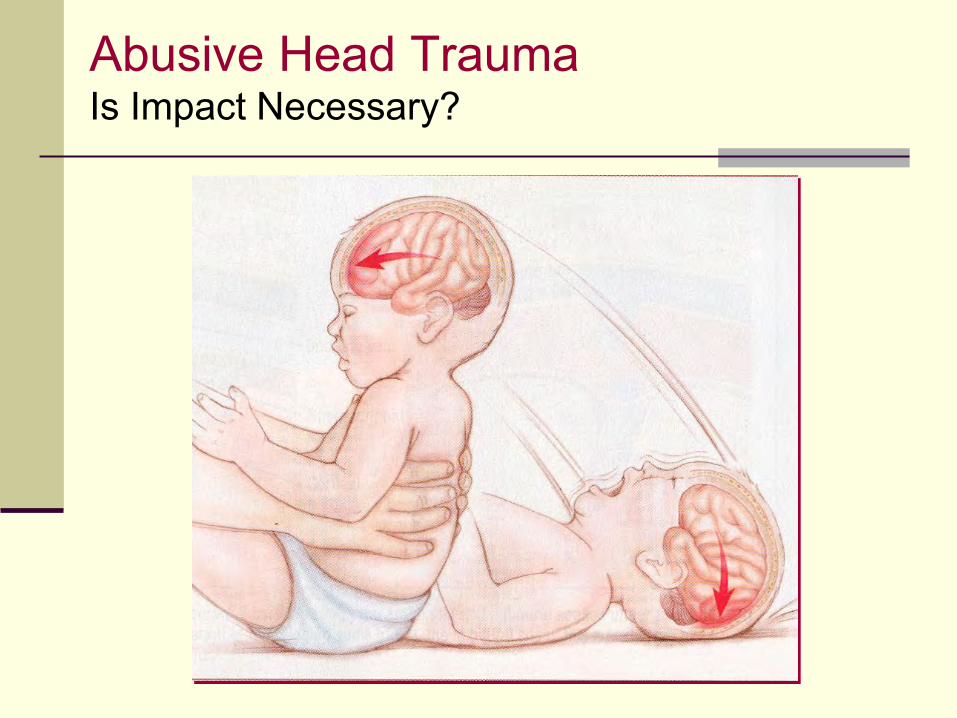
Abusive Head Trauma Is Impact Necessary?
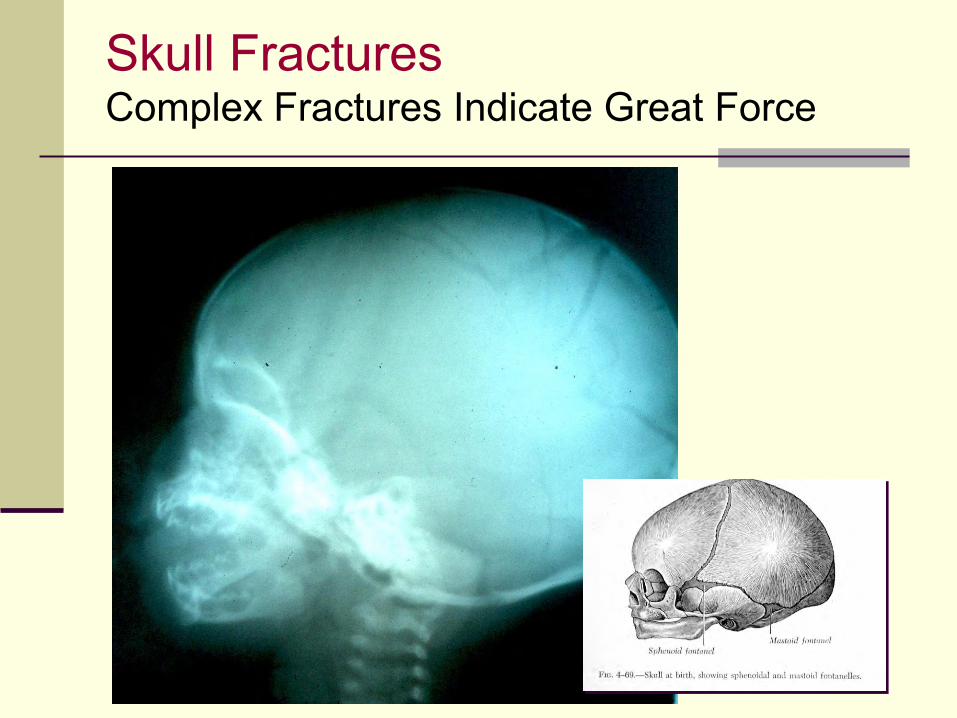
Skull Fractures Complex Fractures Indicate Great Force
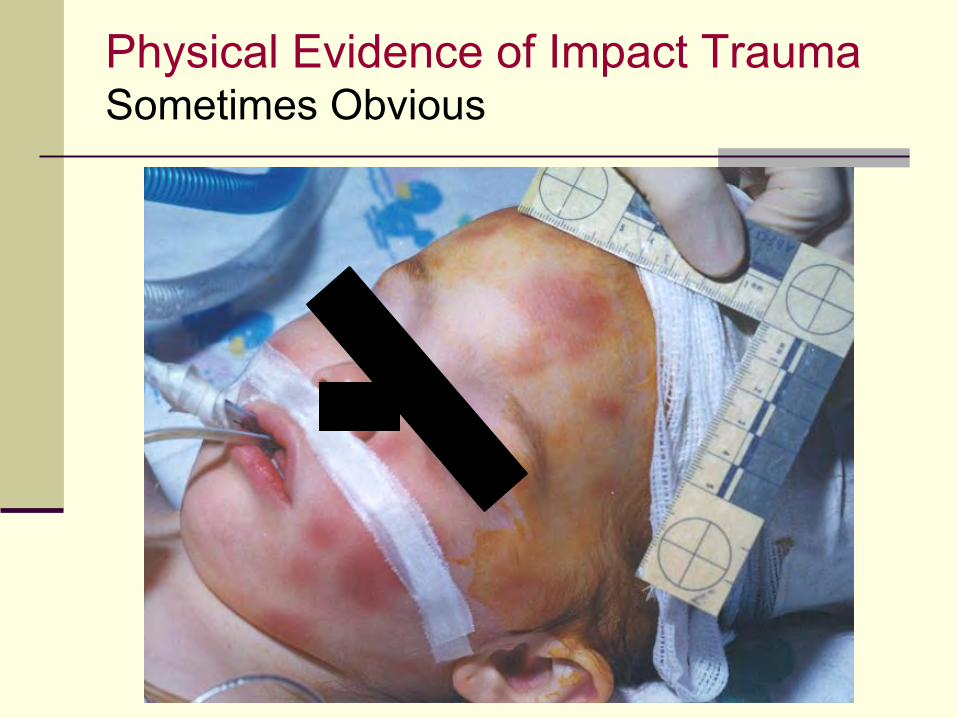
Physical Evidence of Impact Trauma Sometimes Obvious
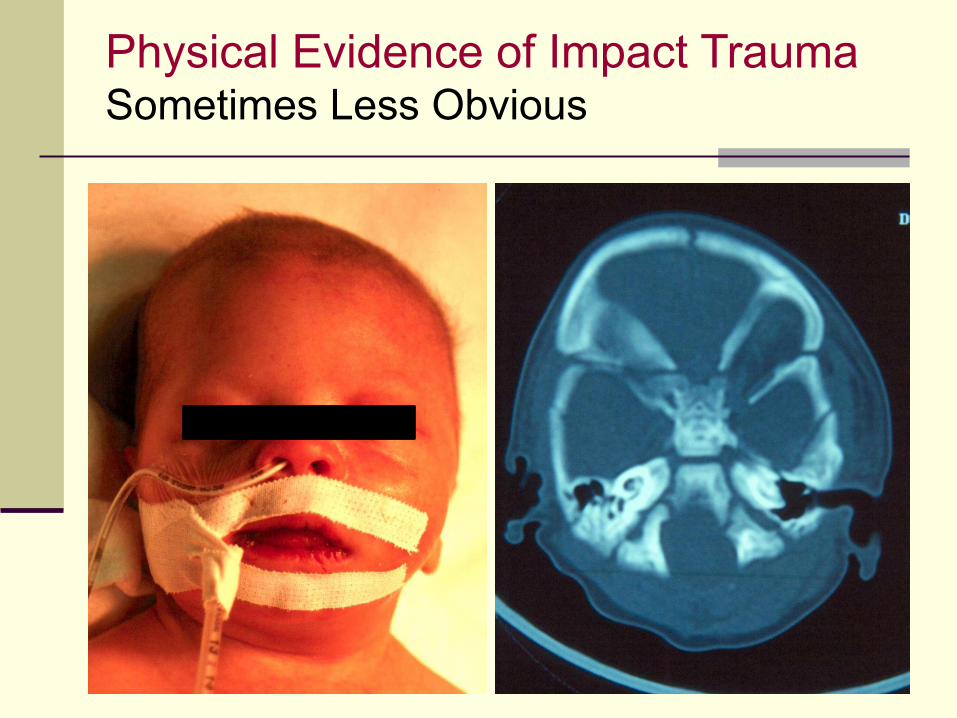
Physical Evidence of Impact Trauma Sometimes Less Obvious
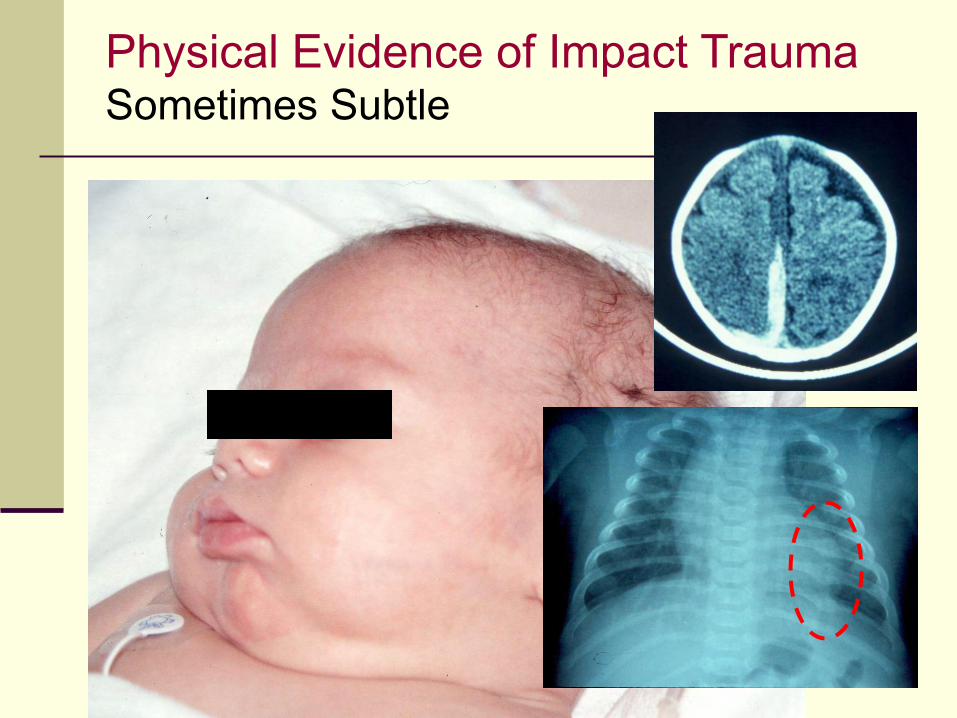
Physical Evidence of Impact Trauma Sometimes Subtle
Physical Evidence of Impact Trauma Sometimes Hidden
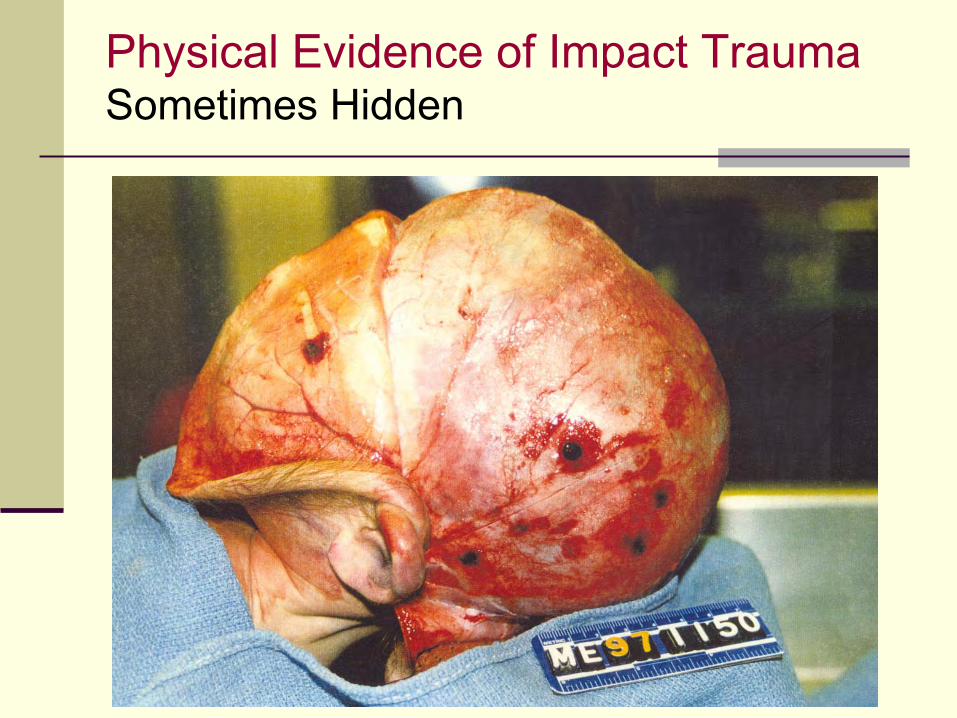
Physical Evidence of Impact Trauma Sometimes Hidden
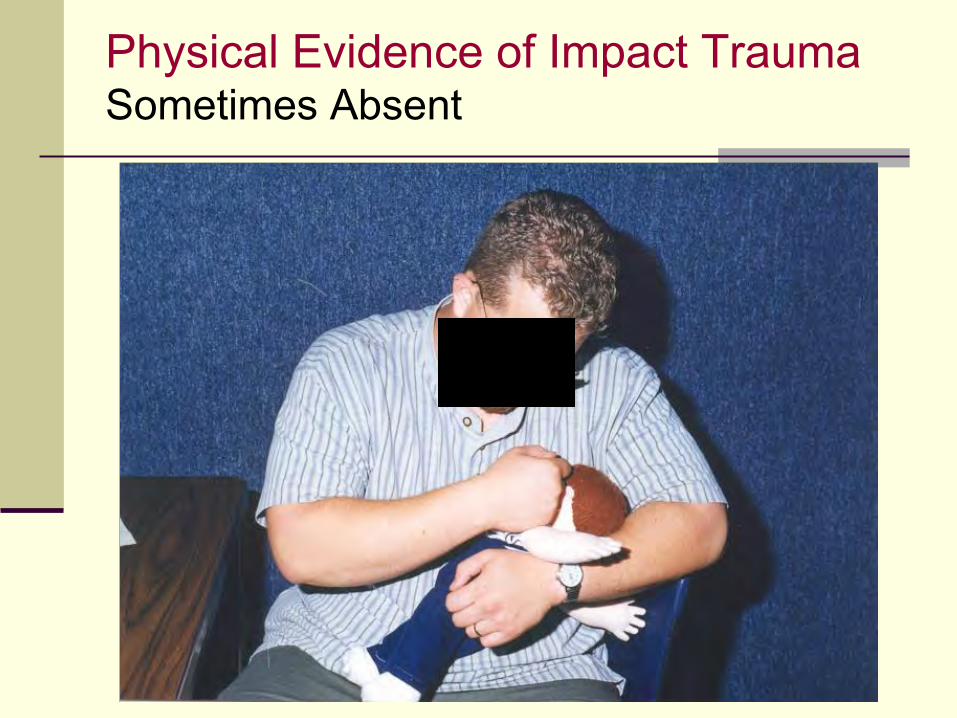
Physical Evidence of Impact Trauma Sometimes Absent
Yes, It Is Possible Shake a Baby to Death
Alexander prospectively examined 24 infants diagnosed with SBS looking carefully for signs of impact trauma
Nine infants died and were autopsied
