Absence of Flow-Limiting Coronary Artery Disease Among Patients Undergoing Emergent Cardiac
Catheterization For ST Segment Elevation Myocardial Infarction in the
National Cardiovascular Data Registry CathPCI Registry:
Implications for Primary Angioplasty Programs Kalon KL Ho, H Vernon Anderson, Richard E
Shaw, Lloyd W Klein, James H Beachy, Christopher P Cannon, Harlan M Krumholz, Susan
Fitzgerald, Anthony Hermann, Kristi Mitchell, John Rumsfeld,
Ralph G Brindis, on behalf of the National Cardiovascular Data Registry
Author Disclosure InformationThe following relationships exist related to this presentation:• KKL Ho: none• HV Anderson: none • RE Shaw: none• LW Klein: none • JH Beachy: none• HM Krumholz: none • S Fitzgerald: none• A Hermann: none • K Mitchell: none• J Rumsfeld: none • RG Brindis: none•CP Cannon: significant research grants from
Accumetrics, AstraZeneca, Bristol-Myers Squibb, Glaxo Smith Kline, Merck, Sanofi-Aventis, Schering Plough
Background•Many hospitals have established primary
angioplasty programs with a goal of providing consistently timely reperfusion for patients with suspected acute ST segment elevation myocardial infarction (STEMI).
•As the locus of control for activation of the cardiac catheterization laboratory (CCL) moves from the cardiologist to the emergency department (ED) and even to pre-hospital activation by emergency medical services, concerns have been raised about “false positive” activations of the primary angioplasty team.