No evidence of impact trauma was found in 12 infants, including 5 of those autopsied
The death rate and spectrum of intracranial injuries noted was the same in those with and without evidence of impact
Alexander R, et al. Incidence of Impact Trauma with Cranial Injuries Ascribed to Shaking. AJDC 144:724-726, 1990.
Perpetrator Confessions to Shaking Some But Not All Also Impact
Study of 81 cases of Abusive Head Trauma over a 20-year period in which perpetrators admitted to their actions 65% boys, 35% girls Ages 2 weeks to 15 months
Actions described: 71% included shaking 46% shaking alone 29% impact only 25% shaking and impact
None of the children were described as behaving normally after the event.
Starling SP et. al. Analysis of Perpetrator Admissions to Inflicted Traumatic Brain Injury in Children. Arch Ped Adolesc Med 158: 454-8, May 2004.
Shaking Injuries Is There and Upper Age Limit?
30 year old Palestinian man died under interrogation by Israeli security forces. Autopsy revealed acute subdural hemorrhage, diffuse axonal injury and retinal hemorrhages.
Carrigan TD et al. Domestic Violence: The Shaken Adult Syndrome. Journal of Accidental and Emergency Medicine 17:138, 2000.
34 year old woman was treated for retinal hemorrhages, subdural hemorrhage and linear bruises on both upper arms due to domestic violence.
Pounder DJ. Shaken Adult Syndrome. American Journal of Forensic Medicine 18:321, 1997.
Abusive Head Trauma in Infants and Children Recent American Academy of Pediatrics Statement
“Although shaking an infant has the potential to cause neurologic injury, blunt impact or a combination of shaking and blunt impact cause injury as well.”
“Pediatricians should use the term ‘Abusive Head Trauma’ rather than a term that implies a single injury mechanism, such as shaken baby syndrome in their diagnosis and medical communication.”
“Shaken Baby Syndrome is a subset of AHT.”
“The goal of this policy statement is not to detract from shaking as a mechanism of AHT . . .”
AAP Committee on Child Abuse and Neglect. Abusive Head Trauma in Infants and Children. Pediatrics 123:1409, May 2009.
Dating Subdural Hematomas Age Can Not Be Reliably Determined
Result of a systematic of 22 published studies describing 973 SDHs on CT and 4 studies describing 83 SDHs on MRI:
“Most time intervals of the different appearances of SDHs onCT and MRI are broad and overlapping. Therefore CT or MRI findings cannot be used to accurately date SDHs.”
Sieswerda-Hoogendoorn T, et.al. Age Determination of Subdural Hematomas with DT and MRI: A Systematic Review. Eur J Radiol 83:1257-68, July 2014.
Result of survey of current practice among radiologists in the Netherlands regarding the dating of subdural hematomas in children:
“The results demonstrate that there is a considerable practice variation among . . . Radiologists regarding the age determination of subdural hematomas. This implicates that dating of subdural hematomas is not suitable to use in court, as no uniformity among experts exists.”
Postema FA, et. al. Age Determination of Subdural Hematomas: Survey Among Radiologists. Emerg Radiol 21:349-58, August 2014.
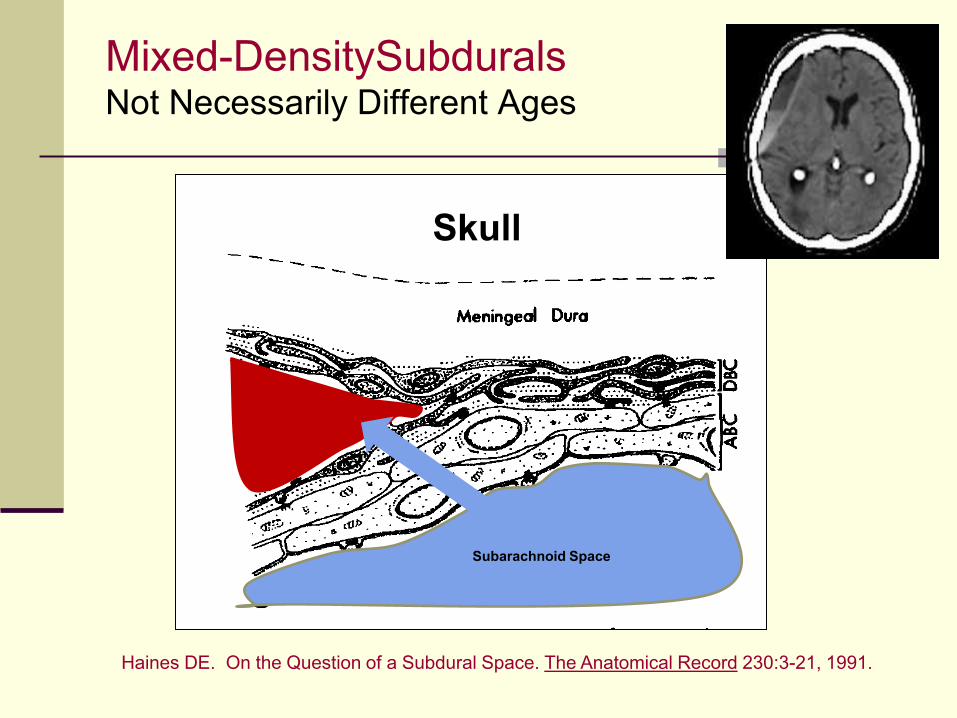
Mixed-DensitySubdurals Not Necessarily Different Ages
Haines DE. On the Question of a Subdural Space. The Anatomical Record 230:3-21, 1991.
Subarachnoid Space
Skull
Fatally Injured Children They Don’t Behave Normally
Willman, et. al. reviewed 138 accidental fatalities involving head injuries
With the exception of one acute epidural hematoma, no child with a fatal head injury acted normal after the injury
When infants suffer life-threatening head injuries, it may be presumed that:
The injury occurred after they were last seen appearing well
The injury was inflicted by the person caring for them at the time they became symptomatic
Willman KY, et. al. Restricting the Time of Injury in Fatal Inflicted Head Injuries. Child Abuse & Neglect 24:929-939, 1997.