Objective•Estimate how often flow-limiting coronary artery disease (CAD) was NOT found among patients undergoing emergent cardiac catheterization for presumed STEMI in the National Cardiovascular Data Registry (NCDR) CathPCI Registry, a large multi-center cardiac catheterization and percutaneous coronary intervention (PCI) quality improvement and outcomes database.
Study Population•From 01 January 2005 – 31 December 2006
–120,676 diagnostic coronary angiograms –614 hospitals
•Procedural status coded as –Emergent
•Ongoing ischemic dysfunction, or•Cardiogenic shock
–Salvage•CPR en route
Study Population
• Since the results of the angiogram (e.g.,
no CAD) can be used to determine
retrospectively that STEMI was not the
indication for the procedure, we did NOT
use the admission symptom presentation
to identify cases of suspected STEMI.
Results•Procedural status: 98.7% emergent
1.3% salvage
•Angiographic results: 91.9% CAD* 8.1% no CAD* 4.9% no stenoses
* CAD: 50% diameter stenosis in an epicardial coronary artery >2 mm in diameter
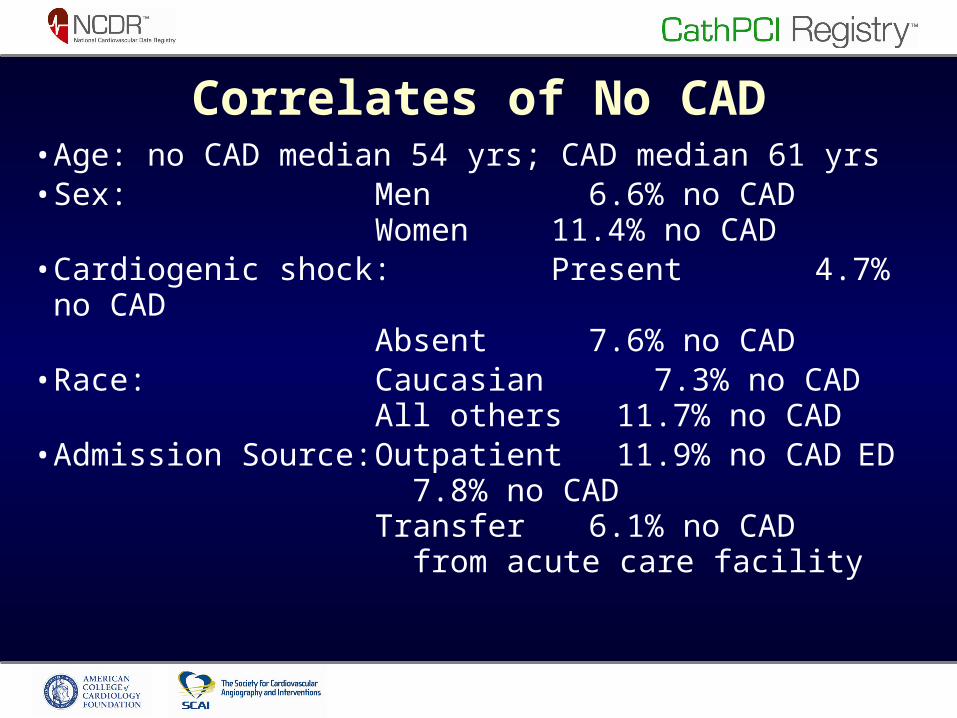
Correlates of No CAD•Age: no CAD median 54 yrs; CAD median 61 yrs•Sex: Men 6.6% no CAD
Women 11.4% no CAD•Cardiogenic shock: Present 4.7% no CAD
Absent 7.6% no CAD•Race: Caucasian 7.3% no CAD
All others 11.7% no CAD•Admission Source: Outpatient 11.9% no CADED
7.8% no CADTransfer 6.1% no CAD from acute care facility
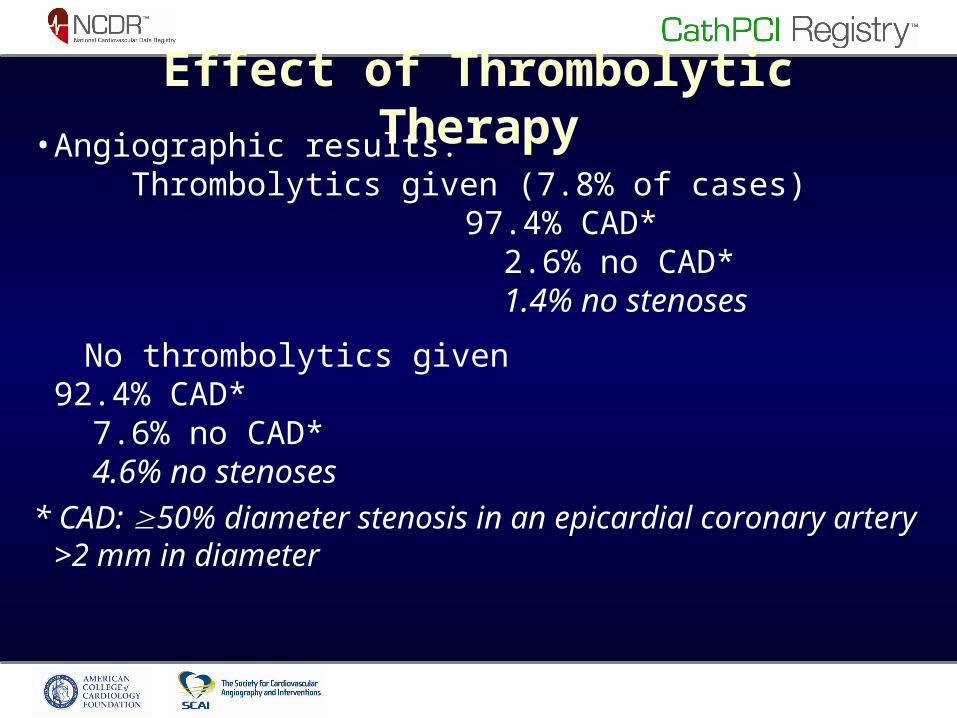
Effect of Thrombolytic Therapy•Angiographic results: Thrombolytics given (7.8% of cases)