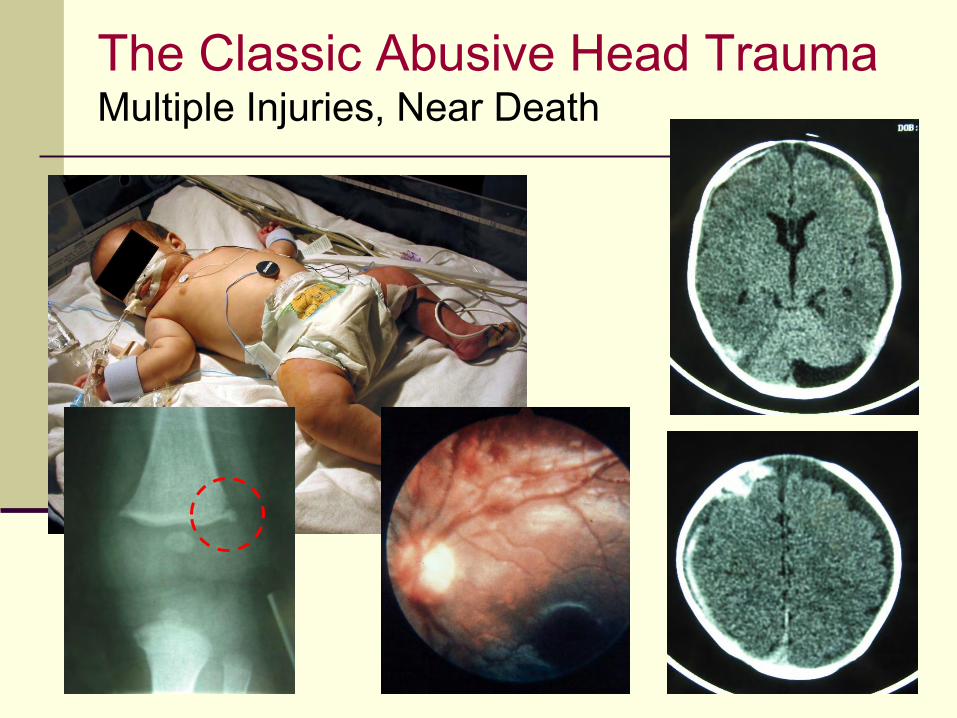
The Classic Abusive Head Trauma Multiple Injuries, Near Death
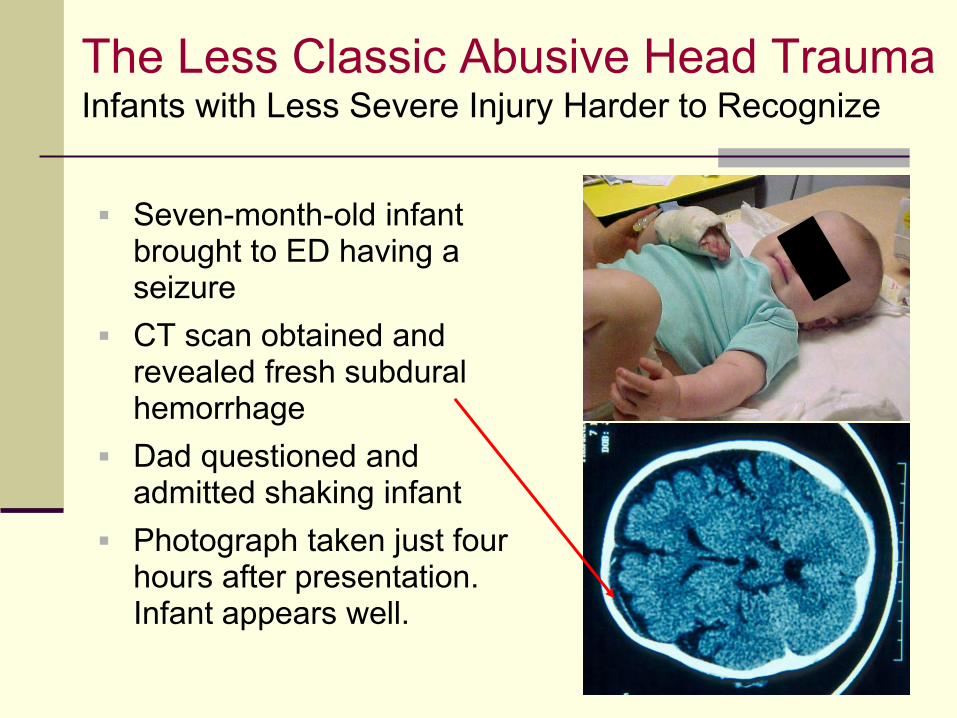
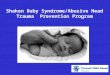
The Less Classic Abusive Head Trauma Infants with Less Severe Injury Harder to Recognize
Seven-month-old infant brought to ED having a seizure
CT scan obtained and revealed fresh subdural hemorrhage
Dad questioned and admitted shaking infant
Photograph taken just four hours after presentation. Infant appears well.
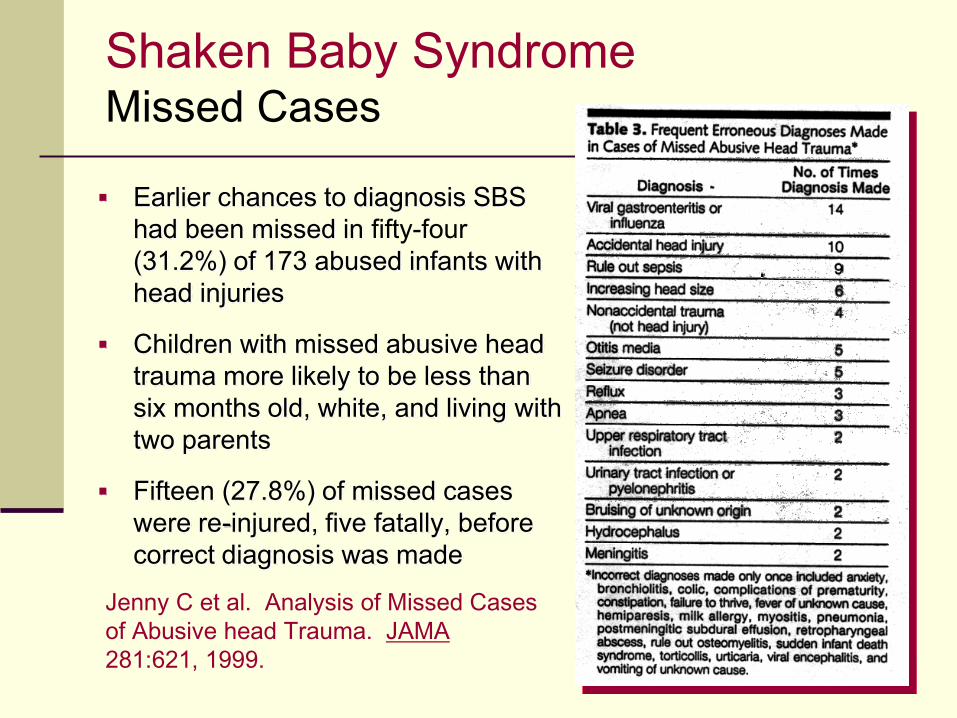
Shaken Baby SyndromeMissed Cases
Earlier chances to diagnosis SBS had been missed in fifty-four (31.2%) of 173 abused infants with head injuries
Children with missed abusive head trauma more likely to be less than six months old, white, and living with two parents
Fifteen (27.8%) of missed cases were re-injured, five fatally, before correct diagnosis was made
Jenny C et al. Analysis of Missed Cases
of Abusive head Trauma. JAMA
281:621, 1999.
Time of Onset of Head injury Symptoms Sometimes Not Possible to Say
Neurological injuries resulting from shaking/impact trauma represent a spectrum of severity
Less severely injured infants may have a more poorly defined time of symptom onset
Identifying the perpetrator in cases with the gradual onset of milder symptoms may be difficult
Injuries Resulting from Short Vertical Falls Rarely Life-Threatening
Series of 246 children age 5 or less who had suffered falls from a height of 60 inches or less 161 had fallen from beds or sofas at home 85 had fallen from beds or stretchers in the hospital
Results: 80% suffered no injury 17 % suffered bumps and bruises There were 3 fractured clavicles, 1 fractured humerus
and 2 simple linear skull fractures No child suffered a severe head or CNS injury
Helfer RE et al. Injuries Resulting When Small Children Fall Out of Bed. Pediatrics 60:533-535. October 1977.
Injuries Resulting from Short Vertical Falls Rarely Life-Threatening
Series of 106 children with history of falls witnessed by a second person other than the caretaker No injuries in 15, including 7 who fell more than 10 feet Bruises, abrasions and simple fractures in 77, including
43 who fell more than 10 feet Severe injuries (intracranial hemorrhages, cerebral
edema, etc.) in 14 who fell between 5 and 40 feet No life-threatening injuries in the 3 who fell less than 10
feet Only death in series was a child who fell from 70 feet
Williams RA. Injuries in Infants and Small Children Resulting from Witnessed and Corroborated Free Falls. J. Trauma 31:1350-1352, 1991.
Injuries Resulting from Short Vertical Falls Rarely Life-Threatening
Series of 207 children less than 6 years of age who fell out of cribs and beds in the hospital 25 inches from beds 41 inches when climbed over bed rails to fall 32 inches from cribs 54 inches when climbed over crib rails
No injury: 86% Mild injury: 14%, including one linear skull fracture and one
fractured clavicle No serious, multiple, visceral or life-threatening injuries
Lyons TJ and Oates RK. Falling Out of Bed: A Relatively Benign Ocurrence. Pediatrics 92:125,1993.
Series of 167 children less than 10 months old who fell from heights of < 48 inches
Results 85% suffered minor or no injury 15% suffered long bone or skull fractures
The only 2 infants with intracranial hemorrhage were discovered to be victims of abuse
No child suffered an intracranial hemorrhage from falling off a bed or being dropped
Tarantino CA et. al. Short Vertical Falls in Infants. Pediatric Emergency Care 15:5, 1999.
Injuries Resulting from Short Vertical Falls Rarely Life-Threatening
Injuries Resulting from Falling Down Stairs Rarely Life-Threatening
Joffe and Ludwig reviewed 363 consecutive pediatric patients seen in the ED who had fallen down stairs
Most injuries were minor
Only 3% were injured sufficiently to be admitted to the hospital
No patient had life-threatening injuries, and none required intensive care
Joffe M and Ludwig S. Stairway Injuries in Children. Pediatrics 82:457, 1988.
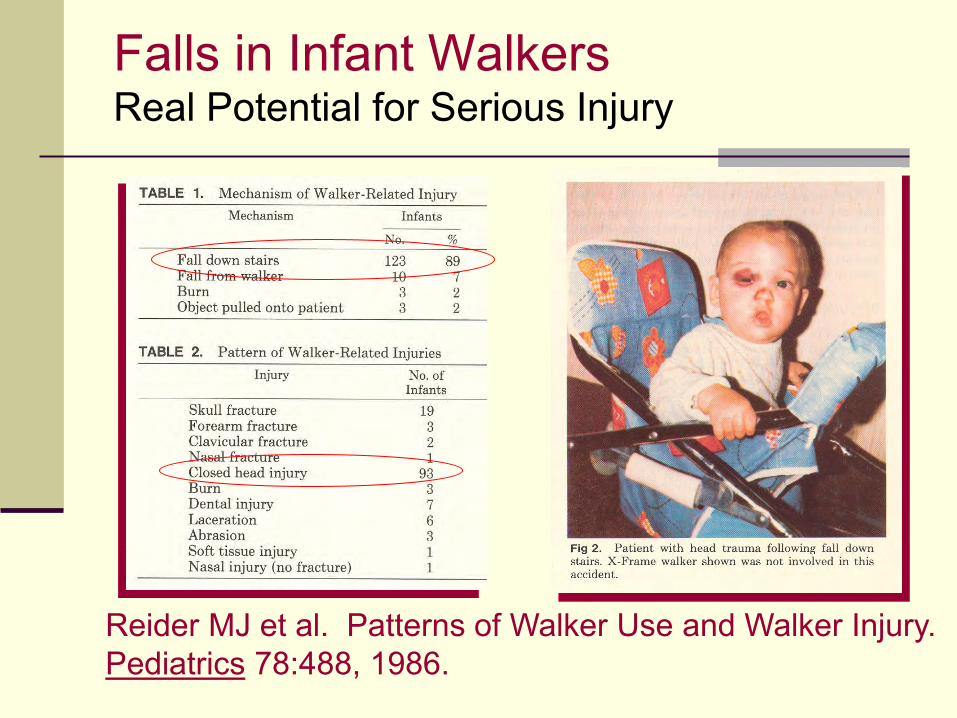
Falls in Infant Walkers Real Potential for Serious Injury
Reider MJ et al. Patterns of Walker Use and Walker Injury. Pediatrics 78:488, 1986.
Serious Head Injuries The Short Fall Defense
Aoki reported a series of 26 infants who suffered acute subdural hematomas following minor head trauma in household falls
Most patients presented with seizures Retinal hemorrhages were present in all
patients Most common mechanism of injury was a fall
backward while sitting or standing with the head hitting a soft item such as a tatami mat
Aoki N and Masuzawa H. Infantile Acute Subdural Hematoma. Journal of Neurosurgery 61:273-280, August 1984.
The Short Fall Defense The Current Leading Proponent
Review of 1988-1999 U.S. Consumer Product Safety Commission data base for head injuries associated with use of playground equipment
Identified 18 fall-related deaths due to head injury Ages: 12 months - 13 years Heights: 2 - 10 feet Twelve of 18 witnessed by non-caretakers Twelve had lucid intervals Four of 16 examined had bilateral retinal hemorrhages
Plunkett J. Fatal Pediatric Head Injuries Caused by Short-Distance Falls. American Journal of Forensic Medicine and Pathology 22:1-12, 2001.