97.4% CAD* 2.6% no CAD* 1.4% no stenoses
No thrombolytics given 92.4% CAD* 7.6% no CAD* 4.6% no stenoses
* CAD: 50% diameter stenosis in an epicardial coronary artery >2 mm in diameter
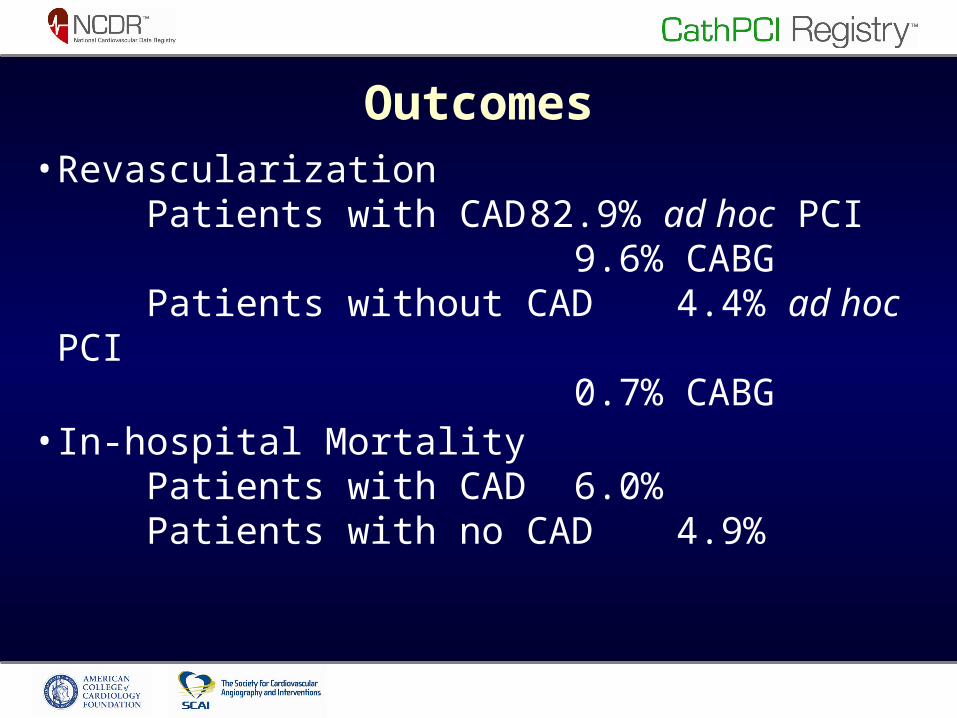
Outcomes•Revascularization Patients with CAD 82.9% ad hoc PCI
9.6% CABG Patients without CAD 4.4% ad hoc PCI
0.7% CABG•In-hospital Mortality Patients with CAD 6.0% Patients with no CAD 4.9%
Limitations•Self-reported data without 100% auditing•Information not uniformly available on suspected STEMI as a specific indication for angiography and other clinical details (e.g., the extent or location of electrocardiographic abnormalities, biomarker results, cocaine use, left ventricular hypertrophy, and the final clinical diagnoses)
•The presence of CAD with 50% diameter stenosis does not mean that the patient was necessarily suffering a STEMI
Conclusions•Among patients undergoing emergent or salvage diagnostic cardiac catheterization nationwide in the NCDR CathPCI Registry (>120,000 cases):
– Finding NO angiographically-apparent flow-limiting CAD was uncommon (<10%).
•No clinical finding or test will perfectly discriminate STEMI from “STEMI mimics”
– Current clinical practice appears to activate primary PCI teams with reasonable specificity.
Acknowledgements
The authors wish to acknowledge the invaluable contributions of
•The participants of the CathPCI Registry•The analytical team at the Duke Clinical Research Institute (Fang-Shu Ou, Barbara Lytle, Matthew Roe)
Recommended

