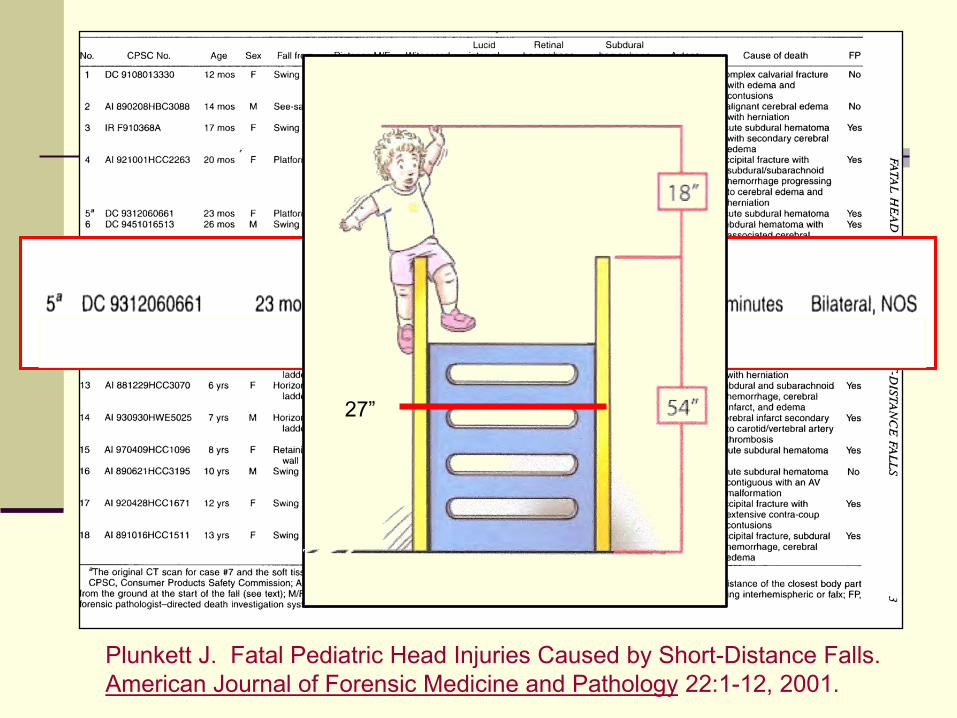
Plunkett J. Fatal Pediatric Head Injuries Caused by Short-Distance Falls. American Journal of Forensic Medicine and Pathology 22:1-12, 2001.
27”
Plunkett’s Short Fall Defense Characteristics of Cited Cases
History of significant fall from playground equipment
Death resulting from effects of mass lesions
Vascular accidents Abnormalities of blood coagulation system Uncorroborated history
Plunkett J. Fatal Pediatric Head Injuries Caused by Short-Distance Falls. American Journal of Forensic Medicine and Pathology 22:1-12, 2001.
Actual Risk of Death from Short Falls Best Estimates
Authors reviewed multiple sources of data related to deaths from short distance falls (less than 4.7 feet) in young children
Review of death certificates from cases identified in the State of California Epidemiology and Prevention for Injury Control Branch database yielded an incidence of 0.48 cases per 1 million children per year.
Data from the CDC database concerning children less than 4 years old indicated an “all fall” (not stratified by height) incidence of 3 cases per 1 million children per year.
The National Consumer Product Safety Commission database indicated an incidence of 0.625 cases per 1 million children per year.
The best estimate for risk of death in an infant or young child from a short fall is less than one in a million young children per year.
Chadwick DL, et. al. Annual Risk of Death from Short Falls Among Young Children. Pediatrics 121:1213, 2008.
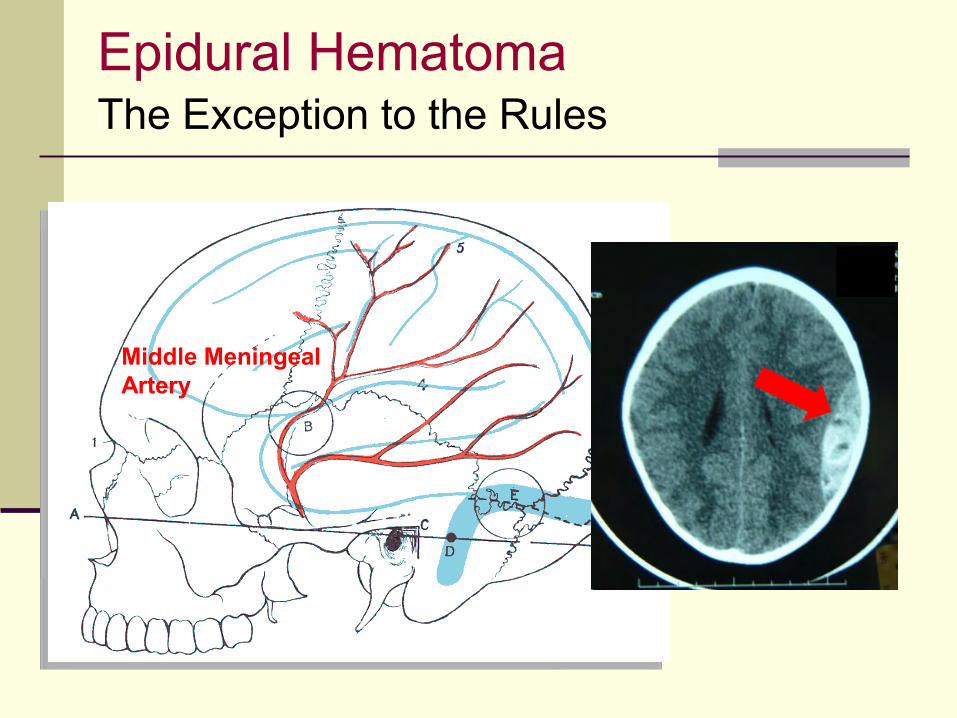
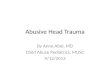
Epidural Hematoma The Exception to the Rules
Middle Meningeal Artery
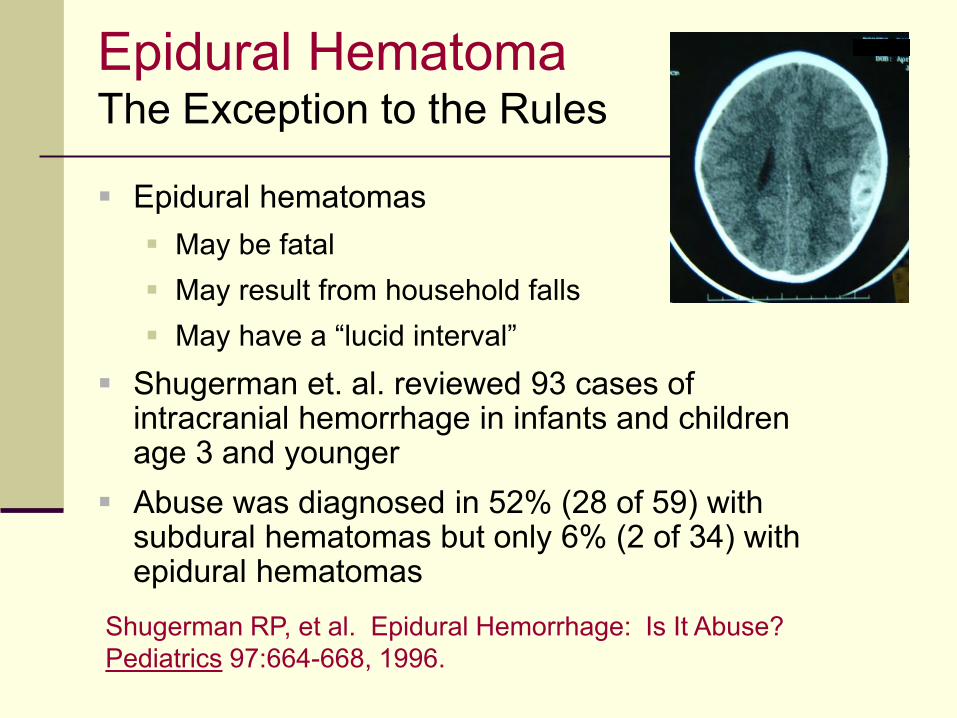
Epidural Hematoma The Exception to the Rules
Epidural hematomas May be fatal May result from household falls May have a “lucid interval”
Shugerman et. al. reviewed 93 cases of intracranial hemorrhage in infants and children age 3 and younger
Abuse was diagnosed in 52% (28 of 59) with subdural hematomas but only 6% (2 of 34) with epidural hematomas
Shugerman RP, et al. Epidural Hemorrhage: Is It Abuse? Pediatrics 97:664-668, 1996.
The “Au Pair Case” Flawed Defenses Offered
The “SODDI Defense” Child is injured by one person but continues to
act well Suddenly decompensates while with another
caretaker
The “Bleed/Re-Bleed” Defense Minor head injury causes subdural hematoma Pseudomembrane forms with neovascularization Second, relatively minor head injury causes more
serious bleeding
Re-Bleeding The Reality
Small blood vessels (neo-vascularization) develop in the septations or membranes that form within chronic subdural hematomas May re-bleed with little or no additional trauma May result in mixed attenuation collections
Such episodes of re-bleeding will be asymptomatic and will not result in acute deterioration of the child’s neurological status
Bleeding will not occur at sites remote from the original subdural or in the subarachnoid space Frasier L, Rauth-Farley K, Alexander R and Parrish R. Abusive
Head Trauma in Infants and Children. G.W. Medical Publishing, St. Lewis, 2006.
“Temporary Brittle Bone Disease” Paterson Now Relates It to Subdurals
Dr. Paterson and Monk (of the University of Dundee School of Business) report 20 infants with multiple fractures, subdural hematomas and retinal hemorrhages that they believe are due to “Temporary Brittle Bone Disease.”
They believe the findings are unlikely to be due to abuse because: There was no “clinical evidence of injury commensurate with the
fracture”, i.e., no bruising “Metaphyseal fractures, when present, were often symmetrical.” Subdural hemorrhages were accepted as being due to falls or
birth injury Included cases in which courts removed children from the parents’
care and/or a parent was convicted in criminal proceedings for charges including murder.
Paterson CR, Monk EA. Temporary Brittle Bone Disease: Association with Intracranial Bleeding. J Pediatr Endocr Met 2013, pp. 1-10.
Geddes proposed that craniocervical trauma occurring “without impact or considerable force” could cause apnea, resulting in hypoxia and cerebral edema
Increased central venous pressure would then cause blood to leak from intracranial and retinal veins
Subdural hematomas and retinal hemorrhages could therefore be a “phenomenon of immaturity,” not abuse
“The Geddes Hypothesis” Hypoxia as Cause of SDH and RH
Geddes Jf et al. Neuropathol Appl Neurobiol 2003 Feb: 29(1):14-22.
Geddes called to testify in Court of Appeals in London in June 2005
Testified her hypothesis was speculative, meant to stimulate debate and not to be taken as fact
Judges found “unified hypothesis can no longer be regarded as a credible or alternative cause of the triad of injuries” of SBS but “excessive trauma” needed
Appeals in four cases then considered in light to these findings
Geddes Disavows Her Hypothesis Says It Was Not Meant to Be Taken As Fact
Richards PG et al. Shaken Baby Syndrome: Before the Court of Appeal. Arch Dis Child 2006;91, 205-206.
Overcoming False Defenses A Valuable Resource
National District Attorneys Association: ndaa.org/pdf/Abusive Head Trauma
Abusive Head Trauma Summary
Abusive Head Trauma is a common cause of serious and fatal injury to infants and young children.
It is very rare for infants and children to suffer life-threatening head injuries in household falls.
Medical providers need to know about false explanations commonly offered by the defense explain serious head injuries.
The term “Abusive Head Trauma” is replacing the term “Shaken Baby Syndrome” since it can sometimes be difficult to determine which infants have only been shaken and which have been shaken and slammed.
Infants do not behave normally after life-threatening head injuries have been inflicted. This is useful in determining who is responsible for the injury.
Recommended